Patient Protection and Affordable Care Act, HHS Notice of Benefit and Payment Parameters for 2027; and Basic Health Program
This final rule contains provisions to improve implementation of the Patient Protection and Affordable Care Act, including payment parameters and provisions related to the HHS-o...
Centers for Medicare & Medicaid Services (CMS), Department of Health and Human Services (HHS).
ACTION:
Final rule.
SUMMARY:
This final rule contains provisions to improve implementation of the Patient Protection and Affordable Care Act, including payment parameters and provisions related to the HHS-operated risk adjustment and risk adjustment data validation (HHS-RADV) programs, as well as 2027 user fee rates for issuers offering qualified health plans (QHPs) through Federally-facilitated Exchanges (FFEs) and State-based Exchanges on the Federal platform (SBE-FPs). This final rule also includes provisions related to civil money penalties (CMPs) for noncompliant issuers and other responsible entities; standards governing agents, brokers, and web-brokers; the expansion and codification of hardship exemption eligibility; implementation of the State Exchange Improper Payment Measurement (SEIPM); provider access standards and essential community provider standards for QHP certification; QHP certification of non-network plans; a prohibition on issuers from including routine non-pediatric dental services as an Essential Health Benefit (EHB); requirements related to defrayal for the cost of any State-required benefits in addition to the EHB; cost-sharing flexibilities for catastrophic and individual market bronze plans; establishment of catastrophic plans with plan terms of up to 10 consecutive plan years; QHP issuer quality improvement strategies (QISs); and revisions affecting which enrollees are included in Federal Basic Health Program (BHP) payment calculations to States. This final rule also includes amendments to implement certain provisions of the Working Families Tax Cut (WFTC) legislation.
DATES:
These regulations are effective on July 20, 2026.
FOR FURTHER INFORMATION CONTACT:
Jeff Wu, (301) 492-4305, Rogelyn McLean, (410) 786-1524, Grace Bristol, (410) 786-8437, for general information.
Ayesha Anwar, (301) 448-3625, or Joshua Paul, (301) 492-4347, for matters related to HHS-operated risk adjustment and HHS-operated risk adjustment data validation.
Aaron Franz, (410) 786-8027 for matters related to user fees.
Brian Gubin, (410) 786-1659, for matters related to agent, broker, and web-broker guidelines.
Zarin Ahmed, (301) 492-4400, for matters related to enrollment of qualified individuals into QHPs and termination of Exchange enrollment or coverage for qualified individuals.
Hannah Armbruster Hill, (301) 492-4343, for matters related to certification standards for QHPs, cost-sharing requirements, and the Actuarial Value Calculator.
Kelly Carda, (312) 886-5210, or Cassandra Thompson, (667) 414-0870, for matters related to Provider Access standards.
Ariana Koenitzer, (410) 786-0724, or Samantha Nguyen Kella, (816) 426-6339, for matters related to Essential Community Provider Standards.
Ariana Koenitzer, (410) 786-0724, or Cassandra Thompson, (667) 414-0870, for matters related to QHP Certification of Non-Network Plans.
Nikolas Berkobien, (667) 290-9903, for matters related to standardized plan options, non-standardized plan option limits and exceptions.
Jenny Chen, (301) 492-5156, or Shilpa Gogna, (301) 492-4257, for matters related to State Exchange and State Exchange Blueprint requirements.
Rebecca Braun-Harrison, (667) 290-8846, or Nia Blasingame, (470) 890-4178, for matters related to civil money penalties of issuers and non-Federal governmental group health plans.
Preeti Hans, (301) 492-5144, for matters related to the Quality Improvement Strategy.
Mary Beth Hance, 410-786-4299, for matters related to the Basic Health Program.
Christina Whitefield, (301) 492-4172, for matters related to the medical loss ratio (MLR) program.
David Mlawsky, (410) 786-6851, for matters related to catastrophic plans with multi-year plan terms.
Jessica Veffer, (301) 492-4827, for matters related to expanding hardship exemptions for individuals ineligible for APTC or CSRs due to projected household income.
SUPPLEMENTARY INFORMATION:
I. Executive Summary
We are finalizing changes to the provisions and parameters implemented through prior rulemaking to implement the Patient Protection and Affordable Care Act and are also finalizing updates to implement new provisions.[1]
These requirements are published under the authority granted to the Secretary of HHS (the Secretary) by the Affordable Care Act and the Public Health Service (PHS) Act.[2]
In this document, we are finalizing changes related to some of the Affordable Care Act provisions and parameters we previously implemented under the authority granted to the Secretary by Public Law (Pub. L.) 119-21, which CMS refers to as the Working Families Tax Cut (WFTC) legislation.[3]
Our goal with these requirements is providing quality, more affordable coverage to consumers while minimizing administrative burden and ensuring program integrity. The changes finalized in this rule are also intended to enhance the role of States in these programs, provide issuers and States with additional flexibilities, reduce unnecessary regulatory burden on interested parties, and improve affordability.
II. Background
A. Legislative and Regulatory Overview
Title I of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) added a new title XXVII to the PHS Act to establish various reforms to the group and individual health insurance markets. These provisions of the PHS Act were later augmented by other laws, including the Affordable Care Act. Subtitles A and C of title I of the Affordable Care Act reorganized, amended, and added to the provisions of part A of title XXVII of the PHS Act relating to group health plans and health insurance issuers in the group and individual markets. The term “group health plan” includes both insured and self-insured group health plans.
In the upcoming sections, we summarize sections of the PHS Act,
( printed page 29527)
Affordable Care Act, and WFTC legislation that are relevant to this final rule.
Section 1301(a)(1)(B) of the Affordable Care Act directs all issuers of qualified health plans (QHPs) to cover the Essential Health Benefit (EHB) package described in section 1302(a) of the Affordable Care Act, including coverage of the services described in section 1302(b) of the Affordable Care Act, adherence to the cost-sharing limits described in section 1302(c) of the Affordable Care Act, and meeting the Actuarial Value (AV) levels established in section 1302(d) of the Affordable Care Act. Section 2707(a) of the PHS Act, which is effective for plan or policy years beginning on or after January 1, 2014, extends the requirement to cover the EHB package to non-grandfathered individual and small group health insurance coverage, irrespective of whether such coverage is offered through an Exchange. In addition, section 2707(b) of the PHS Act directs non-grandfathered group health plans to ensure that cost sharing under the plan does not exceed the limitations described in section 1302(c)(1) of the Affordable Care Act.
Section 1302 of the Affordable Care Act provides for the establishment of an EHB package that includes coverage of EHB (as defined by the Secretary), cost-sharing limits, and AV requirements. The law directs that EHB be equal in scope to the benefits provided under a typical employer plan, and that they cover at least the following 10 general categories: ambulatory patient services; emergency services; hospitalization; maternity and newborn care; mental health and substance use disorder services, including behavioral health treatment; prescription drugs; rehabilitative and habilitative services and devices; laboratory services; preventive and wellness services and chronic disease management; and pediatric services, including oral and vision care.
Section 1302(b)(4)(A) through (D) of the Affordable Care Act establish that the Secretary must define EHB in a manner that: (1) reflects appropriate balance among the 10 categories; (2) is not designed in such a way as to discriminate based on age, disability, or expected length of life; (3) takes into account the health care needs of diverse segments of the population; and (4) does not allow denials of EHB based on age, life expectancy, disability, degree of medical dependency, or quality of life.
Section 1302(e) of the Affordable Care Act establishes standards for catastrophic plans to be offered in the individual market and states that the only individuals who are eligible to enroll in catastrophic coverage are individuals who: (1) are under the age of 30 before the beginning of the plan year; (2) have been certified as exempt from the individual responsibility requirement because coverage is unaffordable; or (3) have been certified as experiencing a hardship for obtaining coverage under a qualified health plan (QHP).
Section 1311(c) of the Affordable Care Act provides the Secretary the authority to issue regulations to establish criteria for the certification of QHPs. Among the criteria for certification that the Secretary must establish by regulation is that QHPs ensure a sufficient choice of providers (section 1311(c)(1)(B) of the Affordable Care Act) and include essential community providers that serve predominately low-income, medically underserved individuals (section 1311(c)(1)(C) of the Affordable Care Act). Section 1311(d)(4)(A) of the Affordable Care Act requires the Exchange to implement procedures for the certification, recertification, and decertification of health plans as QHPs, consistent with guidelines developed by the Secretary under section 1311(c) of the Affordable Care Act. Section 1311(e)(1) of the Affordable Care Act grants the Exchange the authority to certify a health plan as a QHP if the health plan meets the Secretary's requirements for certification issued under section 1311(c) of the Affordable Care Act, and the Exchange determines that making the plan available through the Exchange is in the interests of qualified individuals and qualified employers in the State. Section 1311(c)(6)(C) of the Affordable Care Act directs the Secretary to require an Exchange to provide for special enrollment periods (SEPs) and section 1311(c)(6)(D) of the Affordable Care Act directs the Secretary to require an Exchange to provide for American Indians and Alaska Natives (AI/AN), as defined by section 4 of the Indian Health Care Improvement Act.
Section 1311(d)(3)(B) of the Affordable Care Act permits a State, at its option, to require QHPs to cover benefits in addition to EHB. This section also requires a State to make payments, either to the individual enrollee or to the issuer on behalf of the enrollee, to defray the cost of these additional State-required benefits.
Section 1312(c) of the Affordable Care Act generally requires a health insurance issuer to consider all enrollees in all health plans (except grandfathered health plans) offered by such issuer to be members of a single risk pool for each of its individual and small group markets. States have the option to merge the individual and small group market risk pools under section 1312(c)(3) of the Affordable Care Act.
Section 1312(e) of the Affordable Care Act provides the Secretary with the authority to establish procedures under which a State may allow agents or brokers to (1) enroll qualified individuals and qualified employers in QHPs offered through Exchanges and (2) assist individuals in applying for advance payments of the premium tax credit (APTC) and cost-sharing reductions (CSRs) for QHPs sold through an Exchange.
Sections 1313 and 1321 of the Affordable Care Act provide the Secretary with the authority to oversee the financial integrity of State Exchanges, their compliance with HHS standards, and the efficient and non-discriminatory administration of State Exchange activities. Section 1313(a)(5)(A) of the Affordable Care Act provides the Secretary with the authority to implement any measure or procedure that the Secretary determines is appropriate to reduce fraud and abuse in the administration of the Exchanges. Section 1321 of the Affordable Care Act provides for State flexibility in the operation and enforcement of Exchanges and related requirements.
Section 1321(a) of the Affordable Care Act provides broad authority for the Secretary to establish standards and regulations to implement the statutory requirements related to Exchanges, QHPs and other components of title I of the Affordable Care Act, including such other requirements as the Secretary determines appropriate. When operating an FFE under section 1321(c)(1) of the Affordable Care Act, HHS has the authority under sections 1321(c)(1) and 1311(d)(5)(A) of the Affordable Care Act to collect and spend user fees. Office of Management and Budget (OMB) Circular No. A-25 Revised establishes Federal policy regarding user fees and specifies that a user charge will be assessed against each identifiable recipient for special benefits derived from Federal activities beyond those received by the public.[4]
Section 1321(d) of the Affordable Care Act provides that nothing in title I of the Affordable Care Act must be construed to preempt any State law that does not prevent the application of title I of the Affordable Care Act. Section 1311(k) of the Affordable Care Act specifies that Exchanges may not establish rules that
( printed page 29528)
conflict with or prevent the application of regulations issued by the Secretary.
Section 1331 of the Affordable Care Act provides States with an option to establish a BHP. In the States that elect to operate a BHP, the BHP makes affordable health benefits coverage available for individuals under age 65 with household incomes between 133 percent and 200 percent of the FPL who are not otherwise eligible for Medicaid, the Children's Health Insurance Program (CHIP), or affordable employer-sponsored coverage, or for noncitizens whose income is equal to or below 200 percent of FPL but are ineligible for Medicaid benefits that at a minimum consist of the EHB described in section 1302(b) of the Affordable Care Act. For those States that have expanded Medicaid coverage under section 1902(a)(10)(A)(i)(VIII) of the Social Security Act (the Act), the lower income threshold for BHP eligibility is effectively 138 percent of the FPL due to the application of a required 5 percent income disregard in determining the upper limits of Medicaid income eligibility (section 1902(e)(14)(I) of the Act).
Section 1343 of the Affordable Care Act establishes a permanent risk adjustment program to provide payments to health insurance issuers that attract higher-than-average risk enrollees, such as those with chronic conditions, funded by charges collected from those issuers that attract lower-than-average risk enrollees, thereby reducing incentives for issuers to avoid higher-risk enrollees. Section 1343(b) of the Affordable Care Act provides that the Secretary, in consultation with States, shall establish criteria and methods to be used in carrying out the risk adjustment activities under this section. Consistent with section 1321(c) of the Affordable Care Act, the Secretary is responsible for operating the HHS risk adjustment program in any State that fails to do so.[5]
Section 1401(a) of the Affordable Care Act added section 36B to the Internal Revenue Code (the Code), which, among other things, requires that a taxpayer reconcile APTC for a year of coverage with the amount of the premium tax credit (PTC) the taxpayer is allowed for the year.
Section 1402 of the Affordable Care Act provides for, among other things, reductions in cost sharing for EHB for qualified low- and moderate-income enrollees in silver-level QHPs offered through the individual market Exchanges. This section also provides for reductions in cost sharing for American Indians and Alaska Natives (AI/AN) enrolled in QHPs at any metal level.
Section 1411(f) of the Affordable Care Act requires the Secretary, in consultation with the Secretary of the Treasury and the Secretary of Homeland Security, and the Commissioner of Social Security, to establish procedures for hearing and making decisions governing appeals of Exchange eligibility determinations. Section 1411(f)(1)(B) of the Affordable Care Act requires the Secretary to establish procedures to redetermine eligibility on a periodic basis, in appropriate circumstances, including eligibility to purchase a QHP through the Exchange and for APTC and CSRs.
Section 1411(g) of the Affordable Care Act allows the use of applicant information only for the limited purpose of, and to the extent necessary for, ensuring the efficient operation of the Exchange, including by verifying eligibility to enroll through the Exchange and for APTC and CSRs, and limits the disclosure of such information.
Section 1413 of the Affordable Care Act directs the Secretary to establish, subject to minimum requirements, a streamlined enrollment process for enrollment in QHPs and all insurance affordability programs.
Section 2718 of the PHS Act, as added by the Affordable Care Act, generally requires health insurance issuers to submit an annual medical loss ratio (MLR) report to HHS and provide rebates to enrollees if the issuers do not achieve specified MLR thresholds.
Section 5000A of the Code, as added by section 1501(b) of the Affordable Care Act, requires individuals to have minimum essential coverage (MEC) for each month, qualify for an exemption, or make an individual shared responsibility payment. Under the Tax Cuts and Jobs Act, which was enacted on December 22, 2017, the individual shared responsibility payment is reduced to $0, effective for months beginning after December 31, 2018. Notwithstanding that reduction, certain exemptions are still relevant to determine whether individuals aged 30 and above qualify to enroll in catastrophic coverage under §§ 155.305(h) and 156.155(a)(5).
Section 5000A(e) of the Code defines exemptions from the individual shared responsibility penalty. Section 5000A(e)(5) of the Code defines a hardship exemption as a situation in which an individual experiences difficulty obtaining QHP coverage and provides the HHS Secretary the authority to determine whether an individual has experienced a hardship.
Section 71301 of the WFTC legislation amends 26 U.S.C. 36B(e), effective for plan years beginning on or after January 1, 2027, to provide that a PTC is allowed for the coverage of a lawfully present non-citizen only if the non-citizen is an “eligible alien.”
Section 71302 of the WFTC legislation removes subparagraph (B) of 26 U.S.C. 36B(c)(1), eliminating PTC eligibility for lawfully present individuals with income below 100 percent of the FPL who are ineligible for Medicaid due to their immigration status. Section 71302 is effective for taxable years beginning after December 31, 2025.
Section 71303 of the WFTC legislation, effective to taxable years beginning after December 31, 2027, amends the definition of coverage month such that it would be imprudent to maintain a 2-year failure to file and reconcile (FTR) policy for 2028 and beyond, but it would not be legally prohibited to do so.
Section 71304 of the WFTC legislation amends section 36B of the Code, effective for plan years beginning after December 31, 2025, such that a plan is not considered a QHP, and therefore no PTC is allowed for coverage under the plan, if the plan is enrolled in through a special enrollment period (SEP) that is based solely on the relationship of an individual's expected income to the FPL and not on a change in circumstance (an “income-based SEP”). This provision is effective January 1, 2026.
Section 71305 of the WFTC legislation eliminates, effective for taxable years beginning after December 31, 2025, APTC repayment limits and requires individuals whose APTC exceeds their PTC to increase their tax liability by the amount of the excess.
Section 71307 of the WFTC legislation amends the definition of “high deductible health plan” in section 223(c)(2) of the Code to include bronze and catastrophic plans available as individual coverage through an Exchange, effective for months beginning after December 31, 2025.
1. Premium Stabilization Programs
The premium stabilization programs refer to the risk adjustment, risk corridors, and reinsurance programs established by the Affordable Care Act.
6
( printed page 29529)
For past rulemaking, we refer readers to the following rules:
In the March 23, 2012Federal Register
(77 FR 17219) (Premium Stabilization Rule), we implemented the premium stabilization programs.
In the March 11, 2013Federal Register
(78 FR 15409) (2014 Payment Notice), we finalized the benefit and payment parameters for the 2014 benefit year to expand the provisions related to the premium stabilization programs and set forth payment parameters in those programs.
In the October 30, 2013Federal Register
(78 FR 65046), we finalized the modification to the HHS risk adjustment methodology related to community rating States.
In the November 6, 2013Federal Register
(78 FR 66653), we issued a correcting amendment to the 2014 Payment Notice to address how an enrollee's age for the risk score calculation would be determined under the HHS risk adjustment methodology.
In the March 11, 2014Federal Register
(79 FR 13743) (2015 Payment Notice), we finalized the benefit and payment parameters for the 2015 benefit year to expand the provisions related to the premium stabilization programs, set forth certain oversight provisions, and establish payment parameters in those programs.
In the May 27, 2014Federal Register
(79 FR 30240), we announced the fiscal year 2015 sequestration rate for the HHS-operated risk adjustment program.
In the February 27, 2015Federal Register
(80 FR 10750) (2016 Payment Notice), we finalized the benefit and payment parameters for the 2016 benefit year to expand the provisions related to the premium stabilization programs, set forth certain oversight provisions, and establish the payment parameters in those programs.
In the March 8, 2016Federal Register
(81 FR 12203) (2017 Payment Notice), we finalized the benefit and payment parameters for the 2017 benefit year to expand the provisions related to the premium stabilization programs, set forth certain oversight provisions, and establish the payment parameters in those programs.
In the December 22, 2016Federal Register
(81 FR 94058) (2018 Payment Notice), we finalized the benefit and payment parameters for the 2018 benefit year, added the high-cost risk pool parameters to the HHS risk adjustment methodology, incorporated prescription drug factors in the adult models, established enrollment duration factors for the adult models, and finalized policies related to the collection and use of enrollee-level External Data Gathering Environment (EDGE) data.
In the April 17, 2018Federal Register
(83 FR 16930) (2019 Payment Notice), we finalized the benefit and payment parameters for the 2019 benefit year, created the State flexibility framework permitting States to request a reduction in risk adjustment State transfers calculated by HHS, and adopted a new error rate methodology for HHS-RADV adjustments to transfers.
In the May 11, 2018Federal Register
(83 FR 21925), we issued a correction to the 2019 HHS risk adjustment coefficients in the 2019 Payment Notice.
On July 27, 2018, consistent with45 CFR 153.320(b)(1)(i), we updated the 2019 benefit year final HHS risk adjustment model coefficients to reflect an additional recalibration related to an update to the 2016 enrollee-level EDGE data set.[7]
In the July 30, 2018Federal Register
(83 FR 36456), we adopted the 2017 benefit year HHS risk adjustment methodology as established in the final rules issued in the March 23, 2012 (77 FR 17220 through 17252) and March 8, 2016 (81 FR 12204 through 12352) editions of the
Federal Register
. The final rule set forth an additional explanation of the rationale supporting the use of Statewide average premium in the State payment transfer formula for the 2017 benefit year, including the reasons why the program is operated by HHS in a budget-neutral manner. The final rule also permitted HHS to resume 2017 benefit year HHS risk adjustment payments and charges. HHS also provided guidance as to the operation of the HHS-operated risk adjustment program for the 2017 benefit year in light of the publication of the final rule.
In the December 10, 2018Federal Register
(83 FR 63419), we adopted the 2018 benefit year HHS risk adjustment methodology as established in the final rules issued in the March 23, 2012 (77 FR 17219) and the December 22, 2016 (81 FR 94058) editions of the
Federal Register
. In the rule, we set forth an additional explanation of the rationale supporting the use of Statewide average premium in the State payment transfer formula for the 2018 benefit year, including the reasons why the program is operated by HHS in a budget-neutral manner.
In the April 25, 2019Federal Register
(84 FR 17454) (2020 Payment Notice), we finalized the benefit and payment parameters for the 2020 benefit year, as well as the policies related to making the enrollee-level EDGE data available as a limited data set for research purposes and expanding the HHS uses of the enrollee-level EDGE data, approval of the request from Alabama to reduce HHS risk adjustment transfers by 50 percent in the small group market for the 2020 benefit year, and updates to HHS-RADV program requirements.
On May 12, 2020, consistent with § 153.320(b)(1)(i), we issued the 2021 Benefit Year Final HHS Risk Adjustment Model Coefficients on the CCIIO website.[8]
In the May 14, 2020Federal Register
(85 FR 29164) (2021 Payment Notice), we finalized the benefit and payment parameters for the 2021 benefit year, as well as adopted updates to the HHS risk adjustment models' hierarchical condition categories (HCCs) to transition to the 10th revision of the International Classification of Diseases (ICD-10) codes, approved the request from Alabama to reduce HHS risk adjustment transfers by 50 percent in the small group market for the 2021 benefit year, and modified the outlier identification process under the HHS-RADV program.
In the December 1, 2020Federal Register
(85 FR 76979) (Amendments to the HHS-Operated Risk Adjustment Data Validation Under the Patient Protection and Affordable Care Act's HHS-Operated Risk Adjustment Program (2020 HHS-RADV Amendments Rule)), we adopted the creation and application of Super HCCs in the sorting step that assigns HCCs to failure rate groups, finalized a sliding scale adjustment in HHS-RADV error rate calculation, and added a constraint for negative error rate outliers with a negative error rate. We also established a transition from the prospective application of HHS-RADV adjustments to apply HHS-RADV results to risk scores from the same benefit year as that being audited.
In the May 5, 2021Federal Register
(86 FR 24140) (part 2 of the 2022 Payment Notice), we finalized a subset of proposals from the December 4, 2020
Federal Register
(85 FR 78572) (the 2022 Payment Notice proposed rule), including policy and regulatory revisions related to the HHS-operated risk adjustment program, finalization of the benefit and payment parameters for the 2022 benefit year, and approval of
( printed page 29530)
the request from Alabama to reduce HHS risk adjustment transfers by 50 percent in the individual and small group markets for the 2022 benefit year. In addition, this final rule established a revised schedule of collections for HHS-RADV and updated the provisions regulating second validation audit (SVA) and initial validation audit (IVA) entities.
On July 19, 2021, consistent with § 153.320(b)(1)(i), we released Updated 2022 Benefit Year Final HHS Risk Adjustment Model Coefficients on the CCIIO website, announcing some minor revisions to the 2022 benefit year final HHS risk adjustment adult model coefficients.[9]
In the May 6, 2022Federal Register
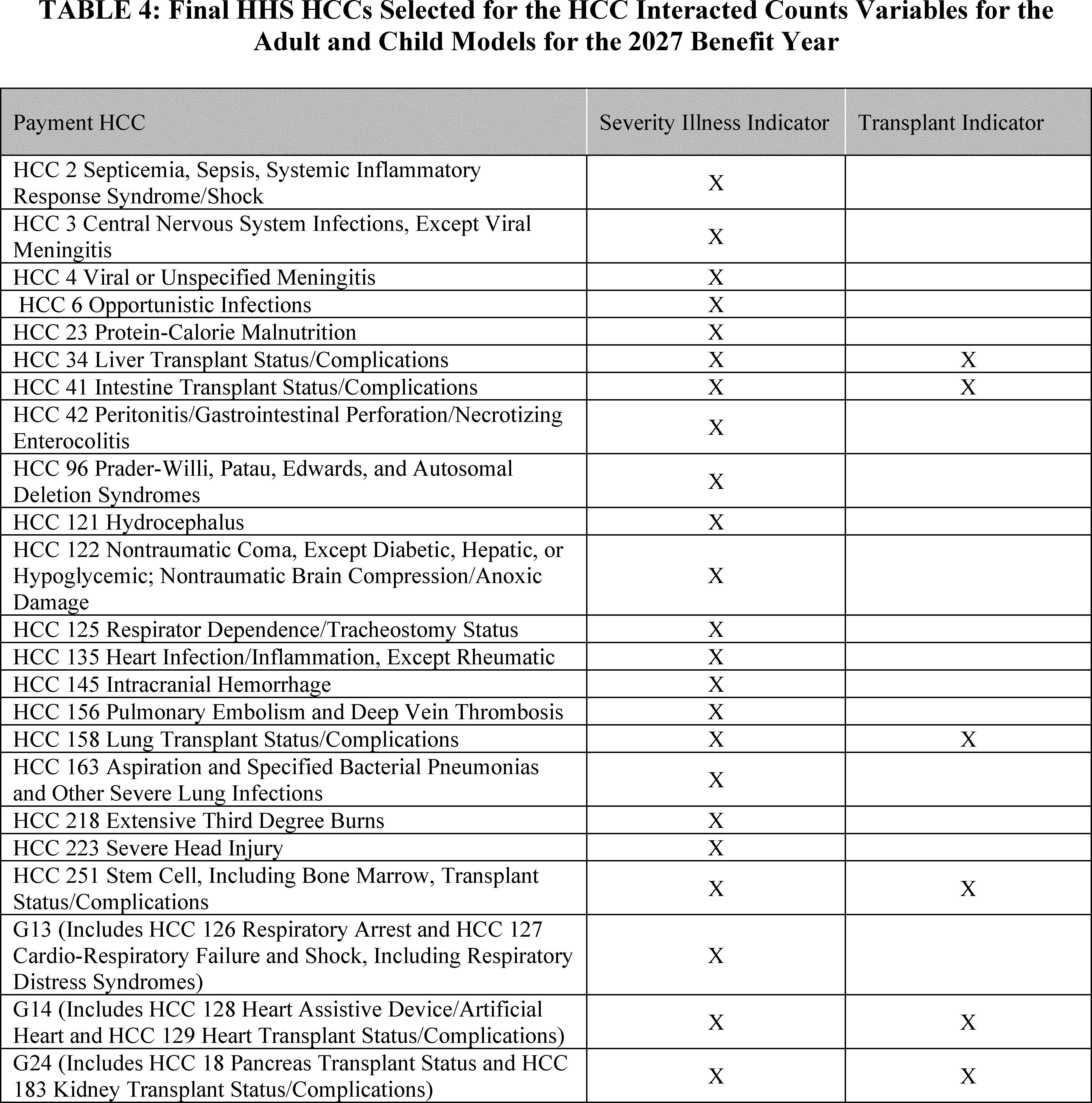
(87 FR 27208) (2023 Payment Notice), we finalized revisions related to the HHS-operated risk adjustment program, including the benefit and payment parameters for the 2023 benefit year, HHS risk adjustment model recalibration, and policies related to the collection and extraction of enrollee-level EDGE data. We also finalized the adoption of the interacted HCC count specification for the adult and child models, along with modified enrollment duration factors for the adult models, beginning with the 2023 benefit year.[10]
We also repealed the ability for States, other than prior participants, to request a reduction in HHS risk adjustment State transfers starting with the 2024 benefit year. We approved a 25 percent reduction to 2023 benefit year HHS risk adjustment transfers in Alabama's individual market and a 10 percent reduction to 2023 benefit year HHS risk adjustment transfers in Alabama's small group market. We finalized further refinements to the HHS-RADV error rate calculation methodology beginning with the 2021 benefit year.
In the April 27, 2023Federal Register
(88 FR 25740) (2024 Payment Notice), we finalized the benefit and payment parameters for the 2024 benefit year, amended the EDGE discrepancy materiality threshold and data collection requirements, and reduced the risk adjustment user fee. For the 2024 benefit year, we approved 50 percent reductions to HHS risk adjustment transfers for Alabama's individual and small group markets and repealed prior participant States' ability to request reductions of their risk adjustment transfers for the 2025 benefit year and beyond. We finalized refinements to HHS-RADV program requirements, such as shortening the window to confirm SVA findings or file a discrepancy report, changing the HHS-RADV materiality threshold for random and targeted sampling, and no longer exempting exiting issuers from adjustments to risk scores and HHS risk adjustment transfers when they are negative error rate outliers. We announced the discontinuance of the Lifelong Permanent Condition List and Non-EDGE Claims in HHS-RADV beginning with the 2022 benefit year.
In the April 15, 2024Federal Register
(89 FR 26218) (2025 Payment Notice), we finalized the benefit and payment parameters for the 2025 benefit year, including the 2025 risk adjustment models and updated the adjustment factors for the receipt of CSRs for the AI/AN subpopulation who are enrolled in zero and limited cost-sharing plans to improve prediction in the HHS risk adjustment models. In addition, we finalized that in certain cases, we may require a corrective action plan (CAP) to address an observation identified in an HHS risk adjustment program audit.
In the January 15, 2025Federal Register
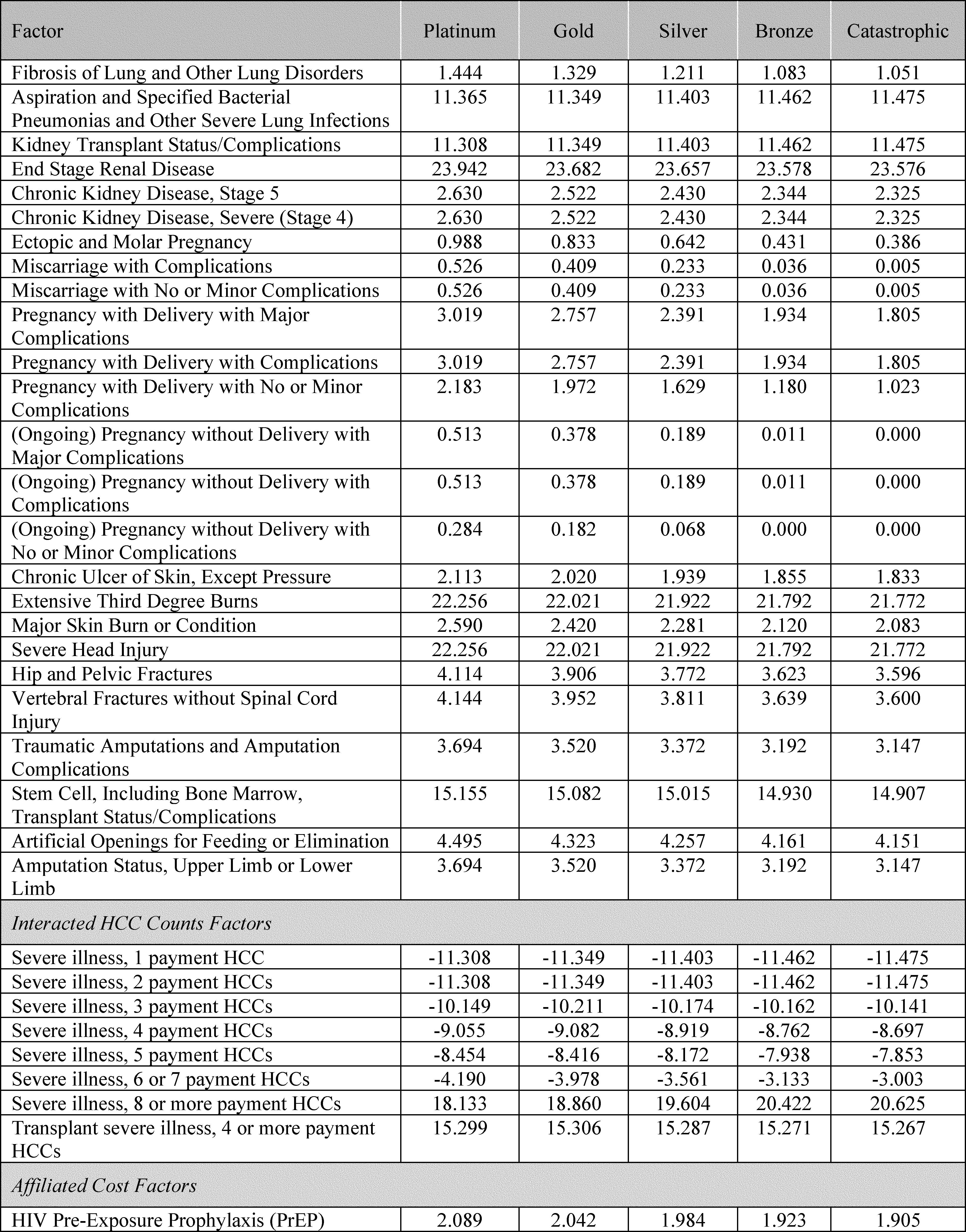
(90 FR 4424) (2026 Payment Notice), we finalized the benefit and payment parameters for the 2026 benefit year, including the 2026 risk adjustment models and updated the adjustment factors, phased out the market pricing adjustment to the plan liability associated with Hepatitis C drugs, and incorporated of pre-exposure prophylaxis (PrEP) as an Affiliated Cost Factor (ACF) starting with the 2026 benefit year. Beginning with the 2025 benefit year, we excluded enrollees without HCCs from the IVA sample, removed the Finite Population Correction (FPC) from the IVA sampling methodology, and replaced the source of the Neyman allocation data used for HHS-RADV sampling with the most recent 3 consecutive years of HHS-RADV data. Beginning with the 2024 benefit year, we modified the SVA pairwise means test and increased the initial SVA subsample size. At § 156.1220(a), we established a new materiality threshold for HHS-RADV appeals.
2. Program Integrity
We have finalized program integrity standards related to the Exchanges and premium stabilization programs in two rules: the “first Program Integrity Rule” issued in the August 30, 2013
Federal Register
(78 FR 54069), and the “second Program Integrity Rule” issued in the October 30, 2013
Federal Register
(78 FR 65045). We also refer readers to the 2019 Patient Protection and Affordable Care Act; Exchange Program Integrity final rule (2019 Program Integrity Rule) issued in the December 27, 2019
Federal Register
(84 FR 71674), as well as the Patient Protection and Affordable Care Act; Marketplace Integrity and Affordability final rule (2025 Marketplace Integrity and Affordability final rule) issued in the June 25, 2025
Federal Register
(90 FR 27074).
In the May 6, 2022
Federal Register
(87 FR 27208) (2023 Payment Notice), we finalized policies to address certain agent, broker, and web-broker practices and conduct. In the April 27, 2023
Federal Register
(88 FR 25740) (2024 Payment Notice), we implemented the improper payment pre-testing and assessment (IPPTA) requirements for State Exchanges to ensure adherence to the Payment Integrity Information Act of 2019. In addition, we finalized allowing additional time for HHS to review evidence submitted by agents and brokers to rebut allegations pertaining to Exchange Agreement suspensions or terminations. We also introduced consent and eligibility application documentation requirements for agents, brokers, and web-brokers that assist Exchange consumers in FFE and SBE-FP States.
In the 2025 Payment Notice, issued in the April 15, 2024
Federal Register
(89 FR 26218), we finalized that the CMS Administrator is the entity responsible for handling requests by agents, brokers, and web-brokers for reconsideration of HHS' decision to terminate their Exchange agreement(s) for cause. We also finalized changes to §§ 155.220 and 155.221 to apply certain standards to web-brokers and Direct Enrollment (DE) entities assisting consumers and applicants across all Exchanges. In the January 15, 2025
Federal Register
(90 FR 4424) (2026 Payment Notice), we addressed our authority to investigate and undertake compliance reviews and enforcement actions occurring at the insurance agency level to hold lead agents of insurance agencies accountable. We also finalized changes to § 155.220(k)(3) to reflect our authority to suspend an agent's or broker's ability to transact information with the Exchange in certain circumstances until the incident, breach, or noncompliance are remedied or sufficiently mitigated to HHS' satisfaction.
( printed page 29531)
3. Market Rules
In the February 27, 2013
Federal Register
(78 FR 13406), we issued the health insurance market rules, including provisions related to the single risk pool. We codified that, for catastrophic plans, issuers may make a plan-specific adjustment to the market-wide index rate based on the expected impact of the specific eligibility categories for those plans. This plan-specific adjustment would be uniform across all of an issuer's catastrophic plans (that is, risk across all catastrophic plans must be pooled).
In that rule, we also codified that a health plan is a catastrophic plan if it: (1) meets all applicable requirements for health insurance coverage in the individual market; (2) does not offer coverage at the bronze, silver, gold, or platinum levels of coverage (3) does not provide coverage of essential health benefits until the enrolled individual reaches the annual limitation in cost sharing; and (4) covers at least three primary care visits per year before reaching the deductible. A catastrophic plan may not impose any cost-sharing requirements for preventive services identified in section 2713 of the PHS Act. We also codified the statutory eligibility criteria identified in section 1302(e)(2) of the Affordable Care Act.
We amended requirements related to index rates under the single risk pool provision in a final rule issued in the July 2, 2013
Federal Register
(78 FR 39870). In the October 30, 2013
Federal Register
(78 FR 65046), we clarified when issuers may establish and update premium rates. In the March 8, 2016
Federal Register
(81 FR 12203), we clarified single risk pool provisions related to student health insurance coverage. We finalized minor adjustments to the single risk pool regulations in the 2018 Payment Notice, issued in the December 22, 2016
Federal Register
(81 FR 94058).
4. Rate Review
In the May 23, 2011
Federal Register
(76 FR 29963) (Rate Review Rule), we implemented a rate review program. We amended the provisions of the Rate Review Rule in final rules published in the September 6, 2011
Federal Register
(76 FR 54969), the February 27, 2013
Federal Register
(78 FR 13405), the May 27, 2014
Federal Register
(79 FR 30239), the February 27, 2015
Federal Register
(80 FR 10749), the March 8, 2016
Federal Register
(81 FR 12203) and the December 22, 2016
Federal Register
(81 FR 94058).
5. Exchanges
We requested comment relating to Exchanges in the August 3, 2010
Federal Register
(75 FR 45584). We issued initial guidance to States on Exchanges on November 18, 2010. In the March 27, 2012
Federal Register
(77 FR 18310) (Exchange Establishment Rule), we implemented the Affordable Insurance Exchanges (Exchanges), consistent with title I of the Affordable Care Act, to provide competitive marketplaces for individuals and small employers to directly compare available private health insurance coverage options based on price, quality, and other factors. This included implementation of components of the Exchanges and standards for eligibility for Exchanges, as well as network adequacy and essential community provider (ECP) certification standards.
In the 2014 Payment Notice and the Amendments to the HHS Notice of Benefit and Payment Parameters for 2014 interim final rule, issued in the March 11, 2013
Federal Register
(78 FR 15541), we set forth standards related to Exchange user fees. We established an adjustment to the FFE user fee in the Coverage of Certain Preventive Services under the Affordable Care Act final rule, issued in the July 2, 2013
Federal Register
(78 FR 39869) (Preventive Services Rule).
In the 2016 Payment Notice, we also set forth the ECP certification standard at § 156.235, with revisions in the 2017 Payment Notice in the March 8, 2016
Federal Register
(81 FR 12203) and the 2018 Payment Notice in the December 22, 2016
Federal Register
(81 FR 94058).
In the 2018 Payment Notice, issued in the December 22, 2016
Federal Register
(81 FR 94058), we set forth the standards for the request for reconsideration of denial of QHP certification specific to the FFEs at § 155.1090.
In an interim final rule, issued in the May 11, 2016
Federal Register
(81 FR 29146), we made amendments to the parameters of certain SEPs (2016 Interim Final Rule).
We finalized these in the 2018 Payment Notice, issued in the December 22, 2016
Federal Register
(81 FR 94058).
In the Market Stabilization final rule, issued in the April 18, 2017
Federal Register
(82 FR 18346), we amended standards relating to SEPs and QHP certification. In the 2019 Payment Notice, issued in the April 17, 2018
Federal Register
(83 FR 16930), we modified parameters around certain SEPs. In the April 25, 2019
Federal Register
(84 FR 17454), the 2020 Payment Notice established a new SEP for certain individuals who become newly eligible for APTC.
In the May 14, 2020
Federal Register
(85 FR 29164) (2021 Payment Notice), we finalized revisions to the parameters of SEPs and the quality rating information display standards for State Exchanges and amended the periodic data matching requirements.
In the January 19, 2021
Federal Register
(86 FR 6138) (part 1 of the 2022 Payment Notice), we finalized only a subset of the proposals in the 2022 Payment Notice proposed rule. In the May 5, 2021
Federal Register
(86 FR 24140), we issued part 2 of the 2022 Payment Notice. In the September 27, 2021
Federal Register
(86 FR 53412) (part 3 of the 2022 Payment Notice), in conjunction with the Department of the Treasury, we finalized amendments to certain policies in part 1 of the 2022 Payment Notice.
In the May 6, 2022
Federal Register
(87 FR 27208), we finalized changes to maintain the user fee rate for issuers offering plans through the FFEs and maintain the user fee rate for issuers offering plans through the SBE-FPs for the 2023 benefit year. We also finalized various policies to address certain agent, broker, and web-broker practices and conduct. We also finalized updates to the requirement that all Exchanges conduct SEP verifications.
In the 2024 Payment Notice, issued in the April 27, 2023
Federal Register
(88 FR 25740), we revised Exchange Blueprint approval timelines, lowered the user fee rate for QHPs in the FFEs and SBE-FPs, and amended re-enrollment hierarchies for enrollees. We finalized a requirement that all plans seeking certification on the Exchanges utilize a provider network. We also finalized policies to update FFE and SBE-FP standardized plan options; reduce the risk of plan choice overload on the FFEs and SBE-FPs by limiting the number of non-standardized plan options that issuers may offer through Exchanges on the Federal platform; and ensure correct QHP information. In addition, we amended coverage effective date rules, lengthened the SEP from 60 to 90 days for those who lose Medicaid coverage, and prohibited QHPs on FFEs and SBE-FPs from terminating coverage mid-year for dependent children who reach the applicable maximum age. We also finalized policies on verifying consumer income and permitting door-to-door assisters to solicit consumers. We finalized provider network and ECP policies for QHPs.
( printed page 29532)
In the 2025 Payment Notice, issued in the April 15, 2024
Federal Register
(89 FR 26218), we required a State seeking to operate a State Exchange to first operate an SBE-FP for at least one plan year, revised Exchange Blueprint requirements for States transitioning to a State Exchange, established additional minimum standards for Exchange call center operations, and required an Exchange to operate a centralized eligibility and enrollment platform on its website. We required State Exchanges and State Medicaid agencies to remit payment to HHS for their use of certain income data, amended re-enrollment hierarchies for enrollees enrolled in catastrophic coverage, revised the parameters around a State Exchange adopting an alternative open enrollment period, and extended the availability of an SEP for APTC-eligible qualified individuals with a projected annual household income no greater than 150 percent of the FPL. We finalized provider network adequacy policies applicable to such Exchanges for Plan Year (PY) 2026 and subsequent plan years. We finalized the policy to maintain FFE and SBE-FP standardized plan option metal levels from the 2024 Payment Notice and finalized an exceptions process to the limitation on non-standardized plan options in FFEs and SBE-FPs. We also finalized the requirement for Exchanges to provide notification to enrollees or their tax filers who have failed to file their Federal income taxes and reconcile APTC for 1 tax year.
In the 2026 Payment Notice, published in the January 15, 2025
Federal Register
(90 FR 4424), we codified a timeliness standard for State Exchanges to review and resolve enrollment data inaccuracies at § 155.400(d)(1), finalized at § 155.1000 that an Exchange may deny certification to any plan that does not meet the criteria at § 155.1000(c), and revised the standards at § 155.1090 for an issuer to request a reconsideration of a denial of certification specific to the FFEs. We also finalized publicly releasing certain data and information that State Exchanges submit to HHS, affirmed that CSR loading practices permitted by State regulators are permissible under Federal law to the extent that they are actuarially justified and the issuer does not receive reimbursement for such CSR, and finalized that we will only release a single, final version of the AV Calculator. We also updated the standardized plan option designs for PY 2026 to ensure these plans continue to have AVs within the permissible
de minimis range
for each metal level, amended § 156.201 to require issuers to meaningfully differentiate standardized plan options from one another, and finalized that HHS would conduct ECP certification reviews in States performing plan management functions beginning PY 2026. We also finalized updates affecting the exchanges in the 2025 Marketplace Integrity and Affordability final rule issued in the June 25, 2025
Federal Register
(90 FR 27074).
6. Essential Health Benefits
We established requirements relating to EHB in the Standards Related to Essential Health Benefits, Actuarial Value, and Accreditation Final Rule, which was issued in the February 25, 2013
Federal Register
(78 FR 12834) (EHB Rule). We established at § 156.135(a) that AV is generally to be calculated using the AV Calculator developed and made available by HHS for a given benefit year. In the 2015 Payment Notice (79 FR 13743), we established at § 156.135(g) provisions for updating the AV Calculator in future plan years. In the 2017 Payment Notice (81 FR 12349), we amended the provisions at § 156.135(g) to allow for additional flexibility in our approach and options for updating of the AV Calculator.
In the 2025 Payment Notice, issued in the April 15, 2024
Federal Register
(89 FR 26218), we revised § 155.170(a) to codify that benefits covered in a State's EHB-benchmark plan are not considered in addition to EHB, even if they had been required by State action taking place after December 31, 2011, other than for purposes of compliance with Federal requirements. We finalized three revisions to the standards for State selection of EHB-benchmark plans for benefit years beginning on or after January 1, 2026: revising the typicality standard at § 156.111 for States to demonstrate that their new EHB-benchmark plan provides a scope of benefits that is equal to that of a typical employer plan in the State; revising requirements such that States do not need to submit a formulary drug list as part of their application unless they are changing their prescription drug EHB; and consolidating options for States to change their EHB-benchmark plans. At § 156.115(d), we removed the prohibition on issuers from including routine non-pediatric dental services as an EHB beginning with PY 2027.
In the 2026 Payment Notice, published in the January 15, 2025
Federal Register
(90 FR 4424), we revised § 156.80(d)(2)(i) to require the actuarially justified plan-specific factors by which an issuer may vary premium rates for a particular plan from its market-wide index rate include the AV and cost-sharing design of the plan.
7. Quality Improvement Strategy
We issued regulations in § 155.200(d) to direct Exchanges to evaluate quality improvement strategies, and § 156.200(b) to direct QHP issuers to implement and report on a quality improvement strategy or strategies consistent with section 1311(g) standards as QHP certification criteria for participation in an Exchange. In the 2016 Payment Notice, issued in the February 27, 2015
Federal Register
(80 FR 10749), we finalized regulations at § 156.1130 to establish standards and the associated timeframe for QHP issuers to submit the necessary information to implement quality improvement strategy standards for QHPs offered through an Exchange. In the 2026 Payment Notice, published in the January 15, 2025
Federal Register
(90 FR 4424), we finalized sharing summary-level QIS information publicly on an annual basis beginning on January 1, 2026, with information QHP issuers submit during the PY 2025 QHP Application Period.
8. Medical Loss Ratio (MLR)
We published a request for comment on section 2718 of the PHS Act in the April 14, 2010
Federal Register
(75 FR 19297) and published an interim final rule with a 60-day comment period relating to the MLR program on December 1, 2010 (75 FR 74863). A final rule with a 30-day comment period was published in the December 7, 2011
Federal Register
(76 FR 76573). An interim final rule with a 60-day comment period was published in the December 7, 2011
Federal Register
(76 FR 76595). A final rule was published in the May 16, 2012
Federal Register
(77 FR 28790). The MLR program requirements were amended in final rules published in the March 11, 2014
Federal Register
(79 FR 13743), the May 27, 2014
Federal Register
(79 FR 30339), the February 27, 2015
Federal Register
(80 FR 10749), the March 8, 2016
Federal Register
(81 FR 12203), the December 22, 2016
Federal Register
(81 FR 94183), the April 17, 2018
Federal Register
(83 FR 16930), the May 14, 2020
Federal Register
(85 FR 29164), the May 5, 2021
Federal Register
(86 FR 24140), the May 6, 2022
Federal Register
(87 FR 27208), and the January 15, 2025
Federal Register
(90 FR 4424) and an interim final rule that was published in the September 2, 2020
Federal Register
(85 FR 54820).
( printed page 29533)
We are finalizing updates in 42 CFR 600.5 to align BHP regulations with section 71301 of the WFTC legislation. Section 71301 of the WFTC legislation amended section 36B of the Code to provide that a PTC is allowed for the QHP coverage of a lawfully present noncitizen only if he or she is an “eligible alien,” effective for plan years beginning on or after January 1, 2027. Because Federal BHP payments to States are based in part on the amount of PTC an individual enrolled in the BHP is eligible for and would have qualified for had he or she been enrolled in a QHP through an Exchange, only lawfully present noncitizens who are considered to be “eligible aliens” will generate Federal BHP payments to the State. We are finalizing a new definition of “eligible noncitizen” at 42 CFR 600.5, cross-referencing 45 CFR 155.20.
In accordance with the OMB Report to Congress on the Joint Committee Reductions for Fiscal Year 2026, the HHS-operated risk adjustment program is subject to fiscal year 2026 sequestration.[11]
Therefore, the HHS-operated risk adjustment program will sequester payments made from fiscal year 2026 resources (that is, funds collected during the 2026 fiscal year) at a rate of 5.7 percent.
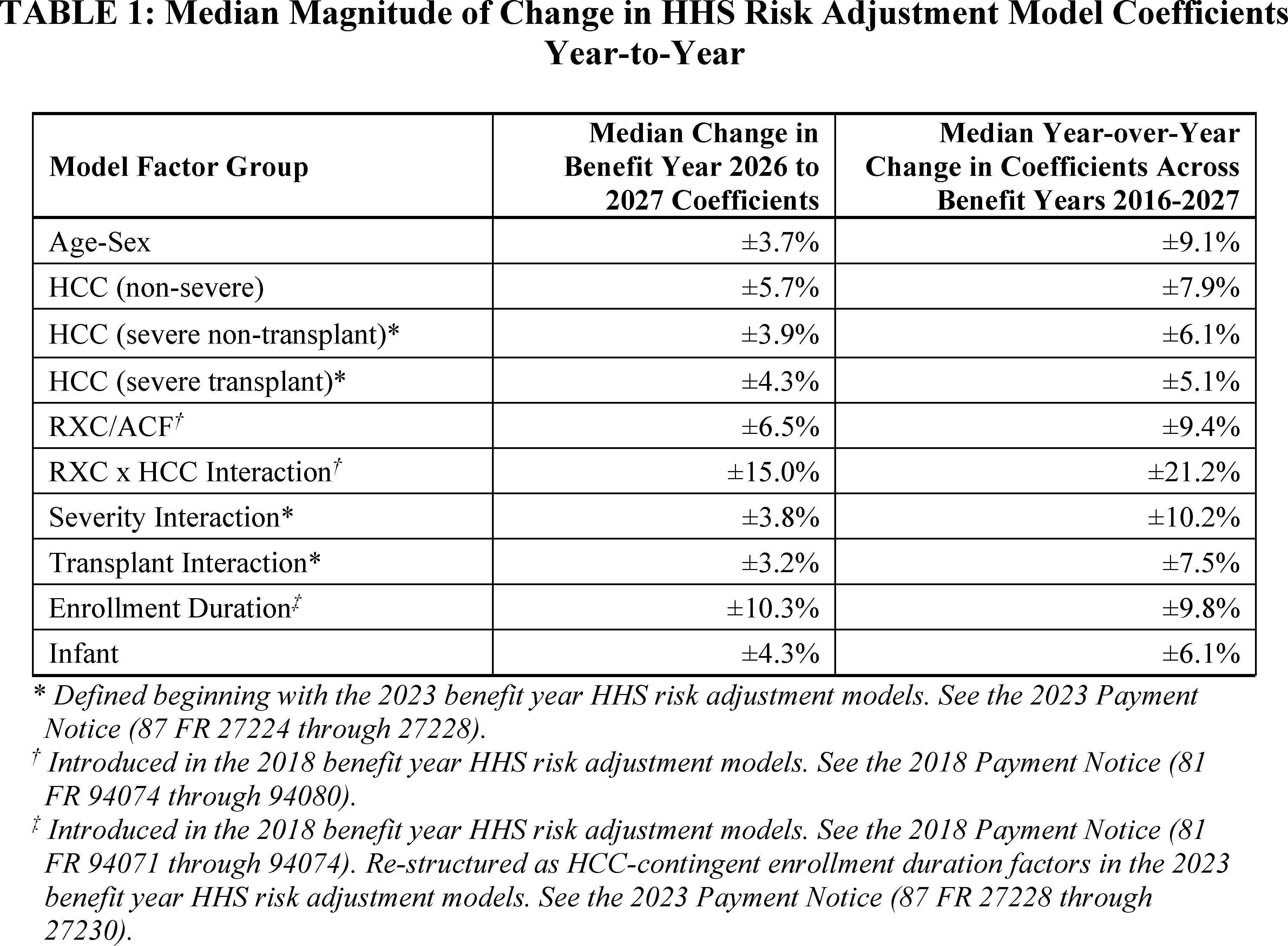
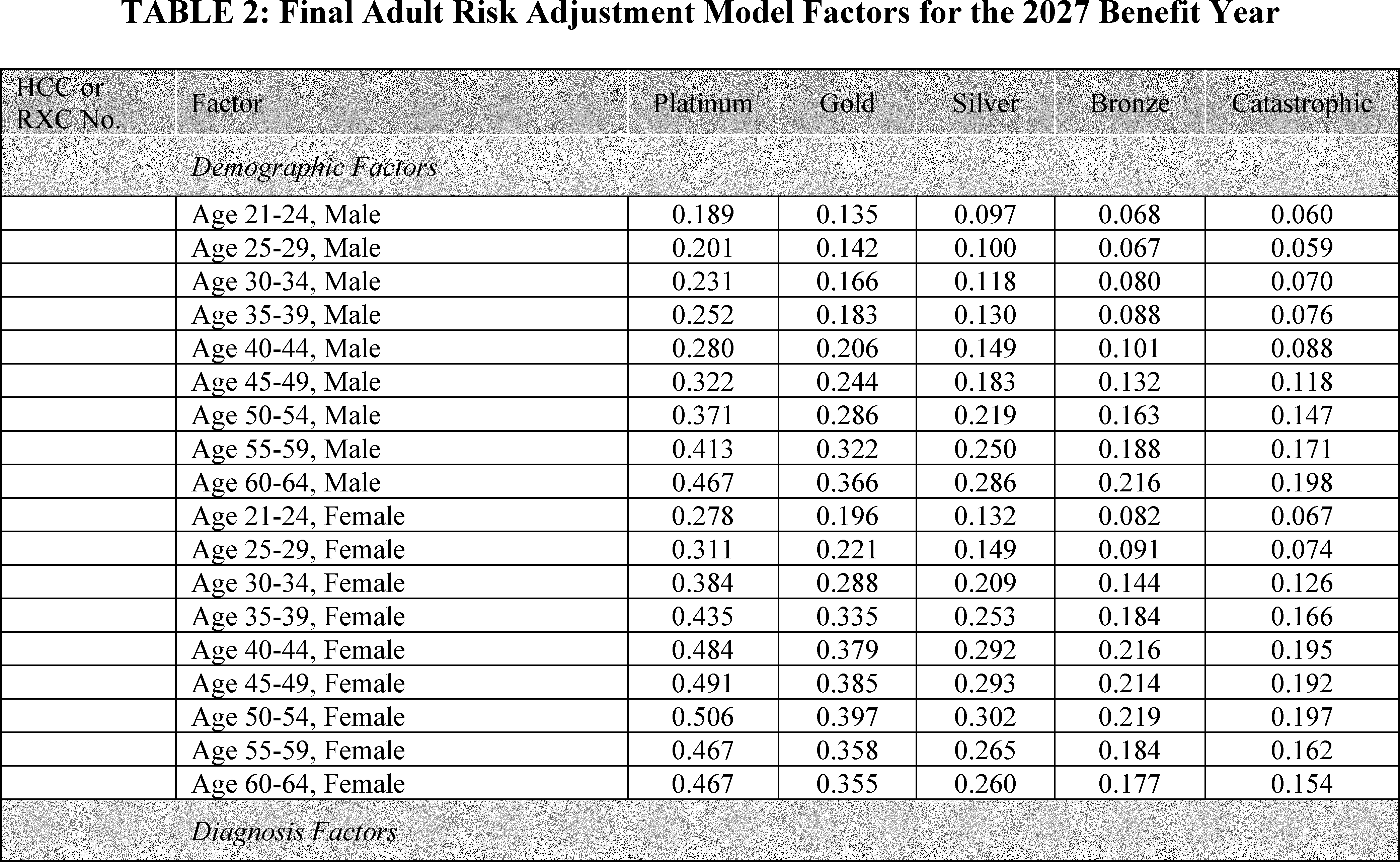
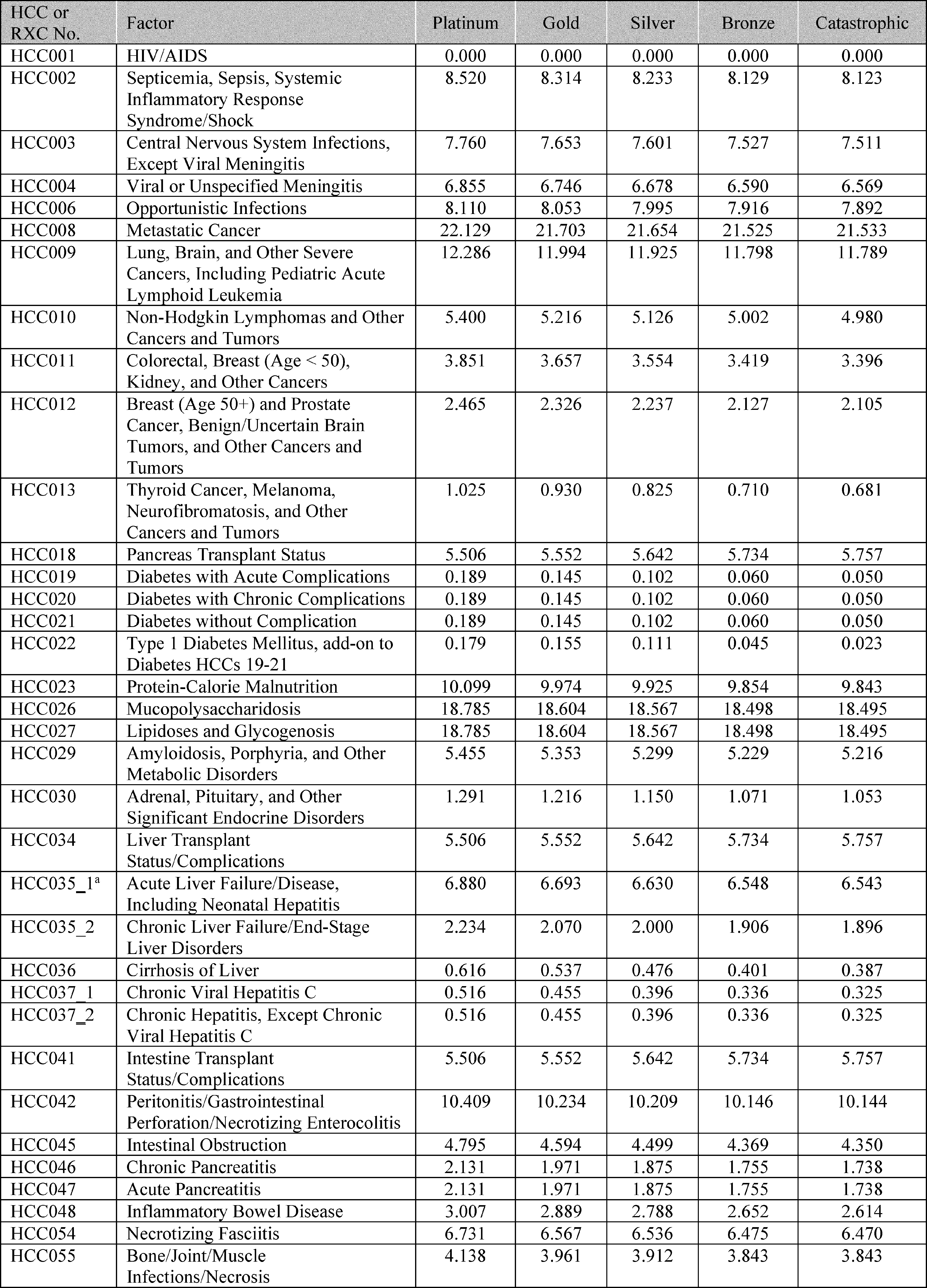
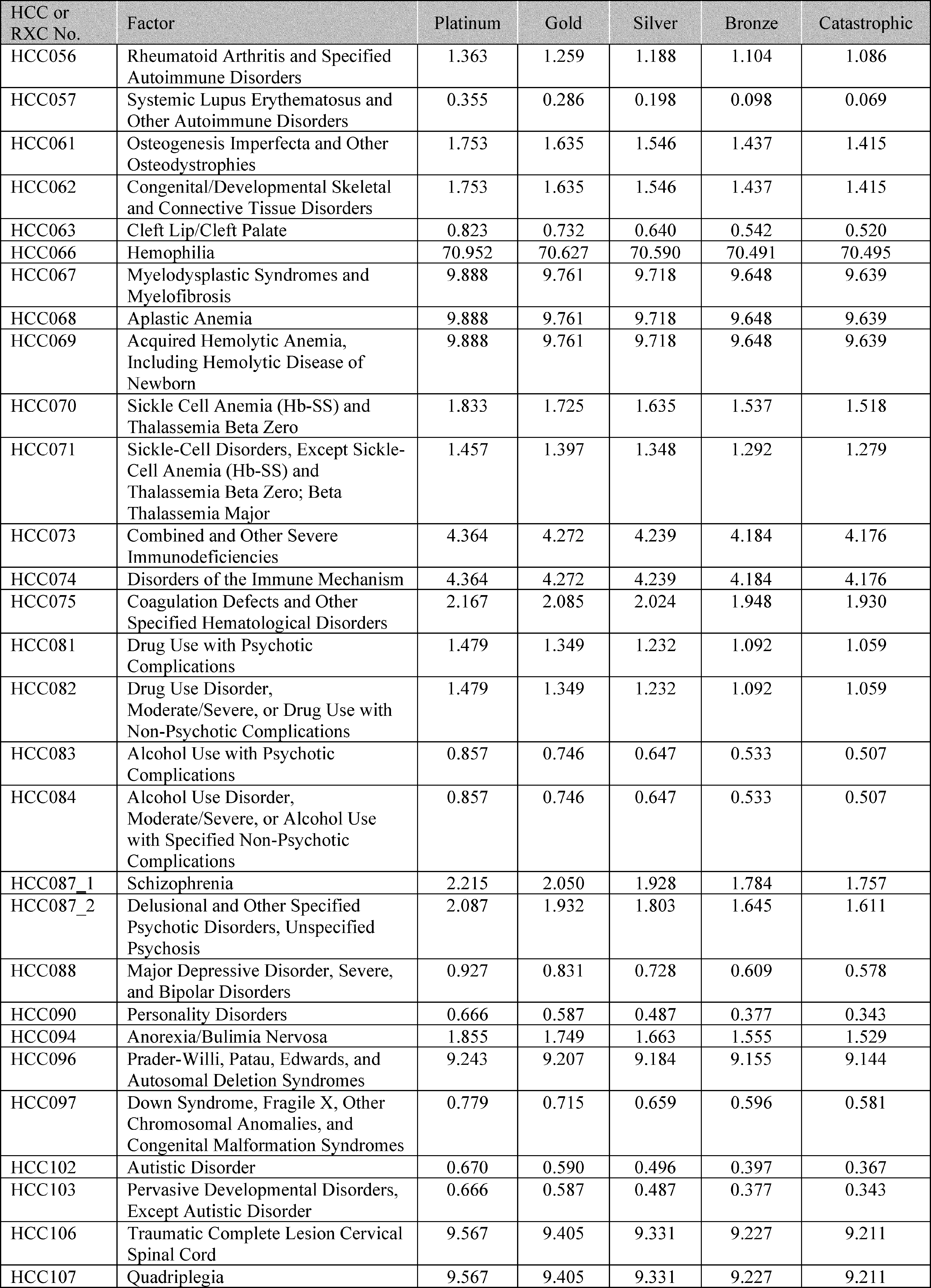
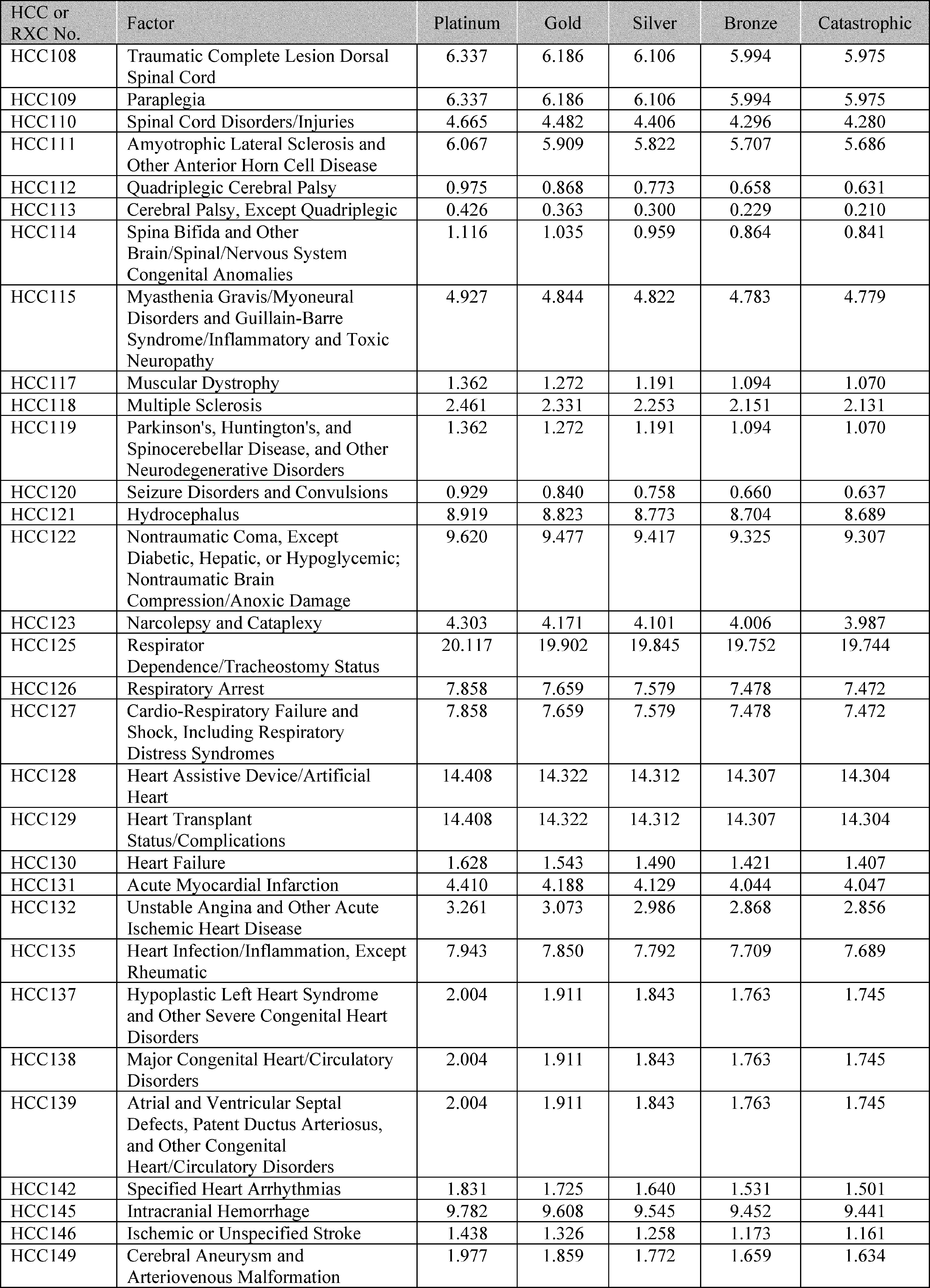
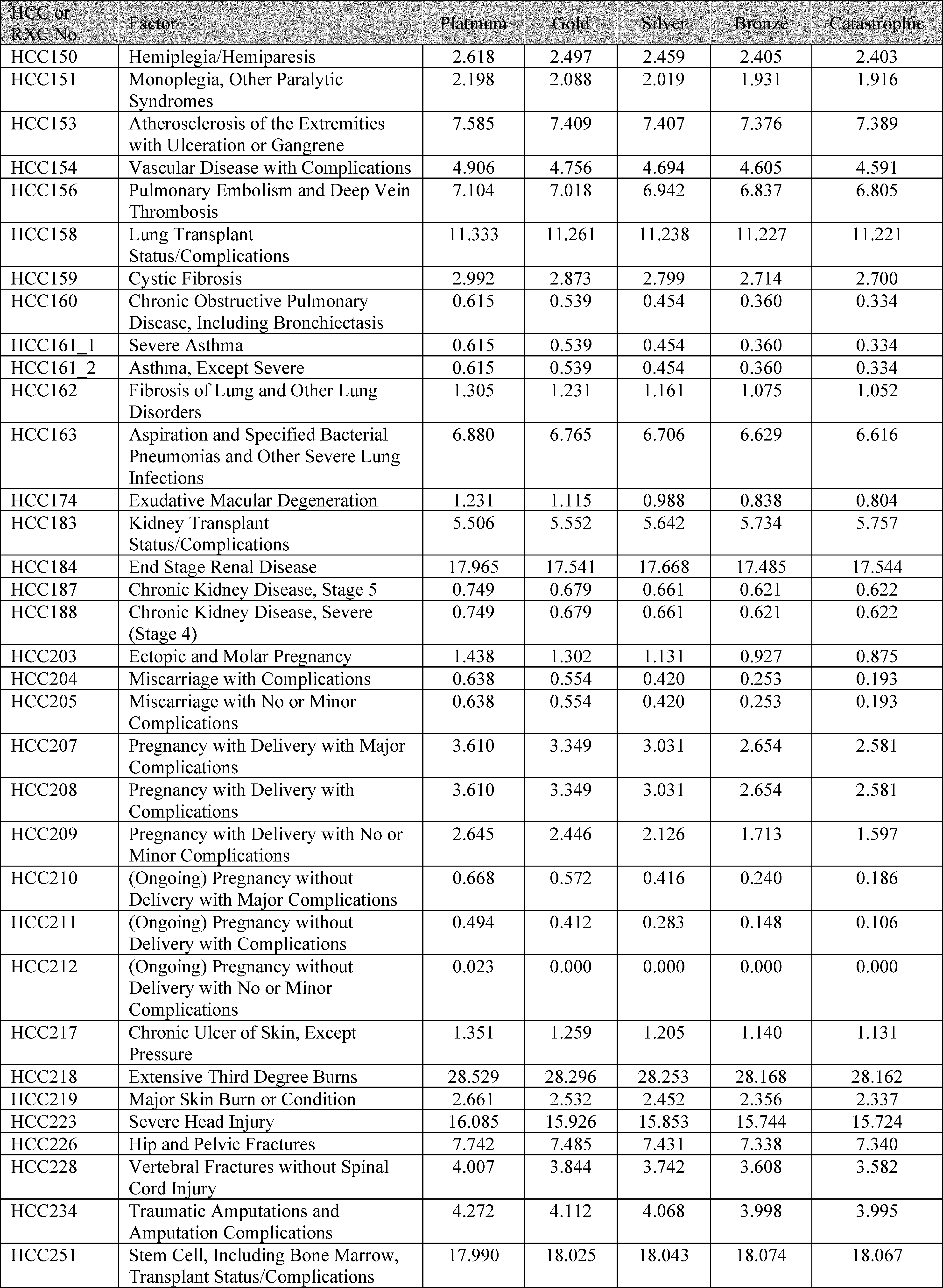
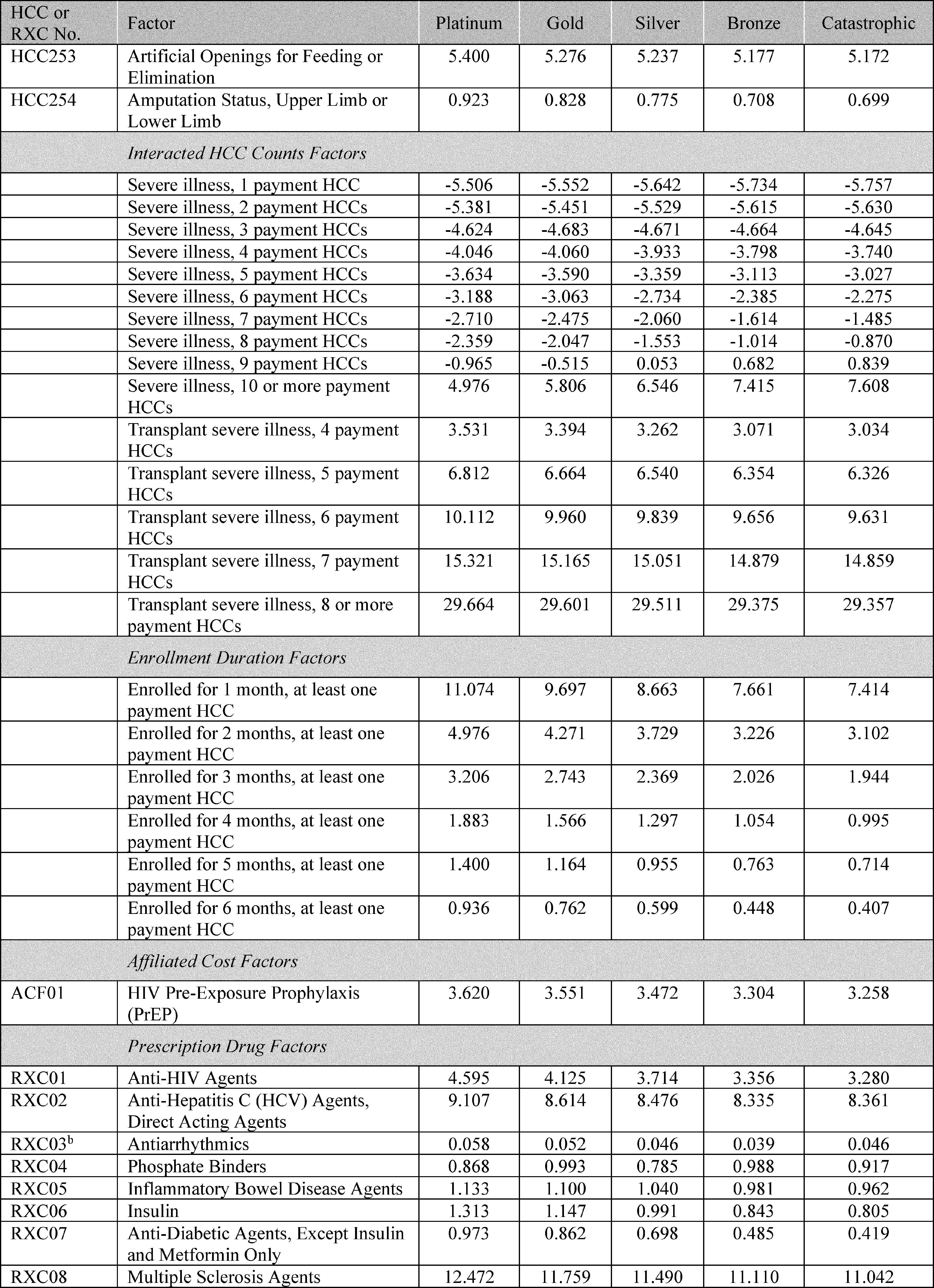
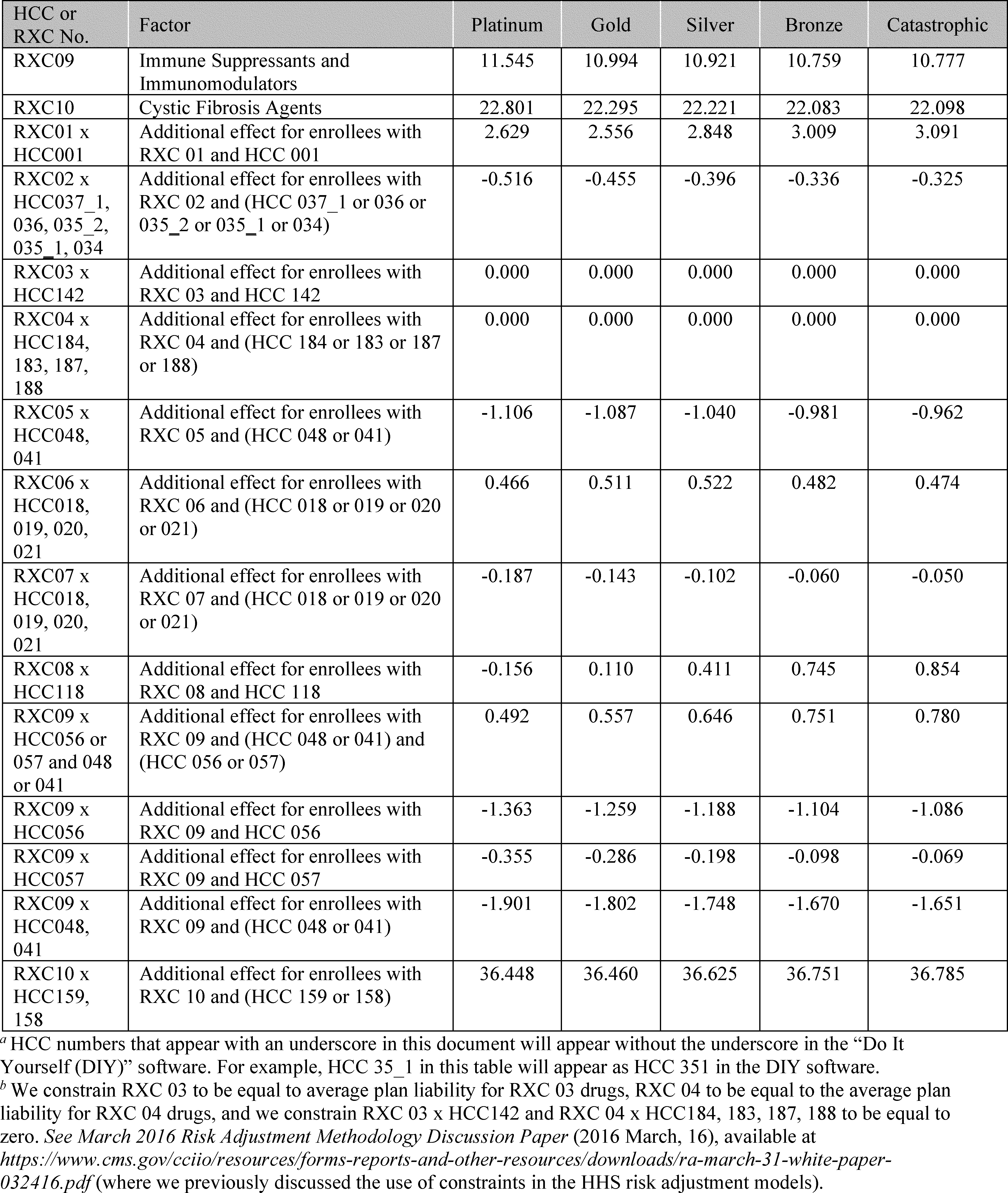
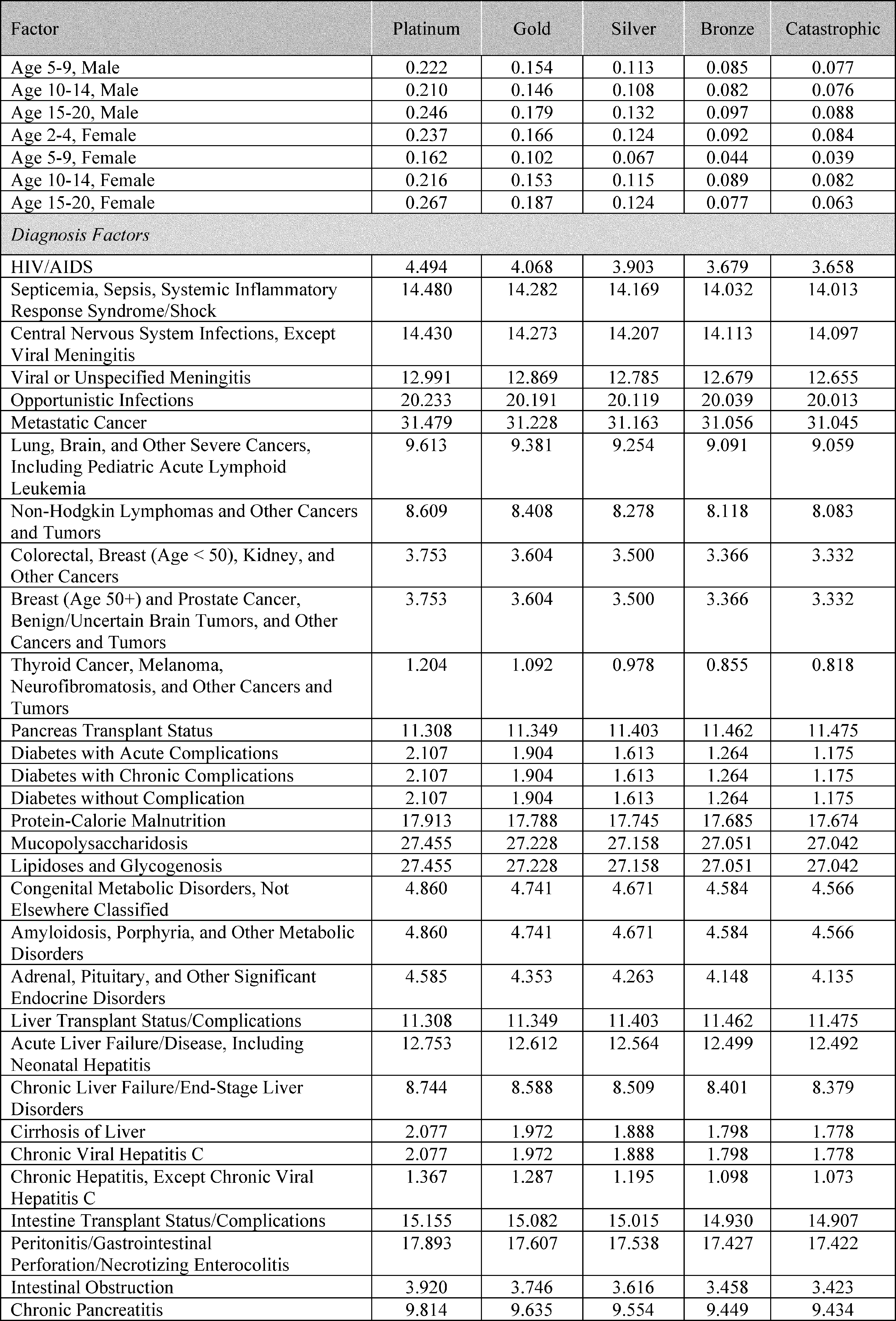
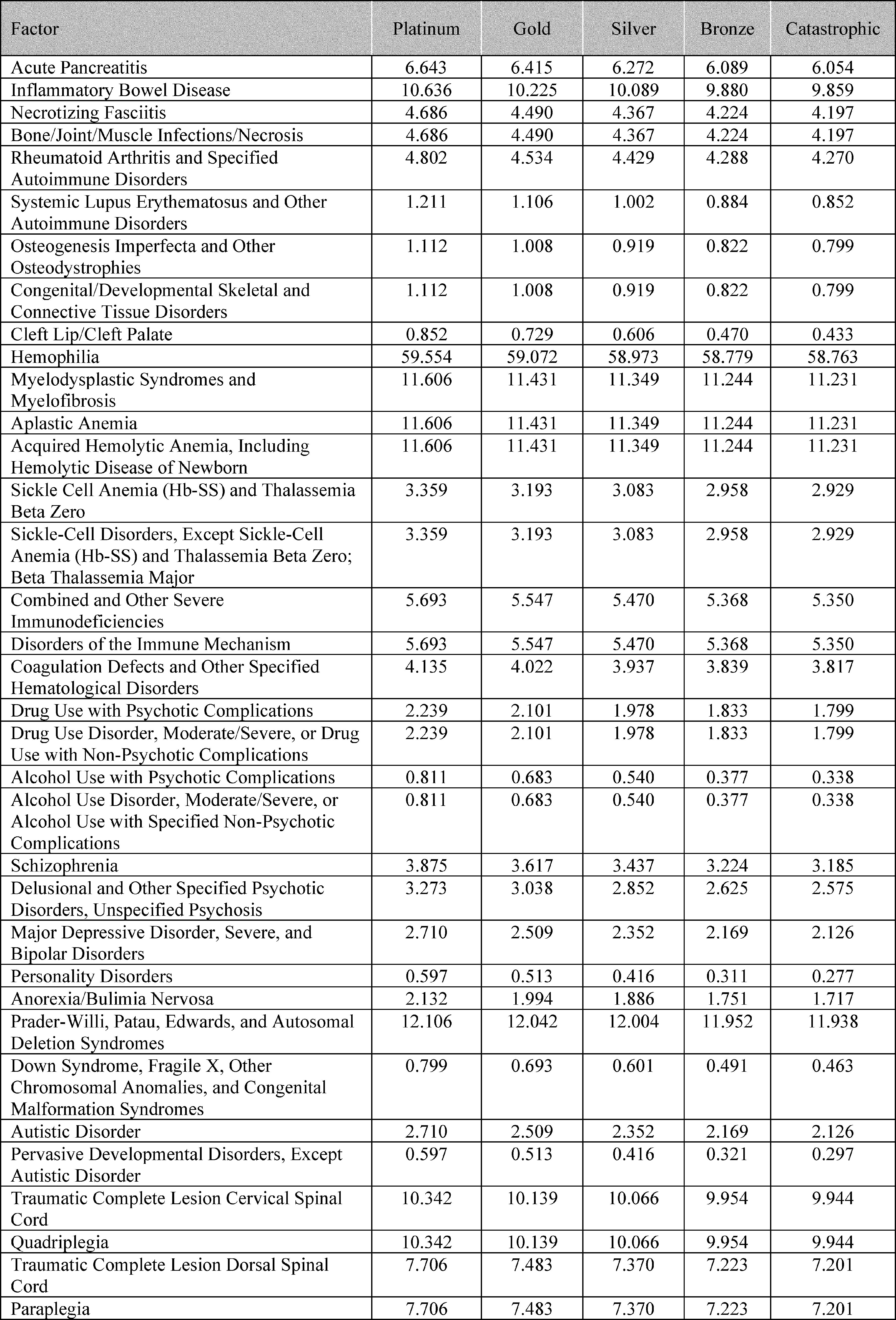
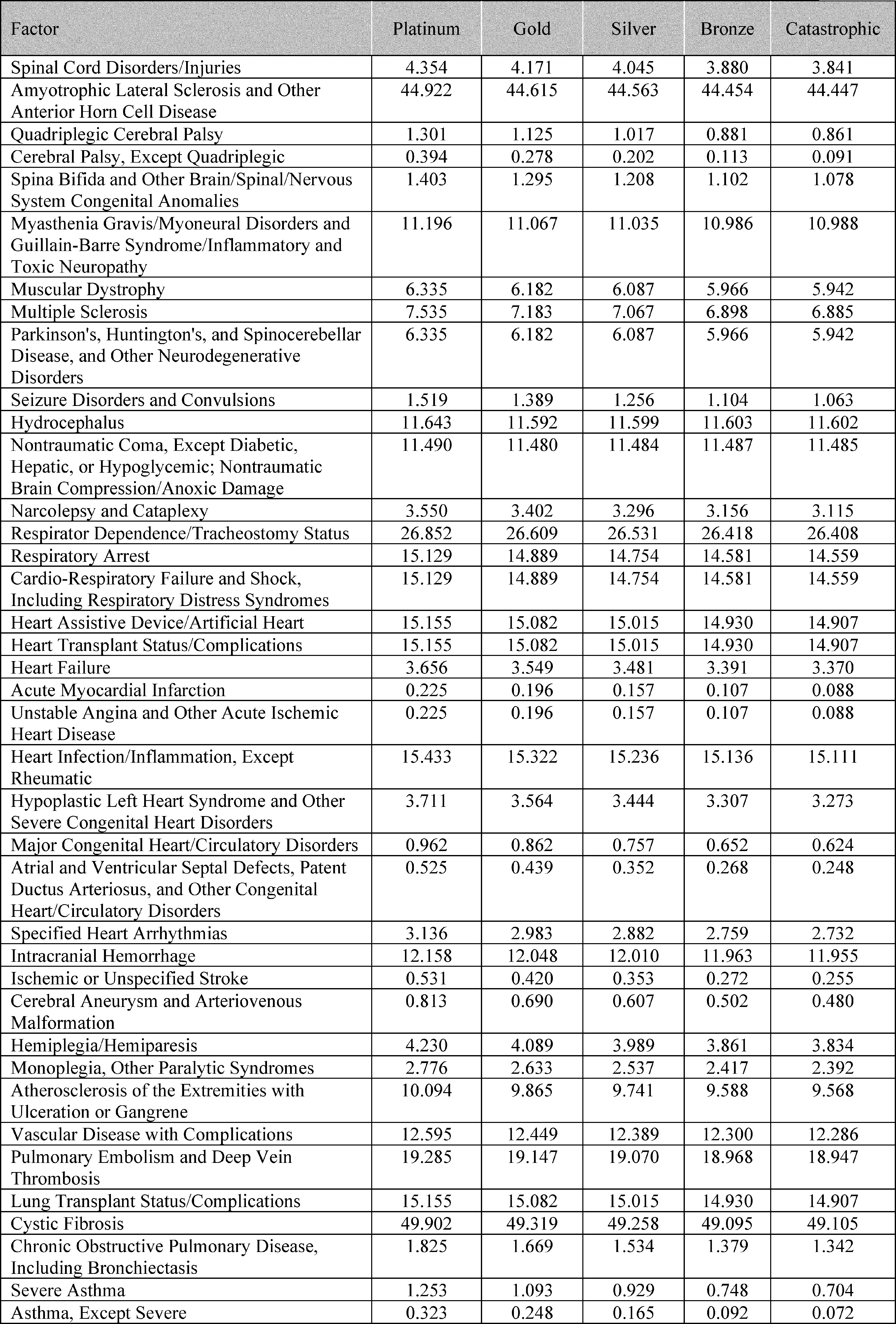
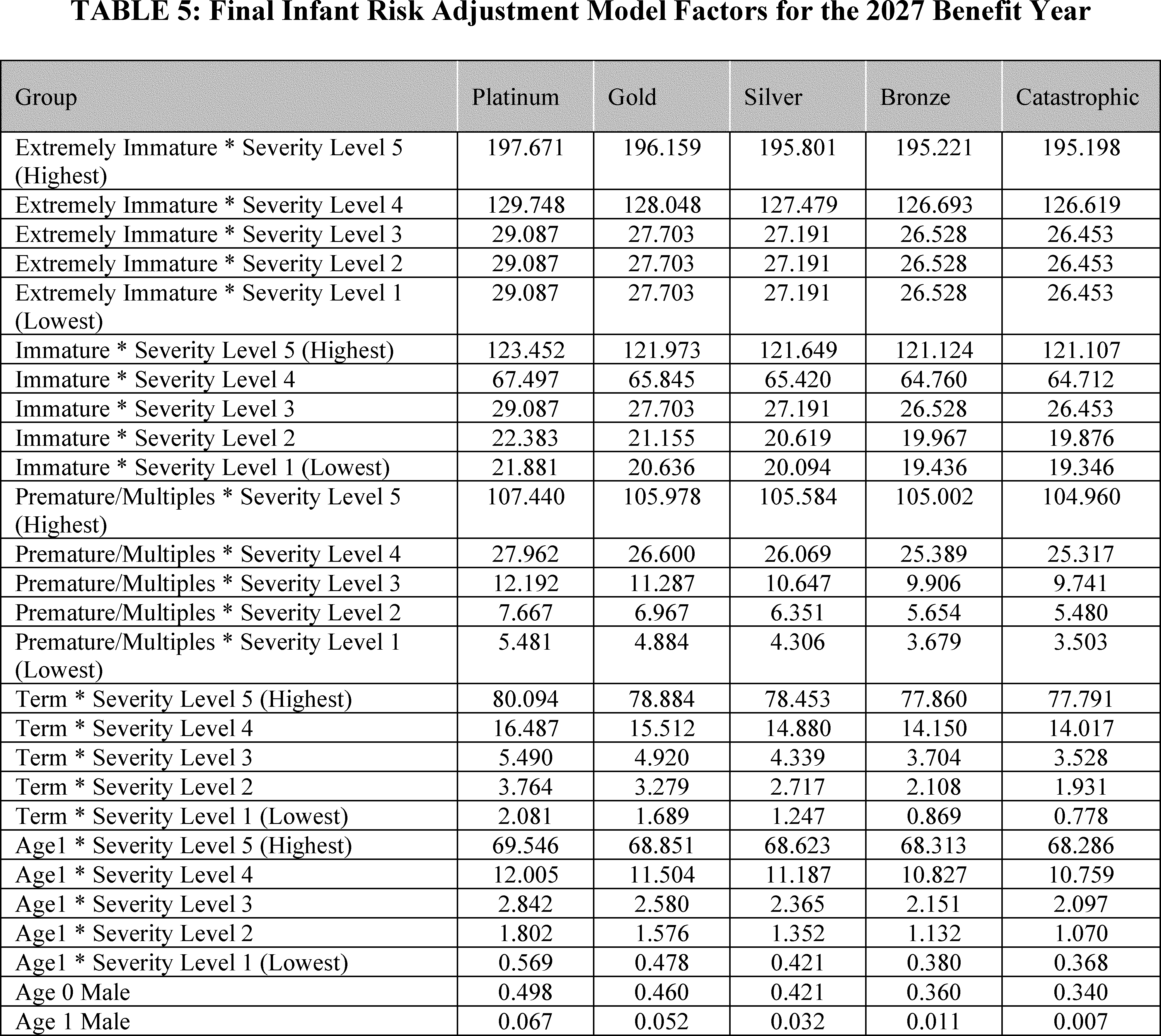
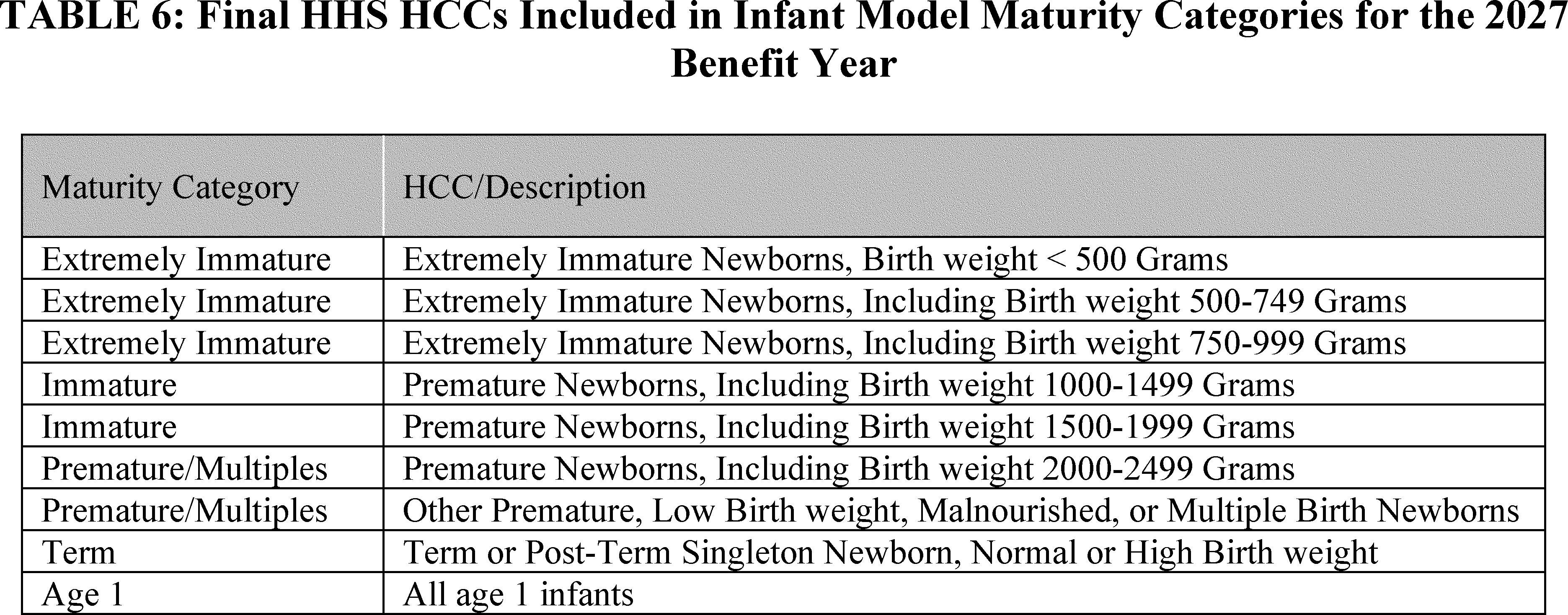
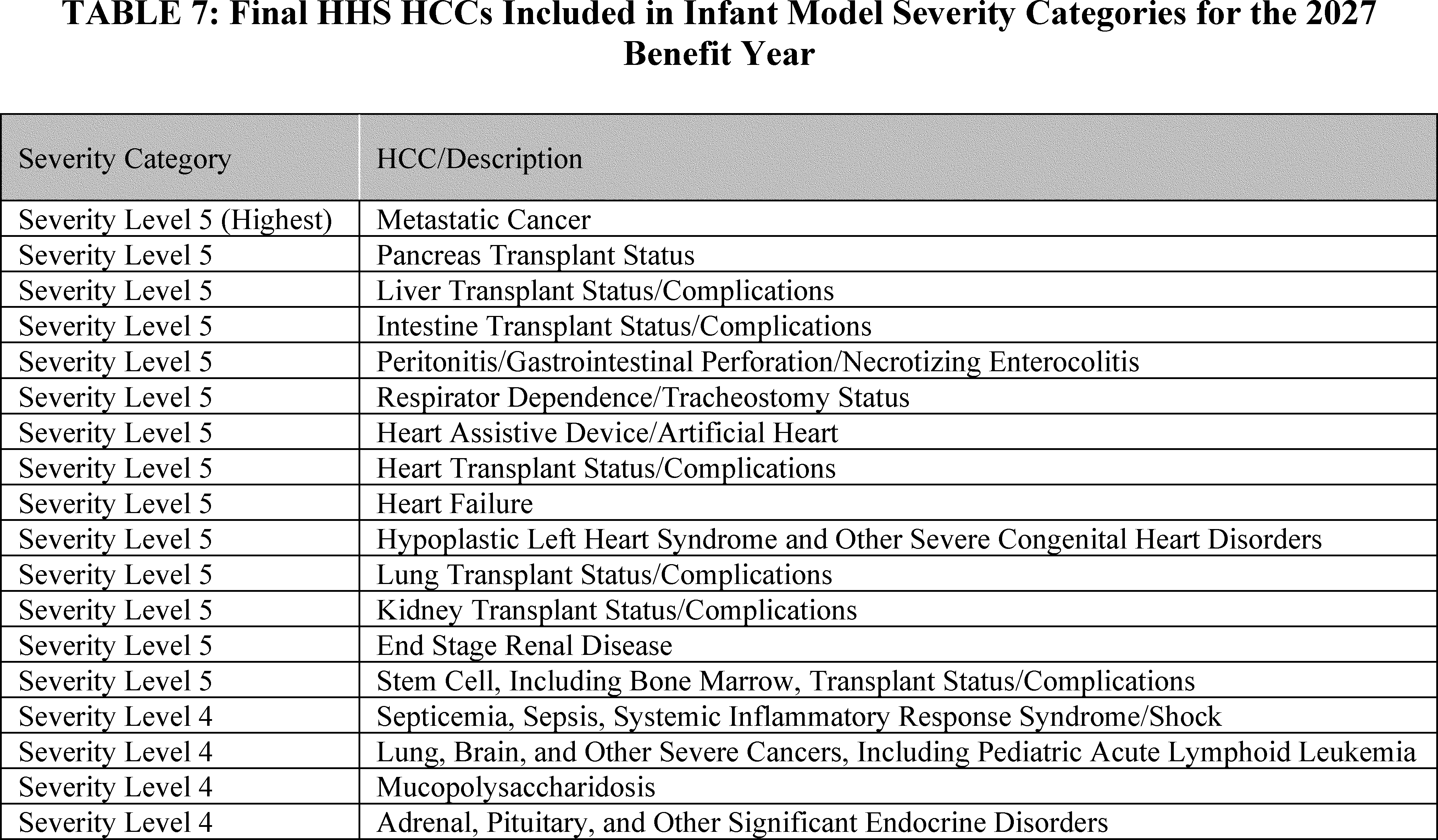
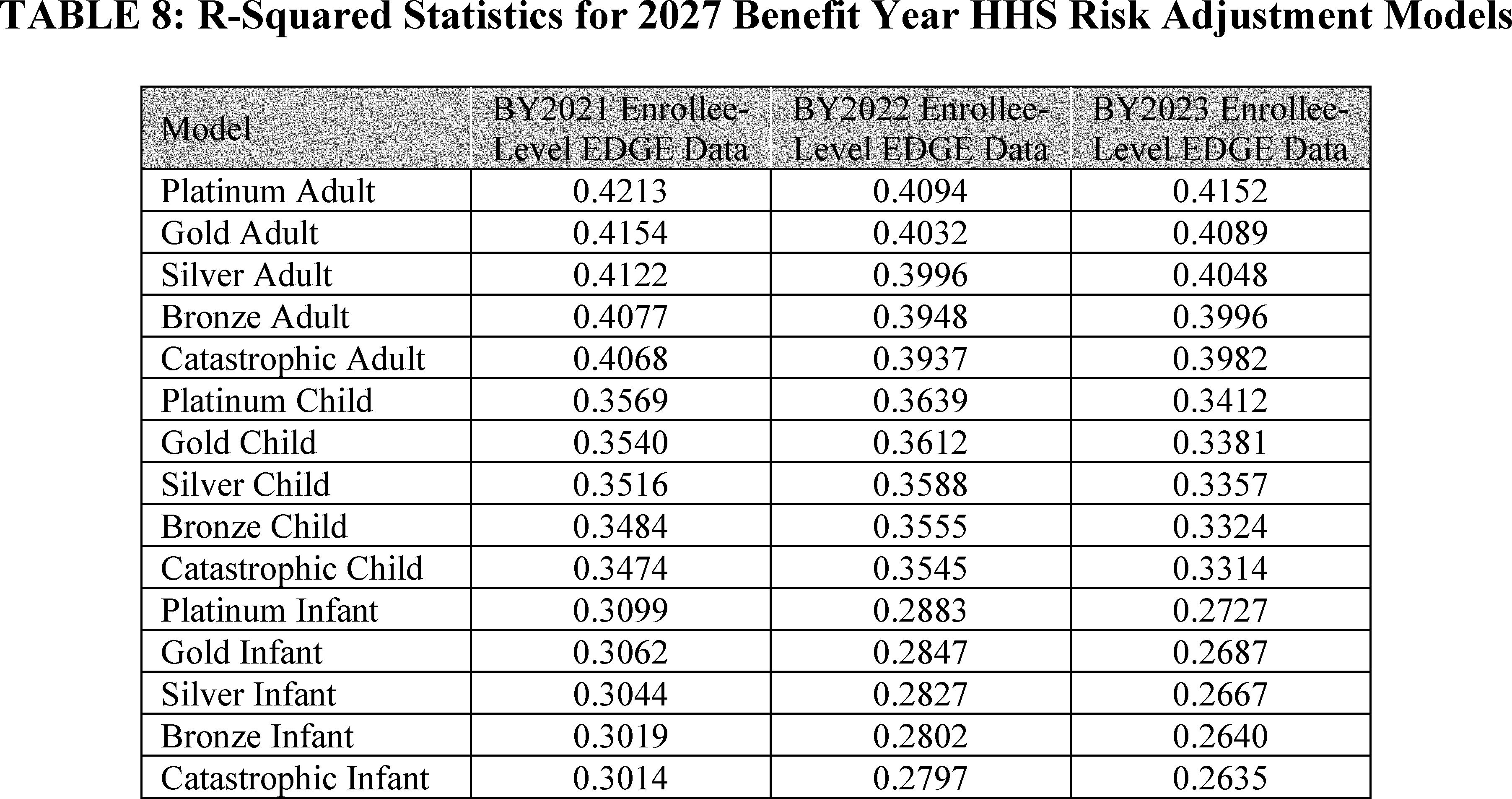
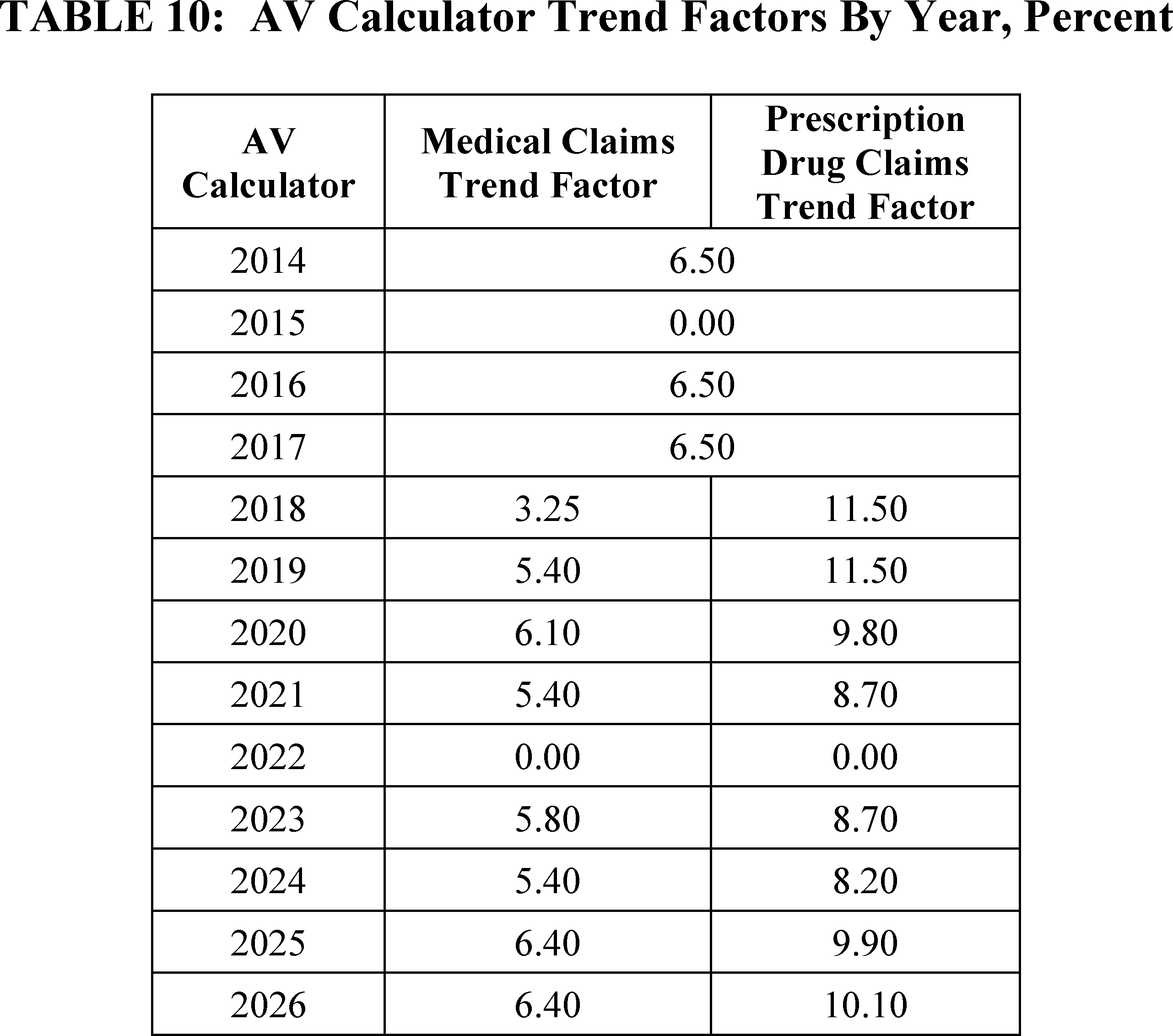
We are finalizing our proposal to recalibrate the 2027 benefit year HHS risk adjustment models using the 2021, 2022, and 2023 benefit year enrollee-level EDGE data. We are also finalizing a risk adjustment user fee rate for the 2027 benefit year of $0.18 per member per month (PMPM).
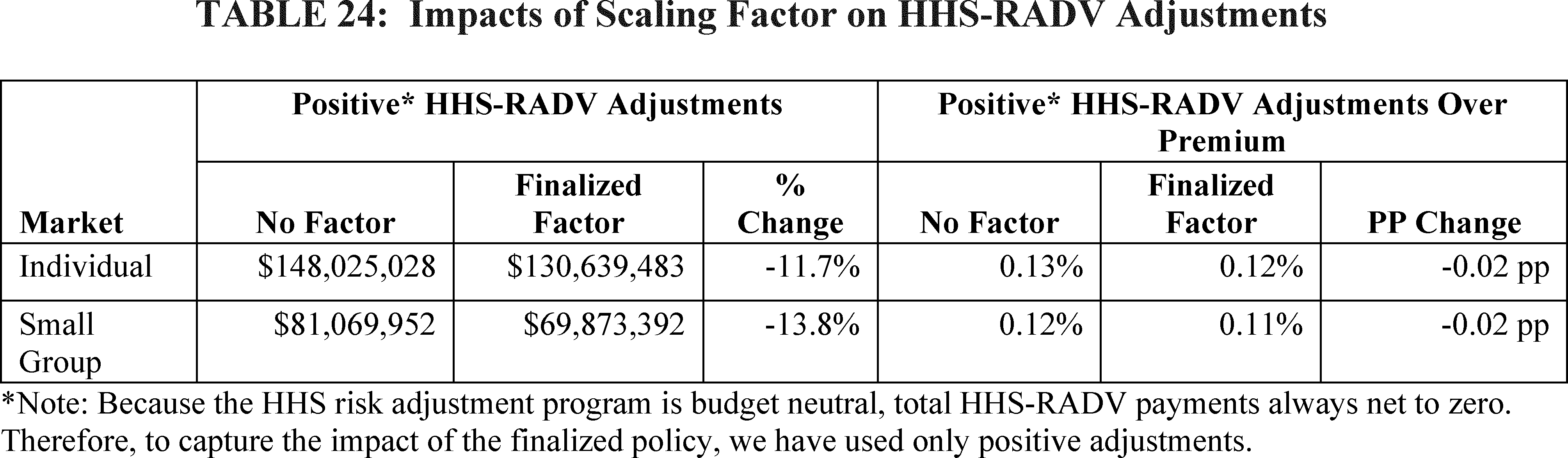
We are finalizing our proposal to modify one intermediate step of the HHS-RADV error estimation methodology starting with 2025 benefit year HHS-RADV to add an additional scaling factor to appropriately estimate the proportion of the issuer's total plan liability risk score (PLRS) that is HCC-related after the removal of no-HCC enrollees from the IVA sample beginning with 2025 benefit year HHS-RADV, as finalized in the 2026 Payment Notice (90 FR 4424).
We are finalizing our proposal to require issuers that intend to load rates to account for unpaid CSRs for the applicable rating year to submit certain information related to CSR loading in their Unified Rate Review Templates (URRTs) and the Actuarial Memoranda for each filing year in which CSRs are not funded beginning with PY 2027 rate filings.[12]
We are finalizing our proposal to remove the requirement at § 155.105(b)(4) that a State seeking to operate a State Exchange must first operate an SBE-FP for at least one plan year.
We are finalizing our proposal to amend § 155.106(a)(2) to rescind the requirement that as part of a State's activities for its establishment of a State Exchange, the State must provide supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements, given preexisting processes per the State Blueprint Application [13]
for CMS to collect supporting documentation from a State as part of a State Exchange implementation efforts.
We are finalizing our proposal to amend § 155.170 with a modification to provide that beginning with PY 2028, a State-required benefit will be considered “in addition to EHB” (and thus not EHB) if it is required by a State action taking place after December 31, 2011; applicable to the small group and/or individual markets; specific to required care, treatment, or services; and not required by State action for purposes of compliance with Federal requirements. Under this finalized policy, such State-required benefits will be considered in addition to EHB regardless of whether the required benefits are embedded in the State's EHB-benchmark plan. Further, we finalize that States must make payments in accordance with § 155.170(b) to defray the cost of any State-required benefits in addition to the EHB. We are also finalizing revisions to the regulatory text at § 156.115(a) to align with this finalized policy.
We are not finalizing amendments to § 155.205(b) to amend the requirement that a State Exchange operate a centralized eligibility and enrollment consumer interface on the Exchange's website for an individual to submit a single streamlined eligibility application and subsequently select a QHP following a determination of eligibility. However, we may consider finalizing this proposal, with or without modifications, in the 2028 Payment Notice rulemaking cycle or another appropriate rulemaking vehicle, and, if so, will respond to comments then.
We are not finalizing our proposal at § 155.221(k) that State Exchanges may elect a new EDE option (SBE-EDE option), in which a State Exchange could seek HHS approval to allow web-brokers to operate enrollment websites as the exclusive pathway through which consumers can apply, receive an eligibility determination from the Exchange, and purchase an individual market QHP offered through the Exchange with APTC and CSRs, if otherwise eligible. However, we may consider finalizing this proposal, with or without modifications, in the 2028 Payment Notice rulemaking cycle or another appropriate rulemaking vehicle.
We are finalizing changes to the existing regulatory authority under § 155.220(j)(2)(ii) and (iii) to require agents, brokers, and web-brokers to use an HHS-approved and -created consumer consent form to meet the eligibility application review requirements and consumer consent documentation requirements.[14]
We will delay the effective date of requiring the HHS-approved and -created consumer consent form so that it is required for enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j). Our finalized policy will eliminate the current flexibility, which allows agents, brokers, and web-brokers to use their own standards and templates for documentation requirements, and instead sets a universal standard that requires agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form.[15]
We considered commenters' suggestion to allow previously signed consent forms to remain valid after the effective date of these policies, but we are not adopting that approach because standardizing the use of the HHS-approved and -created consumer consent form will help ensure consumers and consumers' representatives are provided with all the necessary information before providing consent, and that HHS consistently applies the consumer consent and eligibility application review
( printed page 29534)
documentation requirements uniformly among agents, brokers, and web-brokers moving forward. We are also finalizing our proposal to revise § 155.220(j)(2)(ii) and (j)(2)(iii) to clarify what constitutes a consumer “taking an action” for eligibility application review and confirmation and providing consumer consent.
We are finalizing several new provisions at § 155.220(j)(3) to establish more robust standards of conduct related to the marketing practices of agents, brokers, and web-brokers which would include examples of prohibited marketing practices. Furthermore, we are finalizing our proposal to require agents, brokers, and web-brokers to provide HHS marketing documentation in response to monitoring, audit, and enforcement activities. We also are finalizing our proposal to notify agents, brokers, and web-brokers that they may be held responsible for marketing content created, written, released, or otherwise produced by an entity on their behalf.
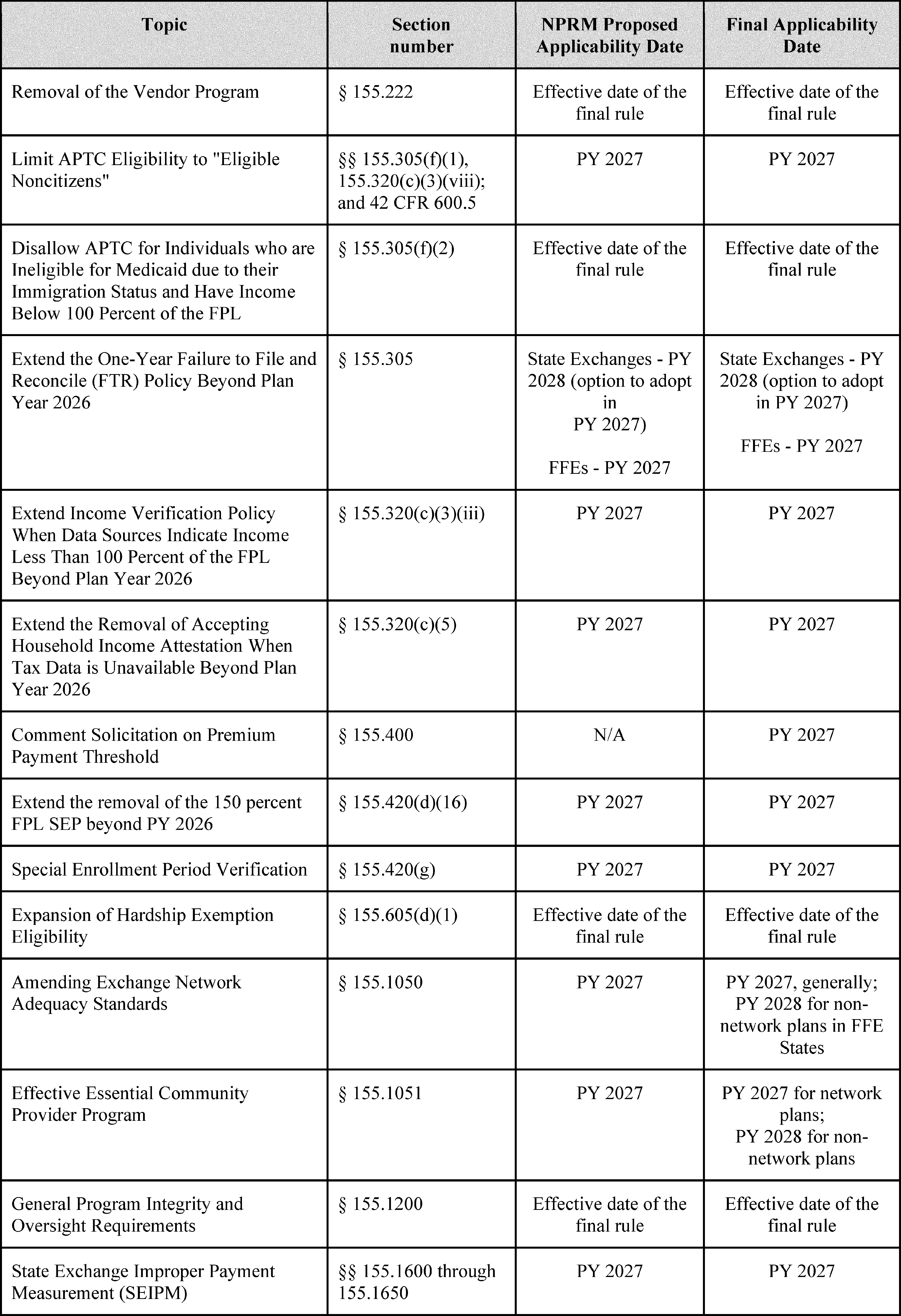
We are finalizing our proposal to discontinue the vendor program, which allows for certain training and information verification functions to be provided by HHS-approved vendors. To accomplish this, we are removing § 155.222.
We are finalizing updates in §§ 155.20, 155.305(f)(1), and 155.320 to align Exchange regulations with section 71301 of the WFTC legislation. Section 71301 of the WFTC legislation amended section 36B of the Code to provide that PTC is allowed for the QHP coverage of a lawfully present noncitizen only if such noncitizen is an “eligible alien.” It also makes conforming amendments to section 1411 of the Affordable Care Act requiring Exchanges to verify applicants' “eligible alien” status effective for plan years beginning on or after January 1, 2027. We are finalizing a new definition in § 155.20, updating our APTC eligibility regulations at § 155.305(f)(1), and adding to our verification regulations in § 155.320 to align Exchange eligibility and verification rules with section 71301 of the WFTC legislation. This finalized policy will also impact Federal payments to States effective January 1, 2027, for individuals enrolled in the BHP who are lawfully present noncitizens but are not “eligible aliens,” as Federal BHP payments attributable to these enrollees will cease beginning January 1, 2027.
To align Exchange regulations with section 71302 of the WFTC legislation, we are finalizing our proposal to remove § 155.305(f)(2) and make conforming updates to §§ 155.320(c)(3)(iii)(A) and 155.420(d)(13). Section 71302 of the WFTC legislation amended section 36B(c) of the Code to provide that PTC is no longer allowed for noncitizens lawfully present in the United States who were ineligible for Medicaid due to their immigration status and have household income below 100 percent of the FPL. Removing § 155.305(f)(2) and updating § 155.320(c)(3)(iii)(A) will align Exchange APTC eligibility and verification rules with section 71302 of the WFTC legislation. This finalized policy will also impact Federal payments to States for individuals enrolled in the BHP who are ineligible for Medicaid due to their immigration status and with household income below 100 percent of the FPL, for whom Federal payments to States are also no longer allowed.
We are finalizing our proposal to revise the failure to file and reconcile process at § 155.305(f)(4) such that Exchanges on the Federal platform will conduct the 1-year policy beginning in PY 2027. State Exchanges will have the option to conduct either the 1-year or 2-year policy in PY 2027 but will be required to conduct the 1-year policy beginning in PY 2028. Under the 1-year policy, an Exchange must determine a tax filer ineligible for APTC if: (1) HHS notifies the Exchange that the tax filer (or their spouse if the tax filer is a married couple) received APTC for a prior year for which tax data will be utilized for verification of income, and (2) the tax filer or tax filer's spouse did not comply with the requirement to file a Federal income tax return and reconcile APTC for that year. This finalized policy, which Exchanges on the Federal platform plan to adopt a year early, will align with the statutory requirement in section 71303 of the WFTC legislation that effectively requires Exchanges to follow the 1-year policy as a requirement for a month to be a coverage month under section 36B of the Code as of PY 2028. We are also finalizing our proposal to remove the notice requirement at § 155.305(f)(4)(ii) for PY 2027 to conform with the notice policy under the PY 2026 policy.
We sought comment on considerations for future policy development and implementation under section 71303 of the WFTC legislation, which imposes new requirements on Exchanges related to eligibility verification. Specifically, we sought comment on: operational considerations for interested parties; effective rollout and communications; required timelines for interested parties to comply with the law; anticipated complexity, costs, burden, enrollment impacts; and any State-specific considerations. We will take comments we received into consideration for any potential guidance or rulemaking.
We are finalizing our proposal to revise § 155.320(c) such that all Exchanges are required to continue conducting the income verifications changes introduced in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) in PY 2027 and beyond, effectively removing the requirement to stop both income verification policies starting in PY 2027. Specifically, we are updating § 155.320(c)(3)(iii) and § 155.320 (c)(3)(vi)(C)(2) to extend the requirement indefinitely to create income data matching issues (DMIs) when trusted data sources indicate that projected consumer household income is under 100 percent of the FPL. Additionally, we are removing § 155.320(c)(5), which outlines the requirement to accept the annual household income attestation when no tax data is returned for a household.
We sought comment on whether we should regulate the option for issuers to implement the fixed-dollar and/or gross percentage-based premium payment thresholds in § 155.400(g) for PY 2027 and beyond. Currently, issuers are only able to implement a net premium percentage-based premium threshold for PY 2026, and effective January 1, 2027, issuers will be able to implement the fixed-dollar and/or either net or gross premium percentage-based thresholds, which was finalized in the 2025 Marketplace Integrity and Affordability final rule. After consideration of public comments and for reasons outlined in the proposed and final rule, we are finalizing for all Exchanges the removal of the fixed-dollar and gross-premium threshold flexibilities.
We are finalizing our proposal to remove § 155.420(d)(16) such that Exchanges will continue to be prohibited from offering the 150 percent FPL SEP in PY 2027 and beyond, in alignment with section 71304 of the WFTC legislation. We are finalizing our proposal to make conforming amendments at §§ 155.420(a)(4)(ii)(D), 155.420(b)(2)(vii), and 155.420(a)(4)(iii).
We are finalizing our proposal to revise § 155.420(g) to remove the restriction for Exchanges on the Federal platform to only conduct Special Enrollment Period Verification (SEPV) for Loss of Minimum Essential Coverage (MEC). We also are finalizing our proposal to require Exchanges on the Federal platform to conduct SEPV for at least 75 percent of new enrollments. These policies were finalized in the 2025 Marketplace Affordability and Integrity final rule but were stayed in
( printed page 29535)
City of Columbus et al.
v.
Kennedy et al.[16]
We are therefore finalizing these provisions as we reproposed in the 2027 Payment Notice proposed rule.
We are finalizing our proposal to amend § 155.605 to codify and expand hardship exemption eligibility. Specifically, this finalized policy will allow individuals who are ineligible for APTC or CSRs due to projected household income below 100 percent or above 250 percent of the FPL to qualify for a hardship exemption under § 155.605(d)(1)(iii). This change will allow individuals aged 30 and older who receive this hardship exemption to enroll in catastrophic coverage, if otherwise eligible.
We are finalizing, for plan years beginning on or after January 1, 2027, our proposal to amend § 155.1050(a)(2) to remove the requirements at § 155.1050(a)(2)(i) and (ii) that State Exchanges and SBE-FPs establish and impose quantitative time and distance network adequacy standards that are at least as stringent as standards for QHPs participating on the FFEs and to no longer require State Exchanges and SBE-FPs to conduct quantitative network adequacy reviews to evaluate a plan's compliance with certain network adequacy standards under § 156.230 prior to certifying any plan as a QHP. Instead, we are finalizing our proposal to restore the requirement at § 155.1050(a)(2) that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards consistent with § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or for plan years beginning on or after January 1, 2027, § 156.236(a) for non-network plans if such plans are allowed to be offered through the Exchange, as applicable.
We also are finalizing, with minor modification, at new § 155.1050(d) our proposal to defer provider access reviews of QHP issuers, with or without a provider network, applying for certification as a QHP to be offered through the FFE, to the FFE States that elect to conduct such reviews, should the FFE State demonstrate sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program under § 155.1050(d)(2) through (d)(4). We note that provisions related to non-network plans will be implemented beginning January 1, 2028.
We are finalizing, with modification, our proposal to implement new requirements for an Effective Essential Community Provider (ECP) Review Program by adding § 155.1051. Under this finalized policy, FFE States may elect to conduct their own ECP certification reviews of issuers, with or without a provider network, that are applying for certification to be offered as a QHP through an FFE, including in States performing plan management. To conduct their own reviews, we are finalizing that FFE States will be required to demonstrate that they have sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective ECP Review Program under § 155.1051. We note that provisions related to non-network plans will be effective beginning on or after January 1, 2028.
We are finalizing our proposal to amend § 155.1200(d) and add new paragraph (e) to permit State Exchanges to satisfy certain requirements of the independent external programmatic audit, as outlined in paragraph (d), by completing the SEIPM process that will be established at 45 CFR 155, subpart Q.
We are finalizing our proposal to add new subpart Q (§§ 155.1600 through 1650) to establish the SEIPM program. The Payment Integrity Information Act of 2019 (PIIA) requires Federal agencies to annually review, measure, and report on the programs they administer that have been determined to be susceptible to significant improper payments. To satisfy the requirements of the PIIA, we are finalizing our proposal to measure improper payments of APTC that are administered by State Exchanges and to annually report statistically valid improper payment estimates in the HHS Agency Financial Report.
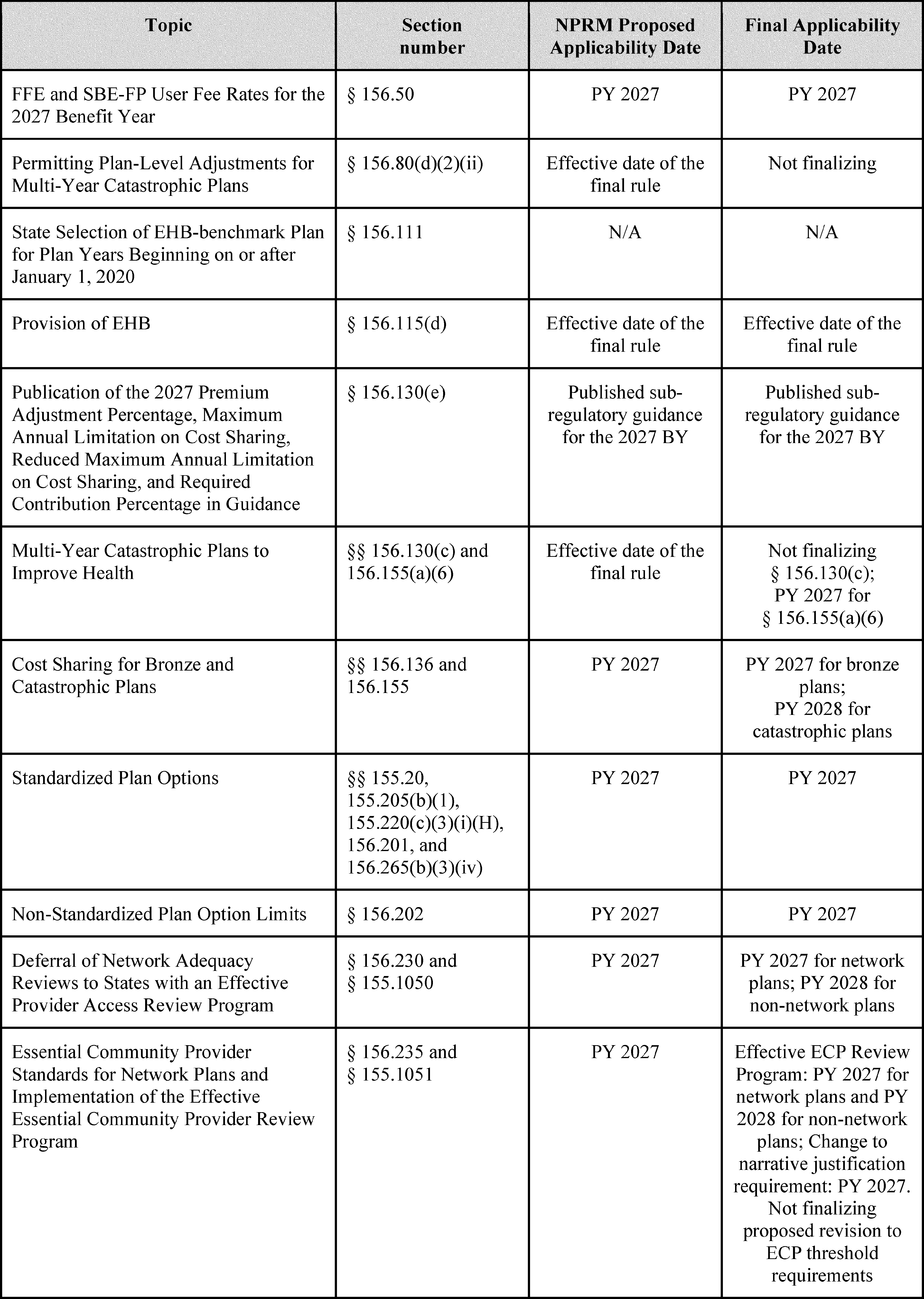
We are finalizing 2027 benefit year FFE and SBE-FP user fee rates of 1.9 percent and 1.5 percent of total monthly premiums, respectively.
We paused review of State applications to select EHB-benchmark plans in accordance with § 156.111. We are reviewing section 1302 of the Affordable Care Act and are considering future rulemaking to revise § 156.111 and EHB standards more broadly.
We are finalizing our proposal to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB.
We are finalizing, with modification, our proposals to amend the requirements for catastrophic plans in § 156.155. We specify that, effective for plan years beginning on or after January 1, 2027, a catastrophic plan has a plan term of either 1 plan year, or of multiple consecutive plan years not to exceed 10 plan years, and that catastrophic plans with terms of at least 2 consecutive plan years may utilize value-based insurance designs to provide benefits before reaching the deductible, pursuant to guidelines issued by the Secretaries of HHS, Labor, and the Treasury under section 2713(c) of the PHS Act. We are not finalizing our proposal to amend § 156.80 to permit issuers of multi-year catastrophic plans to make a plan-level adjustment to the index rate that reflects the length of the entire plan term. We also are not finalizing our proposal to amend § 156.130 to specify that, in the case of a catastrophic plan with a consecutive multi-year term, the annual limitation on cost sharing for the initial plan year of the contract may apply on an annual basis, or on average over the life of the contract.
To address an issue that has arisen in the implementation of section 1302(c) through (e) of the Affordable Care Act, we are finalizing changes to (1) the permissible cost-sharing parameters for individual market bronze plans through new § 156.136 effective beginning PY 2027, with modification to specify that such plans are permitted to exceed the standard annual limitation on cost sharing by up to 130 percent of the standard annual limitation on cost sharing, and (2) the required cost-sharing parameters for catastrophic plans through revisions to § 156.155(a)(3) with a modification to have the revisions to § 156.155(a)(3) be effective beginning PY 2028.
We are finalizing our proposal to remove the following from our regulations effective beginning in PY 2027: the definition of “standardized options” at § 155.20; all requirements pertaining to standardized plan options at § 156.201; the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv); the annual design and publication of these standardized plan options in the applicable Payment Notice for each plan year; and non-standardized plan option limits and exceptions at § 156.202.
We are finalizing our proposal to revise the network adequacy and ECP standards at §§ 156.230 and 156.235 to make clear that these sections contain the provider access standards for all individual market QHPs and stand-alone dental plans (SADPs) and all
( printed page 29536)
Small Business Health Options Program (SHOP) QHPs across all QHP issuers that use a network of providers. We also are finalizing our proposal to revise these sections to remove the requirement that all QHPs must use a network of providers.
Additionally, we are finalizing our proposal to revise § 156.230 to provide that HHS will continue to conduct network adequacy reviews using standards described at § 156.230 for QHP issuers that use a provider network in FFE States that do not elect to conduct such reviews, or in FFE States that HHS has determined do not satisfy the criteria to be considered to have an Effective Provider Access Review Program, as described at § 155.1050(d). We also are finalizing our proposal to add new § 156.236 to allow plans that do not use a network (non-network plans) to receive QHP certification, effective beginning in PY 2028, by demonstrating that they ensure a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, and reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full. As finalized, § 156.236 will set forth provider access and ECP requirements for assessing whether non-network plans provide sufficient choice of providers.
For PY 2027 and subsequent plan years, we are finalizing, with modification, our proposed changes to the QHP certification requirements for ECPs included within a network plan issuer's provider network. First, we are not finalizing our proposal to reduce the minimum percentage requirement from 35 to 20 percent for both medical QHP and SADP issuers. Second, we are finalizing our proposal to modify the narrative justification requirements at §§ 156.235(a)(3) and 156.235(b)(3) to be consistent with systems changes and existing QHP issuer ECP data submission requirements as part of ECP certification reviews.
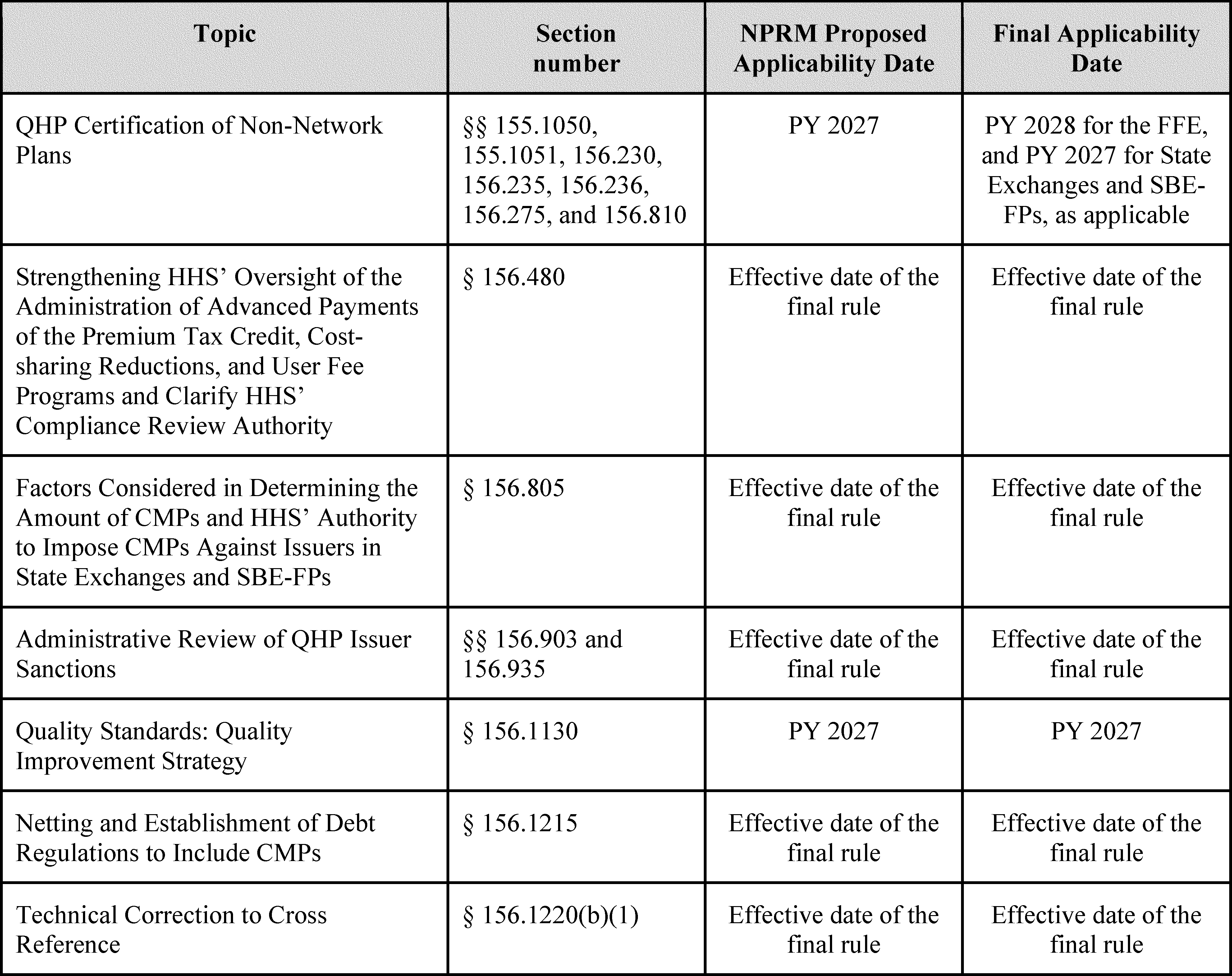
We are finalizing our proposal to modify § 156.480(c) to clarify HHS' authority to audit or conduct a compliance review of an issuer that offers a QHP through an Exchange for the purposes of administering and providing oversight of the APTC, CSR, and user fee programs. We are also finalizing that HHS may conduct a compliance review to assess issuers' compliance with requirements related to these programs as needed or on an annual basis rather than only on an ad hoc basis.
We are finalizing our proposal to amend § 156.805(b) to reiterate in § 156.805(b) that in determining the amount of CMPs, in addition to the factors HHS takes into account when determining a CMP amount listed in § 156.805(b)(1) through (3), HHS will identify the lawful purpose or purposes of the CMP. We are also finalizing our proposal to amend the introductory text of § 150.317 to make corresponding edits for the factors HHS, through CMS, considers when determining the amount of CMPs as enforcement remedies against issuers more broadly or other responsible entities, such as a non-Federal governmental plan sponsor that is subject to applicable PHS Act requirements. In addition, we are finalizing our proposal to amend § 156.805(f) to reiterate that HHS has the authority to impose CMPs against issuers in a State Exchange or SBE-FP for an identified violation of any Exchange requirements applicable to issuers offering a QHP in an Exchange, when a State notifies HHS that it is not enforcing these requirements or HHS determines that a State is failing to substantially enforce these requirements.
We are finalizing our proposal to amend § 156.903 to provide the option for an administrative law judge (ALJ) to issue subpoenas, upon his or her own motion or at the request of a party, if reasonably necessary for the full presentation of a case and to add procedures governing the process for issuing subpoenas. We are also finalizing our proposal to amend § 156.935 to ensure that the discovery provisions set forth therein do not apply to administrative appeals of proposed CMPs for violations identified through audits of the APTC, CSR, or user fee programs conducted in accordance with § 156.480(c).
We are finalizing our proposal to require QHP issuers to submit QISs addressing any two of the five topic areas listed in section 1311(g)(1) of the Affordable Care Act, without mandating which specific topics areas a QHP issuer will be required to address to meet the QIS statutory certification requirement, beginning with PY 2027.
We are finalizing our proposal to amend § 156.1215(b) to provide that CMPs assessed against health coverage issuers and their affiliates under the same taxpayer identification (TIN) number will be subject to netting as part of HHS' integrated monthly payment and collection cycle. We are also finalizing our proposal to amend § 156.1215(c) to provide that any amount owed to the Federal Government by an issuer and its affiliates for unpaid CMP amounts, after HHS nets amounts owed by the Federal Government, will be the basis for calculating the debt.
We are finalizing a technical correction to update a cross reference in § 156.1220.
We sought comment on the impact of the Federal MLR standard on individual market stability and whether HHS should use its authority under section 2718(b)(1)(A)(ii) of the PHS Act and § 158.301 to adjust the Federal MLR standard in a State to promote individual market stability. We also solicited comment on whether and how to amend regulations allowing States to request an adjustment to the MLR standard in their individual market to reduce burden and encourage States to request adjustments, as appropriate, in their State markets. We will take comments we received into consideration as we continue to consider potential adjustments to the Federal MLR standard for particular States' individual health insurance markets.
III. Summary of the Proposed Provisions, Public Comments, and Responses to Comments on the Proposed Rule
A. Part 150—CMS Enforcement in Group and Individual Insurance Markets
1. Factors CMS Uses To Determine the Amount of a Civil Money Penalty (CMP) (§ 150.317)
In the 2027 Payment Notice proposed rule (91 FR 6292, 6327), to align with the proposal discussed in section III.E.14. of the proposed rule, which would reiterate in § 156.805(b) what factors HHS considers when determining the amount of CMPs as enforcement remedies against QHP issuers in Exchanges, we proposed a conforming amendment to § 150.317 introductory text to clarify that HHS, through CMS, will identify the lawful purpose or purposes of the penalty, and take into account the enumerated factors as appropriate for the circumstances. In proposing the conforming edits to § 150.317, we did not propose other changes to the legal bases and procedural processes for imposing CMPs.
We requested comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and section III.E.14. of this final rule, including our responses to comments, we are finalizing as proposed an amendment to the introductory text of § 150.317 to make
( printed page 29537)
corresponding edits for the factors HHS considers when determining the amount of CMPs as enforcement remedies against issuers more broadly or other responsible entities, such as a non-Federal governmental plan sponsor that is subject to applicable PHS Act requirements. We summarize and respond to public comments received on the proposed conforming amendment for the factors HHS considers when determining the amount of CMPs as enforcement remedies at § 156.805(b) in section III.E.14. of this final rule.
B. Part 153—Standards Related to Reinsurance, Risk Corridors, and Risk Adjustment
In subparts A, B, D, G, and H of part 153, we established standards for the administration of the risk adjustment program. The risk adjustment program is a permanent program created by section 1343 of the Affordable Care Act that transfers funds from issuers of risk adjustment covered plans that have lower-than-average risk enrollees to issuers of risk adjustment covered plans that have higher-than-average risk enrollees, which includes issuers with plans in the individual, small group, or merged markets, inside and outside the Exchanges. In accordance with § 153.310(a), a State that is approved or conditionally approved by the Secretary to operate an Exchange may establish a risk adjustment program or have HHS do so on the State's behalf.[17]
HHS did not receive any requests from States to operate risk adjustment for the 2027 benefit year. Therefore, HHS will operate risk adjustment in every State and the District of Columbia for the 2027 benefit year.
1. Sequestration
In accordance with the OMB Report to Congress on the Joint Committee Reductions for Fiscal Year 2026, the HHS-operated risk adjustment program is subject to the fiscal year 2026 sequestration.[18]
The Federal Government's 2026 fiscal year began on October 1, 2025. Therefore, the HHS-operated risk adjustment program is sequestered at a rate of 5.7 percent for payments made from fiscal year 2026 resources (that is, funds collected during the 2026 fiscal year).
HHS, in coordination with OMB, has determined that, under section 256(k)(6) of the Balanced Budget and Emergency Deficit Control Act of 1985 (BBEDCA),[19]
as amended, and the underlying authority for the HHS-operated risk adjustment program, the funds that are sequestered in fiscal year 2026 from the HHS-operated risk adjustment program will become available for payment to issuers in fiscal year 2027 without further congressional action. If Congress does not enact deficit reduction provisions that replace the Joint Committee reductions, the program would be sequestered in future fiscal years, and any sequestered funding would become available in the fiscal year following that year in which the funds were sequestered.
Additionally, we note that the Infrastructure Investment and Jobs Act [20]
amended section 251A(6) of the BBEDCA to extend the sequestration first mandated under the Budget Control Act of 2011 for all non-exempt direct spending programs, including the HHS-operated risk adjustment program, through fiscal year 2031 at a rate of 5.7 percent per fiscal year.[21]
We summarize and respond to public comments received on the HHS-operated risk adjustment program's sequestration rate of 5.7 percent for payments made from fiscal year 2026 resources (that is, funds collected during the 2026 fiscal year).
Comment:
One commenter acknowledged the fiscal year 2026 sequestration rate. Another commenter noted that the sequestration rate applied to fiscal year 2026 collected funds will continue affecting risk adjustment State transfer amounts, which may noticeably impact small issuer margins. Therefore, the commenter recommended ongoing monitoring of solvency and market participation by HHS.
Response:
Although we acknowledge a delay in risk adjustment payments to issuers when funds are sequestered, in accordance with the BBEDCA, any sequestered funds will become available for payments to issuers in the next fiscal year. This sequestration of risk adjustment funds has occurred since the 2015 fiscal year (that is, the 2014 benefit year and first year of the HHS-operated risk adjustment program) and therefore, issuers, including small issuers, are familiar with this process and can anticipate this delay in their risk adjustment payments.
Additionally, we appreciate the recommendation regarding ongoing monitoring of solvency and market participation and note that HHS conducts ongoing monitoring of solvency and market participation each year across issuers of various sizes, including consulting with our actuaries and States.
For reasons outlined in the proposed rule and this final rule, the HHS-operated risk adjustment program will sequester payments made from fiscal year 2026 resources (that is, funds collected during the 2026 fiscal year) at a rate of 5.7 percent.
2. HHS Risk Adjustment (§ 153.320)
The HHS risk adjustment models predict plan liability for an average enrollee based on that person's age, sex, and diagnoses (also referred to as hierarchical condition categories (HCCs)), producing a risk score. The State payment transfer formula [22]
that is part of the HHS Federally certified risk adjustment methodology utilizes separate models for adults, children, and infants to account for clinical and cost differences in each age group.
In the adult and child models, the relative risk assigned to an individual's age, sex, and diagnoses are added together to produce an individual risk score. Additionally, to calculate enrollee risk scores in the adult models, we added enrollment duration factors beginning with the 2017 benefit year,[23]
and prescription drug categories (RXCs) beginning with the 2018 benefit year.[24]
Starting with the 2023 benefit year, we removed the severity illness factors in the adult models and added interacted HCC count factors (that is, additional
( printed page 29538)
factors that express the presence of a severity or transplant HCC in combination with a specified number of total payment HCCs or HCC groups on the enrollee's record) to the adult and child models [25]
applicable to certain severity and transplant HCCs (87 FR 27224 through 27228).[26]
Starting with the 2026 benefit year (90 FR 4424 at 4438), we added a new type of model factor in the adult and child models to account for risk associated with non-demographic enrollee characteristics that do not indicate the presence of a specific active medical condition. We referred to the new type of factor as an “affiliated cost factor” (ACF), thereby distinguishing this new type of factor from RXCs and HCCs, which do indicate the presence of a specific active medical condition.
Infant risk scores are determined by inclusion in one of 25 mutually exclusive groups, based on the infant's maturity and the severity of diagnoses. If applicable, the risk score for adults, children, or infants is multiplied by a cost-sharing reduction (CSR) adjustment factor.[27]
The enrollment-weighted average risk score of all enrollees in a particular risk adjustment covered plan (also referred to as the plan liability risk score (PLRS)) within a geographic rating area is one of the inputs into the State payment transfer formula, which determines the State transfer payment or charge that an issuer will receive or be required to pay for that plan for the applicable State market risk pool for a given benefit year. Thus, the HHS risk adjustment models predict average group costs to account for risk across plans, in keeping with the Actuarial Standards Board's Actuarial Standards of Practice for risk classification.
a. Data for HHS Risk Adjustment Model Recalibration for the 2027 Benefit Year
In the 2027 Payment Notice proposed rule (91 FR 6327), we proposed to recalibrate the 2027 benefit year HHS risk adjustment models with the 2021, 2022, and 2023 benefit years' enrollee-level EDGE data. Consistent with the approach outlined in the 2020 Payment Notice (84 FR 17454 through 17464), we proposed to recalibrate the HHS risk adjustment models for the 2027 benefit year using only enrollee-level EDGE data, and to continue to use blended, or averaged, coefficients from 3 years of separately solved models for the 2027 benefit year model recalibration. Additionally, in the 2027 Payment Notice proposed rule (91 FR 6327), and as outlined in the 2022 Payment Notice (86 FR 24140, 24152), we proposed to use the 3 most recent consecutive years of enrollee-level EDGE data that are available at the time we estimate the draft recalibrated coefficients published in the final rule for the applicable benefit year.[28]
We noted that we believe this promotes stability, meets the goal of the HHS-operated risk adjustment program, and allows issuers more time to incorporate this information when pricing their plans for the upcoming benefit year.
Consistent with our prior approach when a new benefit year of enrollee-level EDGE data becomes available,[29]
we performed reviews of the 2023 benefit year enrollee-level EDGE data to identify potential anomalies prior to incorporating the 2023 benefit year enrollee-level EDGE data as part of the proposed recalibration of the HHS risk adjustment models. Our review did not identify systematic anomalies in the 2023 benefit year enrollee-level EDGE data. Therefore, after considering these analyses, we proposed to determine coefficients for the 2027 benefit year HHS risk adjustment models based on a blend of separately solved coefficients from the 2021, 2022, and 2023 benefit years' enrollee-level EDGE data, with the costs of services identified from the data trended between the relevant year of data and the 2027 benefit year.[30] [31]
The coefficients tables (Tables 2 through 7) reflect the use of trended 2021, 2022, and 2023 benefit year enrollee-level EDGE data, as well as other HHS risk adjustment model updates (including, for example, the multi-year approach finalized in the 2026 Payment Notice (90 FR 4438 through 4440) to phase out the market pricing adjustment to the plan liability associated with Hepatitis C drugs in the HHS risk adjustment models and align Hepatitis C drugs' trending with the trending approach for specialty drugs [32]
).
We sought comment on the proposal to determine 2027 benefit year coefficients for the HHS risk adjustment models based on a blend of separately solved coefficients from the 2021, 2022, and 2023 benefit year enrollee-level EDGE data.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing the 2027 benefit year
( printed page 29539)
coefficients for the HHS risk adjustment models based on a blend of separately solved coefficients from the 2021, 2022, and 2023 benefit year enrollee-level EDGE data, as proposed. We summarize and respond to public comments received on the proposed recalibration of the 2027 benefit year risk adjustment models using 2021, 2022, and 2023 benefit year enrollee-level EDGE data below.
Comment:
A few commenters supported utilizing the 2021, 2022, and 2023 enrollee-level EDGE data to recalibrate the HHS risk adjustment models for the 2027 benefit year as proposed. Other commenters opposed or stated concern about using these years of enrollee-level EDGE data due to concerns about the potential impact of the COVID-19 public health emergency (PHE) on some of these benefit years of enrollee-level EDGE data. A commenter stated that the SEPs available between 2021 and 2023, particularly the SEP for enrollees at or below 150 percent the Federal Poverty Level (FPL), skewed the value of the enrollment duration factors, stating that the expanded SEP eligibility led to many lower-risk individuals joining the market as partial year enrollees and deflated the value of the enrollment duration factors. In this regard, this commenter noted that the proposed 2027 benefit year enrollment duration factors were lower than in prior benefit years.
Response:
We are finalizing the use of the 2021, 2022, and 2023 enrollee-level EDGE data to recalibrate the 2027 benefit year HHS risk adjustment models as proposed. As described in the 2026 Payment Notice (90 FR 4437), our analyses found the 2021 and 2022 benefit year enrollee-level EDGE data is sufficiently similar to prior years of enrollee-level EDGE data such that exclusion of these data years from risk adjustment model recalibration is not warranted. Additionally, as described in the proposed rule (91 FR 6305), our analysis likewise did not identify any data anomalies that would justify excluding 2023 benefit year enrollee-level EDGE data from HHS risk adjustment model recalibration.
We recognize that it is important to carefully consider the impact of using a benefit year of enrollee-level EDGE data in the annual recalibration of the HHS risk adjustment models in situations where a benefit year of data could have significant changes that differentially impact certain conditions or populations relative to others or is sufficiently anomalous relative to expected future patterns of care.[33]
This includes consideration of whether to exclude or adjust that benefit year of data to increase the models' predictive validity or otherwise limit the impact of anomalous trends. For this reason, we conducted extensive analysis on the 2020 benefit year enrollee-level EDGE data to consider its inclusion in HHS risk adjustment model recalibration, as described in the 2024 Payment Notice proposed rule (87 FR 78214 through 78218) and final rule (88 FR 25749 through 25754).
Likewise, when we conducted recalibration of the 2025 and 2026 benefit year risk adjustment models, we conducted similar analyses on the 2021 and 2022 benefit year enrollee-level EDGE data as we did to the 2020 benefit year enrollee-level EDGE data to examine the potential impact of the COVID-19 PHE. We did not find any notable anomalous trends and determined that deviations identified in the 2020 through 2022 benefit year data were within the expected level for any individual data year. As described in the proposed rule (91 FR 6304), we repeated this analysis with the 2023 benefit year enrollee-level EDGE data and did not find any notable anomalous trends. In addition, the blending of the coefficients from the separately solved models further stabilizes any differences across years. As the underlying 2021 and 2022 benefit years' enrollee-level EDGE data used to recalibrate the 2026 benefit year risk adjustment models are identical to the 2021 and 2022 benefit year enrollee-level EDGE data used to recalibrate the 2027 benefit year risk adjustment models, and only differ in that they are trended forward one more year to capture projected 2027 benefit year medical expenditures, the analyses and conclusions discussed in prior rulemaking for those benefit years of data equally apply to the recalibration of the HHS risk adjustment models for the 2027 benefit year.
With respect to the comment about the impact of SEPs available between 2021 and 2023 on enrollment duration factors, we conducted an analysis to examine to what extent changes in the enrollment duration factors could be attributed to these SEPs, including the SEP for enrollees at or below 150 percent FPL, and did not find cause for concern related to the impact of expanded SEP eligibility. Additionally, we note that as currently specified in the HHS risk adjustment models,[34]
the HCC-contingent enrollment duration factors with which the commenter is concerned are assigned to enrollees only if the enrollee also has an HCC appearing in their enrollee-level EDGE data. As such, we would not expect these factors to be impacted by an influx of partial year low-risk enrollees as described in the comment. However, in response to this comment, we further reviewed the HCC-contingent enrollment duration factors since they were first finalized in the 2023 Payment Notice (87 FR 27228 through 27230), and found that the factors were generally at their lowest in the 2023 benefit year, which were recalibrated using 2017, 2018, and 2019 benefit year enrollee-level EDGE data. Notably, these data were not impacted by the SEP specifically identified by the commenter, which was not available until November 26, 2021, the effective date of part 3 of the 2022 Payment Notice (86 FR 53412). As such, we do not presently see evidence that decreases in enrollment duration factors are attributable to the expanded SEP eligibility.
Furthermore, we note that in our annual recalibration of the HHS risk adjustment models, we use blended, or averaged, coefficients from 3 years of separately solved models to provide stability for the risk adjustment coefficients year-to-year, while reflecting the most recent years' claims experience available. We believe that this approach continues to provide stability for all risk adjustment model coefficients, including those of the HCC-contingent enrollment duration factors. However, we also note that the purpose for recalibrating the risk adjustment models on annual basis is to reflect changes in claims experience over time. As such, the mere increase or decrease of a coefficient between benefit years of the risk adjustment models is not necessarily indicative of an issue with the factor or the data.
For these reasons, HHS did not propose and is not finalizing any changes to the HCC-contingent enrollment duration factors as part of this rule. However, as more data years become available, we will continue to
( printed page 29540)
investigate the performance of the HCC-contingent enrollment duration factors. Specifically, as the SEP landscape changes and we have new data to reflect those changes, we will assess the extent to which the HCC-contingent enrollment duration factors fully capture the financial impact of enrollment duration for enrollees who enroll during an SEP. Additionally, we acknowledge that the role of the HCC-contingent enrollment duration factors is to more directly reflect the experience of partial year enrollees, thereby reducing issuers' incentives for risk selection by improving model prediction.[35]
However, as we explain later in this rule, we are also interested in identifying additional incentives for issuers to invest in the long-term health of their enrollees, particularly with regard to preventive services. Although we are declining to make changes to the HCC-contingent enrollment duration factors at this time, we will continue to evaluate these factors and the HHS risk adjustment models to ensure they are appropriately accounting for condition-based risk without producing unintended consequences.
Comment:
One commenter requested that HHS begin including enrollees with capitated claims in the recalibration data set on the basis that many enrollees with capitated claims have a large proportion of costs that do not come from capitated sources. This commenter further noted that enrollees with capitated claims have materially different risk profiles than enrollees without capitated claims, which may have implications for the HHS risk adjustment model coefficients.
Response:
We did not propose modifying our exclusion of enrollees with capitated claims from data used for risk adjustment recalibration for the 2027 benefit year and are not making any change to this policy as part of this final rule. However, we will continue to consider this comment for potential future benefit year recalibration efforts and would propose any changes in future notice and comment rulemaking. As acknowledged by the commenter, we presently exclude enrollees with at least one capitated claim in EDGE from HHS risk adjustment model recalibration because we have some concerns that the methods for computing and reporting derived amounts from capitated claims could be inconsistent across issuers and would not provide reliable or comparable data.[36]
Although HHS currently excludes enrollees with capitated claims for purposes of the risk adjustment model recalibration activities, we plan to continue to evaluate this data and whether to include these enrollees in recalibrating the models in future benefit years.
Comment:
One commenter requested that HHS provide State payment transfer simulation results to help issuers evaluate the effects of the proposed model updates. Another commenter requested a narrative explanation of all substantial changes in coefficients between the 2026 benefit year and 2027 benefit year HHS risk adjustment models.
Response:
The 2027 benefit year HHS risk adjustment model coefficients finalized in this proposed rule are very similar to those finalized for the previous benefit year [37]
and generally varied from their 2026 benefit year values less than we have observed in previous year-to-year changes (Table 1). For example, the age-sex coefficients for the 2027 benefit year HHS risk adjustment models varied from 2026 benefit year values by a median of ±3.7 percent, whereas the median year-to-year change for age-sex factors across all previous HHS risk adjustment model recalibrations is ±9.1 percent. In contrast, the 2027 benefit year coefficients for the adult enrollment duration factors varied from their 2026 benefit year coefficients by a median of ±10.3 percent, whereas the median year-to-year change for HCC-contingent enrollment duration factors since the 2023 benefit HHS risk adjustment models in which they were introduced is ±9.8 percent. However, these values are within 0.5 percentage points of one another, and therefore, we believe these variations fall within the expected range for normal year-to-year variations.
( printed page 29541)
Additionally, we note that the commenter who requested a narrative explanation of substantial changes in the HHS risk adjustment model coefficients did not specify any particular factors that they believe rise to the level of substantial change or otherwise offer a definition of what they viewed as qualifying as “substantial” changes, impeding our ability to provide such a narrative. However, at the same time, we reiterate that the purpose for recalibrating the risk adjustment models on an annual basis is to reflect changes in claims experience over time. As such, the mere increase or decrease of a coefficient between benefit years of the risk adjustment models is not necessarily indicative of an issue with the model factors or the enrollee-level EDGE data. Because changes in the value of coefficients are highly dependent on the context particular to the benefit years of enrollee-level EDGE data used to recalibrate the models, we do not believe that it is feasible to develop a single definition of “substantial” changes that could be applicable to all types of model factors for all benefit years.
Furthermore, with regard to the request for a State payment transfer simulation reflecting the recalibrated coefficients for the proposed HHS risk adjustment models for the 2027 benefit year, we have historically released State payment transfer simulations only when we are proposing or contemplating major model changes, such as in the case of the 2021 Risk Adjustment Technical Paper,[38]
which we accompanied with such a simulation.[39]
For the recalibration of the 2027 benefit year HHS risk adjustment models, we did not propose and are not finalizing any changes, major or minor, to the structure of the risk adjustment models. The only change we proposed and are finalizing for the 2027 benefit year HHS risk adjustment models is the annual recalibration of the coefficients, which involves equally weighting and blending (averaging) factors from separately solved models using the 2021, 2022, and 2023 benefit years of enrollee-level EDGE data instead of the 2020, 2021, and 2022 benefit years of enrollee-level EDGE data. As there is an overlap of two years of enrollee-level EDGE data between the 2026 and 2027 benefit year HHS risk adjustment models, the coefficients between the two benefit years of HHS risk adjustment models are very similar. In the absence of proposing or finalizing major changes to the models' structure, we do not see a need to publish a State payment transfer simulation and note that issuers, other interested parties, and the public were able to rely upon available information (for example, previous benefit year transfers, the proposed 2027 benefit year HHS risk adjustment model coefficients in the proposed rule (91 FR 6305 through 6321), and the most recently available version of the HHS Developed Risk Adjustment Model Algorithm “Do It Yourself” Software [40]
) to assess the impact of the proposed model recalibration updates.
( printed page 29542)
b. List of Factors To Be Employed in the HHS Risk Adjustment Models (§ 153.320)
The 2027 benefit year HHS risk adjustment model factors resulting from the equally weighted (averaged) blended factors from separately solved models using the 2021, 2022, and 2023 benefit year enrollee-level EDGE data are shown in Tables 1 through 7. The HHS risk adjustment adult, child, and infant models are truncated to account for the high-cost risk pool payment parameters by removing 60 percent of costs above the $1 million threshold.[41]
Table 2 contains factors for each adult model, including the age-sex, HCC, RXC,[42]
RXC-HCC interaction, interacted HCC count, ACF, and enrollment duration coefficients. Table 3 contains the factors for each child model, including the age-sex, HCC, interacted HCC count, and ACF coefficients. Table 4 lists the HCCs selected for the interacted HCC count factors that would apply to the HHS risk adjustment adult and child models. Table 5 contains the factors for each HHS risk adjustment infant model. Tables 6 and 7 contain the HCCs included in the HHS risk adjustment infant models' maturity and severity categories, respectively.
We received several comments requesting additional changes to the HHS risk adjustment models that we did not consider or propose in the proposed rule. We respond to these comments below.
Comment:
A commenter requested that HHS study the impact of calibrating the HHS risk adjustment models separately for the individual and small group markets due to differences in the characteristics of the enrollee population between the two markets.
Response:
We did not propose and are not finalizing separate individual and small group market models. We acknowledge the commenter's request that HHS study the impact of calibrating the HHS risk adjustment models separately for the individual and small group markets. We have reviewed this potential approach and, through our analyses, have identified certain concerns with respect to recalibrating separate models for the individual and small group markets. First, we note that creating two separate risk adjustment models for the individual and small group markets for each of the age groups (adult, child, and infant) would significantly increase the complexity of the HHS-operated risk adjustment program by nearly doubling the number of HHS risk adjustment models.[43]
Furthermore, because both the small group and individual markets are subject to the same AV requirements, the only way to distinguish HHS risk adjustment models for the small group market from those for the individual market would be to separate the enrollee-level EDGE data used for HHS risk adjustment model recalibration into individual market and small group market datasets. Because the small group market is substantially smaller than the individual market,[44]
we have concerns that such a separation of datasets may result in sample size issues for models specific to the small group market, particularly for enrollees with high-cost and rare conditions.
As an alternative to creating separate HHS risk adjustment models for the individual and small group markets, we previously considered [45]
adoption of enrollment duration factors by market. However, we did not find a meaningful distinction in relative costs between markets on average once we implemented the HCC-contingent enrollment duration factors presently included in the adult HHS risk adjustment models. Therefore, we determined it would not be necessary to introduce market-specific factors if HCC-contingent enrollment duration factors were implemented. Even though reasons for and patterns of partial-year enrollment differ by market, we concluded that the patterns most relevant for predicting cost (for example, how enrollment duration relates to costs conditional on the presence of HCCs) were the same for both markets. As such, whether we calibrate separate risk adjustment models or only specific HCCs to reflect individual and small group market-specific enrollment dynamics, we continue to believe that the factors for both markets would generally be very similar, meaning that such a separation would add little value to the models while adding additional complexity and raising sample size concerns in regard to the small group market.
We also note that under the State payment transfer formula, we calculate HHS risk adjustment transfers separately for the individual and small group markets (except for in States with merged markets). As such, HHS risk adjustment transfers largely reflect differences in risk between individual and small group market plans separately, partially mitigating the potential for differences between the individual and small group markets to influence HHS risk adjustment transfers. Nevertheless, we intend to continue to analyze the differences in costs and utilization between the individual and small group markets to consider whether these types of changes would be necessary or appropriate in future benefit years.
Comment:
A few commenters identified certain conditions and treatments that they believe are undercompensated in the risk adjustment models, including Graves' disease/hyperthyroidism and its related treatment Tepezza, autism spectrum disorder, and GLP-1 drugs. These commenters requested that HHS reconsider how these conditions and treatments and their associated costs are accounted for in the HHS risk adjustment models. Some commenters requested that HHS generally consider how to address emerging and expensive therapies such as cellular and gene therapies in the HHS-operated risk adjustment program. Another commenter noted a U.S. Senate
report 46
( printed page 29543)
from the Committee on the Judiciary regarding some issuers' discretionary coding and other gaming mechanisms in the context of Medicare Advantage plans that may impact the transfers calculated in the HHS-operated risk adjustment program if similar behaviors are present in issuers' EDGE server submissions.
Response:
For the request to reconsider how Graves' disease/hyperthyroidism and its related treatment Tepezza and their associated costs are accounted for in the HHS risk adjustment models, we note that we recently discussed the approach to the treatment of Tepezza and Graves' disease/hyperthyroidism in the HHS risk adjustment models in the 2025 Payment Notice (89 FR 26248 through 26249) and 2026 Payment Notice (90 FR 4445 through 4446), explaining that thyroid eye disease (thyrotoxicosis), the condition which Tepezza is approved to treat, is currently categorized in a condition category (Other Endocrine/Metabolic/Nutritional Disorders) that is not a payment HCC in the HHS risk adjustment models. Further, all RXCs in the adult HHS risk adjustment models are associated with a payment HCC. We therefore generally have concerns about adding Tepezza to the HHS risk adjustment models at this time as it is currently not intended to treat or prevent the development of a condition included in a payment HCC. For these reasons, HHS did not propose and is not finalizing any changes for the treatment of Tepezza for thyroid eye disease in the 2027 benefit year HHS risk adjustment models. However, HHS intends to continue analysis of Graves' disease/hyperthyroidism and thyrotoxicosis and the use of Tepezza as more data becomes available and may consider potential changes to the treatment of this condition and drug in the HHS risk adjustment models for future benefit years if appropriate.
Regarding the request to modify how the HHS risk adjustment models account for autism spectrum disorder, GLP-1 drugs, and other emerging and expensive therapies such as cellular and gene therapies, we note that in comments on the 2026 Payment Notice (90 FR 4445), some commenters previously identified that it may be appropriate to address treatments associated with autism spectrum disorder (that is, adaptive behavior services), GLP-1 drugs for weight loss,[47]
and emerging and expensive therapies such as cellular and gene therapies using the ACF framework finalized in that rule. As stated in our response to comments about those conditions and treatments in that final rule, we will take these comments into consideration as we consider potential refinements to the HHS risk adjustment models in future benefit years. Although these treatments may be fair candidates for inclusion in the HHS risk adjustment models in the future, we have identified potential causes for concern with their inclusion. For example, we are concerned that there may be a selection issue in current enrollee-level EDGE data in that issuers may require enrollees to have considerable morbidity to be approved for the GLP-1 medications for weight loss. Thus, we continue to consider the utility of and concerns with adding model factors for GLP-1 drugs and weight loss to the HHS risk adjustment models.
For the underprediction for autism spectrum disorder alleged by commenters and the potential remedy of adding adaptive behavior services for autism spectrum disorder and disorders with similar behavioral characteristics to the HHS risk adjustment models, we note that, unlike obesity/overweight, there is a payment HCC for autism spectrum disorder (HCC 102) presently included as a payment HCC in the HHS risk adjustment models. As such, some reflection of the risk associated with autism spectrum disorder is already included. We continue to explore whether adding a model factor for adaptive behavior services to the HHS risk adjustment models is appropriate. Finally, for emerging and expensive therapies such as cellular and gene therapies, we are limited from incorporating many of these treatments into the HHS risk adjustment models due primarily to inadequate data for developing appropriate model variables. Specifically, many of the gene therapies HHS reviewed while considering this issue were completely absent from the claims data for any enrollee in the currently available benefit years of enrollee-level EDGE data. Of those therapies that did appear, sample sizes were extremely low. Without cost data and sufficient sample size in the enrollee-level EDGE data, we are unable to estimate reliable coefficients for potential model factors associated with these therapies. Nevertheless, we reiterate that many of these drugs will be covered to some extent under the high-cost risk pool, which provides a coinsurance rate of 60 percent when an individual or small group market enrollees' claims exceed $1 million.[48]
If we determine that model changes are necessary in regard to GLP-1 drugs, adaptive behavior services/treatments for autism spectrum disorder, or emerging and expensive therapies such as cellular and gene therapies, we would propose to make such changes through future notice-and-comment rulemaking.
In response to the comments raising discretionary coding and gaming concerns, we note that there are risk adjustment model specifications to mitigate the potential for upcoding. For example, we group subsets of payment HCCs into larger aggregate clusters, or HCC coefficient estimation groups.[49]
In these groups, the HCC estimates are constrained to be equal to each other, and each enrollee is only permitted to be credited with risk from any HCC coefficient estimate group once, regardless of the number of HCCs within the group appearing in their enrollee-level EDGE data. This approach serves multiple purposes, two of which are relevant to the commenters' concern. First, these HCC coefficient estimation groups limit diagnostic upcoding by severity within the HCC hierarchies to which they belong; and, second, they reduce additivity within disease categories (but not across disease categories) to decrease the sensitivity of the model to coding proliferation. Furthermore, as stated in the ten principles of risk adjustment [50]
and other HHS risk adjustment model development papers,[51]
in assessing whether to include specific HCCs in the HHS risk adjustment models, we assess whether HCCs are especially subject to discretionary diagnostic coding or
( printed page 29544)
enhanced rates of diagnosis through population screening not motivated by improved quality of care and, if we determine this to be so, exclude the HCCs from the models. The potential for discretionary coding in the HHS risk adjustment models is an area that HHS is consistently monitoring and addressing as needed and will continue to monitor and address in the future as part of our ongoing efforts to continually improve the HHS risk adjustment models.[52]
As we consider potential refinements to the HHS risk adjustment models in the future, we will also continue to monitor the specific conditions and treatments identified by commenters, along with the structure of related model factors (including those that may be subject to discretionary coding and related gaming concerns), and the impact of recent interacted HCC counts and HCC-contingent enrollment duration model specification updates finalized in the 2023 Payment Notice (87 FR 27224 through 27230). As always, as part of our ongoing efforts to continually improve the precision of the HHS risk adjustment models, if we were to pursue changes to the risk adjustment models in the future, we would seek input from interested parties through notice-and-comment rulemaking or other appropriate vehicles.
Comment:
One commenter requested that HHS disburse and collect risk adjustment transfer payments and charges over a longer period of time rather than in annual lump-sum transfers. The commenter suggested that installment payment arrangements and quarterly provisional calculation of transfers, among other mechanisms, would improve financial predictability for participating issuers, particularly in smaller or emerging markets.
Response:
We did not propose modifying the timeline to collect and pay risk adjustment transfers and are not finalizing any such changes at this time. As discussed in the 2026 Payment Notice (89 FR 82308), unlike Medicare Advantage's risk adjustment program, under which CMS make risk-adjusted monthly payments to Medicare Advantage organizations during the coverage year (in advance of each month of coverage) using interim risk scores and then conducts a reconciliation to update risk scores after the final deadline for submission of all risk adjustment data, the HHS-operated risk adjustment program for the individual, small group, and merged markets uses a final data submission deadline 4 months after the end of the benefit year and calculates issuers' PLRSs and the State payment transfer amounts 2 months after that, resulting in State payment transfers being made 8 to 10 months after the end of the benefit year. HHS typically announces State payment transfer amounts no later than June 30 of the year following the benefit year, begins to collect charges in August of the year following the benefit year, and begins to make payments to issuers in the fall of the year following the applicable benefit year. In the 2026 Payment Notice, we solicited comments on the impact of the existing timeline for collection and disbursement of State payment transfers, including the impact of the “time value of money” on issuers' assessment of actuarial risk and the incentives for adverse selection, and what possible solutions or mitigating steps we should consider to address the impact of the time value of money on the HHS-operated risk adjustment program in future rulemaking. We continue to consider that feedback and will take this comment and those previous comments into consideration for future rulemaking, as applicable.
Comment:
One commenter opposed risk adjustment in general on the basis of a belief that risk adjustment and the assignment of risk scores to enrollees based on health conditions is discriminatory.
Response:
We do not agree that the use of factors based on enrollees' age, sex, and health conditions or utilization of services and treatments in risk adjustment is inappropriate or discriminatory. Consistent with section 1343 of the Affordable Care Act, the HHS-operated risk adjustment program reduces the incentives for issuers to avoid higher-than-average risk enrollees, such as those with chronic conditions, by using charges collected from issuers that attract lower-than-average risk enrollees to provide payments to health insurance issuers that attract higher-than-average risk enrollees. The Affordable Care Act limits issuers' ability to establish or charge premiums on the basis of age and prohibits issuers from doing so on the basis of sex or any individual health characteristic other than tobacco use.[53]
However, the cost of care for and actuarial risk of enrollees is, in part, correlated with their age, sex, health conditions (or severity thereof), and likelihood to utilize services and treatments. As such, without the inclusion of factors related to age, sex, health conditions, and use of services and treatments in the HHS risk adjustment models, some issuers would be incentivized to design plans that are less attractive to potential enrollees whose age-sex category, health conditions, or use of services and treatments is predicted to create a higher liability for the issuer. The various factors in the HHS risk adjustment models help alleviate this incentive by ensuring that the actuarial risk of an issuer's enrollee population in a State market risk pool, including issuers that enroll a higher-than-average proportion of enrollees who fall into a high-cost age-sex category or are likely utilizers of high-cost services, is appropriately assessed as part of the calculations under the State payment transfer formula. The use of factors associated with age, sex, health conditions, and the use of services and treatments in the HHS risk adjustment models is therefore necessary, appropriate, and helps reduce the likelihood that discrimination based on any of these factors will occur for health insurance coverage issued or renewed in the individual and small group (including merged) markets.
Comment:
A commenter stated that the CSR adjustment factors for Massachusetts' ConnectorCare Plan Type 1 and Type 2 are too low. A few other commenters stated concerns regarding footnote 27 in the proposed rule (91 FR 6304), which discussed the State-specific CSR adjustment factors for Arkansas' 94 percent AV Medicaid-expansion plans and Arkansas' 100 percent AV Medicaid-expansion plans. These commenters asserted that the 1.46 CSR adjustment factor—which HHS erroneously described as being applicable to Arkansas 100 percent AV Medicaid-expansion plans in footnote 79 of the 2025 Payment Notice (89 FR 26253)—was in fact more appropriate for these plans than the value we clarified in footnote 27 of the proposed rule (91 FR 6304) as being the correct value for these plans (that is, a CSR adjustment factor of 1.12).[54]
Response:
We worked with the relevant State regulators in Massachusetts and Arkansas to identify the appropriate CSR adjustment factors for their State-specific CSR plan variants. Since Massachusetts
( printed page 29545)
transitioned into the HHS-operated risk adjustment program beginning with the 2017 benefit year, the Massachusetts Health Connector, Massachusetts' Exchange, has consistently supported continued use of the 1.12 factor for their wraparound plans and has not indicated that a change is needed.[55]
Therefore, we do not believe that it is necessary to make changes to Massachusetts' wraparound CSR adjustment plan factor at this time and will continue to apply the 1.12 factor for these plans.
We have similarly worked with the Arkansas Department of Insurance to understand the structure of the funding for Medicaid-expansion plans in Arkansas, using this information to identify what CSR adjustment factors are appropriate for these unique State-specific Medicaid-expansion plans. The CSR adjustment factor of 1.12 will continue to apply for both the 94 percent and 100 percent AV Arkansas Medicaid-expansion plans because these plans are identical in their degree of plan liability to Federal CSR plan variants offered on the Exchange for which the CSR adjustment factor of 1.12 is applied. We will continue to align the CSR adjustment factor for both the 94 and 100 percent Medicaid-expansion plans in Arkansas with the 94 percent silver plan variant CSR adjustment factor for the 2027 benefit year and beyond unless changes occur to the Arkansas program. Furthermore, it would not be appropriate to assign Arkansas's 94 percent or 100 percent AV Medicaid-expansion plans the higher CSR adjustment factor for the AI/AN zero cost sharing (-02 variant) or limited cost sharing CSR plan variant (-03 variant) enrollees because the CSR adjustment factors for AI/AN plans are calibrated to reflect the increased plan liability for enrollees in these specific CSR plan variants in the absence of a Federal appropriation for CSRs. In particular, regardless of plan AV, enrollees in AI/AN CSR plans defined at § 156.420(b)(1) and (2) do not experience cost sharing on any item or service that is an EHB furnished directly by the Indian Health Service, an Indian Tribe, Tribal Organization, or Urban Indian Organization (each as defined in 25 U.S.C. 1603), or through referral under contract health services. This feature and other unique characteristics of AI/AN CSR plans do not apply to the 94 and 100 percent Medicaid-expansion plans in Arkansas.
We therefore do not agree that the current State-specific CSR adjustment factors for Massachusetts' ConnectorCare Plan Type 1 and Type 2 are too low, nor do we agree that Arkansas 100 percent AV Medicaid-wrap plans should receive a CSR adjustment factor of 1.46 instead of the CSR adjustment factor of 1.12 that we have deemed appropriate for these plans. As such, we do not believe any State-specific CSR adjustment factors need further adjustment at this time.
( printed page 29546)
( printed page 29547)
( printed page 29548)
( printed page 29549)
( printed page 29550)
( printed page 29551)
( printed page 29552)
( printed page 29553)
( printed page 29554)
( printed page 29555)
( printed page 29556)
( printed page 29557)
( printed page 29558)
( printed page 29559)
( printed page 29560)
( printed page 29561)
( printed page 29562)
c. Model Performance Statistics
As noted in the 2027 Payment Notice proposed rule (91 FR 6327), each benefit year, to evaluate HHS risk adjustment model performance, we examine each model's R-squared statistic and predictive ratio (PR). The R-squared statistic, which calculates the percentage of individual variation explained by a model, measures the predictive accuracy of the model overall. The PR for each of the HHS risk adjustment models is the ratio of the weighted mean predicted plan liability for the model sample population to the weighted mean actual plan liability for the model sample population. The PR represents how well the model does on average at predicting plan liability for that subpopulation.
A subpopulation that is predicted perfectly would have a PR of 1.0. For each of the final 2027 HHS risk adjustment models, the R-squared statistic and the PRs are in the range of published estimates for concurrent HHS risk adjustment models.[56]
Because we blend the coefficients from separately solved models based on the 2021, 2022, and 2023 benefit years' enrollee-level EDGE data, we are publishing the R-squared statistic for each model separately to assess model performance. The R-squared statistics for the 2027 benefit HHS risk adjustment models are shown in Table 8.
We received public comments on the R-squared statistics for the 2027 benefit year HHS risk adjustment models. We respond to these comments below.
Comment:
A few commenters referred to decreases in the R-squared values in their recommendations for HHS risk adjustment model improvements, to which we have responded elsewhere in this rule. One of these commenters suggested that we not recalibrate the HHS risk adjustment models based on these lower R-squared values.
Response:
We note that the R-squared values for the 2027 benefit year HHS risk adjustment models as applied to the 2021 and 2022 benefit year enrollee-level EDGE data improved relative to the R-squared values for the 2026 benefit year HHS risk adjustment models as applied to these data years.[57]
Furthermore, for the adult models (which apply to the majority of enrollees in the enrollee-level EDGE data), the R-squared values for the 2027 benefit year HHS risk adjustment models as applied to the 2023 benefit year enrollee-level EDGE data are higher than the R-squared values for those models as applied to the 2022 enrollee-level EDGE data. Although we will continue to monitor the R-squared values in the future, the R-squared values for 2027 benefit year risk adjustment model recalibration remain high and within the expected range of R-squared values for the type of model used for the HHS-operated risk adjustment program.[58]
We remain confident the HHS risk adjustment models continue to operate effectively and appropriately predict plan liability for an average enrollee.
3. Overview of the HHS Risk Adjustment Methodology (§ 153.320)
In part 2 of the 2022 Payment Notice (86 FR 24183 through 24186), we finalized the proposal to continue to use the State payment transfer formula finalized in the 2021 Payment Notice for the 2022 benefit year and beyond, unless changed through notice-and-comment rulemaking. We did not propose changes to the formula in the 2027 Payment Notice proposed rule (91 FR 6327). We therefore will continue to apply the formula as finalized in the 2021 Payment Notice (86 FR 24183 through 24186) in the States where HHS operates the risk adjustment program in the 2027 benefit year.
Additionally, as finalized in the 2020 Payment Notice (84 FR 17466 through 17468), we will maintain the high-cost risk pool parameters for the 2020 benefit year and beyond, unless amended
( printed page 29563)
through notice-and-comment rulemaking. We did not propose changes to the high-cost risk pool parameters for the 2027 benefit year; therefore, we will maintain the $1 million threshold and 60 percent coinsurance rate.[59]
However, we received comments on the high-cost risk pool parameters and are responding to these comments below.
Comment:
One commenter requested that HHS consider updating the high-cost risk pool parameters to account for inflation to appropriately reflect the evolving distribution of very high-cost claims that fall above the $1 million threshold (“attachment point”) of the high-cost risk pool, which would have the effect of also updating the plan liability for these claims in recalibration for calculating risk scores and HHS risk adjustment transfers.
Response:
We did not propose and are not finalizing changes to the high-cost risk pool parameters for the 2027 benefit year.
The high-cost risk pool is a budget neutral aspect of the HHS-operated risk adjustment program in which payments are funded by a percent of premium charge on all risk adjustment covered plans within the respective national high-cost risk pool (one for the individual market and merged market plans, including catastrophic and non-catastrophic plans, and another for the small group market). In the 2018 Payment Notice (81 FR 94082), we estimated that the percentage of premium charge, which funds high-cost risk pool payments, would most likely not exceed 0.5 percent. When aggregating across the national risk pool markets, this statement has held true. For example, for the 2024 benefit year, the individual market high-cost risk pool charge as a percent of premium was 0.39 percent [60]
and the small group market high-cost risk pool charge as a percent of premium was 0.58 percent.[61]
Aggregated across both the individual and small group markets, the overall high-cost risk pool charge was 0.45 percent of premium. This consistently low percentage of premium charges prevents States and issuers with high-cost enrollees from bearing a disproportionate amount of unpredictable risk. Additionally, we believe that retaining the same parameters for the high-cost risk pool year-over-year promotes stability and predictability in our markets, and we have concerns that indexing the $1 million threshold for inflation would annually vary those parameters.
With these considerations, we continue to believe a $1 million threshold and 60 percent coinsurance rate are appropriate to incentivize issuers to control costs while improving risk prediction under the HHS risk adjustment models. However, we continue to monitor the high-cost risk pool parameters to consider whether adjustments are needed and would propose such changes for future benefit years through notice-and-comment rulemaking if necessary. Comment Solicitation on Retaining Separate Risk Adjustment Transfer Calculations for Individual Catastrophic Plans and Individual Non-Catastrophic Plans under the State Payment Transfer Formula.
In the 2027 Payment Notice proposed rule (91 FR 6327), we solicited comment on whether we should retain separate risk adjustment transfer calculations under the State payment transfer formula for individual catastrophic plans and individual non-catastrophic plans or whether we should calculate State transfers for these plans together in light of the September 4, 2025 guidance entitled “
Guidance on Hardship Exemptions for Individuals Ineligible for Advance Payment of the Premium Tax Credit or Cost-sharing Reductions Due to Income, and Streamlining Exemption Pathways to Coverage.
” [62]
This guidance expanded upon prior FFE hardship exemption policy by expanding eligibility for catastrophic plans starting with PY 2026.[63]
In the 2027 Payment Notice proposed rule (91 FR 6327), we sought comment on the impact of this policy on the HHS-operated risk adjustment program. We will take these comments into consideration as applicable.
4. Risk Adjustment Data Validation Requirements When HHS Operates Risk Adjustment (HHS-RADV) (§§ 153.350 and 153.630)
HHS conducts HHS-RADV under §§ 153.350 and 153.630 in any State where HHS is operating risk adjustment on the State's behalf.[64]
The purpose of HHS-RADV is to ensure issuers are providing accurate high-quality information to HHS, which is crucial for the proper functioning of the HHS-operated risk adjustment program. HHS-RADV also ensures that risk adjustment transfers reflect verifiable actuarial risk differences among issuers, rather than risk score calculations that are based on poor quality data, thereby helping to ensure that the HHS-operated risk adjustment program assesses charges to issuers with plans with lower-than-average actuarial risk while making payments to issuers with plans with higher-than-average actuarial risk. HHS-RADV consists of an initial validation audit (IVA) and a second validation audit (SVA). Under § 153.630, each issuer of a risk adjustment covered plan must engage an independent IVA entity. The issuer provides demographic, enrollment, and medical record documentation for a sample of enrollees selected by HHS to its IVA entity for data validation. Each issuer's IVA is followed by an SVA, which is conducted by an entity HHS retains to verify the accuracy of the findings of the IVA. Based on the findings from the IVA, or SVA (as applicable), HHS conducts error estimation to calculate an HHS-RADV error rate. The HHS-RADV error rate is then applied to adjust the PLRSs of outlier issuers, as well as the risk adjustment transfers calculated under the State payment transfer formula for the applicable State market risk pools, for the benefit year being audited.
a. HHS-RADV Error Estimation Modification To Incorporate IVA Sampling Changes
In the 2027 Payment Notice proposed rule (91 FR 6327), we proposed to modify one intermediate step of the HHS-RADV error estimation methodology starting with 2025 benefit year HHS-RADV. In the 2026 Payment Notice (90 FR 4449 through 4452), we finalized excluding enrollees without
( printed page 29564)
HCCs from IVA sampling beginning with 2025 benefit year HHS-RADV. We noted that this policy will impact the steps in the error estimation methodology during which HCC-associated error rates are applied to adjust issuers' PLRSs, and stated our intent to seek comments on potential modifications to the intermediate steps in the error estimation methodology to ensure that HCC-associated error rates continue to apply to only the proportion of total PLRSs that are associated with HCC-components of EDGE risk scores. As such, we proposed to add an additional scaling factor,
ai, to the error estimation methodology to address this and capture the proportion of an issuer's total risk for the entire population that is associated with enrollees with HCCs. This scaling factor would be added to the final steps of error estimation in which HCC-associated error rates are applied to adjust issuers' PLRSs, and therefore, its addition would not impact the majority of the error estimation methodology, including the calculation of group failure rates, enrollee-level adjustments, or HCC-associated error rates.
The formula for the existing scaling factor
HccPLRSweighti
is the sum of sampled enrollees' stratum-weighted adjusted HCC-associated portion of EDGE risk scores divided by the sum of sampled enrollees' stratum-weighted total EDGE risk score. Because this formula is based on the issuer's sample, it depends on having enrollees with and without HCCs in the audit sample to appropriately estimate the proportion of the issuer's total PLRS that is HCC-related. However, as explained in the 2026 Payment Notice (90 FR 4452), when enrollees without HCCs are excluded from issuers' audit samples beginning with 2025 benefit year HHS-RADV, this formula will only estimate the proportion of enrollees' total EDGE risk scores that is HCC-related for the issuer's population of enrollees with HCCs.[65]
Therefore, as noted in the 2027 Payment Notice proposed rule (91 FR 6327), we proposed to create another scaling factor beginning with benefit year 2025 HHS-RADV that estimates the proportion of the issuer's total PLRS that is associated with enrollees with HCCs using the issuer's EDGE data. Together, these two scaling factors would capture the proportion of the issuer's total PLRS that is HCC-related.
Therefore, we proposed to introduce an additional scaling factor,
ai, as follows:
Where:
meanRiskScorei,h
is the average risk score for all enrollees in stratum
h
in issuer
i'
s EDGE population; and
strBMMi,h
is the total stratum billable member months (BMM) for all enrollees in stratum
h
in issuer
i'
s EDGE population.
We proposed to apply the scaling factor
ai
to the intermediate steps in the error estimation methodology as follows:
TotalERi
=
HccERi
*
HccPLRSWeighti
*
ai
The numerator in the formula for the scaling factor
ai
sums the product of each stratum's mean risk score and total BMM for strata 1 through 9, thereby creating an aggregate risk score for all enrollees with EDGE HCCs in an issuer's EDGE population.[66]
The denominator sums the product of each stratum's mean risk score and total BMM for strata 1 through 10. This includes all enrollees in the issuer's EDGE population including enrollees without HCCs, and thereby creates an aggregate risk score for the issuer.[67]
Overall, the scaling factor
ai
estimates the proportion of the issuer's total PLRS that is associated with enrollees with HCCs and, by combining it with the HCC PLRS weighting factor, we could continue to estimate the proportion of the issuer's total PLRS that is HCC-related after the removal of no-HCC enrollees from the IVA sample beginning with 2025 benefit year HHS-RADV. After leveraging EDGE data from the relevant benefit year to calculate the scaling factor
ai
and the total error rate
TotalERi, we would continue to adjust issuers' PLRSs using the following formula:
AdjPLRSi
= (1−
TotalERi) *
PLRSi
Without adding this additional scaling factor to the error estimation methodology beginning with 2025 benefit year HHS-RADV, the error rate would adjust elements of issuers' total PLRSs that are associated with enrollees without HCCs and are not intended to be adjusted during error estimation.[68]
We believe these adjustments would be inappropriate, and moreover, could result in double adjustments for any identified data errors of non-HCC components, such as demographic and enrollment factors, that are adjusted through separate processes.[69]
Therefore, starting with the 2025 benefit year of HHS-RADV, we proposed to add an additional scaling factor,
ai, to the error estimation methodology to ensure that HCC-associated error rates continue to apply to only the proportion of total PLRSs that are associated with HCC-components of EDGE risk scores.
We sought comments on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed addition of a scaling factor to the HHS-RADV error estimation methodology below.
Comment:
Several commenters supported the addition of the proposed scaling factor for HHS-RADV. Several of these commenters noted that the addition of the scaling factor would more accurately reflect risk and capture the proportion of risk associated with enrollees with HCCs. One commenter
( printed page 29565)
noted that this would better align the error rate calculation used with the basis of that calculation. One commenter noted that this proposal strengthens program integrity while maintaining the intent of HHS-RADV to target errors in the calculations of HCC-related risk.
Response:
We agree with the commenters that this proposal would more precisely capture the risk associated with enrollees with HCCs, better align the error rate calculation with the basis of that calculation, and strengthen program integrity. Specifically, without adding this additional scaling factor to the error estimation methodology beginning with 2025 benefit year HHS-RADV, the error rate would adjust elements of issuers' total PLRSs that are associated with enrollees without HCCs and are not intended to be adjusted as part of this calculation.[70]
We believe these adjustments that would result from the absence of the scaling factor would be inappropriate, and moreover, could result in double adjustments for any identified data errors of non-HCC components, such as demographic and enrollment factors, that are adjusted through separate processes.[71]
Therefore, starting with the 2025 benefit year of HHS-RADV, we are finalizing the incorporation of an additional scaling factor,
ai, into the error estimation methodology to ensure that HCC-associated error rates continue to apply to only the proportion of total PLRSs that are associated with HCC components of EDGE risk scores, as proposed.
Comment:
A commenter suggested that HHS should provide clear operational details regarding application of this scaling factor to help reduce avoidable uncertainty affecting premium development and issuer participation, and noted that a predictable HHS-RADV process is critical for market stability.
Response:
We agree that a stable and predictable HHS-RADV process plays an important role in market stability and that the inclusion of this scaling factor in the error estimation methodology is appropriate to more precisely account for the relevant part of an issuer's population in the calculation of HHS-RADV error rates. We intend to update the HHS-RADV Protocols to reflect the adoption of the new additional scaling factor.[72]
We also provided analysis in the proposed rule (91 FR 6444) on the estimated impact of the proposed policy. Specifically, in the Regulatory Impact Analysis of the proposed rule, we simulated the impact of the additional scaling factor and found that HHS-RADV adjustments to risk adjustment State transfers decreased in magnitude by 11.7 percent in the individual non-catastrophic market (going from $148 million to $139 million) and by 13.8 percent in the small group market (from $81 million to $69.8 million). Because the HHS-operated risk adjustment program, including HHS-RADV adjustments to State transfers, is budget neutral, we would see the same impact on negative risk adjustment State transfers (in other words, risk adjustment charges) and HHS-RADV adjustments, in that both would decrease in magnitude. When examining the impact of the additional scaling factor on HHS-RADV adjustments over premium, our analysis found that there was only a 0.01 percent change in positive HHS-RADV adjustments in both markets when comparing results without the additional scaling factor with results reflecting the adoption of the additional scaling factor. This corresponds with a percentage point (PP) change of −0.02. Because our simulation showed a decrease in premium impact in both the individual non-catastrophic and small group markets, we do not believe that this scaling factor will create uncertainty in premium development and impact issuer participation in the HHS-operated risk adjustment and HHS-RADV programs.
5. HHS Risk Adjustment User Fee for the 2027 Benefit Year (§ 153.610(f))
As noted in the 2027 Payment Notice proposed rule (91 FR 6327), we proposed an HHS risk adjustment user fee for the 2027 benefit year of $0.20 per member per month (PMPM). Under § 153.310, if a State is not approved to operate, or chooses to forgo operating, its own risk adjustment program, HHS will operate risk adjustment on its behalf. For the 2027 benefit year, HHS will operate risk adjustment in every State and the District of Columbia. As described in the 2014 Payment Notice (78 FR 15416 through 15417), HHS' operation of the risk adjustment program on behalf of States is funded through a risk adjustment user fee. Section 153.610(f)(2) provides that, where HHS operates a risk adjustment program on behalf of a State, an issuer of a risk adjustment covered plan must remit a user fee to HHS equal to the product of its monthly billable member enrollment in the plan and the PMPM risk adjustment user fee specified in the annual HHS notice of benefit and payment parameters for the applicable benefit year.
OMB Circular No. A-25 established Federal policy regarding user fees, and specifies that a user charge will be assessed against each identifiable recipient for special benefits derived from Federal activities beyond those received by the general public.[73]
The HHS-operated risk adjustment program provides special benefits as defined in section 6(a)(1)(B) of OMB Circular No. A-25 to issuers of risk adjustment covered plans, because it mitigates the financial instability associate with potential adverse risk selection.[74]
The HHS-operated risk adjustment program also contributes to consumer confidence in the health insurance industry by helping to stabilize premiums across the individual, merged, and small group markets.
For the 2027 benefit year, HHS proposed to calculate the Federal administrative expenses of operating the HHS risk adjustment program. This calculation resulted in a risk adjustment user fee rate of $0.20 PMPM based on our estimated costs for HHS risk adjustment operations and estimated billable member months (BMM) for individuals enrolled in risk adjustment covered plans. As noted in the 2027 Payment Notice proposed rule (91 FR 6324), these costs cover development of the models and methodology, collections, payments, account management, data collection, data validation, program integrity and audit functions, operational analytics, interested parties training, operational support, and administrative and personnel costs dedicated to HHS-operated risk adjustment program activities. To calculate the risk adjustment user fee, we divided HHS' projected total costs for administering the program on behalf of States by the expected number of BMM in risk adjustment covered plans in States where the HHS-operated risk
( printed page 29566)
adjustment program will apply in the 2027 benefit year.
We estimated that the total cost for HHS to operate the risk adjustment program on behalf of all States and the District of Columbia for the 2027 benefit year would be slightly more than $65 million, which is similar to the 2026 benefit year budget.[75]
Similar to prior benefit years, we projected risk adjustment enrollment scenarios for the 2027 benefit year. Based on our estimates, for the 2027 benefit year, we noted that we do not expect enrollment changes to significantly impact collections under this user fee rate.
We stated in the 2027 Payment Notice proposed rule (91 FR 6327) that our intention was to reconsider the enrollment estimates for this final rule. If these newer enrollment estimates are too low in comparison to our proposed user fee estimates, we noted that the final user fee may be higher. We also noted that if these enrollment estimates are higher in comparison to our proposed user fee estimates, the final user fee may be lower. In addition, we noted that if any events result in a deviation from our expectations of current conditions that would significantly change our estimates around costs, enrollment projections, or the finalization of proposed risk adjustment policies between the proposed rule and this final rule, we may modify the proposed HHS risk adjustment user fee rate in the final rule. Because we projected a similar budget to operate the HHS-operated risk adjustment program for the 2027 benefit year as for the 2026 benefit year, we proposed an HHS risk adjustment user fee of $0.20 PMPM for the 2027 benefit year. We sought comment on the proposed HHS risk adjustment user fee rate of $0.20 PMPM for the 2027 benefit year.
As in all years, we consider updated information regarding estimates of costs, enrollment projections, and finalization of risk adjustment policies between the proposed rule and the final rule to determine the final risk adjustment user fee rate. Specifically, between the proposed and final rules, we updated our enrollment projections based on the availability of interim 2025 risk adjustment data, and our projections in enrollment in the off-Exchange individual and small group markets are higher than the estimates that we used for proposed rule.
Because some of our enrollment estimates were higher than previously anticipated, and the costs for the HHS-operated risk adjustment program for the 2027 benefit year have not changed, the PMPM cost of the HHS-operated risk adjustment program for the 2027 benefit year is lower than the proposed HHS risk adjustment user fee rate.
After consideration of comments and our additional data analyses between the proposed and final rules, and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing an HHS risk adjustment user fee rate for the 2027 benefit year of $0.18 PMPM. We summarize and respond to public comments received on the 2027 HHS risk adjustment user fee rate below.
Comment:
Several commenters stated support for maintaining the proposed HHS risk adjustment user fee rate of $0.20 PMPM for the 2027 benefit year.
Response:
We believe that when costs, risk adjustment policies, and projections of enrollment in the HHS-operated risk adjustment program are constant, the HHS risk adjustment user fee rate should remain constant. However, based on more recently available data, we are finalizing an HHS risk adjustment user fee rate for the 2027 benefit year of $0.18 PMPM.
Comment:
Some commenters requested that HHS consider the pricing impacts of the HHS risk adjustment user fee rate.
Response:
We note that we must set the HHS risk adjustment user fee for a given benefit year to secure adequate funding for the HHS-operated risk adjustment program. We are finalizing an HHS risk adjustment user fee rate for the 2027 benefit year of $0.18 PMPM, which is lower than the rate for the 2026 benefit year. We anticipate that the overall impact on pricing of an $0.18 PMPM HHS risk adjustment user fee rate will be minimal, since it is lower than the user fee rate for the 2026 benefit year and because $0.18 PMPM is a very small percent of overall premium.
C. Part 154—Health Insurance Issuer Rate Increases: Disclosure and Review Requirements
1. Submission of Rate Filing Justification (§ 154.215)
a. CSR Reimbursement
Section 1402 of the Affordable Care Act requires issuers to provide cost-sharing reductions (CSRs) to increase the actuarial value of coverage for consumers with incomes between 100 and 250 percent of Federal Poverty Level (FPL) who enroll in silver-level QHPs in the individual market, as well as eligible American Indian/Alaska Native consumers who enroll in QHPs at any metal level. Section 1402 of the Affordable Care Act also states that HHS will reimburse issuers for the cost of providing CSRs to eligible enrollees but does not include a valid appropriation to make such payments.[76]
On October 11, 2017, the Attorney General of the United States provided a legal opinion stating that HHS and the Department of the Treasury could no longer use the permanent appropriation at 31 U.S.C. 1324 to fund CSR reimbursements to issuers. In accordance with that opinion, HHS directed CMS to discontinue CSR reimbursements to issuers until Congress provides an appropriation.[77]
In response to the termination of CSR reimbursement, State Departments of Insurance allowed or instructed issuers to increase (or “load”) premiums either primarily, or only, on silver-level QHPs to offset the issuers' cost of providing CSRs.[78]
There are several ways that issuers have determined the CSR load factor. For example, issuers have loaded silver plans offered on-Exchange to recover expected lost CSRs based on experience, they have loaded silver plans on-Exchange based on an assumed distribution of enrollment and enrollee utilization (sometimes a set amount mandated by the State), or they have loaded all plans at all metal levels by the same amount to spread lost CSRs across the entire individual market (broad loading). These differing approaches may result in loads that produce additional revenue collected from the applied CSR load that exceeds the amount of unreimbursed CSRs by assuming an enrollment and claims distribution that significantly diverges from what actually occurs. Based on our review of actuarial memoranda submitted by issuers for PY 2026, HHS believes these excessive loads on silver plans in particular (and in some cases as mandated by State law) lead to inflated premiums for silver plans, further distort pricing for bronze and
( printed page 29567)
gold plans relative to silver plans, limit consumer choice, and significantly increase the cost of the second lowest-cost silver plan available to a consumer, which in turn increases PTC amounts and Federal expenditures.
b. Rate Filing Justifications Regarding CSRs
Section 2794 of the PHS Act directs the Secretary, in conjunction with the States, to establish a process for the annual review of premium increases for health coverage prior to the implementation of the increase. HHS has historically interpreted this requirement for premiums as referring to the underlying rates that are used to develop premiums. Section 154.215 requires issuers to submit rate filing justifications to CMS and the applicable State (76 FR 29964, 29969).
Under § 154.215(b)(1) through (3), the rate filing justification has three parts. The Unified Rate Review Template (URRT) (Part I of the rate filing justification) is required for all single risk pool products, including new products. It is intended to capture information needed to monitor premium increases of health insurance coverage offered through and outside the Exchanges in the individual and small group markets and ensure compliance with the single risk pool methodology, including allowable market level index rate adjustments to reflect risk adjustment payments and charges, and other Federal rating requirements.[79]
Part II of the rate filing justification is the Written Description Justifying the Rate Increase (Consumer Justification Narrative). Part II is required only for rate increases in single risk pool products that are subject to review (that is, a plan within the product that has a rate increase of 15 percent or greater or a State-specific threshold). Part II is a consumer-friendly narrative that provides the justification for the rate increase, describes the relevant Part I data, the assumptions used to develop the rate increase, and an explanation of the most significant factors causing the rate increase.[80]
An actuarial memorandum (Part III of the rate filing justification) is required for any rate increase in a single risk pool plan. It is also required for any rate filing containing QHPs or whenever a State requires it to be submitted. Further, an actuarial memorandum is required for all plans in States that do not have an Effective Rate Review Program and for which CMS is responsible for reviewing the rate filing.[81]
The Part III actuarial memorandum includes the actuarial reasoning and assumptions, justifications, and methodologies that support the entries in the URRT.[82]
The actuarial memorandum must also capture appropriate actuarial certifications related to the development of the index rate in accordance with Federal regulations, and the development of plan specific premium rates using allowable modifiers to the index rate.[83]
The issuer is required to provide an explanation of how these modifiers are developed and applied to the market-wide adjusted index rate to derive the plan-adjusted index rate.
In a Bulletin issued on May 2, 2025 (PY26 Rate Filing Guidance),[84]
we instructed issuers that make permitted plan-level adjustments to account for CSR amounts provided to eligible enrollees for which the issuer does not otherwise receive reimbursement [85]
(that is, issuers that load premiums) to specify the actual CSRs the issuers paid for PY 2024 in the actuarial memorandum submitted with their PY 2026 rate filing. Issuers report plan-level adjustments when they submit a rate filing justification to the State or CMS for review. States or CMS review those rate filing justifications to ensure compliance with the Federal rating rules, including 45 CFR 156.80.[86]
Specifically, through the PY26 Rate Filing Guidance, and under our authority under § 154.215(a)(2) and (3), we directed issuers that loaded for unreimbursed CSRs to: (1) specify the actual CSRs the issuer paid on behalf of enrollees for PY 2024 (in dollars); (2) specify the CSR load factor for PY 2026 and explain how it was determined; and (3) explain how the additional revenue to be collected from the applied CSR load compares to the expected amount of CSRs that will be provided to enrollees in PY 2026.
Following issuance of the PY26 Rate Filing Guidance, CMS issued additional guidance entitled, “Frequently Asked Questions on Plan Year 2026 Individual Market Rate Filing Instructions,” on May 27, 2025.[87]
We noted that if an issuer was not able to calculate the precise amount of actual CSRs paid for enrollees for PY 2024 by the applicable rate filing deadline, CMS would accept an estimate developed using a reasonable methodology that enables it to estimate the value of CSRs provided for PY 2024 as accurately as possible, detailed in the actuarial memorandum submitted with the PY 2026 rate filing justification.[88]
As noted in the 2027 Payment Notice proposed rule (91 FR 6327), starting with rate filings for the 2027 plan year, we proposed to continue to require issuers that load premiums to submit certain information as specified in the PY26 Rate Filing Guidance in their URRTs and actuarial memoranda for each plan year in which CSRs are not funded. Specifically, in the URRT for the upcoming plan year, issuers would report actual CSR amounts paid on behalf of enrollees and the additional revenue collected from the previously applied CSR load using the most recent annual data that is available prior to the applicable filing year, using the standard methodology set forth in § 156.430(c)(2). In most cases, the most recent annual CSR data would reflect the plan year that is two years before the upcoming plan year (for example, CSRs paid for eligible enrollees and the additional revenue collected from the CSR load applied in PY 2025 would be reported during the 2026 filing year for PY 2027 rate filings).
( printed page 29568)
As described by the Secretary in applicable guidance,[89]
under the CMS standard methodology, issuers re-adjudicate the actual complete set of claims incurred by an enrollee in the cost-sharing reduction plan variation as if they had been enrolled in the associated standard plan to determine the difference the enrollee would have paid in deductibles, copayments, coinsurance, and other out-of-pocket expenses for EHBs (other than premiums and balance billing). The difference equals the amount of CSRs provided by the issuer.[90]
As stated in the 2016 Payment Notice, we believe that the standard methodology is the most accurate method for calculating the actual value of CSRs that the issuer has provided on behalf of enrollees in a plan year.[91]
Additionally, we believe that most issuers are familiar with that methodology, which was required to calculate CSRs paid on behalf of enrollees for the 2017 plan year, the most recent year in which CMS provided advance CSR payments to issuers.
We note that although CMS proposed that issuers use the standard methodology to calculate CSR amounts paid on behalf of enrollees and to submit an aggregate amount of CSRs provided at the plan level on the URRT, this data submission would not require issuers to use the CSR reconciliation process implemented by CMS, as described in § 156.430(c)(2). We believe this proposal would result in a lower burden on issuers as compared to the burden that would be associated with submitting policy-level CSR data to CMS through the CSR reconciliation process. Submission of policy-level CSR data would require direct electronic submissions of data that must conform to our business rules, data element validations, and required file formats. When HHS previously collected such data, it resulted in issuers attempting submissions multiple times before the submission could be accepted by the system. The proposed process will leverage the existing URRT submission process and be much less burdensome.
We also proposed that issuers would include in the URRT the applicable CSR load factor for each plan that would be applied to the market adjusted index rate to calculate the calibrated plan adjusted index rate for the upcoming plan year. We proposed to collect the CSR load factor, if any, to fulfill our responsibility to ensure compliance with § 156.80(d), which requires all permitted plan-level adjustments to be “actuarially justified.” In addition, we proposed that issuers would include in the actuarial memorandum an explanation of the methodology used to determine the load factor. We proposed that issuers would also include in the URRT the additional revenue expected to be collected from the applied CSR load factor and the expected amount of CSRs that will be paid for enrollees for the upcoming plan year. We also proposed that issuers would include in the actuarial memorandum an explanation comparing these amounts. This explanation would allow the State or CMS, as applicable, to determine whether the load factor is actuarially justified and not excessive in relation to the amount expected to be paid for unreimbursed CSRs.
In the 2026 Payment Notice, we stated our expectation that CSR loading practices, to the extent permitted by State regulators, are intended to account for unpaid CSRs. We also noted that, while there is no requirement that a State permit CSR loading, in States that have an Effective Rate Review Program, the State has the responsibility to determine whether an issuer's adjustments to the market-wide index rate for plan-specific factors (including accounting for CSR amounts) are actuarially justified.[92]
We further proposed that an actuarially justified CSR load factor is one that is calibrated on actual experience and that only accounts for the projected revenue loss of unreimbursed CSR payments without materially exceeding that amount. As such, collecting through the URRT and actuarial memoranda information on paid CSRs, additional revenue collected from the previously applied CSR load, CSRs expected to be paid, the CSR load factor and expected resultant additional revenue for the upcoming plan year, the underlying methodology for determining the CSR load factor that would be applied for the upcoming plan year, and an explanation of how the expected additional revenue compares to the amount of CSRs expected to be paid, will benefit State regulators (and CMS in States where CMS functions as the primary reviewer of rates) by providing regulators the data necessary to determine whether CSR load amounts are actuarially justified plan-level adjustments to the index rate under § 156.80.
While we recognize the additional burden on issuers to provide this information, given the significant impact of CSR loading on Federal expenditures through additional premium tax credit (PTC) spending, we believe collection of this information is an important program integrity measure that will help ensure that CSR loads are appropriate to recover lost CSR payments and are not inappropriately inflating Federal expenditures or undermining Federal rating rules.
Therefore, we proposed to collect information on adjustments to the index rate to account for unreimbursed CSRs as described above. We did not propose changes to any regulation text as the collection of these data is already captured under § 154.215(d)(1), which states that historical and projected claims experience must be included in the URRT. Additionally, § 156.80(d)(2)(i) states that plan-level adjustments to account for unreimbursed CSR payments provided to eligible enrollees are permissible only if actuarially justified and permitted by the applicable State authority. We requested comment on all aspects of our proposal to require issuers that intend to load premium rates to account for unpaid CSRs for the upcoming plan year to submit this information in their URRTs and the actuarial memoranda for each plan year in which CSRs are not funded, beginning with PY 2027 rate filings.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. As we stated in the proposed rule, we intend to release guidance on the submission of the required URRT and actuarial memoranda information as part of revised Unified Rate Review Instructions, as we have historically provided detailed guidance to issuers on how to complete each field of the URRT and satisfy the criteria for the actuarial memorandum in the Unified Rate Review Instructions.[93]
We summarize and respond to public comments received on the proposed policy below.
Comment:
A few commenters supported the proposed CSR data collection, stating that they are in favor of increased transparency and
( printed page 29569)
standardized reporting to better understand CSR loading practices and ensure CSR loads align with actual costs. Many other commenters expressed concern that the proposed CSR data reporting requirements would impose significant operational and financial burdens on issuers and may lead to higher premiums.
Response:
We acknowledge that issuers will incur operational and financial burdens as a result of these reporting requirements. However, collection of this information is an important program integrity measure that will help ensure that CSR loads are appropriate to recover lost CSR payments and are not inappropriately inflating Federal expenditures, excessively increasing silver plan premiums paid by unsubsidized enrollees, or undermining Federal rating rules. This information will also benefit State regulators by providing necessary data to determine if their issuers' CSR load amounts are actuarially justified plan-level adjustments to the index rate under § 156.80. We also note that when this information was previously collected through the policy-level electronic data collection process in place for determining the actual amount of CSRs provided under § 156.430, that process imposed additional burden on issuers associated with submitting multiple electronic files through that data collection process. Collecting this CSR information through the URRT will minimize the burden on issuers.
Comment:
Many State insurance departments and Exchanges stressed the importance of preserving State-directed CSR loading methodologies and rate review processes. They opposed Federal standardization that might override State-specific actuarial soundness standards or impose a single CSR loading methodology. Moreover, some commenters stated that CSR load data may vary significantly by State and issuer, making direct comparisons misleading without proper context. They suggested that, to avoid misinterpretation, detailed discussions of CSR load data should be included in actuarial memoranda rather than in standardized templates.
Response:
We agree with commenters that the actuarial memorandum, not the URRT, is the appropriate place to include detailed discussions of CSR load data. We clarify that we are not finalizing a single CSR loading methodology at this time. As stated in the proposed rule, the plan-level adjustments that result from CSR loading must be actuarially justified and calibrated on actual market experience that accounts only for the projected revenue loss of unreimbursed CSR payments without materially exceeding that amount.[94]
CSR loading is meant to recover lost CSR reimbursement and should not be seen as a premium adjustment factor to achieve a desired premium subsidy level. Specifically, silver-plan premiums should not be loaded in a way that purposefully collects more in premium than the expected amount of unreimbursed CSRs to increase subsidy amounts and lower premiums at other metal levels. This practice goes beyond CSR loading and is an inappropriate use of the CSR load factor. We are finalizing this description of actuarially justified plan-specific adjustment factors as proposed.
States with an Effective Rate Review Program are responsible for reviewing proposed rate increases subject to review to determine whether those increases are unreasonable by, in part, examining the reasonableness of the assumptions used by the health insurance issuer to develop the proposed rate increase and the validity of the historical data underlying the assumptions.[95]
Such States are also responsible for reviewing all proposed rate changes for compliance with Federal rating rules. This includes determining whether an issuer's adjustments to the market-wide index rate for plan-specific factors (including accounting for unreimbursed CSR amounts) are actuarially justified and compliant with the single risk pool regulations at § 156.80.
A loading practice that results in additional premium that materially exceeds what is projected to account for the impact of unreimbursed CSRs does not appropriately account for CSRs provided to eligible enrollees as required for permitted plan-specific adjustments to the index rate under § 156.80(d)(2)(i).[96]
As such, in States without an Effective Rate Review Program, CMS may exercise its authority in § 154.205(b) to determine a rate increase is unreasonable if such increase includes a CSR load that was developed based on a methodology that does not reasonably account for the projected amount of unpaid CSRs. In accordance with section 1311(e)(2) of the Affordable Care Act and § 155.1020, CMS may also recommend that the Exchange not make available through the Exchange plans with such an unreasonable rate increase based on patterns or practices of excessive or unjustified premium increases. In evaluating whether a State has an Effective Rate Review Program, as defined in § 154.301, CMS will similarly evaluate whether the State rate review process adheres to the requirements set forth in § 154.301(a)(3) for issuers' assumptions about the premium increases that are necessary to account for unreimbursed CSRs. We do not believe the requirement to submit additional information regarding how unreimbursed CSRs are accounted for within the plan-level adjustments to the index rate interferes with State-directed CSR loading methodologies or rate review processes where these processes comply with the requirements under § 154.301.
We intend to review the submitted CSR data. If issuers provide a State with proposed rate increases which include a CSR load that does not appear to be developed based on a methodology that reasonably accounts for the amount of unpaid CSRs and the State does not deem such rate increases as “unreasonable,” CMS may use its authority under § 154.301(d) to evaluate whether the State has ceased to satisfy the criteria set forth § 154.301(a) and (b) and no longer has an Effective Rate Review Program.
The regulations at § 155.1000 provide Exchanges with broad discretion to certify QHPs that otherwise meet the QHP certification standards specified in Part 156 and afford Exchanges discretion to deny certification of QHPs that meet minimum QHP certification standards, but are nonetheless not in the interest of qualified individuals. As stated earlier in this preamble and in the proposed rule, CSR loading practices that result in QHP premium adjustments that materially exceed the projected revenue loss from unreimbursed CSR payments, or excessively load plans at the silver metal tier beyond expected unreimbursed CSR payments to lower premiums for other metal tiers, do not align with requirements for actuarially justified plan-level adjustments to the index rate permitted under § 156.80(d). Such loading practices can result in significantly higher premiums that harm unsubsidized consumers enrolled in Exchange plans. Accordingly, CMS may determine that denial of an issuer's request for certification on the FFE is warranted if an issuer engages in CSR loading practices that result in premiums that are significantly higher than would reasonably be expected
( printed page 29570)
when accounting for the amount of unreimbursed CSRs in violation of § 156.80(d).
Comment:
Some commenters indicated that changes in CSR loading and premium adjustments could cause shifts in enrollment, raising concerns about market stability. A few commenters noted that such shifts in enrollment could negatively affect American Indian/Alaska Native populations and Tribal health programs reliant on stable silver plan pricing.
Response:
As some commenters stated, when CSR costs are embedded into silver premiums, benchmark premiums rise and Federal PTC spending increases—contributing to fully subsidized bronze and gold plans and leading to unsubsidized enrollees paying higher silver plan premiums. Therefore, it is imperative that regulators ensure that issuers are setting CSR load factors at a level no higher than necessary to fully compensate for unreimbursed CSR amounts provided to enrollees. Imposing a higher load exacerbates shifts in enrollment and decreases market stability.
We appreciate that American Indian/Alaska Native populations and Tribal health programs are especially reliant on stable silver plan pricing. We affirm that CMS engages in tribal consultation for all rulemakings and has worked with the appropriate parties to ensure that any such potential impact is mitigated.
Comment:
Several commenters stated that the proposed definition of “actuarially justified” CSR load factors, which emphasizes calibration on actual CSR experience, may conflict with Affordable Care Act provisions requiring a single risk pool and prohibiting rates based on plan-specific experience. Those commenters recommended that CMS should allow issuers to consider the expected membership distribution and unreimbursed CSR costs at the overall single risk pool or market level when developing CSR load factors, rather than requiring issuers to develop CSR load factors that are specific to their enrolled population. Commenters also recommended that CMS clarify whether “actuarially justified” implies an issuer/plan-level “matching” requirement or whether only experience-calibrated methodologies are acceptable.
Response:
We proposed that an actuarially justified CSR load factor is one that is calibrated based on actual CSR experience rather than an unreasonable projection or assumption. We agree that the Affordable Care Act provisions require a single risk pool and prohibit rates based on plan-specific experience. An actuarially justified CSR load factor should not be based on plan-specific experience; it must be set to only recover expected unpaid CSRs, which we referred to as “actual CSR experience.” We did not propose, and do not intend to imply, that an issuer/plan-level “matching” is required or that only experience-calibrated methodologies are acceptable. We acknowledge that the CSR load amount will be based on a projection of CSR enrollment distribution and costs, but we emphasize that the projection should reflect realistic assumptions. It may be appropriate to consider CSR enrollment across the entire market rather than only considering the specific enrollment of one particular issuer when projecting CSR enrollment and determining the CSR load. For example, some States may require all issuers to use the same CSR load factor on all silver plans, and this practice is permissible so long as the CSR load is based on a reasonable projection of CSR enrollment and utilization of services. In this case, the CSR load factor should be set to only recover expected unpaid CSRs. The CSR load factor should not be used to inflate silver premiums beyond expected unpaid CSR amounts to reduce premiums on other metal tiers and further distort pricing between metal levels.
Comment:
Some commenters requested that CMS clarify the goals and intended uses of the CSR data collection and recommended enhanced communication to consumers about how CSR loading affects premiums and subsidies to improve transparency and understanding.
Response:
As we stated in the proposed rule, the purpose of this proposal is to allow the State or CMS, as applicable, to determine whether the CSR load factor is actuarially justified and not excessive in relation to the amount expected to be paid by an issuer in unreimbursed CSRs. We are concerned that excessive CSR loads on silver plans lead to inflated premiums for silver plans, further distorting pricing for bronze and gold plans relative to silver plans; limit consumer choice; and significantly increase the cost of the second lowest cost silver plan, which in turn increases PTC amounts and Federal expenditures. The additional data will be used to ensure that CSR loads are actuarially justified to compensate for the amount of unreimbursed CSRs. To the extent they exist, CSR loads should be limited to account for the amount of the actual unpaid CSRs. Silver plan premiums should not be increased significantly to achieve a desired subsidy level rather than as a reflection of unpaid CSRs resulting from CSR plan variant enrollees in those plans. If, for example, an issuer projects a 20 percent premium load to silver plans is needed to recover unpaid CSRs, but the issuer applies a 30 percent load to silver plans, that would presumably lower premiums for bronze and gold plans that are unaffected by unpaid CSRs. That load amount greatly exceeds the projected amount of unpaid CSRs and goes beyond the goal of recovering unreimbursed CSR costs. The data collection is intended to ensure that CSR loading is not being used as a tool to achieve a target price point that does not reflect the allowable rating factors.
For the comments recommending communication to consumers about how CSR loading affects premiums and subsidies, these comments are out of scope for this final rule because they do not relate to the specific proposals included in the proposed rule. We note, however, that
Healthcare.gov
, an official consumer-facing CMS website, includes information for consumers regarding CSRs, including how to qualify and an explanation of how CSRs can lower out-of-pocket costs.[97]
Comment:
Several commenters requested CMS to delay implementation to allow for system updates. Many commenters noted that rate filings are due in April and that issuers' current systems cannot generate the requested data. Several commenters anticipated technical difficulties in using the standard methodology set forth in § 156.430(c)(2) to report CSR amounts paid on behalf of enrollees as proposed.[98]
Other commenters requested CMS allow a safe harbor for good faith efforts to calculate actual amounts.
Response:
We recognize that some updates to issuers' systems will be necessary, but we do not agree that a delayed applicability date is warranted. The proposed data collection process is intended to leverage the existing rate
( printed page 29571)
filing process by using the URRT and actuarial memorandum. We proposed that issuers use the standard methodology to determine the amount of CSRs paid by the issuer because we believe it is the most accurate method for such calculation and because of issuers' familiarity with this methodology. While we recognize that many issuers might have to update their systems to calculate the actual value of CSRs provided, we believe that issuers should already be calculating the actual CSRs paid for enrollees, as specified in the PY26 Rate Filing Guidance. That guidance instructed issuers to report the actual CSRs paid for enrollees for PY 2024 in the actuarial memorandum submitted with the 2026 rate filing. While CMS provided flexibility in the May 27, 2025
Frequently Asked Questions on Plan Year 2026 Individual Market Rate Filing Instructions
for issuers that were unable to timely calculate the precise amount of actual CSRs paid for enrollees for PY 2024 to provide an estimate developed using a reasonable methodology detailed in the actuarial memorandum, that flexibility was limited to PY 2026 rate filing justifications.
As stated in the proposed rule, the approach of collecting an aggregate amount of CSRs provided at the plan level on the URRT is less burdensome than the collection of policy-level CSR data through the CSR reconciliation process that was required for all issuers that received advance payment of CSRs prior to the cessation of these payments in October 2017. Therefore, while issuers may incur some additional costs for actuarial analysis, issuers are generally already familiar with the process of calculating the actual amount of CSRs provided using the standard methodology, and the limited additional burden issuers might incur does not warrant a delayed implementation.
We acknowledge that in some States initial rate filings must be submitted in April. We note, however, that those are proposed rate changes, and States typically provide issuers with the opportunity to adjust their rate filings before finalizing them several months later. Likewise, the deadlines for submitting proposed rate changes to CMS are June 1 (for States without an Effective Rate Review Program) or July 15 (for States that have an Effective Rate Review Program). Final rate filings are not due to CMS until August 12 (for filings that contain a QHP in States with Exchanges served by the
HealthCare.gov
platform) or October 15. Issuers in States with earlier deadlines should refer to the 2026 Rate Review Timeline Bulletin [99]
for deadlines for revising their initial rate submissions.
D. Part 155—Exchange Establishment Standards and Other Related Standards
1. Standardized Plan Options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv))
In the 2027 Payment Notice proposed rule (91 FR 6383), we proposed to exercise our authority under sections 1311(c)(1) and 1321(a)(1)(B) of the Affordable Care Act to discontinue the full suite of standardized plan option policies effective beginning in PY 2027. As discussed in greater detail in the preamble section of this final rule addressing § 156.201, we proposed to remove the following from our regulations: the definition of “standardized option” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b) as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv). We also proposed to redesignate paragraphs (c)(3)(i)(I) through (M) of § 155.220 as paragraphs (c)(3)(i)(H) through (L), respectively. Finally, we proposed to cease the annual design and publication of these standardized plan options in the applicable Payment Notice rulemaking for each plan year.
We refer readers to section III.E.8. of this final rule for discussion of our proposals and final policies related to standardized plan options (including proposed amendments to §§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv)) as well as summaries of and responses to public comments received on those proposals. We did not receive any comments in response to our proposal to redesignate paragraphs (c)(3)(i)(I) through (M) of § 155.220 as paragraphs (c)(3)(i)(H) through (L), respectively. For the reasons outlined in the proposed rule and this final rule, we are finalizing these redesignations as proposed.
2. Approval of a State Exchange (§ 155.105)
In the 2027 Payment Notice proposed rule (91 FR 6327), we proposed to remove § 155.105(b)(4) to rescind a requirement made in the 2025 Payment Notice (89 FR 26259 through 26261), that a State seeking to operate a State Exchange must first operate, for at least 1 plan year, a State-based Exchange on the Federal platform (SBE-FP). The original amendment was intended to give States sufficient time to create, staff, and structure a State Exchange. However, in the proposed rule, we recognized that requiring States to first operate as an SBE-FP for at least 1 plan year could potentially create unnecessary barriers for States that are well prepared to implement a State Exchange more immediately.
Sections 1311(b) and 1321(b) of the Affordable Care Act allow States to elect to operate their own health insurance Exchanges to provide individuals and employers with health insurance coverage. Every State that has implemented a State Exchange after 2014—the year the initial 13 State Exchanges began operation—first operated an SBE-FP for at least 1 plan year, before codification of the current requirement in the 2025 Payment Notice. This history shows how first operating an SBE-FP has been the preferred approach. However, in the proposed rule, we stated that we recognize that States may have existing infrastructure, relationships, and expertise that could support a State's successful operation of a State Exchange, without first operating an SBE-FP. For example, FFE States are permitted to elect to perform plan management functions similar to the plan management functionality required of all SBE-FPs.[100]
The infrastructure and the associated interested party relationships and State expertise to support such functionality could be leveraged from a direct FFE to State Exchange implementation. Additionally, the technology infrastructure available today to States for implementation of State Exchanges has become more compatible, such that the technology used to support one State Exchange implementation could
( printed page 29572)
be leveraged by another State Exchange. A State must demonstrate its ability to operationalize State Exchange functional requirements through a well-established and robust review process with HHS. Whether a State first operates an SBE-FP does not change our review process for determining whether a State is ultimately prepared to implement a State Exchange. For the reasons provided in this document, we proposed to remove § 155.105(b)(4), such that a State seeking to operate a State Exchange is not required to first operate an SBE-FP for at least 1 plan year, including its first open enrollment period.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal to rescind a requirement that a State seeking to operate a State Exchange must first operate, for at least 1 plan year, an SBE-FP below.
Comment:
Several commenters opposed the proposal and urged HHS to retain the existing policy. These commenters indicated that removal of the 1-year requirement minimizes consumer safeguards given the potential increased risk that a State implements a State Exchange prior to demonstrated readiness. These commenters further indicated that the requirement for a State to operate an SBE-FP for at least 1 plan year provides States with sufficient time to develop necessary relationships with interested parties and provides interested parties sufficient time to contribute to a State's readiness to operate a State Exchange. A few of these commenters indicated that the current requirement codifies a best practice that States benefit from operating an SBE-FP for at least 1 plan year, and that all States that transitioned from an FFE to a State Exchange over the past several years first operated an SBE-FP, including prior to the codification of the current requirement in the 2025 Payment Notice. These commenters also requested that HHS provide more detail regarding how the current requirement could be an unnecessary barrier to State Exchange implementation, as well as more detail on technological advancements that support removal of the current requirement.
Response:
As discussed in the proposed rule, a State must demonstrate its ability to operationalize State Exchange functional requirements through a well-established and robust review process with HHS. Whether a State first operates an SBE-FP does not change our review process for determining whether a State is ultimately prepared to implement a State Exchange. To expand further, HHS' review process entails a careful analysis of a State's operational readiness to implement a State Exchange according to the regulatory requirements, which, for example, is demonstrated through a series of CMS test cases of eligibility and enrollment functionality, and through discussions about best practices and lessons learned from previous State Exchange transitions. As an example, for the impact of a State Exchange implementation on interested parties, HHS reviews a State's plan and progress toward interested party engagement and communications, as well as interested party activities and progress in meeting State Exchange operations. This includes reviewing State Exchange programmatic requirements for their agents and brokers, assisters, navigators, and issuers, including funding, training and certification activities to ensure compliance. Further, to support minimizing consumer confusion around a transition, we work closely with a State implementing a State Exchange to develop coordinated consumer outreach plan with the intent to minimize consumer disruptions and maintain consumer trust with the State entity operating the State Exchange during a transition.
A State that is deficient in any of the State Exchange functional requirements would not be approved to implement a State Exchange for its intended plan year and would be given the choice to continue demonstrating operational readiness to HHS for a future plan year. Notably, we do not require a maximum number of months required for a State to demonstrate operational readiness to HHS to implement a State Exchange. However, we do require that a State submit its first State Exchange blueprint application to HHS at least 15 months prior to a State's first intended open enrollment as a State Exchange, and the review process with HHS generally begins at that time. This means that HHS review process for a State Exchange implementation could take longer than 15 months, until HHS determines that a State is fully ready to meet the requirements of a State Exchange and adequately support its consumers.
Moreover, as discussed in the proposed rule, the technology infrastructure available today to States for implementation of State Exchanges has become more compatible, such that the technology used to support one State Exchange implementation could be leveraged by another State Exchange. For example, there may be State vendor-supported informational technology platforms, such as call center technology, developed for one State Exchange that can be leveraged for another State Exchange, which could reduce upfront implementation time. Our proposal aims to be supportive of evolving technology growth that could factor into a State's ability to more easily implement a State Exchange that meets all of the required functionality and meets HHS operational readiness review requirements
Comment:
A few commenters supported the proposal and indicated support for State flexibility and reduced barriers in State Exchange implementation. One commenter further recommended that HHS should continue to ensure that a State is ready to implement a State Exchange prior to HHS approval.
Response:
We acknowledge these comments and reiterate that a State must demonstrate its ability to operationalize State Exchange functional requirements through a well-established and robust review process with HHS. As stated above, whether a State first operates an SBE-FP does not change our review process for determining whether a State is ultimately prepared to implement a State Exchange.
3. Election To Operate an Exchange After 2014 (§ 155.106)
In the 2027 Payment Notice proposed rule (91 FR 6327), we proposed to amend § 155.106(a)(2) to rescind a requirement we made in the 2025 Payment Notice (89 FR 26261 through 26263) that, as part of a State's activities for its establishment of a State Exchange, the State must provide, upon request, supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements. Section 155.106(a)(2) requires that States electing to operate a State Exchange submit a State Exchange Blueprint Application to HHS for approval. The current State Exchange Blueprint application provides that we may require live demonstrations of Exchange functionality on the State Exchange's platform, as well as supporting documentation, as evidence of the State's progress toward meeting State Exchange Blueprint application requirements. For clarity, we had finalized in the 2025 Payment Notice to codify that as part of the State's submission of a State Exchange
( printed page 29573)
Blueprint application, HHS has the authority to request supplemental documents it determines necessary for the State to detail its implementation of the required State Exchange functionality. To support deregulation where possible, we proposed to remove what we codified.
The State Exchange Blueprint continues to serve as a vehicle for a State to document its progress toward implementing its intended Exchange operational model. HHS approves a State's Exchange Blueprint Application and subsequently provides approval for a State to operate a State Exchange, based upon a State meeting State Exchange implementation requirements noted in the Blueprint Application. The current Blueprint Application requires a State to sign and agree that HHS may require supporting documentation from a State as evidence of its progress toward meeting State Exchange Blueprint Application requirements, which is part of the overall process for providing a State with approval to operate a State Exchange. Notably, in our experience, States recognize the need for HHS to request supplemental documentation for HHS to assess a State's readiness to operate a State Exchange, which supports a State's successful State Exchange operation. States have provided such supplemental documentation upon HHS request both before and after this requirement was originally codified. Given this preexisting process, we stated in the proposed rule that we do not believe deregulation in this instance is harmful, nor would it lead to burden on States. Therefore, we proposed to rescind the requirement that a State provide, upon request, supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements from § 155.106(a)(2).
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal that a State provide, upon request, supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements below.
Comment:
Several commenters objected to the proposal to rescind the requirement that a State provide, upon request, supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements. A few of these commenters indicated that removal of the requirement, while it may support deregulation per Executive Order 14192, could instead lead to confusion in expectations for a State to demonstrate readiness to HHS to implement a State Exchange. In particular, these commenters noted that removal of the requirement may create uncertainty with regard to the language in the State Exchange Blueprint application, which requires a State to sign and agree that HHS may require supporting documentation from a State as evidence of its progress toward meeting State Exchange Blueprint Application requirements. The remaining commenters that objected to the proposal indicated that maintaining the current regulatory requirement supports HHS ability to confirm that a State is ready to implement a State Exchange.
Response:
Per § 155.106(a)(2), a State must submit a State Exchange Blueprint Application to HHS for approval. As noted in the proposed rule, the State Exchange Blueprint Application includes that HHS may require supporting documentation from a State as evidence of its progress toward meeting State Exchange Blueprint Application requirements. This requirement in the State Exchange Blueprint Application will continue to exist. Notably, in our experience, and as discussed in the proposed rule, States have recognized the need for HHS to request supplemental documentation for HHS to assess a State's readiness to operate a State Exchange through the approval of a State's Blueprint Application. States have long submitted supplemental documentation to HHS upon request prior to the codification of the requirement in the 2025 Payment Notice, since the requirement that a State submit such supplemental document is noted in the State Exchange Blueprint Application. HHS review and feedback of State-submitted supplemental documentation is used to provide a State with meaningful feedback, including best practices observed in other State Exchange transitions and State Exchange and FFE operations, which overall supports a State's successful State Exchange implementation. We will continue to request supplemental documentation from a State seeking to implement a State Exchange, as needed to assess a State's readiness to implement a State Exchange as part of our approval of a State's Blueprint Application.
Comment:
A few commenters supported the proposal and indicated support for deregulation to support State flexibility and reduced barriers in State Exchange implementation.
Response:
We acknowledge these comments and reiterate that a State must demonstrate its ability to operationalize State Exchange functional requirements through a well-established and robust review process with HHS.
4. Amending Requirements for State Exchanges To Operate a Centralized Eligibility and Enrollment Infrastructure (§§ 155.205(b) and 155.221(k))
a. Amending Requirements for State Exchanges To Operate a Centralized Eligibility and Enrollment Platform on the State Exchange's Website (§ 155.205(b))
In the 2027 Payment Notice proposed rule (91 FR 6328), we proposed to revise § 155.205(b)(4) and (5) to remove the requirement that all State Exchanges operate a consumer-facing centralized eligibility and enrollment platform on the State Exchange's website such that a State Exchange could choose to rely entirely on web-brokers (a type of non-Exchange entity) for implementing and operating consumer-facing websites that facilitate the eligibility and enrollment process in a State Exchange pursuant to the proposal in section III.D.4.b. of this final rule. We stated in the proposed rule that these consumer-facing websites operated by web-brokers would facilitate the online submission of eligibility applications by individuals seeking coverage through a State Exchange and facilitate the selection and enrollment into QHPs on a State Exchange for qualified individuals. Further, we stated that these consumer-facing websites operated by web-brokers would also interface with the State Exchange website, which the State would still be required to operate broadly under § 155.205(b), in such a manner as to transmit information from the non-Exchange website to the State Exchange website. We stated that this would facilitate the State Exchange meeting the requirements at §§ 155.205(b)(4) and (5) which requires an Exchange to maintain a website that allows an individual to submit a single streamlined eligibility application to the State Exchange and enroll in coverage through the State Exchange. Operationally, we stated that such consumer-facing websites operated by web-brokers would be required to interface with the information technology platform that the State Exchange would still need to operate to appropriately process applicant eligibility determinations and process enrollment transactions with QHP issuers (that is, the State Exchange's `back-end' eligibility and enrollment
( printed page 29574)
system). We stated that using State Exchange-approved technical specifications and/or standards for those interfaces (for example, web services) would allow the exchange of data between the consumer-facing websites operated by web-brokers and the State Exchange in a manner that is seamless to consumers. Additionally, we stated that such an interface would allow for the transmission of consumer eligibility application information and/or QHP selection and enrollment information necessary for the State Exchange to meet key Exchange functional requirements. These requirements include collecting information from applicants through an HHS-approved single, streamlined eligibility application for insurance affordability programs per §§ 155.310 and 155.405; performing eligibility verifications required at §§ 155.315 and 155.320; performing assessments or determinations of Medicaid/CHIP eligibility required at § 155.302; and performing determinations of eligibility for QHP enrollment and APTC/CSRs at §§ 155.305 and 155.310. This also includes key enrollment functions such as collecting and maintaining records of QHP enrollment for all consumers of the State Exchange as required under § 155.400 and transmitting such enrollment information to CMS and IRS. We stated that such consumer-facing websites operated by web-brokers would also need to allow for consumers to select and enroll into a QHP (that is, through direct enrollment) in order to submit QHP selection and enrollment to the State Exchange. This model, referred to as the State Based Exchange Enhanced Direct Enrollment (SBE-EDE) model, was proposed and discussed in further detail in section III.D.4.b of the proposed rule. In the proposed rule, we stated that State Exchanges that opt to take this approach would be required to establish standards and a process for selecting the web-brokers who they may interface with in this manner, similar to the standards and criteria that we have established for direct enrollment entities at §§ 155.221(j) and 155.220(n), including a requirement that a non-Exchange web-broker entity satisfy all requirements under § 155.110(a).
When HHS finalized the requirement at § 155.205(b) that Exchanges operate a centralized eligibility and enrollment platform on the Exchange's website in the 2025 Payment Notice (89 FR 26271), HHS' intent was to tie together regulatory requirements throughout part 155 regarding the integrated nature of online, real-time automated eligibility functions that Exchanges were intended to perform. This included the intent to clearly affirm the close integration that exists and is necessary between Exchange-operated websites, the online consumer-facing single streamlined eligibility application, and the back-end eligibility system that performs automated eligibility verifications and eligibility determination functions that return real-time, online results to the consumer.
While in the proposed rule we affirmed that State Exchanges are responsible for making all eligibility determinations for QHP coverage and related insurance affordability programs through a centralized eligibility processing system and enrollment records system, requiring State Exchanges to operate a consumer-facing, centralized eligibility and enrollment consumer website that interfaces with the State Exchange's back-end eligibility processing and enrollment records system may prohibitively restrict Exchange flexibility and innovation. While all State Exchanges that do not use the Federal platform currently operate their own eligibility and enrollment consumer interface on the State Exchange's website, we believe that maintaining this requirement in regulation could discourage State Exchanges from pursuing innovative approaches that might better serve their specific populations and enhance the consumer experience, including private sector-focused consumer engagement and enrollment strategies. We believe that providing State Exchanges with flexibility in how they offer their online eligibility and enrollment consumer interface may allow State Exchanges to develop solutions that address the unique needs of their residents and markets. Removing the requirement for an Exchange to operate an eligibility and enrollment consumer interface on its website is a necessary step in order to codify the SBE-EDE option we proposed at § 155.221(k), as described in section III.D.4.b. and previously in this section. Under this option, the ability for State Exchanges to exclusively utilize web-brokers to operate consumer-facing websites that facilitate eligibility and enrollment is the key component.
We noted that sections 1311(c)(5) and (d)(4)(C) of Affordable Care Act do not require Exchanges to operate a centralized consumer-facing eligibility and enrollment website that supports both eligibility determinations for, and enrollments in, QHPs.[101]
Rather, section 1311(d)(4)(C) of the Affordable Care Act provides that an Exchange must maintain an internet website through which enrollees and prospective enrollees of QHPs may obtain standardized comparative information on QHPs available in the State. Exchanges must also undertake certain minimum functions to facilitate the purchase of QHPs under section 1311(b)(1)(A) of Affordable Care Act and make available QHPs to qualified individuals and employers under section 1311(d)(2)(A) of Affordable Care Act. These minimum functions facilitate the purchase of QHPs by helping to make the purchase of QHPs easier and also by administering elements of the structure necessary to make QHPs available. This approach of relying on private sector EDE entities aligns with the general Affordable Care Act framework that relies on and benefits from the government working within the existing health insurance coverage infrastructure rather than taking a purely governmental or public approach to advancing coverage for the individually insured population. The Affordable Care Act does not establish new government-provided health plans but instead creates Exchanges to facilitate the purchase of government-subsidized QHPs through the individual health insurance market. Exchanges support specific statutory functions that make QHPs available to purchase. These functions include certifying that QHPs conform to certain Federal standards in addition to State and Federal standards that govern the individual health insurance market. Exchanges must also provide certain tools to help consumers shop for QHPs, as well as support eligibility determinations and enrollment in other public health care programs such as Medicaid and CHIP. Importantly, these additional standards do not dictate any specific changes to the existing enrollment pathways on the individual market.
In the context of operating an internet website, we interpret the statutory language at section 1311(c)(5) and (d)(4)(C) of Affordable Care Act to require that Exchanges minimally operate an informational website that provides consumers with the ability to view comparative information on QHP options, but that the Exchange may direct consumers to other entities or resources for purposes of facilitating the submission of applications for eligibility
( printed page 29575)
and enrolling enrollment in QHPs, with APTC and CSRs, if otherwise eligible. We stated in the proposed rule that a State Exchange that elects the new SBE-EDE option would continue to be responsible for determining eligibility for, and granting exemption certifications under, section 1311(d)(4)(H) of Affordable Care Act, as applicable; making available an electronic calculator consistent with section 1311(d)(4)(G) of Affordable Care Act; establishing a Navigator program as required under section 1311(d)(4)(K) of Affordable Care Act; and providing for the operation of a toll-free telephone hotline under section 1311(d)(4)(B) of Affordable Care Act. As mentioned earlier and consistent with section 1311(d)(4)(F) of the Affordable Care Act, we stated that a State Exchange that elects to pursue this new SBE-EDE option would continue to be responsible for conducting assessments or determinations of eligibility for Medicaid and CHIP. We stated that they would use the information provided by consumers on the consumer-facing website operated by a web-broker State Exchange's approved single, streamlined eligibility application that is made available on the consumer websites operated by the web-brokers selected by the State Exchange as part of the SBE-EDE option, and for referring individuals who are assessed or determined eligible for Medicaid or CHIP to the appropriate State Medicaid agency for enrollment in those programs.
The State Exchanges that are currently operating have had to engage with private entities in a manner that would similarly translate to what a State Exchange would be doing under the SBE-EDE model, in terms of relying on the services of private entities to develop and operate a consumer-facing website (that is, online eligibility and enrollment portal) that facilitates consumers applying for and enrolling in QHPs through the State Exchange. Most State Exchanges currently in operation have competitively-procured services from a private entity to develop and operate an online eligibility and enrollment portal (including through which an applicant can submit a single, streamlined application for insurance subsidy programs) and consumer-facing QHP enrollment portal on their respective State Exchange website. These online, consumer-facing eligibility and enrollment portals on State Exchange websites facilitate the online submission of consumer eligibility applications and QHP selection and enrollments, and through web interfaces that are seamless to consumers, transmit that information to the State Exchange's back-end eligibility and enrollment processing information system. In the proposed rule, we stated that we believe that in the absence of a centralized consumer facing website for eligibility and enrollment operating on a State Exchange's website under the proposed SBE-EDE approach, web-brokers may provide that service to a State Exchange in a manner that is similar to that which currently exists between State Exchanges and the private entities they have contracted with to operate their centralized consumer-facing online eligibility and enrollment portal on the State Exchange's website. In both approaches, whether a web-broker provides the online eligibility and enrollment portal to consumers outside of the State Exchange's website, as we stated would be the case under this proposal, or a private entity has developed and operates the consumer-facing online eligibility and enrollment portal on the State Exchange's website in a centralized fashion, the State Exchange maintains responsibility for meeting all other Federal requirements for their online consumer assistance functions. As such, we stated that the State Exchange would still need to maintain a website that meets all other website requirements for State Exchanges under § 155.205(b), in the same manner that SBE-FPs are currently required to maintain an informational website for consumers while relying on the Federal eligibility and enrollment platform for eligibility and enrollment functions. In particular, we stated that State Exchanges that elect the SBE-EDE option would be required to meet the minimum Exchange function requirement under section 1311(d)(4)(C) of the Affordable Care Act to maintain a website providing standardized comparative information on such plans to enrollees and prospective enrollees of QHPs.
In the 2025 Payment Notice (89 FR 26271), we amended § 155.302(a) to codify the Exchange's responsibility for conducting eligibility determinations and maintaining records of all QHP enrollments on the Exchange. In the proposed rule, we stated that State Exchanges would still maintain this responsibly if it elects to pursue the new SBE-EDE option and exclusively utilize web-brokers for operating consumer websites that facilitate the eligibility and enrollment process in a State Exchange. Additionally, we stated that enrollment through such a consumer website would still be considered enrolling in a QHP through the State Exchange per § 155.220(c)(3) and proposed § 155.221(k)(2).
We noted in the proposed rule that this proposed amendment would not affect other regulatory requirements throughout 45 CFR part 155 that govern State Exchange eligibility and enrollment functions. For instance, per § 155.405, we stated that State Exchanges would still be required to obtain HHS approval for the eligibility application used on the consumer websites. HHS' review of the State Exchange's eligibility application would follow the currently established processes, including requiring that the State Exchanges demonstrate appropriate functionality to make accurate determination. As such, State Exchanges that do not rely on the Federal eligibility and enrollment platform can continue to meet these obligations without operating a singular, centralized consumer-facing eligibility and enrollment website.
We recognized in the proposed rule that allowing State Exchanges to take this approach would create different consumer experiences in applying for and enrolling in coverage through State Exchanges as compared to an approach where a State Exchange implements and operates a centralized eligibility and enrollment infrastructure. We sought comment on how State Exchanges that implement such an approach can create comparable consumer experience, in addition to comments on HHS oversight and the approval requirements proposed in section III.D.4.b. of this final rule. We sought comment on this proposal.
We received a substantial number of thoughtful and substantive comments on this proposal, reflecting significant stakeholder interest in and engagement with this important policy area. The agency continues to strongly support the goals of the proposal and remains committed to creating flexibility that would allow States to better serve their residents' needs. However, given the volume and complexity of the comments received, we are unable to give those comments the thorough and careful consideration they deserve within the timeframe required to publish this final rule that provides States, health insurance issuers, and other interested parties benefit parameters and other rules they need for the PY 2027 rate setting, plan approval, and QHP certification processes. Rather than address the proposal without the benefit of a complete and deliberate review of the public record, we believe it is in the best interest of interested parties and the public to address this proposal, including all public comments
( printed page 29576)
HHS received in response, during the 2028 Payment Notice rulemaking cycle.
We encourage interested parties to continue engaging with us on this important issue.
b. SBE-Enhanced Direct Enrollment Option (§ 155.221(k))
To build on the success of the EDE pathways and enhance the consumer enrollment experience, in the 2027 Payment Notice proposed rule (91 FR 6330), we proposed to offer additional flexibility to State Exchanges to leverage the benefits of EDE through a private sector-supported consumer engagement and enrollment strategy that is tailored to the needs of local markets. Accordingly, we proposed to add a new paragraph (k) to § 155.221 to establish a process for State Exchanges that do not rely on the Federal eligibility and enrollment platform to elect a new SBE-EDE option, in which the applicable State Exchange could seek HHS approval for web brokers to serve as the exclusive enrollment pathways for operating consumer-facing websites that facilitate the eligibility and enrollment process in a State Exchange. In the proposed rule, we stated that these consumer-facing websites operated by web-brokers will facilitate the online submission of eligibility application by individuals seeking an eligibility determination for, and enrollment in, a QHP offered through the Exchange with APTC and CSRs, if otherwise eligible. Previously, the Exchange DE option was finalized in part 1 of the 2022 Payment Notice Final Rule (86 FR 6151) and later repealed in part 3 of the 2022 Payment Notice (86 FR 53429). We proposed to codify this policy again and to also allow Exchanges to offer their consumers a form of EDE in which the Exchanges rely exclusively on web-brokers to implement and operate the consumer-facing websites through which consumers select and enroll in a QHP without requiring that the Exchanges also operate a centralized consumer-facing eligibility and enrollment website. The proposal applied exclusively to State Exchanges so that, if finalized, the experience and insights of State Exchanges that implement this model could be leveraged by other Marketplaces. We stated in the proposed rule that this would help inform operational considerations were we to expand this model to the FFEs and State Exchanges that use the Federal eligibility and enrollment platform, both of which were included in the previous policy. We stated that since the repeal of the Exchange DE option, many of the policy and operational priorities, as well as then-new Federal laws cited at that time to justify the repeal, are no longer competing for agency resources, and this has created bandwidth to codify a version of the DE option once again.[102]
We stated in the proposed rule that a State Exchange electing to implement the SBE-EDE option will continue to be responsible for meeting and ensuring that all approved EDE partners meet all applicable statutory and regulatory requirements governing application for and enrollment in QHPs. Additionally, we stated that the State Exchange will also continue to be responsible for sharing eligibility determination and enrollment information in coordination with issuers and HHS in accordance with §§ 155.340, 155.400, and 155.430. We stated that the State Exchange will continue to provide HHS enrollment data to ensure accurate APTC payments are made to issuers on behalf of qualified individuals and in support of reconciliation of APTC on individual income tax returns.
In connection with the SBE-EDE option, we stated in the proposed rule that the State Exchange will still be required to make available a website listing basic QHP information for comparison,[103]
and a listing with links to approved partner websites for consumer shopping, plan selection, and enrollment activities. Consistent with section 1311(d)(4)(E) of Affordable Care Act, we stated that the comparative plan information presented on the State Exchange's website will need to continue to utilize a standardized format, including the use of the uniform summary of benefits and coverage established under section 2715 of the PHS Act.[104]
We stated that the standardized comparative information displayed on the Exchange website will also be required to continue to include the quality ratings assigned to each QHP offered through the Exchange.[105]
In addition, we stated that the State Exchange, along with its EDE partners, would continue to be responsible for meeting Federal accessibility standards under § 155.205(c) for individuals living with disabilities and for individuals who have limited English proficiency.[106]
Finally, we stated that all consumer data collected, stored, or transmitted through web-broker platforms operating under the SBE-EDE option would remain subject to the privacy and security standards established at § 155.260 and web-brokers participating in the SBE-EDE option would be subject to HHS oversight and monitoring pursuant to § 155.280 as a non-Exchange entity. We stated that State Exchanges implementing the SBE-EDE option would be required to ensure that web-brokers comply with these protections, including, but not limited to, encryption, access controls, and audit logging requirements.
In the proposed rule, we stated that HHS would maintain oversight authority over State Exchanges under § 155.1200, which would enable enforcement of Federal requirements associated with the SBE-EDE option and would allow HHS to take necessary actions to mitigate program integrity risks inherent in this model. To ensure ongoing compliance and reduce program integrity risks under the SBE-EDE option, we stated that HHS would rely on the State-based Marketplace Annual Reporting Tool (SMART), as a key oversight mechanism. Under § 155.1200(b), we stated that State Exchanges would be required to complete SMART submissions annually, attesting to their compliance with relevant Exchange operational requirements under part 155. Additionally, under § 155.1200(c), we stated that State Exchanges would need
( printed page 29577)
to engage independent qualified auditing entities to perform annual external financial and programmatic audits, which would be included with SMART submissions. We stated that HHS would review all SMART submissions and would issue formal letters to State Exchanges summarizing observations on areas of noncompliance and identifying any required corrective actions. We stated that This SMART-based compliance monitoring process would serve as a critical safeguard against program integrity risks by providing HHS with regular, audited documentation of State Exchange operations and would be relied on under the SBE-EDE model.
Beyond the SMART process, we stated in the proposed rule that HHS would employ additional oversight mechanisms to mitigate program integrity risks. These include formal technical assistance opportunities tailored to SBE-EDE implementation efforts and challenges, as well as ongoing informal communications with State Exchange leadership and staff for proactive, real-time issue identification and resolution. In the proposed rule, we stated that together, these oversight tools—anchored by the SMART compliance monitoring process—would enable HHS to exercise its enforcement authority and ensure that State Exchanges implementing the SBE-EDE option maintain program integrity and meet all Federal requirements.
In the proposed rule, we proposed to modify § 155.221(k) such that, subject to HHS approval, a State Exchange that does not rely on the Federal eligibility and enrollment platform may elect to engage one or more web-brokers described in paragraph § 155.221(a) to facilitate QHP enrollments through its Exchange. We stated that such approved entities would enroll qualified individuals in a QHP in a manner that constitutes enrollment through the Exchange [107]
and would also facilitate consumer submission of eligibility application through the entity's consumer website to the State Exchange to receive eligibility determinations from the State Exchange for APTCs and CSRs.
At § 155.221(k), we proposed requirements for a State Exchange to become an SBE-EDE. We proposed that a newly-transitioning or approved State Exchange must submit an Exchange Blueprint application, or Blueprint revision, to HHS for review at least 15 months prior to the targeted open enrollment launch date as an SBE-EDE.[108]
For an approved State Exchange, this would be considered a significant change to its Blueprint.[109]
We also proposed that the State Exchange must meet all other applicable Federal statutory and regulatory requirements for the operation of an Exchange, including for approved State Exchanges to request and obtain HHS approval for any significant changes to its single, streamlined eligibility application under § 155.405. Following submission of an approved State Exchange's submission of a revised Exchange Blueprint application, in accordance with § 155.105(e), HHS would have up to 90 days [110]
to review the revision and approve or deny the change.
Additionally, in accordance with § 155.105(c)(2), we proposed at § 155.221(k)(1) that a State Exchange that wants to implement the SBE-EDE option would be required to demonstrate to HHS operational readiness for the State Exchange to enroll qualified individuals in a QHP in a manner that constitutes enrollment through the Exchange and to enable individuals to apply for APTC and cost sharing for QHPs, as well as receive assessments or determinations of Medicaid and CHIP eligibility from the Exchange as described in § 155.302, using the eligibility application described in § 155.405. We proposed a new requirement at § 155.221(k)(2) that the State also would receive approval only if it provides HHS with an implementation plan and timeline that details the key activities, milestones, and its communications and outreach strategy to support the transition of enrollment operations to EDE entities. We stated that this is to ensure that HHS and the State have an opportunity to coordinate these details to maximize the chances of a successful transition. We stated that State Exchanges that elect to implement the SBE-EDE option would retain the flexibility to determine their own business controls while complying with § 155.220(n) and § 155.221(j), which outline the applicability of Federal web-broker and EDE requirements to State Exchanges, including requirements related to standardized website disclaimers, web-broker operational readiness, business audit and security and privacy documentation, and display of website changes. We proposed at § 155.221(k)(3) that HHS would not approve a State Exchange to implement the SBE-EDE option unless the State Exchange demonstrates to HHS that at least one EDE entity selected by the State is capable of enrolling all consumers in the State. In particular, we stated that we believe it is critical that State Exchanges that elect to implement the SBE-EDE option establish that at least one EDE entity meets the minimum Federal requirements to participate in the Federally-facilitated Exchange enhanced direct enrollment program, including requirements at §§ 155.220 and 155.221, particularly § 155.220(c)(3)(i)(A) and (D),[111]
to ensure consumers have at least one option through which to view detailed QHP information for all available QHPs in the State, and meets accessibility requirements under § 155.205(c). Therefore, we proposed that if no EDE partner meets these requirements, the State Exchange would be required to continue operation of its own consumer-
( printed page 29578)
facing State Exchange website for purposes of eligibility and enrollment. To assist State Exchanges in meeting requirements to become an SBE-EDE, we stated that State Exchanges could partner with an existing, HHS-approved web-broker EDE partner [112]
as a starting point to develop their own EDE programs, as these entities have already met requirements for HHS approval to participate in the FFE's EDE program. In summary, we proposed in the proposed rule to allow newly-transitioning or approved State Exchanges to make web-brokers the exclusive enrollment pathways to facilitate the online submission of eligibility applications by individuals seeking coverage through the State Exchange, including by adding the following new provisions: § 155.221(k), which describes the proposed SBE-EDE option and approval process; § 155.221(k)(1), which lays out the proposed requirement for a State Exchange to demonstrate operational readiness to enroll qualified individuals in a QHP through approved EDE entities to be considered an SBE-EDE; § 155.221(k)(2), which details the proposed requirement to provide an implementation plan and timeline; and § 155.221(k)(3), which proposed to require that a minimum of one EDE entity selected by the State meets minimum Federal requirements to participate in the FFE's EDE program and is capable of enrolling all consumers in the State in all available plan offerings, as well as meeting certain other requirements. We solicited comment on all aspects of the proposal, including any comments related to interest in pursuing this model among State Exchanges or other interested parties, expanding the option to other Exchange models, anticipated impacts to Exchange operating costs, and any other considerations or recommendations to effectively operationalize the SBE-EDE option. We also sought comment on the appropriate timing for making this option available to State Exchanges, specifically whether HHS should make this option available to State Exchanges for the PY 2028 annual open enrollment period (consistent with the 15-month Blueprint timeline referenced in this section) or delay implementation to PY 2029 (or later) to allow additional transition time for early adopters of the model.
For the same reasons we will not finalize the proposal discussed under section III.D.4.a. earlier in this preamble, we are not addressing finalization of this proposal in this final rule. We intend to consider finalizing this proposal, with or without modifications, in the 2028 Payment Notice rulemaking cycle or in another appropriate rulemaking vehicle in which we would address and respond to all comments received in response to the proposal.
We remind States that State Exchanges can still implement EDE programs regardless of whether we finalize these policies, subject to Federal requirements, including those at §§ 155.200 and 155.221. We remain available to provide technical assistance to State Exchanges interested in working with EDE partners to improve their operations and the experiences of consumers who engage with the Exchange.
5. Additional Required Benefits (§ 155.170)
In the 2027 Payment Notice proposed rule (91 FR 6332), we proposed to revise § 155.170(a) to provide that any State-required benefits would be considered “in addition to EHB” (and thus not an EHB) if they are: required by a State action taking place after December 31, 2011; applicable to the small group and/or individual markets; specific to required care, treatment, or services; and not required by State action for purposes of compliance with Federal requirements. Under this proposal, we stated that such State-required benefits would be considered in addition to EHB regardless of whether the mandated benefits are embedded in the State's EHB-benchmark plan. We proposed that this change would be effective beginning with PY 2027. We also proposed revisions to the regulatory text at §§ 155.170(a)(2) and 156.115(a) to align with this proposal and to have State and issuer responsibilities for State-required benefits appear in a more logical reading order in the CFR.
Section 1311(d)(3)(B) of the Affordable Care Act permits a State to require QHPs offered in the State to offer benefits in addition to the EHB, but requires the State to make payments, either to the individual enrollee or to the QHP issuer on behalf of the enrollee, to defray the cost of these additional State-required benefits.
In the 2013 EHB final rule (78 FR 12838), we finalized a standard at § 155.170(a)(2) that specified that State-required benefits enacted on or before December 31, 2011, even if not effective until a later date, are considered EHBs and therefore the costs of these benefits are not required to be defrayed by the State. The 2017 Payment Notice (81 FR 12242 through 12244) revised § 155.170(a)(2) to make clear that benefits required by State action taking place on or before December 31, 2011 are considered EHB, regardless of whether required benefits were established through legislative action, regulation, guidance, or other State action. We also amended § 155.170(a)(2) to provide that benefits required by State action taking place on or after January 1, 2012, other than for purposes of compliance with Federal requirements, are considered in addition to EHB.
Most recently in the 2025 Payment Notice (81 FR 26264 through 26268), we finalized that, beginning in PY 2025, covered benefits in a State's EHB-benchmark plan are considered an EHB under § 155.170(a)(2) and thus, do not require defrayal by the State. However, we noted that if at a future date the State updates its EHB-benchmark plan under § 156.111 and removes the mandated benefit from its EHB-benchmark plan, the State may have to defray the costs of the benefit under the factors set forth at § 155.170 as it will no longer be an EHB after its removal from the EHB-benchmark plan. Additionally, we noted that beginning in PY 2025, a State that is defraying the costs of a benefit required by a mandate that is in addition to the EHB under § 155.170 will be permitted to cease defraying the costs of that benefit if the benefit was included in its EHB-benchmark plan or upon updating its EHB-benchmark plan to include such benefit coverage. We further clarified that because any covered benefits in a State's EHB-benchmark plan are considered to be an EHB, such benefits are subject to the various rules applicable to EHB, including the prohibition on discrimination in accordance with § 156.125, the annual limitation on cost sharing in accordance with § 156.130, and restrictions on annual or lifetime dollar limits in accordance with § 147.126. We supported the revision to § 155.170(a)(2) finalized in the 2025 Payment Notice in part based on our understanding of States' struggle to understand and operationalize the policy that previously required States to
( printed page 29579)
defray the cost of State-required benefits, even if such benefits were included in the State's EHB-benchmark plan. We stated that finalization of this policy will promote consumer protections and facilitate compliance with the defrayal requirement by making the identification of benefits in addition to the EHB more intuitive.[113]
We have since reevaluated this position and in the proposed rule, stated that we believe we should not jeopardize the affordability of premiums, particularly for unsubsidized enrollees, for an intangible improvement to States' understanding of Federal defrayal requirements. We noted that when States enact benefit mandates, plan premiums must generally increase to account for the additional coverage. In the individual market (in which QHPs are sold), if State-required benefits are EHB, the associated premium increases will be entirely offset for consumers receiving APTC by higher APTC expenditures because the amount of APTC is tied directly to the premium amount. Over time, the accumulation of new State-required benefits that are EHB could substantially increase Federal APTC costs, undermining the purpose of the statutory defrayal policy. While premium increases associated with the accumulation of State-required benefits that are EHB will be offset for subsidized consumers, they are not offset for unsubsidized enrollees because they do not receive APTC. As a result, we stated in the proposed rule that we are concerned that the policy finalized in the 2025 Payment Notice that any covered benefits in a State's EHB-benchmark plan are considered EHB has an outsized impact on unsubsidized enrollees who do not receive APTC, which threatens to disincentivize enrollment amongst this population.
We stated in the proposed rule that our current policy incentivizes States to enact additional State-required benefits and then to select an EHB-benchmark plan under § 156.111 that includes such State-required benefits such that these benefits are considered to be EHB. We stated that this approach drives up premiums, which, in turn, increases Federal APTC expenditures, negatively impacts unsubsidized enrollees, and exacerbates low enrollment amongst this population.
Therefore, we proposed to revise § 155.170(a)(2) to revert to the standard that was in place prior to the 2025 Payment Notice, which required States to defray the cost of applicable State-required benefits at § 155.170(a)(1) taken by State action after December 31, 2011, even if such benefits are included in the State's EHB-benchmark plan beginning with PY 2027. Specifically, we proposed to revise § 155.170(a)(1) to provide that a State mandated benefit will be considered “in addition to EHB” (and thus not EHB) if it is: (i) required by a State action taking place after December 31, 2011; (ii) applicable to the small group and/or individual markets; (iii) specific to required care, treatment, or services; and (iv) not required by State action for purposes of compliance with Federal requirements.
We noted in the proposed rule that the proposed revisions at § 155.170(a)(1)(i) through (iv) would explicitly add into the regulatory text four conjunctive elements that determine when State-required benefits require defrayal. These four elements have long been included as part of a State's defrayal analysis but have not all been included in the regulatory text at § 155.170.[114]
We proposed to add them to § 155.170 to make explicit the specific circumstances that require State defrayal of benefits in addition to EHB. We proposed to revise § 155.170(a)(2) to state: “A State must make payments in accordance with paragraph (b) of this section to defray the cost of any State-required benefits in addition to the EHB.” We also proposed to revise and reorder the requirements for health plans to provide EHB at § 156.115(a) by adding at § 156.115(a)(2) the longstanding requirement that benefits required by State action taking place on or before December 31, 2011 are EHB that must be provided by health plans, and redesignating current paragraphs (a)(2) through (a)(6) as paragraphs (a)(3) through (a)(7). We emphasized in the proposed rule that, other than the proposed change to remove consideration of whether the benefits are included in the State's EHB-benchmark plan from the defrayal analysis, these proposed revisions are not intended to substantively change existing State and issuer responsibility for State-required benefits. We stated that these revisions are only intended to codify longstanding elements of the defrayal analysis, make conforming changes to the regulatory text, and to reorder these responsibilities so they would appear in a more logical reading order in the CFR. In particular, we proposed revisions to § 156.115(a) that would ensure the regulatory text captures all the instances in which a benefit provided in a health plan is an EHB, as this regulation does not reference § 155.170(a)(2).
We stated in the proposed rule that if finalized as proposed, a State would be required to defray the costs of any benefit that does not satisfy the proposed standard at § 155.170(a)(1) by making payments to individual enrollees or to the QHP issuer on behalf of enrollees. We stated that we expect this would better mitigate premium increases and better support unsubsidized enrollees because States would be required to defray the cost of a wider array of State-required benefits than under the existing policy, such that both subsidized and unsubsidized enrollees alike would be shielded from the increase to premiums resulting from State-required benefits.
We stated in the proposed rule that starting in PY 2027, a State that is not defraying the costs of a State-required benefit because of the policy finalized in the 2025 Payment Notice, which designated any benefit covered in the State's EHB-benchmark plan as EHB, would be required to begin defraying the costs of those benefits regardless of whether the benefit is included in its EHB-benchmark plan. We stated that if this proposal is finalized and a State begins defraying costs associated with a State-required benefit and making payments to QHP issuers because it is no longer considered EHB, QHP issuers would be required to update their plan filings accordingly beginning in PY 2027 to reflect that the benefit is no longer covered as an EHB and should not be included in the percentage of premium attributable to coverage of EHB for the purpose of calculating APTC. We clarified in the proposed rule that we would not require States with any such benefits in their EHB-benchmark plans to update their EHB-benchmark plan under § 156.111 to remove the benefit; the proposed revision to § 155.170 would simply render the benefit's inclusion in the
( printed page 29580)
EHB-benchmark plan null and void for purposes of defining the EHB in the State. We also clarified in the proposed rule that a State that wants to avoid defrayal obligations for State-required benefits that are already in the State's EHB-benchmark would be able to do so by repealing the applicable State requirement as being applicable to QHPs. If the State does not repeal or otherwise limit market applicability for the applicable State requirement, we stated that the State would be financially responsible for defraying the costs associated with the State benefit mandate. Given variation in State legislative calendars and session timing, and the need for issuers to update their plan filings and rates to account for benefits that would be defrayed by the State, we solicited comment on finalizing an effective date of PY 2028 instead of PY 2027.
In the proposed rule, we acknowledged that this proposal, a reversion to the standard that was in place prior to the 2025 Payment Notice, constitutes a change in policy for the treatment of State-required benefits under the Affordable Care Act. We stated that we understand that a small number of States and issuers have taken significant action based on current § 155.170, including that some States have sought or are seeking EHB-benchmark plan changes under § 156.111 to add certain State-required benefits as EHB based on the understanding that such EHB additions would be effective indefinitely absent any further EHB-benchmark plan changes under § 156.111 and that the cost of these additions would not require defrayal by the State. We stated that if finalized, any State-required benefit that fulfills the four proposed conjunctive elements at proposed § 155.170(a)(1)(i) through (iv) would require defrayal, regardless of whether the benefit is included in the State's EHB-benchmark plan.[115]
In turn, we stated in the proposed rule that State-required benefits that are in addition to EHB under this proposed policy would not be subject to the rules applicable to EHB, including the prohibition on discrimination in accordance with § 156.125, limitations on cost sharing in accordance with § 156.130, and restrictions on annual or lifetime dollar limits in accordance with § 147.126. We stated that although we do not take these impacts lightly, these changes are necessary to return to the longstanding read of section 1311(d)(3)(B) of the Affordable Care Act and better balance the cost of the EHB for unsubsidized enrollees. We established our longstanding read of section 1311(d)(3)(B) of the Affordable Care Act in the EHB Rule (78 FR 12838) when we finalized that State-required benefits enacted after December 31, 2011, are not considered EHBs and therefore the costs of these benefits are required to be defrayed by the State. We stated that we believe reverting to this foundational read is warranted to remove the incentive from States to enact more benefit mandates that could in turn increase premiums and negatively impact unsubsidized enrollees to the detriment of overall enrollment by this population. The defrayal requirement in section 1311(d)(3)(B) of the Affordable Care Act prevents States from shifting costs to the Federal government through increased Federal expenditures. Over time, the accumulation of new State-required benefits being treated as EHB (without corresponding defrayal by States) could increase Federal outlays and undermine the purpose of section 1311(d)(3)(B) of the Affordable Care Act. While the availability of such benefits as EHB (with the associated protections) is a consideration, so is the overall affordability of coverage and the impact on overall enrollment. If such coverage is so expensive that it is unaffordable, particularly for unsubsidized enrollees, then the entire market suffers and those that cannot afford to enroll do not enjoy any benefits of coverage whatsoever. Our proposal sought to mitigate that risk.
We stated in the proposed rule that we are aware that this proposed policy reversal, if finalized, could also impact health plans that are not directly impacted by EHB requirements. This includes self-insured group health plans and large-group market fully insured plans that must follow the annual and lifetime dollar-limit restrictions on EHB and annual cost-sharing limitation requirements under §§ 147.126 and 156.130.[116]
We stated that this proposal, if finalized, would affect plan sponsors to the extent that a plan sponsor selects a certain State's EHB-benchmark plan for purposes of complying with sections 2707 and 2711 of the PHS Act and that State changes benefits in its EHB-benchmark plan.[117]
We stated that the proposal's impact would also extend beyond these plan sponsors to include BHPs established under Affordable Care Act section 1331 and Medicaid Alternative Benefit Plans (ABPs) implemented under section 1937.
Finally, we noted in the proposed rule that we are aware of State legislation that includes clauses stating that the requirement to defray the costs associated with State-required benefits is precluded if HHS fails to respond to the State's request for confirmation of whether new mandates require defrayal within a certain time. Such provisions are inconsistent with § 155.170, as they inappropriately put the onus on HHS to decide whether the State-required benefit is in addition to EHB. Failure by HHS to respond to a State's request for a determination of whether new mandates require defrayal by the State does not relieve a State from its defrayal obligation. Under § 155.170, it is the State's responsibility to identify which State-required benefits require defrayal. While States are encouraged to reach out to us concerning State defrayal questions in advance of passing and implementing benefit mandates, HHS does not provide determinations of whether the cost of a State-required benefit requires defrayal by the States.
In summary, we proposed to revise § 155.170(a) to provide that any State-required benefits would be considered “in addition to EHB” (and thus not EHB) if they are: required by a State action taking place after December 31, 2011; applicable to the small group and/or individual markets; specific to required care, treatment, or services; and not required by State action for purposes of compliance with Federal requirements. We also proposed revisions to the regulatory text at §§ 155.170(a)(2) and 156.115(a) to align with this proposal and to have State and issuer responsibilities for State-required benefits appear in a more logical reading order in the CFR. We proposed that these changes would be effective beginning in PY 2027.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our
( printed page 29581)
responses to comments, we are finalizing this policy with a modification to delay the effective date to PY 2028. Accordingly, we are finalizing at § 155.170(a)(1) the defrayal policy that is in place for plan years beginning before January 1, 2028. At § 155.170(a)(2)(i) through (iv), we are finalizing the defrayal policy that will be in place for plan years beginning on or after January 1, 2028. At § 155.170(a)(3), we are finalizing the requirement that was proposed at § 155.170(a)(2), which provides that a State must make payments to defray the cost of any State-required benefits in addition to EHB. We are also finalizing § 156.115(a) as proposed to align with the amendments to § 155.170 and to present State and issuer responsibilities for State-required benefits in a more logical sequence within the CFR.
We summarize and respond to public comments received on the proposed State mandate defrayal policy at § 155.170 below.
Comment:
Multiple commenters who supported the proposal stated it clarified State defrayal requirements for benefits that exceed EHB. Commenters supporting the proposal generally agreed that States should bear the cost of newly mandated benefits rather than shifting those costs to consumers through higher premiums or to the Federal Government through increased expenditures. Commenters supporting the proposal expressed concern that, under current policy, States were permitted to incorporate post-2011 mandates into EHB-benchmark plans without defrayal, including by selecting EHB-benchmark plans that already reflect those mandates, thereby circumventing the applicable statutory requirements. These commenters stated that this practice undermines the EHB framework established under section 1311(d)(3)(B) of the Affordable Care Act and weakens fiscal accountability.
Commenters supporting the proposal also highlighted that State benefit mandates can increase premiums, specifically for unsubsidized enrollees who bear the full cost of those increases because they do not receive APTC. These commenters noted that the proposal would help curb this premium growth, improve affordability for unsubsidized individuals, and ensure that Federal subsidies are limited to EHB rather than State mandated benefits.
Response:
We appreciate commenters' support for this proposal. We agree with these commenters and with their assertion that this proposal will better promote premium affordability, particularly for unsubsidized enrollees. We further agree with commenters noting that the policy finalized in the 2025 Payment Notice undermines the EHB framework established under section 1311(d)(3)(B) of the Affordable Care Act and weakens fiscal accountability. As stated in the proposed rule, enactment of State benefit mandates generally increases plan premiums to account for the additional coverage. Section 1311(d)(3)(B) of the Affordable Care Act addresses this by permitting a State to require QHPs offered in the State to offer benefits in addition to the EHB, but requires the State to make payments, either to the individual enrollee or to the QHP issuer on behalf of the enrollee, to defray the cost of these additional State-required benefits. This defrayal requirement prevents States from shifting costs of State benefit mandates to the Federal Government through Federal expenditures. However, the policy finalized in the 2025 Payment Notice undermines this Affordable Care Act protection by allowing more State benefit mandates to be considered EHB. Although any associated premium increases of these benefit mandates that are EHB under the 2025 Payment Notice policy may be entirely offset for consumers receiving APTC, they are not offset for unsubsidized enrollees because these enrollees do not receive APTC.
Comment:
Many commenters who opposed the proposal urged HHS to retain the existing policy finalized in the 2025 Payment Notice, stating that the existing policy improved clarity and consistency in identifying benefits in addition to EHB and reduced administrative complexity associated with defrayal determinations. These commenters stated that the existing policy preserves the appropriate balance between Federal defrayal standards and State flexibility and allows States to better address local health priorities. These commenters also noted that the existing policy resolved prior inconsistencies in which benefits could be treated as both EHB and “in addition to EHB” for defrayal purposes, an inconsistency that commenters stated this proposal would revive if finalized.
Response:
We are not persuaded that the perceived improvement in clarity and reduced administrative complexity offered by the policy finalized in the 2025 Payment Notice is worth the risk it poses to premium affordability and Federal APTC expenditures. We acknowledge that though the policy finalized in the 2025 Payment Notice may have been a preferred process for States in identifying benefits in addition to EHB, the implementation of the policy finalized in the 2025 Payment Notice was at the cost of potentially increasing future Federal outlays by allowing States to avoid Federal obligations by incorporating State-required benefits into their EHB-benchmark plans. The policy we are finalizing aligns with section 1311(d)(3)(B)(ii)(II) of the Affordable Care Act by ensuring that State-required benefits meeting the four conjunctive elements at § 155.170(a)(2)(i) through (iv) require defrayal regardless of whether they are included in the State's EHB-benchmark plan. We believe this reading of the statute is correct and that the improved clarity and reduced administrative complexity associated with the policy finalized in the 2025 Payment Notice does not justify the potential resulting increases in premiums, which would lead to higher APTC outlays and disproportionately burden unsubsidized enrollees in the individual market. Further, we note that States may continue to make determinations on which benefits would be beneficial to enrollees in addressing local health priorities, so long as States adhere to the requirement to defray the costs associated with benefits that would be deemed in addition to EHB under § 155.170(a)(2).
We acknowledge that the policy finalized in the 2025 Payment Notice did resolve the prior classification overlap by providing that a State-mandated benefit incorporated into a State's EHB-benchmark plan would be treated as EHB and therefore not subject to defrayal. However, we do not agree that the 2025 Payment Notice policy was consistent with the underlying statute. Section 1311(d)(3)(B)(ii)(II) of the Affordable Care Act operates independently from the EHB framework at section 1302(b) of the Affordable Care Act. Allowing States to undermine a statutory defrayal obligation through State EHB-benchmark plan design choices conflates the classification of a benefit for EHB purposes with the separate question of whether that benefit triggers defrayal. The four conjunctive elements we are finalizing at § 155.170(a)(2)(i) through (iv) restore the best reading of section 1311(d)(3)(B)(ii)(II) of the Affordable Care Act by ensuring a clear standard for when a benefit requires defrayal, independent from the State's EHB-benchmark plan.
Comment:
Numerous opposing commenters noted that the proposal is a complete reversal of the policy finalized in the 2025 Payment Notice and that States that bolstered certain benefit offerings for their enrollees would be forced to make difficult
( printed page 29582)
financial decisions, which would place certain benefits at risk. Many commenters opposing the proposal stated concern about consumer harm and confusion. These commenters stated that the proposed policy would discourage States from adopting innovative benefit mandates, undermine existing coverage relied upon by consumers, and penalize States for expanding access to services. Many commenters noted that the current policy enabled States to better address specific health needs. These commenters stated concern that by broadening which State mandated benefits require defrayal, the proposal would lead to States repealing mandated benefits, thereby weakening consumer access to valuable coverage. These commenters cited many specific areas of coverage that they claim could be impacted by this proposal, including the opioid crisis, fertility services, biomarker testing, diabetes coverage, cancer benefits, nutrition, chronic conditions, mental health and substance use disorder treatment, and preventive care.
Response:
We do not agree with the commenter's assertions regarding areas of care that would be impacted, as many are already required to be covered as EHBs. For example, issuers subject to EHB requirements must cover benefits within the categories of mental health and substance use disorder services as well as preventive and wellness services and chronic disease management. We also do not believe that this policy limits States' ability to address State-specific health priorities. States may continue to require coverage of additional benefits beyond EHB in the specific areas of coverage that commenters raised. This policy clarifies that States are responsible for defraying the cost of those additional benefits when they meet the definition we are finalizing at § 155.170. We therefore do not agree that finalizing this policy will impact coverage of the benefit areas mentioned by commenters, such as the opioid crisis, fertility services, biomarker testing, diabetes coverage, cancer benefits, nutrition, chronic conditions, mental health and substance use disorder treatment, and preventive care.
We also do not believe the policy will contribute to consumer confusion or potential consumer harm. The finalized policy does not eliminate or restrict any benefit that States choose to mandate. To the extent States choose to repeal or adjust existing State-required benefits, States will have until PY 2028 to communicate with affected consumers and issuers regarding any changes to how those benefits are classified. As discussed in further detail below, we are finalizing this delayed effective date to better support a smooth transition that minimizes disruption to consumers and States. We also anticipate that States choosing to repeal applicable mandates will most likely do so in circumstances where the benefit is otherwise already covered as EHB under the State's existing EHB-benchmark plan. In such cases, the repeal of the State mandate would not result in any loss of coverage for consumers, as the benefit would continue to be provided as EHB under the State's EHB-benchmark plan.
However, we agree with commenters that Federal defrayal policy can influence State decisions to adopt benefit mandates. To the extent commenters are concerned that the proposal may reduce incentives for States to enact new mandates, we note that this is an intended effect. The existing policy
creates
an incentive for States to adopt additional State-required benefits, and the change we are finalizing is designed to address that dynamic. The existing policy also incentivizes States to select an EHB-benchmark plan under § 156.111 that includes such State-required benefits so that those benefits are considered EHB. We believe this approach drives up premiums, which in turn increases Federal APTC expenditures, negatively impacts unsubsidized enrollees, and exacerbates low enrollment amongst this population.
We believe these outcomes outweigh the concerns raised by commenters. When State-required benefits are classified as EHB so long as they are in the State's EHB-benchmark plan, the associated premium increases are offset for subsidized consumers through higher APTC but are not offset for unsubsidized enrollees who bear the full cost of those increases. Over time, the accumulation of State-required benefits treated as EHB could substantially increase Federal APTC expenditures and threaten the affordability of coverage in the individual market, particularly for unsubsidized enrollees who do not receive APTC. If coverage becomes so expensive that it is unaffordable for this population, those consumers may exit the market entirely, forgoing any benefits of coverage whatsoever. The policy we are finalizing is designed to address this dynamic by ensuring that the costs of State-required benefits in addition to EHB are defrayed by States, consistent with the statutory defrayal requirement in section 1311(d)(3)(B) of the Affordable Care Act, rather than passed on to consumers through higher premiums or to the Federal Government through increased APTC outlays.
Moreover, we note that the policy we are finalizing neither prohibits States from mandating benefits nor weakens consumers' access to valuable coverage. States retain the authority to mandate benefits that address the health needs of their consumers so long as the State defrays any such benefits in addition to EHB. The defrayal framework determines only who bears the cost of those benefits, not whether States may require them.
Comment:
Numerous commenters opposing the proposal noted concern that benefits newly classified as in addition to EHB under this proposal (but that would have been EHB under the existing policy) would lose core consumer protections, including nondiscrimination requirements, cost-sharing limits, and prohibitions on annual or lifetime dollar limit caps. Many of these commenters noted concerns that excluding such benefits from cost-sharing protections could increase out-of-pocket costs for consumers and could result in delayed or forgone care, particularly for individuals with serious or chronic conditions. Some commenters stated concern that, by reducing the scope of EHB in this way, this policy could decrease the amount of financial assistance available to Exchange enrollees and negatively impact enrollment. Commenters further stated that the proposal could erode the comprehensiveness of coverage, weaken consumer protections tied to EHB, and make coverage less affordable. Other commenters acknowledged concerns about affordability and premium impacts under the current policy but cautioned that the proposed approach could instead shift costs to States and consumers.
Response:
We acknowledge that, under this policy, certain benefits may no longer be treated as EHB for purposes of the defrayal framework and therefore may not be subject to the consumer protections identified. We note that States may repeal State-required benefits and, if the benefit remains included in the State's EHB-benchmark plan, it will continue to be treated as EHB and subject to applicable consumer protections. In response to commenters stating that the proposed policy could increase out-of-pocket costs for consumers and result in delayed or forgone care, particularly for individuals with serious or chronic conditions, we note that the policy does not prohibit States from making benefit determinations that would provide comprehensive coverage or that require
( printed page 29583)
zero cost-sharing for enrollees with various conditions. States will still be able to make determinations on which benefits would be beneficial for the consumers in their respective States.
For commenters' concerns that this policy could reduce financial assistance available to Exchange enrollees, we note that the policy we are finalizing is designed to achieve the opposite effect. When costs of State-mandated benefits are reflected in premiums, as the policy in the 2025 Payment Notice permitted when a State-mandated benefit was also in the State's EHB-benchmark plan, those higher premiums increase APTC and Federal outlays. For unsubsidized enrollees, this risked directly increasing out-of-pocket premium costs. The policy we are finalizing at § 155.170(a)(2) better helps to moderate premiums and supports the affordability of coverage for subsidized and unsubsidized enrollees alike.
We also do not agree that this policy shifts costs to consumers. To the contrary, the defrayal requirement itself is in part a consumer protection mechanism in that the enrollee is spared the cost in their premiums of State-mandated benefit in addition to EHB that the State defrays. The policy we are finalizing ensures that when a State mandates a benefit that satisfies the four conjunctive elements at § 155.170(a)(2)(i) through (iv), those costs will not be passed through to consumers in the form of higher premiums. This policy ensures that the party responsible for mandating the benefit (the State) is also responsible for defraying its costs.
Comment:
Several commenters noted that States relied on the policy finalized in the 2025 Payment Notice to add benefits as EHB expecting they would not trigger defrayal obligations. Many commenters stated that they opposed the proposal because it would unsettle State reliance interests and impose significant financial and operational burden on States, particularly for those that have already updated their EHB-benchmark plans to add certain State-required benefits as EHB. These commenters stated the proposal could require States to revisit or undo prior policy decisions, resulting in additional costs and operational challenges.
Response:
We acknowledge commenters' concerns that this policy may impose administrative and financial burdens on States, particularly for those States that have already updated their EHB-benchmark plans to add certain State-required benefits as EHB. However, we note the defrayal requirements at § 155.170 previously required States to operationalize their defrayal responsibilities, including developing payment methodologies and conducting actuarial analyses to determine the cost of State-required benefits in addition to EHB. As such, administrative and financial considerations associated with defrayal are not new requirements introduced by this policy. We also understand that a small number of States and issuers have taken action based on current § 155.170, including that some States have sought or are seeking EHB-benchmark plan changes under § 156.111. While some States may need to revisit prior analyses or approaches, we believe that this change is necessary to align State practices with a defrayal framework that better protects premiums and Federal expenditures. As finalized, any State-required benefit that fulfills the four conjunctive elements at § 155.170(a)(2)(i) through (iv) would require defrayal, regardless of whether the benefit is included in the State's EHB-benchmark plan. We acknowledge this is a reversal from the policy finalized in the 2025 Payment Notice. However, we believe that finalizing this proposal aligns with the original intent of the defrayal policy at section 1311(d)(3)(B) of the Affordable Care Act, which prevents States from shifting costs to the Federal government through Federal APTC expenditures.
Comment:
Commenters broadly recommended delaying the effective date of the proposed policy until at least PY 2028. These commenters stated that States need time to assess which benefits would now require defrayal and subsequently coordinate these changes with CMS, issuers, and State Legislatures. The commenters noted that the proposed effective date of PY 2027 would not allow sufficient time to overcome these operational hurdles. Most notably, commenters noted that State legislative calendars and budget processes require additional time to allow for States to consider legislative or regulatory changes and to secure appropriations for defrayal, if necessary. While many commenters supported delaying the effective date of this proposal until PY 2028, some commenters recommended an effective date of PY 2029 or PY 2030 to better align with State legislative cycles, State regulatory processes, and any forthcoming changes to the EHB-benchmark plan update process.
Response:
We acknowledge that States may require more time to operationalize their defrayal obligations under this policy, as finalized, to ensure they have sufficient time to collaborate with issuers, legislative bodies, other respective interested parties, and engage in the fiscal planning involved in the defrayal process. We also acknowledge that providing States enough time to plan for and effectuate the new defrayal requirements is necessary. To assist States in operationalizing their defrayal obligations and ensure they have sufficient time to comply with the new defrayal requirements, we are finalizing an effective date of PY 2028 for this policy. To reflect this delayed effective date, we are finalizing § 155.170 such that § 155.170(a)(1) reflects the policy in place for plan years beginning before January 1, 2028, and § 155.170(a)(2)(i) through (iv) reflects the policy that will be in place for plan years beginning on or after January 1, 2028. We are finalizing § 156.115(a) as proposed to align with this rulemaking and to present State and issuer responsibilities for State-required benefits in a more logical sequence within the CFR. Since this revision is organizational in nature and does not alter the substance of existing or new policy, we are not finalizing a delayed effective date with respect to this provision.
Comment:
Some commenters stated concern that the proposal would apply new defrayal obligations to past State actions taken under prior regulatory frameworks and requested HHS provide a clearer transition framework to avoid retroactive impacts and ensure States have clear notice when adopting future benefit mandates. Several commenters requested that HHS modify the proposed policy in a manner that would not require States to take additional legislative or regulatory action to avoid defrayal for their current EHB-benchmark plan selections. For example, some commenters suggested finalizing modifications to the proposed policy so that it would only apply prospectively, such that benefits mandated by State action from 2012-2027 would not require defrayal if they were considered EHB under the policy finalized in the 2025 Payment Notice. In addition, some commenters supported establishing a safe harbor for fertility treatment mandates, either broadly or limited to States that have already incorporated such benefits into their EHB-benchmark plans, citing advances in medical care and alignment with Federal priorities for this coverage. Other commenters requested that we clarify that benefits added to EHB-benchmark plans to comply with the Mental Health Parity and Addiction Equity Act (MHPAEA) and its implementing regulations do not require defrayal. Finally, some commenters recommended limiting defrayal requirements to State mandates enacted
( printed page 29584)
after the effective date of this final rule and holding States harmless for benefits included in EHB-benchmark plans prior to the effective date of the final rule to address retroactivity concerns.
Response:
We agree that States would benefit from a transition framework that ensures States have clear notice of EHB defrayal requirements when considering which benefits the State will mandate. In response to comments, we are finalizing a modified effective date such that this policy will be effective beginning with PY 2028. We believe this delayed effective date will provide States with adequate notice and time to adopt or revise their benefit mandates in light of this policy change.
In addition, though States relied on the current EHB defrayal policy, we have taken steps to mitigate that reliance. Specifically, we announced in the 2027 Payment Notice proposed rule (91 FR 6368) that we were pausing review of EHB-benchmark plan applications because we are actively conducting a comprehensive review of section 1302 of the Affordable Care Act and considering future rulemaking to revise § 156.111 and other regulations relating to the EHBs. Our notice related to pausing review of EHB-benchmark plan applications in the 2027 Payment Notice proposed rule prevented States from making further updates to their EHB-benchmark plans that would increase reliance on the policy finalized in the 2025 Payment Notice. Any State reliance on the 2025 Payment Notice defrayal policy will also be mitigated by the delayed PY 2028 implementation date of the policy finalized in this final rule. Further, we note that State reliance on the current policy, as is evidenced by State efforts to update EHB-benchmark plans to incorporate State-required benefits, supports the rationale for returning to the longstanding interpretation of section 1311(d)(3)(B) of the Affordable Care Act through the policy we are finalizing. This pattern of State behavior confirms that the 2025 Payment Notice policy created incentives for States to shift the costs of State-required benefits to the Federal government through increased high premiums and increased APTC expenditures. We encourage States to use the period prior to PY 2028 to assess their State-required benefits, identify those that require defrayal under the policy we are finalizing in this final rule, and take any necessary steps to comply with the defrayal framework beginning with PY 2028.
We decline to establish safe harbors or exemptions for specific State-required benefits, exemptions for State-mandated benefits enacted prior to the adoption of the policy in this final rule, or further limits on the scope of this policy. First, we continue to be of the view that a State's ability to avoid defrayal obligations under section 1311(d)(3)(B)(ii)(II) of the Affordable Care Act simply by incorporating a State-required benefit into its EHB-benchmark plan is not consistent with the statutory design, which treats the defrayal determination as a distinct inquiry from the classification of a benefit as EHB. Second, we do not believe these suggested alternatives are necessary when States can take action before PY 2028 to retain specific benefits as EHB in the State's EHB-benchmark plan consistent with section 1302 of the Affordable Care Act (that is, by repealing the State mandate for the benefit or choosing to defray the cost of additional required benefits). We believe States will have adequate time to make any necessary adjustments consistent with their defrayal policy preferences.
Moreover, in response to the comment suggesting a safe harbor for specific services like fertility treatments, we note that the current EHB-benchmark framework utilizes a State-based approach whereby States determine which benefits should be included as EHB. Providing a Federal safe harbor from the defrayal requirement for any specific subset of benefits that do not meet the typicality standard would be at odds with that framework.
Further, we acknowledge comments regarding compliance with MHPAEA. Plans that are required to provide EHBs must cover mental health and substance use disorder services, including behavioral health treatment, as required categories of EHB and must comply with MHPAEA.[118]
We note that under § 155.170(a)(2)(iv), State action taken for purposes of compliance with Federal requirements, which includes MHPAEA, is not considered to be in addition to EHB and will not require defrayal by the State.[119]
Comment:
One commenter requested that HHS withdraw the proposal and stated that finalization of this proposal would create operational and fiscal disruption for States and violate State sovereignty. This commenter stated the policy would interfere with the States' legislative authority by forcing States to repeal existing laws to avoid defrayal obligations. The commenter characterized the proposed policy as inconsistent with principles of State flexibility and autonomy, noting that conditioning defrayal on legislative or regulatory changes could undermine State policymaking processes. Some commenters noted concern that the proposed policy would create uncertainty for States and issuers, undermining their ability to engage in long-term fiscal and operational planning.
Other commenters noted that States are best positioned to determine appropriate benefits for their populations and expressed concern that changes to the Federal defrayal policy could limit States' ability to reflect State-specific needs. One commenter noted their belief that HHS lacks statutory authority to support the proposed policy because in their view, section 1311 of the Affordable Care Act authorizes defrayal for benefits that are in addition to EHB, but it does not authorize HHS to redefine EHB based on the timing of enactment for State-required benefits. Other commenters noted that Congress delegated to the Secretary of HHS the responsibility to define EHB through a stable, employer-based framework designed to promote uniformity, predictability, and nondiscrimination, while preserving State flexibility through EHB-benchmark plan selection, and that the proposed policy undermines the statutory framework for EHB.
Response:
We do not agree that the policy as proposed would be unduly disruptive and that it would intrude on State authority or policymaking processes. The policy we are finalizing does not require States to repeal any existing laws. Rather, consistent with section 1311(d)(3)(B) of the Affordable Care Act and § 155.170, States retain the flexibility to determine whether to maintain State-required benefits that are in addition to EHB and defray the associated costs, or to modify or repeal such requirements. This framework reflects the longstanding statutory requirement that States must defray the cost of benefits in addition to EHB. The final policy preserves State flexibility by allowing States to make policy decisions regarding benefit mandates while ensuring that Federal funds are used consistently with statutory intent and limits. Further, in response to the comments noting that changes to the defrayal policy limits States' ability to reflect State-specific needs, we do not agree with these comments. States may require coverage of benefits that are in addition to EHB; however, States must comply with the defrayal requirements at § 155.170 for such benefits. The
( printed page 29585)
defrayal framework we are finalizing does not constrain what benefits States may require. Rather, it determines who bears the cost of those benefits, thereby preserving States' ability to tailor benefits to the health needs of their populations while ensuring that the associated costs are defrayed by the State rather than passed on to consumers through higher premiums or to the Federal government through increased APTC outlays. Further, we do not agree that the proposed policy or the policy we are finalizing would create uncertainty for States and issuers or undermine their ability to engage in long-term fiscal and operational planning. States that mandate benefits subject to defrayal obligations under § 155.170 are already required to engage in ongoing internal and external operational and fiscal planning, including coordinating with issuers, to ensure they are appropriately effectuating defrayal obligations. Because States are already familiar with the planning processes that defrayal obligations entail, and because the responsibility for meeting those obligations rests with the States under § 155.170, we disagree that the finalized policy would create the level of uncertainty noted by the commenters.
In addition, we do not believe this policy change undermines the statutory framework for EHB. Section 1302(b)(1) of the Affordable Care Act grants the Secretary broad authority to define EHB. Under this authority, we have identified the items and services within the ten EHB categories by relying on State-specific EHB benchmark plans under § 156.111. The defrayal requirement in section 1311(d)(3)(B) of the Affordable Care Act is a distinct statutory provision that operates alongside the Secretary's definition of EHB. The change we are finalizing returns the defrayal framework to its longstanding interpretation prior to the 2025 Payment Notice, under which the scope of EHB in each State continues to be defined by the State's EHB-benchmark plan, while ensuring that the costs of State-required benefits in addition to EHB are defrayed by States. Sections 1302(b)(1) and 1311(d)(3)(B) of the Affordable Care Act are complementary, not competing, statutory directives, and finalizing this policy gives full effect to both.
Comment:
Some commenters stated their belief that HHS' rationale for the proposed policy is unsubstantiated and does not adequately note how the interpretation of section 1311(d)(3)(B) of the Affordable Care Act set forth in the 2025 Payment Notice was inferior to the interpretation of this section underlying this proposal. Some commenters noted that the proposed rule did not demonstrate meaningful changes in State behavior since finalization of the 2025 Payment Notice to support the proposed policy change. Other commenters noted that affordability is far more complex than solely premiums and stated that ensuring benefit coverage and reasonable cost-sharing are substantial components to overall out-of-pocket affordability.
Several commenters also noted that States act judiciously when adopting benefit mandates, emphasizing that such decisions are infrequent, carefully evaluated, and informed by actuarial and regulatory analysis. Some of these commenters noted that States assess the cost and impact of proposed benefit mandates, often relying on State insurance regulators and Federal statutory requirements, including limits on changes to EHB-benchmark plans (such as actuarial value constraints), to ensure minimal effects on premiums.
Commenters further stated that the proposal would not materially change States' ability to add benefits to EHB-benchmark plans under existing EHB-benchmark requirements and, therefore, would not actually address concerns about premium growth. Some commenters stated that EHB-benchmark plan requirements already limit benefit expansion and associated premium increases, and that State benefit mandates are not a primary driver of rising premiums. Others noted that it is too soon to assess the impact of the policy finalized in the 2025 Payment Notice on premiums or Federal spending.
Response:
We do not agree with commenters' allegation that our rationale for this proposed policy is unsubstantiated. Section 1311(d)(3)(B) of the Affordable Care Act provides that, if a State requires a health plan to cover benefits in addition to the EHB, the State shall defray the cost of those additional benefits. This contemplates a distinction between benefits that are EHB and benefits that are in addition to EHB, placing the cost of the latter on the State. We also do not agree that EHB-benchmark plan requirements already sufficiently limit benefit expansion and associated premium increases such that the defrayal framework we are finalizing is unnecessary. The EHB-benchmark plan requirements at § 156.111 do impose constraints on benefit design, including a ceiling on the overall scope of benefits included in the State's EHB-benchmark plan. However, those constraints do not address the cost consequences that arise when a State incorporates State-mandated benefits into their EHB-benchmark plans under the framework established by the 2025 Payment Notice. The interpretation finalized in the 2025 Payment Notice whereby any benefit included in a State's EHB-benchmark plan is automatically considered EHB, effectively allowed States to ignore the distinction between benefits that are EHB and benefits that are in addition to EHB by incorporating State-required benefits into their EHB-benchmark plans. As we stated in the proposed rule, the policy finalized in the 2025 Payment Notice incentivizes accumulation of new State-required benefits as EHB, which increases Federal APTC costs and undermines the purpose of the statutory defrayal policy. The increase in APTC causes premium increases and presents an affordability issue for all enrollees, especially unsubsidized enrollees. To mitigate this risk, we believe that the proposed policy addresses these concerns such that both subsidized and unsubsidized enrollees alike would be shielded from the increase to premiums resulting from State-required benefits. We believe it appropriate to address these concerns proactively.
We do not agree with commenters that stated it is too soon to assess the impact of the policy finalized in the 2025 Payment Notice on premiums or Federal spending. We have observed that a number of States have sought to update their EHB-benchmark plans since finalization of the policy in the 2025 Payment Notice in part to incorporate State-required benefits that would otherwise be subject to defrayal. This pattern of State behavior demonstrates that the 2025 Payment Notice policy did, in fact, influence State decision making regarding EHB-benchmark plan updates and has implications for premium growth. Under the policy finalized in the 2025 Payment Notice, States could incorporate State-required benefits into their EHB-benchmark plans and thereby avoid defrayal obligations entirely, which could effectively shift the cost of those State-required benefits to consumers through higher premiums and to the Federal Government through increased APTC outlays.
We acknowledge commenters' views that affordability is multifaceted and includes factors beyond premiums, such as benefit coverage and cost-sharing. However, premiums remain a primary driver of affordability for many consumers, particularly unsubsidized enrollees, and increases in premiums may also affect Federal spending on APTCs. We also acknowledge commenters' statements that States act judiciously when adopting benefit
( printed page 29586)
mandates and consider cost impacts but believe this policy change is appropriate for the reasons provided in the proposed rule and in this final rule regardless of the frequency or intent of such State actions. Even where individual States carefully weigh the cost implications of benefit mandates, the cumulative effect of State-required benefits being classified as EHB through State EHB-benchmark plan selection, as the 2025 Payment Notice policy allowed, could pose a systemic risk over time to premium affordability and Federal APTC expenditures. Reverting to the pre-2025 Payment Notice standard restores the integrity of the statutory defrayal requirement by ensuring that the costs of State-required benefits in addition to EHB are borne by States and not passed on to consumers through higher premiums or to the Federal government through increased APTC outlays. Regardless of individual State fiscal prudence, the defrayal policy must be designed to align with the statute and to function appropriately across all States.
Comment:
Several commenters stated concern that HHS' pause on reviewing State applications to update EHB-benchmark plans, when combined with the proposed changes to the defrayal policy, effectively forces States to choose between defraying new mandates or repealing them, without the ability to add those benefits as EHB through the EHB-benchmark plan update process. One commenter noted that offering States flexibility to remove State-mandated benefits without being able to change their EHB-benchmark plans impinges on States' decision-making and could reduce the actuarial value of EHB provided, potentially below minimum required generosity levels of the EHB package.
One commenter noted that if benefits enacted after December 31, 2011, are reclassified as non-EHB while HHS has paused review of State applications for EHB-benchmark plan updates, some States could temporarily retain EHB-benchmark plans that include benefits no longer treated as EHB for Federal purposes. This commenter stated concern that, in this situation, States could face defrayal obligations for benefits embedded in their EHB-benchmark plans that they are unable to modify during the pause on EHB-benchmark plan updates.
Response:
As stated in the proposed rule, we are pausing review of State applications to select EHB-benchmark plans in accordance with § 156.111. We are actively reviewing the statutory and regulatory framework governing EHB, including the EHB-benchmark plan selection and update process, to assess whether additional changes may be appropriate. We recognize that, under these circumstances, States may face tradeoffs in determining whether to defray the cost of such benefits or repeal existing requirements. We emphasize that if a State repeals the underlying State action that requires a benefit, that benefit would no longer be considered a State-required benefit for purposes of § 155.170, and the State would not be required to defray its cost even if that benefit remains in the State's EHB-benchmark plan.
We do not agree that this policy risks reducing the actuarial value of EHB or reducing EHB below required minimum generosity standards. Actuarial value is determined at the plan level under the applicable AV standards, while the scope of EHB is defined by the State's EHB-benchmark plan. To the extent a State repeals a State-mandated benefit but does not modify its EHB-benchmark plan, the benefit remains EHB, and the repeal would not affect a plan's actuarial value.
As discussed above, we are finalizing a delayed effective date for the change to the defrayal policy of PY 2028. We believe this delayed effective date and resulting transition period will provide States with sufficient time to adapt to the revised defrayal policy and sufficient time for us to consider any future updates to the EHB framework that may result from this ongoing review.
Comment:
Several commenters stated concern that the proposed policy creates ambiguity regarding whether benefits added or modified through the EHB-benchmark plan selection process at § 156.111 would be subject to defrayal. Other commenters requested that HHS clarify whether a State should repeal a benefit mandate that has already been made EHB through the State's EHB-benchmark plan to avoid defrayal obligations.
One commenter noted that prior HHS guidance distinguished between State-required benefits enacted through separate legislative or regulatory action and those incorporated through the State EHB-benchmark process at § 156.111 and urged HHS to codify this distinction in regulation. This commenter and several other commenters stated that the proposal does not clearly define what constitutes “State action,” making it difficult to determine when updated or expanded benefits would trigger defrayal, particularly given the variety of approaches States have used to update their EHB-benchmark plans. One commenter provided examples from multiple States to illustrate this uncertainty and requested additional clarity to ensure States can continue to update benefits to address local health needs without triggering unintended defrayal obligations.
One commenter requested that HHS collaborate with States to provide clear guidance and technical support on when State benefit mandates require defrayal. Another commenter noted that States vary in their level of engagement with the defrayal process. This commenter noted that some States assess mandate costs or recognize defrayal obligations, but few have a formal defrayal reimbursement process in place. Due to this variation, the commenter noted that HHS should provide a comprehensive document that provides substantive guidance for States in operationalizing their defrayal obligations under the proposed policy.
Response:
Under the policy we are finalizing at § 155.170, a State's obligation to defray is not triggered by the selection or update of its EHB-benchmark plan. This has always been true of the defrayal framework since it was first established in the EHB Final Rule (78 FR 12838). Rather, the obligation arises from the existence of a State-required benefit that is external to the EHB-benchmark plan and considered “in addition to EHB” under § 155.170(a)(2), including where such a requirement duplicates benefits included in the EHB-benchmark plan. We believe the regulatory text as finalized at § 155.170, together with this preamble, reaffirms and clarifies the distinction commenters identified.
The EHB-benchmark selection process at § 156.111 is a distinct Federal regulatory framework from the framework governing defrayal under § 155.170. Accordingly, a State's selection or update of an EHB-benchmark plan under § 156.111 does not constitute a “State action” for purposes of defrayal and, by itself, cannot trigger a defrayal obligation. Instead, for purposes of § 155.170, “State action” refers to a State statute, regulation, guidance, or other requirement, separate from the State's selection or update of its EHB-benchmark plan, that requires QHPs to cover a benefit that is in addition to EHB under § 155.170(a)(2).
States with benefit mandates that duplicate benefits included in the State's EHB-benchmark plan and that seek to avoid a defrayal obligation may repeal the applicable State requirement, such that the benefit continues to be covered as EHB under the EHB-benchmark plan or otherwise limit the applicability of the requirement for
( printed page 29587)
QHPs.[120]
Where a State repeals a State-required benefit that is included in the State's EHB-benchmark plan, the corresponding benefit will continue to be treated as EHB for as long as it is included in the State's EHB-benchmark plan, consistent with § 156.111. Absent repealing the duplicative State-required benefit, the State would be responsible for defraying the associated costs as the benefit would not be EHB.
Based on our experience working with States, many are actively analyzing their State-mandated benefits for potential defrayal obligations and, where applicable, implementing defrayal. In some cases, States may not have established formal reimbursement processes because they have not identified State-mandated benefits that require defrayal under current standards. The absence of a formal defrayal process is not necessarily indicative of non-compliance or unpreparedness, as it may reflect that no such obligation has yet arisen. Additionally, we have provided technical assistance to several States on how to operationalize defrayal, including approaches to and timing of reimbursement. We intend to continue to engage with States and provide technical assistance as needed to ensure States understand when a State-benefit requirement is in addition to EHB and requires defrayal. We intend for this assistance to provide examples and guidance on applying this policy as finalized and how a State could operationalize the defrayal process pursuant to Federal requirements at § 155.170. However, we note that States remain responsible for establishing and maintaining the internal processes and procedures necessary to ensure that defrayal reimbursements to issuers or enrollees are appropriately administered in accordance with § 155.170.
Comment:
One commenter recommended that HHS also revisit its interpretation that State rules related to provider types, cost-sharing, or reimbursement methods do not require defrayal and instead require that mandates that limit cost-sharing are appropriately evaluated as subject to defrayal. Another commenter stated that due to State legislatures frequently passing new mandates with unworkable effective dates, HHS should work with States to implement a determination process for mandates subject to defrayal well in advance of the deadline for impacted plans to file rates with the State.
Response:
State-required benefits for purposes of defrayal are those that are specific to care, treatment, and services that a State requires issuers to offer to its enrollees.[121]
State rules that do not relate to specific benefits include State rules related to provider types,[122]
cost-sharing, benefit delivery method, or reimbursement methods.[123]
While QHP issuers must comply with these requirements, there is no Federal obligation to defray the costs.[124]
This maintains a clear and administrable distinction between benefit mandates that expand the scope of covered services and other State requirements that affect how benefits are delivered or financed.
We note that though the identification and implementation of defrayal obligations is the responsibility of the States, we provide States with robust technical assistance to help with analyzing State mandates and defrayal questions. A State may reach out to and communicate with HHS regarding the final policy, including with questions that relate to identifying which State mandates are in addition to EHB in that State.
Comment:
Some commenters referenced a recent Government Accountability Office (GAO) report recommending that CMS review its oversight of State defrayal obligations. The commenters noted that CMS had indicated in the 2025 Payment Notice that the current policy would improve State compliance by making identification of non-EHB benefits more straightforward. These commenters noted their belief that the GAO-recommended review might support CMS retaining the current policy, rather than adopting the proposed change and stated concern that the proposed rule did not evaluate how the proposed change would affect State compliance with defrayal requirements.
Response:
As noted in the proposed rule, we concurred with GAO's recommendation and are continuing to evaluate our oversight of defrayal requirements. We note that the policy finalized in this rule is not intended to address questions of State compliance with defrayal requirements or HHS oversight. Rather, this policy is grounded in our interpretation of section 1311(d)(3)(B) of the Affordable Care Act and is intended to ensure the appropriate scope of State-required benefits that are considered to be in addition to EHB.
Comment:
Some commenters stated concern that the proposal would have impacts beyond the individual and small group markets because EHB-related consumer protections, such as limits on cost sharing and prohibitions on annual and lifetime dollar limits, also apply to fully insured and self-funded plans. These commenters stated that reclassifying certain benefits as being in addition to EHB could remove these protections and therefore allow fully insured and self-funded plans to impose greater restrictions on coverage.
Response:
As we stated in the proposed rule, we are aware that this policy reversal could impact plans that are not directly subject to the EHB requirements. This includes fully insured and self-funded group health plans that must follow the annual and lifetime dollar-limit restrictions on EHB and annual cost-sharing limitation requirements under §§ 147.126 and 156.130.[125]
The impact would depend on whether a plan sponsor selects a State's EHB-benchmark plan for purposes of complying with sections 2707 and 2711 of the PHS Act. The proposal's impact could extend to other programs that must meet EHB standards, including BHPs under section 1331 of the Affordable Care Act and Medicaid ABPs under section 1937 of the Social Security Act. However, we do not agree that this policy would enable plans to newly impose restrictions on coverage. We note that, to the extent a State repeals a State-required benefit that would otherwise be considered in addition to EHB, and the benefit remains in the State's EHB-benchmark plan, such benefit would continue to be treated as EHB and therefore remain subject to applicable consumer protections.
6. Ability of States To Permit Agents and Brokers and Web-Brokers To Assist Qualified Individuals, Qualified Employers, or Qualified Employees Enrolling in QHPs (§ 155.220(j))
Section 1312(e) of the Affordable Care Act directs the Secretary to establish procedures under which a State may permit agents and brokers to enroll individuals and employers in QHPs through an Exchange and to assist individuals in applying for financial assistance for QHPs sold through an
( printed page 29588)
Exchange. In the 2027 Payment Notice proposed rule (91 FR 6335), we proposed new standards of conduct and additional consumer protection standards related to agents, brokers, and web-brokers who assist consumers with enrollments through FFEs and SBE-FPs. These proposals focus on requirements related to consumer consent documentation (§ 155.220(j)(2)) and requirements related to marketing activities (proposed redesignation at § 155.220(j)(3)).
In addition, section 1313(a)(5)(A) of the Affordable Care Act directs the Secretary to provide for the efficient and non-discriminatory administration of Exchange activities and to implement any measure or procedure the Secretary determines is appropriate to reduce fraud and abuse. Section 155.220 specifies procedures to support the State's ability to permit agents, brokers, and web-brokers to assist individuals, employers, or employees with enrollment in QHPs offered through an Exchange, subject to applicable Federal and State requirements. This includes processes under § 155.220(g) and (h) under which HHS may suspend or terminate an agent's, broker's, or web-broker's Exchange agreement(s) in circumstances that involve fraud or abusive conduct or where there are sufficiently severe findings of noncompliance. This also includes the FFE standards of conduct for agents, brokers, and web-brokers who assist consumers in enrolling in coverage through the FFEs that we established under § 155.220(j) to protect consumers and ensure the proper administration of the FFEs. Consistent with § 155.220(l), agents, brokers and web-brokers who assist with or facilitate enrollment in States with SBE-FPs must comply with all applicable FFE standards, including the requirements in § 155.220. Similarly, consistent with § 155.220(n), web-brokers who assist with or facilitate enrollment in States with State Exchanges must comply with all applicable FFE standards, including the requirements in § 155.220(c)(3)(i)(A), (G), (I), and (j)(2)(i).
In the proposed rule, we stated that we have observed numerous abusive, misleading, and coercive practices that harm consumers both financially and medically, necessitating these proposed amendments.[126]
For example, some agents, brokers, and web-brokers have been incorrectly attesting to, or failing to ascertain, whether consumers are enrolled in other minimum essential coverage. We stated that we have also observed manipulation of income projections and tax household composition to qualify consumers for QHPs in the FFE. Further observations include agents, brokers, and web-brokers enrolling consumers with inaccurate residence addresses to conceal unauthorized enrollments and enrolling deceased consumers. Given these observations and their potential for consumer harm, we proposed the following amendments to § 155.220(j): separating conduct related to consumer enrollment from conduct related to consumer marketing by relocating marketing requirements to redesignated § 155.220(j)(3); establishing new standards of conduct and additional consumer protection standards for agents, brokers, and web-brokers at § 155.220(j)(2); and introducing new marketing requirements in redesignated § 155.220(j)(3).
a. Proposals Related to FFE Standards of Conduct and Mandating a Standard Eligibility Application Review Form and Consumer Consent Form (§ 155.220(j)(2))
Section 155.220(j)(2) sets forth the standards of conduct for agents, brokers, and web-brokers that assist with or facilitate enrollment of qualified individuals, qualified employers, or qualified employees in coverage in a manner that constitutes enrollment through an FFE or SBE-FP, or that assist individuals in applying for APTC and CSRs for QHPs sold through an FFE or SBE-FP.
Section 155.220(j)(2)(i) requires agents, brokers, and web-brokers to provide consumers with correct information and refrain from marketing or conduct that is misleading. Section 155.220(j)(2)(ii) requires agents, brokers, and web-brokers to document that the consumer (or the consumer's authorized representative) has reviewed and confirmed prior to its submission that his or her eligibility application information is accurate. Under § 155.220(j)(2)(ii), agents, brokers, or web-brokers must also provide the FFEs and SBE-FPs with correct information under section 1411(b) of the Affordable Care Act. Section 155.220(j)(2)(iii) also requires agents, brokers, and web-brokers to document the consumer's consent prior to facilitating enrollments through the FFEs. As explained in the 2017 Payment Notice proposed rule (81 FR 12258 through 12264), these standards are designed to protect against agent, broker, and web-broker conduct that is harmful towards consumers or prevents the efficient operation of the FFEs and SBE-FPs.
In the proposed rule, we stated that we have been conducting documentation reviews to determine compliance with eligibility application review documentation requirements and consent documentation requirements. During these reviews, we have found numerous instances of noncompliance, such as documentation not containing the name of the assisting agent, broker, or web-broker, a missing date, and more. While we have engaged in Technical Assistance (TA) or enforcement, when appropriate, given these findings, we stated in the proposed rule that we have determined that HHS would likely reduce consumer harm by revising the current requirements in § 155.220(j)(2)(ii) and (iii).
We proposed to amend existing regulatory authority under § 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and consent documentation requirements. We stated in the proposed rule that our proposal would eliminate the currently broad allowances on the format for meeting these requirements by mandating that agents, brokers, and web-brokers use only the content in the HHS-approved and -created form. We stated the regulation would also be changed to clarify what types of actions constitute a consumer “taking an action” within the meaning of the regulation.
Currently, agents, brokers, and web-brokers are required to document that a consumer, or the consumer's authorized representative, reviewed and confirmed their eligibility application information prior to the submission of the enrollment information. This language was added to the regulations in the 2024 Payment Notice (87 FR 78206) to help combat fraud and reduce consumer harm caused by application submissions containing inaccurate information. Currently, however, there are no specific requirements regarding the format of this documentation, so long as it meets the minimum regulatory requirements under § 155.220(j)(2)(ii)(A). As a result, we have reviewed documentation submitted in response to enforcement activity in both paper and audio recording formats. During these reviews,
( printed page 29589)
we have found that a substantial amount of this documentation lacked regulatorily required information.[127]
These documentation reviews determine next steps, such as engaging in TA or enforcement activity.
Additionally, paper documentation often contains language and formatting that are generally unique to the specific agent, broker, or web-broker. This language can sometimes be complicated or difficult to follow for consumers, leading to potential consumer harm, as explained below. Based on our experience, we stated in the proposed rule that the documentation submitted by a significant number of agents, brokers, and web-brokers frequently failed to meet the required eligibility application review documentation criteria. These criteria may include but are not limited to: an explanation of attestations; required dates; the name of the agent, broker, or web-broker; an affirmative response from the consumer; a review of all application information; and the name of the consumer or authorized representative. Missing or incorrect information on eligibility application reviews can harm consumers. Inaccurate application information may lead to incorrect eligibility determinations, affect a consumer's tax liability, or result in other negative consequences. For example, if a consumer receives an incorrect APTC determination or is unaware they are enrolled, they may incur an unexpected tax liability or costs associated with obtaining a corrected or voided Form 1095-A. Ensuring that a consumer's income determination has been reviewed and confirmed as accurate can help prevent these issues.
Incorrect consumer information on eligibility application reviews may also affect Exchange operations or HHS' analysis of Exchange trends. For example, a high volume of applications containing erroneous information, such as U.S. citizens attesting to not having an SSN, could hinder the efficient and effective operation of the Exchanges on the Federal platform by requiring HHS to divert time and resources to address these discrepancies. While we have processes in place to investigate and adjudicate complaints, these types of complaints can present challenges when the only available evidence consists of conflicting accounts from the parties involved. We generally do not have access to additional contextual information that could help clarify the circumstances. To help address this, the 2024 Payment Notice (88 FR 25740) revised the standards of conduct at § 155.220(j)(2)(ii) to require agents, brokers, and web-brokers to document prior to the submission of information that the eligibility review information under section 1411(b) of the Affordable Care Act was reviewed and confirmed to be accurate by the consumer or their authorized representative, who has been designated in compliance with § 155.227.
Additionally, under § 155.220(j)(2)(iii), as finalized in the 2024 Payment Notice (88 FR 25740), agents, brokers, and web-brokers are required to document consumer consent on the FFEs and SBE-FPs prior to providing enrollment assistance. This documentation must comply with specific regulatory requirements and show that the consumer took an action that created a record that the agent, broker, or web-broker can maintain and produce to confirm that consent was provided by the consumer or their authorized representative.
Presently, there are no specific format requirements for consumer consent documentation, as long as it meets the minimum regulatory requirements under existing § 155.220(j)(2)(iii)(A), which requires a consumer, or their authorized representative, to “take an action” that produces a record that can be maintained and produced by an agent, broker, or web-broker to confirm that the consumer's consent was documented and confirmed to be accurate. While consent must also be documented, this regulation does not explicitly require an agent, broker, or web-broker to obtain it through the same action. During HHS' investigations, we have found that a substantial amount of the submitted consumer consent documentation either lacked the required information, or presented it unclearly, potentially resulting in consumer harm. HHS has consistently received documentation from agents, broker, and web-brokers that failed to include required information, including, but not limited to: the name of the agent, broker, web-broker, or agency receiving consent; the name of the consumer or their authorized representative; the dates of consent; the scope, duration, and purpose of the consent; and the process through which a consumer or their authorized representative may rescind the consent. There have also been instances where documentation of consumer consent was not provided upon request.
Documentation that omits these regulatory requirements does not adequately demonstrate that the consumer, or their authorized representative, provided consent prior to the agent, broker, or web-broker's facilitation of enrollment or provision of enrollment assistance. Submitting consumers' eligibility application reviews without compliant documented consumer consent is harmful to consumers because the consumers or their representatives may be unaware of their enrollments and the submitted enrollment application may contain incorrect information. This could lead to consumers receiving inaccurate eligibility determinations; not receiving plan correspondence; not being able to access more suitable health coverage for which they may qualify; and unexpected tax liabilities.
Given these findings, we proposed amendments to § 155.220(j) to improve the accuracy of application information and better ensure compliance with consumer consent documentation requirements. First, we proposed amending § 155.220(j)(2)(ii)(A) to further clarify expectations for agent, broker, and web-broker compliance and to make clear that the requirements in this provision are not intended to allow for a broad range of interpretations. Specifically, we proposed to revise § 155.220(j)(2)(ii)(A) to state that documentation by agents, brokers, and web-brokers showing that eligibility application information has been reviewed and confirmed to be accurate by the consumer (or the consumer's authorized representative) must be effectuated by having the consumer or the consumer's authorized representative take an action to execute the HHS-approved and -created consumer consent form.[128]
We also proposed redesignating § 155.220(j)(2)(ii)(A)(2) as § 155.220(j)(2)(ii)(A)(3) and amending newly revised § 155.220(j)(2)(ii)(A)
(2)
to describe acceptable and unacceptable actions that either a consumer (or consumer's authorized representative) can take that would allow the agent, broker, or web-broker to demonstrate their confirmation of the review of eligibility application information. Specifically, we proposed that these actions may include: a hand-written or electronic written signature or initials made directly on a document indicating a person's consent, approval, or agreement; an email from the consumer or the consumer's authorized representative; a recorded verbal conversation; or other clear and
( printed page 29590)
verifiable means. We stated that a signature that is simply typed on the documentation or a filled-in check-box would not clearly indicate the eligibility application information was reviewed and confirmed to be accurate by the consumer or the consumer's authorized representative, as we are unable to verify whether the consumer or their authorized representative personally reviewed and confirmed the accuracy of their information based on such a signature or checked box. We further stated that a handwritten signature or handwritten initials made directly on the HHS-approved and -created consumer consent form indicates a consumer's or a consumer's representative's consent because it would more clearly illustrate that the consumer or the consumer's representative indeed gave their consent as it can be compared against another handwritten signature or handwritten initials. We stated that the proposed amendments aim to reduce confusion among agents, brokers, and web-brokers on what constitutes compliant documentation, reduce consumer harm from noncompliant documentation, and enhance HHS' investigative efficiency.
We proposed revising § 155.220(j)(2)(iii)(A) to require agents, brokers, or web-brokers to demonstrate that the consumer or their authorized representative has obtained and reviewed consent documentation by executing an HHS-approved and -created consumer consent form. We stated that this form would fulfill regulatory documentation requirements related to eligibility application review and consumer consent, ensuring all regulatory requirements are in the documentation provided to and reviewed by the consumer or their authorized representative. We stated that it would also streamline the review of potentially noncompliant agents, brokers, and web-brokers, facilitate the removal of noncompliant agents, brokers, and web-brokers from assisting consumers on the Exchange, and protect consumers from potential harm while safeguarding the integrity of the Exchange. Finally, we stated that it would enable more timely resolution of investigations, benefiting agents, brokers, and web-brokers by generally providing faster final determinations from HHS.
We further proposed redesignating current § 155.220(j)(2)(iii)(C) as § 155.220(j)(2)(iii)(D) and revising § 155.220(j)(2)(iii)(C). We stated that newly proposed § 155.220(j)(2)(iii)(C) would require that the action taken by the consumer or their authorized representative to provide consent demonstrate to HHS that consent was indeed given by the consumer or the consumer's representative. We stated that § 155.220(j)(2)(iii)(C) would provide examples of acceptable actions, which mirror those proposed at § 155.220(j)(2)(ii)(A)(
2
). We also proposed that a signature that is simply typed on the HHS-approved and -created consumer consent form or a filled-in check-box would not clearly indicate consent was provided, as, based on this information, we are unable to verify whether the consumer or their authorized representative personally typed the name and completed the checkboxes, or if the agent, broker, or web-broker did so without obtaining actual consent from the consumer or their authorized representative. We stated in the proposed rule that a handwritten signature or handwritten initials made directly on the HHS-approved and -created consumer consent form indicates a consumer's or a consumer's representative's consent because it would more clearly illustrate that the consumer or the consumer's representative indeed gave their consent as it can be compared against another handwritten signature or handwritten initials. Although we released an FAQ [129]
in 2024 clarifying the “take an action” requirement, we are formalizing these expectations in regulation to provide greater transparency.
In summary, we proposed to revise § 155.220(j)(2)(ii)(A) to state that the consumer or their authorized representative must take an action to execute the HHS-approved and -created form, indicating that the eligibility application information has been reviewed and confirmed to be accurate by the consumer (or the consumer's authorized representative). We also proposed redesignating § 155.220(j)(2)(ii)(A)(
2) as § 155.220(j)(2)(ii)(A)(
3) and amending newly revised § 155.220(j)(2)(ii)(A)(
2) to describe the acceptable and unacceptable actions that a consumer (or their authorized representative) can take that would allow the agent, broker, or web-broker to demonstrate the consumer's or the consumer's authorized representative's confirmation of the review of eligibility application information. We also proposed to revise § 155.220(j)(2)(iii)(A) to require agents, brokers, or web-brokers to demonstrate that the consumer or their authorized representative has obtained and reviewed consent documentation by executing an HHS-approved and -created form. Finally, we proposed to redesignate current § 155.220(j)(2)(iii)(C) as § 155.220(j)(2)(iii)(D), and to add new § 155.220(j)(2)(iii)(C). We stated that newly proposed § 155.220(j)(2)(iii)(C) would require that the action taken by the consumer or their authorized representative to provide consent must be clear to HHS on the face of the documentation and would describe acceptable actions.
We sought comment on these proposals.
After consideration of the comments and for the reasons outlined in the proposed rule and this final rule, including our responses to the comments received, we are finalizing these proposals with modifications to delay the effective date of the proposals such that they will apply for all enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j). We are also making modifications to clarify that the proposed acceptable and unacceptable actions in proposed paragraphs §§ 155.220(j)(2)(ii)(A)(
2) and 155.220(j)(2)(iii)(C) are actions that will allow agents, brokers, or web-brokers to demonstrate the consumer or the consumer's authorized representative took an action to execute an HHS-approved and -created consumer consent form to confirm: (1) the eligibility application information has been reviewed and confirmed to be accurate; and (2) the consumer or the consumer's authorized representative took an action to provide consent. As a result, we are keeping the existing standards outlined in § 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) intact, as these provisions will remain in effect for all enrollments through PY 2027. We are adding language to § 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to state that current documentation policies for eligibility application review and consumer consent are effective for enrollments for plan years ending prior to January 1, 2028. We are also finalizing the proposed requirements to document confirmation of the consumer or the consumer's authorized representative's review of eligibility application information and to provide consumer consent using the HHS-approved and -created form as well as the acceptable and unacceptable actions to execute the HHS-approved and -created consumer consent form for enrollments for plan years beginning on or after January 2028, including enrollments under § 155.335(j).
( printed page 29591)
Comment:
Many commenters supported the proposal to mandate use of the HHS-approved and created consumer consent form used by agents, brokers, and web-brokers to meet the eligibility application review documentation requirements and the consumer consent documentation requirements. Specifically, many commenters noted that mandating the HHS-approved and created consumer consent form used by agents, brokers, and web-brokers would: help prevent fraudulent, unauthorized enrollments and inappropriate plan switching; reduce errors by providing a clear process for agents, brokers, and web-brokers to utilize; provide additional clarity concerning compliance matters and accountability; improve transparency between agents, brokers, and web-brokers and consumers; streamline investigations benefiting consumers, agents, brokers, and web-brokers; and provide consumer protection measures such as ensuring consumers have reviewed their eligibility application review documentation.
Response:
We agree that mandating use of the HHS-approved and -created consumer consent form by agents, brokers, and web-brokers provides many benefits to both consumers and agents, brokers, and web-brokers alike.
Comment:
Some commenters noted that this proposal to mandate a standard HHS-approved and -created consumer consent form would impose burdens on agents, brokers, and web-brokers and consumers. Some commenters noted that a previously signed consent form should qualify for ongoing use rather than requiring the consumer to sign a new consent form for each agent, broker, or web-broker interaction. Other commenters noted that requiring a new consent form each time there is an agent, broker or web-broker interaction creates a burden and barrier to customer care. Some commenters stated that agents, brokers, and web-brokers have specifically designed their programs based on the communities they are in, and a mandated HHS-approved and -created consumer consent form would not align with diversified communication strategies employed by agents, brokers, and web-brokers to tailor language and presentations to specific populations of consumers, which could lead to consumer confusion. Some commenters requested HHS to ensure that the HHS-approved and -created consumer consent form is accessible to all consumers, including those with disabilities, limited literacy, or limited English proficiency. Some commenters indicated that this proposal would lead to consumer difficulties and would also unnecessarily target the socio-economically challenged, including those populations who lack digital access, and those populations who would have language barriers, to complete the HHS-approved and -created consumer consent form. Commenters stated that requiring a new HHS-approved and -created consumer consent form with each consumer's application to the Exchanges creates a barrier to consumer care. Commenters noted concern that this proposal applies uniform compliance burdens to all agents, brokers, and web-brokers without distinguishing between lead-driven mass enrollment models and relationship-based agencies that rely on client-initiated contact.
Response:
To clarify, as indicated above, due to concerns raised by commenters, we are delaying the effective date of the use of the HHS-approved and -created consumer consent form by agents, brokers, and web-brokers to enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j). The HHS-approved and -created consumer consent form must be used by agents, brokers, and web-brokers, for all PY 2028 enrollments, including those enrollments under § 155.335(j), and for all new enrollments thereafter. This will help reduce the burden by allowing agents, brokers, and web-brokers ample time to update their processes to incorporate the HHS-approved and -created consumer consent form and finalize outreach to consumers that occurs prior to open enrollment. The HHS-approved and -created consumer consent form does not add new eligibility application review or consumer consent documentation requirements. Agents, brokers, and web-brokers should familiarize themselves and their consumers with the HHS-approved and -created consumer consent form and may utilize the pre-enrollment verification period, beginning August 1, 2027, as prescribed in section 71303(b) of the WFTC legislation, to have consumers sign this form. While the HHS-approved and -created consumer consent form will not be required until PY 2028, agents, brokers, and web-brokers may use the HHS-approved and -created consumer consent form as soon as it is posted on CMS' website.[130]
We intend to post the HHS-approved and -created consumer consent form prior to the 2027 pre-enrollment verification period. The proposed rule governing the use of the HHS-approved and -created consumer consent form does not bar agents, brokers, and web-brokers from creating supplemental materials to assist their consumers. However, the HHS-approved and -created consumer consent form must be used to document (1) eligibility application review, and (2) consumer consent requirements.
As outlined in the proposed rule (91 FR 6335), we stated that the HHS-approved and -created consumer consent form would eliminate the current broad allowances on the format for meeting the eligibility application review requirements and consent documentation requirements. For the reasons stated earlier in this final rule, we believe the HHS-approved and -created consumer consent form to be used by agents, brokers, and web-brokers will: help reduce errors; provide additional compliance clarity for agents, brokers, and web-brokers; streamline investigations; provide additional consumer protections; and ensure that all consumers are being treated equally, reducing discrepancies in how agents, brokers, and web-brokers document eligibility application review and consumer consent.
The HHS-approved and -created consumer consent form will also meet accessibility needs. We intend to make the HHS-approved and -created consumer consent form Section 508 compliant and we plan to translate the HHS-approved and -created consumer consent form into the languages as shown on
HealthCare.gov.
If agents, brokers, and web-brokers need to translate the HHS-approved and -created consumer consent form outside of the languages appearing on
HealthCare.gov,
agents, brokers, and web-brokers can translate the form into languages that do not appear on
HealthCare.gov,
but are prohibited from making any other alterations to the HHS-approved and -created consumer consent form.
To clarify, requirements already exist outlining the substance of what agents, brokers, and web-brokers must document for: (1) eligibility application review requirements, and (2) consumer consent requirements. The only difference, via this rule, is how agents, brokers, and web-brokers must document eligibility application review requirements and consumer consent requirements using the HHS-approved and -created consumer consent form. As a result, we are not adding additional, substantive elements to the HHS-approved and -created consumer
( printed page 29592)
consent form. The effective date of this policy has been delayed one year, so agents, brokers, and web-brokers will be required to use the HHS-approved and -created consumer consent form for all enrollments for plan years beginning on or after January 1, 2028, including those enrollments under § 155.335(j), impacting open enrollment in the fall of 2027 and for all new enrollments thereafter. As a result, agents, brokers, and web-brokers will not be required to use HHS-approved and -created consumer consent form to document (1) eligibility application review, and (2) consumer consent during open enrollment for the fall of 2026. Agents, brokers, and web-brokers may use the HHS-approved and -created consumer consent form, if they wish, during open enrollment during the fall of 2026. The delayed effective date will help reduce the burden by allowing agents, brokers, and web-brokers ample time to update their processes to incorporate the HHS-approved and -created consumer consent form and finalize outreach to consumers that need to happen prior to open enrollment. In addition, previously obtained consent forms and eligibility application review documentation will no longer satisfy the consumer consent documentation and eligibility application review documentation requirements beginning with enrollments and re-enrollments for PY 2028.
Further, we considered commenters' suggestion to allow a previously-signed consent form to remain valid for enrollments after the effective date for this policy. We are not adopting that approach because a core purpose of this policy is to ensure that each consumer action resulting in an application update or enrollment reflects an up-to-date and affirmative expression of the consumer's intent using the standardized HHS-approved and -created form. Allowing prior documented consumer consents and prior documentation of eligibility application review to satisfy this policy could weaken our ability to verify that the consumer took the action associated with each specific transaction, which is central to the program-integrity concerns this policy is designed to address. However, once the consumer or the consumer's representative has taken an action to complete the HHS-approved and -created consumer consent form, the consumer's consent will remain in effect unless the consumer or the consumer's authorized representative revokes consent or if the consent expires as expressly stated on the HHS-approved and -created consumer consent form. This means that for PY 2028, agents, brokers, and web-brokers must use the HHS-approved and -created consumer consent form for all enrollments, including enrollments under § 155.335(j), using the HHS-approved and created consent form to document the consumer's or the consumer's representative's (1) eligibility application review and (2) consumer consent. However, the agent, broker, or web-broker will not need the consumer or the consumer's representative to complete a new HHS-approved and -created consumer consent form for every interaction thereafter if the previously obtained consent is valid and has not been revoked by the consumer or the consumer's representative and the agent, broker, or web-broker's action on behalf of the consumer is within the scope of the consumer consent documentation.
Additionally, we note that the HHS-approved and -created consumer consent form will not be contingent on how an agent, broker, or web-broker obtains a client, as the HHS-approved and -created consumer consent form is used with each consumer regardless of whether an agent, broker, or web-broker's relies on mass lead generation or more personal client relationships. Also, the pre-enrollment verification period will be an optimal time to obtain consumer consent documentation and application eligibility review documentation.
Comment:
Some commenters noted that CMS should prioritize system-based authorization controls within the Exchange application process rather than relying primarily on documentation-based consent requirements. Commenters noted that static consent documentation requirements are unlikely to prevent large-scale unauthorized consumer enrollments.
Response:
We are continuing to evaluate various system controls to mitigate non-compliant behavior among agents, brokers, and web-brokers. However, we do not agree that system-based controls alone are sufficient to address the concerns raised. In addition to possible system controls being implemented, we believe creating and mandating the HHS-approved and -created consumer consent form is necessary because it ensures that all consumers are treated equally and are properly informed of what they are consenting to, and it reduces discrepancies in how agents, brokers, and web-brokers document: (1) eligibility application review requirements, and (2) consumer consent requirements. Standardized documentation complements, rather than replaces, system-based controls by providing verifiable documentation of consumer intent that supports program integrity and oversight activities.
Comment:
Some commenters noted that the HHS-approved and -created consumer consent form would not align well with the diverse communication strategies used by State Exchanges, which tailor language and presentations to their enrollment communities. Commenters indicated that requiring an HHS-approved and -created consumer consent form risks creating confusion by introducing terminology and formats that differ from those consumers encounter elsewhere in the Exchanges' communications.
Response:
The proposed policy for the required use of the HHS-approved and -created consumer consent form only applies to agents, brokers, and web-brokers assisting consumers through the Exchanges on the Federal platform; the proposed requirement would not apply to the State Exchanges. States operating State Exchanges retain the authority to establish their own policies and procedures regarding consumer consent and eligibility application review documentation and are not required to adopt the HHS-approved and -created consumer consent form.
Comment:
Some commenters recommended that HHS clarify what language in the HHS-approved and -created consumer consent form can vary, which would allow EDE entities to make user experience improvements to the display and revise the language to make it more accessible to consumers. Also, some commenters recommended that HHS allow agents, brokers, and web-brokers to document consent using any verifiable method that clearly demonstrates consumer consent, which could be produced during an audit of an agent, broker, or web-broker.
Response:
As outlined in the proposed rule (91 FR 6335), we proposed to require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to limit agents, brokers, and web-brokers discretion in how they meet the eligibility application review and consumer consent documentation requirements to better protect consumers. Requiring agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form reduces the likelihood of consumer manipulation or fraud because each agent, broker, or web-broker must use and collect the content areas stated on the HHS-approved and -created consumer consent form to
( printed page 29593)
document (1) eligibility application review requirements; and (2) consumer consent requirements.
We clarify that the language in the HHS-approved and -created consumer consent form cannot vary. For the reasons stated earlier in this section of this final rule, we believe the HHS-approved and -created consumer consent form to be used by agents, brokers, and web-brokers will help: reduce errors; provide additional compliance clarity for agents, brokers, and web-brokers; streamline investigations; provide consumer protection measures; and ensure that all consumers are being treated equally, reducing discrepancies in how agents, brokers, and web-brokers document: (1) eligibility application review requirements, and (2) consumer consent requirements. Allowing variation in the form would undermine the goals behind this policy to reduce investigation lengths, reduce discrepancies, and ensure all consumers are treated equally. Standardizing that agents, brokers, and web-brokers are required use the HHS-approved and -created consumer consent form will help improve consistency in how we compare and assess compliance with the documentation requirements. An increased level of consistency will increase the efficiency of our compliance determinations, thus supporting our efforts to ensure consumer protections. The standardized HHS-approved and -created consumer consent form ensures that every agent, broker, and web-broker is collecting the same categories of information in the same way, making it easier for us to investigate, perform audits, detect fraud or omissions, and enforce regulatory requirements uniformly. If agents, brokers, and web-brokers are using different modes to collect the eligibility application review and consumer consent documentation outside of using the HHS-approved and -created consumer consent form, it becomes increasingly more difficult to efficiently compare submissions, undermining our oversight. Requiring consistent use of a uniform consent and eligibility application information review form reduces the likelihood of consumer manipulation or fraud because each agent, broker, or web-broker must use and collect the same content areas as stated on the HHS-approved and -created form. This also makes it more difficult for agents, brokers, or web-brokers to omit required information and/or alter how questions are framed to steer outcomes.
As mentioned earlier, it is our intent to make the HHS-approved and -created consumer consent form Section 508 compliant as well as translating the HHS-approved and -created consumer consent form into the languages as shown on
HealthCare.gov.
If agents, brokers, and web-brokers need to translate the HHS-approved and -created consumer consent form outside of the languages appearing on
HealthCare.gov,
agents, brokers, and web-brokers can translate the form, and we clarify that they are prohibited from making any other alterations to the HHS-approved and -created consumer consent form.
Additionally, we clarify in this final rule that recorded telephone calls, in which the agent, broker, or web-broker communicates the entirety of the language in the HHS-approved and -created form to the consumer or the consumers' representative, and the consumer or the consumer's representative provides their verbal consent, is permissible to document: (1) eligibility application review requirements, and (2) consumer consent requirements. Documentation using the whole content of the HHS-approved and -created consumer consent form will be required for all agents, brokers, and web-brokers, for all enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j), impacting open enrollment in the fall of 2027. We make similar clarification for documentation of eligibility application review and consent documentation via email: the email chain used to document either eligibility review and the email chain used to document consent, or both if they are one and the same, must contain the entirety of the language in the HHS-approved and -created form. Further, previously obtained consent forms and eligibility application review documentation will no longer satisfy the consumer consent documentation and eligibility application review documentation requirements beginning with enrollments and re-enrollments for PY 2028. Any recordings and documentation must be maintained by agents, brokers, and web-brokers for 10 years, and provided to HHS upon request. See existing § 155.220(j)(2)(iii)(C).
Since we have clarified with further discussion acceptable methods for satisfying eligibility application review and consent documentation requirements, it is no longer necessary to reference “other means” and we are striking the reference from the policy we are finalizing in both revised §§ 155.220(j)(2)(ii)(A)(2) and 155.220(j)(2)(iii)(C).
Comment:
Some commenters noted that the HHS-approved and -created consumer consent form should also include: listing the issuer's name and plan name in which the consumer is enrolling; the member's premium; subsidies; and financial responsibility; the consumer's income and attestation; an acknowledgement that the consumer does not have or will be losing Medicaid or Medicare; and an internet Protocol (IP) address for digital forms to further strengthen consent documentation.
Response:
We appreciate this comment outlining other suggested information that we can consider capturing in the HHS-approved and -created consumer consent form. Some of the commenters' suggested additional elements, such as plan name, premium information, subsidies, and income attestations, are already captured elsewhere in the enrollment process, and therefore it would be duplicative and burdensome to list this information again on the HHS-approved and created consumer consent form. Similarly, requiring agents, brokers, web-brokers, consumers, or consumers' authorized representatives to manually identify and record their own IP address on the HHS-approved and -created consumer consent form would be technically burdensome and impractical. As such, having agents, brokers, and web-brokers collect this additional information would increase burden without providing commensurate value. Requiring agents, brokers, and web-brokers to collect duplicative information may lead to inefficiencies, increased completion time, and a higher likelihood of inconsistent data. For these reasons, we are not adopting these additional data elements to be included in the HHS-approved and -created consumer consent form at this time.
Comment:
Some commenters noted that we should clarify that the Federal Electronic Signatures in Global and National Commerce Act (E-Sign Act) allows for the execution of the HHS-approved and -created consumer consent form.
Response:
We outline what are acceptable and unacceptable actions that either a consumer or a consumer's authorized representative can take to demonstrate their confirmation of the review of eligibility application information; and the documentation of consumer consent, illustrating that the consumer or consumer's representative indeed gave his or her consent. Specifically, we are finalizing that these actions may include a hand-written or electronic written signature or initials, made directly on the HHS-approved and -created consumer consent form
( printed page 29594)
indicating a person's consent, approval, or agreement; an email from the consumer or consumer's authorized representative; or a recorded verbal conversation.
Additionally, the Electronic Signatures in Global and National Commerce Act, 15 U.S.C. 7001, is the law that gives electronic signatures the same legal effect as paper ones and includes certain consumer-consent and disclosure steps when required information is delivered electronically, see 15 U.S.C. 7001(c)(1)(A) and 15 U.S.C. 7001(c)(1)(B), such as the consumer agreeing to receive the information electronically and being told how to withdraw that consent. E-Sign-compliant methods may be used to sign the HHS-approved and created consumer consent form provided our program integrity requirements are met as set forth above and in this rule.
Comment:
Some commenters stated that telephone calls can still be valid supplemental consent documentation and recommended that previously obtained consent forms should be allowed to count for consumer consent in lieu of the HHS-approved and -created consumer consent form. Also, some commenters recommended that HHS allow agents, brokers, and web-brokers to document consent using any verifiable method that clearly demonstrates consumer consent, which could be produced during an audit of an agent, broker, or web-broker.
Response:
To clarify, for plan years beginning on or after January 1, 2028, recorded telephone calls, in which the agent, broker, or web-broker communicates the entirety of the language in the HHS-approved and -created form to the consumer or the consumers' representative, and during which the consumer or the consumer's representative provides their verbal consent, are permissible to document: (1) eligibility application review requirements, and (2) consumer consent requirements. As stated in this rule, the agent, broker, and web-broker must use the content of the HHS-approved and -created consumer consent form to document (1) eligibility application review requirements, and (2) consumer consent requirements. There will be verbal scripts included with the HHS-approved and -created consumer consent form that agents, brokers, and web-brokers can use for recorded telephone calls, which will contain the content of the HHS-approved and -created consumer consent form.
Previously obtained consumer consent and eligibility application review documentation and other methods used to document consumer consent and eligibility application review prior to PY 2028 will no longer be valid to satisfy consumer consent documentation and eligibility application review documentation requirements beginning with enrollments and re-enrollments for plan years starting January 1, 2028. Agents, brokers, and web-brokers must exclusively use the HHS-approved form for future enrollments (
i.e.,
those beginning on or after January 1, 2028).
Any recordings and consent or eligibility documentation must be maintained by agents, brokers, and web-brokers for 10 years and provided to HHS upon request. See § 155.220(j)(2)(iii)(C).
Comment:
A commenter requested HHS clarify enforcement, accountability, and the respective responsibilities for issuers and carriers [131]
with respect to the HHS-approved and -created consumer consent form.
Response:
To clarify, issuers and carriers will not be required to use the HHS-approved and -created consumer consent form; only agents, brokers, and web-brokers will be required to use the HHS-approved and -created consumer consent form to document: (1) eligibility application review documentation and (2) consumer consent documentation, for enrollments for plan years beginning on or after January 1, 2028.
Comment:
A commenter recommended that consent should be made available at both the (1) agent, broker, and web-broker, and (2) the agency level to ensure a good consumer experience in allowing an agency to service the consumer. The commenter also recommended that HHS should allow consumers to authorize an agency via an agency identifier such as an agency name and agency National Producer Number (NPN), while still recording the acting agent, broker, or web-broker's NPN for each enrollment/servicing action to preserve for auditing purposes and accountability.
Response:
Like the current Model Consent Form,[132]
the HHS-approved and -created consumer consent form will be available for use by agents, brokers, web-brokers, and agencies. We will continue to allow an agency, using the agency's identifier such as the agency's name and agency's NPN, to complete the HHS-approved and -created consumer consent form. Further, the agency's name appearing on the HHS-approved and -created consumer consent form does not prohibit an assisting agent's name and NPN from also appearing on the form.
However, we want to emphasize that even if the name of an agency is used on the HHS-approved and -created consent form, it remains the responsibility of the assisting agent, broker, or web-broker to maintain the documentation for 10 years and produce it to HHS, upon request, even when the agency's name or NPN number appears on the HHS-approved and -created consumer consent form. See § 155.220(j)(2)(iii)(C).
Comment:
We received out of scope comments relating to mandating use of the HHS-approved and -created consumer consent form. For instance, commenters indicated that HHS holds the perception or belief that agents, brokers, and web-brokers are engaging in fraudulent applications for the Exchanges. Commenters also indicated that nobody could accurately project their Adjusted Gross Income (AGI) 16 months ahead of time when doing applications. Commenters also indicated that some agents, brokers, and web-brokers call the Marketplace call center and impersonate consumers, engaging in unauthorized plan switching.
Response:
These comments are outside the scope of this proposal, and therefore we did not consider them for this final rule. We will keep them in mind for future rulemaking or sub-regulatory guidance.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing at revised §§ 155.220(j)(2)(ii)(A)(
2) and 155.220(j)(2)(iii)(C) that agents, brokers, and web-brokers are required to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and consent documentation requirements, effective for enrollments, including enrollments under § 155.335(j), for plan years beginning on or after January 1, 2028. We are also finalizing the acceptable and unacceptable actions that will allow agents, brokers, and web-brokers to demonstrate the consumer or the consumer's authorized representative took an action to execute the HHS-approved and -created consumer consent form. Accordingly, we are also finalizing the redesignation of current
( printed page 29595)
§ 155.220(j)(2)(ii)(A)(
2) as § 155.220(j)(2)(ii)(A)(
3) and current § 155.220(j)(2)(iii)(C) as § 155.220(j)(2)(iii)(D). We are also finalizing corresponding changes to §§ 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to state that current documentation policies for eligibility application review and review and consent are effective for enrollments for plan years ending prior to January 1, 2028. Please note that we may consider future updates to these regulatory provisions through rulemaking, if appropriate, to support implementation.
b. Proposals Related To Creating Standards of Conduct Related to Marketing (§ 155.220(j)(3))
In the 2027 Payment Notice proposed rule (91 FR 6337), we proposed to redesignate current § 155.220(j)(3) to § 155.220(j)(4) and add language at § 155.220(j)(3) to create standards of conduct by which agents, brokers, and web-brokers must adhere when engaging in marketing practices related to assisting or facilitating enrollment of qualified individuals, qualified employers, or qualified employees in FFE coverage, or applying for APTC or CSRs for QHPs sold through an FFE or SBE-FP. We clarify in this final rule that these marketing standards apply to agents, brokers, and web-brokers assisting consumers through FFEs and SBE-FPs. State Exchanges may adopt these standards at their discretion, but they are not required to do so. This proposal would establish marketing requirements and provide a non-exhaustive illustrative list of prohibited marketing practices. The marketing practices we identify and prohibit through the final rule are the most common misleading advertisement types we have discovered on social media websites to date. We identified these prohibited practices based on patterns observed through our monitoring of publicly available advertisements and the types of misleading marketing most frequently reported through the Agent Broker Helpdesk.
In the Patient Protection and Affordable Care Act; Program Integrity: Exchange, SHOP, and Eligibility Appeals final rule (78 FR 54076 through 54081), we established a framework for terminating an agent's, broker's, or web-broker's Exchange agreement(s) for cause in situations in which, in HHS' determination, a specific finding of noncompliance or pattern of noncompliance is sufficiently severe.[133]
Section 155.220(g)(2)(i) states that agents, brokers, or web-brokers may be determined noncompliant for violations of “[a]ny standard specified under this section,” which would include marketing violations under § 155.220(j)(2)(i). Under this existing framework, HHS can terminate an agent's, broker's, or web-broker's Exchange agreement(s) for cause to protect consumers and the efficient and effective operation of Exchanges in cases of sufficiently severe violations or patterns of violations. In such situations, under § 155.220(g)(3), HHS provides the agent, broker, or web-broker with 30 calendar days' notice and an opportunity to resolve and address the finding(s) of noncompliance during that 30 day notice period.[134]
If after 30 calendar days the noncompliance is not addressed to HHS' satisfaction, HHS may terminate the Exchange agreement(s) for cause. Once their Exchange agreement(s) are terminated for cause under § 155.220(g)(1), the agent, broker, or web-broker is no longer registered with the FFE, is not permitted to assist with or facilitate enrollment of a qualified individual, qualified employer, or qualified employee in coverage in a manner that constitutes enrollment through the Exchange, and is not permitted to assist individuals in applying for APTC and CSRs for QHPs.[135 136]
Consistent with § 155.220(h)(1), an agent, broker, or web-broker whose Exchange agreement(s) are terminated can request reconsideration of such action. Reconsideration requests submitted to HHS are handled by a division separate and independent from the one that imposed termination. Section 155.220(h)(2) provides the agent, broker, or web-broker with 30 calendar days to submit their request (including any rebuttal evidence or information) and § 155.220(h)(3) requires HHS to provide agents, brokers, or web-brokers with written notice of HHS' reconsideration decision within 60 calendar days of receipt of the request for reconsideration.
In the 2017 Payment Notice (81 FR 12204), we added section § 155.220(j)(2) to require agents, brokers, and web-brokers to provide consumers with correct information, without omission of material fact, regarding FFEs, QHPs offered through the FFEs, and insurance affordability programs, as well as refrain from marketing or conduct that is misleading, coercive, or discriminatory.
In the proposed rule, we stated that we have found many instances of advertisements that mislead consumers during our reviews of existing advertisements. We stated that we intend to prioritize taking enforcement actions against agents, brokers, and web-brokers who engage in misleading marketing. Complaints regarding misleading marketing can be sent to the Agent Broker (AB) Helpdesk,[137]
and we also intend to increase our monitoring of social media sites and other sources to root out misleading marketing. We explained that if we discover what we believe is misleading marketing, we may begin enforcement by engaging in TA or directly move to following the termination process established in § 155.220(g)(1). We currently use a misleading marketing-specific evaluation method we created to help us determine whether it is appropriate to engage in TA or take an enforcement action in response to an agent's, broker's, or web-broker's marketing practices. This evaluation method utilizes a scoring system, based on the number of ads used in public marketing and number of violations within each ad, to determine which response path to take, with higher scores generally indicating more egregiously noncompliant behavior that would lead to enforcement action. More egregious noncompliant behavior could be related to a large volume of ads being posted or ads containing multiple regulatory violations. We clarified that applying such a universal standard would help ensure all agents, brokers, and web-brokers are treated fairly.
Furthermore, in the proposed rule, we stated that there are instances when it can be difficult or impossible for HHS to determine who is responsible for posting the misleading marketing, hindering HHS' ability to take enforcement actions in those instances. To take an enforcement action, our investigation would need to find information linking the misleading
( printed page 29596)
marketing to a specific agent, broker, or web-broker. We could make this link by receiving contractual information regarding the posting of the marketing, finding agent, broker, or web-broker contact information in the metadata of the posted marketing, or through other reliable means. We stated that we plan to engage in TA to explain our approach when determining misleading marketing, and we would provide guidance to agents, brokers, and web-brokers to bring their materials into compliance with HHS' marketing requirements. While we anticipate each investigation would be different depending on the facts of the case, we stated in the proposed rule that we propose to utilize two mechanisms for agents, brokers, and web-brokers who have engaged in misleading marketing to become compliant. First, we stated that the agent, broker, or web-broker would need to remove the misleading marketing in a timely fashion. This would help ensure no additional consumers would see the advertisement and be misled. Additionally, we stated that we would ask that agents, brokers, and web-brokers review CMS-provided materials on what constitutes compliant marketing practices. This would help educate agents, brokers, and web-brokers to prevent future incidents of noncompliance.
In the proposed rule, we stated that we have found emerging patterns of misleading marketing and have been engaging in TA and enforcement actions when appropriate. We have found numerous examples of misleading marketing, with common issues ranging from guaranteeing zero-dollar enrollment to misrepresenting enrollment timelines. We stated that we believe these misleading marketing practices warrant additional HHS oversight and believe more robust marketing standards of conduct under § 155.220(j) are needed. Although our current regulations provide ample authority to begin our new TA program as described above and take enforcement action against misleading marketing, we proposed to amend our regulations to add more specific language on certain marketing prohibitions so that agents, brokers, and web-brokers know what is and is not permitted in their marketing.
Therefore, we proposed to amend § 155.220(j)(2) to remove “marketing or” from § 155.220(j)(2)(i); separate conduct related to enrollment from conduct related to marketing in newly redesignated paragraph § 155.220(j)(3); expand marketing requirements for agents, brokers, and web-brokers; and codify a non-exhaustive list of prohibited practices, requirements for responding to HHS requests related to marketing, and responsibilities related to marketing conducted by third parties with whom an agent, broker, or web-broker contracts. We also proposed to remove language from § 155.220(j)(2)(i) that defines the term “sex” to include sex characteristics, including intersex traits; pregnancy or related conditions; sexual orientation; gender identity; and sex stereotypes. We stated that this proposed change would recognize a person's sex as referring to an individual's immutable biological classification as either male or female, consistent with Executive Order 14168 (90 FR 8615) that reflects the current policy of the United States. HHS is of the view that because the sexes are not changeable and one's sex is grounded in fundamental and incontrovertible reality, it is not necessary to address ancillary issues of gender ideology in a regulation governing the activities of State-licensed agents, brokers, and web-brokers. Based on our experience overseeing agents, brokers, and web-brokers as they assist consumers with enrollment through the FFE, we stated that we do not believe this change would result in or facilitate any discrimination against consumers.[138]
At § 155.220(j)(3), we proposed that an individual or entity described in paragraph (j)(1) is required to comply with the standards set forth at § 155.220(j)(3).
We proposed at new paragraph § 155.220(j)(3)(i) to require that all conduct involving marketing must comply with the standards of conduct described within § 155.220(j)(2).
We also proposed, at § 155.220(j)(3)(ii), that all agents, brokers, and web-brokers must provide consumers with correct information about FFEs, QHPs offered through the FFE, and insurance affordability programs that does not omit any material facts. We proposed that agents, brokers, and web-brokers must refrain from marketing that is misleading, materially inaccurate, coercive, or discriminates based on race, color, national origin, disability, age, or sex. For purposes of the proposed rule, and consistent with the proposed revisions to § 155.220(j)(2)(i), we stated that the term “sex” refers to an individual's immutable biological classification as either male or female, consistent with Executive Order 14168 (90 FR 8615). This definition applies to all marketing materials and all consumer-facing communications subject to this section.
At § 155.220(j)(3)(iii), we proposed seven examples of prohibited marketing practices. We proposed at § 155.220(j)(3)(iii)(A) that agents, brokers, and web-brokers may not provide cash, monetary rebates, gift cards, travel vouchers, or cash equivalents to induce consumers to enroll or for any enrollment-related inducement.
At § 155.220(j)(3)(iii)(B), we proposed that agents, brokers, and web-brokers may not offer gifts to consumers unless such gifts are: of nominal value; offered to similarly-situated consumers without regard to whether the consumer enrolls; and are not in the form of cash or cash equivalents.[139]
We stated in the proposed rule that nominal value would have the meaning provided by the HHS Office of Inspector General [140]
and our review of nominal gifts would utilize the same prohibitions and allowances currently used in the Medicare Advantage (MA) Program.[141]
Many of these prohibitions on gifts associated with enrollments, excluding permissible nominal gifts, are also prohibited under State law and we stated that our proposals would not attempt to supersede State laws on these topics. We stated that any termination stemming from a violation of one of these finalized standards would be shared with the State(s) where the agent,
( printed page 29597)
broker, or web-broker is licensed, as required under § 155.220(g)(6).
We proposed at § 155.220(j)(3)(iii)(C) to prohibit agents, brokers, and web-brokers from falsely asserting or suggesting that consumers will always qualify for zero-dollar insurance or zero-dollar premiums. This type of advertisement may confuse or mislead consumers into providing an agent, broker, or web-broker their PII based on a false assumption of what they would qualify for. This PII may then be used by the agent, broker, or web-broker to enroll the consumer in a plan without authorization or for other unauthorized purposes. We stated that this proposed language would therefore aim to prevent consumers from providing their PII to agents, brokers, or web-brokers based on a false assumption.
At § 155.220(j)(3)(iii)(D), we proposed to prohibit agents, brokers, and web-brokers from falsely using identical or facsimiles of government or other official logos and notations. We stated in the proposed rule that this proposal is related to providing consumers with correct information and builds on existing language in § 155.220(j)(2)(i) that prohibits having a “. . . direct enrollment website that HHS determines could mislead a consumer into believing they are visiting
HealthCare.gov. . .” We stated that our proposal would extend this requirement to advertisements and broaden its scope to include government websites beyond HealthCare.gov. We stated that we wish to prevent consumers from visiting a website they believe is an official government website or is approved by the government when it is not. We stated that such false assumptions may lead to consumers who otherwise would not give their PII to a private entity to mistakenly believe they are providing their PII to a government entity, increasing the risk that they share sensitive information under false pretenses.
At § 155.220(j)(3)(iii)(E), we proposed to prohibit agents, brokers, and web-brokers from providing inaccurate or misleading information about enrollment timelines and deadlines. In the proposed rule, we stated that this proposal would include actions such as providing false, inaccurate, or misleading information related to SEP deadlines. Inaccurate timelines or misreporting of SEP deadlines may coerce consumers to enroll prematurely, believing they are about to miss an SEP or other enrollment deadline. This may cause consumers to enroll in a plan they may not have chosen otherwise if they realized they had more time to consider their options.
At § 155.220(j)(3)(iii)(F), we proposed to prohibit the misconstruing of legislation, regulations, or Executive Orders, including listing references or citations to fake or incorrect legislation, regulations, or Executive Orders. We stated in the proposed rule that this proposal would encompass advertisements using fictional citations, using misleading characterizations of specific citations, or other deceptive practices related to legislation, regulations, or Executive Orders. We stated that this proposal would help reduce misinformation and disinformation in advertisements, helping to ensure consumers are not misled before providing their PII to an agent, broker, or web-broker.
We also proposed at § 155.220(j)(3)(iii)(G) to prohibit the use of an image, likeness, or quote from a notable figure, such as a celebrity or politician, in an advertisement claiming that the figure has endorsed the agent, broker, web-broker, or their agency when that endorsement is not truthful. We stated in the proposed rule that this would include using artificial intelligence-generated videos, such as, but not limited to, deep fakes, or falsely attributing a quote to the public figure. This behavior may lure consumers into clicking on an advertisement or providing their PII based on a false assumption a public figure has endorsed the product or the person promoting the product. An endorsement would not be truthful if the figure in the advertisement did not actually endorse the product, did not actually speak the words the advertisement says they stated, or other similar behaviors. Furthermore, this behavior may violate State or Federal law on using someone's name, image, or likeness without permission.
The language we would use in proposed § 155.220(j)(3)(ii), and the behaviors we proposed to list in new § 155.220(j)(3)(iii), would better align Exchange requirements with MA requirements and help protect consumers. We stated in the proposed rule that aligning marketing rules for agents, brokers, and web-brokers across the Exchanges would ensure uniformity in enforcement and enhance regulatory compliance, thus creating consistent consumer information. We also stated that we believe these proposals would help ensure advertisements about the Exchanges are accurately providing consumers information about the Exchanges prior to providing their PII and enrolling in a health plan. Accurate advertisements help ensure more consumers enroll on time and provide required supporting documentation in a timely manner, leading to more consumers being enrolled in coverage. We stated that the integrity of the Exchange would be improved by reducing the amount of misleading information being provided to consumers, helping foster an environment where enrollees trust the agents, brokers, and web-brokers providing Exchange enrollment support, as they play an integral role in facilitating enrollments and providing consumers information about the Exchange.
Current §§ 155.220(j)(2)(ii)(A)(2) and 155.220(j)(2)(iii)(C) state HHS or our designee may periodically monitor and audit an agent, broker, or web-broker to assess their compliance with applicable requirements. These requirements allow HHS to request and review eligibility application information and consent documentation to determine compliance with applicable regulations. Therefore, consistent with these other standards of conduct and documentation requirements, we proposed to include the same language in new proposed § 155.220(j)(3)(iv) that agents, brokers, and web-brokers must produce any marketing material upon request in response to monitoring, audit, and enforcement activities conducted consistent with paragraphs (c)(5), (g), (h), and (k) of this section. We stated in the proposed rule that we do not believe a record retention requirement, similar to what is in place in §§ 155.220(j)(2)(ii)(A)(2) and 155.220(j)(2)(iii)(C), is necessary because we would already have access to the marketing materials.
In the proposed rule, we stated that we believe it is the responsibility of all agents, brokers, and web-brokers to ensure advertisements bearing their name or directing consumers to them for Exchange enrollment assistance do not contain misleading information and follow all regulatory requirements. Accordingly, at § 155.220(j)(3)(v), we proposed that an individual or entity described in paragraph (j)(1) of this section would be responsible for ensuring that all marketing-related materials created, written, released, or otherwise produced by the individual or an entity with whom the agent, broker, or web-broker has contracted or engaged to perform marketing on their behalf adhere to the requirements of § 155.220(j)(3)(ii)-(iii) and to make all such marketing-related materials available to HHS upon request in accordance with § 155.220(j)(3)(iv). We stated that an entity working on an agent, broker, or web-broker's behalf under § 155.220(j)(3)(v) could be an agent, broker, or web-broker working for
( printed page 29598)
another agent or broker that has been tasked with creating marketing materials, a third-party marketing organization with whom an agent, broker, or web-broker has contracted to create marketing materials on the agent, broker, or web-broker's behalf, or other similar parties. We stated that this proposal would support HHS compliance actions against agents, brokers, and web-brokers whose marketing materials do not comply with § 155.220(j)(3)(ii)-(iii) when necessary.
In summary, we proposed to redesignate § 155.220(j)(3) as § 155.220(j)(4) and at new § 155.220(j)(3), to clarify standards of conduct for marketing. We also proposed at § 155.220(j)(3)(iv) to require that an individual or entity described in § 155.220(j)(1) must produce marketing materials to HHS upon request in response to monitoring, auditing, or enforcement activities. Finally, we proposed at § 155.220(j)(3)(v) to establish that an individual or entity described in paragraph (j)(1) of this section is responsible for ensuring that all marketing-related materials created, written, released, or otherwise produced by the individual or entity or on their behalf adhere to the requirements of § 155.220(j)(3)(ii)-(iii) and, at § 155.220(j)(3)(iv), to produce to the HHS any marketing-related materials upon request in response to monitoring, audit, and enforcement activities.
We sought comment on all aspects of these proposals. Specifically, we sought comment on additional marketing standards of conduct we should consider for agents, brokers, web-brokers, and third-party marketing organizations to address deceptive marketing practices while minimizing administrative burden. We summarize and respond to public comments received on the proposed marketing standards of conduct below.
Comment:
Many commenters stated these changes would protect consumers by helping avoid confusion and misinformation. They also believed consumers would be less likely to be enrolled in plans that were not suited for their needs and would reduce likelihood of tax liability due to an incorrect application of APTC.
Response:
We agree with commenters who felt the updated standards of conduct on misleading marketing will protect consumers. We believe this will mitigate confusion and misinformation, helping consumers make informed decisions that align with their individual needs. We believe also assisting consumers make informed decisions can reduce the number of consumers who face tax liability, which may happen when misleading marketing leads a consumer to believe they qualify for a $0-premium plan and results in an inadvertent misapplication of APTC. We expect these protections to be effective because the updated standards prohibit misleading marketing practices and require agents, brokers, and web-brokers to ensure the accuracy of materials created directly by them or on their behalf.
Comment:
One commenter stated we should not expand oversight of agents, brokers, and web-brokers as they already are required to comply with numerous Federal and State laws.
Response:
We do not believe these proposals will be overly burdensome on agents, brokers, and web-brokers and are necessary as the existing requirements have not fully prevented misleading or deceptive marketing practices. These proposals do not mandate agents, brokers, or web-brokers create new advertisements to replace existing ones, unless the existing ads are noncompliant, or create advertisements in general. Instead, we are merely providing guidelines and identifying certain prohibitions if an agent, broker, or web-broker were interested in advertising their services. These new standards reinforce current requirements to not engage in marketing that is misleading, coercive, or discriminatory but provide a more detailed explanation of prohibited marketing practices and better clarifies our expectations surrounding marketing. We also believe the consumer protections these standards of conduct will provide would outweigh the minimal burden placed on agents, brokers, and web-brokers.
Comment:
One commenter stated these new standards of conduct would punish those acting in good faith.
Response:
We do not agree that the new standards of conduct for misleading marketing would punish those acting in good faith. Under sections 1311(e)(1), 1311(k), and 1321(a) of the Affordable Care Act and § 155.220(j) and (g), agents, brokers, and web-brokers control the content of advertisements they create, either by creating the ads themselves or by hiring an entity to do so on their behalf. Prior to contracting with a third party, an agent, broker, or web-broker should perform due diligence to help ensure the third party is compliant with all Federal and State laws. The new marketing standards of conduct clearly discuss prohibited behaviors to support compliance and deter misleading marketing practices.
In addition, the enforcement process under § 155.220(g) provides agents, brokers, and web-brokers an opportunity to respond to our findings and submit information to rebut those findings before any termination of an agent's, broker's, or web-broker's FFE Agreements. This process helps ensure that enforcement actions are directed toward noncompliant conduct.
We did not expand the good faith provision in newly redesignated § 155.220(j)(4) (formerly § 155.220(j)(3)) to include the marketing provisions because marketing activities are fully within the control of the agent, broker, or web-broker. The good faith exception primarily applies to circumstances outside the agent's, broker's, or web-broker's control. For example, agents, brokers, and web-brokers rely on consumers to provide accurate household income information. This situation is not relevant to the marketing regulations because, as indicated earlier, these regulations apply only to activities fully within the agent's, broker's, or web-broker's control.
Comment:
Several commenters supported the proposals but worried that they do not address the major contributors of misleading marketing and we should instead focus our efforts on Third-party Marketing Organizations (TPMOs), Field Marketing Organizations (FMOs), agencies, and other large-scale distributors of misleading marketing. These commenters also noted allowing agents, brokers, and web-brokers to report entities engaging in misleading marketing.
Response:
Our proposals focused on individual agents, brokers, and web-brokers because these are the entities with which we enter into Exchange Agreements and, therefore, the entities over which we have enforcement authority. We do not enter into Exchange Agreements with TPMOs, FMOs, agencies, or other entities. However, we encourage individuals with information about any entity engaging in misleading marketing to report such conduct to HHS, their State Department of Insurance, the Department of Justice, or another appropriate Federal or State law enforcement agency.
Comment:
A few commenters stated we need to ensure the new marketing requirements do not have a chilling effect on agents, brokers, and web-brokers trying to legitimately reach and educate consumers.
Response:
We do not wish for the new marketing standards of conduct to discourage agents, brokers, or web-brokers who are complying with the regulations and attempting to help consumers. Our enforcement efforts will focus on agents, brokers, and web-
( printed page 29599)
brokers who create or disseminate misleading marketing materials. Any investigation into misleading marketing would focus on whether a connection exists between the advertisement and the agent, broker, or web-broker who created or disseminated it. We would not take enforcement action against an agent, broker, or web-broker without such a connection. Additionally, our enforcement procedures under § 155.220(g) help prevent any chilling effect by ensuring the agent, broker, or web-broker has the opportunity to respond and provide information to rebut a finding of noncompliance before any termination of an agent's, broker's, or web-broker's Exchange Agreements.
Comment:
Multiple commenters stated we need to protect agents, brokers, and web-brokers acting in good faith, by ensuring we differentiate good faith errors from intentional misconduct, ensure only the advertisement's originator is held responsible, and reducing liability for materials agents, brokers, or web-brokers did not produce themselves. One commenter recommended we change our proposed language to materials “produced under their direction and control.”
Response:
The good-faith discussion in the previous response, including references to the existing good-faith exception in newly redesignated § 155.220(j)(4) and the rebuttal process under § 155.220(g), is applicable here and provides additional information on how we distinguish good faith errors from intentional misconduct. Our investigations of misleading marketing ensure only the person responsible for creating a misleading advertisement is held responsible. As part of our investigation, we review each advertisement, determine who created it, and conduct outreach as needed. If we are unable to determine with certainty who made the advertisement, we would not engage in enforcement.
Our proposal stated that agents, brokers, and web-brokers would be responsible for advertisements created, written, released, or otherwise produced by the individual or an entity acting on their behalf. We believe the “on their behalf” language in our regulations is sufficiently similar to “produced under their direction and control” and, therefore, no change to the language is required. For clarity, we consider an agent, broker, or web-broker responsible for marketing created by a third party only when that third party is contracted, directed, or compensated by the agent, broker, or web-broker. We reiterate that we will not pursue agents, brokers, or web-brokers without sufficient knowledge that they are responsible for their own marketing materials. Additionally, as we do not have oversight authority over TPMO's or lead generators, we could not pursue enforcement against them even if we knew they created an advertisement on an agent's, broker's, or web-broker's behalf. We encourage all agents, brokers, and web-brokers to carefully vet any TPMO, FMO, lead generator, or other third-party entity they collaborate with to ensure they are following all Exchange rules and regulations.
Comment:
Several commenters stated CMS should provide more guidance to agents, brokers, and web-brokers. Several suggestions were made, including that CMS should produce sub-regulatory guidance on misleading marketing, review advertisements prior to publication, create a centralized website with approved materials entities may use, conduct training on misleading marketing, note where this language will be codified, and pair the standards with clear accountability mechanisms, meaningful penalties, and standardized training.
Response:
We will likely create sub-regulatory guidance related to misleading marketing, similar to how we have handled agent, broker, and web-broker proposals in the past. This would likely be a Frequently Asked Questions (FAQ) document. The questions in the FAQ would likely be generated by comments and questions we received during this comment submission window, from questions received during agent, broker, and web-broker webinars, from issues raised when we engaged in technical assistance with agents, brokers and web-brokers over misleading marketing, and through other methods. The webinars we host detail Exchange requirements, emphasizing new requirements, security and privacy, consent, and other topics we want to reinforce. Much of the material, including that related to misleading marketing, is also included in trainings that all agents, brokers, and web-brokers are required to take annually.
At this time, we do not plan to review advertisements prior to publication. With over 100,000 registered agents, brokers, and web-brokers, preliminary review would be too burdensome and would reduce our ability to engage in enforcement actions against noncompliant agents, brokers, and web-brokers in other areas. We believe reducing our ability to investigate noncompliance would be more harmful to consumers than the benefits that advertisement review prior to publication would provide. We believe our new regulations on prohibited marketing practices will sufficiently inform agents, brokers, and web-brokers on what language and tactics should not be included in advertisements such that preliminary review is unnecessary.
We do not plan on creating and maintaining a repository of approved advertisements for general use. Individual agents, brokers, web-brokers, and agencies are free to create their own advertisements. This allows maximum creativity and flexibility when entities create their own marketing campaigns. We also do not want to create a perception that we are endorsing a particular agent, broker, or web-broker, which may happen if an entity were using CMS-created and approved marketing materials.
Comment:
One commenter stated we should be clearer about where the new marketing requirements will be within the regulations.
Response:
The misleading marketing language was proposed, and we are finalizing, the standards of conduct at § 155.220(j). Our proposal discussed the enforcement process as it relates to misleading marketing, including the two pathways: technical assistance or Enforcement. We will also apply the enforcement procedures in § 155.220(g)(1)-(3), which govern notice, the opportunity to respond, and the process for terminating an agent's, broker's, or web-broker's Exchange Agreements, for misleading marketing enforcement, which have been comprehensively detailed in past notice and comment rulemaking, and in the proposed text.
Comment:
Many commenters provided feedback on how misleading marketing should apply to States. Namely, commenters stated we should not apply these requirements to State Exchanges, they should not supersede State laws, and we should share information we gather on misleading marketing, such as terminations related to misleading marketing, with States.
Response:
We do not intend for these requirements to apply to State Exchanges, only to FFEs and SBE-FPs, consistent with § 155.220(j)(1). A State Exchange may choose to adopt similar requirements at their discretion. As required under § 155.220(g)(6), State Departments of Insurance, or the equivalent licensing authority, will be notified of Exchange Agreement suspensions or terminations related to misleading marketing enforcement.
Comment:
One commenter stated that CMS should implement a record-retention period to ensure items requested under audits are available.
( printed page 29600)
Response:
We intentionally did not impose a record-retention period for marketing. We believe it would be unnecessary to require agents, brokers, and web-brokers to maintain their advertisements for 10 years. This is because we actively search for misleading marketing on publicly-facing websites and timely engage in technical assistance or take enforcement actions when appropriate, and we typically have copies of the advertisements in question and do not require the agent, broker, or web-broker to submit the advertisement as part of the investigation. We included this language to ensure agents, brokers, and web-brokers can provide marketing materials they still have at the time of a request in the rare instances when we do not already have the advertisement or when we are conducting an investigation initiated by other means. We believe including this language is prudent to ensure our investigations have the information needed to proceed effectively.
Comment:
One commenter suggested that CMS add a prohibited practice to the list in § 155.220(j)(3). This commenter stated we should restrict marketing of non-QHP coverage that does not distinguish between QHP plans and may lead to consumer confusion.
Response:
We selected the marketing prohibitions in the proposal because they were the most common forms of misleading advertising we discovered during our research. As such, we believed listing these as prohibited practices was paramount. As this is not a static or exhaustive list of prohibited practices, we appreciate this comment and may take it into consideration in future rulemaking.
Comment:
Several commenters opposed the proposed removal of parenthetical language from § 155.220(j)(2)(i) that adds specificity to the interpretation of discrimination “on the basis of sex,” objecting that its removal undermines the enforcement of Section 1557 of the Affordable Care Act and is not in accordance with the interpretation of the 2024 Nondiscrimination in Health Programs and Activities final rule (89 FR 37522 (May 6, 2024)) (hereinafter referred to as the “2024 Final Rule”). Another commenter noted that the footnote 78 in the proposed rule appeared to misinterpret the scope of section 1557, specifically as it applies to all HHS-administered programs and activities, citing the 2024 Final Rule which states, “every health program or activity administered by the Department ensures that nondiscrimination standards are interpreted and applied as consistently and as broadly as possible and provides for application of nondiscrimination standards to the Department consistent with the entities to which it provides Federal financial assistance.”
Other commenters did not accept HHS' statement in the proposed rule that addressing matters related to gender ideology was not necessary in a regulation focused on agents, brokers, and web-brokers, with commenters citing academic literature and Centers for Disease Control and Prevention findings that transgender populations are particularly vulnerable to discrimination. Other commenters stated concern for consumers who may not receive appropriate, non-discriminatory assistance with enrollment into QHPs by agents and brokers if they are not held to the same standards required by other covered entities.
Other commenters agreed with the proposal to remove the language on the grounds that sex is “an immutable, biological binary.” They further noted that the change would better conform with the text of the Affordable Care Act and would be more consistent with the enforcement of President Trump's Executive Order 14168 (90 FR 8615), “Restoring Biological Truth to the Federal Government.” Another commenter noted that the proposal respects the biological differences of men and women “to ensure clarity in law and protect individual privacy.”
Response:
We appreciate commenters' views and note at the outset that this rulemaking does not address Section 1557 of the Affordable Care Act or its enforcement. This finalized policy is adopted pursuant to independent HHS authority under Sections 1312(e) and 1321(a)(1)(A), (B), and (D) of the Affordable Care Act. For more information about enforcement of Section 1557 and its scope, we refer commenters to 45 CFR part 92, the regulations implementing that statute, and to the HHS Office for Civil Rights, which enforces Section 1557. As we noted in footnote 99 of the proposed rule, (91 FR 6292-6486) several court orders affect the implementation of Section 1557's prohibition on sex discrimination. We do not address them here. HHS enforces Section 1557's prohibition on discrimination on the basis of sex stereotypes consistently with the Executive Order 14168 (90 FR 8615) and well-established case law on sex stereotypes.
See, e.g., Pederson
v.
La. State Univ.,
213 F.3d 858, 880-81 (5th Cir. 2000) (holding that under Title IX, “classifications based on archaic assumptions are facially discriminatory” and perpetuate stereotypes) (internal quotations omitted). The removal of the parenthetical language from State-licensed agents, brokers, and web-brokers standards of conduct under § 155.220 does not affect HHS' enforcement of Section 1557 and its implementing regulations. Any question of whether Section 1557 applies to certain entities is a fact-specific analysis conducted under that law.
We appreciate the commenter's concerns and the evidence provided regarding vulnerabilities of certain populations to discrimination. However, as we stated in the proposed rule, based on our direct experience in overseeing agents, brokers, and web-brokers and our familiarity with the State licensing and oversight frameworks that govern these entities, they are already subject to an array of professional requirements that provide meaningful accountability and make additional regulatory action unnecessary and could potentially create undue burden and confusion.
We are finalizing the removal of nondiscrimination language from § 155.220(j)(2)(i) as proposed. For the reasons we previously stated, we do not believe this change would result in or facilitate any discrimination against consumers. We believe this revision effectively implements Executive Order 14168 (90 FR 8615).
After consideration of comments, we are finalizing the standards of marketing conduct policy as proposed. Specifically, we are finalizing the revision of § 155.220(j)(2) to remove “marketing or” from § 155.220(j)(2)(i); the redesignation of § 155.220(j)(3) to separate standards of conduct related to enrollment from standards of conduct related to marketing; the expanded marketing requirements for agents, brokers, and web-brokers at § 155.220(j)(3)(ii); and the codification of a list of prohibited practices, requirements for responding to HHS requests related to marketing, and responsibilities related to marketing conducted by third parties with whom an agent, broker, or web-broker contracts at § 155.220(j)(3)(iii)(A) through § 155.220(j)(3)(iii)(G). Accordingly, we are also finalizing the redesignation of § 155.220(j)(3) as § 155.220(j)(4). We are also finalizing at
( printed page 29601)
§ 155.220(j)(3)(iv) to require that an individual or entity described in § 155.220(j)(1) must produce marketing materials to HHS upon request in response to monitoring, auditing, or enforcement activities; and at § 155.220(j)(3)(v) to establish that an individual or entity described in paragraph (j)(1) of this section is responsible for ensuring that all marketing-related materials created, written, released, or otherwise produced by the individual or entity or on their behalf comply with the requirements of § 155.220(j)(3)(ii)-(iii). We are also finalizing as proposed the removal of language from § 155.220(j)(2)(i) that defines the term “sex” to include sex characteristics, including intersex traits; pregnancy or related conditions; sexual orientation; gender identity; and sex stereotypes.
7. Removal of the Vendor Program (§ 155.222)
In the 2027 Payment Notice proposed rule (91 FR 6340), we proposed to remove § 155.222, which currently governs the vendor program to provide agent and broker training on an annual basis for a given plan year. Removal of this regulation effectively discontinues the vendor program.
The vendor program was established through § 155.222 to be implemented in PY 2016 and beyond to allow the possibility for certain training and information verification functions to be provided by HHS-approved vendors. In the 2016 Payment Notice (80 FR 10749), we outlined in § 155.222(a) the application and approval process for vendors seeking recognition as HHS-approved vendors for FFE training and information verification for agents and brokers. Section 155.222(b) outlines the standards that an entity must meet to be approved by HHS as a vendor and to maintain their status as an approved vendor, and § 155.222(c) provides that the approved list of vendors will be published on an HHS website. Section 155.222(d) describes how vendors will be monitored for ongoing compliance with the standards outlined in § 155.222(b). Section 155.222(e) describes the appeals process available to vendors whose applications are denied, or whose approvals to offer training and information verification are revoked.
The vendor program has low participation rates and has not seen significant growth. Since the program's inception in PY 2016, only six entities have participated as vendors, with only two or three participating in any given plan year. Additionally, agents and brokers who utilize the program only account for 9.3 percent (9,138) of registered agents and brokers in PY 2025. Moreover, since 2015, training completions by agents and brokers through vendors have never surpassed 10 percent. This data indicates consistently low demand for the program. Importantly, eliminating the vendor program would save the Federal Government approximately $300,000 each plan year.
We stated in the proposed rule that if this proposal to discontinue the vendor agent/broker training program is finalized, it would affect neither the quality of nor access to agent/broker annual training. We stated that agents and brokers would continue to have the ability to access training through CMS' existing Marketplace Learning Management System (MLMS) platform. The proposal to discontinue the vendor agent/broker training program only proposed to remove the option of this alternate training platform, one that, as noted, has been historically underutilized.
In summary, we proposed to terminate the vendor program, which allows approved third-party entities to facilitate the annual agent and broker training and registration process for the Exchange, through removal of § 155.222.
We requested comment on the proposal to remove § 155.222 and eliminate the vendor program.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed removal of the vendor program below.
Comment:
Commenters stated concerns that discontinuing the vendor training program for agents and brokers would change agent and broker training requirements. Comments additionally stated concerns that this change would impact the processes for enrollment functionality of the vendors that also facilitate enrollments via Enhanced Direct Enrollment.
Response:
To clarify, we proposed to discontinue delivery of annual FFE agent and broker training through external training vendors only. The FFE Agent & Broker Training Vendor Program was created to provide existing and prospective FFE agents and brokers an opportunity to fulfill annual requirements to complete training for continuing education credit while enabling us to maintain oversight of the program. To ensure that agents and brokers are able to meet Exchange requirements and receive the latest information on assisting consumers in the Exchange, we will continue to offer free FFE training to agents and brokers annually through CMS' MLMS. We are confident that training hosted on CMS' MLMS platform has sufficient capacity to absorb demand from an increasing number of agents and brokers for annual FFE agent and broker training and registration. Other processes, such as enrollment through EDE platforms, are not impacted by this proposal.
Comment:
We received a comment suggesting changes to the vendor program in lieu of discontinuing it.
Response:
In support of our ongoing priority to identify and eliminate fraud, waste, and abuse from FFE programs, it is critical that we retain direct control of the training program's operational integrity and compliance, including providing final course curriculum and redirecting agents and brokers back to the CMS platform to sign agreements upon completion of the course. To ensure that agents and brokers are able to meet Exchange requirements and receive the latest information on assisting consumers in the Exchange, we will continue to offer free FFE training to agents and brokers annually through CMS' MLMS.
Section 71301 of the WFTC legislation established new eligibility requirements for the PTC. Specifically, section 71301 of the WFTC legislation amends 26 U.S.C. 36B(e) to provide that a PTC is allowed for the coverage of a lawfully present noncitizen only if he or she is an “eligible alien.” Section 71301 of the WFTC legislation defines “eligible alien” as an individual who is either lawfully admitted for permanent residence (sometimes referred to as a “lawful permanent resident” or “green card holder”); an individual who has been granted the status of Cuban and Haitian entrant as defined in section 501(e) of the Refugee Education Assistance Act of 1980; or an individual who is lawfully residing in the United States in accordance with the Compacts of Free Association (COFA) as defined at 8 U.S.C. 1612(b)(2)(G) (sometimes referred to as a “COFA migrant”). Section 71301 of the WFTC legislation also makes conforming amendments to sections 1411(a)(1), 1411(a)(2), 1411(b)(3), 1411(c)(2)(B)(ii), and 1412(d) of the Affordable Care Act. These amendments require Exchanges to collect attestations regarding “eligible alien” status for applicants applying for APTC, to verify such attestations with the Secretary of the Department of
( printed page 29602)
Homeland Security, and to determine eligibility for APTC under section 36B of the Code based on whether an applicant is an “eligible alien.” Section 1402(g)(2) of the Affordable Care Act specifies that CSRs are only allowed for applicants who are also eligible for PTC. While section 71301 of the WFTC legislation does not amend section 1402(g)(2) of the Affordable Care Act, because section 71301 limits PTC eligibility for applicants who are “eligible aliens,” section 1402(g)(2) requires that CSR eligibility also be limited to only those who are “eligible aliens.”
In the 2027 Payment Notice proposed rule (91 FR 6341), to align Exchange eligibility and verification rules with section 71301 of the WFTC legislation's amendments to sections 1411 and 1412 of the Affordable Care Act, we proposed to add a new definition of “eligible noncitizen” at § 155.20, providing that the term “eligible noncitizen” would have the same meaning as the term “eligible alien,” as defined in 26 U.S.C. 36B(e)(2)(B), which was newly defined in section 71301 of the WFTC legislation.
We further proposed a technical update to § 155.305(f)(1)(ii) to cross-reference 26 CFR 1.36B-1(d). Currently, § 155.305(f)(1)(ii) states that a tax filer may be eligible for APTC if the Exchange determines that one or more applicants for whom the tax filer expects to claim a personal exemption deduction on his or her tax return for the benefit year, including the tax filer and his or her spouse, meets QHP enrollment eligibility requirements and is not eligible for MEC during the coverage month. We proposed to amend this section to state that a tax filer is eligible for APTC if the Exchange determines that one or more applicants who is a member of the tax filer's family, as defined at 26 CFR 1.36B-1(d), meets QHP enrollment eligibility requirements and is not eligible for MEC during the coverage month. In the proposed rule, we stated that this proposed change better aligns with existing Treasury regulations regarding PTC eligibility and provides a clearer description of the individuals on whose behalf a tax filer may be allowed APTC, given that taxpayers can no longer claim personal exemptions on their Federal income tax returns.[142]
Additionally, we proposed to add § 155.305(f)(1)(ii)(C) to provide that an Exchange must grant eligibility for APTC to individuals who are U.S. citizens, U.S. nationals, or eligible noncitizens provided they meet the other APTC eligibility requirements. To align with the new eligibility requirements for APTC for “eligible noncitizens” established by section 71301 of the WFTC legislation, we proposed to add verification regulations at § 155.320(c)(3)(ix). We stated in the proposed rule that this proposal would establish Exchange verification requirements for applicants who attest to having an eligible noncitizen immigration status as defined at § 155.20. Specifically, we stated that it would require Exchanges to attempt to verify eligible noncitizen immigration status using data from the Department of Homeland Security's Systematic Alien Verification for Entitlements (SAVE) program and proceed with the inconsistency process outlined in § 155.315(f)(1) through (4) when the Exchange cannot verify the information using SAVE data.
As part of this regulatory update, we also proposed to remove duplicative language and correct the lack of headings in § 155.320(c)(3) by removing the first occurrence of § 155.320(c)(3)(viii) and adding headings to § 155.320(c)(3)(vii) and (viii). We stated in the proposed rule that we believe the redundancy resulted from an oversight in previous rulemaking, as both provisions were intended to define “family size” to align with definitions in the Code and related Treasury Regulations. The first provision referenced 26 CFR 1.36B-1(d), while the second referenced section 36B(d)(1) of the Code. We stated that we believe that the regulatory definition in 26 CFR 1.36B-1 is more appropriate for use in our regulations.
Additionally, we noted in the proposed rule that section 71301 of the WFTC legislation will impact Federal payments to States that operate BHPs for individuals enrolled in the BHP who are lawfully present noncitizens but who are not “eligible aliens,” as defined in 26 U.S.C. 36B(e)(2)(B). To align BHP program regulations with this statutory change, we proposed to add a definition of “eligible noncitizen” at 42 CFR 600.5, cross-referencing the definition of the same term at 45 CFR 155.20. The underlying statutory provisions at section 71301 of the WFTC legislation apply to plan years beginning on or after January 1, 2027. We stated that our proposed regulatory amendment would be effective beginning with plan years starting on or after January 1, 2027.
Under section 1331(d)(3)(A)(i) of the Affordable Care Act and 42 CFR 600.605(a), Federal BHP payments to States include 95 percent of both the PTC under section 36B of the Code and the CSR that would have been provided for the fiscal year to eligible individuals enrolled in BHP standard health plans in the State if such eligible individuals had been enrolled in QHPs through an Exchange. Currently, Congress does not fund CSR payments. Therefore, CMS assigns a value of zero to the CSR portion of the BHP payment rate calculation and States receive no BHP funding attributable to that portion.
We proposed to update §§ 155.20, 155.305(f)(1), and 155.320(c)(3)(ix) to align Exchange regulations with section 71301 of the WFTC legislation. Section 71301 of the WFTC legislation amended section 36B of the Code to provide that a PTC is allowed for the coverage of a lawfully present noncitizen only if he or she is an “eligible alien” and made conforming amendments to section 1411 of the Affordable Care Act requiring Exchanges to verify applicants' “eligible alien” status. Accordingly, we proposed to add a new definition in § 155.20, update our APTC eligibility regulations at § 155.305(f)(1), and add to our verification regulations in § 155.320(c)(3)(ix) to align Exchange eligibility and verification rules with section 71301 of the WFTC legislation.
In the proposed rule, we also stated that while sections 71301 and 71302 of the WFTC legislation eliminates eligibility for PTC for certain lawfully present noncitizens, such individuals remain eligible for enrollment in the BHP, provided they meet the eligibility requirements of section 1331(e) of the Affordable Care Act and 42 CFR 600.305. Upon further consideration during the comment period, we are continuing to review how the WFTC legislation impacts the BHP.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these policies as proposed. We summarize and respond to public comments received on the proposed changes to the definition of “eligible noncitizen,” PTC eligibility for eligible noncitizens, and corresponding verification requirements below.
Comment:
Several commenters noted support for these proposals, stating that these policies will strengthen program integrity, reduce reliance on attestations, help streamline the eligibility verification newly required by the WFTC legislation, and restore the intent of the Medicaid waiting period.
Response:
We agree that finalizing the policy as proposed will strengthen
( printed page 29603)
program integrity and will ensure that we comply with the WFTC legislation by granting PTC eligibility for only eligible noncitizens as described under section 71301.
Comment:
One commenter stated that they understood the requirement to align CMS regulations with the WFTC legislation and requested CMS to clearly communicate these policy changes to interested parties, including agents, brokers, and assisters, and to evaluate the resulting impacts on the Exchange population, regional risk pools, and premium stability.
Response:
We acknowledge this comment and plan to communicate with impacted interested parties as we prepare to implement this rule in the FFE. We remain committed to continuous evaluation of Exchange implementation, including evaluating the impacts of this and other policy changes on enrollment, risk pools, and premiums.
Comment:
Many commenters stated concern with the proposal to define eligible noncitizen and to limit eligibility for APTC to U.S. citizens, U.S. nationals, and eligible noncitizens. Commenters raised concerns about the health and well-being of affected individuals, families, and communities, including anticipated reductions in access to affordable health coverage, increased rates of uninsurance and coverage losses, impact on the Exchange risk pool, and cost shifts from preventive care to emergency services. Commenters stated concern that restricting APTC eligibility to only eligible noncitizens would negatively impact populations including people living in rural communities, people with chronic conditions including asthma and blood cancer, women and especially pregnant women, people with low incomes, and young people. By restricting APTC eligibility to only eligible noncitizens, commenters stated concern that younger and healthier people would be disproportionately barred from APTC and may no longer enroll in the Exchange, which could destabilize the Exchange risk pool and increase health insurance costs for other enrollees.
Commenters also stated concerns that many of the noncitizens who will lose their APTC eligibility are low income and may be unable to afford full price health insurance, which could lead to an increased rate of uninsurance and reverse previous gains in coverage of individuals including H-2A visa holders, refugees, and asylees. Commenters noted that with more people becoming uninsured, more people would lack access to preventive care, which could increase overall health care costs and further burden emergency rooms and hospital systems that frequently provide care to patients without health insurance. Commenters also noted that this would reduce provider access, and that uncompensated care will increase healthcare costs and limit access to health coverage, with a commenter noting the particular impact on children. Commenters stated that restricting PTC eligibility to only eligible noncitizens undermines the Affordable Care Act's goal of expanding access to affordable health care services. A commenter stated concern that, due to prioritizing restricting eligibility for noncitizens, HHS was not sufficiently focused on making coverage more affordable for eligible enrollees.
Response:
We acknowledge these commenters' concerns and reiterate that while one of the goals of the Affordable Care Act is to expand access to affordable health coverage, the WFTC legislation restricts PTC eligibility to only eligible noncitizens. We believe the proposal as finalized best aligns with the statutory requirements of the WFTC legislation by only providing APTC for eligible noncitizens.
Comment:
A few commenters stated that the changes made under the proposed rule at § 155.320(c)(3) are duplicative of existing verification rules at § 155.315(c)(2). Commenters stated concern that the new verification requirements at § 155.320(c)(3) create confusion by referencing § 155.315(f)(1)-(4) rather than citizenship-specific procedures at § 155.315(c)(3). Commenters stated concern that the changes at § 155.320(c)(3)(ix) create unnecessary administrative burdens for States as they are duplicative of § 155.315(c)(2).
Response:
We clarify that the changes under § 155.320(c)(3) are not duplicative of the existing rules under § 155.315(c)(2). Section 155.315(c)(2) provides that, for applicants who attest to having a lawfully present status, the Exchange must verify their lawful presence through the Department of Homeland Security (DHS) to determine eligibility for enrollment in a QHP. The new regulations at § 155.320(c)(3) provide that, for applicants who attest to having an eligible noncitizen status, the Exchange must verify their eligible noncitizen status through DHS to determine eligibility for APTC. These requirements are handled in separate sections of our regulations because § 155.315 addresses verification requirements for criteria related to eligibility for enrollment in a QHP through an Exchange, while § 155.320 addresses verification requirements related to eligibility for APTC. For Exchanges that use the Verify Lawful Presence (VLP) Hub service, the requirements of §§ 155.315(c)(2) and 155.320(c)(3) can be met by submitting a single verification request to the service. For Exchanges that do not use the VLP Hub service, we still expect that these requirements can be fulfilled via a single transaction. Finally, we note that § 155.320(c)(3) cross-references § 155.315(f) since if there is a data matching issue (DMI) related to eligible noncitizen status, the Exchange will apply DMI procedures explained there.
Comment:
Some commenters stated concern regarding the use of the DHS's Systematic Alien Verification for Entitlements (SAVE) program, while other commenters supported the use of DHS SAVE. Commenters stated concerns about the quality of DHS SAVE, citing bad data and high error rates, and declared that SAVE is not an efficient process for verifying immigration status, which would place people at risk of not enrolling in health coverage or delayed access to coverage. Commenters also stated concern that this rule expands data transmission requirements, which will heighten fears about information sharing. State Exchanges also stated concern about the feasibility of States establishing new connections to SAVE data as required under the proposed regulation at § 155.320(c)(3)(ix)(A). Commenters also encouraged CMS to provide State-based flexibility in implementing these regulations wherever possible. Some commenters supported using SAVE as they believe it strengthens program integrity and reduces reliance on unsupported immigration attestations.
Response:
We acknowledge these comments. The provision at § 155.320(c)(3) implements the changes that the WFTC legislation made to section 1411 of the Affordable Care Act, which require verification of an individual's eligible noncitizen status with DHS. To conform with these changes, we are finalizing the updates at § 155.320(c)(3)(ix)(A) to verify eligible noncitizen status through DHS SAVE. We clarify that there is no way to verify immigration status through DHS that does not use SAVE.
This proposal does not expand data transmission requirements nor does it require State Exchanges to establish new connections to SAVE. We currently provide a connection to DHS through the VLP Hub service, which connects to DHS SAVE. For Exchanges that already use the VLP Hub service to verify applicants' lawful presence, Exchanges can meet the requirements in this rule
( printed page 29604)
by continuing to submit requests to the VLP Hub service in the same way they do today, and the VLP Hub service will be updated to indicate whether an applicant's eligible noncitizen status is verified. There are some Exchanges that currently meet the requirement to verify lawful presence with DHS through methods other than the VLP Hub service, such as through a direct connection to SAVE's web service or through the SAVE Graphical User Interface (GUI). While these Exchanges will need to establish new processes to determine whether applicants' eligible noncitizen status is verified, they will not need to submit additional data to DHS beyond what is required to verify lawful presence today, and they will not need to establish any new connections to SAVE. Using the VLP Hub service or having a direct connection to DHS SAVE is sufficient to meet the regulatory requirements in this rule and we believe this provides sufficient State-based flexibility to comply with this finalized rule.
Comment:
A few commenters emphasized the importance of providing States with technical assistance for the implementation of this provision stating that the provisions lack sufficient detail for implementation. Other commenters emphasized the importance of communicating clearly with agents, brokers, and assisters to help prevent consumer confusion. Commenters stated that CMS should provide transition protections, provide multilingual notices, and monitor for coverage losses during the implementation since many lawfully present individuals will lose coverage, experience confusion, or become part of the turnover between Medicaid-Exchange coverage. Commenters believe operational guardrails, both at the Exchange level and at the consumer level, that reduce the risk of coverage loss in addition to plain language notices, would help reduce the number of individuals who might mistakenly lose coverage or APTC as a result of these provisions.
Response:
We acknowledge the concerns that commenters expressed about providing assistance to States, agents, brokers, assisters, and consumers, and we will provide technical assistance in response to these concerns in the form of webinars and technical documentation. We plan to leverage existing channels for outreach and education during the individual Exchange Open Enrollment Period, including multilingual channels, to ensure impacted consumers are aware of the changes happening because of this final rule. We intend to monitor changes in enrollment for the impacted population. We are committed to both providing clear and accurate guidance to our partners, and to ensuring compliance with section 71301 of the WFTC legislation such that APTC for noncitizens is limited to only eligible noncitizens, while allowing all lawfully present individuals to remain QHP eligible (if they satisfy all other eligibility requirements). Again, we clarify that the use of the VLP Hub Service is sufficient to meet the verification requirements of this rule.
Comment:
Some commenters stated concern about the impact this proposal will have on the BHP. These commenters were concerned about the potential for coverage loss and churn between insurance affordability programs, the impact on coverage affordability and uncompensated care, and the impact on State government finances and State policy flexibility. Relatedly, several commenters requested that HHS consider providing future guidance relating to transition periods and operational safeguards, as well as provide States with data analysis to minimize coverage loss.
Response:
We acknowledge the commenters' concerns regarding the impact to coverage availability, State finances, and providers. As stated previously, we are implementing these provisions as directed in the WFTC legislation, and we believe this proposal is best aligned with the statute. We intend to monitor changes in enrollment for the impacted population and to BHP funding to States generally. We will be available to provide individual technical assistance to States operating BHPs. We are committed to both providing clear and accurate guidance to our partners, and to ensuring compliance with section 71301 of the WFTC legislation such that Federal BHP funding to States for noncitizens is calculated based only on eligible noncitizens.
Comment:
One commenter stated concern that the changes to the BHP in the proposal add administrative burdens for rural health systems without improving rural access.
Response:
We acknowledge the commenter's concerns and reiterate that the WFTC legislation restricts PTC eligibility for noncitizens, and by extension, Federal payments to States that operate a BHP to only eligible noncitizens. We believe the proposal as finalized best aligns with the statutory requirements of the WFTC legislation by limiting APTC for noncitizens to only those who are eligible noncitizens. Specifically regarding rural health access, we are currently administering the $50 billion Rural Health Transformation Program, which was authorized by section 71401 of the WFTC legislation.
Comment:
One commenter stated concerns about the impact of this proposal on State finances and on changes to BHP data reporting requirements, including systems changes.
Response:
We appreciate the commenter's concerns and will seek to minimize additional reporting burden and systems changes on States that operate BHP programs. Further guidance will be provided regarding reporting changes, and we are committed to providing individual technical assistance to States that operate a BHP.
9. Disallow APTC for Individuals Who Are Ineligible for Medicaid Due to Their Immigration Status and Have Income Below 100 Percent of the FPL (§ 155.305(f)(2))
Section 71302 of the WFTC legislation amended 26 U.S.C. 36B(c)(1) by striking subparagraph (B), which provided that an individual could be considered an applicable taxpayer, and therefore eligible for PTC, if they had household income under 100 percent of the FPL and were a noncitizen lawfully present in the United States who was ineligible for Medicaid due to their immigration status. Because 26 U.S.C. 36B(c)(1)(B) was repealed, such noncitizens are no longer eligible for PTC. Under section 1402(g) of the Affordable Care Act, which provides that an individual is only eligible for CSRs if they are also eligible for PTC for that month, such noncitizens are also no longer eligible for CSRs. This provision is effective for plan years beginning after December 31, 2025.
In the 2027 Payment Notice proposed rule (91 FR 6342), we proposed to remove § 155.305(f)(2) to align regulations with section 71302 of the WFTC legislation. Section 155.305(f)(2) currently requires an Exchange to determine a tax filer eligible for APTC if the Exchange determines that the tax filer is expected to have household income of less than 100 percent of the FPL for the benefit year for which coverage is requested, the tax filer or one or more applicants for whom the tax filer expects to be eligible for a personal exemption is lawfully present and ineligible for Medicaid due to their immigration status, and the tax filer otherwise meets APTC eligibility requirements. Section 71302 of the WFTC legislation amended section 36B of the Code such that PTC is no longer allowed for this population. We stated in the proposed rule that removing
( printed page 29605)
§ 155.305(f)(2) would align Exchange APTC eligibility rules with the Code's PTC eligibility rules, as required by section 1411(a)(2)(A) of the Affordable Care Act.
We also proposed conforming amendments to the verification regulations at § 155.320(c)(3)(iii)(A) and to SEP regulations at § 155.420(d)(13), to remove references to § 155.305(f)(2) and to the population described in that provision.
Additionally, we noted in the proposed rule that section 71302 of the WFTC legislation will impact Federal payments to States that operate BHPs for individuals enrolled in the BHP who are ineligible for Medicaid due to their immigration status and with incomes below 100 percent of the FPL. As stated previously, under section 1331(d)(3)(A)(i) of the Affordable Care Act and 42 CFR 600.605(a), Federal BHP payments to States include 95 percent of the PTC under section 36B of the Code. Following the repeal of 26 U.S.C. 36B(c)(1)(B) by section 71302 of the WFTC legislation, noncitizens who are lawfully present, ineligible for Medicaid due to immigration status, and have household income below 100 percent of the FPL are no longer eligible for PTC. Therefore, States will no longer receive Federal BHP payments attributable to members of this population who are BHP enrollees beginning January 1, 2026.[143]
Section 71302 of the WFTC legislation is applicable beginning January 1, 2026. Section 71302 is self-effectuating, and Exchanges are required to operationalize the changes required to implement these new statutory requirements beginning with eligibility determinations for the PY 2026 even though conforming changes to Exchange regulations will not yet have been finalized.
We proposed to remove § 155.305(f)(2) and make conforming updates to §§ 155.320(c)(3)(iii)(A) and 155.420(d)(13) to align Exchange regulations with section 71302 of the WFTC legislation. We stated that removing § 155.305(f)(2) and updating § 155.320(c)(3)(iii)(A) would align Exchange APTC eligibility and verification rules with the statutory changes enacted by section 71302 of the WFTC legislation. We further proposed conforming amendments to § 155.420(d)(13) to remove the SEP triggering event for individuals with household income under 100 percent of the FPL who did not enroll in coverage while waiting for HHS to verify their citizenship or immigration status, as the intent of this SEP was to provide an enrollment opportunity for individuals described at § 155.305(f)(2) who were not able to verify their eligibility for APTC within their original enrollment window.
We sought comment on this proposal.
After consideration of comments, and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. Section 71302 of the WFTC legislation, which no longer allows PTC for lawfully present noncitizens who are ineligible for Medicaid due to their immigration status and have household income under 100 percent of the FPL, was effective January 1, 2026. The provisions in this section of the rule, which align HHS regulations with this new statutory requirement, are effective upon enactment. We summarize and respond to public comments received on the proposed change below.
Comment:
A few commenters stated support for the proposals and were specifically supportive of front-end verification measures and reduced reliance on self-attestation in the Exchange context, stating these measures will strengthen program integrity. The commenters requested CMS to take more decisive action to eliminate self-attestation entirely for the purpose of improving program integrity.
Response:
We appreciate the comment and acknowledge that finalizing the policy as proposed will strengthen program integrity and will ensure that we comply with the WFTC legislation.
Comment:
One commenter stated concern about the lack of updated guidance, citing risks to uniform enforcement and inconsistent application of Federal law.
Response:
We acknowledge the comment and clarify that since this provision is already in effect per the WFTC legislation, we are updating our regulation to align with the legislation. We acknowledge and recognize the need for updated and timely guidance, and wish to clarify that on December 22, 2025, we published guidance related to this proposal.[144]
Comment:
Many commenters stated concern regarding the proposal to no longer allow APTC for noncitizens who are ineligible for Medicaid due to their immigration status and who have household incomes under 100 percent of the FPL, in alignment with section 71302 of the WFTC legislation. Commenters raised concerns about the health and well-being of affected individuals, families, and communities, including anticipated reductions in access to affordable health coverage, increased rates of uninsurance, impacts to the Exchange risk pool, and cost shifts from preventive care to emergency services. Commenters stated concerns that these provisions would negatively impact populations including people living in rural communities, people with chronic conditions including asthma and blood cancer, women and especially pregnant women, people with low incomes, and young people. A commenter stated concern that, due to prioritizing restricting eligibility for noncitizens, HHS was not sufficiently focused on making coverage more affordable for U.S. citizens.
Commenters stated concern that by disallowing APTC for consumers ineligible for Medicaid because of their immigration status, who have income below 100 percent of the FPL, many immigrants who lose their APTC eligibility are already low income and would be unable to afford full price health insurance, leading to gaps in coverage, an increased rate of uninsurance, and financial strain on immigrant families. Commenters noted that with more people becoming uninsured, more people would lack access to preventive care that could increase overall health care costs and further burden emergency rooms and hospital systems, which frequently serve patients without health insurance. Commenters additionally stated concerns about the increased burden of verification of immigration status, potentially deterring those eligible for coverage due to concerns about how their immigration status data may be used.
Response:
We acknowledge the commenters' concerns and reiterate that the WFTC legislation prohibits PTC for this population. We believe the proposal properly implements the statutory requirements of the WFTC legislation.
Comment:
One commenter stated support for the proposal, stating it would close existing loopholes that allow lawful permanent residents, parolees, and those granted conditional entry to receive the PTC if their income is below the FPL in non-expansion States or below 138 percent of the FPL in expansion States. The commenter noted that under the previous law, noncitizens in the aforementioned groups were able to access premium
( printed page 29606)
subsidies that were unavailable to U.S. citizens in the same income categories.
Response:
We agree that finalizing this proposal will prevent certain noncitizens with incomes below 100 percent of the FPL from receiving APTC and will therefore better align with the PTC eligibility rules that apply to U.S. citizens.
Comment:
A few commenters opposed the proposal, stating it would harm low-income lawfully present individuals by eliminating a pathway to affordable coverage. The commenters also stated this proposal would undermine the Affordable Care Act's goal of expanding coverage, and they requested HHS support policies that expand access to coverage rather than limit it.
Response:
We acknowledge commenters' concerns regarding the potential impacts on access to coverage for individuals who will no longer be eligible for APTC because of this change. As noted in section III.D.8. of this rule, while one of the goals of the Affordable Care Act is to expand access to affordable health coverage, section 71302 of the WFTC legislation eliminates PTC eligibility for this population. We have interpreted section 1411(a)(2)(A) of the Affordable Care Act to require an Exchange to align its APTC eligibility rules with the Code's PTC eligibility rules, and we are therefore proposing to follow these rules for APTC eligibility. We are therefore finalizing this policy to align with the statutory requirements.
Comment:
One commenter stated that eliminating Federal BHP funding for lawfully present noncitizens with income below 100 percent of the FPL who are ineligible for Medicaid due to their immigration status exceeded the requirements of the WFTC legislation.
Response:
We do not agree that these changes exceed the requirements of the WFTC legislation. Section 71302 of the WFTC legislation eliminates eligibility for PTC for lawfully present noncitizens who are ineligible for Medicaid due to their immigration status and have household income below 100 percent of the FPL. Because Federal BHP payment amounts are based in part on the PTC that would have been provided to eligible individuals, these individuals will no longer be included in the calculation of Federal funding to States that operate a BHP. Accordingly, we are finalizing this policy as proposed. See the above preamble for additional discussion of the impact of section 71302 of the WFTC legislation on Federal BHP payments.
Comment:
Some commenters stated concern for the impact this proposal will have on the BHP. These commenters were concerned regarding the potential for coverage loss and churn between insurance affordability programs, the impact on coverage affordability and uncompensated care, and the impact on State government finances and State policy flexibility. Relatedly, several commenters requested that CMS make certain considerations regarding the transition period, such as additional guidance and operational safeguards, and make additional data analysis available to States to minimize coverage loss.
Response:
We acknowledge commenters' concerns. As discussed in detail in our response to comments in section III.D.8. of this final rule, we are finalizing these proposals to conform with the WFTC legislation. We note that per the CMCS Informational Bulletin issued December 10, 2025, “Basic Health Program; Federal Funding Methodology for Program Year 2026,” CMS will exercise enforcement discretion for a period of 3 years and will not take compliance action against any State that does not provide BHP coverage to this population between January 1, 2026, through December 31, 2028. We also will be available to provide individual technical assistance to States operating BHPs.
Comment:
One commenter stated concern that the changes to the BHP in this proposal add administrative burdens for rural health systems without improving rural access.
Response:
As discussed in detail in our response to comments in section III.D.8, while we appreciate the commenter's interest in this issue, we are finalizing these proposals to conform with the WFTC legislation.
10. Failure To File and Reconcile (FTR) Policy (§ 155.305)
In the 2027 Payment Notice proposed rule (91 FR 6342), we proposed to amend paragraph § 155.305(f)(4) so that in PY 2028 and beyond, all Exchanges may not determine a tax filer or their enrollee eligible for APTC if: (1) HHS notifies the Exchange that APTC were paid on behalf of the tax filer, or their spouse if the tax filer is a married couple, for 1 year for which tax data would be utilized for verification of household income and family size, and (2) the tax filer, or the tax filer's spouse if the tax filer files jointly, did not comply with the requirement to file a Federal income tax return and reconcile APTC for that year (referred to as the “1-tax year FTR” process). We also proposed that, at the option of the Exchange, an Exchange may choose to early adopt the 1-tax year FTR policy in PY 2027 if it has the resources and capability to do so, or it can continue to administer a 2-tax year FTR process until PY 2028. We stated that if this proposal is finalized, Exchanges on the Federal platform would adopt the 1-tax year FTR process in PY 2027, as HHS has the resources available to do so.
As background, consumers who receive APTC are required to file an income tax return for the year of coverage pursuant to section 6011(a) of the Code and regulations prescribed by the Secretary of the Treasury. Section 36B(f) of the Code requires taxpayers to reconcile their APTC under section 1412 of the Affordable Care Act with their PTC allowed under section 36B of the Code. FTR regulations, implemented pursuant to the Secretary of HHS' general rulemaking authority under section 1321(a) of the Affordable Care Act, facilitate compliance with those requirements and were implemented as part of the 2012 Exchange Establishment Rule (77 FR 18352 through 18353). Exchange enrollees whose tax filer fails to comply with the requirement to file an income tax return and reconcile APTC as described in § 155.305(f)(4) are referred to as having failed to “file and reconcile.” These individuals are referred to as having an FTR status, and the Exchanges conduct the FTR process to identify such individuals.
In the Exchange Establishment Rule, we finalized the FTR policy in part to prevent a primary tax filer or spouse who has failed to comply with tax filing rules from accumulating additional Federal tax liabilities due to overpayment of APTC. FTR was originally finalized and implemented as a 1-tax year FTR policy and HHS began FTR operations in late 2015. FTR continued as a 1-tax year policy until it was paused in 2021 during the COVID-19 public health emergency (PHE). FTR operations were paused due to concerns that consumers who had filed and reconciled would lose APTC due to IRS processing delays resulting from IRS processing facility closures and a corresponding processing backlog of paper filings.[145]
During the PHE pause, we amended the FTR process such that an Exchange could not determine a tax filer or their enrollee ineligible for APTC until they
( printed page 29607)
have failed to file a Federal income tax return and reconcile APTC for 2-consecutive tax years in the 2024 Payment Notice (88 FR 25814). Specifically, this 2-tax year FTR policy prohibits an Exchange from determining a tax filer or their enrollee eligible for APTC if: (1) HHS notifies the Exchange that APTC were paid on behalf of the tax filer, or their spouse if the tax filer is a married couple, for 2 consecutive years for which tax data would be utilized for verification of household and family size, and (2) the tax filer did not comply with the requirement to file a Federal income tax return and reconcile APTC for those years. We made this change to address operational challenges that required Exchanges to determine someone ineligible for APTC without having up-to-date information on the tax filing status of tax filers, to help consumers who may be confused or may have received inadequate education on the requirement to file and reconcile, to promote continuity of coverage for consumers who may not be aware of the requirement to file and reconcile, and to reduce the administrative burden on HHS.
When we adopted this 2-tax year FTR process, we acknowledged it could place consumers at risk of increased tax liability. To mitigate this concern, in the 2025 Payment Notice (89 FR 26298 through 26299), we required Exchanges to issue FTR warning notices for enrollees in Exchanges who have not filed and reconciled for 1-tax year. We further mitigated this concern when, in the 2026 Payment Notice (90 FR 4424), we also required Exchanges to issue associated warning notices for enrollees in Exchanges who have been identified as not filing and reconciling for 2 consecutive tax years. When we implemented the 2-tax year FTR policy, we also acknowledged the risk for improper enrollment by consumers who know they can ignore their FTR status for an additional year but concluded these instances would be limited as the majority of enrollees comply with FTR. Despite the potential for large tax liabilities and the risk of improper enrollment, we concluded that this policy would have a positive impact on consumers, while still ensuring program integrity as it would provide better continuity of coverage for consumers who may not be aware of the requirement to file and reconcile. We noted that we would continue to monitor the implementation of this new policy, including whether certain populations continue to experience large tax liabilities, and would consider whether additional guidance, or any additional policy changes in future rulemaking, are necessary.
In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), we finalized a return to the 1-tax year FTR process. Specifically, we finalized at § 155.305(f)(4)(iii) that, through the end of PY 2026, Exchanges would be required to find tax filers (or their enrollees) ineligible for APTC if they had a 1-tax year FTR status for PY 2026 only. The finalized regulation provided that Exchanges would revert to the 2-tax year FTR process beginning in PY 2027. We did so for a number of reasons. First, we stated in the 2025 Marketplace Integrity and Affordability final rule that we believe the prior 2-tax year FTR process places a substantially higher number of tax filers at a greater risk of accumulating increased tax liabilities when filing their Federal income taxes. Second, we stated that we believe that the 2-tax year FTR process could incentivize tax filers to not file and reconcile because they would be allowed to keep APTC eligibility for an additional year without filing their Federal income tax return and reconciling APTC. This policy was stayed by the District Court for the District of Maryland in
City of Columbus et al.
v.
Kennedy et al.,
on August 22, 2025. The judge stayed this particular provision after concluding the plaintiffs were likely to succeed in arguing the 1-tax year FTR policy is contrary to law. Due to the Court's decision, the 2-tax year policy remained in place for PY 2026 for all Exchanges.
Under section 36B(b)(1) of the Code, no PTC is allowed for any month that is not a “coverage month.” On July 4, 2025, Congress passed and President Trump signed the WFTC legislation which, under section 71303, amended the definition of “coverage month” under section 36B(c) of the Code for taxable years after December 31, 2027, to provide that a “coverage month” will not include, for any individual enrolled in a QHP through an Exchange, any month for which the Exchange does not meet the requirements of § 155.305(f)(4)(iii), as added by the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074). Section 155.305(f)(4)(iii) reflects the 1-tax year FTR policy proposed in this rule. Thus, under section 71303 of the WFTC legislation, for taxable years beginning after December 31, 2027, no APTC is payable on behalf of any enrollee in an Exchange for any month in which the Exchange has not implemented a 1-tax year FTR policy.
We proposed that for PY 2028 and beyond, an Exchange must determine a tax filer or their enrollee ineligible for APTC, and that, at an Exchange's option, an Exchange may make such a determination for PY 2027 if: (1) HHS notifies the Exchange that APTC was paid on behalf of the tax filer, or their spouse if the tax filer is married, for a year for which tax data would be utilized for verification of household income and family size; and (2) the tax filer, or their spouse if the tax filer is married, did not comply with the requirement to file a Federal income tax return and reconcile APTC payments with PTC the tax filer is allowed to claim on their tax return for that year. If the Exchange does not choose to adopt the 1-tax year FTR policy for PY 2027, they must determine a tax filer or their enrollee ineligible for APTC if: (1) HHS notifies the Exchange that APTC was paid on behalf of the tax filer, or their spouse, if the tax filer is a married couple, for 2 consecutive tax years for which tax data would be utilized for verification of household income and family size; and (2) the tax filer, or their spouse if the tax filer is a married couple, did not comply with the requirement to file a Federal income tax return and reconcile APTC payments with PTC the tax filer is allowed to claim on their tax return for those 2 consecutive years.
We proposed to amend the language at § 155.305(f)(4) to clearly reflect an Exchange's option to implement either the 1-tax year FTR policy or 2-tax year FTR policy for PY 2027 and the 1-tax year FTR policy for PY 2028 and beyond. We proposed to reorganize paragraph (f)(4) to include three sections—Definitions, APTC eligibility, and Notices. We also proposed to revise the language to ensure that notices are sent to consumers that reflect whether the Exchange is implementing the 1-tax year or 2-tax year FTR policies for PY 2027 coverage, and that the Exchange will implement the 1-tax year FTR policy for PY 2028 coverage. In addition, we stated that we are making non-substantive changes to improve the readability and clarity of the regulatory text. We stated that we believe this change is important because it would be imprudent for Exchanges to implement the 2-tax year FTR policy in PY 2028 and thereafter due to the impacts on the definition of coverage month under section 36B(c) of the Code, and allowing Exchanges to voluntarily adopt the 1-tax year policy for PY 2027 gives Exchanges the operational flexibility they need to navigate the vast pre-enrollment verification changes also imposed in section 71303 of the WFTC legislation.
While the revised definition of coverage month that compels Exchanges to implement the 1-tax year FTR policy
( printed page 29608)
is scheduled to take effect for PY 2028 under the WFTC legislation, it is important to exercising existing authorities under the Affordable Care Act and its implementing regulations to implement a 1-tax year FTR policy beginning with enrollments for PY 2027 to protect enrollees from accumulating tax liabilities. Until 2026, the amount of APTC that some consumers were required to repay when filing their Federal income tax return and reconciling their APTC was limited by section 36B(f)(2)(B) of the Code based on their income level as a percentage of the FPL. Section 71305 of the WFTC legislation eliminated those excess APTC recapture limits for tax years beginning after December 31, 2025. As a result, consumers with excess APTC will have their tax liability increased by the entire amount of the excess APTC. Given this, we stated in the proposed rule that we are even more concerned about the potential for high tax liabilities that could accumulate if consumers do not file their Federal income tax returns and reconcile APTC. The current 2-tax year FTR process potentially provides up to 18 months after an initial FTR notice is received for a tax filer to comply with the requirement to file and reconcile APTC received, which would expose the tax filer to up to 18 additional months of excess APTC if the tax filer does not file and reconcile. We previously concluded in the Marketplace Integrity and Affordability final rule (90 FR 27074) that this does not provide reasonable protection against accumulating tax liabilities.[146]
By switching from a 2-tax year FTR process to a 1-tax year FTR process for PY 2027, we stated in the proposed rule that our hope is that consumers would not inadvertently be responsible for repaying the entirety of 18 months of excess APTC if they do not file and reconcile, which is likely a significant financial hardship for many consumers receiving APTC.
The 2025 Marketplace Integrity and Affordability final rule reinstated the 1-tax year FTR policy, but to balance competing concerns, the rule sunset the policy automatically after the end of PY 2026. At the time, we concluded that the 1-tax year FTR policy was needed immediately to reduce the number of improper APTC payments in Exchanges on the Federal platform. However, we also considered that the policy's utility could be less apparent in the context of the expiration of the expanded subsidies and fully-subsidized benchmark plans, which removes much of the incentive for unscrupulous agents, brokers, and web-brokers to fraudulently enroll consumers into Exchange coverage who then may not know they need to file Federal income taxes and reconcile APTC. While we have made progress in reducing improper unauthorized enrollments over the past year, there remains a substantial number of unauthorized enrollments on the Federal platform, and there remains significant risk that persons enrolled without their knowledge will be subjected to surprise tax liability. Finalizing the 1-tax year FTR will mitigate the risk that individuals enrolled in Exchange coverage without their knowledge will amass unintended tax liabilities for 2 years.
When we finalized the sunset of the 1-tax year policy in the finalized 2025 Marketplace Integrity and Affordability final rule, commenters also expressed the following concerns: (1) that the 1-tax year FTR process may result in coverage losses because the tax filing process is complex and consumers are not fully aware of the requirements to file and reconcile, (2) that the 1-tax year FTR process could have a negative impact on the risk pool, and (3) that the 1-tax year process negatively impacts low-income consumers who have a more difficult time predicting and verifying income due to the unpredictable nature of their income. While we acknowledged these concerns in the proposed rule, we stated that we believe that for PY 2027, the overriding policy need for the Federal Exchange is to be able to remove unauthorized enrollments from the Exchange, and the 1-tax year FTR policy enables us to do that better than a 2-tax year FTR policy. As for State Exchanges, which do not all face the same problem for unauthorized enrollments, we stated that we believe that the flexibility to be able to nimbly respond to whatever the Court decides for the final decision in
City of Columbus et al.
v.
Kennedy et al.,
as well as during the implementation of all the other requirements imposed by the WFTC legislation, is the utmost policy goal for PY 2027. However, for PY 2028, our previously stated concerns, which are still valid, become secondary to the goal of ensuring that consumers are eligible for APTC, because APTC is essential for the Exchanges to function as designed in the Affordable Care Act. This is due to the requirement of Exchanges to operate the 1-tax year FTR policy in order for a month to be considered a “coverage month,” thereby ensuring that consumers are eligible for APTC.
In the proposed rule, we stated that we also understand that State Exchanges and other interested parties may have planned their FTR operations based on the sunset of the 1-tax year policy as finalized in the 2025 Marketplace Integrity and Affordability final rule. However, due to the stay imposed by the Court, State Exchanges have not implemented the 1-tax year FTR process for 2026. If the stay continues through PY 2026, they would have nothing to sunset in PY 2027 (that is, the 2-tax year FTR policy would continue). Alternatively, if HHS prevails in
City of Columbus et al.
v.
Kennedy et al.
during PY 2026 and the 1-tax year FTR policy is reinstated for the remainder of the plan year, it would be a burden for Exchanges to revert to a 2-tax year FTR policy in PY 2027 and then revert back to a 1-tax year FTR policy again in PY 2028, if that component of this proposal is finalized. Taking both these potential scenarios into account, we stated in the proposed rule that we believe it would be most prudent to allow State Exchanges the option to choose between a 1- and 2-tax year FTR process for PY 2027. Additionally, as State Exchanges do not report the same problems with unauthorized enrollments as those currently facing the FFEs, there is less reason to require the 1-tax year policy in 2027. Further, we stated that it could be overburdensome to require State Exchanges to implement the 1-tax year FTR policy due to limited operational resources while they implement other requirements of the WFTC legislation.
A review of plan selections during the 2026 open enrollment period shows 29 percent of people enrolled in fully subsidized plans through the Federal platform.[147]
Thus, there remains an opportunity for unscrupulous agents, brokers, and web-brokers to enroll people without their knowledge. In addition, HHS removed APTC from an estimated 430,000 enrollees as of January 1, 2026 for failing to file their Federal tax return and reconcile APTC for 2 consecutive tax years (2023 and 2024 tax years) in accordance with the 2-tax year FTR policy.[148]
This population is already larger than the 235,000 enrollees who lost APTC
( printed page 29609)
eligibility as part of FTR operations for PY 2025 [149]
and this is just the first stage in the process for PY 2026. In the 2025 Marketplace Integrity and Affordability proposed rule, we stated that we believe that FTR status may be an indicator that a current enrollee entering the OEP has income that makes the household ineligible for APTC. This is because, for some households, the income requirement to file a tax return is approximately 100 percent FPL which is the minimum household income to qualify for APTC.[150]
People who inflate their income to qualify for APTC will often have an income low enough to, absent the receipt of APTC, not require them to file taxes. In this case, the FTR status likely reflects a lack of understanding of the need to file taxes based on the receipt of APTC which, if they still think they do not meet the filing requirement based on their income, means they are likely to have an income too low to meet the APTC eligibility threshold. In addition, someone improperly enrolled entirely without their knowledge would also not know to reconcile. Considering our prior analyses that suggest FTR status is a strong indicator that a current enrollee is ineligible for APTC and the growth in enrollees with a 2-tax year FTR status for PY2026, we stated in the proposed rule that we remain very concerned about the number of consumers in the Exchange that were potentially improperly enrolled and remain enrolled.
Though the enforcement of the 1-tax year policy for PY 2026 was stayed after the District Court concluded it would likely be found contrary to law, we stated in the proposed rule that we continue to believe we have a strong statutory basis for applying the 1-tax year policy. In the 2025 Marketplace Integrity and Affordability proposed rule (90 FR 12961), we stated HHS' belief that the Affordable Care Act does not allow HHS to determine someone eligible for APTC if they failed to meet the requirement to file a tax return. Sections 6011 and 6012 of the Code, as implemented under 26 CFR 1.6011-8, require enrollees who receive APTC to file a tax return and reconcile the APTC. Notwithstanding, the District Court reasoned that the policy was likely unlawful because nothing in the statute expressly conditions eligibility on reconciling tax credits. However, our analysis of the statute has focused on the importance of filing a tax return, not reconciling APTC. That's because the tax return is a critical element of the income verification process to qualify for APTC under the statute. As such, filing a tax return is a means of verifying a condition of eligibility and not itself a condition of eligibility. As we explained in the Marketplace Integrity and Affordability proposed rule, the statute requires APTC to be set on the basis of the individual's household income for the most recent taxable year for which information is available. Therefore, the income reported on the tax return for the most recent taxable year establishes the starting point for verifying whether an applicant's income meets the requirements to qualify for APTC. As discussed previously, when the IRS does not have tax return information to verify an applicant's income, section 1412 of the Affordable Care Act requires HHS to establish alternative procedures to determine APTC when there is a change in circumstances or “in cases where the taxpayer was not required to file a return . . .” Because section 1412(b)(2)(B) only references cases where a tax filer was
not required
to file a return, we stated in the proposed rule that we do not believe an applicant who fails to meet the requirement to file a return qualifies for this alternative process for determining APTC. Therefore, to determine and verify household income, it is imperative that consumers file a Federal income tax return when they are required to do so.
While we had previously intended to sunset the 1-tax year policy in PY 2026, due to both the inability to implement it in PY 2026 due to a judicial stay in
City of Columbus et al.
v.
Kennedy et al.,
as well as the WFTC legislation preventing consumers from receiving APTC in any Exchanges not implementing the 1-tax year policy beginning in PY 2028, we stated in the proposed rule that we believe it is best to implement the 1-tax year policy for PY 2028 for all Exchanges, with the option for Exchanges to early adopt for PY 2027 or continue operating the 2-tax year policy for PY 2027. As mentioned previously, we are giving Exchanges the option to continue operating the 2-tax year policy during PY 2027 because, while the Federal Exchange has the resources to early adopt the 1-tax year FTR policy in 2027, many State Exchanges face different financial constraints. This may be particularly true in 2027 when States will have to also implement the other pre-enrollment verification changes required by the WFTC legislation. Therefore, in light of these considerations, we proposed to revise § 155.305(f)(4) to require Exchanges to find consumers ineligible for APTC after they or their tax filer have been determined to have failed to file and reconcile for 1 tax year beginning in PY 2028, or in PY 2027 at the option of the Exchange. We also proposed in § 155.305(f)(4) that an Exchange must operate the 2-tax year FTR process in PY 2027 if they do not elect to operate the 1-tax year FTR process.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed updates to the FTR policy below.
Comment:
Many commenters opposed the proposed policy to revert to the 1-year FTR policy as an option for PY 2027, stating that the 2-year policy strikes a better balance between ensuring that enrollees file their Federal income taxes and reconcile APTC, while also allowing for the fact that the IRS data is often delayed due to long processing times, especially for paper filers and amended Federal income tax returns.
Response:
While we agree that the IRS has previously suffered from long IRS processing times of Federal income tax returns, particularly during the Covid-19 public health emergency, and especially for those filing paper and amended income tax returns, we do not believe this is a sufficient reason to maintain the current 2-year FTR process for an additional year due to the need to protect consumers who are unknowingly enrolled from accruing 3 years of tax liability rather than just 2 years. For example, a low-income consumer below the tax filing threshold could have been fraudulently enrolled in coverage with APTC for year 1, year 2, and year 3 by a third party, but have an offer of affordable employer coverage that disqualifies them from PTC. Under the 2-year policy, the consumer could potentially accrue an unknown tax liability of APTC received in years 1, 2, and 3 before losing APTC either through the strip process at the end of December or the FTR Recheck process during the following spring. They would need to undertake a process to demonstrate that they were fraudulently enrolled in this coverage and have their Form 1095-A voided by an Exchange to demonstrate that they do not owe excess APTC. We also note that, as of May 2, 2026,
( printed page 29610)
electronically filed returns are generally processed within 21 days according to the current timeline on irs.gov. Additionally, as of the same date, original paper filed returns received in March of 2026 were being processed, while amended paper filed returns received in February 2026 were being processed.[151]
Further, we attempt to mitigate the IRS processing times with the FTR Recheck process, which allows enrollees who have filed later in the year to attest that they did in fact file and reconcile, while maintaining eligibility for APTC for the following coverage year until FTR status is then rechecked early in the coverage year. While we are unsure whether all State Exchanges provide the same FTR Recheck process that Exchanges on the Federal platform provide, due to the way that some State Exchanges integrate the FTR process into other periodic data matching processes to obscure FTI, we are providing flexibility for State Exchanges to delay the implementation of the 1-year FTR process until PY 2028. During that FTR Recheck process, Exchanges on the Federal platform compare attestations with more recently updated IRS data to verify whether an enrollee did in fact file and reconcile. If the IRS data indicates that the tax filer did not file and reconcile, then the tax filer or their enrollee receives a notification before a final check of FTR status before the Exchange terminates APTC. Consumers who believe they have erroneously been found ineligible for APTC should contact the Marketplace Appeals Center.
Comment:
Many commenters who are State Exchanges thanked CMS for the flexibility to implement a 1-year FTR policy beginning in PY 2028 because they do not have the operational resources to do so beginning in PY 2027. Conversely, one commenter noted that we should finalize the requirement for State Exchanges to align with the one-year FTR policy in the WFTC legislation in PY 2027, along with the Federal Exchanges.
Response:
We continue to believe that flexibilities for State Exchanges to still conduct the 2-year FTR process in FY 2027 is necessary as we are aware that making the operational changes required for the 1-year policy, including eligibility logic changes and updating notices, is contingent on State budgets and States having the capacity to update their Exchange eligibility logic to shift back to a 1-year FTR policy.
Comment:
Many commenters stated concern that the proposed 1 year policy in PY 2027 would increase coverage loss, especially among those who are lower-income and homeless as they would no longer be able to afford their monthly Exchange premium after APTC is terminated, as well as having a negative impact on the risk pool as those who are sicker are more motivated to navigate administrative burdens to get coverage versus healthier individuals, and thus raising premiums. Relatedly, many commenters supported ensuring that consumers can maintain coverage and also were concerned about the potential increase in IRS delays and the impact that delayed data could have on the 1 year process. Many commenters also believed that a larger tax bill for consumers who faced repayment of excess APTC is preferable over a loss of healthcare coverage. Some commenters also noted that it is much harder for consumers who lack stability in their lives (that is, lack of stable income or a lack of stable housing) to provide documentation to fulfill verification requirements such as FTR compared to consumers who do have stable income and stable housing.
Response:
We understand commenters' concerns about the risk of coverage losses among lower-income individuals. However, we believe that the continued program integrity concerns stemming from improper enrollments merit the need for the option of the early adoption of the 1-year FTR policy. Recently, two executives were sentenced to 20 years in prison for fraudulently enrolling vulnerable consumers experiencing homelessness and mental health and substance abuse disorders.[152]
Consumers enrolled through this type of fraud are more likely to have not filed taxes due to their lower income and vulnerable position, and a 1-year FTR policy would remove them from subsidized coverage more quickly. While we acknowledge that it is harder for consumers who are struggling to file their taxes, we firmly believe that the tax return is the basis of determining a consumer's eligibility for APTC and thus is crucial to the program integrity of Exchanges. Having the consumer's most recent tax return increases the likelihood that the Exchange can verify their income using a trusted data source from another government agency, thereby driving down verification costs and helping to ensure that consumers are eligible for their Exchange coverage. We do not agree with commenters who believe that a larger tax bill for consumers who face repayment of excess APTC is preferable over a loss in healthcare coverage. We also note that for those who have lost coverage, many hospitals have charity care programs where consumers can apply to reduce their medical debt. We further note that, if an enrollee believes that they lost APTC erroneously due to FTR, they can file an appeal with the Marketplace Appeals Center.
Comment:
Many commenters stated concern that HHS does not have the statutory authority to require any failure to file and reconcile process until PY 2028 due to the stay in the
City of Columbus
v.
Kennedy
litigation. A few commenters also stated disagreement with HHS' argument regarding its statutory authority to conduct FTR at all until PY 2028. They noted that there is nothing included in section 1411(b) of the Affordable Care Act that conditions eligibility for APTC on filing a Federal income tax return and reconciling APTC. They also noted that they believe that CMS should be able to look at any year's tax return to determine eligibility, and thus that not filing 1 year's return should not be the basis for denying APTC. One commenter also noted that FTR status affects a consumer's future PTC.
Response:
As we stated in the proposed rule, we believe that we have a statutory basis for applying the 1-year FTR policy before PY 2028. In the 2025 Marketplace Integrity and Affordability proposed rule (90 FR 12961), we stated that we believe that the Affordable Care Act allows HHS to determine someone ineligible for APTC if they failed to meet the requirements to file a Federal income tax return as the tax return provides a main basis for establishing an accurate income estimate. Sections 6011 and 6012 of the Code, as implemented under 26 CFR 1.6011-8, require enrollees who receive APTC to file a tax return and reconcile the APTC. Notwithstanding, the District Court in
City of Columbus
v.
Kennedy
reasoned in the stay that the policy was likely unlawful because nothing in the statute conditions eligibility on filing a Federal income tax return and reconciling tax credits. However, our analysis of the statute has focused on the importance of filing an income tax return, not reconciling APTC. That is because the income tax return is a critical element of the income verification process to qualify for APTC under the statute. As we stated, filing a Federal income tax return is a means of verifying
a
( printed page 29611)
condition of eligibility
for APTC, and is not, in itself, a condition of eligibility. As we previously noted in the 2025 Marketplace Integrity and Affordability proposed rule, the statute requires APTC to be set on the basis of the individual's household income for the most recent taxable year for which information is available. Therefore, the income reported on the Federal income tax return for the most recent taxable year establishes the starting point for verifying whether an applicant's income meets the requirements to qualify for APTC. As discussed previously, when the IRS does not have tax return information to verify an applicant's income, section 1412 of the Affordable Care Act requires HHS to establish alternative procedures to determine APTC when there is a change in circumstances or “in cases where the taxpayer was not required to file a return . . .” Because section 1412(b)(2)(B) of the Affordable Care Act only references cases where a tax filer was
not required
to file an income tax return, we stated in the proposed rule that we do not believe an applicant who fails to meet the requirement to file an income tax return qualifies for this alternative process for determining APTC. Therefore, to determine and verify household income for APTC eligibility, it is imperative that consumers file a Federal income tax return when they are required to do so.
Furthermore, we believe that the impact of the stay is only to invalidate the 2025 Marketplace Integrity and Affordability final rule, thereby reverting Exchanges to the 2-year FTR policy that was previously in effect prior to the stay.
For additional clarification, even if a consumer is determined by HHS to have an FTR status during the FTR process, they or their tax filer can still claim their PTC for the months that they did not receive APTC when they do file their Federal income tax return and reconcile APTC for the applicable tax year. The proposed rule only applies to APTC eligibility, not PTC eligibility.
Comment:
Many commenters stated concern that the Federal tax filing process is complex, and many consumers are not fully aware of the requirements to file and reconcile, especially for the population that is more transient, as well as those not as financially or technologically literate. They noted that many of these consumers are simply unaware of how the tax system works, and consumers are not trying to purposefully game it and potentially incur criminal penalties from not filing Federal income taxes. They recommended States partner with healthcare providers who serve those who are experiencing homelessness to ensure consumers are aware of the need to file and reconcile. Commenters also noted concern about the staffing capacity at the IRS and being able to ensure that consumers who do file and reconcile do not lose their APTC eligibility due to IRS delays.
Response:
We note that we do not have authority over the Federal income tax rules in the Code, nor do we have authority over the IRS budget and staffing levels. We note that the IRS's Volunteer Income Tax Assistance (VITA) curriculum includes information on the requirement to file and reconcile and that through VITA,[153]
IRS-certified volunteers are available to help individuals who need assistance in preparing their own tax returns, including people who make $69,000 or less, persons with disabilities, and limited English-speaking taxpayers.[154]
Information about filing taxes is available at
www.healthcare.gov/taxes.
We will continue to educate consumers about the requirement to file and reconcile using notices throughout the FTR process and also encourage State Exchanges to work with homeless service providers in their States to ensure consumers are aware of the need to file and reconcile.
Comment:
Some commenters noted that HHS did not explicitly mention the change that IRS made regarding e-filing Federal income tax returns. Specifically, they noted that consumers should not be able to file their Federal income tax return and not reconcile their APTC due to the IRS's more recently implemented e-filing rejection code. This e-filing rejection code rejects an e-filed return if IRS records show that that the tax filer's SSN indicates they have received APTC and failed to attach Form 8962 to their tax return. These commenters believed that this should have effectively reduced the number of consumers who attempt to file their Federal income taxes without reconciling APTC.
Response:
We agree with commenters that this e-filing rejection code should have decreased the number of consumers who have filed their Federal income taxes without reconciling their APTC. However, prior to Open Enrollment for PY 2026, consumers who filed but did not reconcile made up almost 15 percent of the total 1-year FTR population. Prior to Open Enrollment for PY 2025, the percentage of consumers who filed but did not reconcile made up 13.3 percent of the total 1-year FTR population.[155]
Since e-filed income tax returns made up 93.3 percent of all individual income tax returns according to IRS data,[156]
it is likely that the percentage of those who filed but did not reconcile bypassed the e-file rejection by attaching a written explanation titled “ACA Explanation,” explaining why the Form 8962 should not be required.[157]
However, it is also possible that a percentage of these tax returns were paper-filed returns, which tend to include a larger percentage of those who encounter e-filing rejections. In sum, the e-filing rejection error does not eliminate the problem of some consumers filing their return but failing to reconcile their APTC.
Comment:
Some commenters stated the need to provide plain language notices to consumers to ensure they are aware of the need to file and reconcile. Commenters noted concern about the fact that IRS privacy rules prevent Marketplace Call Center Representatives from informing consumers directly that the reason they have lost APTC is because they have failed to file and reconcile.
Response:
For applications in which the consumer and the tax filer are the same person, they receive two plain language notices alerting them to the need to file and reconcile. Furthermore, “direct” FTR Recheck notices, which are FTR notices that are sent to the tax filer and can disclose FTI, directly inform tax filers of the need to file and reconcile to remain APTC eligible. They state: “Our records show you (or others in your household) used advance payments of the premium tax credit in 2023 and 2024, but didn't file a Federal income tax return or include IRS Form 8962 “Premium Tax Credit (PTC)” to reconcile the advance payments of the premium tax credit for those years.” In contrast, the “indirect” notices (sometimes called “combined” notices) are sent to the consumer and cannot disclose FTI; and therefore they cannot directly state that somebody has failed to file and reconcile. They provide the following more general information: “Our records show you (or others in your household) used advance payments of the premium tax credit in 2023 and 2024. Every year your household has Marketplace coverage and uses advance payments of the premium tax credit, you or your household's tax filer must file Federal income taxes and reconcile the
( printed page 29612)
premium tax credit you qualified for with the amount you used . . . . If you haven't filed a Federal income tax return with IRS Form 8962 for 2023 and 2024, file now or everyone in your household may lose financial help starting as early as [date].” If a consumer is also the tax filer on their application, they receive both the direct and the indirect notices.
While we are unable to change the privacy requirements at the IRS related to the ability to disclose FTI to anyone besides the tax filer, we believe that our workarounds provide sufficient notice to the consumer of the requirement to file and reconcile. Furthermore, the notices created by HHS are created with plain language guidelines in mind, while also conveying the implications of not filing and reconciling.
Comment:
Some commenters noted that they believe that it is important for consumers to have access to streamlined reinstatement mechanisms to regain eligibility for APTC after consumers file and reconcile.
Response:
Consumers who file their Federal income taxes and reconcile APTC can update their Exchange application and attest to filing and reconciling to regain their APTC eligibility, provided that a check of IRS data verifies that the consumer did in fact file and reconcile. If these consumers remain enrolled in a full cost QHP after their APTC is terminated, then they may qualify for an SEP under § 155.420(d)(6)(i) (for being determined newly eligible for APTC) after IRS data verifies that they did file and reconcile. However, if a consumer terminates their coverage due to inability to pay their full premium after their APTC is terminated, they will need to independently be eligible for an SEP to re-enroll in the Exchange outside of the open enrollment period. Furthermore, when a consumer files their Federal income taxes and reconciles APTC for the current year, they would be eligible for PTC for any months they did not receive APTC if they were otherwise eligible. If a consumer believes they have incorrectly lost their APTC under the failure to file and reconcile process, they can file an appeal at the Marketplace Appeals Center. While ease of restoring APTC is important, we also believe that preventing improper access to APTC is also important. Finally, we are actively monitoring agent, broker, and web-broker behavior for the FTR process.
Comment:
A few commenters stated support of the proposal to align policy with the required legislation as implemented by the WFTC legislation. A few commenters also agreed that reinstating the 1-year look-back will improve program integrity by ensuring enrollees do not remain in subsidized QHPs they do not realize they have or for which they are ineligible.
Response:
We agree that it is best to align the FTR policy with the coverage month requirements under section 71303 of the WFTC legislation when they take effect. We also believe that the 1-year FTR rule is essential to program integrity efforts by the Exchanges to ensure that those who are enrolled in coverage with APTC without their authorization do not face unexpectedly large tax liabilities. This is due to two parts of the FTR process—the removal of APTC as well as the FTR notices. By promptly removing APTC from consumers who do not file and reconcile, we can remove APTC from consumers enrolled without their knowledge or consent. Consumers who have no knowledge of their enrollment are unlikely to pay any portion of plan premiums that are not covered by APTC. Once these consumers do not pay their portion of premium, issuers will be required to cancel coverage for such enrollees no later than the third month the enrollee's portion of the premium remains unpaid, removing the risk that improperly enrolled consumers remain enrolled and amass a large tax liability. In addition, if a tax filer is enrolled without their knowledge and APTC covers the entire premium, the tax filer may be alerted to their enrollment by a notice warning that they need to file a tax return and reconcile past APTC. This notice could prompt the tax filer to contact the Exchange, report the unauthorized enrollment, and cancel their coverage, further reducing risk that the improper enrollment will persist. As a result, program integrity is strengthened by helping improperly enrolled consumers avoid surprise tax liabilities, saving them the burden of unwinding tax liability they did not knowingly incur. Program integrity is also supported and strengthened by ceasing the flow of Federal tax dollars to QHP issuers for persons who did not intend to enroll and saving tax dollars that would be expended by Federal government agencies in investigating and unwinding consumer tax liability flowing from improper enrollments and reconciling APTC paid for improper enrollments.
Comment:
One commenter requested HHS to consider sunsetting the rule after PY 2027.
Response:
If we did not require Exchanges to conduct the 1-year FTR policy in PY 2028, all Exchanges operating anything beside the 1-year FTR policy would be statutorily prohibited from providing APTC. This is because section 71303 of the WFTC legislation provides that, beginning in PY 2028, a month may not be a coverage month, and therefore no PTC may be paid for such month, for an individual if an Exchange does not implement a 1-year FTR policy. Because APTC is essential for the Exchanges to function as designed in the Affordable Care Act, we have determined it is important to impose a 1-year FTR policy beginning in PY 2028.
Comment:
One commenter stated that the text of the WFTC legislation that provides the statutory authority for the 1-year FTR process beginning in PY 2028 points to the 2025 Marketplace Integrity and Affordability final rule's invalidated rule text as being the basis for the statutory requirement. The commenter stated that the statute will be meaningless unless the District Court rules otherwise in
City of Columbus
v.
Kennedy
or Congress acts to specifically require 1-year FTR without reliance on an unenforceable Federal regulation or specifically grants HHS rulemaking authority to require 1-year FTR.
Response:
We do not agree with this interpretation of the statute and believe that we have the authority to conduct the 1-year FTR policy beginning in PY 2027 under section 1412 of the Affordable Care Act, in addition to the express statutory authority provided in the WFTC legislation for PY 2028 and beyond.
Comment:
Some commenters questioned whether this proposal was appropriate given the stay on the 1-year FTR policy for PY 2026 issued by the court in the
City of Columbus
v.
Kennedy
litigation.
Response:
The
City of Columbus
v.
Kennedy
court's stay on the 1-year FTR policy for PY 2026 that was finalized in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) has no impact on the 1-year FTR policy for PY 2027 that is proposed and finalized in this rulemaking. While the 1-year FTR policy for PY 2026 is currently under litigation, as a general matter, Federal agencies are free to engage in further notice-and-comment rulemaking on a policy previously stayed in litigation. Moreover, as discussed previously, circumstances have changed since the finalization of the 2025 Marketplace Integrity and Affordability final rule that provide greater justification for the 1-year FTR policy. In particular, Section 71305 of the WFTC legislation eliminated excess APTC recapture limits which increases the risk for accumulating high tax liabilities if consumers do not file their
( printed page 29613)
Federal income tax returns and reconcile APTC.
Comment:
Some commenters requested that HHS provide more demographic information about the consumers who lose APTC through the FTR process.
Response:
We will consider providing more demographic information about consumers who lose APTC as part of the FTR process. However, we note that these data will be at the aggregate level in order to protect FTI. We also want to note that we are working to provide additional data about FTR consumers. For example, we provided a State by State FTR population breakdown during the past year, which can be found at
https://www.cms.gov/files/document/failure-file-and-reconcile-data-plan-year-2025.xlsx.
Comment:
One commenter supported the 1-year FTR policy and noted that without the FTR policy, consumers would have an incentive to misrepresent their income so that they qualify for the largest subsidy available. They also noted that the FTR process would help address the issues of multiple enrollments across modes of coverage.
Response:
While we appreciate the intent of the comment, we believe that we have more targeted solutions to help with these issues compared to the FTR process. While the tax return should be the primary basis for verifying a consumer's income, we have multiple other methods for annual income verification that would prevent a consumer from qualifying for the largest subsidy available by not filing their Federal income taxes and reconciling APTC. Without IRS documentation, the Exchange would attempt to verify income based on either other trusted data sources or by requiring a consumer to submit documentation to verify their income. If neither of these methods could verify the consumer's income, and the consumer did not have IRS data to use, their APTC would be set at zero. In addition, we run both Medicaid/CHIP periodic data matching (PDM) and Medicare PDM operations twice a year to identify consumers who are dually enrolled and to notify them and either terminate their QHP enrollment or APTC depending on their preference. These processes are more effective and timely than FTR at identifying and notifying consumers enrolled in multiple modes of coverage. While a consumer may receive an FTR notice alerting them of their Exchange coverage, FTR notices inform consumers of the need to reconcile APTC for a previous tax year, whereas Medicare PDM and Medicaid/CHIP PDM notices speak to current enrollment and are thus better suited to identify consumers who are dually enrolled in QHP coverage with APTC and Medicare or Medicaid/CHIP. In addition, Medicare PDM and Medicaid/CHIP PDM notices would directly identify for the consumer that they are dually enrolled in multiple modes of coverage, whereas FTR notices do not speak to that issue.
11. Comment Solicitation on Eligibility Verification Provisions of the WFTC legislation, Section 71303
Section 71303(a) and (b) of the WFTC legislation imposes new requirements on Exchanges related to eligibility verification effective with PY 2028.
Section 71303(a) of the WFTC legislation adds a new paragraph (5) to section 36B(c) of the Code, establishing that a month is not a coverage month for an applicant, and therefore no PTC is allowed for the applicant's coverage for that month, if the month begins before the Exchange verifies the applicant's eligibility to enroll in a QHP and for APTC, “using applicable enrollment information that shall be provided or verified by the applicant.” Section 71303(a) of the WFTC legislation also:
Specifies a minimum set of “applicable enrollment information”;
Clarifies that a past month may be treated as a coverage month if an Exchange later verifies the applicant's eligibility;
Specifies that these verification requirements do not impact eligibility to enroll in a QHP;
Permits the Secretary of the Department of the Treasury to waive these verification requirements when an individual qualifies for an SEP based on a change in family size; and
States that Exchanges are permitted to use “any data available to the Exchange and any reliable third-party sources in collecting information for verification by the applicant.”
Section 71303(b) of the WFTC legislation amended section 36B(c)(3)(A) of the Code such that any plan enrolled in through an Exchange is not considered a QHP, and therefore no PTC is allowed for enrollment in the plan, unless, no later than August 1 of the year before the plan year, Exchanges provide “a process for pre-enrollment verification” that permits any applicant to verify their household income and eligibility for enrollment in such plan for the upcoming plan year.
In the 2027 Payment Notice proposed rule (91 FR 6345), we stated that we plan to issue regulations, guidance, technical assistance, and educational materials in the future to facilitate implementation of these provisions of section 71303 of the WFTC legislation. In the proposed rule, we sought comment on considerations for future policy development and implementation of these provisions of section 71303 of the WFTC legislation. We sought comment on topics including, but not limited to, operational considerations for State Exchanges, issuers, agents and brokers, navigators and assisters, and consumers; and effective rollout and communications. We sought input from interested parties regarding the required timelines to comply with the law, including the requirement that Exchanges establish a pre-enrollment verification process no later than August 1, 2027. We also sought input on the anticipated complexity, costs, burden, enrollment impacts, and any State-specific considerations. We thank commenters for their feedback and will take comments into consideration in future guidance, technical assistance, educational materials, and rulemaking.
Section 71303 of the WFTC legislation also adds new paragraph (6) to section 36B(c) of the Code, regarding failure to file and reconcile; please see section III.D.10. of this final rule for further discussion regarding failure to file and reconcile.
12. Income Verification Policy When Data Sources Indicate Income Less Than 100 Percent of the FPL (§ 155.320(c)(3)(iii))
To support improved payment integrity measures throughout the Exchanges, we finalized a series of income verification provisions in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27121), including revisions to § 155.320(c)(3), to require the submission of documents to verify income when an applicant's attested projected household income is at or above 100 percent of the FPL and trusted data sources indicate the consumer's household income is below 100 percent of the FPL. This policy was a resumption of the requirement to verify income for this subset of consumers that was first finalized in the 2019 Payment Notice (83 FR 16985), a regulation that was later vacated by the U.S. District Court for the District of Maryland in
City of Columbus
v.
Cochran.[158]
Following our discovery of a massive volume of improper enrollments in 2023 and 2024, we re-proposed and finalized this policy in the 2025 Marketplace Integrity and Affordability Rule based on its assessment that additional eligibility
( printed page 29614)
verifications were necessary to prevent improper enrollments and payments of APTC, and to guard against improper enrollment behaviors by agents, brokers, and web-brokers. Based on commenters' concerns, we finalized this rule to sunset at the end of PY 2026 to provide further opportunities to monitor the policy's effects instead of codifying it to be applicable indefinitely. This policy was also sunset with the expectation that the reduction in fully subsidized plans resulting from the expiration of the enhanced PTC would reduce the urgency of its program integrity features and in response to commenter feedback that the measure was not necessary in State Exchanges that had not experienced high levels of improper enrollments. We believed that implementing this policy through the end of PY 2026, when paired with existing program integrity measures and additional measures finalized in the 2025 Marketplace Integrity and Affordability final rule, would strike the right balance between urgent program integrity concerns and long-term enrollment efficiencies. In August 2025, the U.S. District Court for the District of Maryland stayed enforcement of the regulation based on its conclusion that HHS did not meaningfully engage with challenges to the data and reports it used to justify the regulation.[159]
Since the finalization of the 2025 Marketplace Integrity and Affordability final rule and the issuance of the August 2025 court stay, we have continued to focus on finding and stopping improper enrollments, including those supported by inaccurate income estimations. Without the implementation of the stayed income verification regulation requiring documentation of income when an applicant attests to household income above 100 percent FPL and trusted Federal data sources indicate household income is below 100 percent FPL, the use of inflated incomes could have resulted in consumers being improperly enrolled in Exchange coverage, oftentimes without their knowledge. Since October 2025, the Federal Exchange has continued to detect improper enrollments that included suspect attestations of income. For example, we stated in the proposed rule that the Federal Exchange has received reports that agents, brokers, and web-brokers may be using artificial intelligence to impersonate consumers and falsely attest to household income that could potentially qualify the consumers for APTC and CSR benefits they may not be eligible for, something that we were not aware of when we finalized the 2025 Marketplace Integrity and Affordability final rule. Inaccurate household attestations can lead to consumers experiencing hardship when they go to use health coverage and find out they are enrolled in a plan they were unaware of.
Verifying an applicant's household income could result in HHS detecting improper enrollments before APTC can be paid. We stated in the proposed rule that we continue to uncover improper enrollments through reports from consumers, agents, brokers, and web-brokers, and, in particular, issuers. As mentioned in the fact sheet on CMS actions to strengthen program integrity and protect consumers,[160]
in 2025, the Federal Exchange cancelled 250,000 unauthorized enrollments. Additionally, the Federal Exchange stopped APTC for 500,000 enrollees who were found to be concurrently enrolled in Exchange coverage with APTC and other coverage. In the proposed rule, we stated that the proposed policy, if finalized, could go far in protecting Federal funds from being paid to support improper enrollments for those who do not qualify for APTC or those who never intended to enroll in Exchange coverage, especially those who are already enrolled in Medicaid coverage and therefore did not need coverage through the Exchange. We stated that we are of the view that these circumstances present sufficient risk to Exchanges' ability to accurately verify eligibility determinations for APTC. We also stated that we are of the view that we cannot continue to ignore the obvious risk presented by circumstances under which APTC and CSR eligibility is granted, notwithstanding that trusted data sources indicate that an applicant's household income is below 100 percent FPL, making them ineligible for receiving APTC or CSRs. We stated that we believe it is reasonable, necessary, and not unduly burdensome to require individuals to submit documentation to resolve these inconsistencies.
Moreover, submitting documentation to verify income is now even more important to protect applicants from accumulating tax liabilities due to misestimating or misreporting their income. As we explained in relation to the FTR policy in section III.D.10. of this final rule, the WFTC legislation was enacted after the finalization of the 2025 Marketplace Integrity and Affordability final rule removes limitations on repayment of the APTC beginning with PY 2026. Under section 71305 of the WFTC legislation, repayment caps on excess APTC payments discontinued starting in PY 2026. We stated in the proposed rule that under this proposed policy, households would likely receive an income DMI that would require them to submit documents to verify their annual household income and, if they do not verify with documents, would result in the loss of APTC after the 90-day DMI period and protect them from accumulating substantial tax liabilities. The Federal Exchange does have a process that allows consumers to report an unauthorized enrollment, which will allow them to avoid tax liabilities, but this requires the consumers to be aware of the improper enrollment and take actions to correct it. The Federal Exchange also permits issuers to report improper enrollments to HHS, which has the same effect of allowing the consumer to avoid tax liability for an enrollment they were unaware of and did not authorize.
We noted in the proposed rule that Congress did not limit HHS' authority under section 1411 of the Affordable Care Act to verify income under the circumstances targeted by the policy, but granted HHS broad authority and discretion to design verification procedures the HHS Secretary determines appropriate. Section 1411(c) of the Affordable Care Act provides that applicants' previous taxable year household incomes reported on an Exchange application must be submitted to the Secretary of the Treasury for verification. Section 1411(d) of the Affordable Care Act directs HHS or an Exchange to verify the accuracy of information that is not required to be submitted to Treasury, Homeland Security, and Social Security. Income information provided to verify eligibility when there are “changes in circumstances” is not required to be submitted to Treasury. Therefore, under 1411(d), HHS or Exchanges must verify this income information, which includes verifying income through other trusted data sources. If no trusted data source can verify income, section 1411(e)(4) of the Affordable Care Act requires the HHS Secretary to notify the Exchange of the inconsistency and the Exchange to take reasonable steps to resolve the inconsistency, including by contacting the applicant or by taking any additional actions as the HHS Secretary may identify through regulation or other guidance.
If the inconsistency remains unresolved, the Exchange must give the applicant an opportunity to either
( printed page 29615)
present satisfactory documentary evidence or resolve the inconsistency with the Secretary of the Treasury. The policy we proposed in this rulemaking reflects Congress' directives in section 1411(e)(4) of the Affordable Care Act. Given Congress' directive under section 1411(e) of the Affordable Care Act to collect documentation of applicant income in appropriate circumstances, as well as the discretion it granted to the HHS Secretary under the same section, it is difficult to pinpoint circumstances under which a requirement to verify or reconcile inconsistent data would be deemed unreasonable. Accurate income attestation and verification from households has long-ranging implications for payment integrity in the Exchange, with impacts to consumer protection, appropriate agent/broker/web-broker compensation, data integrity, and the expenditure of tax dollars. Increased repayment responsibilities now make these further verifications an essential protection against accumulating tax liabilities. Given HHS' authority, the ongoing need to strengthen program integrity and protect enrollees from accumulating tax liabilities, we proposed to require Exchanges to comply with the requirement in 1411(e)(4) of the Affordable Care Act to set a 90-day inconsistency period for instances where the applicant's attested annual household income cannot be verified by data sources for verifications of eligibility for 2027 coverage and beyond. While we acknowledged in the proposed rule that such a change may impose a burden to State Exchanges and other interested parties, particularly in consideration of work that may have been done to support the 2025 Marketplace Integrity and Affordability final rule, we stated that we believe this proposal is a reasonable exercise of the authority and discretion that Congress vested in the HHS Secretary under section 1411 of the Affordable Care Act and is necessary given the payment integrity and tax liability issues noted above. Furthermore, we stated that we believe that the long-term program integrity savings of this change outweigh the operational costs to the Exchanges, as outlined in the Collection of Information Requirements in section IV of this final rule.
With this in mind, section 1412 of the Affordable Care Act describes the process for determining eligibility for APTC using the process described in section 1411 of the Affordable Care Act. Specifically, section 1412(b)(2) of the Affordable Care Act gives the Secretary authority to define additional verification procedures where a consumer's application reflects a change in the consumer's circumstances when compared to data for the most recent taxable year that is available from the Secretary of the Treasury. In cases, as described previously, where an applicant attests to annual household income at or above 100 percent of the FPL but the IRS indicates it is below 100 percent of the FPL, we stated in the proposed rule that the Exchange would use this authority to determine whether they may be eligible for APTC using their attested annual income amount, given the `changes in circumstances' from their tax data. In cases where trusted data sources cannot verify their income under these circumstances, we proposed to specify that Exchanges on the Federal platform would follow the procedures established under 1411(e)(4) and implemented in § 155.315(f)(1) through (4) to create an annual income DMI for these consumers.
Beyond statutory authority, we stated in the proposed rule that there are concerns regarding program integrity that continue to validate enhanced scrutiny for consumers whose annual household income is indicated by tax data as below 100 percent of the FPL. As we noted in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27121), a GAO study on improper payments determined our control activities, such as income verification policies, related to the accuracy of APTC calculations were not properly designed.[161]
While we originally proposed temporarily instituting this policy in part due to lack of new data around this problem, a more recent GAO study published after the 2025 Marketplace Integrity and Affordability final rule (90 FR 27121) illustrates that this continues to be a problem. This recent GAO study described issues that persist in the payment integrity protections of the Exchange, including vulnerabilities related to potential SSN misuse as well as negative impacts resulting from unauthorized enrollment changes from agents, brokers, and web-brokers.[162]
Specifically, the study identified at least 160,000 applications in PY 2024 that likely had unauthorized changes, which further illustrates the continued problem of some agents, brokers, and web-brokers making changes without the consumer's consent to the consumer's application. The study utilized 20 fictitious applicants to identify program integrity control issues, of which 18 remained improperly enrolled as of September 2025. The GAO argued that, although the results cannot be generalized to the overall population, these cases highlighted vulnerabilities in verification processes that can contribute to APTC reconciliation issues. Specifically, they stated that they highlighted weaknesses in income verification, which we seek to strengthen by finalizing this proposal. We stated in the proposed rule that we find that continued issues on the Exchange with accurately determining APTC eligibility as highlighted in this study present ongoing risks to the financial integrity for the Exchanges and create opportunities for agent, broker, and web-broker driven improper conduct. We stated that this gives further weight to the necessity of the continuation of this income verification policy beyond 2027.
A notable driver of these continued payment integrity concerns, as evidenced by the 2025 GAO findings, is agent, broker, and web-broker behavior. In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27121), we provided evidence connecting agent, broker, and web-broker actions to consumers misrepresenting or overestimating their income and the rise in unauthorized enrollments. We observed that some agents, brokers, and web-brokers and applicants are taking advantage of weaknesses in the Exchanges' eligibility framework to enroll consumers in coverage with APTC without their knowledge, even when the consumers are not eligible. We stated in the proposed rule that the persistence of agent, broker, and web-broker actions to undermine payment integrity highlight the need for continued changes to address improper enrollment and improve the accuracy of income attestations. In recently identified internal data, we found that nearly 80 percent of income DMIs were generated for households who worked with an agent, broker, and/or web-broker in PY 2024. Additionally, we found for PY 2025 that enrollees who worked with an agent, broker, and/or web-broker in PY 2025 generated DMIs at a rate three times higher compared to enrollees who did not work with anyone. This could be indicative of continued agent, broker, and web-broker misconduct including broad miscalculations in household income
( printed page 29616)
attestation for applications assisted by agents, brokers, and web-brokers across Exchanges on the Federal platform, which would result in inaccurate APTC assessments for those households. Overall, as we stated in the proposed rule, the additional income verification outlined within this provision would help address these concerns.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed with one minor edit to § 155.320(c)(3)(vi)(C)(2) to cite paragraph (c)(3)(vi) instead of paragraph (c)(3)(iii)(D) for information on the reasonable threshold. Below, we summarize and respond to public comments received on the proposed policy to perform further income verification processes when the IRS returns income that is below 100 percent FPL but an applicant's attested projected annual household income would consider them an applicable taxpayer according to 26 CFR 1.36B-2(b) for the plan year for which coverage is requested, and is more than a reasonable threshold above the annual household income.
Comment:
A few commenters supported the proposal, stating it would improve program integrity and help prevent fraud, especially regarding improper enrollments. One commenter stated this regarding evidence illustrating overall fraud growing in the Exchanges. One commenter stated that it would help prevent improper subsidy payments to insurance companies. One commenter stated this policy would reduce income manipulation and helps avoid `pay and chase' recovery models.
Response:
We agree that this policy will improve program integrity and help prevent potential fraud. Given the large amount of improper enrollments cited in the proposed rule and in this final rule, we agree that this policy may help limit associated improper enrollments. We also agree that this will help reduce instances of agents, brokers, and web-brokers purposely attesting to an incorrect income amount when assisting consumers through Enhanced Direct Enrollment channels for agents, brokers, and web-brokers, and help prevent improper payments of APTC associated with incorrect income attestations.
Comment:
Some commenters stated support for how the proposal could save taxpayers money by helping prevent the overpayment of APTC.
Response:
We agree that this policy may help ensure accurate income amounts and corresponding APTC determinations, resulting in fewer consumers being subject to large tax liabilities. Without the implementation of this income DMI, Exchanges would provide APTC for households for an entire plan year based on a household income attestation that may not be accurate. Instead, households who cannot verify their household income attestation and who receive this income DMI will only receive APTC during the DMI period as opposed to the entire plan year if their income DMI expires. In addition, this is potentially protecting these households from large tax liabilities due to APTC overpayment in cases where the DMI flags incorrect income information for someone who, instead of earning a lower income as the DMI suggests, ends up expecting to earn a higher income after the DMI is resolved. This will help protect taxpayer dollars as these households with annual household income below 100 percent FPL when they file their taxes may not be required to repay APTC per current IRS rules at 26 CFR 1.36B-2(b)(6). Households who receive this DMI will not necessarily have annual household income below 100 percent FPL when they file their taxes, but we estimate that this population is more likely to fall into this category.
Comment:
One commenter recommended that we should first complete verifications for income before providing APTC payments.
Response:
We acknowledge the comment and understand the desire to complete verifications for income before providing APTC payments. However, as a part of this final rule, we are not proposing or finalizing to deny APTC and CSRs during an income DMI period for this policy. Making that change would conflict with section 1411(e)(4)(B)(i) of the Affordable Care Act, which requires Exchanges to make APTC determinations based on attestation information during an inconsistency period.
Comment:
Some commenters noted the need to ensure that this additional income verification process is accessible and includes clear communication. One commenter stated that it needs to include clear consumer notices, reasonable documentation standards, and accessible assistance pathways.
Response:
We agree that Exchanges need to ensure clear communication and make the process as easy as possible for consumers. Currently, the Federal Exchange sends multiple notices to consumers while a DMI is open, including notices and phone calls when a consumer submits a document to resolve an income DMI, but that document is not sufficient to resolve it. Additionally, consumers can access information on open DMIs and which documents to submit in both their Eligibility Determination Notice and their
HealthCare.gov
account. We will also ensure all notices and other communications are updated in relation to this change. While we still believe we should finalize this proposal given the important program integrity concerns, we continue to understand the need for clear communication to make it easier for consumers to understand their DMIs and next steps.
Comment:
Many commenters stated concerns that this proposal would negatively impact consumers' ability to enroll, and stay enrolled, in affordable coverage and recommended that CMS not finalize the proposal. Specifically, commenters noted that the administrative burden of submitting documents to resolve their income inconsistency is a barrier to enrollment and effectively creates a `red tape' that adds friction and delays that discourage consumers from staying enrolled. Additionally, commenters noted how the expiration of an annual income DMI in this scenario would lead to a loss of APTC, which means consumers would be forced to either drop coverage or pay unaffordable premiums. Overall, commenters believe this would make it harder for people to access and maintain affordable, quality health care.
Response:
We understand that some consumers may end up having their financial assistance reduced or removed, resulting in coverage loss and financial burden. However, the income DMI process allows 90 days to submit documents, including submitting new documents if their previously submitted documents were deemed insufficient to resolve the DMI, and we previously estimated that submitting documentation will only take 1 hour based on historical document submission. Therefore, we believe that the administrative burden of submitting documents is minimal. We also emphasize the importance of consumers receiving accurate APTC eligibility to help protect households from large tax liabilities due to overpayment of APTC, which is why we believe it is important to have this income DMI in place even if some consumers unintentionally lose APTC, and as a result, QHP coverage.
Comment:
Most commenters stated concerns that this will negatively impact specific consumer groups. Commenters stated that low-income consumers will be disproportionately impacted, which is compounded by the fact that they have a more difficult time than other consumers in predicting and verifying income. Commenters noted
( printed page 29617)
how these consumers tend to be self-employed, small business owners, hourly and seasonal workers, farmers, and gig workers, all of which tend to have income that may make it more difficult to both estimate for the future plan year and substantiate their estimate through documentation. Additionally, some commenters noted that these lower income consumers typically are not required to file taxes, so they are more likely to not have tax data available to verify their income.
Response:
We acknowledge that consumers with more unpredictable income, including low-income consumers, may have a more difficult time estimating their income. We have made improvements over the years to account for this concern and recommend that consumers utilize tools such as the income calculator tool to assist with that process.[163]
Additionally, we understand that income can change throughout the year. Consumers who struggle to estimate their income are encouraged to use the tools provided by the Exchanges to provide the best estimate they can, and we highly recommend that consumers update their Exchange application if they have reason to believe that income estimation is no longer accurate. Further, even if a consumer would normally not be required to file a tax return due to their income, once they have received APTC, they are required to file a tax return to reconcile their APTC. For those applying for APTC for the first time who were not required to file a tax return due to their income, verification through other trusted data sources may trigger this DMI and require further documentation to verify income.
For those that experience difficulty identifying documents to submit, we recommend consulting the full list of acceptable documents provided on multiple consumer notices and our website.[164]
The resources provided in the Guide to Confirming Your Income Information may be used to better understand which documents may be most appropriate for confirming current household income.[165]
For example, while some documents such as tax forms may not substantiate attested income for these consumers, many of the other documents can convey future year income such as a paystub that indicates how much is typically earned in a pay period or a self-employment ledger.
While we understand that some consumers may have trouble estimating and proving their income, we emphasize the importance of ensuring that APTC distributed is accurate and fully verified through this additional income verification requirement.
Comment:
Some commenters stated concerns that this additional verification process would result in worse health outcomes and additional burden for consumers already experiencing health issues. Some commenters noted how this would be particularly difficult for consumers they serve at community health centers. One commenter noted how those who have cancer are already facing serious health and administrative challenges that make it particularly difficult to gather documents and deal with a complex eligibility process. Some commenters stated concerns that these consumers would ultimately not be able to resolve their income DMIs and, as a result, lose coverage due to unaffordability, which would result in worse health outcomes due to no longer having coverage while undergoing treatments.
Response:
We understand that some consumers may experience more difficulty than others submitting documents to resolve their income DMI. We recommend submitting documents earlier in the 90-day period to allow more time if the original documents submitted are not sufficient to resolve the DMI. While we acknowledge these concerns and that some consumers may end up having their DMI expired and lose APTC as a result, we continue to emphasize the importance of this policy, especially to help prevent unauthorized enrollments done by some agents, brokers, and web-brokers.
Comment:
Many commenters stated concerns about the costs and burdens of this proposal on Exchanges. Commenters noted that they believe the proposal would increase administrative costs, and that this would result in having to divert funds from other important eligibility and enrollment operations in order to implement and maintain this income verification policy. Many also stated that State Exchanges do not currently have appropriated funds or other resources to implement this change and are especially concerned given the expected upcoming costs associated with the WFTC legislation. Some commenters expressed skepticism that this would result in taxpayer savings related to APTC for consumers whose income DMI expires and do not receive APTC for further months, with one commenter noting that if a consumer ends up in Medicaid after their income DMI expires it does not save the government money.
Response:
We acknowledge the costs associated with implementing this proposal, which are described in more detail in section IV.I. of this final rule. We are confident that the Exchanges on the Federal platform can implement this proposal by the rule's effective date and are not concerned with implementation operations. We acknowledge concerns that State Exchanges have expressed regarding implementation costs and timelines. However, we believe that it is a crucial program integrity measure to require further income verification when a household attests to income greater than 100 percent of the FPL but trusted data sources indicates income less than 100 percent of the FPL because these households are ineligible for APTC. This income verification is a crucial step in preventing households who are not eligible for APTC from receiving any APTC, especially households with annual household income below 100 percent FPL when they file their taxes may not be required to repay APTC given IRS rules at 26 CFR 1.36-2(b)(6). There may be circumstances where this DMI identifies an inaccurate income attestation, in which case further documentation may be needed to protect the individual from accumulating tax liabilities.
Additionally, we believe that the costs associated with implementing and operating this policy are justified, as this is a critical program integrity measure to ensure consumers who may not be eligible for APTC are not erroneously receiving APTC throughout the entire plan year. Because of that, while we understand State Exchanges are concerned about the implementation and ongoing costs, including any upcoming changes due to the passing of the WFTC legislation, we believe that the program integrity gains outweigh the potential costs to State Exchanges. As illustrated later in the regulatory impact analysis section of this rule, we estimate that APTC savings will be greater than operational costs. This is especially true given that many of these consumers may have annual household income below 100 percent FPL when they file their taxes and therefore may not have to pay back the APTC they received. Absent an income DMI, they would likely receive APTC for the entire plan year whereas, with an income DMI, they would only receive APTC during the inconsistency period if income could not be verified. Finally, we emphasize that while some consumers may end up enrolling in Medicaid after APTC is terminated for failing to verify income, we see this as
( printed page 29618)
a positive outcome as it would result in a consumer enrolling in coverage for which they are eligible.
Comment:
Some commenters stated concerns about how this policy would impact the risk pool. Specifically, commenters stated that healthier consumers are less motivated to get insurance, particularly when they encounter administrative burdens such as additional required paperwork, while sick consumers are often more motivated to overcome administrative barriers to coverage. Commenters stated that all of this results in fewer healthy consumers entering the risk pool, which would result in increased premiums for everyone, especially those who do not receive subsidies.
Response:
We acknowledge that administrative barriers can deter healthy people from enrolling. However, we continue to emphasize the need for this policy to help ensure only those truly eligible for APTC receive it. While this policy may deter some healthy people from enrolling, it will also deter many agents, brokers, and web-brokers from intentionally misreporting annual household income to secure a commission.
Comment:
Many commenters stated concerns with the data and studies the proposed rule cited as proof of program integrity concerns. Commenters stated that the policy generally lacks justification, including a lack of proof of widespread unauthorized enrollments, and that the benefits of the proposal are only speculative while the harms are obvious. Some commenters noted how this policy is arbitrary. One commenter noted how the justification of preventing fraud by agents, brokers, and web-brokers is insufficient to justify implementing this proposal. One commenter noted how the high generation of income DMIs by agents, brokers, and web-brokers being an indication of fraud is an overgeneralization, as consumers assisted by them tend to have lower and more variable incomes and less health literacy.
Response:
We do not agree that this policy lacks sufficient justification. A 2025 GAO audit illustrated that program integrity issues continue to exist, with 18 out of the 20 fictitious applications created to identify program integrity issues remaining improperly enrolled through September 2025.[166]
While this is a small sample size, for agents, brokers, and web-brokers who engage in fraudulent or otherwise noncompliant behaviors, the numbers would be much higher. This is compounded by some of them utilizing newer technology such as artificial intelligence that makes it more difficult for the Federal Exchange to address individual cases of fraudulent or improper enrollment. For example, some have attempted to use technology that disguises a speaker's true voice to impersonate consumers. We also continue to see concerning rates of DMIs generated by applications submitted by agents, brokers, and web-brokers. Additionally, many of these consumers with annual household below 100 percent FPL when they file their taxes may not be required to repay APTC per current IRS rules at 26 CFR 1.36B-2(b)(6). Absent this policy, these consumers may receive that APTC for the entire plan year compared to only during the 90-day DMI period. Compounded with potentially fraudulent actions by some agents, brokers, and web-brokers, we expect further income verification could help save taxpayers time and money related to APTC overpayment.
Comment:
Some commenters noted that this proposal is under litigation and is currently stayed in
City of Columbus
v.
Kennedy,
and that an identical policy was struck down in
City of Columbus
v.
Cochran.
These commenters stated they do not believe the proposal has meaningfully changed from what was finalized in the 2025 Marketplace Integrity and Affordability final rule. One commenter stated that this proposed rule does not properly address the sunset provision or public defenses of that rule.
Response:
We believe that this proposed and final rule address concerns raised in both
City of Columbus
v.
Kennedy
and
City of Columbus
v.
Cochran.
As stated in this final rule, after the 2025 Marketplace Integrity and Affordability final rule was finalized, the Federal Exchange has continued to see improper enrollments that include suspected intentionally incorrect attestations of income. This was further illustrated through a 2025 GAO study, also published after 2025 Marketplace Integrity and Affordability final rule was finalized, that resulted in most fictitious enrollments staying enrolled through at least September 2025.[167]
Additionally, we have begun to see some agents, brokers, and web-brokers utilizing newer technology such as artificial intelligence to impersonate consumers and falsely attest to incorrect income amounts with the intention of receiving maximum subsidies. In light of this new information, we find it necessary to finalize this policy removing the sunset that was established in the 2025 Marketplace Integrity and Affordability final rule. Additionally, while the WFTC legislation eliminated the repayment caps on APTC, consumers with annual household income below 100 percent FPL when they file their taxes may not be required to repay APTC per current IRS rules at 26 CFR 1.36B-2(b)(6), further necessitating implementing this income DMI.
Comment:
Many commenters stated concerns related to the requirement for State Exchanges to implement this proposal. Many of these commenters noted that State Exchanges do not have the type of fraudulent behavior this proposal attempts to address because nearly all State Exchanges have expanded Medicaid, which commenters stated eliminates the incentive for inflating income. Additionally, some commenters noted that existing State systems already have robust verification and fraud safeguards, and that this policy will undermine those. Finally, many commenters stated concerns with the large cost and administrative work associated with this policy, especially in relation to other policies being proposed in this rule and upcoming in the future. Overall, these commenters believed that this policy should be optional for State Exchanges.
Response:
We appreciate that State Exchanges may not have experienced the same challenges of agents, brokers, and web-brokers improperly overestimating income resulting in improper payment of APTC and participating in fraudulent behavior. We also acknowledge that many States have additional verification and fraud safeguards and appreciate the work of States to address fraud. Additionally, while the WFTC legislation eliminated the repayment caps on APTC, for households that attest to projected annual household income greater than 100 percent FPL but whose annual household income is less than 100 percent FPL when they file their taxes may not be required to repay APTC when they file their tax return pursuant to 26 CFR 1.36B-2(b)(6), so it is important to protect taxpayer dollars in this scenario by requiring further income verification.
Comment:
Some commenters noted that this proposal does not address interactions with future changes that
( printed page 29619)
will be made due to the WFTC legislation. One commenter stated that this rule should be delayed until those requirements, as well as other program integrity related measures in this proposed rule, go into effect to evaluate if this proposal is necessary or not.
Response:
We understand concerns regarding future implementation of the WFTC legislation and how it will interact with current and future DMI processes, including those in this final rule. As stated in the proposed rule, we are currently considering how changes related to the WFTC legislation will be implemented. However, we believe that this policy is necessary before and after the implementation of changes related to the WFTC legislation given the continued occurrences of agents, brokers, and web-brokers intentionally overestimating income.
Comment:
Some commenters stated that we should better address concerns with IRS data, specifically around data latency and applicants' annual household income often being very different year-to-year. One commenter requested that we rely more on current sources of income data to help streamline verification processes and enhance efficiency.
Response:
We emphasize that while the Exchanges first check IRS data to determine whether they can verify a household's attested income, the Exchanges may continue to utilize additional data sources to verify income. Specifically, once IRS returns income below 100 percent of the FPL for a household whose attested annual household income is at or above 100 percent of the FPL, and the difference between IRS data and the attested annual household income is more than a reasonable threshold, the Exchanges may then check any additional data sources available to them to attempt to verify the household's attested income. In cases where a household's attested annual income cannot be verified through those additional data sources, we believe it is important for consumers to submit documents to demonstrate that their attested annual household income is accurate. Additionally, in response to the commenter who requested that we rely more on current sources of income data, we clarify that the Federal Exchange currently uses the Verify Current Income Hub but continue to allow State Exchanges flexibility in what additional data sources they use beyond IRS, subject to timeliness and accuracy standards.
Comment:
Some commenters stated concerns with requirements regarding the verification process. One commenter stated that consumers who are not eligible for financial assistance should not have to undergo income verification, particularly for consumers who receive individual coverage health reimbursement arrangements (ICHRAs) and qualified small employer health reimbursement arrangements (QSEHRAs). Multiple commenters requested that we allow Exchanges to utilize a threshold rather than automatically set a DMI when attested annual household income does not match IRS data. One commenter stated frustration that States would be required to redetermine Medicaid upon an income DMI generated from this policy expiring.
Response:
We appreciate these comments and would like to provide clarification on the income verification process. For consumers who did not request financial assistance, or where an Exchange determines them ineligible for financial assistance during their application, we do not set an income DMI and they will not receive APTC.
When checking data sources, including IRS, to determine whether they can verify income information, we utilize a reasonable threshold to determine whether the income information from a data source sufficiently close to the information on the application. As mentioned in the proposed and final updates to § 155.320(c)(3)(iii)(A), Exchanges must use a reasonable threshold which cannot be less than 10 percent and can include a dollar amount. The Federal Exchange currently employs a threshold of 50 percent or $12,000. Therefore, in cases where data from IRS is slightly different than attested annual household income, but that difference is within a reasonable threshold, we would not generate an income DMI. Additionally, Exchanges can and should continue to use additional data sources subject to timeliness and accuracy standards as approved by HHS to attempt to verify income information in cases where IRS cannot.
Finally, when an income DMI expires, including in this scenario, consumers would have their eligibility for financial assistance decreased based on IRS data which, in this case, would result in them losing financial assistance altogether. While we believe many of these consumers may be eligible for Medicaid rather than Exchange coverage, we recommend Exchanges find ways to help those consumers apply for Medicaid; however, we are not requiring Exchanges to automatically redetermine their eligibility for Medicaid upon income DMI expiration.
13. Removal of the Requirement To Accept Attestations of Household Income When Tax Data Is Unavailable (§ 155.320(c)(5))
In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), we removed the requirement for all Exchanges to accept an applicant's annual household income attestation when IRS is successfully contacted but the IRS returns no tax data. We finalized the policy to sunset after PY 2026, requiring Exchanges to resume acceptance of applicant attestations of their household income where the IRS, on behalf of the Treasury Secretary, reports that it has no data in response to a verification request under section 1411(c) of the Affordable Care Act. In the 2027 Payment Notice proposed rule (91 FR 6348), we proposed to permanently rescind the requirement under § 155.320(c)(5) that Exchanges accept attestations under the current rule, in favor of requiring Exchanges, beginning with applications for coverage for PY 2027, to collect documentation from applicants to verify an applicant's household income when the IRS returns no data.
There were many reasons that we opted to temporarily pause the requirement for Exchanges to accept household income attestation when tax data is unavailable. As outlined in the 2025 Marketplace Integrity and Affordability final rule, we believed that this policy may have helped contribute to the weakening of the Exchange eligibility system, which some agents, brokers, and web-brokers took advantage of by enrolling consumers in fully-subsidized plans they may not have been eligible for, oftentimes without those consumers' knowledge. Additionally, after reassessing our reasoning for implementing the original policy, we concluded that we no longer agreed that the original income verification process, including time and effort to submit verifying documents, was punitive. Given this, we concluded in the 2025 Marketplace Integrity and Affordability final rule that the administrative burden of the full income verification process was offset by program integrity benefits that reinstating this policy would have.
We finalized this provision in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) because we recognized that the imminent program integrity concerns were being driven by the existence of fully-subsidized plans. We noted that the expiration of the enhanced subsidies coupled with the temporary program integrity requirements enacted by the
( printed page 29620)
rule could alleviate the need for ongoing higher levels of program integrity policies beyond PY 2026. We stated that as the level of improper enrollments decreased in 2026, we expected the lower subsidy levels to appropriately deter future levels of improper enrollments from ever growing so high again, diminishing the returns of the temporary policies we enacted in that rule. In other words, the burden of continuing the temporary policy would reach a point at which it outweighed any benefits.
After further consideration, we proposed in the 2027 Payment Notice proposed rule to remove § 155.320(c)(5), eliminating the requirement to accept an applicant's household income attestation if the IRS does not return any tax data so that for PY 2027 and beyond, Exchanges must generally follow the existing income verification process when the IRS returns no data. We proposed to continue this policy based on our statutory authority and new consideration of impacts from the WFTC legislation.
Section 1411(b)(3)(A) of the Affordable Care Act requires consumers applying for APTC to provide income information described in the Code for the tax year ending the second year preceding the plan year. However, as APTC is determined based on annual household income for the plan year for which they are applying for coverage, when the consumer applies during the open enrollment period, they provide their projected income for the plan year rather than the income from the second year preceding the plan year. Section 1411(c)(3) of the Affordable Care Act requires HHS to submit this income information provided under section 1411(b)(3)(A) of the Affordable Care Act to the IRS for verification without exception. Section 1411(d) of the Affordable Care Act then requires HHS or the Exchanges to verify information submitted on the application that is not required to be submitted to the IRS. This includes income information on “changes in circumstances” under section 1411(b)(3)(B) of the Affordable Care Act as described in section 1412(b)(2) of the Affordable Care Act. Section 1412 of the Affordable Care Act outlines the process for determining APTC. Section 1412(a) directs the Secretary of HHS in consultation with the Secretary of Treasury to establish a program for determining APTC eligibility, and section 1412(b)(2) allows the Secretary of HHS to provide procedures for determining APTC eligibility when a change in circumstance has occurred, which includes substantial changes in income and when the household was not required previously to file a tax return. Finally, section 1412(c)(2)(A) of the Affordable Care Act requires the Secretary of Treasury to provide APTC to issuers on a monthly basis for the plan year.
Historically, given the inconsistency between the statutory requirement for HHS to develop an APTC eligibility process that generally uses income verified by the IRS from the second tax year preceding the plan year, and the fact that HHS must determine eligibility for APTC for the plan year (which occurs significantly after the tax year for which income is used for verification), we have interpreted section 1412(b)(2) of the Affordable Care Act to require households to provide projected annual household income to allow the Secretary of HHS to determine whether a change in circumstance has occurred since the second tax year preceding the plan. In instances where Exchanges receive IRS data as defined in 1411(b)(3)(A) of the Affordable Care Act, the applicant's projected annual household income is compared to that IRS data to determine if it aligns (within certain thresholds) or if there has been a change in circumstance. The Secretary then determines APTC based on projected income per section 1412(b)(2) of the Affordable Care Act if a change in circumstance has occurred and if a change in circumstance has not occurred, meaning the IRS data is aligned with the projected household income, the Exchange is effectively determining APTC based on IRS data for the second tax year preceding the plan year. Furthermore, section 1412(b)(2)(B) allows for instances in which an applicant was not required to file a tax return for the second preceding year to also be considered a change in circumstance, which is one reason why IRS data may not be returned for an applicant. When the IRS cannot verify income and there is a change in circumstance, HHS or the Exchanges then turn to verify income through additional trusted data sources under section 1411(d) of the Affordable Care Act.
In a situation where neither IRS data under section 1411(c)(3) of the Affordable Care Act nor additional trusted data sources under section 1411(d) of the Affordable Care Act can verify income, HHS must then follow the process in 1411(e)(4) of the Affordable Care Act to both require Exchanges to make a reasonable effort to determine the cause of the inconsistency and then allow the applicant the opportunity to correct the inconsistency within a 90-day period. In a situation in which an applicant lacks additional documentation or other supporting evidence of their attested income within the applicable time period, HHS would generally be compelled by statute to deny eligibility for APTC and CSRs based on the inconsistency with IRS data after the 90-day period has ended. In scenarios where IRS does not return income information for a household after the Exchange completes a data request, the statutory framework just outlined establishes additional verifications. When the Exchange's attempt to receive IRS information as stipulated in 1411(b)(3)(A) of the Affordable Care Act is not successful, we stated in the proposed rule that we believe that simply considering that attested annual household income fully verified is insufficient to the authority in section 1411(d) of the Affordable Care Act to verify change in circumstance information stipulated in section 1411(b)(3)(B) of the Affordable Care Act and determine the method of verification, as it does state that the Secretary “shall verify” that information. Absent IRS data, we stated in the proposed rule that we believe that it is necessary to proceed with further verification of this information in order to comply with the requirement in section 1411(d) of the Affordable Care Act to verify it, which would be more than simply accepting attestation.
Therefore, upon further review and consistent with our discussion in the 2025 Marketplace Integrity and Affordability proposed rule (90 FR 12968), we stated in the 2027 Payment proposed rule that we believe the best method of verification to be the current established verification processes for annual income, and that accepting attestation without further verification is not compliant with the requirement to, in some way, verify the information.
Finally, the newly applicable policy from the WFTC legislation provides much stronger motivation to verify consumer income information more stringently than previous practice. Under section 71305 of the WFTC legislation, repayment caps on excess APTC payments will discontinue starting in PY 2026. Absent this proposed policy, we stated in the proposed rule that households for whom IRS returns no data would have their annual household income verified by their attestation of projected household income and, if eligible based on this income, would receive APTC for the duration of the plan year (unless there is a change in eligibility). In contrast, under this proposed policy, we stated that such household incomes
( printed page 29621)
would likely be verified against additional trusted data sources and, if this verification fails, receive an income DMI that would require them to submit documents to verify their annual household income and, if they do not, would result in the loss of APTC after the 90-day DMI period. For years before 2026, section 36B of the Code provided a repayment cap on the maximum amount of excess APTC taxpayers with household income below 400 percent of the FPL were responsible for paying back when filing their Federal income tax for the year of coverage. Absent the proposed policy and with the removal of the repayment caps starting in 2026, we stated that tax filers whose APTC continues uninterrupted and whose actual household income is higher than their projected household income may have excess PTC and, if so, must pay back the full difference between their APTC and PTC, regardless of their income level. Therefore, we stated in the proposed rule that the proposed policy, which ends APTC for consumers who cannot verify their income with documentation, provides an important protection for consumers against significant tax liabilities. The Federal Exchange does have a process that allows consumers to report an unauthorized enrollment, which will allow them to avoid tax liabilities, but this requires the consumer to be aware of the improper enrollment and take actions to correct it. The Federal Exchange also permits issuers to report improper enrollments to HHS, which has the same effect of allowing the consumer to avoid tax liability for an enrollment they were unaware of and did not authorize.
We stated in the proposed rule that this is particularly important for consumers whose income is intentionally or unintentionally misrepresented by agents, brokers, web-brokers, or other intermediaries for enrollment on the Exchange. For example, we stated that many of these agents, brokers, and web-brokers intentionally estimate a household's attested income to receive the maximum amount of APTC possible in order to, even with the expiration of the enhanced subsidies, get consumers into low-cost plans that they may not otherwise be eligible for. While we previously stated in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) that we believe that unauthorized enrollments will decrease as a result of $0 benchmark plans no longer being available due to the expiration of the enhanced subsidies, we stated in the 2027 Payment Notice proposed rule that the removal of the repayment caps necessitates this policy becoming permanent to protect consumers from significant tax liabilities.
For these reasons, we stated in the 2027 Payment Notice proposed rule that we believe that the justifications for sunsetting this policy in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) starting in PY 2027 are now outweighed by the loss of the repayment caps. We had previously stated that the removal of the enhanced subsidies, and likely subsequent decrease in unauthorized enrollments, would mean that the corresponding Exchange costs and consumer burden for additional income verification, potential negative risk pool impact, and potential loss of coverage for low-income consumers would be greater than the positive program integrity benefits of making this policy permanent. We are now of the view that the risk of tax liability for these consumers outweigh those concerns, and providing that protection is necessary even with the costs, burdens, and coverage impacts this policy could result in. We reiterated in the proposed rule that applicants whose income is not returned by IRS would benefit from other verification procedures, including the Exchange checking other data sources beyond IRS and having 90 days to submit documentation to verify their attested annual household income.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. Further, we clarify that § 155.320(c)(5) does not require Exchanges to automatically set an income DMI as soon as IRS returns no data. Likewise, it does not change requirements for the rest of an Exchange's income verification process after the Exchange checks IRS data and IRS returns no data. Rather, this policy simply removes the requirement to accept an applicant's attestation of annual household income when the IRS returns no data. Once the IRS returns no data, Exchanges should continue with the rest of its income verification process under § 155.320(c)(3)(vi). Exchange income verification processes typically include checks of any additional data sources to determine whether the income information on the application can be verified before setting a DMI. Many State Exchanges check available data sources that maintain information specific to the state.
We summarize and respond to public comments received on the proposed policy below.
Comment:
Many commenters supported the proposal, including many commenters who stated the proposal would reduce fraud and protect enrollees against surprise tax bills by verifying attested information.
Response:
We appreciate the commenters' support and agree that this proposal will help mitigate the risk of fraud and large tax liabilities. An accurate annual household income estimate is a critical program integrity element for verifying and determining eligibility for APTC. We believe that checking annual household income against other trusted data sources through the alternative verification process are appropriate measures to ensure that an applicant's attestation of household income is accurate when a tax return is unavailable.
Comment:
Some commenters supported the proposal but provided recommendations such as providing exceptions for certain situations, providing State Exchanges with implementation flexibility, ensuring Exchanges are prepared to implement this proposal without undue harm to consumers, and allowing Exchanges to check additional data sources when tax data is unavailable.
Response:
We acknowledge that commenters believe that exceptions to this policy could be warranted and that they believe this policy should be optional for State Exchanges, but we do not agree as this policy ensures that every income attestation provided by households is verified either through a data source consistent with the requirements under section 1411(d) of the Affordable Care Act or through submitted documentation consistent with the requirements of section 1411(e)(4) of the Affordable Care Act. Given that the WFTC legislation eliminates APTC repayment caps, we have a responsibility to all consumers, regardless of whether they participate in an Exchange on the Federal platform or not on the Federal platform to ensure they are protected from large tax liabilities at tax filing. This requirement can reduce large tax liabilities by requiring that the income that APTC is based on is verified either through a data source or documentation provided by the consumer. Additionally, in the case that the household income is not accurate and cannot be verified, then households will only receive APTC for a limited number of months, specifically, the 90 days while the verification is pending, as opposed to
( printed page 29622)
the entire year if this policy were not finalized.
We appreciate the various comments identifying how this program integrity risk looks different for State Exchanges compared to States on the Federal Exchange. We acknowledge that many State Exchanges have robust income verification processes and can integrate well with additional data sources and their State's Medicaid and CHIP programs, making it more likely that consumers' income will be verified even when tax return data is unavailable. Since the scope of verification data sources State Exchanges have access to when tax return data is unavailable is extensive, this policy should impose limited burden on State Exchanges and their consumers. We believe that the improvements to program integrity and consumer protection outweigh the costs and burden of implementing this policy.
Comment:
Many commenters stated concern with this proposal, stating that it would create barriers for vulnerable consumers and increase administrative costs. Commenters also stated this could destabilize the risk pool because these changes could increase adverse selection because less healthy individuals have greater incentive to put in the time and effort necessary to resolve income verification issues.
Response:
We acknowledge commenters' concerns around administrative burden and risk pool impacts. We believe eligible applicants would likely have documentation to verify their household income. Although reintroducing income verification for applicants for whom IRS does not provide tax return data would increase the burden on some applicants, we do not anticipate this burden would deter many eligible people from enrolling as there are a multitude of documents that can verify income, and additionally, the Exchanges on the Federal platform have provided an extensive guide to verifying income with resources for households that struggle to obtain documentation.[168]
An accurate household income estimate is a critical program integrity element of the Affordable Care Act's framework for verifying and determining eligibility for APTC as, even those these consumers will be responsible for paying back the full amount of the difference between APTC and PTC upon filing their Federal income tax returns due to the removal of the repayment caps, it is still vital that Exchanges make the most accurate determination of APTC possible to protect consumers and federal funds, including funds the Federal government must expend to investigate, identify, and recoup improper APTC payments. We acknowledge the concerns about the impact of this proposal on the risk pool and agree about the importance of maintaining a healthy risk pool, but we believe that the positive impact to program integrity and protecting consumers from tax liability outweigh any negative impacts.
Comment:
Many commenters who opposed the proposal believed that when self-attestation does not match trusted data sources, this is not indicative of fraud but rather people whose income fluctuates often or dramatically enough that their projected household annual income would not match records for previous years. The commenters stated that this often occurs for consumers who are members of vulnerable populations, such as low-income consumers and those with chronic illnesses.
Response:
We acknowledge the commenter's concern about the variable nature of consumer income, especially in vulnerable populations. We proposed to require Exchanges to verify household income with other trusted data sources or through documentation when a tax return is unavailable because we believe it would strengthen program integrity by improving the accuracy of eligibility determinations across all Exchanges. While we acknowledge that these consumers would ultimately have to pay back any excess APTC during tax time given the removal of the repayment caps, it is still important to program integrity both to ensure Exchanges give the best and most accurate APTC eligibility determinations possible. Additionally, removing the requirement to accept attestations of household income when tax data is unavailable will help prevent consumers from large tax liabilities.
Comment:
Some provider groups stated concern that it could take vulnerable enrollees longer than 1 hour to submit documentation related to this income verification requirement.
Response:
We recognize that certain eligible consumer groups may experience longer document submission periods during the verification and data matching process and note that the 1-hour estimate is an average. However, all consumers will still have 90 days to submit documentation to verify their projected household income. We provide a robust list of acceptable documents [169]
that households can submit to resolve their income DMIs, and this list is included in multiple consumer notices and on the CMS website. We recommend that consumers for whom more common documents like paystubs and tax forms are either not available or are inaccurate submit one of many other suggested income documents that may be more available and accurate.
Comment:
Some commenters stated concern that the proposal would harm low-income consumers. They suggest shifting the focus of provisions to address the underlying issue of fraudulent activity by some agents and brokers.
Response:
As mentioned earlier in this section, an accurate annual household income estimate is a critical program integrity element for verifying and determining eligibility for APTC. While HHS is actively addressing unauthorized enrollments involving noncompliant actions by agents, brokers, or web-brokers, we cannot ignore program integrity risks presented by consumer-submitted information. We believe it is important to institute policies that address all program integrity concerns related to all program participants, and not just agents, brokers, and web brokers. This policy will also make it less likely that actions by non-compliant agent, brokers, or web brokers result in undetected improper enrollments.
Comment:
Some commenters noted how this proposal is under litigation and is currently stayed in
City of Columbus
v.
Kennedy,
many of whom stated they do not believe the proposal has meaningfully changed from what was finalized in the 2025 Marketplace Integrity and Affordability final rule. One commenter stated that this proposed rule does not properly address the sunset provision or public defenses of that rule.
Response:
We understand that this specific policy has been scrutinized in the past and understand why that raises concerns. However, we believe that this proposed and final rule address concerns raised in
Columbus v Kennedy.
As described earlier in this section, the WFTC legislation eliminates the excess APTC repayment caps that previously limited many consumers' financial liability when their APTC amount exceeded the amount of PTC they were eligible for based on their actual annual income. Without these caps, consumers who receive excess APTC may be required to repay a large amount. This change, which starts with PY 2026, makes accurate income verification critically important for plan years beyond 2025, which is when this
( printed page 29623)
policy was established to sunset in the 2025 Marketplace Integrity and Affordability final rule. For this reason, and considering the importance of determining accurate APTC amounts and related program integrity considerations of potential improper enrollments or plan switches by agents, brokers, and web-brokers, we find it necessary to finalize this policy removing the sunset provision established in the 2025 Marketplace Integrity and Affordability final rule.
Comment:
Some commenters stated concern that APTC would be denied to consumers if they do not have IRS data available to verify their income.
Response:
We clarify that if IRS data does not immediately verify a consumer's attestation of annual household income, Exchanges would go through the rest of the verification and data matching process. Specifically, Exchanges would check other available income data sources and, if those cannot verify the attested income, generate an income DMI and provide 90 days for the applicant to provide documentation substantiating their attested income. During the 90-day period, all members of the household would be determined temporarily eligible for APTC based on their application attestation (if otherwise eligible) and may use the APTC towards QHP coverage. It is only after that 90-day period has passed that the applicant, if the inconsistency is not verified, would have their APTC removed and be determined ineligible for APTC. Given this, we highly recommend consumers submit documents to verify their income during that 90-day period to ensure they maintain their APTC and health coverage.
14. Premium Payment Threshold (§ 155.400)
In the 2027 Payment Notice proposed rule (91 FR 6349), we sought comment on whether HHS should permanently discontinue regulatory options allowing QHP issuers to implement a fixed-dollar and gross percentage-based premium payment threshold for PY 2027 and beyond. In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), we finalized for PY 2026 that issuers are only able to implement a net percentage-based premium threshold for PY 2026 and, effective January 1, 2027, issuers will be permitted to implement the fixed-dollar threshold and either the net or gross premium percentage-based thresholds.
In the 2017 Payment Notice (81 FR 12271 through 12272), in which HHS established the option for issuers to implement a percentage-based premium payment threshold, we received comment requesting that issuers be allowed to establish a fixed-dollar threshold. At that time, we did not consider implementing a fix-dollar threshold because there can be cases where, due to the payment of APTC on behalf of an enrollee, even a low, flat-dollar amount could represent a large percentage of an enrollee's portion of the premium (81 FR 12272).
In the 2026 Payment Notice (90 FR 4475 through 4478), we implemented an option for issuers to establish a fixed-dollar premium payment threshold policy, under which issuers could consider an enrollee to have paid all amounts due in the following circumstance: the enrollee pays an amount that is less than the total premium owed and the unpaid remainder of which is equal to or less than a fixed-dollar amount of $10 or less, adjusted for inflation, as prescribed by the issuer. In addition, we implemented a gross percentage-based premium payment threshold policy, under which issuers could consider an enrollee to have paid all amounts due when the enrollee pays an amount that is equal to or greater than 98 percent of the gross premium, including payments of APTC, as prescribed by the issuer. If an enrollee satisfies the fixed-dollar or gross percentage-based premium payment threshold policy, the issuer may avoid triggering a grace period for non-payment of premium or avoid terminating the enrollment for non-payment of premium. However, these premium payment thresholds may not be applied to the binder payment.
We stated in the 2025 Marketplace Integrity and Affordability final rule, which was published after the 2026 Payment Notice, that, due to program integrity concerns stemming from the enhanced subsidies, offering these optional threshold flexibilities to issuers could enable a consumer to stay enrolled in a plan they are unaware of after payment of binder. At that time, we finalized modifications to § 155.400(g) that paused through the end of PY 2026 QHP issuers' ability to implement a fixed-dollar or gross percentage-based premium payment threshold. We specified that QHP issuers would regain authority to implement a fixed-dollar or gross-premium threshold after December 31, 2026. We explained that allowing the provision to sunset on December 31, 2026, would address the urgent improper enrollment concerns previously noted without permanently dismantling these premium threshold options.
Overall, HHS observed an increase in the number of unauthorized enrollment (UE) complaints made in 2025 compared to 2024; 229,734 were made in 2024 vs. 341,906 in 2025. However, although HHS continues to see noncompliant behaviors resulting in improper enrollments, we stated in the proposed rule that we believe that program integrity measures implemented over the past year, in addition to the expiration of enhanced APTCs that took effect on January 1 of this year, are likely to lead to a decrease in the number of UE complaints received. Data from the beginning of this year already demonstrate a substantial decrease, with 46,099 UE cases reported in January 2025 compared to 24,053 for January 2026, and this trend is likely to continue.
We have also continued working to implement policies to quickly resolve cases where a consumer may be dually enrolled in Medicaid and a QHP with financial assistance without their consent (referred to as “Medicaid UEs”). We have also implemented multiple data cleanup efforts and have worked with issuers to identify and resolve UEs. We continue to monitor complaints received and UEs resolved to ensure that program integrity concerns continue to decrease.
However, in addition to erroneous and improper enrollment data, we stated in the proposed rule that there is evidence that consumers in many instances are unaware that they remain in coverage. For example, in a recent internal analysis of claims data from 2019 through 2024, we found that among silver plans offered on- and off-Exchange, a significantly higher percentage (34 percent from PY 2023 through PY 2024) of on-Exchange silver enrollments were associated with no claims as compared to off-Exchange silver enrollments (18 to 23 percent from PY 2019 through PY 2024) across all years examined, with the greatest difference occurring in PY 2023 and 2024. This trend was reflected in the percentage of zero claim enrollments in each metal level and was even reflected among enrollees in 94 percent of CSR plans, where out-of-pocket costs are mostly covered by insurers, and where utilization is generally expected to be higher as compared to plans with lower or no cost-sharing assistance available. In addition to this, as we explained in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27140), continued access to zero-dollar bronze plans after the application of APTC increases the risk of fraudulent enrollments and consumers continuing to be enrolled in coverage they do not
( printed page 29624)
want. Despite the discontinuation of enhanced APTCs, it is estimated that 27 percent of enrollees can select a PY 2026 QHP with an after-APTC premium of $0,[170]
and 60 percent can select a PY 2026 QHP with an after-APTC premium of less than $50.[171]
The FFE does not collect data from issuers on whether they have implemented a premium payment threshold policy (nor the threshold type), but we have observed that of all auto re-enrolled consumers who had a $0 premium in 2024 but who newly had a non-zero premium in 2025 (1,831,739 consumers), 9.4 percent owed >$0-$5, 9.9 percent owed >$5-$10, while 27.6 percent of consumers owed >$10-$25, and 53.2 percent of consumers owed >$25.[172]
We stated in the proposed rule that this suggests that while these premium thresholds prevent some consumers from being placed in a grace period, they likely also exacerbate the problem of consumers unknowingly remaining in coverage they did not or no longer want, since many consumers have premiums that fall below the threshold and could avoid delinquency without making paying premiums. With the expiration of enhanced subsidies for PY 2026 and the continued availability of zero-dollar and lower cost plans after application of APTC, we stated in the proposed rule that we are of the view that it may be reasonable and necessary to continue to limit the fixed-dollar and gross-premium percentage-based thresholds beyond PY 2026.
Under the 2025 Marketplace Integrity and Affordability final rule, we finalized that issuers would re-gain the authority to implement fixed-dollar and gross-premium percentage-based thresholds after the end of the 2026 PY. This policy responded to commenter concerns that rescinding QHP-issuer flexibility to implement fixed-dollar and gross-premium percentage thresholds could create barriers to coverage for low-income enrollees who struggle to pay premiums and that consumers with chronic conditions might be able to utilize either the gross-premium percentage-based or fixed-dollar thresholds to avoid coverage gaps. It also acknowledged comments from State Exchanges and State-specific advocacy organizations that limiting this flexibility was unnecessary in States served by State Exchanges that experienced lower rates of improper enrollments.
While we recognized in the proposed rule the additional flexibility these policies might provide to consumers who may struggle in some months to pay their full share of their premium, we stated that we still believe it may be necessary to limit flexibilities to ensure that enrollees do not remain in coverage for extended periods of time without paying at least some of the premium owed. We stated in the 2025 Marketplace Integrity and Affordability final rule that this policy increases the risk that improper enrollments remain undetected, since the enrollee is less likely to receive invoices, and a delinquency or termination notice alerting them to the improper enrollment in the case that the individual or entity submitting the improper enrollment used false contact information. In addition, we stated that an enrollee who stops paying premiums in the belief that this would lead to termination of coverage may instead find that the coverage has continued for several months due to the issuer having implemented a fixed-dollar or gross percentage-based premium threshold, with the additional risk that the enrollee has accumulated a large amount of debt if the issuer has adopted a gross premium percentage-based threshold and the enrollee's gross premium is much higher than the de minimis $10 fixed-dollar threshold. We noted that, in contrast, this is not the case with the long-established net percentage-based threshold, under which enrollees must always pay at least some premium to avoid delinquency or loss of coverage.
As such, in the proposed rule, we stated that we are concerned that allowing the rescission of the fixed-dollar and gross-premium percentage-based threshold flexibilities to sunset for PY 2027 may exacerbate the risks we have outlined. We sought comment from interested parties on whether we should take no regulatory action and allow the policies to sunset at the end of PY 2026, or whether we should amend § 155.400 to rescind these policies for another fixed period of time or permanently in the interest of maintaining program integrity, as the fixed-dollar and gross percentage-based thresholds may hinder efforts at program integrity by allowing consumers to remain enrolled in unwanted coverage after payment of binder. In addition, we sought comment on whether it would be appropriate to grant State Exchanges the flexibility to adopt one or both of these thresholds, even if they remain unavailable for Exchanges on the Federal platform. We also sought comment on any other feedback interested parties may have on other changes HHS can make to the premium payment threshold policy.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing for all Exchanges the removal of the fixed-dollar and gross-premium threshold flexibilities. We summarize public comments received on the comment solicitation below.
Comment:
Most commenters opposed rescinding the fixed-dollar and gross premium percentage-based thresholds and stated that allowing issuers to treat de minimis premium shortfalls as paid helps prevent disproportionate coverage loss for consumers. Such commenters also stated that rescission of the threshold options will put more consumers at risk of delinquency or loss of coverage, particularly women with low incomes, other financially vulnerable populations, and consumers with chronic conditions.
Response:
We acknowledge that the additional thresholds may prevent coverage loss for some enrollees, but as we noted in the proposed rule, they also permit issuers to keep consumers enrolled in coverage while they owe unpaid premiums over an unreasonable period of time. We continue to observe high levels of UE on the Exchanges, and as we noted in the proposed rule, these thresholds may exacerbate this problem by enabling improper enrollments to go undetected for longer periods of time. As a result, we believe it is appropriate to finalize a repeal of the fixed-dollar and gross premium percentage-based thresholds beyond PY 2026.
Comment:
Some commenters stated that keeping the fixed-dollar and gross premium percentage-based thresholds would reduce administrative burden for State Exchanges and issuers, such as the administrative cost associated with the pursuit and collection of unpaid premiums, and delinquency and termination processes. Some commenters also stated that this would reduce administrative burden of having to terminate consumers over small payment errors.
Response:
While we acknowledge that there are costs associated with pursuing unpaid premiums, addressing and preventing persistent UEs is a priority for HHS because they result in increased Federal expenditures in identifying and correcting UEs. Additionally, consumers fraudulently enrolled in coverage with
( printed page 29625)
the fixed dollar and/or gross premium percentage-based thresholds may be receiving the benefit of APTC for a longer period of time due to these policies. Although APTC payments are eventually recouped if the improper enrollment is identified and reported to HHS, investigating improper enrollments and recouping APTC payments to issuers still increases Federal expenditures.
Comment:
Several commenters stated that they did not believe that thresholds contributed to UEs, but that agent/broker behavior contributed to UEs, and that limiting the thresholds would not address this issue. Commenters also stated that requiring binder payment to be paid in full before these thresholds went into effect is a program integrity measure.
Response:
We agree that requiring full payment of binder under this provision is an important program integrity measure. However, it is not sufficient given that issuers have told CMS, both in the context of rescissions and unauthorized reporting processes, that they see evidence of agents, brokers, and web-brokers making binder payments on behalf of enrollees. As a result, enrollees might not detect an improper enrollment and may remain enrolled in coverage while staying within the gross and/or fixed dollar thresholds.
Comment:
One commenter stated that CMS has not provided evidence that premium payment thresholds contribute to improper enrollment, but stated that permitting the new threshold options could contribute to improper enrollment, and that rescinding these flexibilities was imposing concrete harms to address only hypothetical problems—an approach the commenter stated was roundly condemned by the courts in both
City of Columbus
cases.
Response:
We do not agree and point to the improper enrollment and claims data provided in the preamble as evidence that consumers may unknowingly remain in coverage. As detailed in the preamble to this rule, we have provided substantial improper enrollment and claims data supporting our concern that consumers may unknowingly remain in coverage under premium payment threshold policies that allow coverage to continue without a meaningful premium contribution. Specifically, the preamble cites UE complaint trends showing that UE complaints reached historically elevated levels during the period of enhanced APTC availability. In 2024, there were 229,734 UE complaints, which increased to 341,906 UE complaints in 2025. Complaints have only recently begun to decline, with January 2026 UE cases (24,053), which is down substantially from January 2025 UE cases (46,099). Zero-claims enrollment data shows that approximately 34 percent of on-exchange silver enrollments from PY 2023 through PY 2024 were associated with no claims, which we have identified as a potential indicator of fraudulent or UE activity. In addition, almost 20 percent of returning enrollees had a net premium of $10 or less, creating conditions under which fixed-dollar or gross percentage-based thresholds that could allow improperly enrolled individuals to remain in coverage for the entire plan year Taken together, this data supports our determination that the program integrity risks associated with fixed-dollar and gross percentage-based thresholds are concrete and documented—not hypothetical—and that the harms associated with rescinding these threshold options must be weighed against the risk of allowing improper enrollments to persist undetected, during which Federal APTC expenditures continue to accrue on behalf of consumers who may not have knowingly enrolled in coverage.
Comment:
Some commenters stated that issuers, given their specific knowledge of local market dynamics, plan designs, and varying State billing capabilities, are best positioned to establish and update appropriate thresholds, and that a uniform Federal standard fails to account for the wide variation in premiums and payment infrastructure across States.
Response:
We acknowledge that issuers have specific knowledge of market conditions in their service areas. However, the net premium percentage-based threshold ensures consistent program integrity standards across the Exchanges and prevents the inconsistencies in payment obligations that can arise when thresholds vary by issuer. We will continue to evaluate whether a more flexible, issuer-driven approach may be appropriate in future rulemaking, considering both program integrity and consumer protection considerations.
Comment:
One commenter stated that dental plans have considerably lower premiums than medical plans and this flexibility will allow issuers to implement the appropriate type of threshold.
Response:
We acknowledge that standalone dental plan (SADPs) tend to have lower premiums than medical plans, but do not believe that the flexibilities allowed by the fixed-dollar and gross premium percentage-based thresholds outweigh the risk of increased or continued levels of improper enrollments that these thresholds allow.
Comment:
One commenter stated that the fixed-dollar and gross premium percentage-based threshold policies also help stabilize the risk pool, as those with higher health needs are more likely to maintain coverage while those in better health may be more likely to allow coverage to lapse.
Response:
While we agree that healthy individuals may be more likely to drop coverage over time and therefore may be more likely to remain in the risk pool longer when given more generous threshold policies, we do not agree that this justifies retaining the fixed-dollar and gross premium percentage-based thresholds. As documented in the preamble, a significant share of enrollees retained under these more generous threshold policies may be improperly or unknowingly enrolled, and although retaining enrollment for such individuals may have some minor positive impact on the risk pool, this does not outweigh the harms to program integrity this policy will address. We believe the net premium percentage-based threshold promotes a risk pool composed of individuals who are knowingly and actively enrolled—the appropriate foundation for long-term market stability.
Comment:
Several commenters stated that other proposals in this rule such as requiring individuals to proactively confirm enrollment, payer enforcement mechanisms, and proposals to monitor third party payments would better address the issue of UEs.
Response:
We appreciate commenters' suggestions on additional ways to address the problem of UEs on the FFE, and as we implement the longer-term requirements for consumers to confirm their enrollment,[173]
we intend to explore further payer enforcement mechanisms and methods of monitoring third party payments, as well as other ways in which the FFE can reduce the prevalence of misconduct in the future. However, as noted in the preamble to this section, we continue to believe that ending the fixed dollar and gross percentage-based premium thresholds will help address the problem of improper enrollments, and thus we believe it is appropriate to finalize this policy.
Comment:
One commenter stated that they support the collection of additional data about the extent to which these voluntary fixed dollar and/or gross percentage-based premium payment thresholds have been deployed and the
( printed page 29626)
impact of such threshold on the market, both in terms of retaining individuals enrolled in coverage, as well as possible tax and/or premium liabilities.
Response:
We appreciate the commenter's suggestion and intend to continue to collect data on the impact of premium thresholds on the FFEs.
Comment:
Several commenters stated that State Exchanges should be granted the flexibility to set their own premium payment threshold policy and decide whether to allow issuers to adopt such flexibilities based on their local market conditions. Commenters also stated that State Exchanges do not have the same levels of UEs and other fraud that the FFE has seen.
Response:
While we agree that State Exchanges have seen fewer fraudulent enrollments, we still maintain that the continuing number of improper enrollments represent a serious risk to program integrity. Until HHS observes a substantial and sustained decrease in the overall level of improper enrollments, rescinding the fixed and gross percentage thresholds for all Exchanges is necessary to ensure that this problem is not exacerbated. We note that State Exchanges would maintain the flexibility to adopt a net premium percentage-based threshold (which is not being rescinded) or not, based on their policy goals and market needs.
We will continue to work with State Exchanges to monitor improper enrollments.
Comment:
One commenter stated that CMS should only allow issuers to adopt a net percentage-based threshold because a fixed-dollar threshold policy may strain the consumer experience by opening the opportunity for certain enrollees (with a premium less than the fixed threshold amount) to stay active for multiple months, then enter into the grace period when finally exceeding the threshold, and that gross premium percentage-based threshold may confuse members since the enrollee would likely focus their attention to their responsibility amount rather than the total premium.
Response:
We agree with this commenter that a fixed-dollar threshold policy may allow a consumer who has not paid their full premiums to remain in coverage for multiple months. Similarly, a gross premium percentage-based threshold may create confusion for enrollees who are focused on their net premium responsibility—the amount they are required to pay after application of APTC—rather than the total gross premium amount, potentially leading to misunderstandings about their payment obligations and coverage status. For these reasons, we are finalizing the rescission of both the fixed-dollar and gross premium percentage-based threshold options and retaining only the net premium percentage-based threshold, which ensures that enrollees must always pay at least a proportional share of their actual premium obligation to maintain coverage and provides a clear, consistent, and uniform standard across all plan types and income levels.
Comment:
Several commenters supported rescinding the fixed-dollar and gross premium percentage-based thresholds because only allowing the net premium percentage-based threshold would improve consistency and program integrity by ensuring that payment requirements reflect the consumer's actual financial responsibility. Commenters also stated that allowing fixed-dollar and gross premium percentage-based thresholds was inappropriate due to the large amount of improper enrollments. Commenters further stated that issuers have a perverse financial incentive to tolerate improper enrollment since they would continue to receive APTC on behalf of the enrollee. Commenters also stated that rescission of the fixed-dollar and gross premium percentage-based thresholds would also protect those who have been fraudulently enrolled by reducing the likelihood that they remain enrolled and accumulate tax liabilities.
Response:
We agree with commenters that rescinding both the fixed-dollar and gross premium percentage-based thresholds is the appropriate course of action to promote program integrity and protect consumers. The net premium percentage-based threshold most accurately reflects each enrollee's actual financial obligation after application of APTCs, ensuring payment requirements are clear, uniform, and directly tied to the consumer's true financial responsibility. We also acknowledge commenters' observations that issuers would continue to receive Federal APTC payments regardless of whether an individual is knowingly enrolled. We agree that rescinding these threshold options will help protect consumers who have been fraudulently enrolled without their knowledge by increasing the likelihood that improperly enrolled individuals—particularly those who were enrolled with false contact information—can identify that they were improperly enrolled which would ultimately reduce the risk that they accumulate tax liabilities as a result of APTC payments made on their behalf if they were not eligible for QHP coverage or APTC. For these reasons, we are finalizing the rescission of both the fixed-dollar and gross premium percentage-based thresholds for PY 2027 and beyond. We will continue to work with issuers to promote continued monitoring of improper enrollments.
Comment:
One commenter requested that CMS also consider allowing consumers who experience an unexpected payment malfunction that results in termination of their policy to have that policy reinstated if that malfunction was the result of administrative or billing issues from the financial institution.
Response:
While this comment is out of scope for this final rule because it does not relate to the specific proposals included in the proposed rule, we appreciate the feedback and may consider these recommendations for future rulemaking.
15. Extend the Removal of the 150 Percent FPL SEP Beyond Plan Year 2026 (§ 155.420(d)(16))
To align Exchange regulations with section 71304 of the WFTC legislation, in the 2027 Payment Notice proposed rule (91 FR 6351), we proposed to remove § 155.420(d)(16) such that all Exchanges will continue to be prohibited from offering the 150 percent FPL SEP after PY 2026. In addition to removing § 155.420(d)(16), we also proposed conforming amendments to remove §§ 155.420(a)(4)(ii)(D) and 155.420(b)(2)(vii), and to revise § 155.420(a)(4)(iii).
The “150 percent FPL SEP” refers to a monthly SEP that was available, at the option of the Exchange, to individuals who were eligible for APTC and who had household income no greater than 150 percent FPL. This SEP enabled qualified individuals to enroll in an Exchange plan at any time and to change their Exchange plan up to once per month. We originally established the 150 percent FPL SEP in regulation, at the option of the Exchange, in part 3 of the 2022 Payment Notice (86 FR 53412). At the time, we stated that the primary objective of the 150 percent FPL SEP was to “make affordable coverage available to more consumers,” by making it easier for individuals to access the enhanced tax credits provided by section 9661 of the ARP (86 FR 53432). As finalized in part 3 of the 2022 Payment Notice, a consumer was required to have an applicable percentage of zero, meaning that they had access to a silver plan with a zero-dollar monthly premium after the application of APTC, to qualify for the SEP. In the 2025 Payment Notice (89 FR 26218), we removed the requirement that an individual have an applicable percentage of zero to qualify for the 150
( printed page 29627)
percent FPL SEP. In this rulemaking, we cited a commitment to “ensuring that affordable Exchange coverage is available for individuals with lower household incomes,” and required that an individual be eligible for APTC to qualify for the SEP (89 FR 26320).
In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), we finalized a policy that prohibited Exchanges from offering the 150 percent FPL SEP, effective from August 25, 2025, until the end of PY 2026, at which time the prohibition would “sunset” and Exchanges could begin offering the 150 percent FPL SEP again. We stated that pausing the availability of the 150 percent FPL SEP was necessary due to a rise in improper enrollments, including misuse of the SEP by agents, brokers, and web-brokers (90 FR 27114). Exchanges would have been permitted to begin offering the 150 percent FPL SEP again in PY 2027, and this pause was finalized in part due to significant concerns raised by commenters regarding the impact of a wholesale repeal of the SEP on low-income Americans who properly use this SEP pathway (90 FR 27114). We reasoned that after the enhanced subsidies expired and individuals were exposed to greater premium costs, the ability of individuals or actors on behalf of individuals to improperly enroll would be diminished, mitigating the risk of allowing Exchanges to offer the 150 percent FPL SEP (90 FR 27114).
The 2025 Marketplace Integrity and Affordability final rule was finalized on June 25, 2025. Shortly thereafter, on July 4, 2025, the WFTC legislation was signed into law. Section 71304 of the WFTC legislation amended section 36B of the Code such that a plan is not considered a QHP, and therefore no PTC is allowed for coverage under the plan, if the plan is enrolled in through an SEP that is based solely on the basis of the relationship of an individual's expected household income to the FPL and not on a change in circumstance (an “income-based SEP”). This provision is effective January 1, 2026.
Section 1411(a)(2)(A) of the Affordable Care Act provides that, for an individual who is claiming APTC or CSRs, the Secretary must determine whether the individual meets the income and coverage requirements of section 36B of the Code and section 1402 of the Affordable Care Act, respectively. HHS has interpreted section 1411(a)(2)(A) of the Affordable Care Act to require an Exchange to align its APTC eligibility rules with the Code's PTC eligibility rules. Therefore, HHS interprets section 71304 of the WFTC legislation to prohibit an Exchange from paying APTC for anyone enrolled in a plan if any individual enrolls in the plan through an income-based SEP, like the 150 percent SEP, that is not in connection with the occurrence of an event or change in circumstances specified by the Secretary.
Under the regulations finalized in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), Exchanges would have been permitted to resume offering the 150 percent FPL SEP beginning in PY 2027. However, due to requirements established by section 71304 of the WFTC legislation, we stated in the proposed rule that we have determined that permitting Exchanges to offer the 150 percent FPL SEP would provide no additional value and could potentially harm consumers. Throughout prior rulemaking on this topic, we have consistently stated that the primary goal of the 150 percent FPL SEP was to increase consumers' access to affordable coverage (see 86 FR 53432 and 89 FR 26320). We stated in the proposed rule that because consumers who enroll through the 150 percent FPL SEP are no longer allowed APTC for their coverage, permitting Exchanges to offer the 150 percent FPL SEP can no longer achieve this stated objective. Additionally, permitting Exchanges to offer the 150 percent FPL SEP could harm APTC-eligible consumers who enroll through the SEP, as section 71304 of the WFTC legislation prohibits payment of APTC to a plan if any enrollee in that plan enrolled through an income-based SEP.
For the reasons described in this section, we proposed to eliminate the “sunset” of the prohibition on Exchanges offering the 150 percent FPL SEP after PY 2026. To accomplish this, we proposed to remove the paragraph currently at § 155.420(d)(16). We further proposed conforming amendments to remove the paragraphs currently at § 155.420(a)(4)(ii)(D) and § 155.420(b)(2)(vii), which relate to plan category limitations and effective dates for the 150 percent FPL SEP, respectively. Finally, we proposed a conforming amendment to § 155.420(a)(4)(iii), related to plan category limitations, to remove a reference to the 150 percent FPL SEP.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal to extend the removal of the 150 percent FPL SEP below.
Comment:
Many commenters stated support for our proposal to extend the removal of the 150 percent FPL SEP beyond PY 2026. Commenters agreed with CMS' analysis that section 71304 of the WFTC legislation made the SEP much less valuable to consumers, given that consumers who utilized the SEP would not be eligible for APTC. Commenters further stated that Congress had sent a clear message that the 150 percent FPL SEP and other similar income-based SEPs needed to be discontinued.
Response:
We agree with commenters that continuing to prohibit the 150 percent FPL SEP is a sensible policy choice, given that APTC is no longer allowed for consumers who enroll through such SEPs. We also agree that while the WFTC legislation did not expressly prohibit Exchanges from offering the 150 percent FPL SEP, we believe that removing Exchanges' ability to offer the 150 percent FPL SEP likely aligns with Congressional aims.
Comment:
Several commenters stated support for our proposal to eliminate the 150 percent FPL SEP, observing that the SEP had previously made it easier for noncompliant agents and brokers to enroll consumers or change their plans without their knowledge. Commenters stated that eliminating the SEP would improve program integrity.
Response:
We agree with commenters that the 150 percent FPL SEP, in combination with the fully-subsidized benchmark plans available under the American Rescue Plan of 2021 [174]
and the Inflation Reduction Act of 2022,[175]
enabled significant improper enrollment.
Given that APTC is no longer permitted for enrollments through the 150 percent FPL SEP, we do not believe that permitting Exchanges to offer the SEP again would be significantly detrimental to program integrity. However, as noted in the preamble of this section, the 150 percent FPL SEP now offers very limited value to consumers, and we are therefore finalizing our proposal to no longer permit Exchanges the SEP.
Comment:
Several commenters stated support for eliminating the 150 percent FPL SEP, because the SEP had previously contributed to adverse selection. Commenters stated that the ability of individuals to wait until they had health needs to enroll, or to select a more generous plan if their health needs increased, inhibited issuers' ability to predict claims, leading to volatility in pricing and higher overall
( printed page 29628)
premiums. One commenter noted that the adverse selection driven by this SEP induced issuers to set much higher rates for higher-value plans, while allowing narrower network, lower-value plans to set lower rates.
Response:
We agree with commenters that the 150 percent FPL SEP previously contributed to adverse selection, given that it permitted consumers to newly enroll in coverage or to change plans as their health needs changed. We appreciate commenters sharing the ways in which the uncertainty caused by this SEP led to higher and distorted plan pricing.
Comment:
Some commenters supported eliminating the 150 percent FPL SEP because they believe that other SEP opportunities are sufficient to meet consumers' needs, especially given that States' work to “unwind” from the Families First Coronavirus Response Act (FFCRA) continuous enrollment condition and to return to regular eligibility and enrollment processes in Medicaid and CHIP has concluded.
Response:
We agree with commenters. The 150 percent FPL SEP was created in part to provide additional enrollment opportunities for consumers who lost Medicaid after the end of the FFCRA continuous enrollment condition, given the potentially high volume of terminations and the possibility that many consumers would not receive or not understand communications from their State Medicaid Agency (86 FR at 53434). Given that, following the end of the FFCRA continuous enrollment condition, States were required to achieve compliance with Federal renewal timeliness requirements by December 2025, we do not believe that continuing to offer a monthly SEP like the 150 percent FPL SEP is warranted. Consumers who lose Medicaid or CHIP qualify for an SEP for loss of minimum essential coverage under § 155.420(d)(1)(i). Under the special rule at § 155.420(c)(6), Exchanges have the option to permit consumers to access this SEP for 90 days following their loss of Medicaid or CHIP coverage, rather than the 60 days permitted for most other triggering events.
While we agree with commenters that SEPs other than the 150 percent FPL SEP are sufficient to meet consumers' needs, we also reiterate that we do not believe that permitting Exchanges to offer the 150 percent FPL SEP again would provide a meaningful enrollment opportunity given that APTC is no longer permitted for consumers who enroll through the SEP.
Comment:
Some commenters supported eliminating the 150 percent FPL SEP to support continuous, year-round enrollment. Commenters also noted that eliminating the SEP simplifies program rules and reduces consumer confusion.
Response:
We agree with commenters that monthly SEPs like the 150 percent FPL SEP are detrimental to Exchanges' ability to promote continuous, year-round enrollment. We also agree that the recission of the SEP provides Exchanges with an opportunity to re-emphasize the importance of the annual open enrollment period, of maintaining continuous enrollment, and of understanding what SEPs are available to individuals who experience a change in circumstance.
Comment:
One commenter supported the elimination of the 150 percent FPL SEP because they believed that CMS lacked the statutory authority to offer the SEP.
Response:
We appreciate the commenters' support for our proposal and acknowledge there are limits to our statutory authority to establish SEPs. We believe that SEPs should generally be reserved for changes in circumstance, rather than based solely on an individual's income. In the 2025 Marketplace Integrity and Affordability proposed rule (90 FR 12982), we noted that the statute requires a specific set of SEPs that focus on giving people an opportunity to enroll mid-year if they experience a change in their life circumstances, such as a move or the loss of job. We further noted that, in contrast, the 150 percent FPL SEP allows people to enroll at any time during the year based on their existing income, not a change in their income. Like this commenter, commenters to the 2025 Marketplace Integrity and Affordability proposed rule (90 FR 12982) also stated that the 150 percent FPL SEP departed from the ACA's structure to reserve SEPs for those experiencing life events necessitating a coverage change. However, in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27147), we concluded that given the substantial uncertainty over the future of the Exchanges and individual health insurance market, we did not believe a permanent repeal of the 150 percent FPL SEP was appropriate and, instead, finalized a pause to best balance the urgent need for program integrity with the long-term desire for enrollment efficiencies. In this final rule, we are removing this pause and, without further defining the limits of our statutory authority in establishing SEPs, believe removing the pause better aligns with the overall structure and purpose of SEPs.
Comment:
One commenter stated their support for the elimination of the 150 percent FPL SEP because it promotes alignment of SEP standards across on-Exchange and off-Exchange markets.
Response:
We agree that the elimination of the 150 percent FPL SEP promotes alignment of SEP standards across on-Exchange and off-Exchange markets, given that the 150 percent FPL SEP was not available off-Exchange.
Comment:
Several commenters opposed our proposal to eliminate the 150 percent FPL SEP. Commenters stated concerns that eliminating the SEP would disproportionately negatively impact individuals with low or volatile incomes, individuals experiencing frequent changes or gaps in employment, individuals with frequent changes to their household composition, individuals with housing instability, and individuals in States that have not expanded Medicaid by removing an important “safety net” enrollment opportunity. Commenters further stated concern that eliminating the SEP would remove a pathway to coverage for individuals who lose Medicaid or CHIP coverage, particularly given the possibility of noticing delays and of consumer confusion due to the fact that Medicaid and CHIP permit year-round enrollment. Commenters stated that they believed that this provision, particularly when considered in conjunction with a shorter OEP and increased SEP verification, would make it more difficult for consumers to access coverage. Some commenters noted that Exchanges should be permitted to offer the 150 percent FPL SEP because disallowing the SEP would result in consumers having longer periods of uninsurance, and to higher rates of uninsurance overall.
Response:
We acknowledge commenters' concerns regarding the elimination of the 150 percent FPL SEP. However, we reiterate that because section 71304 of the WFTC legislation no longer permits Exchanges to provide APTC for individuals who enroll through the 150 percent FPL SEP, the SEP can no longer provide a meaningful pathway to affordable coverage for the individuals that the SEP was designed to reach. While individuals with volatile incomes and employment situations, for example, may have been most likely to utilize the 150 percent FPL SEP, they are also least likely to be able to afford to enroll in plan absent the availability of APTC. We do acknowledge that if HHS permitted Exchanges to offer the 150 percent FPL SEP, there may be some consumers who would elect to enroll in coverage even though APTC would not be available. However, we do not believe that this is a compelling
( printed page 29629)
reason to permit Exchanges to offer the 150 percent FPL SEP for the following reasons.
First, as stated throughout prior rulemaking related to the 150 percent FPL SEP (86 FR 53432 and 89 FR 26320), the purpose of this SEP was to make affordable coverage available to more consumers. We do not believe that unsubsidized coverage can meaningfully be considered affordable for low-income consumers and therefore do not believe that the 150 percent FPL can achieve its intended purpose.
Second, HHS has an interest in preventing adverse selection. We believe that allowing Exchanges to offer the 150 percent FPL SEP is likely to contribute to adverse selection, given that the consumers most likely to enroll in unsubsidized coverage despite their low incomes are more likely to have significant medical needs.
Third, HHS has an interest in promoting year-round enrollment. Allowing Exchanges to offer the 150 percent FPL SEP would undermine this interest by allowing a pathway that consumers could use to enroll in or change plans at any time, despite not having experienced a meaningful change in circumstances.
We also acknowledge commenters' concerns about access to coverage for consumers losing Medicaid or CHIP. We clarify that, unlike for most other SEPs, Exchanges have the option to permit consumers losing Medicaid or CHIP coverage 90 days to enroll in a QHP through an Exchange, rather than the typical 60 days, per § 155.420(c)(6). We also clarify that, if an individual does not receive timely notice of their loss of Medicaid or CHIP, then the Exchange must permit the individual to enroll in coverage during the 60 days following the date that the individual knew, or should have known, that their loss of Medicaid or CHIP occurred, per § 155.420(c)(5). We believe that these existing policies provide sufficient enrollment options to consumers transitioning from Medicaid or CHIP to QHP coverage through an Exchange.
We acknowledge commenters' concerns that the removal of the 150 percent FPL SEP, when considered in conjunction with a shorter OEP and increased SEP verification, may make it more difficult for certain consumers to enroll in coverage, potentially leading to longer periods of uninsurance or higher overall rates of uninsurance. However, we believe that both the removal of the 150 percent FPL SEP and the shorter OEP, finalized in the Marketplace Integrity and Affordability final rule (90 FR 27074), have the potential to help promote continuous, year-round enrollment for consumers by ensuring that enrollments that occur during OEP are effective January 1, and that there are clear and limited opportunities available for enrollment outside of OEP. We also reiterate that permitting Exchanges to offer the 150 percent FPL SEP would not meaningfully make it easier for low-income consumers to enroll in coverage, given that they would not be permitted to receive APTC for their coverage.
Comment:
We received several comments that opposed the recission of the 150 percent FPL SEP because they believe that individuals who otherwise would have enrolled through the SEP will remain uninsured and will experience negative impacts to their access to healthcare, which may in turn result in additional costs to the healthcare system in the form of greater reliance on more expensive emergency care. Commenters detailed concerns related to the negative individual and population-level impacts of general care delays and avoidance, missed preventive services, interruptions in chronic condition management, decreased utilization of sexual and reproductive health screenings and care, and barriers to access of cancer treatment. Commenters stated that the removal of the 150 percent FPL SEP had the potential to exacerbate existing health disparities for individuals with low incomes. One commenter stated concerns related to downstream impacts on children's educational attainment, and the potential for responsibility for uninsured children's care to shift to already under-resourced schools. One commenter stated concerns that impacted individuals could lose access to trusted providers in the middle of treatment.
Response:
We appreciate commenters' concerns. However, we reiterate that section 71304 of the WFTC legislation prohibits APTC for individuals who enroll through the 150 percent FPL SEP. Because of this, we do not believe that permitting Exchanges to offer the 150 percent FPL SEP is likely to alleviate the concerns that commenters raised regarding potential uninsurance and downstream negative health impacts, given that consumers with incomes at or below 150 percent of the FPL are unlikely to choose to enroll in an unsubsidized QHP.
We do not agree that prohibiting Exchanges from offering the 150 percent FPL SEP could result in enrollees losing access to providers in the middle of treatment. The recission of the 150 percent FPL SEP will not result in individuals who are already enrolled in a QHP through an Exchange losing their coverage. On the contrary, the removal of the 150 percent FPL SEP ensures that individuals do not have the opportunity to change plans mid-year solely on the basis of their income, therefore reducing the risk that consumers may change to a new plan that unexpectedly disrupts their access to existing providers.
Comment:
Some commenters opposed the recission of the 150 percent FPL SEP because they believe that eliminating the SEP will increase individuals' “churn” in and out of coverage, and will reduce continuity of coverage.
Response:
We do not agree that no longer permitting Exchanges to offer the 150 percent FPL SEP will cause increased “churn” or will have negative impacts on continuity of coverage. On the contrary, making it clear to consumers that the only available enrollment opportunities are the annual OEP and specific, time-limited SEPs tied to changes in circumstance promotes continuity of coverage. We fail to see how eliminating the 150 percent FPL SEP contributes to “churn,” given that the availability of the SEP has no impact on consumers ability to keep their Exchange coverage.
Comment:
Some commenters opposed the removal of the 150 percent FPL SEP because they believed that the SEP, while it was implemented, resulted in a lower-than-expected risk of adverse selection. One commenter noted that HHS did not provide evidence that individuals who enrolled through the 150 SEP were more likely than others to be adversely selected. One commenter noted that the 150 percent FPL SEP did not pose a risk of adverse selection because consumers had no incentive not to enroll in and maintain enrollment in low-cost coverage, and that their State Exchange had not identified an adverse selection impact from the SEP. One commenter stated that they believed the 150 percent FPL SEP was an important tool for bringing healthier enrollees into the risk pool and driving down premiums.
Response:
Even if we accept commenters' notions that the 150 percent FPL SEP had a limited, or neutral, or even positive impact on adverse selection, we do not believe that these would be compelling reasons to allow Exchanges to offer the 150 percent FPL SEP. We reiterate that because section 71304 of the WFTC legislation prohibits APTC for enrollments through the 150 percent FPL SEP, the SEP now provides very limited value to consumers and would not serve its purpose of making affordable coverage available to more consumers.
Comment:
One commenter noted that there is no evidence of improper
( printed page 29630)
enrollment through the 150 percent FPL SEP in State Exchanges, and stated that they support “continued state flexibility with regard to all SEPs.”
Response:
Even if we accept commenters' notions that the 150 percent FPL SEP does not drive improper enrollment in State Exchanges, we do not believe this would be a compelling reason to allow Exchanges to offer the SEP. As stated throughout this section, the 150 percent FPL SEP can no longer serve a meaningful purpose given that the WFTC legislation prohibits Exchanges from providing APTC for individuals who enroll through the SEP.
We clarify that § 155.410(a)(2) provides that Exchanges may only permit individuals to enroll in or change QHPs during the OEP or during the SEPs enumerated in 45 CFR 155.420. While § 155.420 provides some limited flexibility to Exchanges, such as by allowing Exchanges to decide whether to consider certain triggering events SEP-qualifying, State Exchanges do not have flexibilities with regard to determining SEP policy beyond those specifically described in § 155.420.
Comment:
Some commenters noted alternatives to no longer permitting Exchanges to offer the 150 percent FPL SEP. One commenter requested establishing a new “narrowly tailored, fraud-resistant” SEP. Other commenters requested implementing oversight policies focused on agents and brokers with a history of fraudulent activity, combined with robust outreach to eligible consumers to ensure that they are able to access coverage.
Response:
We are no longer permitting Exchanges to offer the 150 percent FPL SEP because SEP can no longer serve its intended purpose of promoting access to affordable coverage, given that the WFTC legislation prohibits Exchanges from providing APTC for individuals who enroll through the SEP. We are uncertain what the appropriate parameters for a “narrowly tailored” SEP would be, nor how Exchanges could meaningfully ensure that it was “fraud-resistant.”
We remain committed to addressing fraud, waste, and abuse, including by strengthening oversight of Exchange agents, brokers, and web-brokers. Policies related to strengthening oversight of agents, brokers, and web-brokers are discussed in section III.D.6. of this final rule. We also remain committed to providing consumers with clear and accurate information about the SEPs for which they may be eligible.
Comment:
Some commenters stated that they believed the removal of the 150 percent FPL SEP was harmful, but they understood that HHS' proposal to no longer allow Exchanges to offer the SEP was driven by statute. They requested that HHS identify other administrative options to minimize harm, such as streamlining transitions from Medicaid and CHIP to Exchange coverage, and supporting State Exchanges in exploring additional enrollment pathways. Commenters requested HHS to conduct robust outreach and communication regarding the removal of the 150 percent FPL SEP and to clearly communicate about remaining enrollment options, to mitigate coverage losses.
Response:
We appreciate commenters' recognition that the proposal to no longer allow Exchanges to offer the 150 percent FPL SEP is reasonable given the statutory changes made under section 71304 of the WFTC legislation. We are continually working with State Medicaid and CHIP agencies to streamline transitions between Medicaid or CHIP and Exchange coverage. We will also continue to work with any State Exchanges interested in exploring the limited SEP-related flexibilities available to Exchanges under § 155.420.
We are also committed to providing consumers and all Exchange interested parties with timely and accurate information regarding SEP availability. As part of our implementation of the Marketplace Integrity and Affordability final rule, which prohibited Exchanges from offering the 150 FPL SEP effective August 25, 2025, we updated language on
HealthCare.gov,
and worked with agents and brokers, navigators, and State Exchanges to provide clear information about the upcoming changes. Given that the policy finalized in this rule simply extends the existing prohibition on Exchanges offering this SEP, we plan to continue to provide accurate information regarding SEPs on
HealthCare.gov,
as well as make available frequent opportunities for interested parties to learn about SEP policy and operations.
Comment:
Some commenters noted that section 71304 of the WFTC legislation prohibited APTC for individuals who enroll through the 150 percent FPL SEP, but still felt that CMS should permit Exchanges to offer the SEP. One commenter, a State Exchange, noted that some States offer generous State-funded subsidies to enrollees, and that because individuals who enroll in Exchange coverage through an income-based SEP could still access those state-funded subsidies, that the 150 percent FPL SEP could be valuable to consumers and Exchanges should therefore be permitted to offer the SEP. One commenter stated that HHS should permit Exchanges to offer the 150 percent FPL SEP because individuals who enrolled through the SEP could still access CSRs.
Response:
We acknowledge that there are limited cases in which permitting Exchanges to offer the 150 percent FPL SEP could provide a meaningful pathway to enrollment for some consumers. These include cases in which a State subsidizes enrollees' premiums, or in which an enrollee determines they are able to afford to enroll in an unsubsidized QHP. However, we do not believe that these limited use cases justify permitting Exchanges to offer the 150 percent FPL SEP for a number of reasons.
First, we believe that there is significant likelihood for confusion from both consumers and Exchanges if HHS were to permit an enrollment opportunity that could not be meaningfully used by most enrollees.
Second, while HHS regulations do permit certain limited flexibilities to State Exchanges regarding which SEPs to provide, we also have a compelling interest in promoting clear and uniform SEP policy. Given the high volume of utilization of the 150 percent FPL SEP as compared to other SEPs for which HHS regulations continue to permit limited flexibilities, we believe that permitting Exchanges to offer the 150 percent FPL SEP would damage our ability to promote uniform SEP policy in a way that other existing flexibilities do not. During plan year 2024, approximately 1.9 million consumers enrolled in or changed plans through the 150 percent FPL SEP through the FFE, as compared to fewer than 13,000 consumers who enrolled in or changed plans through the other optional SEPs permitted under §§ 155.420(d)(6)(v) and (d)(13). While we do expect that 150 percent FPL SEP utilization would likely decrease significantly if we were to permit Exchanges to offer the SEP, we still believe that past utilization provides important context about the ways in which allowing the SEP to be offered in States with generous State-funded subsidies could result in differences in SEP policy and functionality that far exceed the differences resulting from other flexibilities permitted under § 155.420.
Finally, we clarify that our interpretation of section 71304 of the WFTC legislation is that Exchanges would be required to prohibit not just APTC, but both APTC and income-based CSRs, for otherwise-eligible individuals who enrolled through the 150 percent FPL SEP. In the preamble in this section, we note that section
( printed page 29631)
71304 of the WFTC legislation amended section 36B of the Code such that a plan is not considered a QHP, and therefore no PTC is allowed for coverage under the plan, if the plan is enrolled in through an SEP that is based solely on the basis of the relationship of an individual's expected household income to the FPL and not on a change in circumstance. We further note that we interpret section 71304 of the WFTC legislation to prohibit an Exchange from paying APTC for anyone who enrolls in a plan through the 150 percent FPL SEP.[176]
Here, we clarify that Exchanges are also prohibited from allowing income-based CSRs for anyone who enrolls in a plan through an income-based SEP. This is because section 1402(g) of the Affordable Care Act provides that CSRs are not permitted for a month unless it is considered a “coverage month” under section 36B of the Code. Under paragraph (c)(2)(A) of section 36B of the Code, a month is generally only considered a coverage month if, as of the first day of the month, the individual is covered by a QHP. Because section 71304 of the WFTC legislation provides that a plan is not a QHP if it is enrolled in through an SEP based solely on income, section 71304 therefore prohibits Exchanges from providing income-based CSRs to individuals who enroll through the 150 percent FPL SEP.
Comment:
One commenter noted their agreement with CMS' proposal to all Exchanges to begin offering the 150 percent FPL SEP again.
Response:
We clarify that this provision will continue the prohibition on Exchanges offering the 150 percent FPL SEP, for the reasons described in the proposed rule and in this section.
Comment:
One commenter opposed HHS' proposal to prohibit Exchanges from offering the 150 percent FPL SEP because the provision was stayed.
Response:
We clarify that the provision of the Marketplace Integrity and Affordability final rule that prohibited Exchanges from offering the 150 percent FPL SEP, effective August 25, 2025, through the end of PY 2026, was not stayed by the Court in
City of Columbus et al.
v.
Kennedy et al.[177]
16. Special Enrollment Period Verification (§ 155.420(g))
In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), we finalized the removal of the restriction for Exchanges on the Federal platform to only conduct Special Enrollment Period Verification (SEPV) for Loss of Minimum Essential Coverage (MEC) cat § 155.420(g). This allowed the Federal Exchange to conduct SEPV for additional SEPs. We also finalized a regulation that required Exchanges on the Federal platform to conduct SEPV for at least 75 percent of new enrollments. The final rule included a provision that both of these provisions were set to sunset on December 31, 2026.
In the 2027 Payment Notice proposed rule (91 FR 6352), we reproposed these provisions as their implementation was stayed by the Court in
City of Columbus et al.
v.
Kennedy et al.
on August 22, 2025.[178]
In reproposing these provisions following the Court's stay, we stated that this proposal reflects changes in circumstances and new supporting information since the original policy was established. This includes the passage of the WFTC legislation and additional insights from the resumption of SEPV for Loss of Minimum Essential Coverage (MEC) that occurred on May 16, 2025 in compliance with current SEP in verification regulations at § 155.420(g) for Exchanges on the Federal platform. Our proposal for the two SEPV policies did not include a sunset provision.
We included the sunset provision in the 2025 Marketplace Integrity and Affordability final rule because we recognized that the then-imminent program integrity concerns were being driven by the existence of fully-subsidized plans. We noted that the expiration of the enhanced subsidies coupled with the temporary program integrity requirements enacted by the rule would right-size Exchange enrollment in PY 2026 and would obviate the need for ongoing higher levels of program integrity policies. We stated that as the excess levels of improper enrollments are reduced in PY 2026, we expected the lower subsidy levels to appropriately deter future levels of improper enrollments from ever growing so high again, diminishing the returns of the temporary policies we are enacting in the rule. In other words, the burden of continuing such policies would have reached a point at which they would outweigh any benefits.
In the proposed rule, we stated that we now believe reproposing these policies (without a sunset) is necessary to ensure integrity in the Exchanges and help limit fraudulent enrollments. The proposal to require Exchanges on the Federal platform to conduct SEPV for the loss of MEC SEP is a return to a previous policy that was implemented pursuant to the 2017 Marketplace Stabilization rule. The SEP verification policy in the 2017 rule was driven in part by a 2016 GAO undercover test study of SEPs. The study observed that self-attestation could allow applicants to obtain subsidized coverage they would otherwise not qualify for and then found 9 out of 12 of GAO's fictitious applicants were approved for coverage on the Federal and selected State Exchanges.[179]
As a result, we implemented verification for the largest SEPs on the Federal Exchange.
Once SEPV was implemented, we studied how the consumer experience was impacted. For PY 2017, a report showed that we averaged a response time of 1-to-3 days to review consumer-submitted documents. In addition, the vast majority (over 90 percent) of SEP applicants who made a plan selection and were required to submit documents to complete enrollment were able to successfully verify their eligibility for the SEP. We conducted additional research for the following plan years through 2021. Based on data from PY 2019, the last year prior to the COVID-19 PHE, which greatly impacted SEPV processing, the majority of consumers (73 percent) were able to submit documents within 14 days of their SEP verification issue (SVI) being generated. Also, we found that the majority of consumers (63 percent) were able to fully resolve their SVI within 14 days of it being generated. That resolution percentage increased to 86 percent by 30 days.[180]
We also found that for PY 2019, only approximately 14 percent or 75,500 individuals were unable to resolve their SVI out of the total population of SEP consumers who received an SVI. We stated in the proposed rule that the data shows that the value of SEPV processing and the program integrity benefits it provides to the Exchanges is greater than the minimal burdens those same processes place on individuals.
We proposed the 75 percent verification threshold for new SEP enrollments because we believe that most Exchanges would be able to meet it by verifying at least two or three of their largest SEP types based on current SEP volumes. The determination of how many enrollments would constitute 75 percent would be required to be based
( printed page 29632)
on enrollment through all SEPs in the prior plan year. We stated that this would provide Exchanges with implementation flexibility so they can continue to decide which special enrollment types to verify and the best way to conduct that verification. We did not propose to require Exchanges to verify eligibility for all SEPs, because we have determined that the cost to verify eligibility for SEPs with very low utilization rates could be greater than the benefit of verifying eligibility for them.
We stated in the proposed rule that for SEPs that are being verified, the Exchange would “pend” the consumer's enrollment, meaning that it would not be effectuated until the Exchange verified eligibility for enrollment through the SEP. If the Exchange is unable to verify such eligibility, we stated that the consumer would not be eligible for enrollment through the Exchange under that SEP, and any plan selection under that SEP would be canceled (meaning, terminated before coverage is effectuated) and would not result in enrollment.
Verification for the loss of MEC SEP, which is required under § 155.420(g), was paused through the Covid-19 PHE to ensure consumers could maintain access to continuous coverage. This pause in verification ended on May 16, 2025. After resuming verification for the Loss of MEC SEP on May 16, 2025, we noticed shifts in enrollment trends begin to occur.[181]
Prior to the resumption of verification, in April of 2025, the Loss of MEC SEP accounted for approximately 330,000 SEP enrollments which was 48 percent of all SEP enrollments at that time in Exchanges that use the Federal platform. As of September 2025, the Loss of MEC SEP accounted for 95,000 SEP enrollments, which was down to 27 percent of all SEP enrollments at that time.[182]
We also noticed during this same period that several other SEP types had their overall percentage of SEP enrollments increase quite substantially. For example, the Move SEP went from 1 percent to 21 percent of all SEPs, and the Medicaid/CHIP Denial SEP increased from 8 percent to 24 percent of all SEP enrollments. We stated in the proposed rule that this data suggests that consumers shifted their SEP attestation so as not to have to provide verification of eligibility for the SEP.
We acknowledged in the proposed rule that some shift in SEP volumes was expected due to our best SEP logic, which is a set of hierarchy rules that Exchanges on the Federal platform use to determine what the “best SEP” is for a consumer (generally based on the most advantageous coverage effective date for the qualifying life event experienced by the consumer, verifiable with documents as required), in the event that they attest to multiple SEP qualifying events, such as losing MEC, while also gaining a dependent. Essentially, consumers are often eligible for more than one SEP type and, once verification resumed, another SEP type may become the best SEP for a consumer. However, the substantial shift cannot be explained by that logic alone as these trends do not match any of our historical SEP enrollment data.
When SEPV was first implemented in 2017 and 2018, we noticed shifts in SEP enrollment patterns that resulted in non-verified SEPs making up a larger portion of the total SEP population. For example, the overall portion of consumers granted a non-verified SEP that made them eligible for the Exchange increased from 2.5 percent in 2017 to 10 percent in 2018. During that same period, the Loss of MEC SEP decreased from 60 percent of all SEPs in 2017 to 54 percent in 2018, and the Medicaid/CHIP Denial SEP decreased from 24 percent in 2017 to 19 percent of all SEPs in 2018. From 2019 to 2024, although SEP enrollment volume increased drastically, the proportion of enrollment though each SEP stayed relatively similar. The introduction of the under 150 percent FPL SEP did result in the volume of other non-verified SEPs decreasing. The only notable changes were that the total portion of loss of MEC SEPs increased 5 percent and Medicaid/CHIP denial decreased 6 percent. Given the mass shift away from the loss of MEC SEP throughout 2025 and the significant growth in non-verified SEPs during the same time frame, we stated in the proposed rule that we believe there is a high likelihood action is being taken to intentionally avoid SEP verification. We stated that we believe this trend is being driven primarily by agent and broker activity as 86 percent of SEP enrollments are through agents and brokers.
In addition to trying to mitigate the concern that individuals are attesting to SEPs they are not eligible for in order to avoid verification, we stated in the proposed rule that we believe SEP verification would also help deter bad actors and those who are ineligible to enroll in coverage from gaining access to the Exchanges. We stated that we believe that this would help to reduce rates by preventing individuals who are waiting until they are sick to enroll from utilizing SEPs for which they may be ineligible. As we explained in the 2025 Marketplace Integrity and Affordability rule, we believe that continued access to zero-dollar bronze plans increases the risk of fraudulent enrollments and ineligible individuals gaining access to coverage through SEPs that do not require verification. We believe that increased SEP verification, as we stated in that rule, would reduce the risk of fraud and ineligible enrollments related to zero-dollar bronze plans in the FFE.
For the reasons provided above, we reproposed without a sunset at § 155.420(g), the provision to remove the restriction for Exchanges on the Federal platform to only conduct SEPV for Loss of MEC, and the provision to require Exchanges on the Federal platform to conduct SEPV for at least 75 percent of new enrollments.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal to resume Special Enrollment Period Verification.
Comment:
Several commenters stated concerns regarding how the proposed policy would apply given
City of Columbus
v.
Kennedy
litigation.
Response:
Though SEPV provisions finalized in the 2025 Marketplace Integrity and Affordability rule were stayed in
City of Columbus
v.
Kennedy,
SEPV was originally enacted with the publication of the 2017 Market Stabilization Rules as a program integrity tool to reduce the incidence of consumers who use an SEP to enroll in coverage when they are not eligible to do so, which caused significant instability to the risk pools and increased the financial burden on issuers. We are finalizing the proposal to resume SEPV to address similar program integrity concerns identified in the 2017 Market Stabilization Rules, but with the added goal of preventing consumers from being subject to unauthorized enrollment and unauthorized plan switches. Specifically, When SEPV was initially implemented, the goal was to reduce the immediate burden on risk pools caused by consumers using an SEP for which they were not eligible to enroll into coverage only when they needed medical care. This current proposal is intended to similarly to protect the risk
( printed page 29633)
pool from adverse selection and to reduce the incidence of unauthorized enrollment and unauthorized plan switches which can more easily be accomplished when an applicant does not have to verify that they are eligible for a SEP (other than provide an attestation).
Comment:
Some commenters stated concern with the perceived increased administrative burden on State Based Exchanges, agents and brokers, as well as consumers. They point to large upfront costs to a State Exchange to develop verification infrastructure, increase time burden on agents and brokers in assisting consumers with submitting documents, and the difficulty that some consumers might experience with locating and requesting documents to resolve their SVI.
Response:
Commenters on the 2025 Marketplace Integrity and Affordability Rule estimated that the initial cost per State Exchange to develop their own verification infrastructure would be $12 to 60 million. While we recognize that these estimated operational costs may be significant, commenters did not address the ongoing impact that adverse selection and improper enrollments may have on the program and consumers. To mitigate the operational impact on SBEs, we proposed, and are finalizing a requirement that they verify only 75 percent of SEP enrollments.
Agents, brokers, and web-brokers currently have access to training and resources that detail the SEP verification process and the documents required to resolve each SVI, therefore, we do not believe that SEPV will increase time burden on agents and brokers in assisting consumers with submitting documents. Additionally, the documentation required to resolve SVIs does not represent a wholly new type of administrative burden for consumers, as consumers may already encounter documentation submission requirements in connection with other eligibility and verification processes.
For example, under a Loss of MEC SEP, which is one of the most commonly utilized SEPs, consumers who lose employer-sponsored coverage may receive documentation from their employer that they could provide to the Exchange to demonstrate eligibility for the SEP. Accordingly, while we recognize that SEPV may impose administrative burden on agents, brokers, web-brokers, and consumers, we do not believe that such burden is unreasonable in light of the program integrity and consumer protection benefits associated with SEPV.
Comment:
Some commenters noted that SEPs in general are underutilized, that self-attestations are sufficient to demonstrate eligibility for most SEPs, that monthly SEPs should be allowed to provide consumers with more flexibility, and that CMS should be working to make enrollment easier, not more difficult. Some commenters suggested that CMS should make a single-button reenrollment option to streamline the reenrollment process for consumers, accept “reliable” self-attestations to justify SEP eligibility, and provide temporary eligibility to consumers while they wait for their SVI to be resolved. Commenters also indicated that consumers prefer to choose a SEP that has no documentation requirement over a SEP with an SVI requirement as a matter of practicality.
Response:
Though enrollment and eligibility should remain as simple as possible to encourage consumer engagement, it must be balanced with a verification process to protect consumers from the real financial and access to care issues that can arise from improper enrollment. Due to unauthorized enrollments, consumers who were originally enrolled in Medicaid and subsequently enrolled in Exchange coverage may experience interruptions in critical medical care as a result of overlapping coverage rules, because Medicaid is generally the payer of last resort and may refuse to pay claims if the consumer is also enrolled in a QHP. Consumers who receive APTCs for which they are not eligible may incur significant tax liabilities, in some cases exceeding $10,000 in a single plan year, for larger households. Though SEP verification could be perceived as a burdensome or unnecessary process, it will help protect the risk pool from adverse selection.
Regarding the suggestion to accept “reliable” attestation, we note that an Exchange generally cannot assess the reliability of an attestation absent supporting documentation. Additionally, even if an Exchange were to accept attestation that it deems reliable, by failing to confirm eligibility through documentation, it could nonetheless facilitate improper enrollments. Nevertheless, we do intend to allow Exchanges to verify at least 75 percent of SEP enrollments because we believe that most Exchanges are able to meet this verification threshold based on current SEP volumes.
We acknowledge that the SEPV requirement adds a minor administrative burden to the enrollment process; however, we are unable to determine whether this burden contributes to consumers foregoing coverage through the Exchange. Consumers may view a single-button re-enrollment process as a convenient option when engaging with the Exchange, but it may also reduce the likelihood that consumers will carefully review their applications or select the SEP most appropriate for their circumstances. As a result, consumers may experience interruptions in coverage or unexpected medical costs. For example, consumers who do not review their applications may remain enrolled in coverage that no longer meets their medical or financial needs, fail to account for changes in plan benefits or provider networks, or neglect to report updated household or income formation that affects eligibility for APTCs. These circumstances may result in gaps in access to care or the reconciliation of excess APTCs on a subsequent tax return.
Awarding temporary coverage to consumers while their SVI is being processed also has the potential to cause harm to consumers. Although we recognize the importance of access to care, consumers who are granted temporary QHP eligibility, use their coverage, and are ultimately found ineligible for the SEP, could become financially responsible for the cost of care received after the issuer cancels coverage and rescinds payment. The current pended plan selection process is required for Exchanges on the Federal platform (which provides that a consumer's enrollment is not effectuated until the Exchange verifies the SVI) balances the consumer's need for access to care while protecting them from unexpected medical costs.
Additionally, granting consumer's eligibility for the 30 days during which their SVI is being processed, regardless of their ability to provide sufficient documentation, could recreate the conditions that initially led to the establishment of SEPV. Allowing temporary eligibility could allow consumers to use a SEP to enroll in coverage only when they need medical care, and then to let the SVI expire and become uninsured after such medical care is received. This would promote adverse selection and could cause significant instability to risk pools.
17. Expansion of Hardship Exemption Eligibility (§ 155.605(d)(1))
In the 2027 Payment Notice proposed rule (91 FR 6353), we proposed to amend § 155.605(d)(1) to codify the expansion of hardship exemption eligibility to individuals who are ineligible for APTC or CSR due to projected household income below 100 percent or above 250 percent of the FPL.
Section 5000A(e)(5) of the Code establishes an exemption from the
( printed page 29634)
individual shared responsibility payment based on hardship or lack of affordability, and section 1302(e) of the Affordable Care Act limits eligibility for catastrophic coverage to individuals under age 30 at the start of the plan year or those who have received a hardship or affordability exemption. Under § 155.605(d), hardship exemptions include circumstances that prevent an individual from obtaining coverage through a QHP. Section 155.605(d)(1) states that the Exchange must grant a hardship exemption to an individual for at least the month before, the month or months during which, and the month after a specific event or circumstance, if the Exchange determines that: (1) the individual experienced financial or domestic circumstances, including an unexpected natural or human-caused event, such that he or she had a significant, unexpected increase in essential expenses that prevented him or her from obtaining coverage under a QHP; (2) the expense of purchasing a QHP would have caused the individual to experience serious deprivation of food, shelter, clothing or other necessities; or (3) the individual has experienced other circumstances that prevented him or her from obtaining coverage under a QHP.
State Exchanges may choose to process exemptions, or they may delegate exemption processing to HHS. Most State Exchanges currently delegate hardship exemption processing to HHS.[183]
HHS published guidance on September 4, 2025, that expanded eligibility for a hardship exemption to individuals ineligible for APTC or CSRs due to projected household income for consumers in FFE States, SBE-FP States, and State Exchange States that delegate their exemption processing to HHS.[184]
We stated in the proposed rule that the proposal to amend § 155.605(d)(1) would expand hardship exemption eligibility to consumers ineligible for APTC or CSRs due to projected household income in all States. We proposed to make this change to improve access to affordable coverage for consumers in all States as we believe there are a substantial number of consumers for whom purchasing a QHP relative to a catastrophic plan could cause a financial hardship. From the year before the Affordable Care Act's main regulations took effect in 2013 to 2026, average monthly premiums on the individual market jumped from $244 to $779—a 219 percent increase, with premiums increasing by 26 percent in 2026 alone.[185]
By comparison, inflation since 2013 increased by 39 percent and average hourly earnings for private sector employees increased by 53 percent.[186]
As these data show, premiums continue to outpace income growth, creating affordability challenges even for consumers who may not qualify for financial assistance. We stated in the proposed rule that we believe the substantial premium increases accumulated since 2013, and the recent spike in 2026, warrant a broad nationwide hardship exemption to allow individuals aged 30 and older to enroll in catastrophic coverage, if otherwise eligible under the proposed household income parameters. We proposed applying this exemption uniformly across all States to ensure consistent consumer protection and access to catastrophic coverage.
To avoid confusion for consumers, we stated in the proposed rule that States that currently process exemptions independently may implement the expanded criteria within their existing systems or delegate processing to HHS. We stated that this proposal does not preempt State authority under section 1321 of the Affordable Care Act, which provides States flexibility in the operation and enforcement of Exchanges and related requirements. States retain discretion to determine how to operationalize this policy—either by adopting the expanded criteria or continuing to delegate exemption processing to HHS. We also stated that we would provide technical assistance to support implementation and ensure that States can exercise this flexibility while maintaining consistent consumer protection nationwide.
We sought comment on the proposal to amend § 155.605(d)(1) to codify and expand hardship exemptions for individuals who are ineligible for APTC or CSR due to projected household income. If finalized as proposed, the expanded hardship exemption policy would take effect on the effective date of this final rule.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed expansion of Hardship Exemption eligibility below.
Comment:
A number of commenters stated support for the hardship exemption expansion, citing significant premium increases in recent years and the affordability challenges faced by consumers who do not qualify for APTC or CSR. Commenters noted that having some insurance coverage is better than being uninsured and recommended that CMS pair the expansion with robust consumer education and plan comparison tools to ensure consumers can make informed enrollment decisions.
Response:
We appreciate the support stated by these commenters and agree that expanding access to affordable coverage options is an important policy goal. Sustained, market-wide premium increases—219 percent cumulative increase from 2013 to 2026, including a 26 percent increase in 2026 alone,[5]
far outpacing inflation and wage growth over the same period—have created a structural barrier to obtaining coverage for individuals who are not eligible for APTC or CSR to offset those costs. The Secretary has determined that these circumstances constitute a qualifying hardship under section 5000A(e)(5) of the Code—a determination grounded in the documented, market-wide divergence between premium costs and income growth over the same period, which has impaired the capability of certain individuals to obtain coverage under a qualified health plan. For individuals with household income below 100 percent of the FPL or above 400 percent of the FPL who are ineligible for APTC, this premium growth represents a significant barrier to coverage because these individuals cannot reduce the cost of coverage through a premium subsidy, leaving them fully exposed to the cumulative premium increases documented above.[187]
Independent analyses confirm
( printed page 29635)
that this burden is particularly acute for older adults in this income range, who face the highest age-rated premiums in the individual market and, absent subsidy assistance, may spend a substantial share of their income on health insurance premiums.[188]
For individuals with projected annual household income between 250 percent and 400 percent of the FPL who are eligible for APTC but ineligible for CSR, the full cost-sharing burden of metal-level plans presents a distinct but related barrier to the capability to obtain coverage under a qualified health plan: while these individuals may reduce their premium through APTC, they remain ineligible for cost-sharing reductions (CSR), which substantially reduce deductibles, copayments, and out-of-pocket maximums for silver-level plan enrollees—in some cases increasing the effective actuarial value of a silver plan from 70 percent to as high as 94 percent. Without CSRs, these individuals face the full cost-sharing burden of metal-level plans, which may impair their ability to obtain coverage under a qualified health plan even where a premium subsidy is available. This final rule addresses those challenges by expanding hardship exemption eligibility consistent with the Secretary's authority under section 5000A(e)(5) of the Code and section 1302(e) of the Affordable Care Act.
Catastrophic plans are intended as a safety-net against total uninsurance—providing meaningful protection against devastating medical expenses and ensuring access to preventive care for consumers who would otherwise be uninsured. This final rule expands the range of coverage options available to consumers; it does not mandate enrollment in any particular plan type. Consumers may use the plan comparison tools and resources available on
HealthCare.gov
to evaluate all available options and select the plan that best meets their individual needs and circumstances. The available enrollment data support this conclusion: according to CMS' 2026 Marketplace Open Enrollment Period Public Use Files, of the 23.1 million consumers who selected health insurance coverage during the 2026 Open Enrollment Period—the first following the effective date of the September 2025 guidance expanding hardship exemption eligibility—only 67,489, or less than 0.3 percent, selected a catastrophic plan,[189]
demonstrating that consumers who can afford QHP coverage are, in practice, continuing to choose QHPs rather than catastrophic plans. We will continue to ensure that
HealthCare.gov
provides clear, accessible information about catastrophic plans, including what is and is not covered before the deductible is met, the absence of dental benefits, that APTC and PTC can only be applied to metal-level QHPs, and that consumers who qualify for the premium tax credit or cost-sharing reductions should compare Bronze and Silver plans, as those plans may be a better value.[190]
We acknowledge, however, that catastrophic plans have low monthly premiums and very high deductibles, and that they are intended as a safety-net against total uninsurance—not as a preferred coverage option for individuals with serious illness, complex conditions, or ongoing health care needs. Consumers with regular health care needs may face significant out-of-pocket costs before most benefits are covered, and individuals enrolled in catastrophic plans do not qualify for PTCs. This final rule expands consumer choice; it does not require any individual to enroll in a catastrophic plan, and it is not intended to steer consumers with significant health care needs away from comprehensive metal-level coverage.
Comment:
Several commenters stated that the proposed expansion of hardship exemption eligibility exceeds the Secretary's statutory authority and constitutes an unlawful attempt to circumvent the affordability exemption standard established by Congress. Commenters noted that Congress deliberately limited catastrophic plan eligibility to three groups, individuals under age 30, individuals who qualify for an affordability exemption under section 5000A(e)(1) of the Code, and individuals who qualify for a hardship exemption under section 5000A(e)(5), and that the proposed rule effectively rewrites these statutory eligibility criteria.
Commenters further noted that Congress constructed a narrow affordability exemption under section 5000A(e)(1) of the Code with specific income-based eligibility criteria and an indexing mechanism under section 5000A(e)(1)(D) that was specifically designed to account for the divergence between premium growth and income growth over time. Commenters stated that the existence of this indexing mechanism reflects a deliberate congressional judgment about how to address premium growth relative to income and that the Secretary cannot use the hardship exemption authority in section 5000A(e)(5) of the Code to create a broader, income-based pathway to catastrophic coverage that replaces or supersedes that statutory standard. In commenters' view, the proposed rule would make catastrophic plans available to approximately 80 percent of adults aged 18-64—including everyone with income below 100 percent of the FPL (approximately $15,650 for a single person) and everyone with income above 250 percent of the FPL (approximately $39,125 for a single person)—a population that commenters noted Congress never intended to have access to catastrophic coverage on a broad, categorical basis.
Commenters also noted that the hardship exemption is limited to individualized, circumstance-specific situations such as an unexpected increase in essential expenses, deprivation of food, shelter, or clothing, or other specific circumstances preventing an individual from obtaining QHP coverage and that the proposed rule adds an income-based exemption without a direct link to the capability to obtain QHP coverage. Some commenters noted that an individual with income above 250 percent of the FPL who could afford a QHP would nonetheless qualify for catastrophic coverage under the proposal, further undermining the connection to hardship. A few commenters requested CMS to withdraw the proposal entirely and to revoke the September 2025 sub-regulatory guidance that initially introduced the expanded eligibility.
Commenters further noted that Congress recently made catastrophic plans eligible to be paired with health savings accounts (HSAs) without amending the statutory eligibility criteria for catastrophic coverage, and that legislation that would have codified and expanded upon CMS' September 2025 guidance, the Health Care Freedom for Patients Act, was considered but not enacted by Congress in December 2025. Commenters stated that these legislative developments reflect a deliberate
( printed page 29636)
congressional judgment against expanding catastrophic plan eligibility in the manner proposed.
Response:
We have carefully considered the statutory authority concerns raised by commenters and provide the following explanation of the legal framework underlying this final rule.
Section 1302(e)(2)(B) of the Affordable Care Act establishes two independent, coordinate pathways to catastrophic plan eligibility based on exemption status: eligibility under section 5000A(e)(1) of the Code (relating to individuals for whom coverage is unaffordable) and eligibility under section 5000A(e)(5) of the Code (relating to individuals who have suffered a hardship for the capability to obtain QHP coverage). The statute does not establish a hierarchy between these two pathways, nor does it provide that the hardship pathway is constrained by the criteria Congress established for the separate affordability exemption. This final rule exercises the Secretary's authority under section 5000A(e)(5) of the Code, a distinct statutory provision, and does not modify, replace, or supersede the affordability exemption standard under section 5000A(e)(1) of the Code.
Section 5000A(e)(5) of the Code grants the Secretary of HHS authority to determine whether an individual has “suffered a hardship for the capability to obtain coverage under a qualified health plan.” This provision grants the Secretary discretion to define the circumstances that constitute a qualifying hardship. The statute does not enumerate or limit those circumstances, nor does it require that the hardship exemption be unavailable to individuals who also fail to qualify for the affordability exemption.
We acknowledge that Congress established specific criteria for the affordability exemption under section 5000A(e)(1) of the Code, including an indexing mechanism under section 5000A(e)(1)(D) to account for premium growth relative to income growth. The existence of that indexing mechanism reflects Congress' approach to the affordability exemption; it does not, however, limit the Secretary's separate authority under section 5000A(e)(5) of the Code to recognize that the cumulative divergence between premium growth and income growth—a 219 percent increase in average monthly premiums from 2013 to 2026, including a 26 percent increase in 2026 alone, far outpacing inflation (39 percent) and wage growth (53 percent) over the same period [191]
—constitutes a hardship for the capability to obtain QHP coverage for a broad population of consumers. The affordability exemption under section 5000A(e)(1) of the Code does not fully account for this hardship for the population addressed by this rule, as described below for each income group. For individuals with a projected household income below 100 percent of the FPL, the hardship exemption under section 5000A(e)(5) of the Code provides an independent and appropriate pathway to relief that operates separately from the affordability exemption calculation. These individuals are generally ineligible for APTC because they are assumed to be eligible for Medicaid—but not all individuals with household income below 100 percent of the FPL are eligible for or enrolled in Medicaid. Certain individuals may be ineligible for Medicaid due to immigration status, categorical eligibility requirements, value of property they own, or other factors, meaning the assumption of Medicaid eligibility that underlies APTC ineligibility based on income does not reflect their actual access to coverage. For these individuals, the hardship exemption under section 5000A(e)(5) addresses a distinct structural barrier—the gap between assumed and actual coverage access—that the affordability exemption framework does not resolve.
For individuals with household income above 400 percent of the FPL who are ineligible for APTC, the full unsubsidized premium cost—which has increased 219 percent since 2013—may or may not exceed the affordability exemption threshold depending on their specific income level, but the hardship exemption under section 5000A(e)(5) provides an independent and appropriate pathway to relief for this population through two pathways.[192]
Under the first pathway, individuals who apply for coverage through the Exchange and attest to a projected household income above 400 percent of the FPL—rendering them ineligible for APTC—will have the hardship exemption automatically adjudicated based on the income information provided in their coverage application. Under the second pathway, individuals may apply directly for the hardship exemption by completing the paper exemption request form [193]
and attesting that they cannot afford coverage because they are no longer eligible for financial assistance; income documentation is not required under this pathway. Both pathways are consistent with the attestation-based framework governing hardship exemption eligibility under § 155.605(d)(1)(iii), eligibility is based on the individual's attested projected household income; no documentation of hardship circumstances is required.
For individuals with projected annual household income between 250 percent and 400 percent of the FPL who are eligible for APTC but ineligible for CSR, the hardship determination rests on a distinct but related basis. While these individuals may reduce their monthly premium through APTC, they remain ineligible for cost-sharing reductions (CSR), which are available only to individuals with household income at or below 250 percent of the FPL enrolled in silver-level plans. CSRs substantially reduce deductibles, copayments, and out-of-pocket maximums—in some cases increasing the effective actuarial value of a silver plan from 70 percent to as high as 94 percent. Without CSRs, individuals in this income range face the full cost-sharing burden of metal-level plans, which may render coverage financially inaccessible as a practical matter even where a premium subsidy is available.
The two exemption pathways address overlapping but distinct circumstances and operate independently of one another. Both pathways respond to the same underlying market condition—sustained, market-wide premium increases that have outpaced inflation and wage growth, creating barriers to obtaining coverage under a QHP. They are distinct, however, in the circumstances each addresses: the affordability exemption under section 5000A(e)(1) of the Code applies a specific, formulaic calculation based on whether the cost of the lowest-cost bronze plan, reduced by any available APTC, exceeds the applicable percentage of household income; the hardship exemption under section 5000A(e)(5) of the Code addresses structural barriers to the capability to obtain coverage that fall outside that formula—including APTC ineligibility due to assumed Medicaid eligibility that does not reflect actual coverage access, the full cost-sharing burden faced by individuals between 250 percent and 400 percent of the FPL who are
( printed page 29637)
ineligible for CSR, and the impact of non-discretionary expenses on the income available for premiums and cost-sharing for individuals above 400 percent of the FPL. The indexing mechanism in section 5000A(e)(1)(D) governs the affordability exemption; it does not constrain the Secretary's independent authority under section 5000A(e)(5) of the Code to respond to the same underlying market conditions through the hardship pathway.
For the characterization of the hardship exemption as limited to individualized, event-specific circumstances, we note that the existing regulatory framework does not support that reading. The hardship exemption eligibility standards at § 155.605(d) were originally established in the 2013 final rule.[194]
That rule established, among other things, a broad “other circumstances” category at § 155.605(d)(1)(iii) under which the Exchange must grant a hardship exemption to an individual who “has experienced other circumstances that prevented him or her from obtaining coverage under a qualified health plan.” The original preamble to § 155.605 explicitly noted that the hardship exemption was drafted with “broad language to include a range of personal scenarios” and that we expected to “clarify these criteria in future guidance,” [195]
reflecting the Secretary's longstanding exercise of discretion to define and expand hardship criteria over time.
Moreover, the use of income-based, categorical criteria in the hardship exemption is not a new development. The Medicaid non-expansion exemption at § 155.605(d)(3) provides a particularly instructive precedent. That exemption was established to address the hardship faced by individuals who were ineligible for Medicaid solely because their State chose not to expand Medicaid eligibility under the Affordable Care Act. As we noted in the 2013 final rule, the Secretary determined that it was appropriate for individuals to be eligible for this hardship exemption even if they remained technically eligible for APTC, recognizing that technical eligibility for a subsidy does not, by itself, ensure that coverage is meaningfully accessible or affordable.[196]
This precedent is directly applicable to individuals between 250 percent and 400 percent of the FPL who are eligible for APTC but ineligible for CSR—for whom the absence of cost-sharing reductions may render coverage financially inaccessible as a practical matter even where a premium subsidy is available. For individuals above 400 percent of the FPL who are ineligible for APTC, the hardship determination is grounded in the individual's attested income or hardship situation, depending on the exemption request pathway (automated or paper form) used. As described previously, the two pathways are consistent with the attestation-based framework governing hardship exemption eligibility under § 155.605(d)(1)(iii) to ensure that the exemption is grounded in an affirmative attestation by the individual, whether of income or of hardship circumstance. The threshold of 400 percent of the FPL is not a fixed measure of financial capacity: the income available for health insurance premiums and cost sharing is further reduced by other essential, non-discretionary expenses—including housing, childcare, eldercare, and other obligations—that are not accounted for in the affordability exemption calculation under section 5000A(e)(1) of the Code. For individuals in this income range for whom those circumstances, combined with the documented, sustained divergence between premium costs and income growth—a 219 percent cumulative increase in average monthly premiums from 2013 to 2026,[197]
far outpacing inflation and wage growth over the same period—have impaired the capability to obtain coverage under a qualified health plan, the hardship exemption under section 5000A(e)(5) provides an appropriate and independent pathway to relief. As described previously, neither the automatic determination nor the paper exemption request form pathways require documentation, and both ensure that the exemption is grounded in an affirmative attestation by the individual—whether of income or of hardship circumstance—consistent with the attestation-based framework governing hardship exemption eligibility under § 155.605(d)(1)(iii).
We further operationalized the Medicaid non-expansion exemption through sub-regulatory guidance issued on November 21, 2014, which established that an individual residing in a State that did not expand Medicaid coverage with household income below 138 percent of the FPL was eligible to claim a hardship exemption—a categorical, income-based determination made without requiring individualized proof of circumstance-specific hardship.[198]
The 2016 final rule further streamlined the Medicaid non-expansion exemption by eliminating the requirement for a denial notice for applicants ineligible for Medicaid because their State did not expand Medicaid coverage, reflecting our ongoing exercise of administrative discretion to reduce barriers to exemption access for populations facing systemic coverage gaps.[199]
While regulatory precedent is not itself dispositive of statutory authority, the Medicaid non-expansion exemption is instructive as evidence of the Secretary's longstanding, consistent, and unchallenged exercise of the same authority under section 5000A(e)(5) of the Code in a comparable context. That precedent supports the following features of the current proposal as applied to individuals between 250 percent and 400 percent of the FPL who are eligible for APTC but ineligible for CSR: (1) the use of categorical, income-based criteria to define a qualifying hardship; (2) the availability of a hardship exemption to individuals who retain some technical access to subsidized coverage; and (3) the Secretary's authority to recognize systemic, structural barriers to coverage—not merely individualized, event-specific circumstances—as qualifying hardships under section 5000A(e)(5). The expansion codified in this final rule is consistent with and builds upon that established regulatory history.
For individuals with projected annual household income above 400 percent of the FPL who are ineligible for APTC, the hardship determination rests on independent grounds, as described above: the 400 percent FPL threshold is not a uniform measure of financial capacity—the income available for health insurance premiums and cost sharing is further reduced by other
( printed page 29638)
essential, non-discretionary expenses not accounted for in the affordability exemption calculation under section 5000A(e)(1) of the Code. For individuals in this income range for whom those circumstances, combined with the sustained, market-wide premium increases documented above, have impaired the capability to obtain coverage under a qualified health plan, the hardship exemption under section 5000A(e)(5) provides an appropriate and independent pathway to relief. As mentioned previously, the automated and paper form pathways are grounded in the attestation-based framework governing hardship exemption eligibility under § 155.605(d)(1)(iii). For the statement that an individual with an income above 250 percent of the FPL who could afford a non-catastrophic QHP would nonetheless qualify for catastrophic coverage under the proposal, we note that this concern does not accurately reflect the purpose or practical effect of this policy. This rule is designed to expand coverage options for consumers who face structural barriers to affordable coverage—not to redirect consumers away from non-catastrophic QHPs. Consumers who can afford and prefer a non-catastrophic QHP remain free to enroll in one; this rule does not alter that choice. The hardship exemption expands the range of options available to consumers, consistent with the Secretary's authority under section 5000A(e)(5) to define qualifying hardship circumstances.
We note that the hardship exemption expansion does not create a new entitlement or mandate enrollment in catastrophic coverage—it expands the range of options available to consumers who face structural barriers to obtaining coverage under a qualified health plan. The policy's purpose is to ensure that consumers who cannot meaningfully access metal-level coverage have a pathway to some coverage, consistent with the Secretary's authority under section 5000A(e)(5) of the Code.
For individuals between 250 percent and 400 percent of the FPL who remain eligible for APTC, we note that, for individuals who are ineligible for CSR, APTC eligibility alone does not ensure that coverage is meaningfully affordable or adequate. Individuals in this income range are not eligible for CSR, which are available only to individuals with household income at or below 250 percent of the FPL enrolled in silver-level plans. CSRs substantially reduce deductibles, copayments, and out-of-pocket maximums—in some cases increasing the effective actuarial value of a silver plan from 70 percent to as high as 94 percent.[200]
Without CSRs, individuals between 250 percent and 400 percent of the FPL face the full cost-sharing burden of metal-level plans, which may render those plans financially inaccessible as a practical matter even where APTC is available. As we recognized in the context of the Medicaid non-expansion exemption—where some individuals technically eligible for APTC were nonetheless deemed to face a qualifying hardship—the Secretary's determination that a population faces a qualifying hardship is grounded in the practical and financial realities of coverage access, not merely in technical subsidy eligibility.
For the request to revoke the September 4, 2025, sub-regulatory guidance, we decline to do so. That guidance was issued under the Secretary's authority under section 5000A(e)(5) and section 1311(d)(4)(H) of the Affordable Care Act,[201]
and this final rule codifies and extends that guidance consistent with the same legal authority.
For the statement that Congress' decision not to enact the Health Care Freedom for Patients Act, or its decision not to amend the statutory eligibility criteria when making catastrophic plans eligible to be paired with HSAs, reflects a congressional judgment against expanding catastrophic plan eligibility, we note that the failure of legislation to pass does not, as a general matter, constitute a prohibition on agency action within existing statutory authority.[202]
The Secretary's authority under section 5000A(e)(5) exists independently of any subsequent legislative proposals. This final rule is grounded in the text, structure, and purpose of both section 1302(e) of the Affordable Care Act and section 5000A(e)(5) of the Code, and we are finalizing this provision accordingly.
Comment:
Several commenters expressed concern that expanding hardship exemption eligibility would destabilize the individual market risk pool. Because catastrophic plans are included in a separate risk pool from metal-level plans under the HHS-operated risk adjustment program, commenters stated that drawing healthier enrollees into catastrophic coverage could increase premiums for those remaining in metal-level plans. Commenters specifically characterized this dynamic as drawing consumers from “high-actuarial value (AV) plans to low-value plans,” weakening the broader Exchanges. Commenters further stated that CMS is effectively creating a parallel catastrophic insurance market that would compete with metal-level Exchange plans, an outcome they contended is contrary to the Affordable Care Act's design and structure. Commenters requested that CMS evaluate how the expanded eligibility interacts with the methodology of the HHS-operated risk adjustment program to ensure that risk adjustment transfers accurately reflect the relative health risk of enrollees across plan types and support market stability, including by pooling catastrophic and non-catastrophic plan risk calculations under the State payment transfer formula to create a larger, more resilient risk pool.
Commenters also noted concerns about the interaction between the hardship exemption eligibility expansion and other proposed changes to catastrophic coverage, including the proposed allowance of multi-year catastrophic plan terms at §§ 156.130(c) and 156.155(a)(6) and proposed cost-sharing modifications at § 156.155(a)(3). Commenters stated that the cumulative effect of these changes could accelerate adverse selection dynamics, drawing younger and healthier consumers away from comprehensive metal-level plans and raising premiums for those who remain in those plans. Community health advocates warned of a “dual harm” scenario in which patients enrolled in catastrophic plans delay or avoid needed care due to high-deductible barriers—undermining continuity of care and worsening health outcomes—while community health centers simultaneously experience revenue loss and increased uncompensated care burden. At least one commenter stated that the proposal is counter to sound public policy and should be withdrawn. Commenters also requested that CMS conduct and publish an actuarial analysis quantifying the projected impact on Exchange risk pools, premiums, and Federal subsidy costs before implementation.
Response:
We have carefully considered the risk pool concerns raised by commenters. We acknowledge that catastrophic plans are included in the
( printed page 29639)
single risk pool for the individual market; however, catastrophic plans are subject to separate risk adjustment calculations under the HHS-operated risk adjustment program. Because catastrophic plans are subject to separate risk adjustment calculations, catastrophic plans that enroll lower-risk individuals than metal-level plans do not compensate metal-level plans for enrolling higher-risk individuals through risk adjustment transfers. We acknowledge that this dynamic, and changes in enrollment patterns more broadly, may affect the composition of the individual market risk pool. However, these concerns do not outweigh the significant and well-documented barriers the Secretary has determined have prevented a broad population of consumers from obtaining coverage under a QHP, constituting a qualifying hardship under section 5000A(e)(5). As described previously in this final rule, the Secretary has determined that the income-group-specific circumstances faced by each of these populations—including sustained, market-wide premium increases and, for individuals between 250 percent and 400 percent of the FPL, the full cost-sharing burden of metal-level plans in the absence of CSR—constitute a qualifying hardship with respect to the capability to obtain QHP coverage under section 5000A(e)(5).[203]
For the characterization of this policy as creating a “parallel insurance market” that competes with metal-level Exchange plans, we note that catastrophic plans have always been available through the Exchanges alongside metal-level plans for eligible consumers and all plans—including catastrophic plans—remain subject to the same QHP certification requirements, consumer protection standards, and essential health benefit requirements that apply to all Exchange plans.[204]
We acknowledge, however, that expanding the population eligible for catastrophic coverage has the potential to affect the composition of the individual market risk pool, and we do not minimize that concern.
We have considered the request to combine risk adjustment transfer calculations for catastrophic and non-catastrophic plans under the State payment transfer formula. We are not combining these calculations in this final rule. As discussed in section III.E.6 of this final rule (§ 156.155(a)(6)), we believe the existing HHS risk adjustment methodology is flexible enough to appropriately accommodate catastrophic plans—including multi-year catastrophic plans—without changes to the HHS risk adjustment models or State payment transfer formula. Risk adjustment transfers for catastrophic plans will continue to be calculated separately from metal-level plans on a plan year basis, consistent with current practice. This applies equally to multi-year catastrophic plans, for which risk adjustment transfers will continue to be calculated on a plan year basis, as described in section III.E.6 of this final rule.
We acknowledge that if catastrophic plan enrollment grows substantially, maintaining separate risk adjustment calculations for catastrophic and non-catastrophic plans could have a more pronounced effect on premiums for metal-level plans. The available enrollment data from the first Open Enrollment Period following the effective date of the September 2025 guidance—during which only 67,489 consumers, or less than 0.3 percent of the 23.1 million total plan selections, selected a catastrophic plan—demonstrates that the actual impact on the metal-level risk pool has been minimal to date. This minimal uptake is consistent with the risk pool assumptions underlying 2027 rate submissions and demonstrates that consumers who can afford and prefer metal-level coverage are, in practice, continuing to choose metal-level plans. We will monitor catastrophic plan enrollment, and risk profile, and will consider whether changes to the HHS risk adjustment methodology—including whether to combine catastrophic and non-catastrophic risk adjustment calculations—are warranted through future notice-and-comment rulemaking.
For the “dual harm” concern raised by community health advocates—that patients enrolled in catastrophic plans may delay or avoid needed care due to high-deductible barriers, while community health centers simultaneously experience revenue loss and increased uncompensated care burden—we note that this concern applies broadly to high-deductible coverage and is not unique to the expanded hardship exemption. Catastrophic plans have always been available to eligible consumers, and the expanded eligibility does not alter the cost-sharing structure of those plans. Moreover, by reducing the number of uninsured, we expect that broadening access to catastrophic coverage will improve revenues and reduce uncompensated care burdens for community health centers. We note that the hardship exemption expansion benefits consumers broadly—it is not targeted at or limited to any particular geographic community or health center service area, and the policy's consumer protection benefits accrue to individuals regardless of where they receive care. As discussed in section III.E.7. of this final rule, to the extent permitted by applicable Federal and State law, issuers of catastrophic plans may offer arrangements designed to reduce the up-front financial barrier associated with high deductibles. Such arrangements could be designed to reduce the up-front financial barrier that can lead to delayed or avoided care.
For the request to withdraw the proposal, we decline to do so for the reasons set forth throughout this final rule.
For the request that CMS conduct and publish an actuarial analysis quantifying the projected impact on Exchange risk pools, premiums, and Federal subsidy costs before implementation of this policy, we note that we will continue to monitor market conditions and enrollment trends and will transparently report on these impacts as data from PY 2026 becomes available.
We note that the hardship exemption guidance underlying this codification was issued on September 4, 2025—sufficiently in advance of PY 2027 rate filing cycle—and that the streamlined online application process launched November 1, 2025, the start of the 2026 Open Enrollment period.[205]
Issuers therefore had the opportunity to account for the expanded eligibility in their 2027 rate submissions. The September 4, 2025 guidance was in effect beginning November 1, 2025—the start of the 2026 Open Enrollment Period—and issuers filing 2027 rates during the standard rate review period were able to draw on actual 2026 enrollment experience under the expanded eligibility when developing their 2027 rate submissions.[206]
We do not anticipate that this particular provision will materially disrupt 2027 rate filings because issuers had both advance notice of the expanded eligibility and the
( printed page 29640)
opportunity to observe actual enrollment behavior under the expanded criteria prior to submitting their 2027 rates. As noted above, the 2026 Open Enrollment Period data confirms that catastrophic plan uptake under the expanded eligibility was minimal [207]
—consistent with the risk pool assumptions underlying 2027 rate submissions.
This rule expands the criteria under which individuals may qualify for a hardship exemption under § 155.605(d)(1); it does not alter the rules governing the exemption itself, including the annual nature of exemption eligibility. Concerns about catastrophic plan design—including risk adjustment methodology, multi-year plan terms (including the eligibility carry-through question for individuals who qualify based on a hardship exemption at initial enrollment in a multi-year term), and cost-sharing parameters—are addressed in sections III.E.2 (§ 156.80(d)(2)(ii)), III.E.6. (§ 156.155(a)(6)), and III.E.7. (§ 156.155(a)(3)) of this final rule.
Consumers retain full freedom of choice in the Exchanges. Individuals who qualify for this hardship exemption are not required to enroll in catastrophic coverage—they may continue to shop for and enroll in any available metal-level plan, if eligible. We will continue to monitor market conditions, enrollment trends, and the impact of the expanded eligibility on metal-tier risk pools, premiums, and serious-illness populations, and will transparently report on these impacts as data from PY 2026 becomes available. We are committed to considering corrective regulatory action in future rulemaking if monitoring data reveals material harm to the risk pool or to consumers with serious illness or complex health care needs. Concerns about multi-year catastrophic plan protections—including right to transition to other coverage, such as a metal-level plan, during a special enrollment period triggered by a qualifying life event and pre-enrollment counseling for high-risk applicants—are addressed in section III.E.6. of this final rule.
Comment:
Commenters stated concern that expanding access to catastrophic plans through the hardship exemption would expose consumers—particularly those with chronic conditions, complex health needs, or limited financial resources—to unaffordable out-of-pocket costs. Commenters noted that catastrophic plans do not cover services other than preventive services and three primary care visits until an enrollee reaches the annual maximum out-of-pocket limit, and that most care would not be covered until an individual spends $15,600 (individual) or $31,200 (family) in a single year. Some commenters characterized catastrophic plans as “junk” coverage that shifts the entire burden of health care risk onto the individual and urged CMS to focus on lowering out-of-pocket costs rather than expanding access to plans with limited pre-deductible coverage.
Commenters also raised concern that consumers eligible for APTC could be targeted by aggressive marketing and induced to enroll in catastrophic coverage based on lower premiums, without fully understanding the coverage limitations. Commenters emphasized that APTC-eligible consumers should not be encouraged to forgo tax credits in favor of catastrophic plans that offer less comprehensive coverage and higher cost-sharing exposure. The underinsurance risk was also highlighted: while catastrophic plans offer protection against major medical events for individuals with low-to-no-health care needs, consumers with routine or ongoing health care needs may face thousands of dollars in out-of-pocket costs before any meaningful coverage applies.
One commenter noted that catastrophic plans generally do not include dental benefits, and that consumers—especially those with limited financial flexibility—may not realize they need to purchase a separate SADP to maintain access to oral health services.[208]
Additional commenters raised concerns about the disproportionate impact of high-deductible catastrophic plans on individuals with complex or chronic conditions and about consumers who may not fully understand the limitations of catastrophic coverage at the time of enrollment.
Response:
We acknowledge these concerns and recognize that catastrophic plans are not the right fit for every consumer. This final rule expands consumer choice—it does not require any individual to enroll in a catastrophic plan and it does not create disparate advantage for catastrophic plans over metal level plans in any way.
Catastrophic plans cover the same 10 EHBs as other Exchange plans, including preventive services at no cost, and cover at least three primary care visits per year before the deductible is met.[209]
These plans are specifically designed to provide financial protection against worst-case scenarios, such as serious illness or injury that could result in devastating medical expenses. For consumers who are currently uninsured because they cannot afford a metal-level plan, access to catastrophic coverage could provide meaningful protection and ensure access to preventive care.
We acknowledge, however, that catastrophic plans have low monthly premiums and very high deductibles, and that they are intended as a safety-net against total uninsurance—not as a preferred coverage option for individuals with serious illness, complex conditions, or ongoing health care needs. Consumers who are concerned about exposure to high deductibles may also wish to explore additional coverage options, such as supplemental insurance products for hospital indemnity, critical illness, or accidents
—
that may help offset deductible costs, which in some circumstances may be a preferred complement or alternative to a higher-premium metal-level plan. Consumers should carefully evaluate the terms, limitations, and costs of any supplemental product before purchasing. Consumers with regular health care needs may face significant out-of-pocket costs before most benefits are covered, and individuals enrolled in catastrophic plans do not qualify for PTC. This final rule expands consumer choice; it does not require any individual to enroll in a catastrophic plan, and it is not intended to steer consumers with significant health care needs away from comprehensive metal-level coverage. As
HealthCare.gov
advises, consumers who qualify for PTC or CSR should compare bronze and silver plans, as those plans may be a better value.
Consumers will have full visibility into their APTC and CSR eligibility upon completing their Exchange application. The plan shopping experience on
HealthCare.gov
is designed to present consumers with personalized eligibility information and plan comparison tools that clearly display premiums after tax credits, cost-sharing obligations, and coverage differences across all available plan
( printed page 29641)
types.[210]
Consumers who are eligible for APTC will be able to see the net premium cost of metal-level plans after applying their tax credits, enabling a fully informed comparison before selecting a catastrophic plan. We will continue to enforce applicable marketing standards and nondiscrimination requirements to ensure that issuers, agents, and brokers present catastrophic plan options accurately and do not steer consumers toward or away from particular plan types based on health status or other protected characteristics.[211]
Consumers who are eligible for APTC should be made aware that those credits can only be applied to metal-level QHPs—not to catastrophic plans—and that forgoing APTC in favor of a lower-premium catastrophic plan may result in significantly higher total health care costs, particularly for individuals with ongoing health care needs. We will continue to ensure that
HealthCare.gov
provides clear, accessible information about catastrophic plans—including that APTC can only be applied to metal-level QHPs and that forgoing APTC in favor of a catastrophic plan may result in higher total health care costs—so that consumers can make fully informed coverage decisions.
For the dental coverage gap, catastrophic plans do not include dental benefits, and consumers enrolling in catastrophic coverage who wish to maintain access to dental services should consider purchasing a separate SADP. We will ensure that consumer education resources clearly communicate this limitation.[212]
We are expanding the criteria under which individuals may qualify for a hardship exemption under § 155.605(d)(1); it does not alter the exemption redetermination process or the rules governing catastrophic plan design. Concerns about the catastrophic plan design—including cost-sharing modifications, multi-year catastrophic plan terms, plan-level adjustments, and risk adjustment methodology—are addressed in sections III.E.7. (§ 156.155(a)(3)), III.E.6. (§ 156.155(a)(6)), and III.E.2. (§ 156.80(d)(2)(ii)) of this final rule. The available enrollment data, as discussed previously, demonstrate that consumer uptake of catastrophic coverage under the expanded eligibility has been minimal, which is consistent with the risk pool assumptions underlying those provisions.
Comment:
Commenters raised concerns about the proposal's interaction with State-level individual mandate laws and State-run hardship exemption processing systems. Some commenters stated appreciation for HHS' recognition that States are in the best position to regulate their individual insurance markets and for allowing each State to determine what products are sold, while raising concerns about the practical implications of the Federal expansion of eligibility for catastrophic coverage for States with their own mandates and exemption frameworks. Commenters requested that States that enforce their own individual mandates or process their own hardship exemptions retain sole discretion to determine the scope of their hardship exemptions, and that CMS exempt such States from any requirement to broaden hardship exemption eligibility for catastrophic coverage.
One State Exchange reported that no carriers currently offer catastrophic plans through its platform, representing a complete on-exchange market withdrawal by carriers that had sold these plans in 2025. The Exchange noted that this market exit coincided with the expansion of hardship exemption eligibility guidance released by HHS in September 2025, and that carriers indicated these plans were financially unsustainable under the expanded eligibility framework. The State Exchange stated that it will be able to resume offering catastrophic plans if any carriers choose to do so in the future, and that it and the State insurance regulator intend to proactively seek information from carriers to determine whether future plan designs or revised market conditions may alter their interest in offering catastrophic plans. The State Exchange also noted that the proposed multi-year catastrophic plan structure would present significant implementation and technical challenges.
Other commenters noted concerns about the operational challenges created by the rulemaking timeline relative to State rate filing deadlines. A few commenters requested CMS to delay the implementation date to PY 2028 or later, arguing that by the time the final rule is published, it will be too late for carriers to update rates for PY 2027. Additional commenters noted broader State authority and preemption concerns and noted that the 30-day comment period was insufficient for a proposed rule of this scope and complexity.
Response:
We acknowledge the important role that States play in operating and enforcing their Exchanges and related requirements. This final rule does not preempt State authority under section 1321 of the Affordable Care Act, which provides States flexibility in the operation and enforcement of Exchanges and related requirements.[213]
States retain discretion to determine how to operationalize this policy within their existing systems.
For States that enforce their own individual mandates or process their own hardship exemptions, this final rule establishes a Federal floor for hardship exemption eligibility that applies to consumers in all States. States that independently process exemptions may implement the expanded criteria within their existing systems. States that prefer to delegate exemption processing to HHS may do so. We will provide technical assistance to support implementation and ensure that States can exercise this flexibility while maintaining consistent consumer protections nationwide. Unlike regulatory actions that reduce coverage and predictably increase uncompensated care burdens, this rule expands coverage options for individuals who would otherwise be uninsured, reducing—not increasing—the fiscal burden on safety-net providers. Any claim that this rule harms community health centers would require speculation about individual consumer choices that are not traceable to this rulemaking.
For the request that States that enforce their own individual mandates or process their own hardship exemptions retain sole discretion to determine the scope of their hardship exemptions and be exempted from any requirement to broaden hardship exemption eligibility for catastrophic coverage, we decline to adopt this approach. We believe it is an important policy that all consumers—regardless of the State in which they reside—have access to the hardship exemption eligibility criteria established under Federal law, including the expanded criteria codified in this final rule. Consistent with the structure of the Exchange program, this final rule establishes a Federal floor for hardship exemption eligibility. States that independently process exemptions may implement the expanded criteria within their existing systems; States that prefer to delegate exemption processing to HHS may do so. We do not believe it would be appropriate to allow States to
( printed page 29642)
narrow the scope of Federal hardship exemption eligibility for their residents, as doing so would create inconsistent consumer protections across States and undermine the uniform access to catastrophic coverage that this rule is designed to provide. Section 1321 of the Affordable Care Act provides States flexibility in the operation of their Exchanges, but we do not believe that flexibility extends to narrowing the eligibility criteria for catastrophic coverage under section 1302(e) of the Affordable Care Act or exempting residents from the hardship exemption standards established under section 5000A(e)(5) of the Code.
States that have enacted their own individual mandate laws retain sole discretion to determine the scope of hardship exemptions for purposes of their own State mandate penalties—but that discretion is separate from, and does not affect, the hardship exemption criteria under section 5000A(e)(5) of the Code and section 1302(e) of the Affordable Care Act that govern eligibility for catastrophic coverage.
We acknowledge the report that no carriers currently offer catastrophic plans through one State Exchange and that the on-exchange market withdrawal coincided with the September 2025 guidance. Carrier participation decisions are made independently by issuers based on their own actuarial and business assessments, and the availability of catastrophic plans on any given Exchange is subject to issuer participation choices that are outside our direct control. We will monitor carrier participation trends in catastrophic plan markets and will consider whether additional regulatory or sub-regulatory action is warranted to support issuer participation and market stability.
For the implementation timeline and rate filing deadline concerns, we note that the expanded hardship exemption guidance underlying this codification was issued on September 4, 2025—well in advance of the PY 2027 rate filing cycle—and that the streamlined online application process launched November 1, 2025.[214]
Issuers therefore have the opportunity to account for the expanded eligibility in their PY 2027 rate submissions. Because this final rule codifies guidance that has been in effect since November 1, 2025—the start of the 2026 Open Enrollment Period—issuers filing 2027 rates during the standard rate review period were able to draw on actual 2026 enrollment experience under the expanded eligibility when developing their rate submissions.[215]
The 2026 enrollment data demonstrate that catastrophic plan uptake under the expanded eligibility was increased but overall still a small part of the overall market, with only 67,489 consumers selecting a catastrophic plan out of 23.1 million total plan selections,[216]
which is consistent with the risk pool assumptions underlying 2027 rate submissions. We therefore do not anticipate that codification of this guidance will materially disrupt PY 2027 rate filings for this provision specifically. We acknowledge that other novel catastrophic plan proposals finalized in this rule—including multi-year plan terms and cost-sharing modifications—present more complex pricing considerations, which are addressed in the relevant sections of this final rule.
We acknowledge that the interaction between this provision and other proposed changes to catastrophic coverage may present additional actuarial complexity for issuers; those interactions are addressed in the relevant sections of this final rule. We will work with States and issuers to facilitate timely and effective implementation and will provide additional operational guidance as needed.
For the comment period length, we note that the proposed rule was published in the
Federal Register
on February 11, 2026, with a comment period consistent with applicable APA requirements.[217]
We carefully considered all comments received and have addressed the substantive concerns raised in this final rule.
Comment:
Commenters stated that the hardship exemption expansion is premature and that CMS lacks sufficient data to evaluate its impact before codifying and further expanding the policy. Commenters noted that the expanded hardship exemption has been in effect for only one enrollment period—since September 2025—and that issuers need additional enrollment experience to develop actuarially sound pricing for catastrophic plans. Commenters requested CMS not to build additional policy structures on top of an exemption whose scope and market impact remain untested and recommended that CMS conduct and publish an actuarial analysis quantifying the projected impact on Exchange risk pools, premiums, and Federal subsidy costs before implementation. Commenters also requested gathering additional data and interested parties' feedback before finalizing the interaction between the expanded hardship exemption and other proposed changes to catastrophic coverage, including multi-year plan terms and cost-sharing modifications.
Response:
We acknowledge that the expanded hardship exemption, first established through HHS guidance issued on September 4, 2025, has been in effect for a limited period and that complete enrollment data for PY 2026 is not yet available. The underlying hardship challenge driving this policy, however, is well-documented and does not require additional enrollment data to justify action. Sustained, market-wide premium increases—a 219 percent cumulative increase from 2013 to 2026, including a 26 percent increase in 2026 alone, far outpacing inflation (39 percent) and wage growth (53 percent) over the same period,—have created a structural barrier to obtaining coverage for individuals who cannot access APTC or CSRs to offset those costs. For individuals with household income below 100 percent of the FPL or above 400 percent of the FPL who are ineligible for APTC, this premium growth represents a direct and unmitigated barrier to coverage. For individuals between 250 percent and 400 percent of the FPL who are eligible for APTC but ineligible for CSR, the full cost-sharing burden of metal-level plans represent a distinct but related barrier to the capability to obtain coverage under a qualified health plan. While these individuals may reduce their premium through APTC, they remain ineligible for cost-sharing reductions (CSR), which substantially reduce deductibles, copayments, and out-of-pocket maximums for silver-level plan enrollees—in some cases increasing the effective actuarial value of a silver plan from 70 percent to as high as 94 percent. Without CSRs, these individuals face the full cost-sharing burden of metal-level plans, which may render coverage financially inaccessible as a practical matter even where a premium subsidy is available. The Secretary has determined that these circumstances constitute a qualifying hardship for the capability to obtain coverage under section 5000A(e)(5) of the Code—a
( printed page 29643)
determination grounded in the documented, market-wide divergence between premium costs and the financial resources available to this population.
We acknowledge that commenters have raised a policy concern—not a statutory one—about whether we should gather additional enrollment data before codifying and expanding the hardship exemption. We decline to delay finalizing this policy for that purpose for the following reasons. First, the underlying hardship driving this policy is well-documented through existing market data, including the sustained, market-wide premium increases described above, and does not require enrollment data from the expanded eligibility period to establish a sufficient evidentiary basis for action. Second, the September 4, 2025, guidance has been in effect since November 1, 2025, and delaying codification would create regulatory uncertainty for consumers and issuers who have been operating under the expanded eligibility for the duration of the 2026 Open Enrollment Period. Third, the enrollment data that is available—including the 2026 Open Enrollment Period data discussed above—demonstrates that the policy has had minimal market impact, which is consistent with the risk pool assumptions underlying this rule. Finally, we are committed to ongoing monitoring of enrollment trends and market conditions and will consider corrective regulatory action in future rulemaking if monitoring data reveals material harm. This monitoring commitment is the appropriate mechanism for addressing data gaps—not delaying a rule that addresses a present and ongoing hardship.
As previously discussed, the population facing these the income specific circumstances constitute a qualifying hardship with respect to the capability to obtain coverage under section 5000A(e)(5) of the Code and warrant a timely policy response. We will continue to monitor enrollment trends and market conditions as data from PY 2026 becomes available and will transparently report on the impact of the expanded eligibility on risk pools, premiums, and the health care needs of enrollees in catastrophic plans, to the extent such data is available through existing CMS data systems and reporting mechanisms. We are committed to considering corrective regulatory action in future rulemaking if monitoring data reveals material harm. Concerns about actuarial pricing, product design, and the interaction with other catastrophic coverage proposals—including multi-year catastrophic plan terms, cost-sharing modifications, plan-level adjustments, and risk adjustment methodology—are addressed in sections III.E.2. (§ 156.80(d)(2)(ii)), III.E.6 (§ 156.155(a)(6)), and III.E.7. (§ 156.155(a)(3)) of this final rule.
Comment:
At least one commenter stated support for the hardship exemption expansion, noting that it presents an opportunity to reconsider how individual market coverage can function within defined-contribution employer models such as ICHRAs. The commenter described a two-layer healthcare strategy in which employees enroll in an affordable bronze or catastrophic Affordable Care Act plan—funded primarily with employer-provided ICHRA dollars—as protection for major medical events, while supplementing that coverage with an HSA savings strategy for everyday health care needs.
Response:
We appreciate the commenter's perspective on the interaction between the hardship exemption expansion and the ICHRA framework. We agree that the expanded hardship exemption, combined with the existing eligibility of catastrophic plans for HSA pairing, may create new opportunities for consumers and employers to design coverage strategies that balance premium affordability with protection against major medical expenses. Consumers participating in ICHRAs who qualify for the hardship exemption under § 155.605(d)(1) will be able to use their ICHRA funds toward catastrophic plan premiums, consistent with applicable ICHRA rules,[218]
and may also contribute to an HSA if their ICHRA is an HSA-compatible ICHRA and they are otherwise eligible to contribute to an HSA.[219]
We note, however, that consumers considering this strategy should carefully evaluate whether a catastrophic plan meets their individual health care needs—particularly those with ongoing or complex health care needs who may face significant out-of-pocket spending before the deductible is met.
Comment:
Commenters noted concerns about the adequacy of consumer disclosures for catastrophic plans, particularly for populations with limited health insurance literacy, reduced access to enrollment assistance, or challenges navigating digital-first enrollment systems. Commenters noted that these populations may not fully understand how catastrophic plan deductibles, cost-sharing, and pre-deductible limits operate in practice, increasing the likelihood that they will delay or forgo care and encounter access barriers only after a health need arises. Commenters requested that CMS require issuers to provide robust, plain-language consumer disclosures that accurately describe how catastrophic coverage functions in practice, including covered benefits, deductibles, cost-sharing, and pre-deductible services. Commenters also requested CMS to incorporate information about these Exchange policy changes into Navigator and Outreach & Enrollment (O&E) staff training curricula to ensure that assisters—including those serving Community Health Center (CHC) patient populations—are equipped to provide clear, accurate, and timely information to consumers.
Response:
We appreciate these commenters' emphasis on the importance of plain-language consumer disclosures and assister training, and we share their commitment to ensure that consumers have the information they need to make informed coverage decisions.
Plain-Language Disclosure Requirements:
We and issuers are already subject to robust plain-language requirements under both Federal law and the Affordable Care Act. Under the Plain Writing Act of 2010, Federal agencies are required to use clear communication that the public can understand and use, and agencies are required to submit annual compliance reports on each agency's plain language web page.[220]
We recognize that plain language is especially important in the context of health care services, where clear, concise, and jargon-free communication helps address the needs of those with limited literacy or limited health literacy skills. In addition, the Affordable Care Act requires all health plans and issuers to provide consumers with a Summary of Benefits and Coverage (SBC)—a short, easy-to-understand document written in plain language and in a standard format—at key points in the enrollment process, including upon application and at renewal.[221]
The SBC includes standardized coverage examples and is accompanied by a uniform glossary of commonly used health insurance terms. These requirements apply to
( printed page 29644)
catastrophic plans. Consistent with § 147.200, issuers are required to provide consumers with an SBC at key points in the enrollment process—including upon application and at renewal—and the SBC must be made available to consumers upon request at any time. For multi-year catastrophic plans, consistent with the framework described in section III.E.6. of this final rule (§ 156.155(a)(6)), the SBC must be provided upon initial enrollment in the multi-year term. Because multi-year catastrophic plans do not have a renewal date until the expiration of the multi-year term, the SBC renewal trigger under § 147.200 would not apply within the multi-year term itself—it would apply at the end of the term, when the enrollee's coverage is renewed for a new term. Issuers of multi-year catastrophic plans must also make the SBC available upon request at any time during the multi-year term, consistent with the general requirements of § 147.200. In the individual market, the SBC accessible to consumers during the plan comparison and selection process; consumers may also request the SBC at any time and must receive it within seven business days of the request. Under § 147.200(a)(2), the SBC must include the plan's cost-sharing provisions—including the deductible, coinsurance and cost-sharing obligations—and coverage examples illustrating how the plan covers care in common medical scenarios, helping consumers understand their potential out-of-pocket costs.
We conclude that the existing SBC requirements, together with the
HealthCare.gov
consumer education resources and assister training in this final rule, provide a sufficient framework for ensuring that consumers enrolling in catastrophic plans have access to clear, accurate, and comparable information about their coverage. We are not finalizing additional disclosure requirements specific to catastrophic plans in this rule. We will, however, monitor consumer comprehension and enrollment outcomes under the expanded hardship exemption eligibility and will consider whether additional plan-specific disclosure requirements—including disclosures targeted to consumers with chronic conditions or complex health care needs—are warranted through future notice-and-comment rulemaking.
Existing HealthCare.gov Consumer Education Resources:
We maintain robust plain-language consumer education resources on
HealthCare.gov
specifically designed to help consumers understand and compare their coverage options, including catastrophic plans. These resources include:
A dedicated Catastrophic Health Plans page that clearly notes who qualifies for catastrophic coverage, and what these plans cover. The page describes the pre-deductible benefits—preventive services at no cost, at least three primary care visits per year before the deductible, and notes that all 10 EHBs are covered but are subject to the plan deductible. The pages also directs consumers who qualify for APTC or CSR to compare bronze and silver plans before selecting a catastrophic plan.[222]
A Health Plan Categories page that presents a plain-language comparison of bronze, silver, gold, platinum, and catastrophic plan categories, including estimated cost-sharing percentages, deductible levels, and guidance on HSA eligibility for bronze and catastrophic plans.[223]
A “What Marketplace Health Insurance Plans Cover” page that describes the 10 EHBs required of all Marketplace plans and notes that adult dental and vision coverage are not EHBs—directly addressing the dental coverage gap concern raised by commenters.[224]
A plan comparison tool that presents consumers with personalized eligibility information, estimated costs after tax credits, and side-by-side plan comparisons.
We recognize that the adequacy of consumer disclosures is particularly important for populations with limited health insurance literacy, reduced access to enrollment assistance, or challenges navigating digital-first enrollment systems. For these consumers, the existing disclosure framework provides meaningful protections. As previously described, issuers are required under § 147.200 to make the SBC available at key points in the enrollment process, including upon application and at renewal, and upon request. The SBC provides standardized, plain language information about the plan's cost-sharing provisions, covered benefits, and coverage examples. Navigators, Certified Application Counselors (CACs), and other assisters also play a critical role in supplementing these disclosures—particularly for consumers who may not fully understand how catastrophic plan deductibles, cost-sharing, and pre-deductible limits operate in practice. As previously discussed, we will ensure that updated assister training materials address the specific needs of these populations, including guidance on how to walk consumers through the SBC, explain the practical implications of catastrophic plan cost-sharing, and help consumers understand when a metal-level plan may better serve their health care needs.
Agent, Broker, Web-Broker, Navigator, and Assister Training: We provide robust and ongoing training, resources, and technical support to agents, brokers, and web-brokers as well as Navigators, CACs, and other assisters throughout the plan year. PY 2026 Marketplace registration and training—available in both English and Spanish—is, at the time of publication of this final rule, live for new and returning agents, brokers, and web-brokers on the MLMS.[225]
We also host ongoing webinars and office hours throughout the year. Information on upcoming training events, topics and registration is available on
CMS.gov
via REGTAP.[226]
Additional support resources for agents, brokers, and web-brokers—including a dedicated FAQ website, a Video Learning Center, a library of guidance documents, newsletters, and quick reference guides, and access to Marketplace Help Desks—are available on the Agent and Broker Resources website. For Navigators, CACs, and other in-person assisters, PY 2026 FFE Assister Certification Training—including Navigator and CAC training courses and microlearning modules—is available through the CMS Training for Navigators, Agents, Brokers, and Other Assisters page. CMS also provides assisters with access to the Assister Support Hub, which serves as a centralized portal for training, help desk contacts, enrollment applications, and other operational resources. Outreach and enrollment resources—including partner toolkits, multilingual consumer materials in languages including Arabic, Chinese, French, Russian, and Vietnamese, and materials tailored to special populations—are available on the In-Person Assisters page on
CMS.gov. Before and during the 2026 open enrollment, which began on November 1, 2025, we provided training and resources to agents, brokers,
( printed page 29645)
assisters, and navigators specifically addressing the expansion of hardship exemption eligibility, including guidance on how to explain the differences between catastrophic and metal-level plans and the circumstances under which consumers may benefit from—or should carefully consider alternatives to—catastrophic plan enrollment. We will continue to provide updated training materials, resources, and office hours to support assisters as this policy is codified and implemented for the upcoming open enrollment in November 2026 and future years.
We agree that assisters play a critical role in helping consumers—particularly those with chronic health conditions who may have complex health care needs or limited health insurance literacy—make informed enrollment decisions. We will ensure that updated Navigator and open enrollment training curricula reflect the expanded hardship exemption eligibility, the coverage characteristics and cost-sharing obligations of catastrophic plans, the absence of dental benefits in catastrophic plans, and the importance of helping consumers understand how their APTC, PTC, and CSR eligibility interacts with their plan choices.[227]
We will also ensure that training materials address the specific needs of chronic health condition patient populations, including individuals managing chronic conditions or multiple comorbidities for whom catastrophic coverage may not be the most appropriate option.
Given our network adequacy review proposals at §§ 156.230 and 155.1050(d) (which are described in greater detail later and in section III.E.10 of this final rule), in the 2027 Payment Notice proposed rule (91 FR 6354), we proposed, for plan years beginning on or after January 1, 2027, to restore network adequacy authority back to the State Exchanges and SBE-FPs through the removal of requirements at § 155.1050(a)(2)(i) and (ii), which require State Exchanges and SBE-FPs to establish and impose quantitative time and distance network adequacy standards that are at least as stringent as standards for QHPs on the FFEs. We proposed to amend § 155.1050(a)(2) to return to the requirement that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards specified in § 156.230(a)(1)(ii) and (iii) for network plans, or proposed § 156.236(a) for non-network plans, as applicable. These proposals sought to align § 155.1050 with the proposed changes in § 156.230.
In the 2025 Payment Notice (89 FR 26218), we finalized § 155.1050(a)(2)(i)(A) to require that, for plan years beginning on or after 2026, State Exchanges and SBE-FPs establish and impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs under § 156.230. We also finalized § 155.1050(a)(2)(i)(B), which requires that, for plan years beginning on or after January 1, 2026, State Exchanges and SBE-FPs conduct quantitative network adequacy reviews to evaluate a plan's compliance with network adequacy standards under § 156.230(a)(1)(ii), (a)(1)(iii), and (a)(2)(i)(A) prior to certifying any plan as a QHP, while providing a QHP certification applicant the flexibilities described under § 156.230(a)(2)(ii) and (a)(3) and (a)(4).
In the proposed rule (91 FR 6355), we proposed to remove these requirements to align with our proposals to add § 155.1050(d). We also proposed to revise § 156.230 to include language to differentiate areas where requirements are applicable to all QHP issuers that use a provider network, and where requirements are applicable to only QHP issuers that use a provider network in FFE States, including States performing plan management, that do not elect to conduct their own provider access reviews or that HHS has determined have not demonstrated sufficient authority and the technical capacity to conduct network adequacy reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program, as described later in this section and in section III.E.10 of this proposed rule. We also proposed these changes in recognition of the longstanding authority State Exchanges and SBE-FPs previously had to develop and enforce network adequacy standards and, given this past authority and experience, their network adequacy review capabilities and expertise.
The proposal also sought to restore the authority that State Exchanges and SBE-FPs originally had in establishing network adequacy standards for their QHPs and issuers, acknowledging that State Exchanges and SBE-FPs have the experience and expertise to be the best positioned entities to develop network adequacy standards for their distinct consumer markets.
Through our recent assessment of State Exchange and SBE-FP implementation of the network adequacy policy finalized in the 2025 Payment Notice (91 FR 6355), many State Exchanges and SBE-FPs demonstrated they have network adequacy standards and reviews in place that met or exceeded the requirements finalized in the 2025 Payment Notice. We stated in the proposed rule (91 FR 6355) that we are aware that some State Exchanges made updates in the lead up to PY 2026. Throughout 2024, State Exchanges and SBE-FPs provided us with detailed answers to a survey (OMB Control Number: 0938-1341 (CMS-10592)/Expiration date: April 30, 2027) on existing statutory, regulatory, and/or sub-regulatory authorities and policies in place to conduct network adequacy reviews that impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs. We met with each State Exchange and SBE-FP to discuss in detail what they were currently doing to assess network adequacy and any modifications they were working toward prior to PY 2026. State Exchanges and SBE-FPs described a wide variety of approaches, including assessing compliance with time and distance standards, as was required in the 2025 Payment Notice and assessing compliance with time or distance individually due to geographical considerations, appointment wait times, or provider enrollee ratios.
We stated in the proposed rule that the variety amongst the State Exchanges and SBE-FPs regarding how they chose to implement their unique approaches underscored the importance of restoring authority to State Exchanges and SBE-FPs, since these States can better take into consideration the needs of specific enrollee populations stemming from factors such as provider supply shortages and topography. Indeed, while some State Exchanges and SBE-FPs made modifications or updates to their network adequacy policies in the lead-up to implementation, we ultimately determined that most State Exchanges and SBE-FPs were either already aligned with the requirements described at § 155.1050(a)(2)(i), or were granted the exception described under § 155.1050(a)(2)(ii), meaning we determined that the State established and imposed time and distance standards at least as stringent as those for QHPs on the FFEs, or that the State established and enforces alternate quantitative network adequacy standards that are reasonably calculated to ensure a level of access to providers
( printed page 29646)
that is comparable to the Federal network adequacy standards established for QHPs under § 156.230(a)(1)(iii), (a)(2)(i)(A), and (a)(4).
This proposal also sought to align with proposed § 155.1050(d) and remove an unnecessary layer of Federal regulatory burden on State Exchanges and SBE-FPs while maintaining consumer protections through the existing, robust State-level processes for setting network adequacy requirements for issuers and reviewing QHP network adequacy within their respective State Exchange or SBE-FP that such State Exchanges and SBE-FPs demonstrated to us were already in place prior to PY 2026. Due to the well-established, long-existing approaches that State Exchanges and SBE-FPs demonstrated to us were already in place, we stated in the proposed rule that we have a high level of confidence that restoring § 155.1050(a)(2) to the requirements in place prior to PY 2025 would not result in consumers losing reasonable access to services without unreasonable delay. Generally, most State Exchanges and SBE-FPs have demonstrated through surveys and subsequent conversations that they are conducting network adequacy reviews in compliance with § 155.1050(a)(2)(i) and the remainder of State Exchanges and SBE-FPs were conducting network adequacy reviews that satisfied the criteria for an exception described at § 155.1050(a)(2)(ii).
Separately, concurrent with the proposal to amend § 156.230, to implement changes to reviews of network adequacy for QHP issuers in FFE States that demonstrate sufficient authority and the technical capacity to conduct such reviews and elect to do so, we proposed the addition of § 155.1050(d), which would establish an Effective Provider Access Review Program.
We proposed at § 155.1050(d)(1) that, beginning PY 2027, we would defer provider access reviews of QHP issuers' plans, with or without a provider network, applying for certification to be offered as a QHP through an FFE, to States that elect to conduct such provider access certification reviews, provided the State has demonstrated sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d)(2) through (d)(4). We proposed at § 155.1050(d)(2) to clarify that FFE States considered to have an Effective Provider Access Review Program must ensure that a QHP issuer that uses a network of providers ensures that the in-network providers, as available to all enrollees, include essential community providers (ECPs) in accordance with § 156.235, and maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay. The QHP issuer's provider network must also be consistent with the rules for network plans in section 2702(c) of the PHS Act.
At § 155.1050(d)(3), we proposed that FFE States considered to have an Effective Provider Access Review Program must ensure that a QHP issuer that does not use a network of providers (a non-network plan) provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that services will be accessible without unreasonable delay.
At § 155.1050(d)(4), we proposed the factors necessary for a State operating on the FFE to be considered to have an Effective Provider Access Review Program. We also proposed to revise § 155.1050(a)(1) to clarify that an FFE State that has elected to conduct provider access reviews and has been determined to have an Effective Provider Access Review Program must ensure that each QHP provides sufficient access to providers in a manner that meets the standards specified in § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or proposed § 156.236(a) for non-network plans, as applicable. A detailed discussion of this proposal can be found in section III.E.10 of this final rule. Additionally, we stated in the proposed rule that we would encourage State Exchanges and SBE-FPs to use their network adequacy authority to conduct similar provider access reviews that consider criteria consistent with those outlined at § 155.1050(d)(2) through (d)(4) and described in section III.E.10. of this final rule.
In summary, we proposed to amend § 155.1050(a)(2) to eliminate, for plan years beginning on or after January 1, 2027, the requirements under § 155.1050(a)(2)(i) and (ii) for State Exchanges and SBE-FPs. We proposed to revise § 155.1050(a)(2) to require that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards specified in § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or proposed § 156.236(a) for non-network plans, as applicable (91 FR 6354). We also proposed the addition of § 155.1050(d), which is described in greater detail in section III.E.10 of this final rule.
We sought comment on this proposal. We also sought comment on what level of transparency is necessary and appropriate to safeguard public trust in Effective Provider Access Review Programs. While we are not specifically contemplating any particular form of new disclosure in this space at this time, we stated in the proposed rule that we are interested in public feedback on which elements of process and which outputs of Effective Provider Access Review Programs should be subject to public disclosure.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing with modifications the proposed policy to restore network adequacy authority back to the State Exchanges and SBE-FPs through the removal of requirements at § 155.1050(a)(2)(i) and (ii) and amending § 155.1050(a)(2) to return to the requirement that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards specified in § 156.230(a)(1)(ii) and (iii) for network plans, or proposed § 156.236(a) for non-network plans if such plans are allowed to be offered through the Exchange, as applicable. While we finalized in section III.E.12. of this final rule to delay implementation of allowing non-network plans to receive certification to be offered as QHPs through the FFE beginning PY 2028, State Exchanges and SBE-FPs retain full discretion and authority to determine the appropriate implementation timeline for their States if allowing non-network plans to be offered through State Exchanges or SBE-FPs. Accordingly, under § 155.1050(a)(2), State Exchanges and SBE-FPs may allow non-network plans to be offered through the Exchange for plan years beginning on or after January 1, 2027, as applicable. We also finalized a clarification under § 155.1050(a)(2) to suggest these States may allow non-network plans to be offered through the Exchange if such plans are allowed to be offered through the Exchange to preserve the State's authority to determine whether non-network plans are appropriate for their markets. We refer readers to section III.E.12. of this final rule for a more detailed discussion of the rationale to allow State Exchanges and SBE-FPs to offer the non-network plans through their Exchanges
( printed page 29647)
beginning PY 2027, as applicable. We summarize and respond to public comments received on this proposal to restore network adequacy authority back to the State Exchanges and SBE-FPs below. In section III.E.10. of this final rule, we summarize and respond to public comments received on the proposal to allow FFE States to elect to conduct provider access reviews if they meet the criteria for having an Effective Provider Access Review Program and discuss modifications we are finalizing to this proposed policy.
Comment:
A number of commenters expressed support for both policies at §§ 155.1050 and 156.230 to both restore flexibility and authority to State Exchanges in their network adequacy reviews and to allow FFE States to demonstrate they have Effective Provider Access Review Programs. These commenters agreed that States are better positioned to evaluate local provider availability and that many States (across all Exchange types) have already invested in their capacity to examine provider access in recent years. Commenters noted the “rigorous” criteria for an FFE State to qualify as an Effective Provider Access Review Program and agreed that these criteria required for States to conduct provider access reviews, detailed under § 155.1050(d)(2) through (d)(4), fulfill the responsibility under the Affordable Care Act to assure plans offer sufficient access to providers. Commenters stated support for the continued data collection and offers of continued technical assistance to States as they implement Effective Provider Access Review Programs as well as other States' work to develop network adequacy standards and review processes with the intention to qualify in subsequent plan years.
Additionally, we received multiple comments stating support for the restoration of State Exchange and SBE-FP flexibility and authority to develop network adequacy standards unique to their populations. Commenters agreed that States are often better positioned to evaluate network adequacy than Federal regulators, due to their intimate knowledge of local market dynamics and geographic considerations. Several State Departments of Insurance stated their support for a restoration of the approach that emphasizes State oversight and emphasized intent to ensure consumer protections and timely, reasonable access to in-network providers.
Response:
We concur that the restoration of flexibilities and authority to State Exchanges and SBE-FPs will be beneficial. With this policy change, we intend to recognize the work that State Exchanges and SBE-FPs are already doing to regulate QHP issuers and ensure consumers in their States have sufficient access to robust provider networks under § 156.230(a)(1)(ii) and (iii) and under § 156.236(a), should they choose to allow non-network plans to be offered on their State Exchanges or SBE-FPs. Moreover, this policy will remove duplicative oversight that is best performed by the States.
For the reasons stated earlier in this section of this final rule, we agree that the criteria for an FFE State to conduct provider access reviews through an Effective Provider Access Review Program are robust and ensure each State can protect consumers while encouraging flexibility and innovation in provider access reviews. Additionally, the continued collection of provider access data (described further in section III.E.10 of this final rule) will provide an extra layer of consumer protection through our visibility and responsiveness at the Federal level. For example, we will be able to analyze the provider data collected during the QHP certification process to assist in addressing any complaints we may receive from external interested parties; appointment wait time (AWT) secret shopper surveys will ensure we maintain a level of awareness around appointment wait times for primary care provider and behavioral health providers; and we can leverage our existing infrastructure of provider data collection to support FFE States as they develop and implement provider access reviews.
Comment:
Many commenters stated opposition to removing the “Federal as a floor” approach by rescinding the requirement that State Exchanges and SBE-FPs implement quantitative network adequacy standards as stringent as those applied in FFEs, specifically the time and distance standards outlined at § 156.230(a)(2)(i). Commenters supported Federal standards that included consistent benchmarks and uniform standards. The commenters stated concern that the removal of these requirements would make it difficult to objectively evaluate the adequacy of provider networks across States and may result in reductions in timely access to care. Additionally, several consumer advocacy groups commented that rescinding the requirement for State Exchanges and SBE-FPs to implement standards as stringent as those for FFEs could result in a lack of consistent oversight and accountability across Exchanges. The general consensus of comments opposing removing a “Federal floor” highlighted potential impacts on consumer access to care for mental health and substance use disorders and specialty care due to potentially narrower provider networks. This group of commenters requested retaining Federal standards as a minimum “Federal floor.”
Response:
We acknowledge concerns associated with removing requirements for State Exchanges and SBE-FP States to implement quantitative time and distance standards as-stringent-as those for QHPs participating on the FFEs. While a single, uniform Federal network adequacy standard comes with certain advantages, we believe that, as it relates to State Exchanges and SBE-FPs, there is also the potential for disadvantages, including impeding States' ability to respond to their unique market needs by requiring them to dedicate their limited capacity to a one-size-fits all policy that may not best reflect the needs of that State.
In response to the 2025 Payment Notice, State Exchanges and SBE-FPs implemented various unique approaches to conform to the rule's requirements that State Exchanges and SBE-FPs implement network adequacy time and distance standards at least as stringent as standards for QHPs participating on the FFEs, or be granted an exception if the State demonstrates that the Exchange applies and enforces alternate quantitative network adequacy standards that are ensured by Federal network adequacy standards established for QHPs under § 156.230(a)(1)(iii), (a)(2)(i)(A), and (a)(4). Instead of requiring States to react to our policies, we believe that restoring authority to the States will enable them to proactively adapt their Exchange standards to meet their market's needs, as they will be better able to take into consideration the needs of their enrollee population related to factors such as provider supply shortages and topography. We previously determined that generally most State Exchanges and SBE-FPs were already aligned with the requirements now being rescinded at § 155.1050(a)(2)(i), meaning that they had time and/or distance standards we determined to be as-stringent-as our Federal standards, or had implemented alternative network adequacy review activities that allowed them to be granted the exception, and we encourage these States to maintain these standards. The restoration of the previous flexibilities can support State Exchanges and SBE-FPs to conduct their review activities according to their local markets without requiring the State Exchange or SBE-FP to adhere to the one-size-fits-all Federal time and
( printed page 29648)
distance standards. With this policy change in effect, State Exchanges and SBE-FPs now have the authority to adapt their standards as they see fit. Notably, based on interactions with States and subsequently gaining additional understanding of their existing work, we believe States will not see this change in policy as an opportunity to roll back their current programs, but rather will instead stay the course and continue to dedicate resources to refining their long-existing network adequacy reviews and adapt to State-specific needs.
Comment:
A few commenters stated that removing the requirement for State Exchanges and SBE-FPs to conduct network adequacy reviews prior to QHP certification could have a negative impact on consumers if the State chooses to perform retrospective reviews (that is, reviewing network adequacy after issuers have been certified for the plan year). Furthermore, commenters stated concern that many State regulatory agencies currently lack capacity to conduct network adequacy reviews prior to certifying plans. As such, several commenters requested that we require State Exchanges and SBE-FPs to publicly report their network adequacy standards, network adequacy review results, and review methodologies to provide visibility into non-compliant networks.
Response:
We acknowledge commenters' concerns that the removal of the requirement to conduct network adequacy reviews prior to certification could result in States Exchanges and SBE-FPs rolling back operations and agree there are consumer protection benefits to requiring QHP issuers be reviewed for network adequacy prior to QHP certification. However, State Exchanges and SBE-FPs are still required to ensure, per the State's authority, that each QHP provides sufficient access to providers in a manner that meets standards under §§ 156.230(a)(1)(ii) and (iii) for network plans, or, for plan years beginning on or after January 1, 2027, § 156.236(a) for non-network plans (if such plans are allowed to be offered through the Exchange), as applicable. Notably, we require a State to attest to meeting these standards as part of our approval for a State seeking to implement a State Exchange or SBE-FP. We continue to encourage State Exchanges and SBE-FPs to conduct network adequacy reviews prior to QHP certification, though we will be finalizing the policy as proposed. However, we recognize State Exchanges and SBE-FPs may choose to implement provider access review activities that may be better instituted at other times during the plan year. For example, appointment wait time reviews may be more appropriately conducted during the plan year itself with results informing mid-year corrective actions or future plan year requirements.
We are also mindful that the change we are finalizing provides a potential opportunity for State Exchanges and SBE-FPs to invest their resources in the implementation or continuation of network adequacy reviews that may be different than reviewing for time and distance standards (whether prior to QHP certification or after) but more appropriate for the consumers in that State. States Exchanges and SBE-FPs may also find value in adopting a continuous monitoring approach through “spot check” reviews conducted throughout the plan year, offering more flexible and ongoing oversight compared to relying on a single review prior to QHP certification.
Though restoring the flexibilities does technically result in removing the requirement at § 155.1050 for State Exchanges and SBE-FPs to conduct reviews prior to certification, this does not mean that State Exchanges and SBE-FPs will not continue to do so. We are aware of State Exchanges and SBE-FPs that conducted network adequacy reviews prior to QHP certification even before we codified this requirement in PY 2026 and we do not have any indication that States intend to roll back operations that were in place prior to PY 2026. We are aware, based on surveys conducted in PY 2024 that prior to PY 2026, State Exchanges and SBE-FPs largely mirrored HHS' network adequacy reviews prior to QHP certification. As such, this policy change will remove redundant oversight and return authority to the States. Moreover, the increased flexibility will enable States Exchanges and SBE-FPs to conduct network adequacy reviews that fit the needs of their market, and we encourage State Exchanges and SBE-FPs to continue applying measures to assess network adequacy beyond time and distance requirements.
Additionally, we will not require State Exchanges and SBE-FPs to establish public reporting measures for QHP compliance with State network adequacy standards, as our intention is to restore flexibility to the State Exchanges and SBE-FPs and reduce burden. We believe that State Exchange and SBE-FP review of these requirements for QHP certification is sufficient and aligns with the Federal Exchange approach. We also believe that requiring public reporting of issuer network adequacy review results may risk making public proprietary business information. Publishing this information may also lack sufficient context, especially when any noted network deficiencies may be due to geographic limitations or provider availability, or when a deficiency may be in the process of remediation by the issuer.
While there are no current Federal requirements for State Exchanges or SBE-FPs to make public their network adequacy standards, operations, or results, many State Exchanges and SBE-FPs already have public-facing documentation of their network adequacy standards and requirements, though they may or may not make public the results of network adequacy reviews. We would encourage all States to refer to the resources available on the network adequacy page of the QHP certification website,[228]
including the available templates, other application resources and requirements, instructions, and frequently asked questions as they implement their programs and consider items to make publicly available. We encourage interested parties to consult directly with their State regulators concerning visibility to ensure consumer protection and sufficient access to care.
Comment:
Several commenters stated concern that removing the policy under § 155.1050(a)(2)(i)(A) may disproportionately impact access for rural consumers, especially those seeking behavioral health or substance use disorder services. Commenters noted that States may “relax,” or eliminate network adequacy standards for time and distance thereby harming rural consumers who might lose access to providers within a reasonable distance. Commenters highlighted potential consequences if status quo network adequacy is not retained: longer travel times, fewer in-network options, delayed care, and increased out-of-network claims.
Response:
We acknowledge concerns that removing the requirements at § 155.1050(a)(2)(i)(A) could result in changes to provider networks, including more narrow networks in rural areas specifically. However, we believe the restoration of State authority over network adequacy standards for State Exchanges and SBE-FPs is supportive of an efficacious Exchange. Additionally, we encourage States to consider these commenters' concerns when assessing the network adequacy of QHP issuers operating in their rural markets. Moreover, State Exchanges and SBE-FPs will still be required under
( printed page 29649)
§ 155.1050(a)(2) to ensure that each QHP meets applicable standards specified in § 156.230(a)(1)(ii) and (iii) for network plans. This includes the requirement that a QHP that uses a provider network maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay. They will also be required to ensure non-network plans ensure access to a range of providers, including providers that specialize in mental health and substance use disorder services, that accept the non-network plan's benefit amount as payment in full, under proposed § 156.236(a) for non-network plans, beginning on or after PY 2027, if the State intends to allow such plans to be offered through the Exchange.
While we seek to provide flexibility to State Exchanges and SBE-FPs in the determination of how to achieve the aforementioned access requirements, we do not agree that the removal of the requirement to implement time and distance standards as stringent as the Federal standards for QHPs in State Exchanges will directly result in further reductions in access for rural consumers. Reviewing for time and distance standards is only one way to assess a QHP for network adequacy, and removing the requirement to implement our Federal standards allows State Exchanges and SBE-FPs to innovate in their approach, acknowledging the limitation of Federal time and distance standards which may be insurmountable for a QHP to achieve in rural areas due to market factors such as provider shortages. Removing this requirement restores flexibility to the State Exchange and SBE-FP to assess and address rural access issues in ways that may be most appropriate for that particular State, beyond time and distance standards, such as through assessing provider-enrollee ratios, for example, or investing limited resources towards working directly with provider interested parties to increase numbers and types of providers located in rural areas as well as utilizing leverage with QHPs in their States to contract with more available providers in a rural area to ensure as much access as possible for their residents. State Exchanges and SBE-FPs have sufficiently demonstrated their capacity to assess the needs of their consumers across all geographies, and we believe that States are best situated to evaluate the unique network adequacy requirements necessary to ensure proper access to behavioral health and substance use disorder services. Any additional oversight from Federal regulators would be duplicative and risk misunderstanding the needs of each market.
Comment:
Several commenters responded to our request for comment on the level of transparency necessary and appropriate to safeguard public trust in FFE States' Effective Provider Access Review Programs. Commenters called for strong transparency efforts and opportunity for public comment on their FFE State's ability to implement and maintain an Effective Provider Access Review Program. These included requests for public facing documentation of an FFE State's network adequacy standards, publishing issuer deficiencies and any justifications (for example, explanations of deficiencies such as insufficient numbers of providers or facilities) and exceptions (for example, allowances of certification despite deficiencies) granted by the FFE State, information around consumer complaints, information on inaccuracies in provider directories, and notifications of and updates on any proposed timelines for an FFE State to demonstrate that it will meet standards to become an Effective Provider Access Review Program.
Response:
We appreciate the responses to our request for comment regarding transparency. While we will continue to consider commenters' points, at this time we will not include additional requirements concerning FFE State transparency as it relates to their election, application, development, or operation of an Effective Provider Access Review Program. Regarding requests for the publishing of issuer deficiencies, justifications, exceptions, and consumer complaints, we believe that requiring public disclosure of this information may risk detailing proprietary business information, including contracting details and network development strategies. We also believe that publishing this information may lack context and will not benefit consumers, particularly when deficiencies or complaints are due to geographic limitations or provider availability. Regarding inaccurate provider directories, we note that provider directory information is highly dynamic and changes frequently and we believe that public reporting of provider directory inaccuracies may pose significant operational burden and would not be useful as it is operationally infeasible to do so in real time.
Regarding requests for public-facing documentation of an FFE State's network adequacy standards, we believe that the criteria required under § 155.1050(d)(4) that the State have their provider access standards set forth in statute or regulation, and the FFE State's provider access review process includes reporting systems for provider access metrics and documentation of methodology and the State provides descriptions of all data collection systems, resources, templates, and methodologies used by the State is sufficient for public notice and review because we believe these and the other criteria set a satisfactorily high bar to qualify provider access reviews that should instill consumer confidence in their FFE State's ability to conduct provider access reviews without risking disclosure of issuer's confidential business information, including contracting details and network development strategies, which would be inappropriate. We would refer FFE States with an Effective Provider Access Review Program to our Network Adequacy QHP Certification web page as a model for items to make publicly available regarding provider access reviews. Regarding notifications of and updates on any proposed timelines for an FFE State to demonstrate that it will meet standards to become an Effective Provider Access Review Program, we note that numerous factors may influence a State's timeline that may cause frequent revision, which may ultimately cause more confusion for the public. However, we plan to publicly share a list of States that elect to conduct provider access reviews and have been determined to have an Effective Provider Access Review Program, once that determination has been made. We will continue to evaluate the appropriate scope and format of any necessary public disclosures and highly encourage interested parties to engage with their State regulators to achieve a level of transparency that all parties find satisfactory.
19. Effective Essential Community Provider Review Program (§ 155.1051)
In the 2027 Payment Notice proposed rule (91 FR 6355), beginning PY 2027, we proposed to allow FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of an issuer's plans with or without a provider network in their State applying for certification as a QHP to be offered through an FFE. We stated that we would allow FFE States to conduct such ECP certification reviews provided the State demonstrates sufficient authority and the technical capacity to conduct these reviews by satisfying the
( printed page 29650)
applicable criteria established by HHS to be considered to have an Effective ECP Review Program, which we proposed to implement at § 155.1051. This policy and related summaries of and responses to public comments received are discussed in more detail in section III.E.11 of this final rule.
20. General Program Integrity and Oversight Requirements (§ 155.1200)
In the 2027 Payment Notice proposed rule (91 FR 6355), we proposed to amend § 155.1200 to add new paragraph (e) to permit State Exchanges to satisfy certain requirements of the independent external programmatic audit, as outlined in paragraph (d), by completing the proposed State Exchange Improper Payment Measurement (SEIPM) process that would be established at 45 CFR part 155, subpart Q. We also proposed to amend § 155.1200(d) to reduce duplication between the proposed State Exchange SEIPM program described in proposed subpart Q and the annual independent external programmatic audit requirements and standards described at § 155.1200(c) and (d).
The Payment Integrity Information Act of 2019 (PIIA) (Pub. L. 116-117) requires Federal agencies to annually estimate and report on improper payments in the programs they administer that have been determined to be susceptible to significant improper payments. Pursuant to the PIIA, we proposed to establish a SEIPM program, as we have determined that APTC payments administered by State Exchanges are susceptible to significant improper payments and are subject to additional oversight.[229]
The PIIA defines significant improper payments as those exceeding either $100 million or exceeding $10 million and 1.5 percent of the program outlays. The proposed SEIPM program requirements are set forth in new proposed subpart Q, as discussed in section III.D.21. of this final rule.
We stated in the proposed rule that the proposed SEIPM program would specify a methodology to develop State Exchange improper payment estimates and provide for the accurate calculation, and subsequent reporting, of an improper payment rate in HHS' Agency Financial Report (AFR). To ensure the accurate and consistent calculation of improper payments via the SEIPM program, we proposed to require that State Exchanges provide HHS with access to certain State Exchange data, including eligibility determinations and enrollment information. We further proposed that State Exchanges found to have significant improper payments could, to correct improper payment root causes, be required to develop corrective action plans (CAPs).
Our authority to oversee the State Exchanges arises from the program integrity and oversight requirements they must meet that are specified at section 1313(a) of the Affordable Care Act and at §§ 155.1200 and 155.1210. Key State Exchange reporting requirements at § 155.1200(b) include the annual submission of: (1) a financial statement in accordance with generally accepted accounting principles; (2) a report showing compliance with Exchange requirements; and (3) performance monitoring data.
Pursuant to § 155.1200(c) and (d), each State Exchange is also required to engage or contract with an independent qualified auditing entity that follows generally accepted government auditing standards to perform annual independent external financial and programmatic audits that address compliance with 45 CFR part 155, subparts D and E, or other 45 CFR part 155 requirements as specified by HHS. State Exchanges must provide HHS the audit results, including CAPs to address any audit-identified material weaknesses or significant deficiencies, and we monitor these CAPs until findings are resolved, pursuant to § 155.1200(c)(2). These audits allow us to oversee State Exchange compliance with eligibility and enrollment standards. In sub-regulatory guidance, we specify that the scope of the audits must also include 45 CFR part 155, subparts C and K.[230]
We proposed to amend § 155.1200(d) to reduce duplication between the proposed SEIPM program described in subpart Q and the annual independent external programmatic audit requirements and standards described at § 155.1200(c) and (d). We proposed to add § 155.1200(e) to permit a State Exchange to satisfy certain annual independent external programmatic audit requirements, as described at § 155.1200(d), by completing the proposed required annual SEIPM program process. We stated in the proposed rule that these certain audit requirements would be limited to compliance with 45 CFR part 155, subparts D and E, and would be specified in guidance we would issue. We also proposed to amend § 155.1200(d) to cross-reference proposed § 155.1200(e) to minimize duplication between the annual programmatic audit requirement and proposed SEIPM program. We stated that this would allow us to continue to require an annual independent programmatic audit of other subparts beyond eligibility and enrollment, while reducing duplication for oversight of eligibility and enrollment provisions.
We stated in the proposed rule that we believe this policy would reduce duplicative efforts and burden on State Exchanges that would otherwise be required to fully comply with the programmatic audit requirements and SEIPM, while also maintaining the programmatic audits for requirements not reviewed as part of SEIPM.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received below.
Comment:
Most commenters supported the effort to reduce duplication between the proposed SEIPM program and the annual independent external programmatic audit requirements, while expressing concerns about the timeline and feasibility of SEIPM. The commenters agreed the policy would avert duplication and costly administrative inefficiencies.
Response:
We appreciate the support and affirm that a central goal of the proposed amendments to § 155.1200(d) and the addition of § 155.1200(e) is to streamline oversight obligations for State Exchanges while maintaining program integrity safeguards. We agree that reducing duplicative audit requirements will allow State Exchanges to allocate administrative resources more efficiently without compromising the integrity of Federal oversight. The concerns raised by the commenters regarding timeline and feasibility are addressed in the SEIPM section below.
Comment:
One commenter, expressing concern about the operational feasibility of SEIPM, suggested utilizing data from the existing annual independent external programmatic audit to assess improper APTC payments, in lieu of SEIPM, or, alternatively, removing APTC-verification requirements from the SMART. Another commenter also sought specific clarification on how existing audit requirements would
( printed page 29651)
actually be reduced or eliminated with the introduction of SEIPM.
Response:
The PIIA requires a specific methodology for developing improper payment estimates and calculating an improper payment rate for inclusion in HHS' AFR, and the existing SMART audit framework was not designed to satisfy these statutory requirements. Therefore, a distinct program, that we proposed as SEIPM, is necessary to fulfill our PIIA obligations. While the annual independent external programmatic audit will continue to be required, we will issue sub-regulatory guidance specifying the specific programmatic audit requirements that may be satisfied through SEIPM participation, including the required APTC-verification requirements within SMART. We remain committed to working collaboratively with State Exchanges to ensure that the SEIPM program is implemented in a manner that is operationally feasible, consistent with our PIIA obligations, and that minimizes any potential audit duplication.
Comment:
One commenter did not agree with the proposal, stating that this will no longer be an independent evaluation and will result in inconsistencies.
Response:
We clarify that proposed § 155.1200(e) is designed to permit State Exchanges to satisfy certain annual independent external programmatic audit requirements through completion of the SEIPM process, while still continuing to maintain the annual independent external programmatic audit of additional subparts and requirements, separate from the SEIPM.
21. State Exchange Improper Payment Measurement (SEIPM) (§§ 155.1600 through 155.1650)
In the 2027 Payment Notice proposed rule (91 FR 6356), we proposed to establish the SEIPM, pursuant to the PIIA,[231]
to measure improper payments of APTC administered by a State Exchange. To codify the proposed SEIPM requirements, we proposed to establish a new subpart Q at 45 CFR part 155. The PIIA requires Federal agencies to periodically review programs and activities to identify those susceptible to significant improper payments, and to report improper payment estimates for such programs. The PIIA defines significant improper payments as those exceeding $100 million or those exceeding $10 million and more than 1.5 percent of program outlays. In FY 2016, we conducted improper payment risk assessments for the Health Insurance Exchange programs and concluded that the APTC program is susceptible to significant improper payments. Between FY 2017 and FY 2019, we developed and piloted activities for measuring improper payments of APTC, which led to developing the Exchange Improper Payment Measurement Program for Exchanges administered through the FFE. Through that initiative, HHS began annual reporting of improper payment estimates in the FY 2022 Annual Financial Report (AFR) for APTC administered through the FFE.[232]
However, due to our lack of regulatory authority to collect the same information from State Exchanges, we could not do the same for APTC administered through State Exchanges.
As a result, we proposed in the 2023 Payment Notice proposed rule (87 FR 584) to establish the SEIPM program, which would have required State Exchanges to submit certain information to HHS so that HHS could report an improper payment estimate of APTC administered by State Exchanges. We proposed that it would begin in calendar year 2024, but a significant volume of public comments stating that State Exchanges would need additional time and guidance to prepare for SEIPM persuaded us not to finalize that proposal. Instead, we proposed in the 2024 Payment Notice (77 FR 78206, 78213) to establish an Improper Payment Pre-Testing and Assessment Program (IPPTA) that would be mandatory for State Exchanges and where they would participate in pre-audit activities to prepare them to comply with audits required under the PIIA. We said that activities under the proposed IPPTA program would (1) prepare State Exchanges for the planned measurement of improper payments, (2) test processes and procedures that support HHS' review of determinations of APTC made by State Exchanges, and (3) provide a mechanism for HHS and State Exchanges to share information that will aid in developing an efficient measurement process. We finalized the IPPTA in the 2024 Payment Notice (88 FR 25740).
In the 2027 Payment Notice proposed rule, we stated that IPPTA was currently underway and the first cohort of eight State Exchanges had completed all of the information submission requirements for ten or more sampled tax households. We had completed the review process for the first cohort of State Exchanges and had communicated to them the findings. As of the time of publication of the 2027 Payment Notice, data collection had been completed for all ten State Exchanges in the second cohort.
The main challenge that HHS and State Exchanges have experienced with IPPTA relates to the quantity of data that the State Exchange must submit in order for HHS to accurately determine whether each payment of APTC was proper or improper. For each tax household, there may be multiple QHP policies, and multiple enrollees who were determined eligible for APTC, all of which invoke specific requirements for determining eligibility. These factors cause considerable volume and complexity in the data that would be required for SEIPM.
Additionally, in the 2027 Payment Notice proposed rule we stated that each State Exchange operates its own platform with a unique data architecture, making it challenging to develop a unified process by which State Exchanges could submit the requisite information. For the purposes of IPPTA, we developed a Data Request Form (DRF) to enable the automated collection of information that proved to be an effective tool for six of the eight State Exchanges in the first cohort. For the other two State Exchanges, however, some of the data had to be collected manually and not through the DRF because those States were unable to successfully submit all of the data required for measurement in the DRF format and structure. As a lesson learned from that data collection process, we proposed to allow a more flexible mechanism for SEIPM data collection.
To mitigate some of the challenges that exist with the data collection, we have automated the data validation process that allows us to assess each submitted DRF and to coordinate with the State Exchanges to correct data when inconsistencies are identified. For SEIPM, in the 2027 Payment Notice proposed rule we stated that we would use the DRF while also allowing flexibility in data submissions for allowing data to be submitted in native formats, which would lessen the burden on State Exchanges.
We proposed to establish a new subpart Q at 45 CFR part 155 (containing §§ 155.1600 through 155.1650) to codify the SEIPM requirements. We proposed to require State Exchanges to annually submit to HHS the information required for HHS to produce an estimate of improper payments in accordance with OMB
( printed page 29652)
Circular No. A-123 requirements.[233]
We proposed to measure all State Exchanges annually unless we specify otherwise and to report the calculated estimate of improper payments in the HHS AFR. In the proposed rule, we stated that State Exchanges already are required to conduct annual independent external programmatic audits, so we proposed to minimize duplication of those audit requirements with the proposed SEIPM program, as described in proposed § 155.1200(e). We additionally proposed that any State Exchange in its first year of operation would be required to participate in a 1-year SEIPM preparation phase prior to being required to satisfy the SEIPM requirements. We stated that the proposed regulations at subpart Q would be applicable beginning in January 2027.
In the 2027 Payment Notice proposed rule, we stated that this proposal would address a critical gap in improper payment oversight, as the PIIA requires Federal agencies to estimate and report on improper payments in programs determined to be susceptible to significant improper payments. We noted that, while we have established an improper payment measurement for the FFE, (that is, the Federal Exchange Improper Payment Measure or FEIPM),[234]
State Exchanges have operated without comparable systematic measurement of APTC improper payments. The FFE's improper payment measurement is overseen by the Payment Accuracy and Reporting Group (PARG), within the CMS Office of Financial Management (OFM), which has developed comprehensive methodologies and systems to ensure accurate measurement and reporting. By extending similar measurement methodologies to State Exchanges through SEIPM, HHS would ensure consistent oversight and accountability across all exchange types, promoting parity in program integrity efforts nationwide. We solicited public comment on this proposal, and discuss in further detail below comments we received. Commenters generally supported program integrity goals but raised concerns about implementation timing, annual cadence, burden, data collection and sampling, IPPTA readiness, and overlap with existing audit requirements.
a. Purpose and Scope (§ 155.1600)
We proposed to add a new subpart Q to 45 CFR part 155, which would establish State Exchange responsibilities.
We proposed to add a new § 155.1600 that would convey the purpose and scope of the SEIPM. At § 155.1600(a), we proposed the SEIPM would be an initiative through which HHS measures improper payments of APTC that are administered by State Exchanges, described in more detail in proposed § 155.1610. We proposed to use the results of SEIPM to produce an estimate of improper payments of APTC aggregated across State Exchanges.
At § 155.1600(b), we proposed that unless specified otherwise by HHS, all State Exchanges on an annual basis would be required to submit information that is necessary to support the SEIPM processes. In the proposed rule, we stated that the data and information we would require from State Exchanges would be essential for us to conduct accurate improper payment measurement, as it is not available through any other existing sources or systems. Unlike the FFE where we have direct access to enrollment and payment data, State Exchanges operate independent systems that contain eligibility determinations, enrollment records, and APTC calculation data necessary for HHS to make improper payment assessment under the SEIPM. Without State Exchanges submitting the proposed information, we noted that we would be unable to fulfill our statutory obligations under the PIIA to measure and report improper payments. We stated that the proposed annual submission requirement would ensure that we have access to the most current and complete data necessary to produce statistically valid improper payment estimates and identify areas for program improvement.
At § 155.1600(c), we proposed that HHS would publish in its AFR an estimate of improper payments aggregated across all State Exchanges. Publication in the HHS AFR would ensure that APTC improper payment estimates are subject to the same transparency and accountability standards as other major HHS programs.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1600 below.
Comment:
Some commenters supported the goal of improving oversight of APTC payments administered by State Exchanges but expressed concern that the SEIPM framework would be operationally complex, duplicative of existing audit activities, and burdensome given variation in State Exchange systems. Several commenters stated that they experienced challenges with IPPTA, including significant manual effort and difficulties with data mapping and automation limitations. Other commenters stated concern that SEIPM would require significant continuous manual effort to complete data mapping and transformation. Some commenters stated concern about scaling the smaller scope of the IPPTA process to the SEIPM and stated that they would require more technical assistance to understand the program. Other commenters requested additional program details including data requirements, appeals, timelines, sampling, and enforcement. Some commenters also noted that an annual cycle may create continuous operational demands and limit the time available to implement corrective actions between measurement periods.
Response:
We appreciate commenters' support for improving oversight and acknowledge the operational considerations associated with implementing SEIPM across State Exchanges with varying system architectures. We also recognize that State Exchanges are subject to existing audit and oversight requirements.
However, we continue to believe that SEIPM is necessary to address a critical gap in HHS' ability to comply with the PIIA. Under the PIIA, Federal agencies are required to identify programs susceptible to significant improper payments and to produce reliable, statistically valid estimates of improper payments on an annual basis, including reporting through the AFR. While HHS has established such measurement for APTC administered through the Federally-facilitated Exchange, no comparable, systematic measurement currently exists for APTC administered by State Exchanges. Existing audits and reporting mechanisms do not produce the statistically valid improper payment estimates required under the PIIA, nor do they support consistent, nationwide measurement of payment accuracy.
SEIPM is designed to enable HHS to meet these statutory obligations by establishing a uniform framework for collecting the data necessary to calculate improper payment rates and to
( printed page 29653)
support ongoing, annual measurement and reporting. Without this framework, HHS would be unable to produce complete and comparable improper payment estimates across all Exchange types, as required under Federal law.
Accordingly, while we acknowledge commenters' concerns regarding burden and operational complexity, we are finalizing § 155.1600 as proposed. Many commenters supported the effort to reduce duplication between the proposed SEIPM program and the annual independent external programmatic audit requirements. We will continue to support State Exchanges through sub-regulatory guidance and technical assistance to facilitate implementation in a manner that is as efficient and workable as possible while ensuring compliance with PIIA requirements.
Comment:
Several commenters requested that SEIPM operate on a less frequent cycle to reduce burden and allow State Exchanges additional time to implement corrective actions between measurement periods.
Response:
We acknowledge commenters' concerns regarding the operational demands of an annual measurement cycle and the time needed to implement corrective actions. Under the Payment Integrity Information Act of 2019 (PIIA) and OMB Circular No. A-123, Federal agencies are required to produce and report improper payment estimates on an annual basis for programs identified as susceptible to significant improper payments. The sampling and measurement framework established through SEIPM is designed to support these statutory requirements.
While some Federal improper payment measurement programs operate on multi-year cycles, those approaches reflect program-specific design considerations, including program structure, data availability, and sampling methodologies. In contrast, SEIPM is designed to support ongoing, annual oversight of APTC payments administered by State Exchanges and to align with the existing annual improper payment measurement conducted for the Federally-facilitated Exchange.
Moving to a less frequent cycle could reduce the timeliness of improper payment identification and limit HHS' ability to conduct consistent, ongoing monitoring across all Exchange types. Additionally, annual measurement supports more timely identification of errors and facilitates ongoing program oversight.
While we recognize commenters' concerns regarding operational burden and the time required to implement corrective actions, we believe that these activities can occur on an ongoing basis within an annual measurement framework. Accordingly, we are finalizing § 155.1600 as proposed.
Comment:
Some commenters opposed extending SEIPM related enforcement to issuers, emphasizing that issuers do not determine eligibility or APTC payment processes, issuer enforcement is addressed in other provisions, and therefore issuers should not be held accountable for SEIPM requirements. One commenter requested HHS to require State Exchanges to publish all standards, companion guides, and instructions to issuers regarding APTC eligibility so that they have clear expectations on how data should be reconciled and can support State Exchanges in maintaining accurate enrollment records to reduce the risk of improper payments.
Response:
We clarify that the SEIPM scope and requirements codified under Subpart Q are specific to State Exchanges in relation to the improper payment measurement, and that SEIPM enforcement and requirements
will not
directly impact issuers. We acknowledge that State Exchanges coordinate with their issuers to reconcile enrollment and ensure that appropriate documentation, such as Companion Guides and reconciliation instructions, are shared between State Exchanges and their participating issuers.
Comment:
A commenter requested that HHS avoid implementing policies that could create Federal overreach and disrupt Exchange stability. The commenter requested HHS to implement SEIPM with safeguards to protect data privacy, define Federal oversight scope, and prioritize aggregate reporting structures. This commenter also stated concern about Federal overreach to withhold funding in connection to program integrity programs, which could impact the stability of the Exchanges.
Response:
We appreciate this comment, but do not agree that SEIPM may create Federal overreach as it is statutorily mandated under the PIIA. In January 2024, we began the IPPTA to help prepare States for SEIPM. While some State Exchanges are still undergoing IPPTA activities, we believe we can make operational adjustments to apply further lessons learned from those activities as we implement SEIPM. We do not believe that SEIPM will negatively affect Exchange stability, but, rather, will provide State Exchanges with information to help reduce improper payments of APTC. We further clarify that we will put safeguards in place to protect data privacy and adhere to privacy and security Federal requirements. We also note that the most significant enforcement actions under the Failure to Comply provision would only be utilized when there are severe and repeated instances of noncompliance by a State Exchange without mitigating circumstances.
b. Applicability Date and Implementation (§ 155.1605)
In this section of the 2027 Payment Notice proposed rule, we proposed to add new § 155.1605, which would establish SEIPM's applicability date.
At proposed new § 155.1605(a), we proposed that this subpart would be applicable beginning January 1, 2027, which we believe would provide State Exchanges with sufficient time to begin the SEIPM. In the proposed rule, we noted that for State Exchanges that have participated in IPPTA, the proposed January 1, 2027, applicability date would mean that those State Exchanges would submit the proposed required information and would be subject to improper payment measurement under the SEIPM beginning in 2027 for PY 2026, with the improper payment estimate being reported for the first time in 2028. We stated that this proposed timeline would allow State Exchanges to establish the operational infrastructure and baseline processes to support the SEIPM, such as conducting comprehensive system assessments to identify data collection and reporting capabilities; developing or modifying existing information systems to capture and transmit the required the SEIPM data elements; establishing internal policies and procedures for data validation and quality assurance; training staff on the SEIPM requirements and reporting protocols; and conducting testing and validation of new systems and processes before the effective date. Additionally, we noted that the foundational framework established through IPPTA would have provided State Exchanges with sufficient experience and understanding of their data capabilities and measurement processes to support the transition to SEIPM by January 1, 2027. Any technical adjustments, data collection refinements, or procedural clarifications identified during the IPPTA implementation could be incorporated into the SEIPM through sub-regulatory guidance, allowing for improvements without requiring additional rulemaking or timeline extensions. State Exchanges in the first year of operation would undergo the preparation phase proposed in § 155.1640 and would begin the Measurement Year in 2028 for PY 2027.
( printed page 29654)
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1605 below.
Comment:
Many commenters stated that the proposed January 1, 2027 applicability date is premature and recommended delaying implementation until 2028 or later. Some commenters noted that IPPTA is ongoing, that key technical and operational questions remain outstanding, and that State Exchanges require additional time to prepare. Several commenters requested delaying implementation until after completion of IPPTA and receipt of final results, and indicated that additional time would be needed to incorporate lessons learned and implement necessary system or process changes. Some commenters stated concerns that the delay in issuance of the Proposed Rule and subsequent Final Rule would give State Exchanges less than a year to interpret and prepare data requirements, which would not provide sufficient time to prepare for SEIPM.
Some commenters requested phased implementation approaches, including delaying initial reporting or gradually increasing program scope. Commenters further noted that State Exchanges may be undergoing significant system transitions or modernization efforts and may be simultaneously implementing other Federal eligibility and enrollment requirements in 2027 and 2028 such as those required under the Working Families Tax Cut (WFTC) legislation, which may impact Exchange operational readiness. Some commenters also stated concern that SEIPM implementation during 2027 may overwhelm Exchanges' operational readiness due to the system changes required under the WFTC legislation.
Several commenters noted that they had not yet received IPPTA results and therefore could not fully assess the operational impact of SEIPM and urged HHS to delay implementation and allow State Exchanges to provide additional feedback on operational feasibility.
Response:
We are not adopting the recommendation to delay implementation. We acknowledge commenters' concerns regarding implementation timing, including recommendations to delay implementation until after completion of IPPTA, to allow additional time to incorporate lessons learned, and to adopt phased implementation approaches. We also recognize that some State Exchanges are undergoing significant system transitions or modernization efforts and may be implementing other Federal and State policy changes that could affect operational readiness. We further acknowledge that some State Exchanges have not yet received final IPPTA results and may require additional time to evaluate findings and assess the operational impact of SEIPM.
Nevertheless, we continue to believe that the January 1, 2027 applicability date will provide sufficient time for State Exchanges to prepare, particularly in light of experience gained through IPPTA and an approach in SEIPM to allow a flexible form of data submission which will reduce the State burden. While IPPTA will continue through 2026, it has already generated substantial operational insight into data submission, validation, and review processes, which has informed the development of SEIPM. Although IPPTA is ongoing, we believe the insights gained to date provide a sufficient foundation to proceed with implementation, and additional refinements can be incorporated as the program evolves.
The timing for State Exchanges to begin the submission of the universe data that is described in § 155.1615(b)(2) is planned to begin in March 2027. This will be a summary set of information that, while lengthy in volume, would not require intensive query development to produce. The timing for the State Exchanges to begin the submission of the tax household data is planned to begin in April 2027. This will be the detailed set of data specific to the selected sample that we will use to conduct the review. We note this timeline to point out that although formal implementation begins in January 2027, State Exchanges have a buffer of several additional months to prepare for the practical requirements which will not start until March 2027 and would not expand until April 2027.
Importantly, delaying implementation would extend the period during which HHS lacks a comprehensive and statistically valid improper payment measurement for APTC administered by State Exchanges. Under the PIIA, Federal agencies are required not only to identify programs susceptible to significant improper payments, but also to produce and report improper payment estimates on an ongoing, annual basis. At present, HHS fulfills this requirement for APTC administered through the Federally-facilitated Exchange but does not have a corresponding measurement for State Exchanges.
Further delay would therefore postpone HHS' ability to fully meet its statutory obligations to measure and report improper payments across the entirety of the APTC program. We believe it is appropriate to proceed with implementation once sufficient foundational testing has occurred, rather than waiting for all potential refinements to be resolved, particularly where additional operational details can be addressed through sub-regulatory guidance. Accordingly, we are finalizing § 155.1605 as proposed. We will continue to consider interested party feedback and operational experience during implementation and will provide additional guidance and support to State Exchanges, as appropriate, to facilitate readiness.
c. Definitions (§ 155.1610)
In the 2027 Payment Notice proposed rule, we proposed to add § 155.1610 to codify the following definitions that would be used in this subpart that are specific to SEIPM and key to understanding its processes and procedures:
Annual Program Schedule
would mean the document issued by HHS to each State Exchange that would prescribe the dates by which key SEIPM milestones must be met.
Administrative Appeal
would mean the process by which a State Exchange may request HHS to review and reconsider a Difference Resolution Decision. The appeal would be the second and final level for a State Exchange to contest findings of error or improper payment as it relates to APTC.
Administrative Appeal Decision
would mean the HHS final appeal decision resulting from a State Exchange's request for an appeal of one or more error or improper payment findings that are documented in a Sampled Unit Assessment Package.
Corrective Action Plan
(
CAP) would mean the plan a State Exchange develops to correct errors resulting in improper payments identified through SEIPM.
Difference Resolution
would mean the process by which a State Exchange may initially request HHS to reconsider one or more error or improper payment findings documented in a Sampled Unit Assessment Package. The Difference Resolution would be the first level of review.
Difference Resolution Decision
would mean the HHS decision resulting from a State Exchange's request for a Difference Resolution of one or more
( printed page 29655)
findings that are documented in a Sampled Unit Assessment Package.
Error
would mean a finding by HHS that a State Exchange did not correctly apply a requirement of subparts D and E of this part related to: (1) eligibility for, and enrollment in, a QHP; (2) eligibility for APTC, and calculated amount of APTC; (3) redeterminations of eligibility during a plan year; (4) eligibility redeterminations for the purposes of re-enrollment.
Measurement Year
would mean the calendar year in which the processes described in § 155.1625 would be initiated. The Measurement Year immediately follows the plan year and would be the second year of the SEIPM Cycle.
Reporting Year
would mean the calendar year in which HHS would report the improper payment rate for State Exchanges as required under § 155.1625(c), following completion of the measurement processes for the applicable plan year. The Reporting Year would immediately follow the Measurement Year and would be the last year of the SEIPM Cycle.
Sampled Unit Assessment Package
would mean the collection of findings and supporting documentation that HHS would prepare in order to record errors at the tax household level using the process described in § 155.1625.
State Exchange Improper Payment Measurement
or
SEIPM
would mean the process by which HHS would estimate improper payments of APTC that are administered by State Exchanges as required under the PIIA, which would include a review of a State Exchange's determinations regarding (1) eligibility for and enrollment in a QHP; (2) eligibility for APTC, and calculated amount of APTC; (3) redeterminations of eligibility determinations during a plan year; (4) eligibility redeterminations for purposes of re-enrollment.
SEIPM Cycle
would mean the 3-year period consisting of the plan year, Measurement Year, and Reporting Year during which the complete APTC-related improper payment measurement and reporting processes would occur.
Tax household
would mean the applicant, the applicant's spouse if the applicant is married and files a joint return, and all individuals who are dependents of the applicant or spouse as defined in 26 U.S.C. 152.
We sought comment on these proposals.
We did not receive any comments in response to the proposed § 155.1610. For the reasons outlined in the proposed rule, we are finalizing this policy as proposed.
d. Information Submission (§ 155.1615)
We proposed to add § 155.1615 to specify what information State Exchanges would be required to submit under the SEIPM program. We noted that the collection of such information would be necessary to allow HHS to produce a statistically valid estimate of improper payments of APTC. In the proposed rule, we stated that the general framework of this proposed provision would be that the information submission would consist of three parts: (1) the program documentation that would be used to inform the review criteria; (2) the universe, which would be a summary listing of the tax households that received APTC payments for the respective plan year, from which HHS would select a random sample; (3) tax household data which would be the detailed level of data for each sampled tax household necessary for making a determination as to whether each APTC payment was proper or improper.
At § 155.1615(a), we proposed that HHS would issue an Annual Program Schedule to all State Exchanges no later than January 5th of the Measurement Year. We proposed that the Annual Program Schedule would specify the dates by which all the proposed information required under this section would be due to HHS. This timeline would ensure that State Exchanges receive clear guidance and sufficient advance notice of their submission requirements at the beginning of each Measurement Year, enabling State Exchanges to plan and allocate appropriate resources for compliance with the program's data collection and documentation requirements.
At § 155.1615(b), we proposed that, on an annual basis, each State Exchange would be required to submit or make available to HHS the information specified in paragraphs (b)(1) through (b)(3).
At § 155.1615(b)(1), we proposed that each State Exchange would be required to submit or make available to HHS program documentation that would consist of policy, operational, and technical documentation concerning business rules and APTC calculations that pertain to enrollment and eligibility processes of the State Exchange, as well as information that describes the data system architecture of the State Exchange such as entity relationship diagrams and data dictionaries. We noted that additional parameters for the information described would be communicated in sub-regulatory guidance. We further stated that the program documentation would be essential for establishing the improper payment measurement framework for each State Exchange because it would enable us to assess whether the State Exchange's policies and procedures align with Federal requirements and would be used to develop State-specific review criteria that reflect each State Exchange's unique operational framework.
We proposed at § 155.1615(b)(2) that a State Exchange would be required to submit or make available to HHS the universe of data from which HHS would draw the sample. That universe would, for the plan year being reviewed, consist of a listing of the population of tax households that have associated QHP enrollments and payments of APTC. We proposed that for each tax household within the universe, the State Exchange would be required to submit or make available to HHS the following information: (1) Exchange assigned policy identifier; (2) tax household grouping identifier; (3) SSN inconsistency indicator; (4) citizenship inconsistency indicator; (5) lawful presence inconsistency indicator; (6) annual income inconsistency indicator; (7) non-employer sponsored minimum essential coverage inconsistency indicator; (8) employer sponsored minimum essential coverage inconsistency indicator; (9) incarceration inconsistency indicator; (10) residency inconsistency indicator; (11) number of tax household members; and (12) APTC amount paid over the duration of the plan year. The inconsistency indicators would be a data value for each tax household identifying the presence or number of data match inconsistencies of the specified type. As an example, for the first tax household in the universe, if the data within the State Exchange established that the consumer's attested citizenship status did not match the source of record to which the Exchange is required to verify citizenship status, the citizenship inconsistency indicator would be populated to show that an inconsistency existed for that tax household.
In the 2027 Payment Notice proposed rule, we noted that statistical validity requires that the sample be drawn from a comprehensive and accurately defined population to ensure that the resulting estimates are representative of the entire APTC program within each State Exchange. We stated that this provision would be necessary because without access to the complete universe of tax households having QHP enrollments and APTC payments, we would be unable to establish sampling strata or to calculate the sampling weights that
( printed page 29656)
would inform the aggregate improper payment rate. Additionally, information about eligibility verification inconsistencies within the universe would allow for risk-based stratification, ensuring that tax households with recorded inconsistencies would appropriately be represented in the sample to improve the precision and accuracy of error rate calculations. For instance, the improper payment risk may be higher in tax households with recorded inconsistencies because it would trigger additional required enrollment and eligibility verification processes that State Exchanges would need to conduct manually, leaving them susceptible to human error.
We stated that the total APTC payment amounts for each tax household in the universe would be necessary to calculate proper monetary weights for the improper payment estimates, ensuring that the financial impact of errors would be accurately reflected in the final statistics. This comprehensive approach would enable HHS to produce improper payment estimates meeting the requirements of PIIA.
At § 155.1615(b)(3), we proposed that a State Exchange would be required to submit or make available to HHS tax household data for each sampled tax household. The tax household data would consist of the comprehensive information that is necessary for HHS to use in conducting the processes described at § 155.1625.
At § 155.1615(b)(3)(i), we proposed that State Exchanges would be required to submit or make available to HHS, for each sampled tax household, information pertaining to the calculation of the APTC benefits paid, including monthly enrollment premium amounts, monthly APTC payment amounts, monthly Second Lowest Cost Silver Plan Premium amounts, and the amount of each monthly premium that is attributable to EHB. We noted that this information would be essential for us to verify the accuracy of APTC calculations and ensure that APTC were computed correctly based on the applicable benchmark plan and EHB requirements. We proposed at § 155.1615(b)(3)(ii) that State Exchanges would be required to submit or make available to HHS enrollment information that would include information relevant to dates and amounts of effectuation payments, premium payment amounts, and policy start and end dates. This enrollment data would enable HHS to confirm that APTC payments were made for valid coverage periods and that the timing and amounts of payments align with policy effectuation and premium payment requirements. We further proposed, at § 155.1615(b)(3)(iii), that State Exchanges would be required to submit or make available to HHS information relevant to the determination of eligibility for an SEP, where applicable, which would include information collected by the State Exchange about consumer attestations and representations regarding SEP eligibility criteria, copies of documentary evidence submitted by applicants, electronic verification information, and timing information. We noted that this SEP-related information would allow HHS to assess whether APTC payments were appropriately authorized during SEPs and whether proper verification procedures were followed to confirm SEP eligibility.
At § 155.1615(b)(3)(iv), we proposed that State Exchanges would be required to submit or make available to HHS information about the timing of QHP certification or approval, the coverage area of the associated QHP, and the timing of any QHP decertification or suppression. In the proposed rule, we stated that this QHP certification information would be necessary to verify that APTC payments were made only for QHPs that were properly certified and available in the consumer's coverage area during the relevant time periods.
At § 155.1615(b)(3)(v), we proposed that, to the extent applicable, for each person who is included in the APTC payment calculation, the State Exchange would submit or make available to HHS: (A) information collected by the State Exchange about consumer attestations regarding QHP and APTC eligibility factors and demographic information relevant to initial QHP enrollment and eligibility; (B) APTC eligibility and payment determinations, including evidence of required data verifications, and which could also include the electronic source consulted, the timing of required verifications, and the results of the verification; (C) information relevant to QHP and APTC manual eligibility verifications and the resolution of electronic verification inconsistencies, which could include copies of documentary evidence submitted by QHP enrollees, the timing of submissions, the timing of adjudication, and information about good faith extensions; and (D) information relevant to QHP and APTC eligibility redeterminations, such as information about automatic annual redeterminations, the timing and results of periodic examinations of data sources, and policy or application changes initiated by the consumer and resultant electronic or manual eligibility verifications. We stated in the proposed rule that this comprehensive individual-level information would enable HHS to reconstruct and validate the complete eligibility determination process for each household member, ensuring that APTC payments were based on accurate demographic information and proper verification procedures, and were made through appropriate eligibility determinations and redeterminations.
In the 2027 Payment Notice proposed rule, we stated that these data elements have been proven effective through their use in the FFE improper payment measurement program, where they have enabled reliable assessment of APTC payment accuracy and identification of root causes of improper payments, and demonstrated they provide the necessary information to conduct comprehensive improper payment reviews. Additionally, through IPPTA, we noted that we have completed the collection of this data for the first cohort of eight State Exchanges for 10 or more sampled tax households. In making the transition from IPPTA to SEIPM, we believe that each State Exchange would be able to use the automation developed during IPPTA to scale the process for submitting data for a larger number of samples. We sought comments on whether there were additional data elements that would be required under this section to support accurate improper payment measurement, or whether any of the proposed data categories would present operational challenges for State Exchanges. We also solicited comments on alternative data submission mechanisms that could streamline the process while maintaining data security and integrity, including comments on the feasibility of automated data transmission methods, preferred file formats, or technical specifications that would facilitate efficient data exchange between State Exchanges and HHS.
At § 155.1615(b)(3)(vi), we proposed that the State Exchange would submit or make available to HHS any consumer submitted documents that were used to establish new or continued eligibility for enrollment in a QHP and APTC.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1615 below.
( printed page 29657)
Comment:
Many commenters stated that the SEIPM information submission requirements are overly burdensome, operationally complex, and would require significant manual effort, including data extraction, transformation, validation, and reconciliation. Commenters noted that State Exchange systems are not designed around a uniform Federal reporting format and that the proposal lacks sufficient specificity regarding final data formats, timelines, and technical requirements to allow State Exchanges to fully assess feasibility and cost. Commenters also noted that certain required information elements such as documentary evidence may not be captured in existing State Exchange systems and therefore may require significant manual retrieval.
Several commenters further stated concern regarding the scope and granularity of required data elements, including the submission of detailed consumer-level documentation, and noted that these requirements may not be readily automated in SEIPM. Some commenters also requested that SEIPM leverage existing data elements within State Exchange systems, where feasible, to reduce the need for system modifications and manual data transformation and requested additional technical specifications to support implementation planning.
Response:
We appreciate these comments and recognize that the information submission requirements under § 155.1615 are comprehensive and may require operational effort, particularly given variation in State Exchange data systems. We acknowledge commenters' concerns regarding the level of effort required to retrieve documentation and prepare case-level submissions, including that certain information may not be readily available within existing systems and may require manual retrieval. We also recognize concerns regarding the scope and granularity of required data elements, including the submission of detailed consumer-level documentation, as well as commenters' recommendations to leverage existing data elements within State systems and align requirements with current data structures where feasible.
In addition, we acknowledge requests for greater clarity regarding technical specifications, including data definitions, reporting formats, and submission requirements. However, we continue to maintain that the proposed data elements are necessary to support a statistically valid and reliable improper payment estimate, consistent with requirements under the PIIA and OMB Circular No. A-123.
Specifically, the collection of program documentation, a complete universe of tax households receiving APTC, and detailed case-level data for sampled households is essential to support valid sampling, accurate eligibility and payment review, and proper extrapolation of findings to the full population. Without this information, HHS would be unable to construct sampling frames, apply appropriate statistical weighting, or determine whether APTC payments were made in accordance with Federal requirements. As a result, HHS would be unable to produce improper payment estimates that meet Federal standards for accuracy and reliability.
We also note that this framework is consistent with that used in the Federally-facilitated Exchange improper payment measurement program and has been tested through IPPTA, where it has proven effective to support the comprehensive review of eligibility determinations and APTC calculations. While we acknowledge that State Exchanges operate different systems, we believe the proposed framework appropriately reflects the minimum data necessary to conduct improper payment measurement across all Exchange types.
With respect to commenters' concerns regarding operational specificity, we note that the regulation establishes the scope of required information, while detailed technical specifications, submission formats, and operational instructions will be provided through sub-regulatory guidance. This approach allows HHS to adapt technical requirements as needed while maintaining a consistent regulatory framework. Accordingly, we are finalizing § 155.1615 as proposed.
Comment:
Commenters stated concern that differences in State Exchange data architecture make standardized data submission difficult and may require significant manual effort, including mapping State data elements to Federal reporting requirements. Some commenters stated concern that HHS underestimated the SEIPM complexity which will require layers of historical data across multiple households and the administrative and financial burden it will place on State Exchanges. Some commenters also expressed concern that system modifications and additional staffing would be required to produce the information required for SEIPM. One commenter stated that the proposed alternative data collection solution will still require significant mapping, validation, and reconciliation.
Response:
We acknowledge that State Exchanges maintain diverse system architectures and that mapping data elements to a common framework may require effort. For this reason, we proposed to allow flexibility in how data may be submitted, including the ability for State Exchanges to provide data in native formats without conforming to a standard structure. We believe this approach appropriately balances the need for standardized measurement with operational feasibility.
We acknowledge that implementation of SEIPM may require States to allocate resources to support data submission and program participation. However, we continue to believe that these requirements are necessary to support HHS' statutory obligations under PIIA and to ensure accurate measurement of improper payments. The data descriptions specified in § 155.1615 are designed to capture the information required to evaluate eligibility determinations, verify APTC calculations, and assess compliance with Federal requirements. We do not believe that the collection of information needed to support measurement would necessitate system modifications. Accordingly, we are finalizing this provision as proposed.
Comment:
Several commenters requested clarification regarding whether any required data elements would constitute Federal Tax Information (FTI) and raised concerns about associated compliance and security implications.
Response:
We acknowledge the importance of appropriately safeguarding FTI and other sensitive information. We will ensure that all data collection, transmission, and storage under SEIPM comply with applicable Federal privacy and security requirements, including those governing FTI where applicable. We intend to provide additional clarification regarding data handling expectations through sub-regulatory guidance. Accordingly, we are finalizing § 155.1615 as proposed.
Comment:
One commenter stated concern that documentation requests issued near renewal deadlines or coverage effective dates may create consumer and assister uncertainty and therefore impact coverage stability.
Response:
We appreciate this comment and recognize the importance of advance planning with consideration to timeframes that impact open enrollment and/or coverage stability. We believe that the Annual Schedule and release of additional sub-regulatory guidance will provide State Exchanges
( printed page 29658)
with the necessary timelines and allow for preparation so that Exchange core operations are not negatively affected.
Comment:
Some commenters requested detailed technical specifications such as data submission definitions, data collection formats, and timelines. A commenter stated concern that the proposed timing for issuance of the Annual Program Schedule, no later than January 5 of the Measurement Year, would not provide sufficient lead time for State Exchanges to prepare for submission requirements.
Response:
We appreciate these comments and recognize the importance of advance planning. We believe that issuance of the Annual Program Schedule at the beginning of the Measurement Year provides timely and consistent communication of program requirements. In addition, we will provide State Exchanges with ongoing technical assistance leading up to and during the SEIPM program, which will support overall preparation. We also intend to provide supplemental information, where appropriate, through sub-regulatory guidance. Therefore, we are finalizing this provision as proposed.
e. Sampling Procedures (§ 155.1620)
We proposed to add § 155.1620 to address the sampling procedures. At § 155.1620(a), we proposed that at the beginning of each calendar year, HHS would calculate a sample size in aggregate across all State Exchanges. We stated that the sampling methodology would be designed to achieve two complementary objectives: produce a highly precise aggregate estimate for all State Exchanges and generate individual State Exchange estimates for program management purposes. While some individual State Exchange estimates might have wider confidence intervals than others due to smaller sample sizes, they would meet minimum statistical validity thresholds and provide valuable insights for State-specific program improvements and oversight activities.
We proposed that we would aggregate the estimated dollar amounts of improper payments from each State Exchange to calculate a total estimated amount of improper payments for all participating State Exchanges. We noted that this aggregation process would mathematically combine the individual State Exchange improper payment estimates to produce a comprehensive national estimate. The aggregated estimate would be weighted by State Exchange size, such that a State with $5 billion in APTC would be weighted more heavily in the aggregate State Exchange improper payment rate than a State with $1 billion in APTC. We stated that this weighting approach would ensure that the aggregate State Exchange improper payment rate would accurately reflect the relative financial impact of each State Exchange's improper payment performance on the overall APTC program.
In the proposed rule, we stated that this dual-purpose sampling approach would balance statistical rigor with practical program management needs, ensuring that HHS could meet Federal reporting requirements for precise program level estimates while providing State Exchanges with actionable data for program improvement efforts. The methodology would recognize that perfect precision at the individual State Exchange level would require prohibitively large sample sizes, while the primary statutory requirement is for accurate improper payment measurement and reporting at a program level.
At § 155.1620(a)(1), we proposed that the sample size would be calculated to estimate an improper payment rate. That rate would be estimated across all Exchanges using Generally Accepted Accounting Principles (GAAP).
At § 155.1620(a)(2), we proposed to develop sample sizes specific to each State Exchange, which would take into consideration several factors in determining each State Exchange's sample size for the current SEIPM cycle. We provided that the first factor, at § 155.1620(a)(2)(i), would be overall APTC expenditures associated with the State Exchange; higher APTC expenditures would generally warrant larger sample sizes as they would represent greater financial risk to the Federal Government and have more significant impact on aggregate national improper payment estimates. The relative amount of a State Exchange's APTC payments would amplify the importance of accurate measurement. For example, if a single State Exchange were to account for 20 percent of overall APTC payments made across all State Exchanges, any improper payments within that State would have a proportionally larger impact on the aggregate national improper payment rate. The large share of total APTC payments would necessitate a larger sample size to meet the statistical precision goals and also would not introduce excessive uncertainty into the national aggregate estimate.
At § 155.1620(a)(2)(ii), we proposed to take into consideration a second factor, State-level precision goals for the current SEIPM cycle. We noted that precision goals would establish the acceptable margin of error for improper payment rate estimates at the State level. We proposed that we would set precision targets that balance statistical reliability with operational feasibility, taking into account factors such as State-specific APTC volumes, available resources, and the need for meaningful measurement. We proposed that precision goals could vary by State based on Exchange size, with larger Exchanges held to tighter precision standards due to their greater impact on aggregate national estimates. These precision goals would ensure that State-specific improper payment rates would be statistically meaningful and could support targeted corrective actions while balancing measurement accuracy with resource constraints.
At § 155.1620(a)(2)(iii), we proposed to consider a third factor, the improper payment rate from the State Exchange's previous SEIPM cycle. State Exchanges that are measured as having higher improper payment rates could require larger sample sizes to achieve the same level of statistical precision and confidence as State Exchanges that are measured as having lower improper payment rates. Additionally, we noted that State Exchanges that demonstrate high variability in their previous cycle measurements could need increased sampling to establish more reliable baseline estimates. Conversely, State Exchanges with consistently low and stable improper payment rates could support smaller sample sizes to maintain adequate precision and confidence, which would allow for efficient resource allocation across the SEIPM program.
At § 155.1620(a)(3), we proposed that we would establish minimum and maximum sample sizes to ensure statistical validity while maintaining operational feasibility across State Exchanges of varying sizes. While the sampling methodology design would produce statistically valid improper payment estimates at both the aggregate State Exchange level and individual State Exchange levels, we recognized that the precision of improper payment estimates at the State Exchange level would vary based on State Exchange size and corresponding sample sizes. State Exchanges with smaller APTC populations may have smaller sample sizes resulting in wider confidence intervals and higher margins of error for their individual estimates. Despite these precision limitations, individual State Exchange estimates would meet minimum statistical validity thresholds and would provide meaningful data for program oversight and improvement purposes. We noted that SEIPM's primary focus would remain producing
( printed page 29659)
a precise and reliable estimate for all State Exchanges, where individual State Exchange results would provide State-specific insights within the constraints of their respective sample sizes.
At § 155.1620(b), we outlined proposed sample selection procedures. We proposed that, on an annual basis, HHS would select random samples of tax households from the data provided by each State Exchange as described in § 155.1615(b)(2). We proposed to use the tax household as the sampling unit because a tax household encompasses all individuals whose income and circumstances are considered together for APTC purposes, which would make it the most appropriate and meaningful unit for measuring payment accuracy.
At § 155.1620(c), we outlined proposed State Exchange coordination and notification procedures that would be necessary to support SEIPM. We proposed at § 155.1620(c)(1) that, following receipt of the universe data from State Exchanges as described in § 155.1615(b)(2), HHS would notify each State Exchange of the specific records selected for review. Such notification would include: (i) the total number of sampled tax households selected for the State Exchange; (ii) a unique identifier for each sampled tax household; and (iii) any specific instructions or requirements needed to facilitate HHS' review of the sampled records. We stated that this information would be intended to give State Exchanges the information necessary to provide the documentation required. This process would help ensure that State Exchanges have clear notification of the specific tax households that have been sampled. This would also help foster efficiencies and accurate submission of the tax household data required under § 155.1615(a)(3).
In the proposed rule, we noted that we would protect all data exchanged during the SEIPM process in accordance with the Federal Information Security Modernization Act of 2014 (FISMA), which mandates comprehensive security controls for Federal information systems, and the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy and Security Rules (45 CFR parts 160 and 164), which require administrative, physical, and technical safeguards to protect the privacy of protected health information and to ensure the confidentiality, integrity, and availability of all electronic protected health information. Additionally, all data transmissions would utilize encryption protocols compliant with National Institute of Standards and Technology (NIST) Special Publication 800-53 security controls and our Acceptable Risk Safeguards (ARS) framework, with access restricted to authorized personnel only through role-based access controls and continuous monitoring as required under the Federal Information Security Management Act.
At § 155.1620(c)(2), we proposed that HHS would provide the sampled records notification described in paragraph (c)(1) of this section no later than 60 calendar days after receipt of the universe data from all State Exchanges. This 60-day timeframe would ensure that HHS would have sufficient time to complete the sampling process across all participating State Exchanges. We stated that the proposed timeline would account for the complexity of coordinating sampling activities across multiple State Exchanges with varying data submission schedules and allow for quality assurance review of the sampling methodology before notification. This approach would balance the need for thorough sampling coordination with the operational requirements for timely completion of improper payment measurement processes.
At § 155.1620(c)(3), we proposed to establish procedures for extending the sampling notification timeline when unforeseen circumstances would warrant additional time for HHS to complete the sampling process. We proposed at § 155.1620(c)(3)(i) that HHS could extend the 60-day timeline specified in paragraph (c)(2) of this section under three specific circumstances: when technical issues would prevent completion of the sampling process within the standard timeframe; when data quality issues would require additional coordination with State Exchanges before sampling can be completed; or when other circumstances beyond HHS' control would necessitate additional time to ensure accurate sampling methodology.
We proposed at § 155.1620(c)(3)(ii) to establish notification and transparency requirements when HHS would determine an extension would be necessary. Under paragraph (c)(3)(ii), HHS would: (A) notify all affected State Exchanges in writing of the extension and the revised notification date; (B) provide the reason for the extension; and (C) confirm the impact, if any, on subsequent SEIPM cycle timelines. In the proposed rule, we stated that this provision would reflect that unforeseen technical or operational challenges potentially could arise when coordinating complex sampling across multiple State Exchanges. Where not properly addressed, such challenges could compromise the sampling methodology accuracy or completeness, so this provision would balance the need for timely program milestone progress with the requirement for statistically sound sampling procedures. By limiting extensions to specific, defined circumstances and requiring transparent communication with State Exchanges, this approach would maintain accountability while providing necessary operational flexibility to ensure the integrity of the SEIPM measurement process.
In the proposed rule, we stated that the notification requirements proposed at § 155.1620(c)(3)(ii)(A) through (C) would also ensure that State Exchanges would remain informed of any timeline adjustments and could plan for the case documentation preparation activities. This transparency would support the collaborative nature of the SEIPM program while maintaining predictable timelines for all participating parties.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1620 below.
Comment:
Some commenters stated concern regarding the methodology associated with sampling requirements and stated that the factors used to determine sample size would not provide sufficient predictability for State Exchanges to estimate workload and resource needs. Commenters also noted that larger sample sizes necessary to achieve statistical precision may significantly increase workload, particularly where manual processes are required, and that case complexity may further affect the level of effort required for sample review. Some commenters requested providing greater predictability in sample size or adopting phased or incremental increases in sample size to support operational planning.
Response:
We appreciate these comments and acknowledge that sample sizes may vary from between 50 and 250 across State Exchanges. This variability is necessary to ensure that improper payment estimates meet applicable standards for statistical validity and precision. As described in § 155.1620(a)(2), sample sizes are determined based on factors such as APTC volume, precision goals, and prior improper payment rates, all of which are standard considerations in developing statistically sound sampling
( printed page 29660)
methodologies. We acknowledge commenters' concerns regarding the relationship between sample size and operational feasibility, including the potential impact of larger sample sizes on workload, particularly where manual processes are required. We also recognize that variation in case complexity may affect the level of effort required for sample review, as well as requests for greater predictability and phased approaches to sampling.
We also note that one commenter appeared to assume that the SEIPM sampling approach is designed to achieve a specific margin of error at the individual State Exchange level, such as a margin of error of less than 5 percent. This is not the intent of the SEIPM sampling design. As described in § 155.1620(a), the sampling methodology is designed to produce a precise estimate at the aggregate program level across all State Exchanges, consistent with requirements under the Payment Integrity Information Act of 2019 (PIIA).
While State-specific estimates will be produced for program management and oversight purposes, they are not required to meet the same precision thresholds as the aggregate estimate. As a result, individual State Exchange sample sizes may vary and may not be designed to achieve a specific margin of error at the State level. This approach allows us to balance statistical rigor with operational feasibility across State Exchanges of varying sizes.
While we recognize that variability may present operational planning challenges, establishing fixed or highly predictable sample sizes could undermine the reliability of the resulting estimates. We intend to provide additional operational detail, including expectations regarding sampling, through sub-regulatory guidance to support State Exchange planning. Accordingly, we are finalizing § 155.1620 as proposed.
Comment:
One commenter stated concern that the proposed sampling methodology, including the use of inconsistency indicators for stratification, could result in samples that overrepresent higher-risk cases and therefore not reflect overall program performance. One commenter requested HHS to consider APTC enrollment instead of APTC paid to calculate sample sizes across State Exchanges as varying incomes and variance in plan premiums may skew sample sizes. Another commenter requested that HHS prioritize aggregate reporting structures instead of application-level data.
Response:
We do not agree that the proposed methodology introduces bias. Stratified sampling is a widely accepted statistical approach used to improve the precision and reliability of estimates, particularly in programs where risk is not uniformly distributed. The use of inconsistency indicators as one of several stratification factors is intended to ensure that the sample appropriately represents variation within the population and supports accurate estimation of improper payment rates.
We also acknowledge commenters' concerns regarding the use of APTC expenditures as a factor in determining sample sizes. As described in § 155.1620, APTC payment amounts are used to appropriately weigh the financial impact of improper payments and ensure that estimates accurately reflect the magnitude of Federal expenditures. While alternative approaches, such as using enrollment counts, were suggested, we believe that incorporating APTC payment amounts is necessary to produce statistically valid estimates that reflect the financial risk associated with improper payments across State Exchanges.
We further acknowledge commenters' requests for additional State-level detail in reporting. As described in § 155.1625(c), HHS will provide State Exchanges with State-specific improper payment reports to support program oversight and improvement, while aggregated reporting will be used to meet Federal reporting requirements under PIIA.
The sampling methodology, consistent with the PIIA and OMB Circular No. A-123 guidance, is designed to produce statistically valid estimates representative of the full population at the aggregate program level. Accordingly, we are finalizing § 155.1620 as proposed.
Comment:
One commenter stated that the FFE improper payment measurement methodology has an insufficient sample size and imprecise margin of error and requested HHS to adopt a statistical methodology similar to the GAO.
Response:
We appreciate this comment but do not agree that the FFE improper payment measurement methodology is insufficient. The FFE methodology is designed in accordance with OMB Circular No. A-123 guidance, which establishes Federal standards for improper payment measurement, including requirements related to statistical validity, precision, and confidence intervals.
We acknowledge the commenter's interest in alternative statistical approaches; however, the methodology used for the FFE—and proposed for SEIPM—reflects established Federal standards for improper payment estimation and is designed to produce reliable and defensible results at the program level.
Accordingly, we are not adopting an alternative statistical methodology and are finalizing this approach as proposed.
f. Determining Payment Errors (§ 155.1625)
In the proposed rule, § 155.1625 outlined the process by which HHS would determine payment errors. At § 155.1625(a), we proposed procedures for HHS' review of records obtained through SEIPM and identification of payment errors from such records. We proposed at § 155.1625(a)(1) that HHS would, for each sampled record, conduct a comprehensive review using standardized review criteria designed by HHS. This approach would ensure consistency in methodology across all participating State Exchanges while accommodating necessary variations in review procedures where State Exchanges have effectuated State-specific operational approaches. We stated that we would design the criteria to minimize reviewer variability while maintaining the flexibility needed to address State-specific operational differences for which Federal regulations allow. The review criteria would be established using the requirements described in this part in conjunction with the program documentation that would be submitted by each State Exchange. We would make available a general overview of the review methodology on the CMS website.
At § 155.1625(a)(2), we proposed to conduct reviews using the tax household information provided under § 155.1615(b)(3), including any relevant consumer-submitted documents that would be gathered by the State Exchange as part of the enrollment process and provided to HHS. We noted that this approach would ensure that HHS reviews would be based on the same information that was available to State Exchanges at the time of their original APTC-related determinations.
At § 155.1625(a)(3), we proposed that the review would identify whether the State Exchange made any errors related to the following resulting in improper payment of APTC: (i) enrolling or re-enrolling a consumer into a QHP for which APTC was paid; (ii) consumer eligibility for APTC being paid on their behalf; (iii) calculating the APTC amount that was paid on the consumer's behalf; and (iv) taking required actions upon changes to a consumer's application that would affect APTC-related eligibility or payment amount.
( printed page 29661)
We stated in the proposed rule that this approach would ensure that HHS could identify and measure all types of improper payments related to APTC, providing a complete assessment of payment accuracy to meet Federal improper payment measurement requirements under the PIIA while supporting program integrity objectives.
At § 155.1625(a)(4), we proposed to apply consistent review standards based on the APTC-related determination requirements established in 45 CFR part 155, subparts D and E, and other applicable provisions of part 155. By anchoring review standards in existing regulations, we would ensure that the State Exchange's performance would be evaluated against the same statutory and regulatory framework that governs their APTC-related determinations. This regulatory framework would ensure that any identified errors would be based on clear violations of established requirements rather than subjective interpretations of the program's goals.
We proposed at § 155.1625(b) how HHS would evaluate each error to determine an improper payment amount. At § 155.1625(b), we proposed that, for each error identified, we would: (1) calculate the correct APTC amount, based on the requirements of section 36B of the Internal Revenue Code and the applicable implementing regulations; (2) determine an improper APTC payment amount, which is the difference between the amount paid and the correct amount; (3) document the error within a Sampled Unit Assessment Package and provide the Sampled Unit Assessment Package to the State Exchange; and (4) extrapolate the identified improper payments from the sample to estimate the total improper payment amount for the State Exchange's entire universe of APTC payments, using statistically valid methodologies that comply with OMB Circular No. A-123 guidance on improper payment estimation.
At § 155.1625(c), we proposed how HHS would report improper payment rates. We proposed at § 155.1625(c) that HHS would make available to the public in the AFR: (1) an aggregate improper payment rate estimated across the FFE and all State Exchanges; and (2) an aggregate improper payment rate estimated across all State Exchanges, pursuant to 31 U.S.C. 3352(c)(1)(B); and also that HHS would provide to each State Exchange a report that would document the State-specific improper payment rate and error analysis. We stated in the proposed rule that this reporting approach would ensure PIIA compliance while providing State Exchanges with actionable data to improve their program operations and reduce future improper payments. The State-specific reports would facilitate corrective action planning, while the aggregate public reporting would support congressional oversight and public accountability for the overall integrity of the APTC program.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1625 below.
Comment:
Some commenters stated concern that data limitations or operational challenges could result in situations where incomplete or unavailable documentation would lead to findings of improper payments, even where underlying eligibility determinations may have been appropriate. Commenters noted that documentation may not always be readily available within State systems and may require manual retrieval, and expressed concern that complex cases involving multiple eligibility or enrollment changes may increase the likelihood of incomplete documentation being identified during review as errors and/or improper payments. One commenter requested that HHS provide a detailed non-aggregated summary of improper payments by State Exchanges when determining errors for transparency.
Response:
We appreciate these comments. We acknowledge commenters' concerns regarding the availability of documentation and the operational challenges associated with compiling and submitting complex case-level data, particularly where information may need to be retrieved manually or where cases involve multiple eligibility or enrollment changes. We continue to note that the methodology outlined in § 155.1625 appropriately reflects Federal standards for determining improper payments. Under the PIIA and OMB Circular No. A-123, agencies must determine whether payments were made in accordance with applicable statutory and regulatory requirements, based on the information and documentation available to support those determinations.
The SEIPM review process is designed to assess payment accuracy using the same information that was available to the State Exchange at the time of the original eligibility and payment determinations, along with any supporting documentation maintained by the State Exchange. Where sufficient documentation is not available to support that a payment was made in accordance with applicable requirements, the payment may be classified as improper, consistent with Federal improper payment measurement standards. This approach reflects longstanding Federal requirements that determinations be supported by appropriate documentation.
At the same time, we recognize the operational challenges associated with compiling and submitting complex data across diverse State Exchange systems. As discussed in § 155.1615, we are allowing flexibility in data submission approaches, including the ability to submit data in formats that align with State Exchange system architecture where appropriate. We believe this flexibility will help reduce unnecessary burden, improve the accuracy and completeness of submitted data, and support more reliable improper payment determinations.
We also note that the SEIPM process includes opportunities for State Exchanges to provide additional information or clarification through the Difference Resolution and administrative appeal processes prior to finalization of findings. We believe that these processes, including opportunities for clarification and appeal, provide an appropriate balance between ensuring accountability and recognizing operational realities.
We also acknowledge commenters' request for more detailed, non-aggregated reporting of improper payments by State Exchanges. As described in § 155.1625(c), HHS will provide State Exchanges with State-specific improper payment reports to support program oversight and improvement, while aggregated reporting will be used to meet Federal reporting requirements under PIIA. We believe this approach appropriately balances transparency with the need for consistent, program-level reporting. Accordingly, we are finalizing § 155.1625 as proposed.
Comment:
A commenter requested clarification on how certain data will be used, including eligibility verification and consumer demographic information, some commenters requested clarification on FTI data elements and requested that FTI field be removed from data requirements.
Response:
We appreciate this comment and clarify that we will use all data for the purpose of estimating and reporting an improper payment estimate. We also clarify that we will
( printed page 29662)
follow all Federal requirements related to data retention, privacy, and security. We will also follow FTI rules as established by 26 U.S. Code § 6103.
g. Difference Resolution and Administrative Appeal Process (§ 155.1630)
In new § 155.1630, we proposed procedures for Difference Resolution and administrative appeals of SEIPM findings. This section proposed a process that would allow State Exchanges to challenge HHS determinations regarding error findings and associated determinations of improper payments. This comprehensive dispute resolution framework would ensure that State Exchanges receive fair consideration of their challenges to SEIPM findings while maintaining the integrity and efficiency of the improper payment measurement process. The proposed procedures would provide State Exchanges with meaningful opportunities to present evidence and legal arguments, while also supporting HHS' statutory obligations to produce timely and accurate improper payment estimates under PIIA. Additionally, the structured approach would promote consistency in how disputes would be handled across all State Exchanges, while reducing administrative burden and ensuring that legitimate concerns about error classifications or methodological applications would receive appropriate review and consideration.
At § 155.1630(a), we proposed the Difference Resolution process. We proposed at § 155.1630(a)(1) that the State Exchange could make a written Difference Resolution request to HHS in accordance with proposed § 155.1630(c) to dispute HHS' error and improper payment findings within 30 calendar days after the issuance of a Sampled Unit Assessment Package. The proposed 30-day timeframe for State Exchanges to submit written Difference Resolution requests would balance the need to give State Exchanges sufficient time to review the Sampled Unit Assessment Package with the need for administrative efficiency and timely resolution of the SEIPM process.
At § 155.1630(a)(2), we proposed procedures for HHS' review of Difference Resolution requests. We proposed that upon receipt of a Difference Resolution request, HHS would: (i) engage with the State Exchange in a collaborative process to examine the disputed findings and any additional documentation provided by the State Exchange; (ii) evaluate the disputed findings by applying the same protocol used in the original review while considering whether the State Exchange's position was supported by the existing or newly provided evidence; and (iii) prepare the Difference Resolution Decision. We stated that this collaborative approach would ensure that State Exchanges would have a meaningful opportunity to present their perspective and provide additional context that may not have been available during the initial assessment, while maintaining consistency in evaluation standards. The process would balance the need for thorough consideration of State Exchange concerns with administrative efficiency, promoting fair resolution of disputes while preserving the integrity of the SEIPM measurement methodology.
We proposed at § 155.1630(a)(3) that HHS would communicate the Difference Resolution Decision to a State Exchange within 90 calendar days of receiving the written request for a Difference Resolution. The Difference Resolution Decision would include a summary of the analysis and rationale that informed the decision. This timeline would balance the need for thorough review of a State Exchange's dispute with administrative efficiency requirements, and allow sufficient time for comprehensive analysis while ensuring timely resolution.
Proposed § 155.1630(b) would establish an internal agency administrative appeal process for HHS' Difference Resolution Decision. At § 155.1630(b)(1), we proposed that, for a finding that the State Exchange and HHS could not resolve through Difference Resolution, the State Exchange could make a written request for an administrative appeal to HHS in accordance with proposed § 155.1630(c) within 15 business days after the issuance of the Difference Resolution Decision. We noted that we believe the 15 business day timeline for filing an administrative appeal would strike an appropriate balance between providing State Exchanges adequate time to prepare comprehensive administrative appeals while ensuring prompt resolution of disputes and maintaining administrative efficiency. This shorter appeal period, compared to the initial 30-day timeline to request Difference Resolution, would reflect that the basis of the administrative appeal would have been established and well-described during the Difference Resolution phase, and that the State would not be able to submit new evidence or documentation that had not already been submitted during the Difference Resolution process, although it could provide additional context to clarify evidence that had been submitted. We stated that, as a result, we expect that 15 business days would provide State Exchanges with sufficient opportunity to review the Difference Resolution Decision and prepare a focused administrative appeal that would build upon the previously established record. Furthermore, the administrative appeal timeframe would help ensure that the overall SEIPM cycle would remain on schedule, preventing delays that could affect HHS' ability to meet Federal improper payment reporting deadlines and provide timely program oversight.
At § 155.1630(b)(2), we proposed that upon receipt of an administrative appeal request, HHS would (i) assign the administrative appeal request to one or more qualified reviewers who were not part of the State Exchange team; (ii) conduct a comprehensive review of the disputed findings using the administrative record established during the Difference Resolution process; (iii) evaluate the disputed findings by applying the same protocol used in the original review while considering whether the State Exchange's position is supported by the evidence; and (iv) prepare the administrative appeal decision for the completed review based on a preponderance of the evidence. At § 155.1630(b)(3), we proposed that HHS would issue the administrative appeal decision within 90 calendar days of receipt of the written request for administrative appeal. The administrative appeal decision would include a summary of the analysis and rationale that informed the decision.
In the proposed rule, we stated that HHS would utilize internal staff to conduct administrative appeal adjudications under this provision. The agency would assign qualified internal reviewers who possess appropriate expertise in Federal eligibility and payment requirements and who had not been involved in the original review to ensure objectivity in the administrative appeals process. These reviewers would independently review the appeal, without consultation with the individuals who had executed the dispute resolution. This approach would maintain program consistency while providing State Exchanges with an independent review of disputed findings. The internal agency administrative appeal process described in this section would be an administrative review conducted by agency staff, not a judicial proceeding or formal adjudication requiring an Administrative Law Judge.
We stated that the 90-day timeline would provide sufficient opportunity
( printed page 29663)
for thorough analysis of complex eligibility and payment determinations while ensuring timely resolution that would support the overall SEIPM cycle schedule. The requirement to include analysis and rationale in the administrative appeal decision would promote transparency and enable State Exchanges to understand the basis for final determinations, supporting both accountability and potential future process improvements.
We proposed at § 155.1630(c) that all Difference Resolution and appeal requests would be required to contain the following: (1) a clear statement of the specific finding(s) being challenged; (2) all factual and legal bases for filing the request; and (3) evidence directly related to the finding(s), which could include: (i) clarifying information regarding data interpretation; or (ii) legal citations supporting the State Exchange's position. These submission requirements would ensure that HHS would receive sufficient information to conduct meaningful review of disputed findings while enabling State Exchanges to present their strongest arguments and supporting evidence in a structured format that would promote efficient dispute resolution.
We proposed at § 155.1630(d) the treatment of pending Difference Resolution Requests and appeal requests. At § 155.1630(d)(1), for Difference Resolution Requests or administrative appeals resolved in favor of the State Exchange during the current SEIPM cycle, we proposed that: (i) HHS would adjust the affected improper payment rate calculations for the SEIPM cycle; and (ii) updated aggregate rates would be reflected in current cycle reporting. This approach would ensure that corrections identified through the Difference Resolution or appeals process would be incorporated into the current measurement cycle's results, providing the most accurate and complete improper payment estimates for public reporting and program management purposes. We stated that, by adjusting calculations and updating aggregate rates, HHS could maintain the integrity and reliability of SEIPM findings while ensuring that legitimate State Exchange concerns would be reflected in the final reported statistics for the applicable measurement period.
We proposed at § 155.1630(d)(2) provisions for Difference Resolution Requests or administrative appeals resolved in favor of the State Exchange after completion of the SEIPM cycle. At § 155.1630(d)(2), we proposed that, should the decision result in material changes to aggregate rates, HHS would publish amended aggregated improper payment rates in subsequent AFRs or other appropriate public reporting mechanisms as well as notifying affected State Exchanges of any amendments to previously published rates. We noted that, should a decision not result in material changes to aggregate rates, no action would be taken. This framework would ensure that significant corrections identified through post-cycle Difference Resolution Requests or administrative appeals would be incorporated into the public record through amended reporting, maintaining the accuracy and integrity of published improper payment data while avoiding unnecessary administrative burden for minor adjustments that would not materially affect aggregate statistics. The notification requirement for affected State Exchanges would promote transparency and enable States to understand how successful challenges would impact previously published rates, support ongoing program improvement efforts, and maintain the integrity of the SEIPM measurement process.
At § 155.1630(e), we proposed that, for good cause, HHS could extend the timelines for accepting a Difference Resolution request or administrative appeal request or for issuing a Difference Resolution Decision or Administrative Appeal Decision. Good cause would be established for situations including but not limited to: (1) the need for additional technical analysis or consultation with subject matter experts to resolve complex eligibility determination issues; (2) delays in receiving necessary supplemental information or clarification from the State Exchange; (3) the volume or complexity of the dispute requiring additional time to ensure a thorough and accurate decision; or (4) unforeseen circumstances, including system failures, staffing constraints, or other administrative challenges that could materially impact HHS' ability to complete the review. HHS' failure to timely issue a Difference Resolution or Administrative Appeal decision would not indicate an acceptance of the State Exchange's position and would not be a basis to decide in favor of the State Exchange.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1630 below.
Comment:
Several commenters had concerns that the proposed timelines for Difference Resolution and administrative appeals may be insufficient given the volume and complexity of sampled cases. Commenters noted that reviewing findings, retrieving supporting documentation, and preparing submissions may require more time than the proposed timeframes allow, particularly for larger samples or more complex cases. Commenters also requested additional flexibility in the timelines and clearer guidance regarding documentation requirements. Some commenters also requested detailed technical specifications on the Difference Resolution and administrative appeals process.
Response:
We appreciate these comments and acknowledge that the time required to review findings and prepare submissions may vary depending on sample size and case complexity. We recognize that certain cases may require additional time to retrieve documentation or provide clarification.
As described in § 155.1630(e), HHS may extend timelines for Difference Resolution requests or administrative appeals for good cause, including circumstances where additional time is needed to complete technical analysis, obtain supporting documentation, or address complex eligibility determinations. We believe this flexibility appropriately balances the need for thorough review with the need to maintain timely completion of the SEIPM cycle.
We also intend to provide additional guidance, as appropriate, to support State Exchanges in navigating the Difference Resolution and administrative appeal processes. Accordingly, we are finalizing § 155.1630 as proposed.
h. Corrective Action Plan (CAP) (§ 155.1635)
We proposed to add § 155.1635 to, at our discretion, require a State Exchange to develop and submit a CAP to correct errors identified through the SEIPM process. Our goal would be to establish a set of minimum requirements, using the standards provided at Appendix C to OMB Circular No. A-123, to support State Exchanges in developing, implementing, and monitoring a CAP. We stated in the proposed rule that, should this provision be finalized as proposed, we would issue future sub-regulatory guidance to further detail CAP requirements and processes, and
( printed page 29664)
finalize an approved SEIPM CAP Paperwork Reduction Act (PRA) package following future notice-and-comment rulemaking. We further noted that, should these provisions be finalized as proposed, the first improper payment report would be published in the Fall 2028 AFR and we would anticipate the first SEIPM CAP(s) would be due in early 2029.
At § 155.1635(a), we proposed that HHS could, at its discretion, require a State Exchange to develop and submit a CAP to correct errors identified through the SEIPM process. We would not anticipate that SEIPM CAP standards and requirements would markedly differ from the standards employed by other improper payment measurement programs, such as the Medicaid and CHIP Payment Error Rate Measurement program.
At § 155.1635(b), we proposed that a State Exchange's CAP would need to address errors that would be included in the State Exchange improper payment report described in § 155.1625(c)(2). At § 155.1635(b)(1), we proposed that, in developing a CAP, a State Exchange would be required to conduct an error analysis, which could include reviewing causes, characteristics, and frequency of errors that are associated with improper payments. We proposed that a State Exchange would be required to review the findings of the analysis to determine specific programmatic causes to which errors would be attributed, if any, and to identify root improper payment causes. Further, at § 155.1635(b)(2), we proposed that the State Exchange would be required to determine the corrective actions that would be implemented to address improper payment root causes and prevent recurrence. Finally, at § 155.1635(b)(3), we proposed that the CAP would be required to incorporate measurable milestones, accountability mechanisms, regular monitoring and validation of progress, documentation of implemented corrective actions, and regular status updates. We proposed that the CAP would be required to include all of the following items for each identified error: (1) the specific corrective action; (2) status of the corrective action; (3) scheduled or actual implementation date of the corrective action; (4) key personnel that would be responsible for implementing each corrective action; and (5) a plan for monitoring the effectiveness of the corrective action.
At § 155.1635(c), we proposed that a State Exchange would be required to develop a CAP implementation schedule, implement the CAP in accordance with that schedule, and regularly evaluate whether the initiatives were effective at reducing or eliminating error causes. We stated that it would be critical that a State Exchange maintain regular communication with HHS regarding any evaluation findings, particularly to ensure that the State Exchange would determine specific programmatic causes to which errors would be attributed. Therefore, we proposed that a State Exchange would be required to provide updates on CAP implementation progress in a manner and frequency specified by HHS, but at least annually.
At § 155.1635(d), we proposed that if a State Exchange would: (1) fail to submit a CAP when one had been required; (2) submit an incomplete CAP that would fail to address all parts of a CAP as specified at 155.1635(b)(3); (3) fail to implement a CAP; or (4) submit a CAP otherwise found unacceptable by HHS following technical assistance provided by HHS, that HHS could determine that a State Exchange had failed to substantially comply with SEIPM requirements and could take actions outlined in § 155.1650 to ensure program integrity and effectiveness.
We sought comment on these proposals.
After consideration of the comment and for the reasons outlined in the proposed rule and this final rule, including our responses to the comment, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed below.
Comment:
One commenter opposed the CAP provision, as part of overall opposition to the SEIPM proposal.
Response:
We acknowledge the various concerns related to SEIPM and have responded to the specific concerns through our other responses.
i. SEIPM Preparation Phase (§ 155.1640)
We proposed new § 155.1640 to create a SEIPM preparation phase. At § 155.1640(a), we proposed that any State Exchange in its first year of operation would be required to participate in a 1-year SEIPM preparation phase prior to participating in SEIPM. We stated in the proposed rule that the proposed preparation phase would be designed to familiarize State Exchanges with the SEIPM processes and requirements. At the beginning of the following year, or, in other words, the second year of operation for the State Exchange, we proposed that the State Exchange would undergo SEIPM to measure improper payments for the preceding plan year, its first year of operation. We noted that this implementation timeline would ensure that newly operating State Exchanges would have the opportunity to participate in the preparation phase before undergoing full SEIPM measurement, thereby preparing the State Exchange for the SEIPM measurement. In essence, HHS would ensure that a State Exchange would test processes and procedures to prepare for SEIPM.
We proposed at § 155.1640(b) that, to satisfy the requirements of the SEIPM preparation phase, a State Exchange would be required to: (1) complete the information submission requirements in § 155.1615(b)(1) and (3) using information from the most current plan year for a sample size not to exceed 10 unique tax households that address scenarios specified by HHS; (2) undergo the review procedures in 155.1625(a) and (b); and (3) participate in HHS' technical assistance activities, which could include: (i) training on SEIPM requirements and procedures, (ii) system readiness assessments, (iii) data quality validation exercises, and (iv) process improvement recommendations. Such a preparation phase approach would promote administrative efficiency by ensuring State Exchanges would have adequate time and resources to develop robust improper payment measurement capabilities before full implementation. Without such a preparation period, State Exchanges could struggle to produce the data that would be necessary for determining accurate measurements.
At § 155.1640(c), we proposed that, at the beginning of each calendar year, HHS would provide any State Exchange that would be subject to this section with a schedule that would span a 12-month period and that would specify when the requirements of this section would have to be completed.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1640 below.
Comment:
A commenter requested HHS to extend the preparation phase for new State Exchanges by at least two years so that State Exchanges can determine the resources needed to comply with SEIPM. Other commenters noted broader concerns regarding implementation readiness, including the need for additional time to develop systems, processes, and staffing capacity to support SEIPM requirements.
Response:
We acknowledge the commenter's request to extend the
( printed page 29665)
SEIPM preparation phase by two years, however, we will finalize this provision as proposed. We believe the one year preparation phase will be adequate to prepare State Exchanges for SEIPM and will limit the reporting gaps mandated by PIIA. Regarding the commenters' broader concerns regarding implementation readiness and the time required for State Exchanges to prepare for SEIPM requirements, we note that the SEIPM preparation phase is designed to support this transition by providing State Exchanges, particularly those in their first year of operation, with an opportunity to test processes, validate data submission approaches, and receive technical assistance prior to full participation in SEIPM.
We believe that this preparation phase, together with ongoing technical assistance and guidance, will help support operational readiness and facilitate a more effective transition to SEIPM requirements. Accordingly, we are finalizing § 155.1640 as proposed.
j. Minimizing Potential Duplicate Audit Requirements (§ 155.1645)
We proposed to add new § 155.1645 to permit HHS, to the extent possible, to minimize duplication between the requirements of the SEIPM program described in subpart Q and the annual independent external programmatic audit requirements and standards under § 155.1200(c) and (d). Under § 155.1200(c) and (d), each State Exchange is required to engage or contract with an independent qualified auditing entity to perform an annual independent external programmatic audit to review compliance with 45 CFR part 155 subparts D (eligibility) and E (enrollment), and other requirements under part 155, as specified by HHS, and to provide the audit results to HHS.
In the proposed rule, we stated that, among other things, this external auditing process allows HHS to oversee compliance with eligibility and enrollment standards to ensure that State Exchanges are conducting accurate eligibility determinations and enrollment transactions, including requirements across multiple State Exchange operational areas that exceed the scope of review under the SEIPM program because they do not involve payments of APTC. Section 155.1200(d) further requires that a State Exchange complete an audit to ensure appropriate financial and operational safeguards are in place to avoid making inaccurate eligibility determinations and enrollment transactions, which would include those related to administering APTC and CSRs.
We noted that §§ 155.1200 and 155.1210 were not intended to serve as the type of measurement program contemplated by the PIIA. Program integrity audits completed under § 155.1200(c) and (d), especially as they relate to requirements under subparts D and E, focus on reviewing the processes and procedures that a State Exchange has established to verify that a qualified individual meets eligibility requirements. We stated that these programmatic audits do not review, estimate, or report on the amounts or rates of improper payments resulting from inaccurate eligibility determinations and enrollment transactions. SEIPM would both ensure a review of the accuracy of State Exchange eligibility verification processes and identify improper APTC payments resulting from inaccurate eligibility determinations and enrollment transactions.
To meet the requirements of the PIIA, reduce burden on State Exchanges, and ensure consistency across State Exchanges in terms of our review methodology, we proposed that a State Exchange's participation in SEIPM would satisfy certain duplicative annual independent external programmatic audit requirements, particularly the review of compliance with provisions of subparts D and E that may result in improper payment of APTC. Should this provision be finalized as proposed, we stated in the proposed rule that we would issue sub-regulatory guidance to identify which programmatic audit requirements could be satisfied through completion of SEIPM for a given plan year. We expressed our belief that this policy would reduce duplicative efforts and burden on State Exchanges that would otherwise be required to fully comply with programmatic audit requirements and SEIPM, while also maintaining the programmatic audits for requirements not reviewed as part of SEIPM.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed below.
Comment:
Many commenters noted overlap with State-based Marketplace Annual Reporting Tool (SMART), State Based Marketplace Inbound File (SBMI) submissions, issuer audits, and other oversight requirements. Some commenters stated support for minimizing duplicate requirements between SEIPM and the independent external programmatic audit requirement, but also stated burden concerns as some State Exchanges have negotiated contracts in place for multiple years to satisfy the independent external programmatic audit requirement and requested delay in SEIPM specific to this issue.
Response:
We appreciate commenters' support for the goal of reducing duplicative audit obligations and acknowledge the concerns raised regarding the breadth of existing oversight mechanisms applicable to State Exchanges. We recognize that State Exchanges are subject to a range of Federal oversight requirements and we share commenters' interest in reducing duplication and burden. The amendment of § 155.1200 is specifically designed to address this concern by permitting State Exchanges to satisfy certain SMART annual independent external programmatic audit requirements, specifically those related to compliance with 45 CFR part 155, subparts D and E, through completion of the SEIPM process. Regarding the concern about multi-year audit contracts, we acknowledge that some State Exchanges have entered into multi-year agreements with independent auditing entities to satisfy the annual programmatic audit requirement. We will provide clear sub-regulatory guidance specifying the audit requirements that may be satisfied through SEIPM participation, and we encourage State Exchanges to engage with their auditing entities to discuss potential scope adjustments consistent with the finalized § 155.1200(e) provisions and factor this guidance into their contract planning and renewal processes going forward.
Comment:
Several commenters requested clarification on how SEIPM would reduce or replace existing audit processes. A commenter also requested clarification on whether HHS would grant exemptions annually for the independent external programmatic audit and requested that HHS remove the APTC verification requirements from the SMART to avoid duplication.
Response:
We appreciate this comment and we clarify that the amendment of § 155.1200 will permit State Exchanges to satisfy certain SMART annual independent external programmatic audit requirements, specifically those related to compliance with 45 CFR part 155, subparts D and E, through completion of the SEIPM process. We will provide clear sub-regulatory guidance specifying the audit requirements that may be satisfied through SEIPM participation.
( printed page 29666)
k. Failure To Comply (§ 155.1650)
We proposed to add new § 155.1650 that would address what would happen should a State Exchange fail to comply with the SEIPM requirements. In the proposed rule, we stated that this proposed section would create clear criteria for determining when a State Exchange had failed to substantially comply with SEIPM requirements and would establish appropriate remedial measures to ensure program integrity and effectiveness.
At § 155.1650(a), we proposed to establish a general principle that would govern improper payment classification throughout the SEIPM program. We proposed that HHS would classify APTC payments as improper when a State Exchange failed to provide adequate documentation demonstrating that such payments were made in accordance with applicable Federal requirements. We noted that this principle would align with Federal improper payment measurement standards established under PIIA which require agencies to classify payments as improper when there is insufficient documentation to determine if a payment is proper or improper. The burden of providing adequate supporting documentation would rest with State Exchanges as the entities responsible for making APTC eligibility determinations and payment calculations, ensuring that Federal funds were distributed in accordance with Federal requirements.
We proposed to specify at § 155.1650(b)(1) through (5) when HHS would determine a State Exchange had failed to substantially comply with this subpart by providing specific, measurable criteria addressing the most critical aspects of State Exchange participation in SEIPM, which would consist of the following: (1) failure to submit required data or documentation within the timelines specified in the Annual Program Schedule; (2) submitting data or documentation found to be incomplete, inaccurate, or in a format that would reasonably prevent effective review; (3) failure in the CAP process; or (4) demonstrates a pattern of more than five instances during a SEIPM cycle in which the State Exchange fails to respond within 30 calendar days, or provides a non-responsive answer, to HHS requests for clarification or additional information.
In the proposed rule, we stated that such a proposed compliance framework would balance the need for clear, enforceable standards with recognition that State Exchanges operate complex systems and may encounter operational challenges. We noted that the proposed criteria would focus on substantial compliance failures that would genuinely affect the integrity and effectiveness of the SEIPM program as opposed to minor technical violations that would not materially affect improper payment measurement activities. Such standards would ensure that State Exchanges would provide necessary information within established timeframes to support the overall SEIPM cycle and enable HHS to meet Federal improper payment reporting obligations, while maintaining data quality sufficient to support reliable measurement results. The framework would promote accountability and ensure effective program administration across all participating State Exchanges, while maintaining the collaborative relationship necessary for successful SEIPM implementation. By establishing clear expectations for data submission timeliness, quality standards, corrective action implementation, and ongoing communication, these proposed compliance criteria would support the accuracy of improper payment estimates and the overall integrity of the APTC program oversight process.
At § 155.1650(c), we proposed to establish a process to provide State Exchanges notice and opportunity to address compliance deficiencies before HHS would implement remedial measures. We proposed that before implementing measures under paragraph (d) of this section, HHS would provide written notice to the State Exchange specifying the nature of the noncompliance and the potential consequences, and allow the State Exchange a reasonable opportunity to cure the noncompliance or demonstrate that compliance had been achieved. This notice and cure provision would promote collaborative problem-solving between HHS and State Exchanges. We stated that the written notice requirement would ensure that State Exchanges would have clear understanding of the specific compliance deficiencies and the potential consequences of continued noncompliance, and would enable them to take appropriate corrective action. HHS would set the cure period to be commensurate with the complexity of the compliance issue.
At § 155.1650(d), we proposed to establish a framework of remedial measures that HHS could implement should a State Exchange fail to substantially comply with SEIPM requirements and such failures undermine or prohibit HHS' efficient administration of Exchange improper payment measurement activities. We stated that this provision would provide HHS with appropriate enforcement tools to secure State Exchange compliance while maintaining program integrity and ensuring effective oversight of APTC administration. We proposed that HHS could implement measures or procedures to secure the State Exchange's compliance with the requirements of this subpart which are proposed to include: (1) enhanced monitoring and reporting; (2) mandatory implementation of specific operational procedures or controls; and (3) on-site visits to State Exchange facilities to assess operational procedures, data systems, and compliance with program requirements.
In the proposed rule, we stated that this graduated enforcement approach would recognize that different compliance failures may require different remedial responses, allowing HHS to tailor interventions to the specific nature and severity of the noncompliance. Enhanced monitoring and reporting requirements would provide ongoing oversight for State Exchanges experiencing compliance difficulties, while mandatory operational procedures or controls would address systemic deficiencies that could be contributing to improper payment risks. On-site visits would enable HHS to conduct comprehensive assessments of State Exchange operations, identify root causes of compliance failures, and provide targeted technical assistance to support improvement efforts.
At § 155.1650(e), we proposed that HHS could initiate proceedings to revoke a State Exchange's authority to operate if a State Exchange continued to fail to comply after implementation of initial remedial measures under paragraph (d) of this section. Revoking a State Exchange's authority to operate would represent the most serious enforcement action available and would be reserved for cases where other remedial measures had failed to secure the State Exchange's compliance, and the State Exchange's continued operation would pose unacceptable risks to program integrity and enrollee protection.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed § 155.1650 below.
Comment:
Several commenters stated concern that the proposed consequences for noncompliance are severe,
( printed page 29667)
particularly given the operational complexity of SEIPM and the potential challenges State Exchanges may face in meeting program requirements. Commenters noted that potential outcomes, including corrective action plans and possible revocation of a State Exchange's authority to operate, are significant. A few commenters also requested that HHS exercise flexibility in enforcement during initial implementation, particularly during periods of system transition or adaptation to new requirements. A commenter opposed the provision entirely arguing it is extremely punitive and recommended that punitive measures be applied in stages to provide State Exchanges with the opportunity to correct any failures. Another commenter expressed concern about Federal overreach to withhold Exchange funding in connection with program integrity programs, which may negatively affect the stability of the Exchanges.
Response:
We appreciate these comments, but disagree that the proposed framework would be overly severe and result in Federal overreach. We acknowledge commenters' concerns regarding enforcement during initial implementation, particularly considering operational complexity, system transitions, and the time required to fully implement SEIPM requirements. The provisions in § 155.1650 establish a graduated and flexible approach to addressing noncompliance, beginning with notice and an opportunity for the State Exchange to cure deficiencies before any remedial measures are implemented. This framework is designed to allow for consideration of operational circumstances affecting compliance and to provide State Exchanges with the opportunity to address issues before further action is taken.
The available actions are intended to ensure that HHS can effectively administer improper payment measurement activities and maintain program integrity, while allowing for appropriate consideration of the nature and severity of noncompliance. More significant actions, such as revocation of a State Exchange's authority to operate, would be reserved for circumstances in which a State Exchange persistently fails to comply, after consideration of any mitigating circumstances at the Federal and State level, and where other remedial measures have not been effective.
We recognize that during implementation, State Exchanges will experience challenges and difficulties while working in good faith to comply with the provisions of this subpart. We will be seeking a collaborative partnership with the State Exchanges to mitigate or relieve any such difficulties without resorting to the enforcement actions described in this provision.
E. Part 156—Health Insurance Issuer Standards Under the Affordable Care Act, Including Standards Related to Exchanges
1. FFE and SBE-FP User Fee Rates for the 2027 Benefit Year (§ 156.50)
In the 2027 Payment Notice proposed rule (91 FR 6366), for the 2027 benefit year, we proposed an FFE user fee rate of 2.5 percent of total monthly premiums and an SBE-FP user fee rate of 2.0 percent of total monthly premiums.
Section 1311(d)(5)(A) of the Affordable Care Act permits an Exchange to charge assessments or user fees on participating health insurance issuers as a means of generating funding to support its operations. If a State does not elect to operate an Exchange or does not have an approved Exchange, section 1321(c)(1) of the Affordable Care Act directs HHS to operate an Exchange within the State. Accordingly, in § 156.50(c), we state that a participating issuer offering a plan through an FFE or SBE-FP must remit a user fee to HHS each month that is equal to the product of the annual user fee rate specified in the annual HHS notice of benefit and payment parameters for FFEs and SBE-FPs for the applicable benefit year and the monthly premium charged by the issuer for each policy where enrollment is through an FFE or SBE-FP. OMB Circular No. A-25 established Federal policy regarding user fees and what the fees can be used for.[235]
OMB Circular No. A-25 provides that a user fee charge will be assessed against each identifiable recipient of special benefits derived from Federal activities beyond those received by the general public.
a. FFE User Fee Rate for the 2027 Benefit Year
Based on estimated costs, enrollment in the FFEs (including anticipated enrollment loss due to certain States transitioning from the FFE to SBE-FPs or from SBE-FPs to State Exchanges), and premiums for the 2027 benefit year, we proposed a 2027 user fee rate for all participating FFE issuers of 2.5 percent of total monthly premiums.
Section 156.50(c)(1) provides that, to support the functions of FFEs, an issuer offering a plan through an FFE must remit a user fee to HHS, in the timeframe and manner established by HHS, equal to the product of the monthly user fee rate specified in the annual HHS notice of benefit and payment parameters for the applicable benefit year and the monthly premium charged by the issuer for each policy where enrollment is through an FFE. As in benefit years 2014 through 2026, issuers seeking to participate in an FFE in the 2027 benefit year will receive two special benefits not available to issuers offering plans in State Exchanges: (1) the certification of their plans as QHPs; and (2) the ability to sell health insurance coverage through an FFE to individuals determined eligible for enrollment in a QHP. For the 2027 benefit year, issuers participating in an FFE will receive special benefits from the following Federal activities:
Provision of consumer assistance tools;
Consumer outreach and education;
Management of a Navigator program;
Regulation of agents and brokers;
Eligibility determinations;
Enrollment processes; and
Certification processes for QHPs (including ongoing compliance verification, recertification, and decertification). Activities performed by the Federal Government that do not provide issuers participating in an FFE with a special benefit are not covered by the FFE user fee.
The proposed user fee rate reflected our estimates for the 2027 benefit year of costs for operating the FFEs, premiums, enrollment, and transitions in Exchange models from the FFE and SBE-FP models to either the SBE-FP or State Exchange models. The total enrollment in Exchanges in States anticipated to transition from operating an SBE-FP to a State Exchange model represents premiums for which we will no longer collect user fees, and the total enrollment in Exchanges in States anticipated to transition from an FFE to an SBE-FP model represents premiums for which we will assess user fees at the lower SBE-FP rate. Thus, these anticipated transitions impact our total projected collections, may affect the FFE and SBE-FP user fee rates, and were considered as part of our calculation of our proposed user fee rates.
As stated in the proposed rule, to develop the proposed 2027 benefit year FFE user fee rate, we considered a range of costs, premiums, and enrollment projections. For the 2027 benefit year FFE user fee rate, we estimated that budget costs would be lower in 2027 than the budget costs that we used to
( printed page 29668)
project the 2025 and 2026 benefit year FFE user fee rates. Specifically, while we stated that we expect small increases in costs from the 2026 benefit year to the 2027 benefit year will be due to the structure of contracts and inflationary pressure, recent efficiency exercises have reduced baseline cost structures that were used in the projection of budgets for benefit years 2025 and subsequent years.
We took several factors into consideration in choosing which premium and enrollment projections will inform the proposed 2027 FFE user fee rate. First, for our estimated premium trend rate projections, we expected premiums will increase in 2026. We also expected that while the rate of premium increase will be smaller in benefit year 2027 increases in premiums will persist.
For the 2021 through 2025 benefit years, the individual non-catastrophic market risk pool in all States generally experienced increased enrollment. Our 2026 estimates accounted for projected decreased 2026 benefit year Exchange enrollment in the individual market due to the impact of the expiration of the enhanced PTC subsidies. For the 2027 benefit year, we estimated a further decrease in Exchange enrollment in the individual market due to the expiration of subsidies at the end of the 2025 benefit year as well as the effects of the WFTC legislation and the Marketplace Integrity and Affordability final rule (90 FR 27074).[236]
After taking into consideration a projected reduced budget, enrollment decreases, and a higher premium trend rate, we proposed a 2027 benefit year FFE user fee rate of 2.5 percent of total monthly premiums, which is the same as the 2026 benefit year FFE user fee rate. We stated in the proposed rule that based on our estimates, the proposed FFE user fee rate will allow us to have sufficient funding available to fully fund user fee-eligible FFE activities. We noted that if any events occurring between the proposed rule and the final rule significantly changed our estimated FFE operational costs, or if our enrollment or premium projections changed (especially based on the availability of more recent data), we may finalize an FFE user fee rate that differs from the proposed rate to reflect those changes. We acknowledged that the 2026 open enrollment period closed prior to release of the proposed rule, but we stated that we did not consider that data in developing the proposed user fee rates because the data available at the time was too premature to use for our proposed rule estimates. As discussed in the proposed rule, our intention was to reconsider the enrollment estimates for the final rule. We stated that if the actual 2026 enrollment numbers are lower than the projected enrollment numbers we used to set the proposed user fee rate, the final 2027 user fee rate may be higher. We also stated that if the actual 2026 enrollment numbers are higher than our projected enrollment numbers, the 2027 user fee rate may be lower.
b. SBE-FP User Fee Rate for the 2027 Benefit Year
In the 2027 Payment Notice proposed rule (91 FR 6367), we proposed to charge issuers offering QHPs through an SBE-FP a user fee rate of 2.0 percent of the monthly premium charged by the issuer for each policy under plans offered through an SBE-FP for the 2027 benefit year.
In § 156.50(c)(2), we specify that an issuer offering a plan through an SBE-FP must remit a user fee to HHS, in the timeframe and manner established by HHS, equal to the product of the monthly user fee rate specified in the annual HHS notice of benefit and payment parameters for the applicable benefit year and the monthly premium charged by the issuer for each policy where enrollment is through an SBE-FP. SBE-FPs enter into a Federal platform agreement with HHS to leverage the systems established for the FFEs to perform certain Exchange functions and enhance efficiency and coordination between State and Federal programs. The benefits provided to issuers in SBE-FPs by the Federal Government include use of the FFE information technology and call center infrastructure used in connection with eligibility determinations for enrollment in QHPs and other applicable State health subsidy programs, as defined at section 1413(e) of the Affordable Care Act, and QHP enrollment functions under 45 CFR part 155, subpart E. The user fee rate for SBE-FPs is calculated based on the proportion of total FFE costs associated with Federal activities that provide SBE-FP issuers with special benefits, including costs that are associated with the FFE information technology infrastructure, the consumer call center infrastructure, and eligibility and enrollment services.
To calculate the proposed SBE-FP user fee rate for the 2027 benefit year, we used the same assumptions related to budget, enrollment, and premiums as we used for the proposed FFE user fee rate. As we stated in the proposed rule, the user fee rate for SBE-FPs is calculated based on the proportion of the total FFE costs associated with Federal activities that provide SBE-FP issuers with special benefits, which we stated we continue to estimate to be approximately 80 percent of total FFE costs. These FFE costs associated with Federal activities that provide SBE-FP issuers with special benefits include the costs associated with the FFE information technology infrastructure, the consumer call center infrastructure, and eligibility and enrollment services. Additionally, we stated that the proposed user fee rate for SBE-FP issuers for the 2027 benefit year includes assumptions about States transitioning from either the FFE model to an SBE-FP, or from an SBE-FP to a State Exchange for the 2027 benefit year, which impacts the SBE-FP enrollment projections.
Based on this methodology and our projected reduced budget, enrollment decreases, and a higher premium trend rate that were described in section III.E.1.a. of the proposed rule, we proposed a 2027 benefit year SBE-FP user fee rate of 2.0 percent of total monthly premiums, which is the same as the SBE-FP user fee rate we established for the 2026 benefit year. Specifically, we noted in the proposed rule that changes in budget, enrollment, and premium trends have the same impact for the SBE-FPs as the FFE. We further noted that if any events occurring between the proposed rule and the final rule significantly change our estimated Federal platform operational costs, or if our enrollment or premiums projections change (especially based on the availability of more recent data), we may finalize an SBE-FP user fee rate that differs from the proposed rate to reflect those changes.
We sought comment on the proposed 2027 benefit year FFE and SBE-FP user fee rates.
After the proposed rule was published, we revised our premium projections because of newly available data analysis based on the 2026 open enrollment period that occurred between November 2025 and January 2026. This data analysis found that 2026 premiums increased from what we previously estimated and used for the proposed 2027 user fee rates. After consideration of comments, the reasons outlined in the proposed rule and this
( printed page 29669)
final rule, including our responses to comments, and revised premium projections, we are finalizing a 2027 benefit year user fee rate for all participating FFE issuers of 1.9 percent of total monthly premiums and a user fee rate for all participating SBE-FP issuers of 1.5 percent of total monthly premiums. We note that we establish FFE and SBE-FP user fee rates annually using the most recent data and assumptions available at the time to project costs, premiums, and enrollment.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these 2027 user fee rates as described in the above paragraph. We summarize and respond to public comments received on the proposed FFE and SBE-FP user fee rates for the 2027 benefit year below.
Comment:
Most commenters supported the 2027 benefit year user fee rates, with several of these commenters supporting user fee rates that adequately fund Federal programs. Some commenters supported increasing the 2027 user fee rates. These commenters stated that a higher user fee rate could be used to enhance user fee-funded services, such as Navigators and consumer outreach and education.
Response:
Due to revising our projections between the proposed and final rules based on newly available data, we are finalizing a lower FFE user fee rate of 1.9 percent of total monthly premiums and a lower SBE-FP user fee rate of 1.5 percent of monthly premiums for the 2027 benefit year. We revised our premium trend projections between the proposed and final rules based on newly available data as a result of the 2026 open enrollment period that showed higher 2026 premiums than previously estimated when setting the proposed 2027 user fee rates. We believe the 2027 benefit year user fee rates of 1.9 percent of total monthly premiums for FFE issuers and 1.5 percent of total monthly premiums for SBE-FP issuers will ensure sufficient funding of Federal programs and do not believe that higher user fee rates are needed to maintain current funding for Navigators and consumer outreach and education. Further, we note that in finalizing the 2027 user fee rates in this final rule that are lower than the current 2026 user fee rates, we are putting downward pressure on 2027 premiums compared to if the user fee rates remained the same between the 2026 and 2027 benefit years.
Comment:
Some commenters requested increased transparency on user fees, wanting additional information on how user fees support HHS' policy goals for the Exchanges. Some of these commenters requested enumerated costs of providing Federal eligibility and enrollment platform service and infrastructure to each State.
Response:
In the proposed rule (91 FR 6366 through 6368), we provided information on the assumptions used to calculate the proposed 2027 benefit year user fee rates, including the assumptions related to budget, enrollment, and premiums. In this final rule, we provide information on our revised assumptions used to calculate the finalized 2027 benefit year user fee rates and explain why our assumptions changed between the proposed and final rules. HHS collects user fees in accordance with section 1311(d)(5)(A) of the Affordable Care Act, which permits an Exchange to charge assessments or user fees on participating health insurance issuers as a means of generating funding to support its operations. Therefore, our goal in collecting user fees is to collect user fees at a rate that will allow us to sustain the operations of the FFEs and SBE-FPs.
2. Permitting Plan-Level Adjustments for Multi-Year Catastrophic Plans (§ 156.80(d)(2)(ii))
As discussed in section III.E.6. of the 2027 Payment Notice proposed rule (91 FR 6370), we proposed to modify the requirements for catastrophic plans at § 156.155(a)(6) to specify that a catastrophic plan may have a plan term of either 1 year, or of multiple consecutive years not to exceed 10 years, and sought comment on whether to also specify such standards for individual market metal level plans. To align with that proposal and comment solicitation, and under our authority to implement the single risk pool requirements in section 1312(c)(1) and (2) of the Affordable Care Act, in the 2027 Payment Notice proposed rule (91 FR 6368), we proposed to amend § 156.80(d)(2)(ii) to permit issuers of multi-year catastrophic plans to make plan-level adjustments to the index rate that reflect the length of the entire term. We stated in the proposed rule that such plan-level adjustments would account for the benefit design characteristics of such plans, such as their deductible and maximum out-of-pocket cost structure. We further stated that the proposal to codify standards for catastrophic plans to have multi-year terms of up to 10 consecutive years would clarify certain aspects of the structure of multi-year plans, such as permitting such plans to cover certain additional preventive service benefits before an enrollee satisfies their deductible and annual limitation on cost sharing. We stated that allowing issuers of multi-year catastrophic plans to make plan-level adjustments to the index rate would permit these issuers to take such plan design features into account when developing premiums for such plans. We further stated that, given that these plan design features, which are discussed in section III.E.6 of this final rule, will be unique to multi-year catastrophic plans, it would be appropriate for issuers to take them into account when setting premiums for such plans. We stated that an issuer's calculation of the magnitude of this plan-level adjustment must be accurate, and therefore, must be actuarially justified.
We sought comment on all aspects of the proposal, including whether a separate plan-level adjustment based on term length should be permitted for multi-year catastrophic plans, and whether and the degree to which the risk profile of multi-year catastrophic plans that are otherwise identical to single year catastrophic plans would justify plan-level adjustments over and above those that would be made to account for the different features of such plans.
After consideration of comments, we are not finalizing this proposal because, as discussed below, current regulations already allow issuers to make plan-level adjustments to account for the benefit design characteristics of multi-year catastrophic plans. We summarize and respond to public comments received on the proposal.
Comment:
Several commenters noted their belief that plan-level adjustments to each multi-year catastrophic plan are unnecessary, citing varying reasons. One commenter stated that current rules already allow issuers to apply a plan-level adjustment that reflects the AV and cost-sharing design of a plan, which would already account for multi-year catastrophic plans' unusual deductible and MOOP structure. Another commenter noted their belief that CMS had not articulated a reason why any other multi-year plans' benefit characteristics might justify a plan-level adjustment. Another commenter stated that issuers of multi-year plans will need to set premiums for such plans on an annual basis to comply with statutory requirements, obviating the need for a plan-level adjustment that accounts for the length of the plan term.
Response:
We agree that current regulations at § 156.80(d)(2) that permit plan-level adjustments to the index rate already permit appropriate plan-level adjustments for multi-year catastrophic
( printed page 29670)
plans. Specifically, current regulations at § 156.80(d)(2)(v) permit a plan-level adjustment for the expected impact of the specific eligibility categories for catastrophic plans, and this provision would apply to multi-year catastrophic plans as well as 1-year catastrophic plans. Additionally, current regulations at § 156.80(d)(2)(iv) permit all plans, including catastrophic plans, to make a plan-level adjustment for administrative costs, excluding Exchange user fees. To the extent a multi-year catastrophic plan has lower administrative costs than a 1-year plan, this could be considered through such a plan-level adjustment. Also, as discussed below, this final rule will permit multi-year catastrophic plans to utilize value-based insurance designs to provide benefits before reaching the deductible, under guidelines issued by the Departments of HHS, Labor, and Treasury (the Departments) under section 2713(c) of the PHS Act. Current regulations at § 156.80(d)(2)(i), which permit plan-level adjustments for the actuarial value and cost-sharing design of the plan, would permit a plan-level adjustment to take into account the actuarial value and cost-sharing design adjustments that would result from the implementation of any such value-based insurance design after guidelines are issued by the Departments. We do not agree that setting rates for multi-year plans on an annual basis will obviate the need for plan-level adjustments to the index rate for such plans, because the calculation of the factors that can be taken into account when making plan-level adjustments can vary from year to year. However, such plan-level adjustments are already permitted under current regulations.
We note that in making plan-level adjustments for multi-year catastrophic plans, such plans can have different rates from each other only if they are different plans, as that term is defined in § 144.103.
Comment:
A commenter stated that plan-level index-rate adjustments associated with multi-year catastrophic terms may introduce additional complexity into premium comparability and consumer understanding.
Response:
We do not agree. Plan and premium comparability and consumer education have been HHS' and health insurance issuers' focus long before passage of the Affordable Care Act. We will continue to evaluate, implement, and offer methods and resources aimed at making plan comparisons and coverage choices clearer for consumers, including choices involving multi-year catastrophic plans. As with any novel coverage offering, we further expect health insurance issuers and consumer advocates will engage in activities to educate consumers on how to evaluate and compare multi-year plans to other coverage offerings. For these reasons, we are of the view that concerns regarding consumer confusion do not outweigh the potential positive benefits of making new, more affordable opportunities for coverage available in the individual market.
Commenter:
One commenter stated that because catastrophic plan enrollees turn over frequently, a multi-year catastrophic plan is unlikely to develop meaningfully different risk characteristics than a traditional single-year offering.
Response:
Under current regulations, risk characteristics for catastrophic plans, that is, the expected impact of the specific eligibility categories for those plans, can be considered when making plan-level adjustments for such plans. To the extent such characteristics vary based on the length of the term, those variations can be considered when making plan-level adjustments for multi-year plans. Given that multi-year plans would offer a unique opportunity for longer-term insurance contracts with the potential for greater out-of-pocket savings over time, we believe it is premature to conclude there will be no meaningful difference between the risk characteristics of single-year and multi-year offerings. Under this final rule, individuals who are under the age of 30 or who are eligible for a hardship or affordability exemption when first enrolling in a multi-year catastrophic plan are considered eligible for the duration of the multi-year term. Therefore, it is likely that multi-year catastrophic plans would have an older population than 1-year catastrophic plans, resulting in different risk characteristics. Also, for reasons stated earlier, it is our view that features of multi-year catastrophic plans might cause enrollees to remain in the plans for extended periods, reducing the churn that the commenter mentions.
3. State Selection of EHB-Benchmark Plan for Plan Years Beginning on or After January 1, 2020 (§ 156.111)
Section 1302 of the Affordable Care Act provides for the establishment of an EHB package that includes coverage of EHBs (as defined by the Secretary), cost-sharing limits, and AV requirements. Among other requirements, the law directs that the EHBs be equal in scope to the benefits provided under a typical employer plan, and that they include at least the following 10 general categories and the items and services covered within the categories: ambulatory patient services; emergency services; hospitalization; maternity and newborn care; mental health and substance use disorder services, including behavioral health treatment; prescription drugs; rehabilitative and habilitative services and devices; laboratory services; preventive and wellness services and chronic disease management; and pediatric services, including oral and vision care.
We established requirements relating to the coverage of EHBs in the EHB Rule (78 FR 12834). In the 2019 Payment Notice (83 FR 17009), we added § 156.111 to provide States with additional options from which to select an EHB-benchmark plan for plan years beginning on or after January 1, 2020. We revised the EHB-benchmark plan selection process in the 2023 Payment Notice (87 FR 27290) and the 2025 Payment Notice (89 FR 26218).
As we stated in the 2027 Payment Notice proposed rule (91 FR 6368), we have paused review of State applications to select EHB-benchmark plans in accordance with § 156.111. We are actively conducting a comprehensive review of section 1302 of the Affordable Care Act, as we are considering future rulemaking to revise § 156.111 and other regulations relating to the EHBs.
We received several comments regarding this pause. We summarize and respond to public comments received below.
Comment:
Many commenters stated that they did not agree with the approach CMS has taken to pause the review of State applications to update their EHB-benchmark plans. These commenters urged CMS to resume its review and approval of pending EHB-benchmark plan applications under current regulations, noting that States that have submitted such applications to CMS used a considerable number of resources to do so, and that the States' proposed changes that are currently pending address current gaps in their EHB-benchmark plans. In addition, some commenters requested that CMS prioritize regulatory clarity before making procedural changes. Specifically, these commenters suggested that any revisions to § 155.170 regarding State-mandated benefits should first be formally codified through rulemaking, and noted that codifying clear regulations would provide States with the certainty needed to effectively design EHB-benchmark plans and submit EHB-benchmark plan updates. Some commenters requested that CMS preserve the current framework that gives States flexibility to update their EHB-benchmark plans
( printed page 29671)
specific to their populations, support State innovation initiatives to modernize their EHB-benchmark plans, and establish a transparent process for future review and approval of EHB-benchmark plan changes.
Response:
We acknowledge that commenters have concerns regarding the pause in the review of State applications to update their EHB-benchmark plans and the effort and resources States applied to the application process. However, we believe that approving State EHB-benchmark plan applications and then immediately proposing a new policy that has the potential to render those changes moot or to require further revisions would potentially create greater burdens and hardship for States. Thus, while we realize that the pause creates some uncertainty, it gives HHS time to ensure that the policies implementing section 1302 of the Affordable Care Act are rooted, as required, in the “best reading” of the statute. See
Loper Bright Enters.
v.
Raimondo,
603 U.S. 369 (2024). We will take these comments into consideration as we conduct a comprehensive review of section 1302 of the Affordable Care Act. We appreciate that States are trying to address gaps in coverage by updating their EHB-benchmark plans and believe that this is a worthy objective. While we realize that the pause may seem to frustrate that objective, we believe that the review of section 1302 of the Affordable Care Act and EHB policy in general can facilitate the same goal of helping coverage better meet consumers' needs.
4. Provision of EHB (§ 156.115(d))
In the 2027 Payment Notice proposed rule (91 FR 6368), we proposed to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB.
In the EHB Rule (78 FR 12834), we finalized at § 156.115(d) that issuers of a plan offering EHBs may not include, among other services and benefits, routine non-pediatric dental services as an EHB, even if the State's current EHB-benchmark plan includes such services as covered benefits. Section 1302(b)(2) of the Affordable Care Act directs the Secretary, in defining the EHBs, to ensure that they are equal in scope to the benefits provided under a typical employer plan. In the proposed EHB Rule (77 FR 70644), in support of the proposed prohibition at § 156.115(d), we noted that routine non-pediatric dental services are not typically included in the medical plans offered by employers and are often provided as excepted benefits [237]
by the employer.
In the 2025 Payment Notice, we finalized removal of this prohibition at § 156.115(d) for plan years beginning on or after January 1, 2027. In support of this policy, we noted, as we did in the 2025 Payment Notice proposed rule (88 FR 82597), that a more natural reading of section 1302(b)(2) of the Affordable Care Act is one that considers all the benefits typically covered by employers, regardless of whether such benefits are historically considered a “health benefit” or whether such benefits are “typically covered” by an employer's major medical plan. We also stated that based on recent data, it appeared that routine non-pediatric dental services were commonly covered as an employer-sponsored or other job-based benefit to a degree that warranted removing the prohibition on coverage of these services as an EHB. We further stated that oral health has a significant impact on overall health and quality of life,[238]
and that removing the prohibition on issuers from including routine non-pediatric dental services as an EHB will remove regulatory and coverage barriers to expanding access to routine non-pediatric dental benefits for those plans that must cover EHBs. We further stated that this policy will allow States to work to improve non-pediatric oral health and overall health outcomes, which are disproportionately low among marginalized communities such as people of color and people with low incomes.[239]
However, to better align our regulation at § 156.115(d) with section 1302(b)(2)(A) of the Affordable Care Act, which directs that the scope of EHBs be equal to the scope of benefits provided under a typical employer plan, in the 2027 Payment Notice proposed rule we proposed to reinstate the regulatory prohibition on issuers from including routine non-pediatric dental services as an EHB. In the proposed rule, we acknowledged that in the 2025 Payment Notice proposed rule (89 FR 26342), we previously interpreted section 1302(b)(2)(A) of the Affordable Care Act as supporting a more natural reading that considers all the benefits typically covered by employers, regardless of whether such benefits are historically considered a “health benefit” or whether such benefits are “typically covered” by an employer's major medical plan. Upon further consideration of the statutory framework, we stated in the proposed rule that we now believe a more precise interpretation of section 1302(b)(2)(A) of the Affordable Care Act should apply.
Specifically, we stated that we believe the language of section 1302(b)(1) of the Affordable Care Act, which outlines the 10 EHB categories and specifically includes, “Pediatric services, including oral and vision care,” suggests that Congress did not view routine non-pediatric oral and vision care as an EHB at the time the Affordable Care Act passed. We further stated that this language indicates Congress' intention to differentiate pediatric from non-pediatric dental services and explicitly limit EHB coverage to pediatric oral care. We stated that if Congress had intended for non-pediatric dental services to be included in the list of the 10 EHB categories it would have explicitly included these services, as it explicitly included pediatric oral care. Thus, we stated that the best reading of the statute, which only mentions pediatric oral care, indicates non-pediatric oral care was not meant to be included as an EHB.
In the proposed rule, we acknowledged that the 10 EHB categories set the floor for what constitutes EHB and that routine non-pediatric dental services could theoretically be added on top of this minimum set of EHBs. However, we noted that the EHB typicality standard at section 1302(b)(2)(A) of the Affordable Care Act requires the scope of EHB to be equal to the scope of benefits provided under a typical employer plan, as determined by the Secretary. As we stated in the 2025 Payment Notice (89 FR 26345), the statutory term “a typical employer plan” is ambiguous as to whether it references a single major medical plan, or the entire suite of benefits provided by the employer. We stated that given Congress' intent reflected in section 1302(b)(1) of the Affordable Care Act to specifically include pediatric oral care and not non-pediatric oral care as an EHB category, and the fact that standalone non-pediatric dental plans are excepted benefits, we now interpret “a typical employer plan” under section 1302(b)(2)(A) to refer to an employer's major medical plan rather than the entire suite of benefits typically covered
( printed page 29672)
by employers. We stated that this interpretation of the typicality standard, along with the statutory framework that distinguishes pediatric from non-pediatric dental services, warrants reinstating the regulatory prohibition on issuers from including routine non-pediatric dental benefits as an EHB.
Additionally, we noted that KFF Employer Health Benefits surveys in recent years show most employers do not include dental benefits as part of their traditional medical plan. In KFF's 2019 survey, 59 percent of small firms (3-199 workers) and 92 percent of large firms (200 or more workers) offered separate dental benefits.[240]
More recently in KFF's 2023 survey, 90 percent of small firms and 94 percent of large firms offered separate dental plans.[241]
We stated that since these benefits are typically offered as separate insurance products and are not included in the traditional medical plan, they should not be included in the scope of benefits used to establish the scope of the typical employer plan. Additionally, we noted that while a high percentage of large firms offer separate dental benefits, small firms are less likely to offer any dental benefits (as indicated by the KFF survey data cited above) and small firms comprise the majority of employers in the U.S.[242]
The 2019 KFF survey data was cited in the 2025 Payment Notice (89 FR 26343) as evidence that routine non-pediatric dental services are commonly covered as an employer-sponsored or other job-based benefit. However, we stated that the relevant consideration is not whether routine non-pediatric dental services are commonly covered as an employer-sponsored or other job-based benefit, but whether employers offer these benefits as part of their medical plans or as separate benefits. We further stated that this separation of dental benefits from medical coverage as indicated by KFF's surveys further supports the interpretation that Congress intended to omit non-pediatric dental coverage from the 10 categories of EHBs. We stated that employers traditionally and commonly offering dental coverage as separate plans, as demonstrated by the KFF surveys, is consistent with Congress' determination that non-pediatric dental coverage should not be a part of the 10 EHB categories representing core medical benefits required to be offered in small group and individual plans.
Further, in the proposed rule we acknowledged that oral health can have a significant impact on overall health and quality of life. We clarified that the proposed prohibition on including routine non-pediatric dental services as an EHB would not prevent States from addressing non-pediatric oral health and overall health outcomes through alternative policy mechanisms. We noted, for example, that States could mandate coverage of routine non-pediatric dental services as a non-EHB and defray the cost associated with that benefit. We stated that we believe achieving better alignment of the regulatory requirements at § 156.115(d) with section 1302(b)(2)(A) of the Affordable Care Act regarding the EHB typicality standard outweighs these other policy considerations.
We stated in the proposed rule that if the proposal to prohibit issuers from including routine non-pediatric dental services as an EHB were finalized, there would be fewer operational concerns for issuers associated with States adding routine non-pediatric dental services as an EHB. As we acknowledged in the 2025 Payment Notice (89 FR 26347), if States added routine non-pediatric dental services as an EHB, States would need to consider that some medical plans may not currently have infrastructure or experience working with Current Dental Terminology (CDT) codes that report dental procedures to dental payers. More specifically, for plans that do not directly reimburse using dental codes, the transition to new coding will require investments in technology, staff, and internal expertise. As we further stated in the 2025 Payment Notice (89 FR 26347), these investments may have led to additional premiums and an overall increase in health care spending. Under the proposal, we stated that issuers would not have to consider operational and cost concerns related to developing infrastructure around CDT codes. Additionally, we noted that, as we stated in the 2025 Payment Notice (89 FR 26347), if States added routine non-pediatric dental services as an EHB, this may have required plans to establish new networks of dental providers if plans did not already have such networks available.
Furthermore, we stated in the proposed rule that if this proposal were finalized, we believe there would be fewer impacts on cost-sharing and stand-alone dental plans (SADPs). As we stated in the 2025 Payment Notice (89 FR 26343), while section 1302(b)(4)(F) of the Affordable Care Act permits a medical QHP sold on the Exchange to omit coverage of pediatric dental EHB services if an SADP is offered through an Exchange,[243]
there is no statutory basis to extend this exception to routine non-pediatric dental services. We stated that absent the change we proposed, this would have meant that plans subject to an EHB-benchmark plan that includes routine non-pediatric dental services as an EHB would be prohibited from omitting such coverage on the basis that an SADP already provides such coverage through an Exchange. We stated that this would have required routine non-pediatric dental EHB services to be embedded in medical plans, which would have potentially impacted cost-sharing, as such embedded non-pediatric benefits would be subject to any applicable plan deductible, unless a State requires pre-deductible coverage. We further stated that depending on the benefits, pre-deductible coverage could have also made the plan incompatible with health savings accounts (HSAs). Additionally, we stated that requiring such embedded benefits would have conflicted with the established market structure in which non-pediatric dental services are more commonly provided through SADPs.[244]
Further, as we acknowledged in the 2025 Payment Notice (89 FR 26347), there could have been impacts on SADP premiums sold on the Exchange if a State added routine non-pediatric dental benefits as an EHB, leading to potential disparities between dental plan premiums on- versus off-Exchange. We noted that under §§ 146.145(b)(3) and 148.220(b)(1), limited-scope dental plans are considered excepted benefits that are not required to provide EHBs. Thus, we stated that if a State adds routine non-pediatric dental benefits as an EHB, SADPs are not required to cover such benefits, whether on- or off-Exchange.
In addition, we noted in the proposed rule that the proposal to prohibit routine non-pediatric dental services from being covered as an EHB would not impact
( printed page 29673)
the typicality test at § 156.111(b)(2)(ii), as the methodology and requirements for the typicality test remain unchanged. The typicality test is a quantitative comparison that measures whether the actuarial value of a State's proposed EHB-benchmark plan falls within the range of actuarial values of typical employer plans in the State. We noted that, as we stated in the 2025 Payment Notice (89 FR 26346), nothing in regulation prohibits a State from including the quantitative value of routine non-pediatric dental services, routine non-pediatric eye exam services, long-term/custodial nursing home care benefits, or non-medically necessary orthodontia in its typicality analysis. Specifically, we noted that if a typical employer plan used in the typicality comparison includes any of these services, the actuarial value of those services may be included when calculating that employer plan's overall value for purposes of the typicality test. We stated that this does not mean, however, that these services may be covered as EHBs in the State's EHB-benchmark plan itself. We stated, in summary, that, while the proposal would change what services are permitted to be covered as an EHB, it would not alter how States conduct the typicality test or what may be considered when calculating the actuarial value of typical employer plans for comparison purposes. We stated that States would still be required to ensure the value of covering all the benefits in the State's proposed EHB-benchmark plan is between (or equal to) the value of the least and most generous typical employer plans in the State.
We acknowledged in the proposed rule that under the current policy, States could have submitted applications to HHS to add routine non-pediatric dental services as an EHB by the May 7, 2025 deadline for effectiveness in PY 2027 via the EHB-benchmark update application process under § 156.111. We further acknowledged that although no States submitted applications to make this change by the May 7, 2025 deadline, other States may have already begun work towards their applications to update their EHB-benchmark plan to add routine non-pediatric dental services as an EHB for a future plan year. We noted that the proposal, if finalized, would therefore frustrate these States' efforts.
We sought comment on the proposal to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB, including the impact the proposal, if finalized, would have on health insurance coverage in the individual, small group, and large group markets, as well as on self-insured plans. We stated that if finalized as proposed, the proposed policy to prohibit coverage of routine non-pediatric dental services as an EHB would be effective upon the effective date of the final rule.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing, as proposed, our proposal to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB. We summarize and respond to public comments received on the proposed policy below.
Comment:
A majority of commenters opposed this proposal. Many of these commenters stated that they opposed the proposal because of the important and direct role oral health plays in overall health, well-being, and quality of life, including nutrition, chronic disease management, and employability. Several commenters noted the important impact oral health has on chronic conditions, including but not limited to HIV/AIDS, diabetes, and cancer. Many commenters also noted the importance of preventive care as it relates to oral health. Some commenters noted that growing research has confirmed the connection between oral and whole-body health, and stated that the proposed prohibition is inconsistent with the Trump Administration's “Make America Healthy Again” (MAHA) initiative, pointing to public statements by Secretary Kennedy acknowledging that oral health plays a critical role in overall health and quality of life. One commenter stated their hope that the MAHA movement would influence policymakers to consider the body as a whole entity, rather than continuing to separate oral health from medical care. Many commenters also stated that they opposed this proposal because it does not address the importance of improving oral health disparities and achieving health equity by improving low-income/economic disparities, rural disparities, and racial disparities in oral health.
Response:
We agree that oral health plays an important role in overall health, well-being, and quality of life, including nutrition, chronic disease management, and employability. However, this alone does not mean that issuers must be required or permitted to cover all benefits that could broadly improve health or further public health initiatives as an EHB. Regarding commenters who stated that this proposal is inconsistent with the Trump Administration's “Make America Healthy Again” initiative, we acknowledge the Administration's commitment to improving overall health and well-being, including oral health. However, the EHB framework is a statutory and regulatory structure subject to the typicality standard at section 1302(b)(2)(A) of the Affordable Care Act, and policy goals related to whole-person health can be advanced through mechanisms outside of the EHB framework. As we stated in the proposed rule, the prohibition on issuers from including routine non-pediatric dental services as an EHB would not prevent States from addressing non-pediatric oral health and overall health outcomes through alternative policy mechanisms. We noted, for example, that States could mandate coverage of routine non-pediatric dental services as a non-EHB and defray the cost associated with that benefit. If States mandate coverage of routine non-pediatric dental services as a non-EHB and defray the cost, this could help improve oral health outcomes, including overall health, well-being, and quality of life, and could help address oral health disparities, including those affecting low-income individuals, rural communities, and racial and ethnic minorities, to the extent States choose to exercise this option. States are well-positioned to tailor such mandates to the specific oral health needs and disparities present in their populations. We continue to believe achieving better alignment of the regulatory requirements at § 156.115(d) with the typicality standard at section 1302(b)(2)(A) of the Affordable Care Act outweighs these other policy considerations.
Comment:
Many commenters stated that they opposed this proposal because it removes State flexibility to allow issuers to include routine adult dental services as an EHB. Several commenters contended that EHB prohibitions stifle State flexibility to address urgent and unmet health care needs. Some commenters stated that States should retain the authority to assess the needs of their populations and design benefit packages accordingly. One commenter noted that the Affordable Care Act's framework for EHBs was designed to allow States to define benchmark plans reflecting the specific health care priorities, disease burden, and population health needs of their residents. This commenter stated that this was a deliberate and appropriate policy design choice, as States are closer to their populations, have direct knowledge of their public health
( printed page 29674)
challenges, and are accountable to their constituents in ways that Federal regulators are not. This commenter also noted that restricting State authority in this domain would predictably worsen health outcomes, drive avoidable emergency department utilization, and increase long-term health care expenditures, and that the proposal would override State-level policy judgments without superior clinical evidence. Several commenters also noted that removing State flexibility risks widening gaps in access to oral health care, particularly in rural and medically underserved communities.
Response:
We acknowledge commenters' concerns regarding State flexibility. While we recognize that the 2025 Payment Notice provided issuers with flexibility to include routine non-pediatric dental services as an EHB, we believe the prohibition we are finalizing better aligns with the statutory intent of the Affordable Care Act, which classified only pediatric oral benefits as EHB under section 1302(b)(2)(A). We do not believe that this policy impermissibly restricts State flexibility, as States retain the ability to address routine non-pediatric dental coverage through other mechanisms, including mandating coverage as a non-EHB.
We also do not agree that this policy overrides State-level policy judgments without justification. Given that the Affordable Care Act expressly identifies pediatric oral health services, and not routine non-pediatric dental services, as an EHB category, the EHB framework is not the appropriate vehicle for expanding routine non-pediatric dental coverage, and reinstating the prohibition at § 156.115(d) reflects a considered determination to restore alignment with the statutory structure.
Regarding the commenter who argued that the Affordable Care Act's EHB framework was deliberately designed to allow States to define benchmark plans reflecting their specific health care priorities, disease burden, and population health needs, we agree that the EHB framework at § 156.111 grants States flexibility in designing their EHB-benchmark plans. However, that flexibility outlined in regulation operates within the statutory framework established by the Affordable Care Act, including the typicality standard at section 1302(b)(2)(A) and the EHB categories at section 1302(b)(1), which do not require, and in our view do not permit, the inclusion of routine non-pediatric dental services as an EHB. The EHB framework at § 156.111, which allows for State flexibility, does not override the statutory boundaries within which that flexibility must be exercised.
Regarding commenters' concerns that this policy would worsen health outcomes, increase emergency department utilization, and increase long-term health care expenditures, we acknowledge, consistent with our position in the 2025 Payment Notice, that oral health and overall health are inextricably linked. We further acknowledge that lack of access to routine non-pediatric dental services may contribute to an increase in emergency department visits and downstream health care expenditures. We note that employers must also balance these potential downstream health care expenditures with the added costs of routine non-pediatric dental services and as discussed further below, the typical employer continues to offer dental coverage as a separate plan from their major medical plan. By design, the statutory framework for establishing EHBs aims to align with the cost-benefit analysis made by the typical employer. We also recognize commenters' concerns regarding access to oral health care in rural and medically underserved communities, although we do not agree that this policy will widen existing gaps in access to care. States retain meaningful tools to address routine non-pediatric oral health needs outside of the EHB framework; for example, by mandating coverage of routine non-pediatric dental services as a non-EHB benefit and, where applicable, defraying the associated costs. To the extent that States exercise these options, they can help mitigate the risk of worsening health outcomes, increased emergency department utilization, and downstream costs associated with unmet dental care needs. States are well-positioned to tailor such mandates to the specific oral health needs and access challenges present in their populations, including those in rural and medically underserved areas. We therefore do not agree that this policy unduly restricts State action to address the oral health needs of their populations; rather, it ensures that the EHB framework remains consistent with the Affordable Care Act's statutory structure while preserving State flexibility through other available mechanisms.
Comment:
Many commenters who opposed this proposal stated that permitting issuers to include routine non-pediatric dental services as an EHB makes such coverage more accessible and affordable for enrollees. Several of these commenters noted that allowing issuers to include routine non-pediatric dental services as an EHB supports more comprehensive and affordable coverage options for enrollees by reducing fragmentation between medical and dental coverage. One commenter stated that classifying the oral cavity as separate from the rest of the human body is medically incorrect, pointing to the routine requirement for dental clearance before major medical procedures. Some commenters noted that removing the ability of issuers to include routine non-pediatric dental services as an EHB would mean such dental benefits would continue to only be available as separate plans from major medical health insurance policies, creating logistical and affordability barriers to access. Many commenters also noted that inclusion of routine non-pediatric dental services as an EHB extends Exchange consumer protections to these services—including MLR standards, annual and lifetime limit prohibitions, and cost-sharing protections—which ensure that premium dollars are directed towards patient care rather than issuer overhead. Several commenters further stated that prohibiting inclusion of routine non-pediatric dental services as an EHB would undermine broader goals of fostering competition and lowering overall health care costs. A few commenters also noted that the prior decision to allow issuers to include routine non-pediatric dental as an EHB in the 2025 Payment Notice was made following a diligent review of extensive interested party feedback. A few commenters also noted that individuals who lose Medicaid coverage often turn to the Exchange for affordable health insurance coverage, and that allowing issuers to include routine non-pediatric dental services as an EHB would help ease transitions between coverage programs and support more consistent access to dental care for low- and middle-income individuals.
Response:
We acknowledge commenters' concerns regarding affordability, coverage fragmentation, and Federal consumer protections. We note that, prior to the 2025 Payment Notice, issuers were prohibited from including routine non-pediatric dental services as an EHB under § 156.115(d), such that the absence of EHB protections for adult dental coverage has historically been the status quo in the individual and small group markets. By reinstating this prohibition, we are restoring alignment with that longstanding baseline. Moreover, we note that routine non-pediatric dental coverage in the private market—including through SADPs—has not historically been subject to the full suite of EHB-related consumer protections, such as the prohibition on annual and
( printed page 29675)
lifetime dollar limits and cost-sharing limitations under section 1302(c)(1) of the Affordable Care Act. The structure we are reinstating is therefore consistent with how adult dental coverage has long been offered and accessed by consumers and does not represent a reduction in protections relative to the market as it existed prior to the 2025 Payment Notice.
In response to the commenter who noted that classifying the oral cavity as separate from the rest of the human body is medically incorrect, we agree; as we mentioned in the 2025 Payment Notice, we agree that oral health and overall health are inextricably linked. However, the distinction drawn here is not a medical one, but a statutory and market-based one: routine non-pediatric dental benefits have historically been administered, priced, and delivered separately from major medical coverage, and reinstating the prohibition at § 156.115(d) is consistent with this established structure and with the typicality standard under § 156.111(b)(2)(i) and section 1302(b)(2)(A) of the Affordable Care Act.
As we stated in the proposed rule, the prohibition on issuers from including routine non-pediatric dental services as an EHB would not prevent States from addressing these concerns through alternative policy mechanisms. States may, for example, mandate coverage of routine non-pediatric dental services as a non-EHB and defray the associated costs. Additionally, routine non-pediatric dental coverage remains broadly available to consumers, including through SADPs offered on the Exchange, which are specifically designed to administer dental benefits. We continue to believe that achieving better alignment with the typicality standard at section 1302(b)(2)(A) of the Affordable Care Act outweighs these other policy considerations.
We also do not agree with commenters who stated that reinstating the prohibition at § 156.115(d) undermines the goals of fostering competition and lowering overall health care costs. States retain the ability to mandate routine non-pediatric dental coverage as a non-EHB benefit, and SADPs will remain available on the Exchange, which supports robust competition among dental issuers and preserves consumer choice. In response to commenters who noted that the prior decision to allow issuers to include routine non-pediatric dental as an EHB was based on extensive interested party input, we acknowledge that the 2025 Payment Notice was informed by that feedback. However, upon further evaluation of relevant regulatory and policy considerations, we have determined that reinstating the prohibition better aligns with the statutory structure of the Affordable Care Act and the typicality standard at section 1302(b)(2)(A) of the Affordable Care Act.
Further, we acknowledge commenters' concerns regarding coverage continuity for individuals transitioning from Medicaid to the Exchange. We recognize that such transitions can create gaps in access to dental care, particularly for low- and middle-income individuals. However, as we have previously mentioned, States retain the ability to address routine non-pediatric dental coverage through alternative mechanisms outside of the EHB framework, including by mandating such coverage as a non-EHB benefit and defraying the associated costs, which could help support more consistent access to dental care for individuals navigating coverage transitions.
Comment:
Many commenters stated that they support this proposal because it better aligns with the statutory intent of the Affordable Care Act. Many commenters stated that they support this proposal because it appropriately realigns § 156.115(d) with section 1302(b)(2)(A) of the Affordable Care Act, which explicitly designates pediatric, not non-pediatric, dental services as an EHB. One commenter noted that, as CMS has recognized and as Kaiser Family Foundation data confirms, routine adult dental services are not typically included in employer-sponsored major medical coverage, and that reinstating the prohibition on issuers including routine non-pediatric dental services as an EHB restores statutory consistency and avoids unnecessary market disruption. One commenter also stated that this proposal better aligns with the Affordable Care Act's statutory framework and congressional intent by reaffirming a consistent interpretation of the “typical employer plan” standard. One commenter stated that classifying routine non-pediatric dental as an EHB under the Ambulatory Patient Services category, as was stated in the 2025 Payment Notice final rule, is inconsistent with how that category is commonly understood, which is referring to medical care delivered on an outpatient basis, such as office visits and urgent care. This commenter also stated that this categorization does not align with how employer-sponsored coverage typically treats dental care, representing a significant departure from longstanding industry practice.
On the other hand, many commenters who opposed the proposal disagreed with the legal argument that Congress intended only for pediatric dental services to be an EHB. Many of these commenters noted their belief that Congress' decision not to include routine non-pediatric adult dental services as an EHB was not a permanent exclusion, but reflected market considerations at the time of the Affordable Care Act's enactment. These commenters also noted that Congress granted HHS authority under sections 1302(b)(4)(G) and (H) of the Affordable Care Act to periodically review and update EHB to reflect evolving evidence, market practices, and consumer needs, indicating that EHB standards are intended to be dynamic. One commenter stated that the ten categories of EHBs are only a minimum and HHS can include other benefits as EHBs. This commenter also noted that the Affordable Care Act does not link EHB coverage to excepted benefits and stated that HHS offers “wildly differing and at-times erroneous interpretations” of the “typical employer plan” provision. Some commenters opposing this proposal also stated that routine non-pediatric dental services are commonly covered in employer-sponsored plans, suggesting that this exclusion may not be warranted under the typical employer plan standard. At least one of these commenters explained that according to Delta Dental, approximately 90 percent of employers with 500 or more employees offer dental benefits.[245]
At least one of these commenters also stated that HHS should continue to allow issuers to include routine non-pediatric dental benefits as an EHB to ensure Exchange beneficiaries are not disadvantaged compared to individuals with private coverage.
Additionally, one commenter stated that the proposed prohibition on issuers including routine non-pediatric dental services as an EHB is procedurally invalid and inadequately justified. This commenter contended that the Department failed to abide by the procedural requirements in section 1302 of the Affordable Care Act, which include a requirement for the Secretary of Labor to conduct a survey of employer-sponsored coverage and for the Secretary of HHS to submit a report to Congress, and that this failure deprived States and commenters of the
( printed page 29676)
ability to meaningfully engage with the underlying data. This commenter further stated that CMS' reliance on section 1302(b)(1)(J) of the Affordable Care Act, which explicitly includes pediatric oral care as an EHB, as evidence that Congress intended to exclude adult dental from EHB is illogical, and that CMS improperly substitutes “typical employer plan” with “typical major medical employer plan” to avoid confronting evidence that employer plans commonly cover adult dental benefits.
A few commenters also warned that a final rule reinstating this prohibition could be vulnerable to challenge under the APA's arbitrary and capricious standard if CMS fails to meaningfully engage with the substantial body of peer-reviewed evidence on oral-systemic health linkages, the cost savings of preventive dental care, and the consequences of dental coverage gaps on emergency department utilization and population health. One commenter expressed their belief that the proposal is arbitrary and capricious because it does not reasonably explain departing from the view cited in the 2025 Payment Notice that routine non-pediatric dental services can reflect a typical employer plan and promote health equity.
Response:
We agree with commenters that this change better aligns § 156.115(d) with section 1302(b)(2)(A) of the Affordable Care Act. While we agree with commenters that the statute provides authority for periodic review of EHB, the statute also requires CMS to adhere to the “typical employer plan” standard when determining the scope of EHB. Consistent with this standard, typical employer-sponsored health plans do not typically include comprehensive adult dental services within their medical benefit packages. More often, routine non-pediatric dental coverage is available through products separate from the employer-sponsored major medical coverage.
In response to commenters who stated that routine non-pediatric dental services are commonly covered in employer-sponsored plans and therefore meet the typical employer plan standard, we acknowledge that many employers offer dental benefits. However, as discussed further below, the relevant inquiry under the typicality standard is whether routine non-pediatric dental services are typically included in employer-sponsored major medical plans, not whether employers offer dental benefits through any vehicle, including SADPs or limited-scope excepted benefit dental plans. The data cited by commenters reflects employer dental benefit offerings broadly and does not establish that routine non-pediatric dental services are typically included within major medical coverage. We also disagree with the characterization that HHS has offered erroneous interpretations of the “typical employer plan” provision; as explained in the proposed rule and in this final rule, our current interpretation reflects a reasoned and well-supported reading of the statutory framework consistent with the regulatory history at § 156.115(d).
In response to commenters who stated that the Congress' decision not to include non-pediatric dental services as an EHB was not a permanent exclusion and that HHS has authority to update EHB standards under section 1302(b)(4)(G) and (H) of the Affordable Care Act, we agree that the statute requires periodic review of EHB. We also acknowledge that the ten EHB categories established in section 1302(b)(1) of the Affordable Care Act represent a minimum floor, and that HHS retains discretion to include additional benefits as EHBs. However, the exercise of that authority and discretion must remain consistent with the typicality standard at section 1302(b)(2)(A) of the Affordable Care Act. We have evaluated the relevant evidence and policy considerations and have determined that reinstating the prohibition better aligns with the statutory structure and the typicality standard, as routine non-pediatric dental services are not typically included in employer-sponsored major medical plans.
Further, we do not agree with the commenter who stated that this proposal is procedurally defective because the Secretary of Labor failed to conduct a survey of employer-sponsored coverage and the Secretary of HHS failed to submit a report to the Congress before proposing to revise EHB. Reinstating the prohibition at § 156.115(d) restores the longstanding regulatory baseline that existed prior to the 2025 Payment Notice and was developed after considering the Secretary of Labor's survey of employer-sponsored coverage,[246]
and is supported by a reasoned explanation consistent with the requirements of the APA. We also do not agree with the commenters who stated that our reliance on section 1302(b)(1)(J) of the Affordable Care Act as evidence that the Congress intended to exclude routine non-pediatric dental services from EHB is illogical. The explicit inclusion of pediatric oral care in the statutory EHB categories, combined with the absence of any corresponding inclusion of routine non-pediatric dental services, supports our interpretation that the EHB framework was not designed to require coverage of routine non-pediatric dental services. We further do not agree that we have improperly substituted “typical employer plan” with “typical major medical employer plan.” As we previously noted in the proposed rule, the statutory term “a typical employer plan” is ambiguous, but given Congress' intent reflected in section 1302(b)(1) of the Affordable Care Act and the fact that standalone non-pediatric dental plans are excepted benefits, we interpret a “typical employer plan” to refer to an employer's major medical plan. We also acknowledge that the Affordable Care Act does not explicitly link EHB coverage to excepted benefits; however, the prohibition at § 156.115(d) is independently grounded in the typicality standard at section 1302(b)(2)(A), and the structure of the excepted benefits framework is relevant evidence that routine non-pediatric dental services are not typically included in employer-sponsored major medical plans.
In response to commenters who raised APA concerns, we have considered the evidence on oral-systemic health linkages, the cost-effectiveness of preventive dental care, and the ability of States to address dental coverage gaps through alternative mechanisms outside of the EHB framework, as reflected throughout this preamble. We have determined that, notwithstanding these important public health considerations, reinstating this prohibition better aligns with the statutory structure of the Affordable Care Act and the typicality standard, and that States retain meaningful tools to address adult oral health needs outside of the EHB framework.
We also do not agree with the commenter who stated that Exchange enrollees would be disadvantaged compared to individuals with private coverage. First, we note that EHB applies to all non-grandfathered individual and small group market plans, which is inclusive of some private coverage. Second, we are required by statute to ensure that EHB is equal in scope to a typical employer plan. A policy goal such as equalizing coverage generosity across markets does not negate that statutory requirement. We also believe that routine non-pediatric dental coverage remains available to many Exchange enrollees
( printed page 29677)
through SADPs, which often offer adult benefits, and are the same vehicle through which the majority of privately insured individuals access dental benefits.
Lastly, in response to the commenter who stated that classifying routine non-pediatric dental as an EHB under the Ambulatory Patient Services category is inconsistent with how that category is commonly understood, we appreciate this concern and understand why the inclusion of dental services under a category typically associated with outpatient medical care, such as office visits and urgent care, may seem incongruous. However, we note that categorization of EHBs in a State's EHB-benchmark plan is not Federally defined or required. Any State categorization of a benefit within a particular EHB category does not independently determine whether a benefit may be included as an EHB, and we do not believe the categorization question has bearing on the EHB-benchmark application or approval process.
Comment:
Many commenters who supported this proposal expressed concerns with the policy finalized in the 2025 Payment Notice, which would have required issuers to embed adult dental benefit, that is, incorporate routine non-pediatric dental coverage directly into a QHP medical plan rather than offer such coverage as an SADP, when such issuers elected to include non-pediatric dental services as an EHB. These commenters noted that enrollees would be subject to a combined medical and dental deductible, effectively creating an “illusory benefit” for routine non-pediatric dental services. Many of these commenters also noted that embedded dental benefits are inconsistent with how most enrollees receive dental benefits (that is, through SADPs), and that the current policy leads to market disruption for SADP issuers by undermining the SADP market. One commenter also noted that the current regulation creates a structural misalignment in the delivery of dental services, because SADPs, which are the primary vehicle through which most enrollees access dental benefits, cannot offer non-pediatric dental as an EHB, resulting in inconsistent treatment of pediatric and adult dental services and confusion for consumers and providers. Several commenters also noted that the regulation currently in effect would increase operational and administrative costs for medical QHPs and result in market disruption for SADPs and enrollees. Some commenters noted that SADPs offer specialized expertise in dental networks, claims administration, and benefit design tailored to oral health care. A few commenters noted that not all QHPs have dental networks, much less networks of the size and scope of SADPs, which further contributes to the illusory nature of the embedded benefit.
A few commenters also noted that annual benefit maximums would not apply to adult dental EHB services if embedded into QHPs, which would raise the costs of PPO dental plans and drive issuers toward offering narrower-network Dental Health Maintenance Organizations (DHMOs) to control expenses. These commenters noted that these DHMO networks would lack the capacity to absorb large numbers of new enrollees, resulting in care disruptions, reduced access to the broader PPO options consumers prefer, and a potential decline in quality of care. These commenters also warned that this shift toward DHMO networks would create substantial financial barriers for consumers and risk eroding the competitive SADP market that currently helps keep dental coverage affordable. One commenter additionally noted that embedding adult dental benefits into QHPs would limit consumer choice and reduce access to affordable coverage.
Some commenters also stated that reinstating the prohibition would correct what they characterized as administrative overreach and preserve a stable dental insurance market currently serving millions of enrollees, and noted that embedding these benefits into QHPs could reduce consumer choice, increase costs, subject services to higher cost-sharing, and disrupt existing dental provider networks.
However, some commenters who opposed this proposal stated that QHPs already possess the necessary infrastructure to offer adult dental benefits, as evidenced by the 36 States where QHPs already embed such benefits.[247]
One commenter stated that operational concerns regarding CDT codes are not a sufficient justification for the prohibition, as CDT coding is a long-standing administrative standard and issuers already handle specialized coding for other benefits. This commenter also noted that provider network concerns are manageable, as dental networks are widely established and issuers already coordinate with SADPs. One commenter also stated that SADPs have low annual maximums (around $1,500), which limit access to comprehensive care. Additionally, one commenter noted that States could have addressed cost-sharing concerns related to an embedded non-pediatric dental benefit under the current policy by requiring separate dental and medical deductibles, rather than requiring pre-deductible coverage, and that this approach could also address potential incompatibility with health savings accounts (HSAs).
Response:
We appreciate the comments in support of this proposal and agree that these considerations further support finalizing the proposal as proposed. As we discussed in the proposed rule, routine non-pediatric dental benefits are typically provided through separate products that are structured and priced differently from major medical coverage. To the extent that States, using the flexibility under the current policy, updated their EHB-benchmark plans to allow issuers to include routine non-pediatric dental services as an EHB, such coverage would have needed to be embedded in QHPs, which could have impacted SADPs. Specifically, embedding routine non-pediatric dental services as an EHB within a QHP would have required non-pediatric dental coverage to be subject to the QHP's combined medical and dental deductible, unless a State required pre-deductible coverage. This structure is inconsistent with how dental benefits are typically delivered and accessed, that is, through SADPs, which are structured and priced separately from major medical coverage and generally do not subject enrollees to a combined medical deductible. As a result, enrollees may have found the embedded dental benefit difficult to access due to high deductible thresholds, creating what commenters described as an “illusory benefit.” Further, pre-deductible dental coverage would be incompatible with requirements for an HSA. We also agree with the commenter who noted that the current policy created a structural misalignment by prohibiting SADPs from offering non-pediatric dental as an EHB while permitting QHPs to do so, which could result in inconsistent treatment of pediatric and non-pediatric dental services and may cause confusion for consumers and providers. We also agree with commenters that not all QHPs have dental networks, which would have further limited enrollees' practical ability to access embedded dental benefits. Although, as we mentioned in the 2025 Payment Notice, issuers could have contracted with a dental vendor to administer the routine non-pediatric dental benefits under the current policy, it would have likely increased costs for the issuers.
( printed page 29678)
Additionally, we agree with commenters that SADPs offer specialized expertise in dental networks, claims administration, and benefit design that is specifically tailored to oral health care, which is expertise and infrastructure that is distinct from that of medical QHPs.
While we do not necessarily agree with commenters' concerns that the current policy limits consumer choice, we do believe that prohibiting routine non-pediatric dental services from being covered as an EHB is a better approach for market stability. Including routine non-pediatric dental services as an EHB could have disrupted the existing SADP market by reducing enrollee demand for separate dental plans. Additionally, SADPs are the primary avenue through which enrollees access non-pediatric dental benefits in the existing market, and reinstating the prohibition better aligns the Exchange market with that established market structure. We also acknowledge commenters' concerns that, because annual benefit maximums would not apply to non-pediatric dental services embedded as an EHB in a QHP, this could have raised the costs of PPO dental plans and may have created incentives for issuers to offer narrower-network dental HMOs to control expenses—networks that may have faced challenges absorbing large numbers of new enrollees, which could have potentially resulted in care disruptions and reduced access to the broader PPO options consumers prefer. Embedding adult dental services as an EHB in QHPs could have undermined the SADP market by reducing enrollee demand for SADPs, given that dental coverage would already be incorporated into their QHP. We agree with commenters who noted that reinstating the prohibition preserves the stable dental insurance market structure that currently serves millions of enrollees. Additionally, States and issuers may have faced various operational challenges, including the need to establish new dental provider networks, develop infrastructure for processing CDT codes, and ensure seamless enrollment and cost-sharing arrangements, which are burdens that could have further destabilized the existing SADP market structure. We acknowledge that some commenters stated that these operational concerns are overstated, pointing to the 36 States where QHPs already embed non-pediatric dental benefits as evidence that the necessary infrastructure exists, and asserting that CDT coding is a long-standing administrative standard that does not present a meaningful barrier. Although CDT coding is an established standard, there is operational complexity that arises from integrating two distinct types of codes with claims processing practices. We also acknowledge the argument that dental provider network concerns are manageable given the widespread establishment of dental networks and existing coordination between QHP issuers and SADPs. While we recognize that some issuers have developed capacity to embed dental benefits, we do not believe that the existence of such capacity in certain markets is sufficient to conclude that the operational and market disruption concerns raised by the majority of commenters are without merit. Moreover, the fact that some QHPs currently embed adult dental benefits does not mean that such embedding is consistent with how dental benefits are typically structured or accessed, nor does it resolve the structural concern that embedding dental coverage within a combined medical deductible framework creates an illusory benefit for enrollees. We further note that the existence of coordination between QHP issuers and SADPs does not mean all QHP issuers already have the dental network infrastructure necessary to administer embedded dental benefits as an EHB at scale. We also acknowledge the comment that SADPs have low annual maximums that may limit access to comprehensive care; however, SADP benefit limits reflect how those products are designed and priced in the market and are not a consequence of this prohibition. States retain the ability to address benefit adequacy through other mechanisms, including State insurance mandates.
However, we note that these potential effects on SADPs would have depended on the State-specific decisions regarding EHB-benchmark plans and would not have necessarily occurred uniformly across all States. Specifically, under the current policy finalized in the 2025 Payment Notice, it would have been up to each State to determine whether to add routine non-pediatric dental services as an EHB and, if so, to define the scope of those benefits, within the confines of the typicality standard under § 156.111(b)(2)(i). Because States likely would have taken varied approaches to adopting routine non-pediatric dental services as an EHB, any resulting impact on SADPs would not have been uniform or guaranteed across all States.
In response to the commenter who suggested that States could have required separate dental and medical deductibles as an alternative to pre-deductible coverage under the current policy, we acknowledge this as a potential State-level option; however, we note that this does not resolve the broader concern that embedded dental coverage is inconsistent with how dental benefits are typically delivered and accessed.
Comment:
Many commenters also discussed the cost implications of this proposed policy. Many of the commenters who supported this proposal stated that the current policy, which permits issuers to include routine non-pediatric dental services as an EHB, results in increased operational and administrative costs, which increases issuer burden and administrative complexity. Some commenters also noted that mandating coverage of routine non-pediatric dental benefits in Affordable Care Act plans raises plan costs, premiums, and Federal subsidies, while creating pressure for other States to adopt the same benefit as EHB since they share in the costs and subsidies. One commenter stated that designating routine non-pediatric dental services as an EHB would increase adverse selection risk and increase premiums. Another commenter supported this proposed policy because they stated an improperly structured routine non-pediatric dental services EHB could create consumer confusion, increase cost sharing, and lead to coverage loss.
Some commenters who opposed this proposal stated that reinstating the prohibition on issuers including routine non-pediatric dental services as EHB would deny consumers Federal premium tax credits and cost-sharing reductions for the dental portion of their coverage, strip EHB protections—including prohibitions on annual and lifetime limits and cost-sharing caps—and require States to defray the costs associated with routine non-pediatric dental benefits from their own budgets. Many commenters also stated that this proposal would increase downstream costs, and that it is significantly less costly to provide preventive dental services upfront than to pay for avoidable emergency room visits for dental emergencies. Some commenters cited relevant data, including one commenter who explained that according to the American Dental Association, a dental Emergency Department (ED) visit costs approximately three times more than an office visit ($749 vs. $90-$200), with national ED dental costs totaling approximately $1.6 billion annually (one-third of which is paid by
( printed page 29679)
Medicaid),[248]
and that every dollar invested in preventive dental care may save $8 to $50 in downstream costs.[249]
Other opposing commenters noted that excluding routine non-pediatric dental services from EHB would increase unmet dental needs, raise cost-sharing, shift costs to States and local communities, discourage plan inclusion, and further limit access for adults facing financial and geographic barriers to care.
Some commenters had recommendations for CMS if the proposal to reinstate the prohibition on inclusion of routine non-pediatric dental services as an EHB were finalized. One commenter recommended that if the proposal is finalized, CMS clearly articulate the viable pathways through which States and issuers may continue to support routine non-pediatric dental access outside the EHB framework without creating coverage fragmentation or administrative complexity that deters enrollment. In addition, this commenter also encouraged CMS to evaluate and describe the likely consumer impacts of the policy, including whether it increases the likelihood that consumers forgo dental coverage entirely and whether coverage separations create barriers for patients who require coordinated medical and dental care.
Response:
We agree with the commenters concerns that the current policy allows for increased operational and administrative costs, which increases issuer burden. We note that we acknowledged in the 2025 Payment Notice that removing the prohibition on inclusion of routine non-pediatric dental services as an EHB may have increased costs for issuers that would have needed to expand their networks to cover these services, and that some States would have been more affected than others given that the size of non-pediatric dental networks varies by State. By reinstating the prohibition at § 156.115(d), this policy avoids these potential network expansion costs and the associated operational and administrative burdens on issuers. Additionally, as noted in the proposed rule, no State elected to add routine non-pediatric dental services as an EHB under the current policy finalized in the 2025 Payment Notice. Accordingly, this policy change will not result in new costs to States or Federal programs relative to the current baseline of State EHB-benchmark plans.
Regarding commenters' concerns that the current policy would lead to increased plan costs, premiums, and Federal outlays, we acknowledge that plan costs, premiums, and Federal outlays would have likely increased under the current policy in States that adopted routine non-pediatric dental services as an EHB. However, as we noted in the 2025 Payment Notice (89 FR 26348), despite the prohibition on annual and lifetime dollar limits for EHB and States' ability to choose how comprehensive a routine non-pediatric dental EHB would be, there would have been a limit on the extent to which premiums and Federal outlay could increase because States' ability to increase benefit generosity is constrained by the typicality standard at § 156.111(b)(2)(i), which requires that the scope of benefits of a State's EHB-benchmark plan fall within the range defined by the State's least and most generous typical employer plans.
In response to the commenter who stated that the current policy, which allows for the designation of routine non-pediatric dental services as an EHB, would increase adverse selection risk, we note that, as stated in the 2025 Payment Notice, adverse selection has not been a significant concern in prior EHB-benchmark plan applications, and the Affordable Care Act has established mechanisms—including the risk adjustment program, premium subsidies, and limited enrollment windows—to help prevent unchecked adverse selection.
We also acknowledge the commenter who stated that an improperly structured routine non-pediatric dental services EHB could create consumer confusion, increase cost sharing, and lead to coverage loss. Embedding routine non-pediatric dental services as an EHB within a QHP would have subjected those services to the QHP's combined medical and dental deductible—a structure inconsistent with how a majority of consumers access dental benefits—which could have rendered the benefit difficult to use in practice, increased effective cost sharing relative to standalone dental products, and potentially discouraged enrollment. Reinstating the prohibition avoids these outcomes by preserving the SADP market structure through which consumers are accustomed to accessing dental benefits.
We acknowledge commenters' concern that reinstating the prohibition would deny consumers Federal premium tax credits and cost-sharing reductions for the dental portion of their coverage. However, because no State added routine non-pediatric dental services as an EHB under the current policy, no enrollees are currently receiving APTC or CSRs for such coverage. Accordingly, reinstating the prohibition does not result in a loss of existing enrollee subsidies. In response to commenters' concerns regarding the loss of EHB consumer protections, including the prohibition on annual and lifetime limits and cost-sharing caps, we refer readers to our discussion regarding those concerns earlier in this preamble to § 156.115(d). We also acknowledge that reinstating the prohibition would generally require States to defray the costs of routine non-pediatric dental benefits if they choose to mandate such coverage. States retain the flexibility to determine whether to mandate such coverage and take on the associated defrayal costs.
For commenters' concerns related to downstream costs and the cost-effectiveness of preventive dental care, we acknowledge, as we noted in the proposed rule and the 2025 Payment Notice, that oral health and overall health are inextricably linked, and that improving access to routine dental services can yield downstream savings in overall health care expenditures and reduce costly emergency room visits for dental care. A discussion of the downstream cost data cited by commenters, including emergency department utilization costs and the cost-effectiveness of preventive dental care, is included in the Regulatory Impact Analysis section of this final rule. However, we note that this prohibition does not prevent States from addressing non-pediatric oral health outcomes through alternative policy mechanisms. For example, States could mandate coverage of routine non-pediatric dental services as a non-EHB benefit and defray the associated costs. We emphasize that States retain meaningful tools to address oral health needs outside of the EHB framework, which States can use to improve access to dental health services and reduce costly emergency room visits for dental care.
We also acknowledge the recommendation that CMS articulate viable pathways for States and issuers to support access to non-pediatric dental services outside the EHB framework and evaluate likely consumer impacts. As noted throughout this section, States may mandate non-EHB routine non-pediatric dental coverage and defray associated costs, and SADPs remain
( printed page 29680)
available on the Exchange. We believe these mechanisms mitigate the risk that consumers forgo dental coverage entirely or face barriers to coordinated medical and dental care.
Comment:
A few commenters noted clinical quality and patient safety concerns related to this proposal. One commenter who supported this proposal stated that embedding routine non-pediatric dental in the EHB framework without adequate actuarial value creates perverse economic incentives that drive down reimbursement rates, which this commenter stated could lead to substandard care and irreversible patient harm. This commenter further contended that keeping routine non-pediatric dental outside the EHB framework preserves market-based quality incentives.
On the other hand, one commenter who opposed this proposal noted that dental exams are a required component of care before cancer patients begin certain treatments (such as chemotherapy, radiation, and stem cell transplants) because untreated oral infections can cause serious, irreversible complications, including osteonecrosis of the jaw. This commenter stated that prohibiting issuers from including routine non-pediatric dental services as an EHB would put access to these necessary preventive services at risk.
Response:
We appreciate the comments that raise clinical quality and patient safety concerns. In response to the commenter who supported this proposal, we note that the SADP market is specifically structured to deliver dental benefits, with established networks and reimbursement methodologies tailored to dental care. We agree that embedding adult dental in the EHB framework could risk disrupting this established SADP structure, potentially undermining the quality and reimbursement incentives specific to the SADP market.
In response to the commenter who raised concerns about cancer patients' access to pre-treatment dental care, we acknowledge that dental clearance is an important component of care for patients undergoing certain cancer treatments, and that untreated oral infections can cause serious complications. However, the prohibition on including routine non-pediatric dental services as an EHB does not eliminate access to dental care for these patients. Routine non-pediatric dental coverage remains available through SADPs offered on the Exchange, and States retain the ability to mandate such coverage as a non-EHB benefit and defray the associated costs. We therefore do not believe this prohibition forecloses access to the preventive dental services that cancer patients require prior to treatment.
5. Publication of the 2027 Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage in Guidance (§ 156.130(e))
As established in part 2 of the 2022 Payment Notice (86 FR 24238), starting with the 2023 benefit year, for benefit years in which we are not making changes to the methodology to calculate the premium adjustment percentage index (PAPI), the required contribution percentage, and the maximum annual limitation on cost sharing and reduced maximum annual limitation on cost sharing, we publish these parameters in guidance annually by January of the year preceding the applicable benefit year. In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27166 through 27168), we finalized a change to the methodology for calculating these parameters starting with the 2026 benefit year such that we will use private health coverage premiums (excluding Medigap and the medical portion of accident insurance [“property and casualty” insurance]) as the definition of premiums for calculating the premium adjustment percentage and related parameters. In the 2027 Payment Notice proposed rule (91 FR 6370), we did not propose to change the methodology for calculating these parameters for the 2027 benefit year. As such, these parameters are not included in this rulemaking. Instead, we published the 2027 benefit year parameters in guidance,[250]
using the methodology finalized in the 2025 Marketplace Integrity and Affordability final rule.
We summarize and respond below to public comments received regarding the publication of the 2027 PAPI, the maximum annual limitation on cost sharing, the reduced maximum annual limitation on cost sharing, and the required contribution percentage in guidance.
Comment:
Several commenters expressed support for the annual update to PAPI, the associated payment parameters, and the data used to calculate PAPI as well as concerns regarding PAPI's effects on year-over-year maximum annual limitation on cost sharing growth, the affordability of catastrophic plans, and coverage limitations. Some commenters provided recommendations related to cost sharing and policy measures to stabilize or slow the growth of the maximum annual limitation on cost sharing.
Response:
While these comments are out of scope for this final rule because they do not relate to the specific proposals included in the proposed rule, we appreciate the commenters' attention and feedback.
6. Multi-Year Terms for Catastrophic Plans To Improve Health (§§ 156.130(c) and 156.155(a)(6))
In the 2027 Payment Notice proposed rule (91 FR 6370), we proposed to codify requirements under which issuers of catastrophic coverage may enroll individuals for multiple plan or policy year terms with periods of up to 10 years. We proposed modifying the requirements for catastrophic plans in § 156.155 to specify that a catastrophic plan has a plan term of either 1 plan or policy year, or of multiple consecutive plan or policy years not to exceed 10 years.
We proposed that catastrophic plans with terms of at least 2 plan or policy years may utilize value-based insurance designs (VBID) to offer benefits for preventive services under section 2713(c) of the PHS Act, in addition to those specified in section 2713(a) of the PHS Act, without the enrollee having to first satisfy their deductible or annual cost-sharing limitation. We requested comment on the proposal at § 156.130, that issuers of multi-year catastrophic plans have the option to apply the annual limitation on cost sharing for each plan year of the contract on an annual basis, or, on average, over the life of the contract. We stated, for example, that as an alternative to applying the annual limitation on cost sharing on an annual basis, an issuer could opt to offer a 5 year catastrophic plan that would apply the annual limitation as follows: the average over 5 years of the annual limitation on cost sharing in the plan equals the average over 5 years of the annual limitation on cost sharing as required by statute. Alternatively, we stated that the issuer could opt to vary the annual limitation on cost sharing in the plan by disease, for example, cancer, if that disease requires treatment that spans multiple years, so long as the average over all plan participants and over years of the annual limitation on cost sharing equals the average over 5 years of the annual limitation on cost sharing as required by statute. We stated that the value of
( printed page 29681)
varying the annual limitation on cost sharing in the plan over time in a long-term plan is that a higher annual limitation in early years may allow the plan to lower the limitation in later years to entice participants to remain in the plan for its duration, without altering the expected actuarial value of the plan over its duration as of the plan's start date.
Finally, as more fully discussed in section III.E.2. of this final rule, we proposed to amend § 156.80(d)(2)(ii) to allow issuers of multi-year catastrophic plans to make a plan-level adjustment to the index rate. We stated that this proposal was intended to promote innovation in health coverage plan design that could exert downward pressure on premiums and costs, while increasing access to coverage and care and improving health outcomes.
We proposed that an individual who satisfies the requirements for a catastrophic plan at the time of enrollment in the plan under section 1302(e)(2) of the Affordable Care Act would remain eligible for the duration of its multi-year term.[251]
We sought comments on the proposal and how it would interact with other laws.
We stated in the proposed rule that given the large increases in premiums for health coverage in recent years, we are interested in offering additional alternatives for individuals to enroll in less expensive options. We stated that we believe that Congress' recent decision to designate all catastrophic and bronze plans as high-deductible health plans, as well as our recent broadening of the hardship exemption for individuals to qualify for catastrophic health plans,[252]
is in keeping with that objective. We stated that we also believe that when individuals receive preventive services and effective disease management, those interventions can help reduce costs in the long run,[253]
which in turn may ease pressure on premiums. However, we noted that issuers that do a particularly effective job of promoting these sorts of interventions often do not reap the long-term advantages of those reduced costs because they might retain those enrollees for only short durations and therefore cannot moderate premiums accordingly. We stated that this is because the single-year plan terms in the individual market promote churn where individuals cycle out of particular individual market plans, with enrollees often switching health insurance issuers on a frequent basis,[254]
sometimes annually.[255]
We stated that, in such cases, an individual who receives such interventions while enrolled with a given issuer for 1 plan or policy year, and thereby may improve their health prospects for the future, is often not enrolled with that same issuer when those health benefits accrue. We stated that, in this way, the incentives for individual market issuers differ from those for large employers, that often have an incentive to invest in the health of their long-term employees through wellness programs and offering of other workplace programs that promote physical fitness, smoking cessation, and other initiatives aimed at reducing sick days and improving long term health outcomes.
We stated in the proposed rule that, in addition to incentivizing investments in health promoting activities, health insurance contract terms that exceed a year may decrease the administrative costs associated with marketing and enrollment and encourage alternative pricing structures where administrative efficiencies are reflected in lower premiums and enrollees in plans with multi-year terms are insulated from short-term premium spikes. We stated that, from the perspective of the individual, remaining enrolled with the same plan or issuer for a longer period of time might also promote adherence to disease management programs, and thus promote better overall long-term health. Because of the potential positive impacts on enrollee health and plan affordability, we proposed modifying the requirements for catastrophic plans in § 156.155(a)(6) to specify that a catastrophic plan has a term of either 1 plan or policy year, or of multiple consecutive plan or policy years not to exceed 10 years. We stated in the proposed rule that if we should finalize the proposal to codify requirements for multi-year catastrophic plans, we would consider expanding these or other similar requirements to multi-year plans of one or several metal levels.
We noted that section 1302(e)(1)(B) of the Affordable Care Act specifies benefits that catastrophic health plans are required to provide pre-deductible, including three primary care visits per year and preventive services specified in section 2713 of the PHS Act. Section 2713(a) of the PHS Act requires applicable health plans to cover: (1) evidence-based items or services that have in effect a rating of “A” or “B” in the current recommendations of the United States Preventive Services Task Force (USPSTF); (2) immunizations that have in effect a recommendation from the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention for the individual involved; (3) for infants, children, and adolescents, evidence-informed preventive care and screenings provided for in the comprehensive guidelines supported by the Health Resources and Services Administration (HRSA); and (4) for women, such additional preventive care and screenings not described in paragraph (1) as provided for in comprehensive guidelines supported by HRSA.
Section 2713(c) of the PHS Act authorizes the Secretary to develop guidelines to permit health plans to utilize VBID. As described above, we stated in the proposed rule that we believe broadening plan terms beyond a single plan or policy year for catastrophic plans would increase the value provided to consumers in the form of better incentives for the issuer to invest in the long-term health of its enrollees. As such, we proposed under our authority at section 2713(c) of the PHS Act that catastrophic plans with a term of at least 2 plan or policy years may utilize a VBID in the context of designing health coverage for preventive services such that benefits related to said design may be offered prior to satisfaction of the plan's deductible and prior to satisfying the plan's cost-sharing limitation, in addition to those benefits that can be offered prior to satisfaction of the plan's deductible and cost-sharing limitation enumerated in section 1302(e)(1) of the Affordable Care
( printed page 29682)
Act. We sought comment on the types of benefits plans could offer under the proposal, such as benefits that are designed to improve the long-term health of enrollees. We noted that any such benefits must satisfy all applicable non-discrimination requirements. While the proposal was limited to catastrophic plans, we also sought comment on whether additional clarification or guidance specific to the group market is necessary.
We proposed at § 156.130 that issuers of multi-year catastrophic plans have the option to apply the annual limitation on cost sharing for each plan year of the contract on an annual basis, or, on average, the life of the contract. We stated, for example, that the limitation applicable to a specific year under each plan year of the coverage could be divided by 12 to determine the monthly limit on cost sharing under the plan.
We noted in the proposed rule that, currently, enrollees can experience dramatic coverage changes when insurance contracts reset or change from one year to the next as deductibles and out-of-pocket limits reset. We further noted that this can lead to significant shifts in cost sharing from month to month for the same services. We stated that given that multi-year plans would not be subject to renewal at year's end (other than after the final year of the multi-year term), we believe it is appropriate to allow for a benefit structure that does not reset every 12 months. We stated that we believe that providing a consistent, predictable monthly out-of-pocket limit would reduce consumer confusion, improve financial planning, and bolster adherence to treatment plans.
We stated in the proposed rule that under the example above under which an issuer chooses to divide by 12 to determine the monthly limit on cost sharing, the monthly limitation on cost sharing during any plan or policy year contained in the multi-year plan would reflect one-twelfth of the annual limitation for the plan or policy year for which the Federal annual limitation has been calculated. We stated that it is our view that this approach is consistent with how the annual limitation on cost sharing must be calculated by plans. We further stated that under the proposal to set requirements for catastrophic plans with multi-year terms, issuers would be able to choose the length of the multi-year term up to a maximum of 10 years, and could offer as many or as few such plans as desired, with different maximum terms. We also stated that issuers would not be required to offer a 1-year plan that is otherwise identical to each multi-year plan. We noted that catastrophic plans with multi-year terms would continue to be subject to the Affordable Care Act guaranteed availability and guaranteed renewability requirements for individuals who are eligible for catastrophic plans under Federal law (as is the case for catastrophic plans with terms of 1 year). We further noted that individuals dropping coverage under a multi-year catastrophic plan, either at the end of the term or mid-term, would be treated the same as individuals dropping coverage under a 1-year policy either at the end of the year or mid-year, respectively, for open enrollment and special enrollment periods. Additionally, we noted that other Federal requirements, including, but not limited to, the Mental Health Parity and Addiction Equity Act, the Women's Health and Cancer Rights Act, the Newborns' and Mothers' Health Protection Act, Michelle's Law, and the No Surprises Act, would continue to apply to such coverage.
We stated in the proposed rule that under current policy, an enrollee could terminate their enrollment in a multi-year catastrophic plan at any time and for any reason, without a penalty or being liable for the premium for the remainder of the multi-year term. An issuer could discontinue the product or exit the market under the same guaranteed renewability exceptions that apply generally under section 2703 of the PHS Act. That said, we stated that we understand the importance of certainty for issuers and enrollees in unlocking the aforementioned benefits of multi-year plans and the improvements in incentives they create. We sought comment on how Federal policies could promote continuous coverage in multi-year plans and defray the risk of termination by either the enrollee or issuer, including by promoting continuous coverage for individuals who churn in and out of the individual market through the use of individual coverage health reimbursement arrangements.
We stated in the proposed rule that all multi-year catastrophic plans would be expected to disclose that the plan has a multi-year term, and the length of that term. We further stated that, to the extent multi-year catastrophic plans utilize the monthly method of applying the annual limitation on cost sharing discussed earlier in this preamble, plans would be expected to include that information in marketing and enrollment materials.
We also stated that under the proposal, issuers could apply the deductible that applies in the first year of coverage on an annual basis for each year within the coverage, or divide the annual deductible by 12, and apply it equally to each month of the policy throughout the entire term of coverage, similar to how a multi-year plan could choose to apply the annual limitation on cost sharing, as discussed in this section of the rule. We stated, for example, that if the plan had an annual deductible of $6,000, it could apply
1/12
of that deductible monthly ($500 per month). We sought comment on if, and the degree to which, a plan could modify the amount of the annual deductible for each year of the multi-year policy.
We acknowledged that multi-year plans in individual health insurance markets represent a novel idea that could necessitate changes to other programs and processes that affect individual and group market plans. We stated, for example, that we would need to consider how to treat multi-year catastrophic plans for purposes of the HHS-operated risk adjustment program, but to do that we would want to consider what the benefits and drawbacks are to each option.
Therefore, we sought comments on all aspects of the proposal, including whether there are any specific plan duration terms that would incentivize enrollees to adopt longer term, health-promoting habits. We also requested comment on ways that plans with multi-year terms could be a more affordable option for consumers over single-year terms, including how premiums and rating practices for these plans might differ from other catastrophic plans that have a standard 1-year term; and whether plan terms of more than 10 years would better facilitate rating and promote lower premium products. We also sought comment on if and how any terms of coverage should be permitted to change over the course of the multi-year term, such as reduced deductibles or other cost-sharing, or reduced maximum cost-sharing requirements, and in what intervals such changes could be permitted.
We also requested comment on whether any further modifications to HHS risk adjustment regulations under 45 CFR part 153 may be needed to align with any expected differences in rating practices and any resulting risk selection; whether we should use the same catastrophic HHS risk adjustment models regardless of whether the catastrophic plan is offered for a standard plan year or on a multi-year basis or whether we should have separate models or factors for these catastrophic plans (or enrollees in catastrophic plans) offered on a multi-year basis and, if so, what data, trending
( printed page 29683)
assumptions, and plan benefit design assumptions should be used for those models; whether we should calculate risk adjustment transfers for catastrophic plans offered for a standard plan year separately from risk adjustment transfers for catastrophic plans offered on a multi-year basis; and whether and how the State average premium term in the State payment transfer formula [256]
should be modified to account for the influence of the length of the plan term in regard to the State average premium term of the formula, plan allowable rating factor, or for any other reason (78 FR 15428 through 15434). We also requested comment on whether and how plans with longer terms should be treated for MLR purposes, particularly whether the current MLR standard set forth in 45 CFR part 158 is appropriate for measuring revenue and claims experience of multi-year plans, and whether multi-year plans should be considered under the same book of business as plans with a traditional 1-year plan term for purposes of MLR. We also sought comment on what incentives or disincentives issuers would have to offer multi-year catastrophic plans, potential administrative barriers for issuers, and how long it would take issuers to develop and offer these plans. We sought comment on whether to require or permit issuers to offer multi-year terms for individual market catastrophic and metal level plans, and if so, which ones and why. We requested comment on potential interactions between this proposal and the health insurance market rules in 45 CFR parts 144 and 147, including rules for guaranteed availability and guaranteed renewability, fair health insurance premiums, specifically for premium variations based on age and restrictions to the 3:1 age rating, and uniform modifications to coverage; and whether more regulatory changes would be needed to effectuate this policy. Finally, we requested comment on how this proposal would exist and interact with other laws related to tax policy such as health savings accounts and individual coverage health reimbursement arrangements (ICHRAs), and any changes, either to the proposal or such other laws, that would resolve any such conflict between the proposal and those laws.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy, applicable for plan years beginning in 2027, with the following modifications. We are finalizing § 156.155(a)(6) with minor revisions to refer to “plan years” instead of “years” for greater clarity and precision. We are also finalizing modifications stating that multi-year catastrophic plans may utilize VBID to provide benefits before reaching the deductible, pursuant to guidelines issued by the Secretaries of HHS, Labor, and the Treasury under section 2713(c) of the PHS Act. We are not finalizing the proposed conforming amendments to § 156.155(a)(1), as multi-year catastrophic plans, like other catastrophic plans, must meet all applicable requirements for health insurance coverage in the individual market. We also are not finalizing the proposed addition of § 156.130(c), which provided that in the case of a catastrophic plan with a multi-year term, the annual limitation on cost sharing for the initial plan year of the contract may apply on an annual basis, or on average over the life of the contract. Therefore, as finalized, a multi-year catastrophic plan could have a term of up to 10 consecutive plan years, individuals eligible for catastrophic coverage at the time of enrollment would remain eligible for the duration of the multi-year term, and coverage could be provided before the deductible is met for certain VBID benefits to be specified in future guidance. Otherwise, there would be no material differences between the regulatory requirements for such plans and 1-year catastrophic plans, although as described in the preamble of the proposed rule and in the response to the public comments, the longer coverage terms of such plans could result in valuable advantages to both issuers of such plans and their enrollees.
We summarize and respond to public comments received on the proposal below.
Comment:
Several commenters supported the proposed standards for multi-year catastrophic plans. Commenters stated that such plans would give unsubsidized or price-sensitive consumers another lower-premium option, expand HSA use, spread risk over a longer horizon, lessen the up-front financial shock that can make annual catastrophic coverage hard to use, reduce churn, encourage investment in prevention and care management, and reduce the hassle and costs of annual health insurance plan selection. One commenter noted that an individual has more knowledge of their projected health status for the next year, than for the next several years, and can therefore engage in adverse selection more easily when selecting a plan each year than if selecting a plan over a longer term.
Response:
We agree with these commenters, and, as discussed above, we set forth some of these reasons for proposing regulatory modifications to allow for the offering of catastrophic plans with terms of multiple consecutive plan years.
Comment:
One commenter questioned the comparison we made in the proposed rule between permitting individuals to remain enrolled in multi-year catastrophic plans so as to allow the issuers to reap the benefits of a healthier enrolled population over time, and the efforts large employers make in their health plans to encourage wellness for their long-term employees. The commenter stated that we failed to provide evidence to support our statement that benefits provided by large group employers result in better health outcomes among their employees compared to individual market enrollees. The commenter also suggested that extending the duration of an individual market contract does not make it comparable to an employer-employee relationship or make individual market coverage equivalent to employer-sponsored coverage.
Response:
Our comparison was limited. We noted that issuers that do a particularly effective job of promoting prevention and wellness often do not reap the long-term advantages of those reduced costs of a healthier population because they might retain those enrollees for only short durations and therefore cannot moderate premiums accordingly. We noted that therefore, the incentives for individual market issuers differ from those for large employers, that often have an incentive to invest in the health of their long-term employees through wellness programs and offering of other workplace programs that promote physical fitness, smoking cessation, and other initiatives aimed at reducing sick days and improving long term health outcomes. We did not state that employer-sponsored coverage produces better health outcomes than individual market coverage. We also did not suggest that multi-year catastrophic plans create an employer-like relationship. We recognize these relationships are fundamentally different.
( printed page 29684)
Comment:
Some commenters disagreed with our statement that multi-year catastrophic plans could moderate premiums by decreasing the administrative costs associated with marketing and enrollment. The commenters stated that premium increases are primarily driven by medical costs and that we did not provide evidence supporting administrative savings.
Response:
We agree that medical costs are a primary driver of premium increases. However, we believe that reductions in marketing and administrative costs associated with multi-year catastrophic plans could help moderate premiums increases. We did not conclude that such reductions would occur, only that they
may
occur (91 FR 6371).
Comment:
Several commenters stated that allowing individuals to remain enrolled in a catastrophic plan for the duration of its multi-year term violates the Affordable Care Act. They stated that eligibility for catastrophic coverage must be determined annually and stated that individuals who no longer satisfy the eligibility criteria for a plan year—because they are 30 and older or no longer qualify for a hardship or affordability exemption—cannot remain enrolled. Some commenters also raised concerns that allowing multi-year enrollment conflicts with eligibility verification requirements, such as section 71303 of the WFTC legislation and other eligibility verification provisions of the proposed rule.
Response:
Under section 1302(e) of the Affordable Care Act, an individual is eligible for enrollment in a catastrophic plan “for any plan year” if the individual has not attained the age of 30 before the beginning of “the plan year” or has a certification in effect “for any plan year” that the individual qualifies for a hardship or affordability exemption. We interpret “the plan year” as the first plan year of coverage and interpret “any plan year” as the first plan year of coverage plus any other plan year within the term of coverage. Therefore, an individual who is eligible for a catastrophic plan for the first plan year of the coverage remains eligible for the entire term of coverage until renewal, as coverage following renewal is a different term of coverage. This interpretation applies to catastrophic plans with both single-year and multi-year terms. In response to commenters' concerns that this interpretation does not align with the eligibility verification requirements of the WFTC legislation, generally, the purpose of verification is to protect Federal spending on premium tax credits. Because enrollees in catastrophic plans cannot receive such financial assistance, it is our view that annual verification of eligibility for catastrophic coverage with regard to enrollees in multi-year catastrophic plans is not contemplated by the statute.
Comment:
Some commenters suggested that multi-year catastrophic plans would conflict with the Affordable Care Act's 12-month plan year framework and related requirements, including guaranteed availability, the annual limitation on cost sharing, MLR, risk adjustment, and rating rules.
Response:
We acknowledge that a plan year or policy year is generally defined as a 12-month period.[257]
The proposal did not change that definition. Instead, it would allow a single contract to span multiple plan or policy years. Such a plan would be subject to guaranteed availability during every open enrollment period and would be available for enrollment through a special enrollment period in a manner no different than 1-year catastrophic plans (that is, plans with a term of one 12-month plan year), as well as the rating rules that require issuers in the individual market to set their rates on a plan year basis (that is, annually). Additionally, given that we are not finalizing certain proposals related to the annual limitation on cost sharing, for each 12-month plan year within a multi-year catastrophic plan, the plan must comply with the Federal annual limitation on cost sharing that applies for that plan year. As stated below, we are not making any changes to the treatment of multi-year plans for purposes of MLR and rebate calculation and reporting requirements under part 158 in this rulemaking.
Furthermore, we believe that the HHS risk adjustment methodology is flexible enough to appropriately accommodate multi-year catastrophic plans without making changes to the HHS risk adjustment models or State payment transfer formula. First, as described elsewhere in this preamble, multi-year catastrophic plans would be required to update their out-of-pocket maximums annually, to account for the updated maximum annual limitation on cost sharing that would apply for each plan year included in the catastrophic plans' contract term. As such, the plan liability assumptions that underlie the HHS risk adjustment models for a given plan year would be largely consistent between multi-year and single-year catastrophic plans, resulting in HHS risk adjustment models for catastrophic plans that are applicable regardless of the contract term of the plan. Furthermore, risk scores calculated from the HHS risk adjustment models would continue to be calculated on a plan year basis. For example, an enrollee who remained enrolled for the entirety of the first plan year of a multi-year catastrophic plan's contract term but ended their enrollment in the second plan year of the contract term would receive no HCC-contingent enrollment duration factor in their risk score for the first plan year because HCC-contingent enrollment duration factors only apply to adult enrollees with 6 or fewer months of enrollment. This enrollee could receive an HCC-contingent enrollment duration factor in their risk score for the second plan year to the extent that they also have an HCC recorded in their enrollee-level EDGE data for that plan year. The enrollee's HCCs, RXCs, and demographic factors would similarly be determined on a plan year basis using their age, diagnoses, and prescription drugs from the claims and demographic data in the plan's enrollee-level EDGE data for the applicable plan year. Similarly, we will be able to continue to conduct HHS-RADV activities with reference to the HCCs, RXCs, and demographic factors that appear in a multi-year plan's enrollee-level EDGE data for an applicable plan year.
For the State payment transfer formula, the Statewide average premium used for catastrophic plan risk adjustment transfers is an enrollment-weighted average premium for all catastrophic plans in the State. Likewise, all plan-level variables in the State payment transfer formula are enrollment-weighted variables. As such, these variables can all be updated for an applicable plan year using the data of the enrollees who remain enrolled in the plan for that plan year. We will continue to calculate HHS risk adjustment transfers (and HHS-RADV adjustments to HHS risk adjustment transfers) on a plan year basis across all catastrophic plans with active enrollment in that plan year by using the enrollee-level EDGE data for the applicable plan year and the applicable plan years' HHS risk adjustment models for catastrophic plans.
Comment:
Several commenters stated that the proposal did not include enough detail to allow for meaningful comment or implementation. One commenter suggested that this lack of
( printed page 29685)
detail violated the Administrative Procedure Act. Several commenters indicated that the rule should not be finalized due to what they characterized as uncertainty about the proposal's requirements, and others suggested that the proposal not be applicable until at least 2028. Commenters stated that certain details of the proposal were too uncertain for issuers to implement, including, among others, which provisions would be fixed at the time a multi-year contract is effectuated, whether premiums would be fixed, whether rate increases for the whole term would be set at the initial filing, and whether rating area factors would be fixed. For changes within the plan, one commenter stated that any mid-term changes in premiums, benefits, or networks would constitute issuer gaming that denies consumers their chosen coverage.
Other questions raised by commenters, which they stated were not sufficiently addressed, include: Would enrollees progress through the age curve each year? Would the issuer have to keep any dependents on the contract until the full term expired? Would covered benefits be fixed? What valuation assumptions would be fixed? Would issuers be able/required to adjust rates annually as part of the annual single risk pool premium filing? How would coverage apply for newly added dependents during the plan's term? How would premiums be handled for consumers who move between rating areas? Would the plan-level adjustment for multi-year catastrophic plans have a trend component, like the quarterly trend adjustment in the small group market? If the adjustment functions like a quarterly trend, when would premium refilings be permitted? If premium refilings are permitted, would refilings affect the rates of currently issued products? How would multi-year plans be treated under State 1332 waiver programs? What kinds of novel financial reporting issues would multi-year plans raise under GAAP and statutory accounting? What discount rates would be appropriate for any longer-term valuation of benefits? Would any cash value accumulate if there is a disconnect between premiums collected and benefits received over the contract term? What modifications to regulatory capital requirements would be warranted for multi-year plans to reflect the increased risk they pose to issuers? What additional rate review requirements would be required for multi-year catastrophic plans, particularly if contract terms are largely fixed at pricing.
Response:
We believe the proposal included detail sufficient to satisfy the Administrative Procedure Act. However, we will provide additional guidance or rulemaking, as necessary, to address certain aspects of this policy.
In response to the comments that stated that any mid-term changes in premiums, benefits, and networks would constitute issuer gaming that denies consumers their chosen coverage, we note that we expect benefits and networks to generally remain stable for the length of the term, and such coverage would continue to be subject to applicable Federal and State laws, and premiums will vary annually as issuers of multi-year plans comply with the single risk pool, risk adjustment, and other requirements that impact rating.
For rate setting, rate calculations for multi-year plans, including plan-level adjustments, would be determined each year, as they are for a 1-year plan that renews each year. Thus, rate increases for the whole term would not be set at the initial filing; premiums for the entire term and rating area factors would not be fixed at effectuation, but would be set annually; and enrollees would not progress through the age curve each year. Rather, as with 1-year plans, the enrollee's age as of the date of policy issuance or renewal must be used, under § 147.102(a)(1)(iii). With respect to multi-year catastrophic plans, the date of renewal is the first day the coverage is renewed after the multi-year term has expired. For example, if an individual enrolls in a catastrophic plan with a term of 5 consecutive plan years, the date of renewal would be the first day following the expiration of the 5 plan-year term. With respect to the comments regarding valuation assumptions and discount rates, we note that rates for a multi-year catastrophic plan would be set annually under the single risk pool requirements in § 156.80. We defer to the appropriate governing boards for any novel financial reporting issues that multi-year plans might raise under GAAP and statutory accounting standards. For any modifications to regulatory capital requirements for multi-year plans, issuers would be subject to the capital requirements set by State regulators. For the question about what additional rate review requirements would be required for multi-year catastrophic plans if contract terms are largely fixed at initial pricing, we again note that rates would not be set in advance for the entire term of the policy, but would be set annually, under the single risk pool requirements set forth at § 156.80. Therefore, no additional rate review requirements would be required or necessary. The issuer would keep any dependents on the contract until the full term expired, unless the enrollee voluntarily dropped the dependent from coverage or the dependent ceases to satisfy the plan's terms of eligibility for dependent coverage, consistent with 45 CFR 147.120. Coverage would apply for newly added dependents during the plan's term, and premiums for consumers who move between rating areas would be handled no differently than in 1-year plans. State law would determine whether a multi-year catastrophic plan may have a cash value that the policyholder may borrow against, or for which the plan could be sold.
For section 1332 waivers, the Departments of HHS and the Treasury recognize that multi-year plan designs may raise unique considerations over the waiver period. To the extent a waiver application, waiver amendment, or other proposed change presents such considerations, the Departments of HHS and the Treasury will address them through the appropriate section 1332 waiver processes. Specifically, the Departments of HHS and the Treasury will continue to seek public comments on each waiver application or proposed waiver amendment and consider those comments in assessing whether the waiver application or proposed waiver amendment, satisfies the statutory guardrails set forth in section 1332(b)(1)(A) through (D) of the Affordable Care Act.
Comment:
One commenter questioned how issuers can consider the claims experience of all enrollees in all health plans in the individual market (other than grandfathered plans) when setting rates for multi-year plans under the single risk pool provision at § 156.80 if future plans are not yet designed.
Response:
As is the case with 1-year plans, issuers do not base rates on plans that do not yet exist.
Comment:
Several commenters stated general support for disclosures to consumers as applied to multi-year catastrophic plans. These commenters recommended disclosures describing the differences and limitations of these arrangements, including mid-term cost, benefit, and provider network changes; disclosures of any variable rate terms to consumers at the outset, while having consumers proactively indicate they understand the terms and conditions of their coverage, including any limitations or excluded benefits; disclosure of rights to terminate coverage; disclosure at enrollment of the full annual limitation on cost sharing and deductible (and any other material cost-sharing features);
( printed page 29686)
and disclosures about the practical implications of multi-year enrollment, including the consumer's ability to change plans, transition between metal levels, or move to other coverage when circumstances change.
Response:
We expect issuers of multi-year catastrophic plans to furnish the disclosures mentioned in the proposed rule, in which we stated that we expect such issuers to disclose that the plan has a multi-year term and the length of that term. The length of the term of an insurance policy is universally disclosed by issuers for 1-year policies and is generally required by and enforced by States, so our expectation is in line with what issuers currently disclose. We note that no commenters objected to those disclosures. The other disclosures mentioned by the commenters are either not as universally disclosed by issuers, so we therefore do not expect issuers of multi-year catastrophic plans to necessarily disclose them, or are required to be disclosed under current law and regulations. For example, the summary of benefits and coverage requires issuers, including issuers of catastrophic plans, to disclose benefits and benefit limitations. To the extent the disclosures mentioned by the commenters go beyond those disclosures, issuers of multi-year catastrophic plans may provide them.
We also proposed that, to the extent multi-year catastrophic plans utilize the proposed monthly method of applying the annual limitation on cost sharing discussed earlier in this preamble, plans would be expected to include that information in marketing and enrollment materials. Given that we are not finalizing that method of applying the annual limitation on cost sharing, issuers of multi-year catastrophic plans would not be expected to make such disclosure in marketing and enrollment materials.
Comment:
One commenter stated that there are some fundamental infrastructure challenges to implementing multi-year plans. The commenter mentioned maintaining accurate, auditable accumulators across a multi-year plan term, given that current health plan administration systems are designed around annual accumulator cycles, with deductibles and out-of-pocket maximums resetting January 1. The commenter stated that certification of multi-year plans should include an assessment of the issuer's infrastructure capability to manage multi-year accumulator lifecycles with audit-grade integrity.
Response:
As mentioned above, for out-of-pocket maximums, multi-year catastrophic plans would have their out-of-pocket maximums reset annually, to account for the updated out-of-pocket maximums that would apply for the next plan year. Thus, they could not have out-of-pocket maximums that accumulate across multiple plan years, nor could deductibles accumulate across multiple plan years. Therefore, there is no reason for our QHP certification processes to include an assessment of the issuer's infrastructure capability to manage multi-year accumulator lifecycles.
Comment:
One commenter stated that multi-year catastrophic plans in each market area should also be limited to issuers that have already sold plans in the Affordable Care Act's Exchange for several years—and these issuers should each be limited to offering a single multi-year plan. The commenter stated that this would also deter issuers from neglecting or abandoning mature plans with sicker pools of enrollees. Another commenter stated that limiting the proposal initially to catastrophic multi-year plans with a 2-year term would allow for a controlled pilot, minimizing systemic risk while enabling regulators and interested parties to monitor outcomes and gather data.
Response:
We might consider future rulemaking to propose expanding the standards in these final regulations to other types of plans, but first, we wish to evaluate the experience of issuers and enrollees in multi-year catastrophic plans. If we were to limit these final regulations to the types of issuers or to the contract duration the commenters mention, we do not believe we would have a sufficient universe of issuer and longer-term enrollee experience with such plans to be able to make such an evaluation. We note that to the extent the issuer of a multi-year catastrophic plan discontinues the product, an enrollee would have the same legal protections under special enrollment and under open enrollment periods to select another plan, and the same plans from which to select, as do enrollees in 1-year plans that an issuer might discontinue. Therefore, there is no reason to limit the universe of multi-year catastrophic plans in the manner the commenters suggest. Additionally, given the aforementioned benefits that we believe multi-year plans can afford enrollees, we do not want to arbitrarily limit the universe of issuers that may offer such plans, provided they comply with all applicable requirements.
Comment:
For our comment solicitation on if, and to what degree, a plan could modify the amount of the annual deductible for each year of a multi-year plan, one commenter stated that allowing plans to collect more premiums or submit patients to higher cost sharing on the front end as a way to “entice” participants to remain in the plan for its duration do not align with the inherent purpose of these statutory limits to protect patients from untenable out-of-pocket costs in a given plan year and should not be allowed. However, this same commenter stated that, regarding mid-plan changes for multiple-year plans, if term changes would benefit the patient, such as reduced deductibles or cost sharing to entice a patient to remain enrolled in a particular plan, these changes should be permitted.
Another commenter stated that multi-year plans should allow deductible carryover or premium stability features—for example, if an enrollee does not meet the deductible in year one, the issuer could offer premium stability or enhanced benefits in subsequent years. This commenter also stated multi-year plans should be permitted to incorporate higher out-of-pocket cost exposure in early years paired with reduced exposure, enhanced benefits, or premium stability in subsequent years for continuously enrolled individuals, while another commenter stated that multi-year plans should be permitted to provide upfront pledges of rebates to premiums for those who remained enrolled.
Another commenter stated that people often cannot predict when they will experience a health condition. This commenter and other commenters stated that front-loading cost sharing early in a multi-year term will lead people to forego needed care early, leading to high costs and suffering. Several commenters stated it is unreasonable for enrollees to be expected to pay higher cost sharing in the early years of a term, as they might not be able to afford to. Other commenters stated that multi-year designs can create consumer expectations that value will accrue over time (for example, if cost sharing is structured to be less burdensome later in the term), but if a product is discontinued mid-term, or if CMS were to later prohibit this practice, enrollees may not be able to realize the benefit trajectory that was offered at enrollment. According to one commenter, this risk is structural and is not fully addressed through general disclosures.
Response:
We appreciate the comments we received on this topic. However, section 1302(e) of the Affordable Care Act prohibits catastrophic plans from covering any benefits, other than as provided for in section 2713 of the PHS Act and at least
( printed page 29687)
three primary care visits, until an enrollee has satisfied the annual limitation on cost sharing for the applicable plan year, as determined by statute. This means catastrophic plans cannot impose a deductible or annual limitation on cost-sharing other than the applicable limit on cost sharing for the applicable plan year. Therefore, we are not finalizing the provision in proposed § 156.130(c), which would have provided that, in the case of a multi-year catastrophic plan, the annual limitation on cost sharing for the initial plan year of the contract may apply on an annual basis, or on average over the life of the contract.
However, varying cost sharing by plan year in a manner that deviates each year's cost sharing from its statutory limitation on cost sharing would not be statutorily prohibited for other metal-level plans and might be a very appealing feature to some enrollees. Unlike catastrophic plans, which are prohibited from setting their annual limitation on cost sharing for a plan year above or below the applicable limit for that plan year, metal-level plans may set their annual limitation on cost sharing for a plan year below the statutory limitation for that plan year, provided the plan satisfies the appropriate actuarial value standards for its metal tier.[258]
Thus, multi-year metal-level plans would have flexibility to set an annual limitation on cost sharing that declines each year over the life of the contract, provided it is below the statutory limitation for each plan year. We also note that, unlike catastrophic plans, the deductible for a metal-level plan for a given plan year does not have to equal the annual limitation on cost sharing for that plan year, and metal-level plans are permitted to provide benefits following satisfaction of the plan's deductible, before the annual limitation on cost-sharing is met.
Insurance with vanishing or reduced deductibles over the life of the insurance contract has become more common in certain insurance markets such as automobile insurance. We believe such a feature has the potential to be of great value to both issuers and enrollees in the health insurance context. To the extent the promise of more generous coverage as a plan term progresses would cause an enrollee to remain in the plan, this would help further ensure that an issuer's focus on offering preventive and wellness benefits in the earlier years of the term might pay off in the form of a healthier enrollment base, which could encourage issuers to focus on offering and promoting such benefits. Also, the promise of more generous benefits in later years of the term might incentivize enrollees to remain in their plan, even after carefully considering other options, as the increased benefits might be superior to those other options. Depending on issuers' and enrollees' experience with multi-year catastrophic plans, we might consider through rulemaking extending multi-year standards to metal level plans, including applying the declining cost sharing concept to such plans.
We note that multi-year and 1-year catastrophic plans may be able to offer relief from the high deductible and maximum annual limitation on cost sharing through other mechanisms. For example, issuers of catastrophic plans could consider financing the deductible by providing enrollees a loan. To the extent permitted by applicable Federal and State law, this could be especially helpful for enrollees who, before reaching their deductible, incur a large amount of medical costs within a short period of time. Under this approach, as long as the loan terms require repayment, the plan would not be considered to be covering those services prior to satisfaction of the deductible for purposes of section 1302(e)(1)(B)(i) of the Affordable Care Act. To the extent permitted by applicable Federal and State law, issuers of multi-year catastrophic plans could offer repayment flexibility as defined in the loan contract with the enrollee.
For the comment suggesting an adjustment to an individual's premium from one year within a multi-year catastrophic plan to the next, based on whether or not the individual had satisfied their deductible, we note that such an adjustment, or any other based on a factor other than those permitted in § 147.102(a), is prohibited.
Comment:
Several commenters discussed the idea of the annual limitation on cost sharing being prorated on a monthly basis. One commenter stated that allowing enrollees to meet one-twelfth of the annual limitation per month, after which the plan would cover benefits for that month (other than for preventive services, or primary care visits below the applicable threshold) would violate section 1302(e) of the Affordable Care Act, as it would allow issuers to cover benefits in a plan year prior to the enrollee incurring expenses equal to the annual limitation.
A few commenters stated that allowing the annual limitation on cost sharing to be prorated on a monthly basis would help to alleviate up-front “shock” of high out-of-pocket costs. Another commenter stated that allowing deductibles or limitations on cost-sharing thresholds to reset on a monthly or similarly frequent basis would undermine the core purpose of catastrophic coverage by repeatedly restarting a consumer's financial exposure during ongoing treatment. One commenter stated that an annual limitation on cost sharing that is prorated monthly could be significantly favorable to consumers in lowering limitations on cost sharing for specific services within a month. However, this commenter pointed out that a range of challenges exist, including that claims can take 6 months or more to be paid. This commenter stated that, at most, that means the payment can occur in the next plan year, but potentially 6 or more monthly limitation on cost sharing cycles, which could lead to consumer confusion and additional administrative complexity. This commenter also stated that new consumer utilization patterns such as stacking services within a month to take advantage of the lower limitations on cost sharing could arise, particularly if multiple, higher cost elective services are in play. The commenter stated that this could lead to material increases in actuarial value which, if unpriced for, could create significant solvency challenges. This commenter also stated that current actuarial continuance does not take into account how consumer behavior might change under a monthly benefit.
Another commenter stated that smaller monthly limits would help both acute and chronic patients by limiting the one-time cost burden for the former and spreading known, recurring costs over the year for the latter. This commenter stated that limiting monthly cost sharing to one twelfth of the annual limit will likely benefit individuals with single acute medical events, while being harmful to either healthy individuals who face higher premiums if actuarial value increases or to individuals with chronic medical costs if actuarial value is held constant but monthly limits increase.
Response:
We appreciate the comments submitted on this topic. As stated above, section 1302(e)(1)(B)(i) of the Affordable Care Act states, in
( printed page 29688)
relevant part, that a catastrophic plan “provides no benefits for any plan year until the individual has incurred cost-sharing expenses in an amount equal to the annual limitation in effect under subsection (c)(1) for the plan year.” Therefore, a plan that prorates the annual limitation on cost sharing on a monthly or other basis would not meet the statutory definition of a catastrophic plan. We stated above how a catastrophic plan, to the extent permitted by applicable law, may exercise loan repayment flexibility to protect enrollees from high deductibles and maximum out-of-pocket costs. However, should we propose, in a separate rulemaking, standards for metal-level plans to have multi-year terms, we note that monthly prorated deductibles could be permissible under applicable statute. This is because for metal-level plans, the deductible can be an amount different than the maximum limitation on cost sharing, and Federal law does not prohibit metal-level plans from providing coverage for costs incurred below the maximum limitation on cost sharing set by the plan. As we stated above, depending on issuers' and enrollees' experience with multi-year catastrophic plans, we might consider proposing through rulemaking standards for issuers of metal-level plans to offer plans with multi-year terms as set forth for catastrophic plans in this final rule, at which time we might propose to allow annual deductibles to be prorated monthly or over another interval.
Comment:
Several commenters suggested that disease-specific annual limitations on cost sharing in multi-year catastrophic plans would discriminate based on health status, in violation of several different Federal statutes. One commenter stated that disease-specific limitations on cost sharing would also create significant confusion for both physicians and patients, particularly for individuals with multiple chronic conditions whose care cannot be attributed to a single diagnosis. Another commenter stated that such limitations would allow issuers to design plans that are highly unattractive to sicker people, while one commenter stated that a limitation on cost sharing based on disease should not be permitted if prohibited by State law.
Response:
We are not finalizing the provision in the preamble to the proposed rule that would have permitted disease-specific limitations on cost sharing if that disease requires treatment that spans multiple years, so long as the average over all plan participants and over years of the annual limitation on cost sharing equals the average over the life of the contract of the annual limitation on cost sharing as required by statute. As stated above, the limitation on cost sharing for each plan year of a catastrophic plan must equal the statutory maximum annual limitation on cost sharing for that plan year and cannot vary by disease or other health status.
Comment:
One commenter noted that multi-year plan terms can be misaligned with current employer plan cycles, and expressed concern about potential administrative and compliance complexities of attempting to align multi-year plans with annual employer benefit updates, such as for ICHRAs and qualified small employer health reimbursement arrangements (QSEHRAs).
Response:
Group health plans and QSEHRAs are not always offered by employers on a calendar year cycle, and therefore might not align with individual health insurance coverage. Therefore, the issue the commenter mentions is not unique to multi-year plans. The Departments continue to see great promise in ICHRAs and QSEHRAs, and will continue to examine how to make them easier and more attractive for employers to offer, including examining how such arrangements could be integrated with multi-year catastrophic plans.
Comment:
One commenter remarked that States will need clear guidance regarding expectations for review and oversight.
Response:
As the market for multi-year catastrophic plans develops, we expect to provide such guidance, and we welcome suggestions from States in this regard.
Comment:
One commenter suggested that CMS monitor enrollment in multi-year catastrophic health plans and their impact on individuals with chronic conditions or disabilities and report these data publicly.
Response:
We appreciate the comment, and it is something we might consider doing in the future.
Comment:
One commenter suggested stronger pre-enrollment counseling about multi-year catastrophic plans for high-risk applicants.
Response:
We agree that it is important for individuals to understand their coverage options prior to enrollment. We encourage agents, brokers, web-brokers, and assisters to help consumers evaluate whether a multi-year catastrophic plan meets their needs. We expect to issue materials to assist such parties and issuers in that regard.
Comment:
We received several comments related to the proposal that multi-year catastrophic plans with a plan term of at least 2 consecutive years may utilize VBID to provide benefits for preventive services under section 2713 of the PHS Act beyond those specified in section 2713(a)(1) through (a)(4) prior to the enrollee's satisfaction of the plan's deductible and prior to satisfying the plan's annual limitation on cost sharing. Several commenters supported allowing multi-year catastrophic plans to utilize VBID to cover additional preventive services before the plan's deductible and annual limitation on cost sharing is satisfied. Other commenters opposed this approach. They stated that the Secretary's authority under section 2713(c) of the PHS Act does not permit expanding the types of services that catastrophic plans may cover before an individual satisfies their deductible or annual cost-sharing limitation. Commenters also stated that VBIDs referenced in section 2713(c) of the PHS Act are not intended to refer to preventive services beyond those listed in section 2713(a)(1) through (a)(4) of the PHS Act.
Response:
Section 2713(c) of the PHS Act states, the Secretary may develop guidelines to permit a group health plan and a health insurance issuer offering group or individual health insurance coverage to utilize value-based insurance designs. This provision contains no language restricting VBID to the specific categories of preventive services enumerated in section 2713(a) of the PHS Act. Section 1302(e) of the Affordable Care Act provides that a catastrophic plan provides no benefits for any plan year until the enrollee has incurred cost-sharing expenses in an amount equal to the annual limitation on cost sharing, except for at least three primary care visits and “except as provided for in section 2713” of the PHS Act. The statute cross references section 2713 in its entirety, not solely subsection (a). Accordingly, section 1302(e) of the Affordable Care Act incorporates both the mandatory coverage requirements set forth in section 2713(a) of the PHS Act and the Secretary's authority under section 2713(c) of the PHS Act to permit VBID. Reading these provisions together, catastrophic plans may provide pre-deductible coverage for benefits furnished under VBID guidelines issued under section 2713(c) of the PHS Act.
Prior sub-regulatory guidance issued by the Departments has generally described VBID as health plan designs that provide incentives for enrollees to utilize higher-value and/or higher-
( printed page 29689)
quality services or venues of care.[259]
While we acknowledge the Departments have made other statements associating VBID with preventive health services, those statements were made in the context of rulemaking regarding coverage of recommended preventive services and should not be construed to limit the VBID construct to recommended preventive services enumerated in section 2713(a) of the PHS Act.[260]
Having reexamined the statutory delegation in section 2713(c) of the PHS Act, we conclude that the plain text of the statute contains no language restricting the guidelines developed for VBID to the specific categories of preventive services enumerated in section 2713(a). The approach finalized in this rule is consistent with that understanding and with prior HHS rulemakings [261]
encouraging issuers within the individual and small group market to design plans that empower consumers to receive high-value services at lower cost.
The Departments believe that incentivizing high-value care, including utilization of services related to wellness and prevention, has the potential to improve health outcomes and therefore reduce utilization and plan expenditures over time, in a number of ways. Issuers of multi-year plans would be uniquely suited to reap the benefits of a healthier population that remains in the plan over several years. One way of achieving this is through an adjustment to the out-of-pocket cost of services if furnished by certain providers, to encourage enrollees to seek services from lower-cost providers. For example, the preventive service regulations at 26 CFR 54.9815-2713(a)(3), 29 CFR 1590.715-2713(a)(3), and 45 CFR 147.130(a)(3) generally permit group health plans and group and individual health insurance coverage that have a network of providers to impose cost-sharing requirements on recommended preventive services delivered by an out-of-network provider. Another such potential way is by promoting, via cost saving incentives, services linked to emerging technologies, or services that have been identified as reducing morbidity or severity of illness, including services for which new evidence demonstrates that the health benefits outweigh their cost. We believe that for all these reasons, VBID might have positive, valuable implications for issuers of multi-year plans, and for their enrollees.
For these reasons, consistent with the delegation of authority in section 2713(c) of the PHS Act, we are finalizing the proposed provision at § 156.155(a)(6) with modifications to state that multi-year catastrophic plans may utilize VBID to provide benefits before reaching the deductible, pursuant to guidelines issued by the Departments under section 2713(c) of the PHS Act. Accordingly, the Departments intend to issue guidelines on how plans and issuers may implement VBIDs, including the scope of services that may be offered with reduced or no cost sharing in a manner designed to promote high-value care. The Departments intend to issue these guidelines in the near future. Until the guidelines are issued and applicable, multi-year catastrophic plans may provide pre-deductible coverage only for preventive services described in section 2713(a) of the PHS Act and benefits for at least three primary care visits per year.[262]
We are also finalizing a conforming amendment at § 156.155(a)(3), providing that catastrophic plans provide no benefits before the annual limitation on cost sharing is reached, except as provided in paragraph (a)(6).
Comment:
Several commenters stated concern that enrollees could be “locked into” multi-year catastrophic plans.
Response:
Enrollees may terminate coverage in multi-year catastrophic plans at any time without penalty. They may also enroll in other coverage during the annual open enrollment period or special enrollment periods, if otherwise eligible.[263]
Therefore, they will not be locked into multi-year catastrophic plans. We acknowledge that certain benefit designs may create incentives to remain enrolled, and we expect issuers to disclose those features. To the extent those benefit designs cause individuals to remain enrolled, they would be doing so by choice, not because they are “locked into” their plan.
Comment:
Some commenters stated that multi-year plans would not reduce the churn and disputed that coverage in a multi-year plan is materially different than 1-year contracts for health insurance coverage.
Response:
We do not expect multi-year plans to eliminate churn. However, we believe the extended contract term of these plans has the potential to reduce churn for some enrollees, particularly where plan features make continued enrollment attractive. As previously stated, issuers of multi-year catastrophic plans would have more incentive to promote preventive and wellness benefits for their enrollees. In so doing, this could lead to a healthier enrolled population, resulting in moderated premiums, which is a major factor for consumers when choosing to remain in coverage. We also disagree that multi-year catastrophic plans could not be materially different from plans with a standard 1-year contract term. For example, as described above, we are finalizing that multi-year catastrophic plans could implement VBID, under guidelines issued by the Departments under section 2713(c) of the PHS Act. Such a design could potentially offer valuable benefits that are typically not offered by 1-year plans. We also note that Germany offers an example of how the availability of plans with terms that exceed 1 year has potential to reduce churn. Although many different public health insurance plans are offered with indefinite term lengths in Germany, and even though enrollees can switch plans annually, 39 percent never switch plans in their lifetime.[264]
Comments:
Some commenters expressed concern that enrollees in multi-year plans may not reassess coverage annually.
Response:
The high level of churn in the individual health insurance market among individuals who are not automatically re-enrolled in coverage through an Exchange suggests that a significant number of consumers reassess their coverage annually, and there is no reason to believe that consumers enrolled in multi-year catastrophic plans will not do so, although as stated above, it is our view that many consumers in such plans, even after reassessing their coverage options, may decide to remain in their multi-year plan, given the potential
( printed page 29690)
advantages outlined above for doing so, such as the positive impact of VBID programs.
Comment:
One commenter stated that multi-year plans would limit enrollment in later years, which would violate guaranteed availability.
Response:
Multi-year catastrophic plans must comply with all applicable requirements for health insurance coverage in the individual market, including the guaranteed availability requirements under section 2702 of the PHS Act. Individuals who qualify for catastrophic coverage may enroll in a multi-year catastrophic plan during open enrollment or a special enrollment period, if otherwise eligible, regardless of when the plan was first offered to other policyholders. For example, if an issuer offers a multi-year plan with a contract term of 10 consecutive plan years, and an eligible individual wishes to newly enroll in the plan, the issuer would be required under guaranteed availability to accept that individual for a coverage term that starts in the calendar year in which the individual first enrolled, and ends on December 31 of the calendar year that is 9 years after the calendar year in which the individual first enrolled. This is true, regardless of how many years the issuer had been offering that plan prior to the plan year for which the applicant first seeks coverage under the plan.
Comment:
One commenter stated that issuers should not be required to offer multi-year catastrophic plans and that States should be able to restrict or prohibit these plans.
Response:
We agree. This final rule establishes a regulatory framework for multi-year catastrophic plans. It does not require issuers to offer multi-year catastrophic plans nor limit the ability of States to restrict or prohibit them.
Comment:
Commenters stated mixed views on extending multi-year plan standards to metal-level plans. One commenter supported applying the standards across all metal tiers to maintain competitive balance. Other commenters opposed or recommended delaying any extension until impacts are better understood. Several commenters cited insufficient detail to evaluate the proposal and its extension to other plans. One commenter noted that lower cost sharing in metal-level plans compared with catastrophic plans increases issuer risk and may discourage multi-year plan offerings at other metal levels without greater rating flexibility. Some commenters also raised potential legal barriers related to pre-verification requirements for PTC-eligible coverage under section 71303 of the WFTC legislation.
Response:
Given the newness of this concept to health insurance in the United States, we are not extending multi-year standards to metal-level plans in this final rule. We will evaluate experience with multi-year catastrophic plans and engage in dialogue with States, issuers and others to inform potential future policy proposals related to multi-year plans.
Comment:
Many commenters stated that the MLR considerations in the context of multi-year plans that were outlined in the proposed rule are important and urged HHS to clarify how such plans would be treated for MLR purposes before implementing the proposal. One commenter suggested that multi-year plans continue to be subject to the existing MLR standards. Another commenter suggested that a multi-year aggregation method for MLR purposes could be more appropriate to account for potentially lower claims in the early years of the policy.
Response:
We appreciate these comments and appreciate the two commenters that offered substantive suggestions related to the MLR standards and methods applicable to multi-year catastrophic plans. We note that section 2718(b)(1)(B)(ii) of the PHS Act already requires the MLR to be calculated annually based on the average of 3 years of experience. In addition, issuers will be issuing new cohorts of multi-year policies each year, and multi-year plans will be aggregated with other individual market plans in the MLR calculation. Therefore, over time, we do not expect the timing of multi-year plan claims to significantly impact MLRs. Given the absence of other specific recommendations, we are not making any changes to the treatment of multi-year plans for purposes of MLR and rebate calculation and reporting requirements under part 158 in this rulemaking.
7. Cost Sharing for Bronze and Catastrophic Plans (§§ 156.136 and 156.155)
To address an issue that has arisen in the implementation of section 1302(c) through (e) of the Affordable Care Act, in the 2027 Payment Notice proposed rule (91 FR 6373), we proposed changes to the permissible cost-sharing parameters for individual market bronze plans through new proposed § 156.136 and to the required cost-sharing parameters for catastrophic plans through revisions to § 156.155(a)(3).
Section 1301(a)(1)(B) of the Affordable Care Act directs all issuers of QHPs to cover the EHB package described in section 1302(a) of the Affordable Care Act, which includes coverage of the benefits described in section 1302(b) of the Affordable Care Act, adherence to the cost-sharing limits described in section 1302(c) of the Affordable Care Act, and meeting the AV levels established in section 1302(d) of the Affordable Care Act.
Section 2707(a) of the PHS Act, which is effective for plan or policy years beginning on or after January 1, 2014, extends the requirement to cover the EHB package to non-grandfathered individual and small group health coverage, irrespective of whether such coverage is offered through an Exchange. In addition, section 2707(b) of the PHS Act directs non-grandfathered group health plans to ensure that cost sharing under the plan does not exceed the limitations described in section 1302(c)(1) of the Affordable Care Act.
Section 2707(a) of the PHS Act and section 1302 of the Affordable Care Act direct issuers of non-grandfathered individual and small group health insurance plans (including QHPs) to ensure that these plans adhere to the levels of coverage specified in section 1302(d)(1) of the Affordable Care Act (except for catastrophic plans described in section 1302(e) of the Affordable Care Act). Section 1302(c) of the Affordable Care Act limits the annual cost sharing incurred under a health plan to the maximum annual limitation on cost sharing. Section 1302(d)(2) of the Affordable Care Act provides that a level of coverage of a plan, or its AV, is determined based on its coverage of the EHB for a standard population. Section 1302(d)(1)(A) through (D) of the Affordable Care Act requires a bronze plan to have an AV of 60 percent, a silver plan to have an AV of 70 percent, a gold plan to have an AV of 80 percent, and a platinum plan to have an AV of 90 percent. Section 1302(d)(2) of the Affordable Care Act directs the Secretary to issue regulations on the calculation of AV and its application to the levels of coverage. Section 1302(d)(3) of the Affordable Care Act requires the Secretary to develop
de minimis
variations in AV calculations.
Section 1302(e) of the Affordable Care Act permits an individual market health plan not providing a bronze, silver, gold, or platinum level of coverage to be a catastrophic health plan that is treated as meeting the levels of coverage specified in section 1302(d)(1) of the Affordable Care Act for a plan year. A catastrophic plan may be offered only in the individual market and only to qualified individuals who have not attained age 30 before the beginning of the plan year, or to qualified individuals who are exempt from the requirement to
( printed page 29691)
maintain minimum essential coverage under section 5000A of the Internal Revenue Code by reason of a hardship exemption or an exemption described in section 5000A(e) of the Internal Revenue Code relating to the affordability of coverage. Catastrophic coverage must provide coverage for the EHB and must meet the statutory requirement to cover at least three primary care visits before the plan deductible is applied. In addition, catastrophic plans must comply with all other requirements applicable to QHPs except those specifically modified by section 1302(e) of the Affordable Care Act, and they must be offered through the Exchange in the same manner as other qualified health plans. We codified the requirements for catastrophic plans at § 156.155 in the Exchange Establishment Rule.
In the proposed rule, we provided an overview of how HHS has implemented the AV requirements of the Affordable Care Act, including a discussion of the major components of AV calculation. We reiterate this overview in the sections that follow. In the proposed rule, we went on to explain that we have discovered an inherent and unavoidable issue for implementation of the cost-sharing provisions of the EHB package in section 1302(c) through (e) of the Affordable Care Act that will eventually make issuer compliance with all these provisions mathematically impossible. We noted that this issue has first become evident for bronze and catastrophic plans, though without further changes, it will eventually impact silver plans and plans at higher metal tiers. To mitigate the worsening issue, in the proposed rule, we proposed to create new optional cost-sharing parameters for bronze plans and to revise the cost-sharing requirements for catastrophic plans in the individual market only.
a. The Three Major Components of AV Calculation
AV is the anticipated covered medical spending for coverage of EHB [265]
paid by a health plan (1) for a standard population, (2) computed in accordance with the plan's cost sharing (that is capped by the maximum annual limitation on cost sharing), and (3) divided by the total anticipated allowed charges for EHB coverage provided to the standard population. The denominator of this calculation is the average allowed cost of all services for the standard population in the year for a specified metal tier; the numerator is the share of average allowed cost covered by the health plan, using the cost-sharing parameters specified. These are the three major components of AV calculation, and year-over-year changes in each of them influence how AV calculation changes year-over-year.
AV Component #1: The Standard Population.
In accordance with section 1302(d)(2)(A) of the Affordable Care Act, HHS develops and provides a standard population for the AV Calculator that resemble enrollees who are likely to be covered by individual and small group market health insurance in a particular year. The costs and utilization of this population are currently derived from the enrollee-level EDGE data. As the AV Calculator Methodology that HHS releases each year in connection with the AV Calculator describes in detail,[266]
we apply adjustments to the claims and enrollment data of the standard population, including weighting to account for the expected demographic distribution across individual and small group plans, and use it to create a series of continuance tables that underlie the AV Calculator. Our annual updates to the AV Calculator's standard population ensure accordance with generally accepted actuarial principles and methodologies. Generally, the claims and enrollment data indicate that the standard population is costlier to cover each year, which leads to a corresponding rise in AV each year. If we did not update the AV Calculator to account for changes in the standard population, the AV Calculator would not accurately account for the enrollees who are likely to be covered by individual and small group market health insurance in a particular year, and would be increasingly nonrepresentative of the people who enroll in metal-tier plans.
AV Component #2: The Maximum Annual Limitation on Cost Sharing.
Section 1302(c) of the Affordable Care Act sets the maximum annual limitation on cost sharing [267]
which limits an enrollee's overall financial responsibility by restricting the maximum out-of-pocket (MOOP) limit for a plan. For PY 2014, section 1302(c)(1)(A) of the Affordable Care Act sets this limit at the maximum cost-sharing limit for high-deductible health plans (HDHPs) under section 223(c)(2)(A)(ii) of the Internal Revenue Code of 1986—that is, $6,350 for a self-only plan. Section 1302(c)(1)(B) of the Affordable Care Act requires HHS to update the maximum annual limitation on cost sharing annually. For plan years after 2014, section 1302(c)(1)(B)(i) of the Affordable Care Act sets the limit for a self-only plan at the product of the 2014 value and the PAPI, the percentage (if any) by which the average per capita premium for health insurance coverage for the preceding calendar year exceeds such average per capita premium for health insurance coverage for 2013.[268]
Under section 1302(c)(1)(B)(ii) of the Affordable Care Act, the maximum annual limitation on cost sharing for other plans, like coverage other than self-only, is twice the limit of a self-only plan. In accordance with § 156.130(e), in years where HHS is not making methodological changes, HHS will release the PAPI in guidance that will include the maximum annual limitation on cost sharing amount for the applicable benefit year.[269]
Using PAPI, the maximum annual limitation on cost sharing for self-only coverage has risen from $6,350 in PY 2014 to $12,000 in PY 2027 (see Table 9).
( printed page 29692)
The maximum annual limitation on cost sharing impacts AV calculation since it changes the maximum amount that an enrollee may have to pay out-of-pocket each year. When the maximum annual limitation on cost sharing increases from year-to-year (which it typically does), it has the effect of decreasing year-over-year AVs. This is because plans can increase their MOOPs with a higher maximum annual limitation on cost sharing, which means enrollees typically need to pay more out-of-pocket for the EHB than they did in previous years, which would lower AV.
AV Component #3: EHB Costs.
We also adjust the AV Calculator each year with an update to the cost of EHB that is provided to the AV Calculator's standard population, again to ensure accordance with generally accepted actuarial principles and methodologies and section 1302(d)(2)(A) of the Affordable Care Act. We project historical claims data for medical items and services and prescription drugs covered as EHB for the standard population for the next plan year. We often refer to this projection as the “trend factor.” For years that we used a trend factor in the AV Calculator, we have set it for an increase of between 3.25 percent and 6.50 percent for medical costs and between 6.50 percent and 11.50 percent for prescription drug costs.[270]
Table 10 sets forth the AV Calculator trend factors from 2014 to 2026.
( printed page 29693)
We review a variety of data sources on medical services and prescription drug claims costs, including rate data from the Unified Rate Review Templates (URRTs) and National Health Expenditure data from the HHS Office of the Actuary, to develop and select the proposed adjustment to health care costs. This health care cost update also impacts AV calculation; as health care becomes more expensive, the generosity of a plan's AV increases as an enrollee needs to receive less medical care than in previous years to reach the maximum annual limitation on cost-sharing. If we did not apply this trend factor, the AV Calculator would not account for changes in the cost of health care and would be less and less accurate each year, inconsistent with section 1302(d)(1)(A)'s instruction to calculate AV based on the “actuarial value of the benefits provided under the plan.”
b. The Rates of Change for the Three Major AV Components
As we stated in the proposed rule, together, these three major components of AV calculation affect AV differently each year, depending on how the health of the standard population, the maximum annual limitation on cost sharing, and EHB costs all change, and at different rates. We noted that, ideally, the effect of a higher statutory maximum annual limitation on cost sharing each year would allow plans to exactly offset the year-over-year increase on AV created by the more expensive standard population and increased EHB costs required by the statute. We stated that would mean that the net impact of the three major factors on AV would be zero each year, and in turn any particular plan with the same cost-sharing structure would have the same AV year-over-year. We further stated that we believe this is the actuarially preferred approach, because it would allow for relatively consistent cost sharing and benefits design year-over-year, which promotes consumer understanding. We noted, however, plans do not have the same AVs each year because the three factors change at different rates.
We stated in the proposed rule that for nearly every year since 2014, the effect of updating the AV Calculator with the most recent data on the standard population and health care costs has led to a faster rise in AV with the same cost sharing structure than can be mitigated by the effect that a higher maximum annual limitation on cost sharing has on decreasing AV.[271]
We stated that, in other words, the effects of updating the standard population and health care costs every year to maintain the accuracy of AV calculations typically results in AVs increasing year-over-year, and the effects of an increased maximum annual limitation on cost sharing make AVs decrease year-over-year, but not enough to offset health care costs in the standard population. We noted that this is the outcome of the PAPI—calculated from the percentage difference between the average per capita premium for health coverage for the preceding calendar year and the average per capita premium for health coverage for 2013—being outpaced by the increasing costs of the health care for the population enrolling in metal-tier plans. We stated that this means we expect that a particular plan with the same cost-sharing structure has a
higher
AV year-over-year, even if
( printed page 29694)
nothing about the plan changes. We noted that we discussed this previously as long ago as 2016 in the 2018 Payment Notice proposed rule [272]
and most recently in the Marketplace Integrity and Affordability final rule.[273]
We noted in the proposed rule that this shift often forces issuers to change other parts of a plan's cost-sharing structure (to make the plan less generous) to conform to the relevant
de minimis
ranges that we permit for plans at § 156.140 in accordance with section 1302(d)(3) of the Affordable Care Act. We stated that such changes are not actuarially sound, because the same plan, with the same cost-sharing structure, should have generally the same AV year-over-year. Over the years, as stated below, we have also modified the methodology by which issuers calculate AV, in an effort to mitigate some of these challenges. However, we stated that modifications made to ensure that plans at a certain metal tier can continue to exist do not carry the level of fidelity to AV calculation that may be justified by generally accepted actuarial principles and methodologies, and we stated that we believe we have reached a point at which further modifications would undermine the integrity of AV calculation and threaten our ability to implement section 1302(d) of the Affordable Care Act in such a compliant manner.
We stated in the proposed rule that the discrepancy in the rates of change of the three components have a magnified effect on the ability of issuers to design plans that conform to the
de minimis
ranges or that offer what issuers consider desirable; thus, issuers have narrower options to adjust cost sharing in their plan offerings each year. We further stated that if current trends persist, eventually the maximum annual limitation on cost sharing will be too low to allow for an AV calculation for the most basic bronze plan design, with a deductible set to the maximum annual limitation on cost sharing, that is within widened
de minimis
ranges, even with the use of an AV Calculator that caps claims. Thus, we stated that an actuarial issue exists in the implementation of the statutory text of section 1302(c) through (e) of the Affordable Care Act and the observed differences in the trend rates of the competing factors: PAPI (setting the maximum annual limitation on cost sharing and therefore plans' MOOP limit) and AV (which rises with increasing claims costs), discussed in greater detail in later lettered subsections.
We also stated that since we expanded the bronze
de minimis
range in 2018, we have seen a clear increase in the percentage of bronze plans at the upper end of the permissible
de minimis
range (+5 percent). In 2025, approximately 18 percent of FFE bronze plans were not in the expanded
de minimis
range, down from approximately 81 percent in 2018.
We further
stated that, today, bronze plans appear increasingly more as silver plans than bronze plans. As previously noted, over the years we have changed the methodology underlying the AV Calculator (for example, by imposing a spending cap) and expanded the
de minimis
ranges (for example, by creating expanded bronze plans) to allow bronze
( printed page 29695)
plan viability. However, we stated that we believe further changes to the AV Calculator methodology and
de minimis
ranges for the purpose of preserving bronze plans would near the outer boundary of our statutory authority to address this issue under section 1302(d)(3) of the Affordable Care Act. We noted that when bronze plans have an AV between 62 and 65 percent, they are closer to the bottom of the silver
de minimis
range (66 percent) than they are to the bottom of the bronze
de minimis
range (56 percent or 58 percent, depending on the year). We stated that this clearly undermines the integrity of silver plan cost-sharing designs and makes it more difficult for consumers to distinguish between the two metal tiers.
However, we noted that the maximum annual limitation on cost sharing limits issuers' options in bronze plan design. We stated that we believe issuers may have designed competitive plans that would be attractive for bronze plan consumers but that are ineligible for sale because they need to have a higher MOOP than is permissible under the maximum annual limitation on cost sharing. Specifically, we stated that the existing permissible MOOP leads to issuers offering higher deductible bronze plans over time because costs have risen faster than the permissible MOOP, requiring plans to raise cost-sharing below the permissible MOOP to meet the AV range for bronze plans. We noted that by 2024, the average deductible for bronze plans exceeded $7,000. We further noted that with a $9,450 maximum annual limitation on cost sharing that year, these plans look increasingly like catastrophic plans with a deductible that is almost set to the maximum annual limitation on cost sharing, and this includes expanded bronze plans that have an AV of up to 65 percent. We stated that the convergence of non-expanded bronze plans with catastrophic plan design is even more stark when viewing the median (or midpoint) of the deductibles and MOOPs of all the bronze plans offered on the FFEs alongside the maximum annual limitation on cost sharing over the last few years (Table 12).
We noted in the proposed rule that this convergence in the deductible and MOOP in these plan designs with the maximum annual limitation on cost sharing occurred at the same time the AV of bronze plans increased (Table 11). We stated that if issuers lowered deductibles in existing bronze plans but held their MOOP and average copayment rate between the deductible and MOOP constant, those plans would have higher AVs and risk appearing more like silver plans than bronze plans, or having to meet the requirements described at § 156.140(c) to be an expanded bronze plan. We further noted that issuers could feasibly lower the AV of their bronze plans by raising the deductible in those plans, but few offer such plans (Table 11).
We also stated in the proposed rule that plans could increase their MOOP to offer plans with lower deductibles and copayment rates. We noted that variation in MOOPs and deductibles across bronze plans in 2024 reveals that, for the median bronze plan a $1 higher MOOP is associated with a 58 cent lower deductible. We also noted that there is less response to the MOOP in higher metal tiers, consistent with the idea that the MOOP affects deductibles more at lower AV levels. We stated, however, as claims continue to rise at a rate greater than the growth in the statutory maximum annual limitation on cost sharing (due to rising faster than the index calculated based on how much premiums have increased), a higher MOOP may eventually be warranted to tamp down deductibles for plans seeking to maintain their AV compliance with higher metal tiers than bronze, as well. We noted, however, the deductible and MOOP of most plan designs at the other metal tiers have not converged with the maximum annual limitation on cost sharing; in other words, silver plans and higher metal tier plans appear to still have appropriate flexibility in their cost sharing design, as observed by their wider ranges of deductibles, pre-deductible coverage, and MOOPs compared to non-expanded bronze plans (see Table 12).
We stated that, of the metal plans, bronze plans are most susceptible to increases in AV because they have the lowest AV (60 percent), and the highest allowable maximum annual limitation on cost sharing typically requires issuers to cover more than 60 percent of allowed claims. We further noted that issuers have fewer options to adjust the cost sharing for bronze plans compared to other metal level plans and, as noted previously, are increasingly designing them to have a deductible near or equal to the maximum annual limitation on cost sharing. To address this increase in AV for bronze plans in the short-term, we stated that we have already utilized the authority at section 1302(d)(3) of the Affordable Care Act to revise § 156.140(c) to expand the allowable de minimis range for bronze plans to a maximum of 65 percent AV, and refer to these plans as “expanded bronze” plans.[275]
As we stated in the proposed rule, we began to reduce the distortion created by outliers with very high spending in the AV Calculator's standard population beginning in 2021 by implementing a cap on enrollee spending at $1,000,000. In later years, we capped enrollee spending at the 99.50th percentile of annual allowed amounts for all enrollees in the claims data. We noted in the proposed rule that without this cap, many, if not all, bronze plan designs would already be non-viable. We stated, for example, that utilizing the 2027 version of the AV Calculator without the enrollment cap, we estimate that all bronze plan AVs would be 5 to 6 percentage points higher than with it. We also stated that based on internal analysis, all existing non-expanded bronze plans offered in the FFEs in PY 2026 would have an average AV of 65.1 percent if calculated using an AV
( printed page 29696)
Calculator that did not apply the enrollment cap. The simulated AV results ranged from 64.5 percent to 68.0 percent, which is much higher than the currently permitted maximum of 62 percent. We further estimated the effect on the other metal levels without the cap and found standard silver AVs would be 4 to 5 percentage points higher; gold plan AVs would be 1 to 2 percentage points higher; and platinum plan AVs would be up to 1 percent higher.
We stated in the proposed rule that as AVs increase year-over-year, absent some other administrable regulatory solution, we may need to consider continuously expanding the cap on enrollee spending beyond the 99.50th percentile to preserve plan design viability, particularly for bronze plans. We stated that we know expanding this cap is not a permanent solution. We noted that the AV Calculator becomes less accurate, and less representative of the standard population as more and more enrollees are excluded from it. Moreover, we noted that the continued cap expansion does not align with the statutory requirements for determining the AV. We stated that while the initial cap may have reasonably been set from the Secretary's discretion to define a standard population, the continued expansion of the cap clearly serves a separate purpose. We stated, however, without it, bronze plans will eventually become entirely non-viable, which is not a result that Congress could have intended. Thus, we stated that an issue exists in the implementation of sections 1302(c) through (e) of the Affordable Care Act and, to date, we have chosen to address it by applying flexibility in the determination of the AV. However, we stated that if current trends persist (and we have no reason to believe they will not), eventually the maximum annual limitation on cost sharing will be too low to allow for an AV calculation for a bronze plan design with a deductible set to the maximum annual limitation on cost sharing that is within widened
de minimis
ranges, even with an AV Calculator that uses a spending cap.
We stated in the proposed rule that we are not aware of any administrable, actuarially sound regulatory alternatives that we might propose that could address these issues to preserve the integrity of AV calculations and the comparability between the levels of coverage. As discussed above, we stated in the proposed rule that we can continue to expand the cap on enrollee spending beyond the 99.50th percentile as a temporary solution, but we hesitate to do so to preserve the integrity of AV calculations, as section 1302(d)(1)(A) of the Affordable Care Act directs the calculation of AV based on the “actuarial value of the benefits provided under the plan.” We noted in the proposed rule that we have also considered not trending the AV Calculator to account for changes in the standard population or for changes in EHB costs. We noted that this would make AV rise less quickly year-over-year. However, we stated that we believe doing so would render the AV Calculator wholly inaccurate actuarially. We also stated in the proposed rule that we have also considered proposing changes to EHB policy to reduce the scope of benefits that are covered as EHB to address this issue, but the calculation of AV does not so readily factor in the scope of covered benefits under the plan. We stated that we believe changing the current EHB benchmark framework and potentially making significant changes to covered benefits is an extreme approach that would yield minor benefits, if any because AV is a measurement of the cost sharing imposed by an issuer on whatever benefits the plan covers as EHB, and not a measurement of the EHB themselves. Additionally, as we noted in the proposed rule, section 1302(b)(2)(A) of the Affordable Care Act requires HHS to define the EHB to cover items and services covered within 10 specific categories of benefits such that their scope is equal to the scope of benefits provided under a typical employer plan; the statute does not create ability to define the EHB to accommodate AV calculations. In addition, we stated that we believe there are no changes to the PAPI methodology that would raise the annual limitation on cost sharing enough to preserve the viability of AV calculations, even in the short-term, though we solicited comment on whether there are any regulatory changes we might make to the PAPI that would address this AV issue.
We sought comment on other administrable regulatory alternatives that we might consider that could address these issues to preserve the integrity of AV calculations and the comparability between the levels of coverage long-term. However, we stated at the time of the proposed rule that we believed no administrable alternatives exist because the issue is one of innate mathematical incongruence, not methodological decisions. In the end, we stated that we believe the differing rates of changes between the three major factors of AV calculation pose an insurmountable regulatory problem created by the cost-sharing provisions of section 1302 of the Affordable Care Act.
c. Statutory Adherence
As discussed in the proposed rule (91 FR 6379), we proposed to revise the cost-sharing parameters for bronze plans and to revise the cost-sharing requirements for catastrophic plans, respectively, to adhere to the cost-sharing provisions of section 1302 of the Affordable Care Act, given this regulatory issue.
Consistent with longstanding principles of statutory interpretation, we sought to give effect to all provisions of the Affordable Care Act so that they operate together in a coherent structure.[276]
We stated in the proposed rule that the Supreme Court has recognized that agencies should adopt statutory interpretations that harmonize related provisions wherever possible and should implement statutes in a manner that advances the overall statutory scheme.[277]
However, where two statutory requirements cannot reasonably be satisfied simultaneously, an agency must act in a manner that best effectuates congressional intent and preserves the operability of the relevant statutory framework.[278]
We stated in the proposed rule that we believe that maintaining the AV requirement for metal-level plans is the more specific and operational statutory instruction, and adherence to it best serves Congress' intent. We stated that the AV requirement applies only to a defined subset of plans offered in the individual and small group markets, and establishes precise quantitative benchmarks that define the statutory coverage tiers themselves. We further stated that, by contrast, the maximum annual limitation on cost sharing applies broadly across all plan types and markets and functions as a general consumer protection ceiling rather than a plan-defining metric. In addition, we noted that compliance with the AV requirements necessitates detailed, plan-level calibration of cost-sharing parameters and is central to preserving Congress' deliberate creation of distinct
( printed page 29697)
metal-level coverage categories, whereas the maximum annual limitation on cost sharing operates as a uniform backstop that does not distinguish among plan types. Thus, we stated in the proposed rule that we are prioritizing the highly specific statutory AV requirement over the generally applicable maximum annual limitation on cost-sharing.
We stated in the proposed rule that interpreting the AV requirement as the more specific statutory directive is consistent with how the Affordable Care Act, as originally passed, treated another conflict between cost-sharing limits and AV calculations. As originally passed, the Affordable Care Act included an annual limitation on deductibles for employer-sponsored plans under section 1302(c)(2) of the Affordable Care Act.[279]
Recognizing that this limitation would conflict with the AV, the statute provided that the limitation “shall be applied in such a manner so as to not affect the actuarial value of any health plan, including a plan in the bronze level.” [280]
Congress ultimately entirely abandoned any limitation on deductibles for employer-sponsored plans in 2014, while leaving in place the relevant AV requirements.[281]
We stated that this statutory history suggests that Congress did not intend maximum annual cost-sharing requirements for employer-sponsored plans to disrupt the AV calculation requirements.
For these reasons, we concluded in the proposed rule that the proposals that followed represented a reasonable and legally permissible approach to implementing section 1302 of the Affordable Care Act that gives effect to Congress' core design of distinct coverage tiers while preserving the overall operability of the statutory framework. Accordingly, we stated that the proposals reflect our obligation to implement section 1302's interrelated provisions in a manner that is understandable and workable.
d. An Incremental Approach
In the proposed rule, we noted that any regulatory framework that permits plans to exceed the maximum annual limitation on cost sharing should be as limited as possible to still implement section 1302(c) through (e) of the Affordable Care Act so that these paragraphs operate together in as coherent a structure as Congress could have intended. We stated that since the issue becomes more pronounced each year due to the growing disparity in the rates of change among the three major components of AV calculation, absent a statutory change, we believe we should implement regulatory solutions in a gradual, proportional manner.
To that end, we stated that we view the set of proposals that followed as only the beginning of necessary regulatory changes to the cost-sharing parameters for metal-tier and catastrophic plans. Catastrophic and bronze plans are the two plans most demonstrably and presently affected by this issue, and so we proposed changes to the cost-sharing parameters for these plans first in the hopes of giving enrollees more PY 2027 options at lower premiums and with more attractive plan designs. Because we seek to minimize the extent that these plans may exceed the maximum annual limitation on cost sharing, we stated in the proposed rule that we anticipate proposing future amendments to the applicable regulations through notice and comment rulemaking to address other metal tiers—at the point that the growing disparity in the rates of change among the three major components of AV begins to affect these higher tiers, and after sufficient research into how to prevent unintended effects on the calculation of premium tax credits.
We stated in the proposed rule that, as demonstrated above, standard silver plans would already be non-viable if we had not already adjusted the standard population by capping enrollee spending at the 99.50th percentile of annual allowed amounts for all enrollees in the claims data. We stated that we considered proposing changes to the permissible cost-sharing parameters for silver plans in the proposed rule but chose not to at that time. Rather, we stated that our intent in the future would be to propose changes to the cost-sharing parameters for silver plans, when necessary, through future notice and comment rulemaking. Second-lowest cost silver plans are used as the benchmark to determine premium tax credit amounts. We stated that seeking changes to the permissible cost-sharing parameters for silver plans could have an outsized impact on the overall affordability of plans for subsidized enrollees, and we stated that we sought to minimize any destabilizing effects of the proposed policy by assuming such an incremental regulatory approach. We stated that for now, we would monitor and consider future incremental action we may take to change the cost-sharing parameters for the other metal tiers, and we invited comments about how we might calculate an appropriate threshold for flagging that the cost sharing incongruence is severely limiting silver plan design. We also sought comment on other implications that may exist for silver plans that do not exist for bronze and catastrophic plans.
e. Bronze Plan Cost-Sharing Parameters
To ensure that plans designated at the bronze metal level can continue to exist in the future and to also preserve a meaningful difference between the AVs of bronze and silver plans, which we believe was part of the congressional intent of having metal tiers, in the 2027 Payment Notice proposed rule (91 FR 6380), we proposed to add new § 156.136 that states, for plan years beginning on or after January 1, 2027, if an issuer offers a bronze plan (as defined at § 156.140(b)(1)) in the individual market that complies with the cost-sharing requirements at § 156.130 and the levels of coverage requirements at § 156.140, it may also offer, within the same service area, bronze plans that utilize a cost-sharing design that exceeds the maximum annual limitation on cost sharing at § 156.130 by amounts in increments of 50 dollars to achieve an AV within the standard bronze
de minimis
variation at § 156.140(c), calculated as described in § 156.135.
We further proposed, that, in order for an issuer to avail itself of the ability to offer individual market bronze plans that utilize a cost-sharing design that exceeds the maximum annual limitation on cost sharing, the issuer must also offer at least one individual market bronze plan in the same service area that utilizes a cost-sharing design that does not exceed the maximum annual limitation on cost sharing at § 156.130 and complies with the levels of coverage requirements at § 156.140. We stated that this proposed flexibility is necessary to support the design and offering of bronze plans with AVs closer to the 60 percent intended by the Affordable Care Act. We stated that the MOOP for such individual market bronze plans must be in increments of 50 dollars. Under the proposal, we stated that we would not specify a strict dollar amount as the upper bound by which issuers could exceed the maximum annual limitation on cost sharing; rather, issuers would calculate this amount so that it fits within the narrower bronze
de minimis
range at § 156.140(c). We stated that we do not believe it is necessary to set such an upper bound because plan MOOPs would still be restricted by the
( printed page 29698)
requirement that the plan's AV comply with the levels of coverage requirements at § 156.140. However, we sought comment on whether we should set a strict dollar amount as the upper bound by which issuers could exceed the maximum annual limitation on cost sharing upon finalization of this final rule, and if so, what the upper bound should be.
In addition, we noted in the proposed rule that limiting this additional flexibility for bronze plans to issuers that also offer a bronze plan that complies with the existing cost-sharing requirements in the same service area ensures that, to the extent a bronze plan is available, there would be at least one in the service area that meets the maximum annual limitation on cost sharing. We stated that by allowing a wider range of possible cost-sharing designs at the bronze metal tier in the individual market, we would create opportunities for issuers to offer plans that are appealing to more consumers with lower premiums and more pre-deductible coverage than would have been possible without this proposal.
In the proposed rule, we considered imposing no precondition that issuers offer a bronze plan within the same service area that utilizes a cost-sharing design that does not exceed the maximum annual limitation on cost sharing at § 156.130 to offer bronze plans that utilize a cost-sharing design that exceeds the statutory maximum annual limitation on cost sharing. However, we stated that we believe the precondition is necessary at this time because bronze plans are barely still viable in 2027 without the 99.50th percentile cap (a bronze plan with a deductible equal to maximum annual limitation on cost sharing has an AV of 63.91 percent in 2027) and we believe consumers must retain access to bronze plans that do not exceed the maximum annual limitation on cost sharing so that we can best signal our good faith efforts to adhere to the statute.
We stated in the proposed rule that if it is no longer possible to design a bronze plan with a MOOP set at or below the maximum annual limitation on cost sharing and a permissible bronze AV, then it would also no longer be possible to take advantage of the new proposed flexibility in bronze plans' allowed MOOP limit: as in, it would no longer be possible to additionally offer a non-expanded (standard) bronze plan with a higher MOOP limit. We stated that the proposed flexibility relies on the issuer already offering a bronze plan in the same service area which has a permissible bronze AV and complies with that plan year's maximum annual limitation on cost sharing as a prerequisite to setting a higher MOOP for additional bronze plans. If the market reaches this point, as we warned in the proposed rule—that a bronze plan with a MOOP set at the maximum annual limitation on cost sharing will be unable to fit within the bronze AV
de minimis
range according to that year's AV Calculator—we stated that we would need to propose a new approach to maintaining bronze plans' viability through future notice-and-comment rulemaking.
Thus, we stated in the proposed rule that we intend to require such plans for as long as these bronze plans remain actuarially viable; however, under the overall incremental approach described earlier, we stated that we may revisit this precondition in future rulemaking as AVs continue to rise. Given these circumstances, we considered and requested comment on whether we should allow an adjustment to the result of the AV Calculator (which uses the 99.50th percentile cap) that approximates an AV calculation based on a standard population which includes those highest-cost enrollees (that is, approximates what the AV output would be from an AV Calculator which includes claims from the 0.50th highest percentile). We sought comment on how to better align with standard actuarial practice in our interpretation of the AV Calculator's outputs in light of the statutory incongruence described in this section, and how future AV Calculators might appropriately include more of these high-cost enrollees in its standard population without causing unnecessary disruption to existing plans that seek to remain in the same metal tier in the following plan year. Alternatively, we sought comment on whether an issuer should be permitted to offer bronze plans which exceed the maximum annual limitation on cost sharing to achieve an AV between 58 and 62 percent only after a default adjustment to the 2027 AV Calculator's output for that plan design which approximates what the plan's AV would be if measured by an AV Calculator without a spending cap, and on whether a future release of the AV Calculator, such as the PY 2028 AV Calculator, could reduce or remove the spending cap.
We further proposed that this flexibility would apply only in the individual market, and rounded down to the next lowest multiple of 50 dollars. Specifically, we stated that we believe individual market consumers in particular would be interested in more plan choices offering lower deductibles and lower premiums. We further stated that we believe prospective consumers who do not qualify for APTCs may be deterred from enrolling in individual market plans due to the benefit design of current bronze plans. We stated that providing additional plan design flexibility may encourage individual market enrollment and in turn promote a healthier risk pool by capturing currently uninsured people.
We stated that, as already is the case, States that are the primary enforcers of AV standards would be responsible for ensuring that issuers that design bronze plans that exceed the maximum annual limitation on cost sharing do so to achieve an AV within the standard (non-expanded) bronze
de minimis
ranges at § 156.140(c). Title XXVII of the PHS Act contemplates that States will exercise primary enforcement authority over health insurance issuers in the group and individual markets to ensure compliance with health insurance market reforms, which include the EHB requirements in 45 CFR subpart B. Under the proposal, we stated that States that enforce Affordable Care Act insurance market requirements would retain their primary enforcement authority over the EHB, and may determine that a particular bronze plan design unnecessarily exceeds the maximum annual limitation on cost sharing. We further stated that HHS would conduct such reviews of bronze plans offered in States where HHS directly enforces Affordable Care Act insurance market reform requirements.[282]
We invited comments about the enforcement of this proposed flexibility.
We sought comment on the proposal. Specifically, we sought comment on what, if any, additional requirements we should consider in order for issuers to avail themselves of the flexibility to exceed the maximum annual limitation on cost sharing. For example, we also considered whether to propose allowing bronze plans to exceed the maximum annual limitation on cost sharing only when bronze plans would otherwise be non-viable (that is, impossible to design). In addition, we noted that we were interested in comments discussing
( printed page 29699)
what additional consumer protections we can consider implementing to educate and notify consumers about individual market bronze plans that have a MOOP that does not exceed the maximum annual limitation on cost sharing. For example, we welcomed comments on imposing disclosure requirements on any such bronze plan to explain the plan's higher MOOP in the Summary of Benefits and Coverage (SBC) and on an Exchange website, though we noted that any such changes would be unlikely for PY 2027 due to time constraints preventing appropriate time to discuss and make a formal proposal in consultation with other Executive agencies including the Department of Treasury and Department of Labor. We sought comment on whether this policy should also apply to the small group market. We also sought comment on whether we should annually set a precise amount by which an issuer could utilize a plan design with cost sharing that exceeds the maximum annual limitation on cost sharing, or whether the proposed regulatory language is precise enough to limit the instances in which an issuer could offer such a plan. We sought comment on operational effects of this policy, such as whether these plans would be considered the same plan under § 157.106(e)(3)(iv), and what impact this would have on plan crosswalking. We sought comment on these additional requirements related to permitting a high MOOP for some bronze plans, or any others commenters may identify, that we might finalize in this rule.
In the proposed rule, we noted that as we contemplate how this policy could apply to plans at higher metal levels, we were seeking comment on what special considerations may exist for those plans, and particularly for silver plans in determining the second lowest cost silver plan. We also sought comment on whether this flexibility should also apply to cost-sharing variants. Finally, we sought comment on whether we should propose changes to the bronze de minimis range and expanded bronze policy at § 156.140(c)(1).
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing the addition of § 156.136 with the following modification: we are narrowing the flexibility proposed for individual market bronze plans such that these bronze plans are permitted to exceed the standard annual limitation on cost sharing by up to 130 percent of the standard annual limitation on cost sharing, rounded down to the nearest $50 increment. For PY 2027, that is $15,600 for self-only coverage and $31,200 for other than self-only coverage, based on multiplying the market-wide individual annual limitation on cost sharing by 1.3, that is, $12,000 × 1.3 = $15,600. We reiterate that the policy being finalized applies to individual market bronze plans only. We summarize and respond to public comments received on the proposal below.
Comment:
Many commenters stated concerns that allowing bronze plans to exceed the standard annual limitation on cost sharing at § 156.130 would increase out-of-pocket costs for consumers. These commenters cited that high deductibles are already required for bronze plans and warned of the proposal's potential cascading negative outcomes related to affordability generally, including unexpected higher out-of-pocket spending, increased medical debt, consumers dropping coverage upon understanding the effects of the plan's annual limitations on cost sharing, increased uncompensated care (particularly for rural and safety-net providers), and negative health outcomes due to delayed or foregone care. Several commenters raised affordability concerns specific to people with diabetes. Several commenters cited peer-reviewed studies and other publications [283]
demonstrating that enrollment in high-deductible health plans is associated with reduced adherence to care compared to enrollment in more affordable plans. A few commenters stated that the proposed change would effectively void the maximum annual limitation on cost sharing requirement by not specifying any ceiling on the MOOP limit that could be permitted for individual market bronze plans, and suggested specifying a strict dollar amount for the allowed upper bound. One of these commenters generally opposed changes that would increase out-of-pocket costs for consumers while citing particular concern with the lack of a strict dollar amount capping the annual limitation on cost sharing, which HHS had suggested in the proposed rule (91 FR 6380) as an alternative. In contrast, another one of these commenters generally approved of greater flexibility in plan designs, including for bronze plans, but they still approved of setting a specific maximum limit so as to increase the likelihood that a plan would use the proposed flexibility.
Response:
We appreciate the concerns raised by commenters regarding the affordability of plans with higher annual limitations on cost sharing. We acknowledge that higher out-of-pocket maximums can present financial challenges for some enrollees, particularly those with significant health care needs such as those with diabetes. We understand broadly that financial challenges can lead to forgone care, medical debt, and dropping coverage. We are aware of the body of research suggesting that high cost sharing can affect health care utilization and adherence, and we take these findings seriously. We understand that this proposal could shift more of the increasing costs of health care and potentially result in more enrollees who are unable to pay for their share of the cost. Still, we note that neither the proposed policy nor the policy finalized in this final rule require any issuer to offer an individual market bronze plan with a plan design that exceeds the standard annual limitation on cost sharing at § 156.130. Issuers retain full discretion over whether to offer such plans, and States may prohibit issuers from offering bronze plans that exceed the standard annual limitation on cost sharing at § 156.130 in their markets. As issuers that offer bronze plans with a design that exceeds the standard annual limitation on cost sharing will be required to offer at least one bronze plan in the same service area that does not exceed the maximum annual limitation on cost sharing under this policy as finalized, consumers shopping in the individual market will continue to have access to bronze plans with the standard annual limitation on cost sharing, as well as plans at other metal tiers. For the consumers who select one of the bronze plans that uses this new flexibility to set a higher MOOP limit, although they would have a higher MOOP, they would likely have lower premiums and potentially more plan designs from which to choose, including with varying cost sharing. Some commenters seemed to expect that some bronze plans having a higher MOOP limit would cause rural and safety-net providers financial harm by increasing uncompensated care; however, increasing consumer concern around affordability could also drive enrollees
( printed page 29700)
to seek more cost-effective care and skip unnecessary visits. Therefore, while we understand concerns about affordability and the consequence of lack of affordability, we are not persuaded that the policy we are finalizing in this rule will lead to such adverse results that providers would be subject to higher financial losses from providing uncompensated care. In fact, we believe that people with significant health care needs will be much less likely to enroll in bronze plans in general, and even less likely to enroll in bronze plans with increased annual limitations on cost sharing.
We believe that this policy has several potential benefits. A higher annual limitation on cost sharing will provide issuers with greater benefit design flexibility in their QHP offerings. This in turn could encourage currently unsubsidized, uninsured consumers to enroll. These consumers who have forgone coverage due to cost are often healthier, and the addition of individual market bronze plans using this flexibility will improve the overall risk pool, which can bring down premiums for all enrolled in these plans. We believe that these potential benefits outweigh the potential risks related to affordability, particularly when the potential risks that commenters raised (such as increases to uncompensated care and delayed care) can be mitigated by a consumer selecting a bronze plan with a standard annual limitation on cost sharing or a plan offered at a different metal level, in which they would receive more covered care.
In response to comments requesting that we set a specific ceiling on the MOOP limit for individual market bronze plans, we are finalizing our proposed addition of § 156.136 with a modification to add a ceiling on an individual market bronze plan's highest permissible MOOP limit. We believe setting this upper limit appropriately constrains the flexibility provided to issuers while preserving the policy's purpose of ensuring the continued availability of individual market bronze plans with plan designs that are attractive to consumers. We specifically selected the upper bound of 130 percent of the annual limitation on cost sharing for several reasons. First, this percentage is consistent with the multiplication factor we are finalizing for the catastrophic plan annual limitation on cost sharing starting with PY 2028, which provides a consistent framework. Second, a 130 percent ceiling preserves the core consumer protection function of the annual limitation on cost sharing, ensuring no bronze plan enrollees are subject to out-of-pocket costs that are disproportionate to the plan's bronze-tier design. At the same time, it provides issuers with sufficient flexibility to offer these additional bronze plan designs that are meaningfully distinct from standard bronze plans and catastrophic plans. Third, we considered whether a lower multiplier (such as 110 or 120 percent) would be sufficient to address the plan design viability problem identified in the proposed rule and concluded that a lower ceiling would not provide issuers with adequate flexibility to design bronze plans with meaningfully lower deductibles and more pre-deductible coverage. A 130 percent ceiling allows issuers to shift cost-sharing structure in a way that is actuarially meaningful, to enable lower deductibles offset by a higher MOOP among other plan designs, without exposing consumers to unlimited or unconstrained out-of-pocket liability. The 130 percent ceiling therefore functions as a consumer protection constraint on the outer boundary of issuer flexibility, not as an incentive to maximize cost sharing (that is, we do not expect every additional bronze plan to set the highest MOOP limit possible). For PY 2027, the 130 percent ceiling corresponds to $15,600 for self-only coverage and $31,200 for other than self-only coverage.
We are finalizing a ceiling of 130 percent of the annual limitation on cost sharing in this final rule for these reasons and in response to comments, as we agree that issuers would be more likely to offer such plans in the future if we provided greater clarity on the upper bound of what would be permissible for these additional bronze plans. We also agree that having a nationally established upper limit is an important consumer protection. We are considering whether to propose in future rulemaking a methodology by which we could annually establish a percentage, or another factor by which this upper bound is calculated from the annual limitation on cost sharing, in the annual guidance in which CMS releases the premium adjustment percentage, maximum annual limitation on cost sharing, reduced maximum annual limitation on cost sharing, and required contribution percentage for a given benefit year.
Comment:
Many commenters stated concern about the potential impact of the higher proposed MOOP limits for catastrophic plans and bronze plans on market risk and premiums for metal tier plans. Some commenters specifically warned that a shift in enrollment between higher-MOOP catastrophic plans and APTC-eligible metal tier plans could result in significant, unintended changes to APTC amounts. Several of these commenters stated concern about shifting risk and enrollment and warned of a possible bifurcation of the market between higher-MOOP catastrophic plans and APTC-eligible metal tier plans, fearing it could distort risk pools and increase premiums for subsidized enrollees. One commenter suggested that creating a clearer AV separation between bronze plans and silver plans would help restore rate separation between the two plan types. Several commenters requested that CMS provide more detailed estimates of the combined impact of the proposed bronze MOOP flexibility and catastrophic plan MOOP increase on enrollment, risk, and premiums before finalizing either proposal. Several commenters supported our efforts to find ways to bring lower premium plans to the Exchange that could entice healthy (unsubsidized, but unable to afford full-cost metal tier coverage) enrollees to maintain their enrollment in an individual market health insurance plan, while expressing disagreement with our projected net impact of these plan design policies.
Response:
We agree with commenters who recognized the importance of expanding access to lower-premium plan options for price-sensitive, unsubsidized enrollees. We also appreciate the concerns raised about potential risk pool and premium impacts and acknowledge that changes to plan design flexibility can affect enrollment patterns and, consequently, risk pool composition and premiums. In response to commenters who did not agree with our projected net impact, we acknowledge that projections of enrollment response to plan design changes involve inherent uncertainty. We note that the policy is optional for issuers and does not displace existing bronze plan offerings; accordingly, the downside risk of an adverse enrollment shift is constrained by the continued availability of standard bronze plans and plans at other metal tiers.
We further note that the flexibility in setting a MOOP limit no higher than 130 percent of the standard annual limitation on cost sharing for some bronze plans is designed to expand, not contract, the range of bronze plan designs available to consumers. We agree that encouraging more offerings of lower costing bronze plans—such as less generous bronze plans within the non-expanded AV
de minimis
range—will aid in differentiating bronze plans from silver plans, resulting in the benefit of more variation in plan design available to enrollees. By allowing issuers to offer bronze plans with lower
( printed page 29701)
deductibles and more pre-deductible coverage (made possible by a higher MOOP limit), we believe this policy would attract currently uninsured individuals who are deterred by the high deductibles of bronze plans and not eligible for subsidies, which could improve the overall risk pool. We expect issuers to design plans that are more appealing to enrollees, as this flexibility enables offering more pre-deductible coverage that quickly raises a plan's calculated AV, as opposed to coverage that is not provided on a pre-deductible basis. When a benefit is provided pre-deductible, it has a greater impact on AV, because the plan bears the cost of those services prior to the consumer meeting any deductible, thus increasing the plan's expected expenditures relative to a standard population. In contrast, when the same benefit is subject to a deductible, a greater portion of the cost is shifted to the enrollee, reducing the plan's share of total allowed costs and, consequently, its AV, and fewer people are expected to use the benefit.
We do not expect a significant APTC spending impact from this flexibility afforded to additional bronze plans, as we are not extending the flexibility to silver plans, nor do we expect such significant offerings of and enrollment into these bronze plans with higher MOOP limits such that it would skew the market's risk. We will monitor the impact of this policy on enrollment, risk pool composition, and premiums and will consider whether additional action is warranted in future rulemaking. We do not expect any unique compounding effects in PY 2028 and future plan years when catastrophic plans are newly required to adhere to a higher annual limitation on cost sharing, including in plan years when some of those catastrophic plans utilize the flexibilities afforded to multi-year plans discussed in section III.E.6. of this final rule. We disagree with commenters who viewed the combined effect of these two proposed policies as requiring a unified impact analysis prior to finalization. We have analyzed enrollment and premium effects of current plan policy decisions on bronze plans and catastrophic plans, as described in the preceding sections. We are not convinced that attempting to project the combined enrollment effects of these two policies would yield instructive results given the range of issuer design choices, State market conditions, and consumer behavior variables that will determine actual uptake. We have relied on available data—including enrollment trends in catastrophic and bronze plan tiers, AV modeling, and the risk adjustment framework applicable to catastrophic plans—to inform our assessment of likely market effects. We believe they represent a reasonable basis for the policy as finalized. Our view is that this policy will attract currently uninsured, price-sensitive consumers without materially disrupting the risk pool for subsidized metal tier enrollees, which is supported by available enrollment data, actuarial modeling, and the optional, issuer-discretionary nature of the policy.
Comment:
Several commenters noted their belief that CMS lacks statutory authority to finalize a policy with an increased annual limitation on cost sharing for catastrophic plans and bronze plans. Several commenters stated that the proposed policy would allow issuers to exceed the annual limitation on cost sharing for catastrophic plans and some bronze plans, which commenters stated is not reflective of Congress' intent when passing the Affordable Care Act. Although some commenters agreed with CMS that the increasing difficulty in creating bronze plans is problematic and a few commenters agreed with CMS about the value in differentiating catastrophic plans and bronze plans, they opined that only Congress can fix this problem.
Some commenters stated that the proffered justification for the policy—the impossibility of creating a bronze plan within the current
de minimis
range—is a policy justification and not an actual statutory conflict, since it is still possible to create a bronze plan. They stated that mathematical difficulty is not the same as mathematical impossibility. Therefore, some commenters suggested that CMS' reliance in the proposed rule on
Gustafson
v.
Alloyd Co.,
513 U.S. 561, 570 (1995), is misplaced. Other commenters noted that even if it were impossible to create bronze plans within the AV
de minimis
range, this does not permit CMS to disregard the statute. Some commenters noted that nothing requires issuers to offer bronze plans.
Some commenters stated that because CMS has modified the AV Calculator in the past to ensure that issuers can continue to create bronze plans, CMS could continue to use this approach, and the statutory impossibility noted in the proposed rule does not actually exist. Those commenters stated that CMS has an obligation to first consider less harmful alternatives and that to do otherwise would be arbitrary and capricious.
Response:
We do not agree with commenters that we lack statutory authority to adopt the proposed flexibility to allow issuers to offer individual market bronze coverage with a non-standard annual limit on cost sharing. As noted above, the policy finalized in this final rule does not require any issuer to offer such a bronze plan, and consumers will continue to be able to purchase bronze plans with the standard annual limitation on cost sharing, as well as plans at other metal tiers. Issuers also retain full discretion over whether to offer such plans, and States may prohibit issuers from offering bronze plans with non-standard annual limitations on cost sharing in their respective individual markets. This flexibility will expand access to affordable, comprehensive coverage in the private market, which aligns with the Congress' intent when passing the Affordable Care Act's private market reforms and consumer protections.[284]
It will provide an additional, affordable coverage option to Americans.
While we believe that there are policy benefits to allowing issuers greater flexibility in plan design, which should in turn give consumers additional choice, the ultimate purpose of this policy is to ameliorate a statutorily created problem. Section 1302 of the Affordable Care Act establishes parameters for the AV and annual limitation on cost sharing policies. We have modified these policies over the years, within the confines of section 1302 of the Affordable Care Act. Some policies have changed how the annual limitation on cost sharing is calculated, which has resulted in an increased annual limitation on cost sharing (90 FR 27166 through 27168). Other policies, such as changing the standard population, have modified how AV is calculated, which has generally resulted in issuers being able to continue to design bronze plans. However, we believe that we have exhausted reasonable methodological changes to calculation of AV and the annual limitation on cost sharing. Although we could attempt to finalize additional changes to the AV Calculator methodology or underlying data sources to preserve bronze plans, we are not convinced that such changes would comply with section 1302(d) of the Affordable Care Act and risks rendering the AV Calculator meaningless. Specifically, as we stated earlier in this rule and in the proposed rule, we are not aware of any administrable, actuarially sound regulatory alternatives that could mitigate this problem. We provided examples of alternatives that we considered but did not implement,
( printed page 29702)
such as trending the AV Calculator to account for changes in the standard population. However, we believe mathematical adjustments made for the sole purpose of guaranteeing certain AV outputs would make the AV Calculator meaningless, and such adjustments to lower the AV results for bronze plans may not be enough to maintain compliance with section 1302(d)(1)(A) of the Affordable Care Act (that is, that a qualified health plan offered at the bronze level of coverage would be designed such that it provides benefits “that are actuarially equivalent to 60 percent of the full actuarial value of the benefits provided under the plan”). Therefore, we continue to believe that a real statutory conflict exists, and that the best way to solve the conflict is to give issuers the flexibility, at their option, to offer plans exceeding the standard annual limitation on cost sharing as long as they offer a plan that meets the standard annual limitation on cost sharing. This resolution both ensures that plans meeting the standard annual limitation on cost sharing will be available and that all plans will meet the statutorily-created AV requirements.
We do not agree with commenters that this approach deviates from congressional intent. The Congress included requirements for AV and the annual limitation on cost sharing as consumer protections that must by their nature function together. Specifically, the annual limitation on cost sharing is an important input when calculating AV. We believe that allowing issuers to optionally offer plans with a non-standard annual limitation on cost sharing if they also offer at least one plan with the standard annual limitation on cost sharing is the most reasonable option, given that it preserves what commenters believe to be congressional intent regarding AV (that is, issuers can create bronze plans within the bronze
de minimis
range) and the annual limitation on cost sharing (that is, consumers will still have access to plans that meet with the standard annual limitation on cost sharing). We considered other options, such as making further changes to the AV policy, which would likely violate section 1302(d) of the Affordable Care Act and most likely need to apply to plans at all metal levels (and certainly all plans at the bronze level, thus not giving consumers any plans that meet statutory AV requirements). We further considered whether to do nothing and let bronze plans become non-viable altogether. Although there is no requirement for issuers to offer bronze plans, as noted previously, we believe that congressional intent was, at a minimum, for bronze plans to be able to exist. We noted in the proposed rule that there are several factors that influenced our decision to propose this policy; namely, the fact that without further changes, it will soon become impossible to create a bronze plan, and the need for the AV Calculator, policy, and underlying methodology to the AV Calculator to reflect an accurate representation of AV and the components of AV such as the standard population and not something shoehorned due to a mathematical problem. Thus, of the various options we identified, the policy we finalize in this rule is one that meets the statutory requirements, because it allows the existence of plans that meet AV, with an underlying sound AV methodology, and that meet the annual limitation on cost sharing. The other options we identified would put us clearly out of compliance with AV requirements or cause bronze plans to become non-viable. Although issuers are not required to offer bronze plans, a plain reading of section 1302(d) of the Affordable Care Act, which creates the bronze metal tier, would assume Congress created the bronze tier with the assumption that there is a viable, long-term market for such plans and that at least some issuers would offer them. This assumption that bronze plans are meant to remain viable is borne out by the consistent availability of bronze plans on the Exchanges since PY 2014, as described earlier in this section. In PY 2025 alone, there were 101 bronze plan options offered on-Exchange in the FFE which had approximately 5.4 million enrollees combined (see Table 11: Percentage of FFE Bronze Plans by AV Percentage, 2018 through 2025). But the problem is not solely limited to bronze plans: as noted in the proposed rule, without further action, this problem will eventually extend to the silver metal tier as well, and issuers are required to offer plans at the silver metal level. The unpredictable progression of plan design viability underscores why additional efforts to rectify this statutory incongruence by changing the AV methodology could not fully resolve this issue while simultaneously introducing more uncertainty into the QHP market. We commit not to deviate from generally accepted actuarial principles, despite commenters supporting further alterations to the AV methodology aimed at ensuring that appealing plan designs are still possible. We emphasize again that we will monitor the viability of silver plans, gold plans, platinum plans, and the reduced cost sharing plan variations but have not observed the same immediate negative impacts we have discussed as particularly impacting catastrophic plans and bronze plans. While these pressures are most visible at these lowest tiers now, accepting further AV methodological changes to maintain the viability of bronze plans would imply that we believe such changes to maintain other metal tiers are similarly acceptable. Yet such a result would be noncompliant with section 1302(d) of the Affordable Care Act. We note that finalization of this policy in no way precludes further congressional action.
We disagree with commenters that our reliance on
Gustafson
is misplaced on the grounds that it is still feasible to create bronze plans and that we could have made further changes to the AV Calculator to ensure that bronze plans can continue to exist in future plan years. We are finalizing a policy designed to ensure consumer access to bronze plans with the standard annual limitation on cost sharing—it is not an acknowledgment that the underlying conflict does not exist. It is well established that we already made methodological changes to the AV Calculator as a result of the increasing difficulty creating bronze plans. As we stated in the proposed rule and in this final rule, the AV of a bronze plan with a deductible set to the standard annual limitation on cost sharing is already 63.91 percent in PY 2027, which exceeds the standard bronze
de minimis
range, and we have no reason to believe this trend will reverse. We also discussed that although we are contemplating future changes, as we do every year before releasing the AV Calculator, we also believe that our policy must also reflect Congress' intent establishing AV and metal tier requirements and only allowing issuers to use a
de minimis
variation. While we will continue to explore changes to the AV Calculator, we believe that further AV Calculator changes to preserve the existence of bronze plans would jeopardize our compliance with section 1302(d) of the Affordable Care Act. As held in
Gustafson,
the solution here is to ensure that neither section of the statute is superfluous. We believe that the final policy and approach adopted in this final rule preserves the two statutory sections being able to be read in tandem.
Comment:
A few commenters supported our existing interpretation of and approach to the AV Calculator's methodology and results, as reflected in the 2027 AV Calculator, such as including a spending cap for the highest cost enrollees. No commenters
( printed page 29703)
supported adjusting the 2027 AV Calculator or future AV Calculators to remove the spending cap or its impact on AV Calculator calculations.
Response:
While these comments are out of scope for this final rule because they are not specifically about the proposed changes to the cost sharing of catastrophic plans and individual market bronze plans, we appreciate the commenters' attention and feedback.
Comment:
Several commenters urged CMS to decline to finalize the proposal entirely, or at the very least to provide more detailed estimates of the impact of the change to the annual limitation on cost sharing applicable to bronze plans, both in isolation and in combination with other proposed changes to catastrophic plans, before finalization. Another commenter stated that the policy was premature and that CMS should conduct additional data modeling and research before finalizing the proposal. Some commenters stated concerns about finalizing this policy for PY 2027. Several commenters noted that QHP certification and rate and form filings for PY 2027 have already commenced, making timely implementation difficult. In particular, some commenters noted that the timing would be overly burdensome for States with a State Exchange. Some commenters also noted potential litigation related to this proposal as a reason to delay implementation.
Response:
We appreciate the timing concerns raised by commenters and acknowledge that QHP certification and rate and form filings for PY 2027 have already commenced. We note, however, that nothing in this final rule requires issuers to offer a bronze plan with a plan design that exceeds the standard annual limitation on cost sharing at § 156.130; issuers that have already filed bronze plan designs are not required to modify those designs to increase the plans' MOOP limit for PY 2027. Additionally, States, including those with a State Exchange, could prohibit issuers from offering bronze plans that exceed the standard annual limitation on cost sharing at § 156.130. Therefore, we believe that this flexibility for both issuers and States sufficiently mitigates the timing concerns raised. Nothing in this final rule requires issuers to refile bronze plans for PY 2027. If an issuer wishes to amend its rate and form filing and QHP application materials and believes that it has time to do so, this final rule permits that, subject to any State requirements.
We disagree with comments that this policy should be more fully researched prior to finalization. We conducted robust research and analyses prior to proposing this policy. In fact, prior to proposing this policy, we spoke with States about the difficulty in creating bronze plans and have also made changes to the AV Calculator to ameliorate this difficulty, as stated in the AV Calculator methodology documents that we issue annually.[285]
The difficulty in creating a bronze plan is not a new problem; indeed, we spoke of this problem in the 2017 Market Stabilization Rule (82 FR 18369) when we created the expanded bronze
de minimis
range. For enrollment and premium impact estimates, we note that this policy is optional for issuers and does not require any issuer to offer a bronze plan with a non-standard MOOP. The range of potential enrollment effects is therefore bound by issuer discretion, State authority to prohibit such plans, and the continued availability of standard bronze plans and other metal tier options. We do not believe that projecting enrollment effects with a degree of precision that could inform policymaking is presently feasible given the range of issuer design choices, State market conditions, and consumer behavior variables that will determine actual uptake. We believe that the policy we are finalizing in this rule represents the best possible outcome since it ensures that bronze plans that meet the standard annual limitation on cost sharing at § 156.130 continue to exist and also preserves the integrity of the AV Calculator, such that there still is a meaningful differentiation between metal tiers. We also do not believe that commenters' perceived litigation risk is a justification to delay implementation. Nothing requires issuers to offer these plans, nor States to certify or approve them. In addition, nothing prevents issuers from conducting a risk assessment when deciding whether to offer these plans for PY 2027. We reiterate that we will monitor the impact of this policy and will consider whether additional action is warranted in future rulemaking.
Comment:
Several comments stated that consumers would need robust education about bronze plans with expanded MOOPs to ensure they understand what they are purchasing. One commenter requested that CMS propose this policy through a Tri-Department rule with the Departments of Labor and Treasury, and propose corresponding updates to the SBC to inform consumers if their bronze plan exceeds the annual limitation on cost sharing at § 156.130. A few commenters noted that there should be required consumer disclosures when a bronze plan has an annual limitation on cost sharing that exceeds that at § 156.130. A few other commenters cited the need for a robust consumer education campaign prior to any issuer offering such plans. Many commenters stated that people who help consumers select coverage, such as assisters, agents, brokers, and web-brokers, should be required to undergo training on these changes. One commenter cited a study noting that a large percentage of adults have difficulty understanding cost sharing.
Response:
We agree that consumer education is of the utmost importance and that individuals such as assisters, agents, brokers, and web-brokers who help consumers select and enroll in coverage have a special role in this. We appreciate the specific suggestion that such individuals helping consumers be required to undergo training on these changes so that they can help consumers make informed decisions. We often provide training and information to such individuals and will consider ways to facilitate this in the future. The annual limitation on cost sharing for any plan offered on an Exchange is already displayed to consumers during the plan selection process on
HealthCare.gov
and State Exchange websites, regardless of whether the plan's MOOP limit exceeds the standard annual limitation on cost sharing defined by § 156.130. Consumers can compare plans' MOOP limits, including plans with higher MOOP limits offered under this policy, alongside the premiums, deductibles, and other cost-sharing information. This existing display infrastructure provides a meaningful baseline of consumer transparency, and we encourage State Exchanges to ensure that their plan display similarly makes the MOOP limit of each plan prominent and accessible to consumers. To the extent that consumers may find cost sharing confusing, we are confident that the resources we have mentioned will mitigate such confusion. We take consumer education seriously, and for that reason we regularly review changes to
HealthCare.gov,
educational materials, and CMS-created training for those who help consumers.
Given that issuers, Exchanges, and the SBC currently provide information about the annual limitation on cost sharing and plans' MOOP limits, we do not believe that the SBC requires an amendment to specifically note when a given plan's MOOP limit exceeds the standard annual limitation on cost sharing set by § 156.130. As such, because we are not proposing any
( printed page 29704)
amendments to the SBC, we also do not believe that Tri-Department rulemaking is required in this instance. Further, we believe that consumers want to know the specific dollar amount of their plan's MOOP limit, and are less concerned by the conceptual definition of the standard annual limitation on cost sharing or by how much their plan's MOOP limit exceeds it. For example, nothing prohibits an issuer from offering a bronze plan with a MOOP limit lower than the standard annual limitation on cost sharing set forth at § 156.130. However,
HealthCare.gov
does not flag these plans' MOOP limits as being under the statutory maximum, relative to the standard annual limitation on cost sharing.
Comment:
Some commenters raised questions about the operational effects of this policy. One commenter requested confirmation of whether bronze plans with a higher permitted MOOP limit would be considered the same plan under § 157.106(e)(3)(iv), for the purposes of crosswalk, as the bronze plan with a standard MOOP offered by the issuer in the same area.
Several commenters opposed the extension of the flexibility to silver plans, and specifically warned about the mixed impact of the proposed requirements on catastrophic plans alone as shifting overall risk and premium shifts for the wider QHP and insured market (see the next subsection for in-depth discussion). One commenter stated concern about the possibility of market disruption and subsequent negative impact to American Indian and Alaska Native (AI/AN) plan variations.
Response:
Issuers and States may request additional operational guidance to assist with PY 2027 operations, such as for the purposes of determining the automatic plan crosswalk hierarchy and its treatment of bronze plans with higher MOOP limits. Auto-enrollment into and out of these bronze plans will follow the existing hierarchy under § 156.335(j), including the bronze plans that have a MOOP limit set higher than the standard annual limitation on cost sharing as permitted by this new plan design flexibility.
Given that we did not receive comments that supported extending the flexibility in the annual limitation on cost sharing to the small group market, higher metal tiers including silver plans, or plan variants, we are finalizing this policy as applicable to the individual market only and are not extending this flexibility to the small group market at this time. We appreciate the concerns raised about potential effects for those enrolled in AI/AN plan variations and other metal tiers, and are also finalizing this policy without applying it to the on-Exchange cost sharing plan variations (including plan variations only available to AI/AN enrollees) or any other metal tiers (that is, to the silver, gold, and platinum plans). As stated in the proposed rule, we intend to continue researching what might be an appropriate threshold for determining that a silver plan (or higher metal tier plan) has become too difficult or impossible to create, and any potential unanticipated or negative effects related to AI/AN plan variations. We will continue to monitor whether similar challenges arise in the small group market or in the cost-sharing plan variations, as well as operational implications of the combined plan policy changes, and we will consider whether further action through future rulemaking is warranted.
f. Catastrophic Plan Cost-Sharing Requirements
To best preserve a meaningful difference between the AVs of bronze and catastrophic plans, in the 2027 Payment Notice proposed rule (91 FR 6382), we proposed to amend § 156.155(a)(3) to require catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the maximum annual limitation on cost sharing, rounded down to the next lowest multiple of 50 dollars, is reached.
We stated in the proposed rule that the issue regarding the implementation of the maximum annual limitation on cost sharing and AV also impacts catastrophic plans. We noted that issuers do not have flexibility in varying the cost sharing for catastrophic plans; the Affordable Care Act requires catastrophic plans to have a deductible and MOOP set to the maximum annual limitation on cost sharing and provide few specific benefits pre-deductible at section 1302(e)(1)(B). We stated that because of this rigidity, catastrophic plans do not have prescribed AV requirements. Nevertheless, we stated that the perceived value of catastrophic plans is still affected by the conflict. We estimated that the year-over-year AVs for catastrophic plans are gradually rising, just like metal-tier plans. However, we noted that they are rising at an even faster rate than bronze plans.
We noted that an eligible consumer might prefer to select a bronze plan over a catastrophic plan if the catastrophic plan has a similar premium to the bronze plan and has a comparable AV to a bronze plan, but the bronze plan is able to provide more pre-deductible benefits and lower deductibles and MOOPs. We stated that this obvious choice is evident in enrollment data; enrollment in catastrophic plans on the FFEs has decreased every year since 2016 while bronze plan enrollment has increased. In 2016, nearly 100,000 people enrolled in catastrophic plans, but only about 20,000 people enrolled in catastrophic plans in 2025. Since we expanded the bronze de minimis ranges in 2018, enrollment in bronze plans has more than doubled from about 2.5 million to about 5.4 million in 2025. We stated that we believe the continuous rise in AVs for bronze plans and the decrease in enrollment for catastrophic plans may be causally connected, though we sought comment on other potential reasons to explain this phenomenon.[286]
We stated in the proposed rule that we believe that catastrophic plans only appeal to consumers when there is a clear difference in the perceived value between catastrophic and bronze plans. We stated that when there is such a clear difference, the healthier consumers that are generally eligible and best suited to enroll in catastrophic plans are more motivated to select a catastrophic plan in lieu of a bronze plan. We stated that this is plainly what Congress intended.
Accordingly, we proposed a revision to § 156.155 that would more clearly distinguish catastrophic plans from bronze plans. We proposed to require catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the standard annual limitation on cost sharing, rounded down to the next lowest multiple of 50 dollars, is reached, beginning in 2027. We stated that for PY 2027, this amount would be $15,400. We stated that we chose to propose multiplying the standard annual limitation on cost sharing by a factor of 130 percent because we estimated this would lower the estimated AV for these catastrophic plans to 55 percent; we stated that by definition, increasing the cost sharing
( printed page 29705)
for which consumers are responsible in a plan design reduces some of the market pressure that drive increasing premiums. We stated that we believe this is a reasonable estimate for a theoretical AV of catastrophic plans, as it strikes a balance between comprehensiveness of coverage and premium affordability for healthier enrollees.
We stated that this higher cost-sharing limit for catastrophic plans would allow for a more meaningful difference between the cost sharing typically expected for catastrophic and bronze plans and would allow issuers to more aggressively price catastrophic rates lower so that cheaper catastrophic plans would appeal to the kinds of consumers that we believe should tend to be enrolled in catastrophic plans especially the healthy, non-subsidized enrollees who may be disincentivized from enrolling in a QHP due to the rise in costs. However, we sought comment on whether we should strive for a theoretical AV for catastrophic plans that is higher or lower than 55 percent, including whether we should phase in this multiplication factor over a number of plan years to ease the impact on catastrophic plan cost sharing, and how the availability of catastrophic plans at 130 percent of the maximum annual limitation on cost sharing would affect the landscape of plans available to consumers. We reserved the ability to finalize a different factor than 130 percent in the final rule after reviewing public comments. In addition, we solicited comments that address whether, in potentially finalizing this proposal, we should not require catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the maximum annual limitation on cost sharing. Alternatively, we solicited comments that address whether we should, in potentially finalizing this proposal, require issuers to offer, in the same service area, at least one catastrophic plan that provides no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 100 percent of the maximum annual limitation on cost sharing, as a precondition to being able to offer catastrophic plans that provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the maximum annual limitation on cost sharing. We also solicited comment on whether we should, in potentially finalizing this proposal, alternatively allow catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount that could be less than 130 percent of the maximum annual limitation on cost sharing (but not less than 100 percent). We stated in the proposed rule that this proposed approach for catastrophic plans harmonizes plan and market outcomes with section 1302(c) through (e) of the Affordable Care Act to the greatest extent possible to preserve meaningful catastrophic plan availability without jeopardizing the integrity of the metal-tier framework that Congress envisioned. And, we stated that while raising the maximum annual limitation for catastrophic plans beyond what Congress specified is not an action we take lightly, we believe that, due to the mathematical irreconcilability created by current section 1302(c) through (e) of the Affordable Care Act, this proposal is necessary and most narrowly-tailored to ensure the coherent implementation of the Affordable Care Act's overall statutory scheme with as minimal disruption to consumers as possible. Per the previous section, we also proposed to allow issuers to offer catastrophic plans with a multi-year term: all catastrophic plans that an issuer wishes to offer for PY 2027 would be required to use the higher annual limitation on cost sharing.
We also sought comment on whether there would be impacts to HHS risk adjustment as a result of requiring catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the standard annual limitation on cost sharing, rounded down to the next lowest multiple of 50 dollars, is reached—or as we are referring to it in this final rule, the catastrophic plan annual limitation on cost sharing. Finally, we considered whether the guidance document on the “Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage,” or another regulatory vehicle, might be more appropriate for annually releasing this additional flexibility for defining plans' annual limitation on cost sharing, and invited comment on where to release and seek comment on the updated annual limitations on cost sharing ahead of each plan year.
We sought comment on all aspects of this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing the amendment to § 156.155(a)(3) as proposed, with the following modifications: we are delaying implementation of the policy until PY 2028 and modifying the dollar amount calculation provided in the proposed rule to correct an inadvertent mathematical computation error in the proposed rule's calculation of 130 percent of the maximum annual limitation on cost sharing. We summarize and respond to public comments received on the proposal below.
Comment:
Some commenters noted that the proposed rule's calculation of 130 percent of the standard annual limitation on cost sharing for PY 2027 appeared to contain a mathematical error. Specifically, commenters noted that 130 percent of $12,000 equals $15,600, not $15,400 as stated in the proposed rule.
Response:
We appreciate commenters identifying this error. The proposed rule inadvertently stated that 130 percent of $12,000 equals $15,400, which is incorrect. Because we are not finalizing this policy for PY 2027, this matter is moot for catastrophic plans but remains relevant to bronze plans as discussed in the previous subsection. We will consider finalizing the annual limitation on cost sharing applicable to catastrophic plans for a given plan year in the annual PAPI guidance entitled, “Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage”, except when we propose methodology changes through notice-and-comment rulemaking. We are finalizing the annual limitation on cost sharing for catastrophic plans as 130 percent of the standard annual limitation on cost sharing, rounded down to the next lowest multiple of $50, to be effective in PY 2028.
Comment:
Some commenters supported the proposal and noted that if finalized, it would spur innovation and improved plan designs.
Response:
We agree with these commenters. It is our hope that this final policy will give issuers additional flexibility to innovate and create new plan designs.
Comment:
Many comments stated concern that requiring catastrophic plans to use an annual limitation on cost sharing equal to 130 percent of the standard annual limitation on cost sharing would significantly increase out-of-pocket costs for catastrophic plan enrollees. Commenters noted that catastrophic plans already require enrollees to pay most costs until
( printed page 29706)
reaching high out-of-pocket limits, and that increasing the MOOP for these plans would expose enrollees to substantial financial risk. Several commenters cited studies demonstrating that high cost-sharing is associated with reduced adherence to care, delayed treatment, and worse health outcomes. Commenters representing patients with chronic conditions, including diabetes, stated particular concern that high deductibles would discourage early treatment and worsen outcomes for individuals who need ongoing care. Some commenters stated that the 130 percent factor is too high and would expose enrollees to unacceptably high out-of-pocket costs. A few commenters emphasized that protecting people from bankruptcy was a core part of the Affordable Care Act. Other commenters suggested that CMS should phase in the multiplication factor over a number of plan years to ease the impact on catastrophic plan cost sharing. A few commenters were critical of using a theoretical AV for catastrophic plans as a design target, noting that the statute does not require AV for catastrophic plans, and stated that this did not provide a sufficient legal basis for exceeding the statutory MOOP. Some commenters suggested using a sliding income-based scale for the annual limitation on cost sharing. Some commenters supported the proposal broadly, but noted their belief that current premiums for catastrophic plans are too high and would need to be substantially lower to see substantial enrollment growth.
Response:
We appreciate the concerns raised by commenters regarding the affordability of catastrophic plans under this proposed policy. We acknowledge that higher out-of-pocket maximums can present financial challenges for some enrollees, particularly those with significant health care needs. We are aware of the body of research suggesting that high cost sharing can affect health care utilization and adherence, and we take these findings seriously.
However, we note that the purpose of this policy is to restore a meaningful distinction between catastrophic plans and bronze plans—a distinction that Congress plainly intended and that has been eroded by the gradual rise in the AV of catastrophic plans. As enrollment data demonstrates, catastrophic plan enrollment on the FFEs has decreased every year since 2016, from nearly 100,000 enrollees in 2016 to approximately 20,000 enrollees in 2025. We believe this decline is attributable in part to the convergence of catastrophic and bronze plan AVs, which has made catastrophic plans less attractive to the healthy, non-subsidized enrollees for whom they were designed. Commenters recognized current catastrophic plan premiums are too high to drive enrollment growth, a fact that supports the policy's rationale: the current convergence of catastrophic and bronze plan AVs has eliminated the premium differential that makes catastrophic plans attractive. By restoring a meaningful AV distinction, we believe this policy will make catastrophic plans more attractive to these consumers, potentially lowering catastrophic plan premiums and improving the overall risk pool for catastrophic plans, and increasing catastrophic plan growth.
We do not refute the studies cited by commenters about the impact of the financial burden of high cost-sharing on chronically ill and low-income individuals. Consumers who are aware of their chronic illness and use health insurance coverage to manage it would not be likely to select catastrophic coverage, even when they qualify for it. The net impact we anticipate on low-income consumers who are eligible for catastrophic plans will hopefully attract the enrollment of price-sensitive consumers, ideally capturing younger, healthy individuals who would otherwise go uninsured. An uninsured individual has no bankruptcy protection against health costs, let alone a required limitation on any of their out-of-pocket health spending. A catastrophic plan enrollee with a 130 percent MOOP has a defined, capped out-of-pocket maximum. The policy therefore improves financial protection relative to the alternative of no coverage, even if it does not provide the same protection as a metal tier plan.
After consideration of comments, we are finalizing a multiplication factor of 130 percent of the maximum annual limitation on cost sharing for catastrophic plans, as proposed. We believe this factor appropriately balances the need to restore a meaningful AV distinction between catastrophic and bronze plans with the need to minimize disruption to catastrophic plan enrollees. We estimate that this factor will generally result in an AV of approximately 55 percent for catastrophic plans, which we believe is a reasonable estimate that strikes a balance between comprehensiveness of coverage and premium affordability for healthier enrollees.
We acknowledge that catastrophic plans are not subject to the AV requirements established in section 1302(d) of the Affordable Care Act. However, we believe that using an estimated AV as a reference point for calibrating the catastrophic plan annual limitation on cost sharing is a reasonable and transparent approach to achieving the policy's goal: restoring a meaningful distinction between catastrophic plans and bronze plans. The 55 percent estimated AV is not a binding requirement imposed on catastrophic plans; rather, it is an analytical tool that allows us to estimate the relative value of catastrophic plan coverage and to set the 130 percent multiplication factor in a principled, quantifiable manner.
We appreciate the comment about a sliding scale annual limitation on cost sharing. Currently, people in cost sharing variant plans at the silver metal tier have reduced cost sharing and a corresponding reduced annual limitation on cost sharing. A phase-in across plan years would defer the correction while the underlying problem continues to compound; a linear percentage-based calculation limiting cost sharing proportionally to the generosity of the metal tier or reduced cost-sharing plans goes beyond the scope of what we considered for finalization: there is no evidence of negative plan outcomes from incongruent policies at the higher metal tiers, and we are not finalizing any cost sharing changes to silver, gold, or platinum tiers, or cost sharing reduction variations. As previously stated, we anticipate that plans with a higher annual limitation on cost sharing will have lower premiums.
We agree that protection against bankruptcy was a key reason the Affordable Care Act was enacted in law, and we discuss congressional intent further in the next response to comments. These final rules provide greater flexibility for States and plans to determine what QHPs are best tailored to their markets; it does not prohibit future enrollees from selecting a metal-tier plan with a MOOP limit set at or below the standard annual limitation on cost sharing as an option for protecting themselves from higher out-of-pocket medical costs. This policy will give enrollees access to more affordable (and quantifiably more) QHP choices.
Although we believe that the actuarial problem driving this proposal—the gradual convergence of catastrophic and bronze plan AVs—warrants immediate action, we are delaying the implementation (but not approach) of the multiplication factor for calculating the catastrophic plan annual limitation on cost sharing to PY 2028. A phased approach delays the restoration of a meaningful distinction between the two plan types but minimizes the impact on Exchanges, plans, and enrollees for PY 2027, giving Exchanges and plans time
( printed page 29707)
to plan. The delay will prevent issuers from having to refile plans, which would be required if this policy were finalized for PY 2027. Although a phased approach would also prevent this, we believe that this could cause confusion for issuers and consumers that would need to adapt annually to a new percentage.
Comment:
Several commenters stated that the proposal to require catastrophic plans to have an annual limitation on cost sharing that is 130 percent of the statutory annual limitation is not contemplated by the statute. Others stated that there is no requirement in the Affordable Care Act for bronze plans to be differentiated from catastrophic plans.
Response:
We disagree. As stated in the proposed rule and earlier in this final rule, we believe that Congress did intend for differentiation between bronze plans and catastrophic plans to exist. For the reasons set forth below, we are finalizing this policy as proposed, but with a 1-year delay in effective date. Section 1302(e) of the Affordable Care Act establishes the catastrophic plan as a distinct coverage category, separate from the metal tier plans (bronze, silver, gold, and platinum) established under section 1302(d) of the Affordable Care Act. Congress' decision to create catastrophic plans as a separate statutory category—with their own eligibility criteria, benefit design requirements, and enrollment restrictions—reflects a deliberate legislative choice to maintain a distinct coverage option for eligible individuals.
Section 1302(c)(1) of the Affordable Care Act establishes the annual limitation on cost sharing and directs the Secretary to update this limit annually. Critically, the statute does not expressly prohibit the Secretary from establishing a differentiated cost-sharing limit for catastrophic plans, nor does it mandate that the same numerical limit apply uniformly across all plan types. As noted previously, our intent is for different statutory sections to operate together coherently and harmoniously. We also understand our charge to apply the best reading of the statute, under the principles of statutory construction affirmed in
Loper Bright Enterprises
v.
Raimondo,
603 U.S. 369 (2024) (directing courts and agencies to apply the best reading of the statute). We believe the best reading of section 1302 of the Affordable Care Act, taken as a whole, supports the Secretary's authority to calibrate cost-sharing parameters in a manner that gives meaningful effect to the distinct statutory category Congress created.
In response to the commenters that stated that the statute does not
require
differentiation between bronze and catastrophic plans, we agree that the statute does not mandate a specific numerical differential. However, the absence of an express mandate does not preclude the agency from exercising its rulemaking authority to implement a policy that is consistent with the statute's structure and purpose. The Affordable Care Act's creation of a separate catastrophic plan category would be rendered largely meaningless if catastrophic plans were, in practice, indistinguishable from bronze plans in their cost-sharing design. As we stated in the proposed rule, catastrophic plans are subject to mandatory benefit design parameters—including the requirement to cover three primary care visits prior to the deductible—that do not apply to bronze plans. These requirements increase the actuarial cost of catastrophic plans relative to bronze plans without a corresponding adjustment to the cost-sharing structure, resulting in catastrophic plans that are less attractive to eligible consumers and, in many markets, functionally equivalent to or less favorable than bronze plans. This outcome is inconsistent with Congress' evident intent to preserve catastrophic coverage as a meaningful, lower-cost option for eligible individuals.
By setting the annual limitation on cost sharing for catastrophic plans at 130 percent of the standard limit, we are exercising our regulatory authority to ensure that the catastrophic plan category remains a viable and distinct option in the market—one that reflects the higher cost-sharing structure Congress contemplated when it created this separate coverage tier. This approach is a reasonable and permissible exercise of the Secretary's authority under section 1302 of the Affordable Care Act and is consistent with the overall structure of the Affordable Care Act.
Comment:
A few commenters addressed the methodology for estimating the PAPI. These commenters recommended that we revise the PAPI methodology to better reflect per capita claims cost growth in the individual health insurance market, so that the annual adjustment to the maximum annual limitation on cost sharing better tracks the claims experience of the population in the individual market. In regard to whether the PAPI methodology should only reflect individual market claims, one commenter recommended that any future methodology adjustments should consider financial protection and affordability, which may include interactions with AV calculations, premium tax credit changes, and the long-term impacts of cost-sharing limits. Several commenters addressed whether the PAPI guidance document entitled “Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage,” or a regulatory vehicle, would be the appropriate vehicle for releasing updated catastrophic plan MOOP limitations annually. Some commenters stated a preference for notice-and-comment rulemaking for any annual updates to the catastrophic plan MOOP, to ensure public input on the multiplication factor and resulting dollar amounts.
Response:
We believe that this annual rulemaking is the appropriate vehicle for releasing updated catastrophic plan MOOP limitations annually, as it provides the opportunity for notice and comment. While the other comments about the PAPI methodology are out of scope for this final rule because they do not relate to the specific cost sharing proposal included in the proposed rule, we appreciate commenters' attention and feedback.
Comment:
Several commenters, including representatives from many State insurance authorities and Exchanges, recommended that CMS delay the effective date of the requirement that catastrophic plans use a catastrophic plan annual limitation on cost sharing defined as a percentage higher than the standard annual limitation on cost sharing. These commenters stated that CMS had not provided sufficient time for States, issuers, and other interested parties to assess the combined impact of the cost sharing changes to catastrophic plans and bronze plans, as well as the multi-year catastrophic plans that will be permitted under the policy being finalized elsewhere in this final rule. Many commenters urged CMS to decline to finalize the proposal entirely, citing concerns about consumer harm and the adequacy of CMS' impact analysis. Several commenters noted that QHP certification and rate and form filings for PY 2027 have already commenced. One State indicated it would consider setting its own MOOP limits applicable within its State alone. Several commenters warned of possible unintended impacts to plan selection, risk pool composition, and premiums—including a potential bifurcation of the market between catastrophic plans and APTC-eligible metal tier plans—and stated that these impacts had not been
( printed page 29708)
adequately modeled before the proposal was made. Several commenters recommended delaying the implementation of the proposed cost sharing changes until further research is conducted into forecasting the combined impact of the plan design changes.
Response:
We appreciate these comments regarding implementation of the requirement that catastrophic plans use a catastrophic plan annual limitation on cost sharing defined as a percentage higher than the standard annual limitation on cost sharing. Unlike the flexibility for MOOP limits for bronze plans, which is optional for issuers, all catastrophic plans must set their plans' MOOP limit to the catastrophic plan annual limitation on cost sharing under this policy, as finalized, which does not provide issuers with the same degree of discretion to delay or decline implementation. We acknowledge that this distinction makes the timing concerns raised by commenters particularly salient for the catastrophic plan proposal.
In response to comments requesting delayed implementation, we are finalizing this requirement with an effective date starting in PY 2028 to allow issuers, States, and Exchanges additional time to prepare. We believe this approach appropriately balances the need to address the underlying actuarial challenge with the operational concerns raised by commenters, particularly since PY 2027 QHP certification has already commenced, and rate and form filings have largely been submitted.
We note, however, that the underlying actuarial problem driving this proposal—as in, the gradual convergence of catastrophic and bronze plan AVs—has been developing for several years, and that we have been monitoring and discussing this issue since at least the 2017 Market Stabilization Rule. We do not believe that further delay would meaningfully change the actuarial trajectory or the need for regulatory action, but have chosen to delay implementation by 1 year to ease the impact on issuers, States, and Exchanges.
States do not have the authority to set separate, unique annual limitations for catastrophic plans offered in their markets, and if offered in their Exchange, these plans must meet the Federal requirements. States that wish to limit the impact of this policy on their markets may exercise their Exchange authority under § 155.1000(e) to decline to certify any catastrophic plans from being offered in PY 2028 and future years.
As addressed in the in the preceding section, we believe we have conducted sufficient forecasting before finalizing this policy. We acknowledge that projections of enrollment response to plan design changes involve inherent uncertainty. We believe that the policy we are finalizing in this rule represents the best possible outcome since it ensures that meaningful difference be restored between catastrophic plans and bronze plans. We believe this policy would attract currently uninsured individuals who are not eligible for subsidies but deterred by the high premiums of metal tier plans, which could improve the overall risk pool. We note that offering catastrophic plans is optional for issuers. Nothing prevents issuers from conducting a risk assessment when deciding whether to offer these plans for PY 2028 and future plan years that are subject to the cost-sharing changes. We will continue to monitor the impact of this policy on catastrophic plan availability, enrollment, premiums, and risk pool composition, and will consider whether additional action is warranted in future rulemaking.
Further, we do not expect any unique compounding effects in PY 2028 and future plan years when catastrophic plans are newly required to adhere to a higher annual limitation on cost sharing, including in plan years when some of those catastrophic plans utilize the flexibilities afforded to multi-year plans discussed in section III.E.6. of this final rule. We do not agree with commenters who viewed the combined effect of these two policies as requiring a unified impact analysis prior to finalization. We have analyzed enrollment and premium effects of current plan policy decisions on bronze plans and catastrophic plans, as described in the preceding sections. We are not convinced that attempting to project the combined enrollment effects of these two policies would yield instructive results, given the range of issuer design choices, State market conditions, and consumer behavior variables that will determine actual uptake. We have relied on available data—including enrollment trends in catastrophic and bronze plan tiers, AV modeling, and the risk adjustment framework applicable to catastrophic plans—to inform our assessment of likely market effects. We believe they represent a reasonable basis for the policy as finalized. Our view is that this policy will attract currently uninsured, price-sensitive consumers without materially disrupting the risk pool for subsidized metal tier enrollees, which is supported by available enrollment data, actuarial modeling, and the optional, issuer-discretionary nature of the policy.
8. Standardized Plan Options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv))
a. Introduction
In the 2027 Payment Notice proposed rule (91 FR 6383), we proposed to exercise our authority under sections 1311(c)(1) and 1321(a)(1)(B) of the Affordable Care Act to discontinue the full suite of standardized plan option policies effective beginning in PY 2027. Specifically, we proposed to remove the following from our regulations: the definition of “standardized option” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b), as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv). Finally, we proposed to cease the annual design and publication of these plans in the applicable Payment Notice rulemaking for each plan year.
b. Regulatory History
Standardized options were first introduced in the 2017 Payment Notice and codified at § 155.20 (81 FR 12289 through 12293). These standardized option plan designs were subsequently updated in the 2018 Payment Notice (81 FR 94107 through 94112). The 2018 Payment Notice (81 FR 94118) also introduced the authority for HHS to differentially display standardized options on
HealthCare.gov
at § 155.205(b)(1), which allowed consumers to filter all available plan options to view only standardized options and receive an accompanying message explaining how standardized options differed from non-standardized options. The 2018 Payment Notice (81 FR 94118) also introduced standardized option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP
( printed page 29709)
at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv).[287]
Standardized options were then discontinued in the 2019 Payment Notice (83 FR 16974 through 16975). However, the discontinuance was challenged in the United States District Court for the District of Maryland. On March 4, 2021, the court decided
City of Columbus, et al.
v.
Cochran.[288]
The court reviewed nine separate policies HHS had issued in the 2019 Payment Notice, vacating four of them. The court vacated the policy finalized in the 2019 Payment Notice that ceased HHS' practice of designating some plans in the FFEs and SBE-FPs as “standardized options,” a policy that we, in the 2019 Payment Notice (83 FR 16974 through 16975), stated was intended to maximize innovation by issuers in designing and offering a wide range of plans to consumers.
As a result, in part 2 of the 2022 Payment Notice (86 FR 24264 through 24265), we announced our intent to engage in rulemaking under which we would propose to resume designation of standardized options and propose specific designs in more detail in PY 2023. Thus, in the 2023 Payment Notice (87 FR 27310 through 27322), we reintroduced standardized plan options to enhance the consumer experience, increase consumer understanding, simplify the plan selection process, and combat discriminatory benefit designs.[289]
We required FFE and SBE-FP issuers offering QHPs in the individual market to offer these plans, but we exempted FFE and SBE-FP issuers offering QHPs in the small group market as well as issuers in State Exchanges from these requirements. We also exempted issuers of QHPs in FFEs and SBE-FPs that were already required to offer standardized plan options under State action taking place on or before January 1, 2020, such as issuers in the State of Oregon,[290]
from the requirement to offer the particular standardized plan option plan designs specified by HHS in rulemaking.
In the 2023 Payment Notice (87 FR 27312), we finalized standardized plan options at the following metal levels: one bronze plan, one bronze plan that meets the requirement to have an AV up to 5 points above the 60 percent standard, as specified in § 156.140(c) (known as an expanded bronze plan), one standard silver plan, one version of each of the three income-based silver CSR plan variations, one gold plan, and one platinum plan. We did not finalize standardized plan options for the AI/AN CSR plan variations as provided for at § 156.420(b) given that the cost sharing parameters for these plan variations are already largely specified.
In the 2023 Payment Notice (87 FR 27312), we finalized two sets of standardized plan options to accommodate different States' cost sharing laws. Specifically, the first set of standardized plan options applied to all FFE and SBE-FP issuers, except issuers in Delaware, Louisiana, and Oregon. The second set of standardized plan options applied only to issuers in Delaware and Louisiana to accommodate these two States' specialty prescription drug cost sharing laws.
We designed these standardized plan options to resemble the most popular QHP offerings that millions of consumers were already enrolled in by taking the following steps: selecting the most popular cost sharing type for each benefit category; selecting enrollee-weighted median cost sharing values for each of these benefit categories based on PY 2022 cost sharing and enrollment data; modifying these plans to ensure they were able to comply with applicable State cost sharing laws; and decreasing the AVs for these plan designs to be at the floor of each AV
de minimis
range, primarily by increasing deductibles.
In the 2023 Payment Notice (87 FR 27313), we also resumed the differential display of standardized plan options on
HealthCare.gov
under the authority at § 155.205(b)(1), including those standardized plan options required under State action taking place on or before January 1, 2020. In addition, we resumed enforcing the standardized plan option differential display requirements for approved web-brokers and QHP issuers using a DE pathway to facilitate enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv).
As such, web brokers and QHP issuers were once more required to differentially display standardized plan options in accordance with § 155.205(b)(1) in a manner consistent with how standardized plan options are displayed on
HealthCare.gov,
unless we approve a deviation. Any requests from web brokers and QHP issuers seeking approval of an alternate differentiation format are reviewed based on whether the same or a similar level of differentiation and clarity is provided under the requested deviation as is provided on
HealthCare.gov.
In the 2024 Payment Notice (88 FR 25847 through 25855), we maintained a high degree of continuity with our approach to standardized plan options finalized in the 2023 Payment Notice. However, in contrast to the policy finalized in the 2023 Payment Notice, at § 156.201(b), we finalized for PY 2024 and subsequent plan years to no longer include a standardized plan option for the non-expanded bronze metal level—primarily due to AV constraints and the infeasibility of designing such a plan.
In the 2025 Payment Notice (89 FR 26357 through 26362) and in the 2026 Payment Notice (90 FR 4493 through 4500), we continued to maintain a high degree of continuity with the approach to standardized plan options finalized in the immediately preceding Payment Notices (that is, the 2024 and 2025 Payment Notices). In each rulemaking, we made only minor modifications to the plan designs to ensure they continued to have AVs within the permissible
de minimis
range for each metal level. Additionally, in the 2026 Payment Notice, we finalized a requirement for FFE and SBE-FP QHP issuers in the individual market offering multiple standardized plan options within the same product network type, metal level, and service area to meaningfully differentiate these plans from one another in terms of included benefits, provider networks, included prescription drugs, or a combination of some or all these factors at § 156.201(c).
We explained that this requirement was based in part on our experience with the meaningful difference standard, which was previously codified at § 156.298. The meaningful difference standard was introduced in the 2015 Payment Notice (79 FR 13813 through 13814), revised in the 2017 Payment Notice (81 FR 12312 and 12331), and subsequently discontinued and removed from our regulations in the 2019 Payment Notice (83 FR 17027). The meaningful difference standard was originally intended to enhance the consumer experience on
HealthCare.gov
by preventing duplicative plan offerings and limiting plan proliferation.
We refer readers to the preambles to the 2023, 2024, 2025, and 2026 Payment Notices discussing § 156.201 (87 FR 27310 through 27322, 88 FR 25847
( printed page 29710)
through 25855, 89 FR 26357 through 26362, and 90 FR 4493 through 4500, respectively) for more detailed discussions regarding our approaches to standardized plan options in previous plan years. We also refer readers to the preambles to the 2015, 2017, and 2019 Payment Notices discussing § 156.298 (79 FR 13813 through 13814, 81 FR 12312 and 12331, and 83 FR 17027, respectively) for more detailed discussions regarding our approaches to the meaningful difference standard in previous plan years.
c. Current Proposal
In the 2027 Payment Notice proposed rule (91 FR 6384), we proposed, effective beginning in PY 2027, that FFE and SBE-FP QHP issuers in the individual market would no longer be required to offer standardized plan options. Further, we stated in the proposed rule that we would remove the following from our regulations: the definition of “standardized options” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b), as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the authority to differentially display standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv). Finally, we stated we would cease the annual design and publication of these plans in the applicable Payment Notice for each plan year.
In the proposed rule (91 FR 6384), we stated that nothing under the proposal would impact or preclude State-enacted standardized plan option requirements, including the requirement for issuers in the State of Oregon to offer such plans.[291]
Thus, we stated that under the proposal, Oregon issuers would continue to be subject to State requirements. However, standardized plan options offered under those State requirements would no longer be differentially displayed on
HealthCare.gov,
and approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP would no longer be required to differentially display standardized plan options offered under those State requirements (such as the requirement in the State of Oregon). We also noted that nothing under the proposal would preclude State Exchanges from requiring their respective issuers to offer standardized plan options or from differentially displaying such plans on their respective enrollment platforms.
We also clarified (91 FR 6385) that while we proposed to discontinue the requirement for issuers to offer standardized plan options, the annual design and publication of these plans in the applicable Payment Notice each plan year, and the differential display of these plans on
HealthCare.gov
and DE pathways, we were not proposing to require issuers to discontinue their existing standardized plan option offerings altogether. Instead, we stated that under the proposal, issuers would be permitted to choose whether to discontinue their existing standardized plan option offerings altogether or continue offering them with either the same or modified cost sharing, while we simultaneously discontinue the differential display of these plans and designation of these plans as standardized plan options.
We further stated (91 FR 6385) that under the proposed approach, if issuers wished to discontinue their existing standardized plan option offerings altogether, they would be permitted to do so, and enrollees in these plans would be crosswalked to a different plan in accordance with the crosswalk hierarchy at § 155.335(j). Additionally, we stated that if issuers wished to continue offering these existing standardized plan options with the same cost sharing, they would also be permitted to do so, and enrollees in these plans would continue to be auto-reenrolled in these plans from one plan year to the next, absent selecting a different plan or discontinuing coverage. However, we stated that these plans would no longer be visually distinguished as standardized plan options on
HealthCare.gov
or the DE pathways. Finally, we stated that if issuers wished to continue offering these existing standardized plan options but also wished to modify these plans' cost sharing structures, they would be permitted to do so, but these issuers would continue to be subject to the requirements under the definition of “plan” at § 144.103 and to the uniform modification requirements at § 147.106.
d. Rationale for Proposal
We proposed this approach for several reasons. To begin, when we reintroduced standardized plan options in the 2023 Payment Notice (87 FR 27316 through 27317), we noted that
City of Columbus
vacated the discontinuation of standardized plan options in the 2019 Payment Notice. We then stated that several commenters stated that HHS was not legally obligated to resume standardized plan options under this ruling. These commenters stated that the previous Administration simply provided insufficient justification for discontinuing standardized plan options, but that discontinuing them was not unlawful. These commenters suggested that instead of resuming standardized plan options, HHS should issue a new rule with a more thorough explanation than what was provided in the 2019 Payment Notice explaining why standardized plan options should remain discontinued.
In response to these comments, in the 2023 Payment Notice (87 FR 27316 through 27317), we acknowledged and agreed that
City of Columbus
did not require HHS to resume standardized plan options. However, we stated that this ruling caused us to reevaluate our previous decision to discontinue standardized plan options in the 2019 Payment Notice. We also stated that we believed it was appropriate to resume standardized plan options at that time since the contemporary market conditions differed significantly from the market conditions present when standardized plan options were discontinued in the 2019 Payment Notice—namely, the individual market was no longer considered to be at risk of destabilization.
In the 2023 Payment Notice (87 FR 27316 through 27317), we further stated that the stabilization of the individual market was demonstrated by the proliferation of plan offerings, increased issuer participation in the Exchanges, and record enrollment. We thus stated that resuming standardized plan options at that time could play a constructive role in enhancing the consumer experience, increasing consumer understanding, and simplifying the decision-making process for consumers on the Exchanges, despite the fact that
City of Columbus
did not legally obligate HHS to do so.
In the 2023 Payment Notice (87 FR 27316), we further stated that we believed standardized plan options could play an important role in that simplification by allowing consumers to compare offerings based on other meaningful features outside of cost sharing structures, such as premiums, networks, formularies, and quality ratings. We then stated that employing standardized plan option requirements at that time would allow consumers to
( printed page 29711)
more easily and more meaningfully differentiate between choices and select a plan that meets their unique health care needs.
Thus, issuers that offer QHPs through the FFEs and SBE-FPs have been required to offer standardized plan options at every product network type, at every metal level (with the exception of the non-expanded bronze metal level since PY 2024), and throughout every service area they offer non-standardized plan options since PY 2023. As such, we stated in the proposed rule (91 FR 6385) that we have accumulated 4 plan years of experience (PY 2023 through PY 2026) administering these standardized plan option policies. We stated that this cumulative experience provides us with a comprehensive and nuanced perspective regarding weighing both the advantages and disadvantages of requiring FFE and SBE-FP QHP issuers to offer standardized plan options, whether this strategy aligns with our originally articulated objectives with standardized plan option policies, and whether this strategy has yielded the intended results.
We stated (91 FR 6385) that based on this experience, we concluded that requiring FFE and SBE-FP QHP issuers to offer standardized plan options is an ineffective strategy in enhancing the consumer experience, increasing consumer understanding, and simplifying the plan selection process—the originally articulated objectives of employing our standardized plan option policies. We stated that this is primarily because requiring issuers to offer standardized plan options at every product network type, at every metal level, and throughout every service area that they offer non-standardized plan options led to an increase in the total number of QHPs that issuers offer through the FFEs and SBE-FPs in PY 2023 (the first year in which the requirement to offer these plans was introduced), which exacerbated plan proliferation—directly counteracting our originally articulated objectives.
In fact, we stated (91 FR 6385) that the resumption of standardized plan options and the introduction of the requirement for FFE and SBE-FP QHP issuers to offer standardized plan options coincided with an increase in the weighted average number of total plans available per enrollee from 108 in PY 2022, the year before the introduction of the requirement to offer standardized plan options, to 114 in PY 2023, the year in which this requirement was introduced, with most of this increase in plan offerings being comprised of standardized plan options. Furthermore, we noted that plan proliferation as measured by the weighted average number of total plans offered per issuer (which is derived by dividing the weighted average number of total plans available per enrollee by the weighted average number of total issuers per enrollee) increased from 16.9 in PY 2022 to 17.3 in PY 2023—meaning each issuer on average tended to offer a higher number of plans after the imposition of the requirement to offer standardized plan options than the year before this requirement was made effective.[292]
Furthermore, we noted (91 FR 6386) that even with the introduction of the non-standardized plan option limit of four in PY 2024 and its reduction to two as well as the introduction of the exceptions process in PY 2025, the net impact of both the requirement to offer standardized plan options as well as the subsequent imposition of non-standardized plan option limits and exceptions on the weighted average number of total plans available per enrollee and the weighted average number of total plans offered per issuer (including both standardized and non-standardized plan options) was marginal—despite the substantially increased regulatory complexity and the associated burden of creating and submitting certification applications for new plans (standardized plan options) and correspondingly adjusting existing portfolios of plan offerings (non-standardized plan options).
Specifically, we noted that the weighted average number of total plans available per enrollee decreased from 114 in PY 2023 to 100 in PY 2024 and remained consistent at 100 in PY 2025. We further noted that the weighted average number of total plans offered per issuer decreased from 17.3 in PY 2023 to 14.7 in PY 2024 and 13.7 in PY 2025. Thus, we noted that from PY 2022, before this suite of standardized plan option policies was introduced, there was a weighted average number of 108 total plans available per enrollee and a weighted average number of 16.9 total plans offered per issuer, whereas in PY 2025 (after several consecutive years imposing novel layers of requirements), these same measures were 100 and 13.7, respectively.
We stated (91 FR 6386) that we do not believe the marginal net reductions in the weighted average number of total plans available per enrollee and the weighted average number of total plans offered per issuer achieved by introducing this suite of standardized plan option and non-standardized plan option limit requirements warrant imposing additional burden on issuers or impeding issuer innovation in plan design choice. We stated that this is especially true given that these metrics continue to remain significantly elevated compared to only several plan years ago. We noted, for example, that in PY 2020, the weighted average number of total plans available per enrollee was 39, and the weighted average number of total plans offered per issuer was 11.1. We noted that the impact of our non-standardized plan option limits and exceptions process policies on these metrics and plan proliferation were discussed in greater detail in section III.E.9. of the proposed rule.
We stated (91 FR 6386) that the increase in the weighted average number of total plans available per enrollee from PY 2022 to PY 2023 (which arose primarily from the introduction of the requirement for issuers to offer standardized plan options), even taken altogether with the subsequent marginal net reductions in PY 2024 and PY 2025 (which arose primarily from the introduction of the non-standardized plan option limit of four in PY 2024 and the reduction of this limit to two as well as the introduction of the exceptions process in PY 2025), is particularly important.
We noted (91 FR 6386) that we have utilized this metric, the weighted average number of total plans per enrollee, as opposed to the unweighted average number of total plans per enrollee, as the primary metric by which to evaluate plan choice overload because utilizing weighted averages takes into consideration the number of enrollees in a particular service area when calculating the average number of plans available to enrollees. We stated that as a result of weighting averages by enrollment, service areas with a higher number of enrollees have a greater impact on the overall average than service areas with a lower number of enrollees. Thus, we stated that weighting averages by enrollment allows a more representative metric to be calculated that more closely resembles the actual experience of enrollees.
Therefore, we stated (91 FR 6386) that, as measured by this metric, the weighted average number of total plans per enrollee, the plan proliferation that occurred subsequent to the introduction of the requirement for FFE and SBE-FP QHP issuers to offer standardized plan options in PY 2023 is inconsistent with our originally articulated objectives of
( printed page 29712)
enhancing the consumer experience, increasing consumer understanding, and simplifying the plan selection process for consumers on
HealthCare.gov
—even with the marginal net reductions that occurred subsequent to the introduction of non-standardized plan option limits and its reduction from four to two in PY 2024 and PY 2025, respectively. As we stated in the comment solicitation on choice architecture and preventing plan choice overload in the 2023 Payment Notice (87 FR 27345 through 27347), we noted that this is because increasing the total number of plans that consumers must compare and evaluate increases the risk of plan choice overload, suboptimal plan selection, and unexpected financial harm.
We stated (91 FR 6386) that based on our 4 plan years of experience (PY 2023 through PY 2026) administering this suite of standardized plan option and non-standardized plan option limits and exceptions policies, we have concluded that a marginal net reduction in the number of plan choices in the FFEs and SBE-FPs created by the approach of imposing requirements to offer standardized plan option and imposing non-standardized plan option limits and exceptions has significant disadvantages—namely, imposing additional burden and constraining issuer innovation and consumer choice.
We further noted (91 FR 6386) that the FFEs operate under constraints that differ substantially from other contexts in which standardized plan options have been implemented, such as in States with a State Exchange model type. In particular, we stated that there is a significant degree of heterogeneity on the FFEs (for example, in terms of consumer demographics, health care needs, and preferences) given that there are currently 28 States with an FFE model type, and it is impractical to design a standardized plan option offering that issuers must conform to regardless of the market dynamics in a given location. We further stated that we do not believe that it is feasible for HHS to more precisely tailor specific plan designs and requirements to the unique circumstances and market conditions in each State and update these plan designs on an annual basis. Finally, we stated that we do not believe that such an approach would be warranted in the first place given the limited efficacy that these policies have demonstrated in the last several years.
Relatedly, we stated (91 FR 6386) that the strategy of requiring issuers to offer standardized plan options as well as differentially displaying these plans on
HealthCare.gov
and the DE pathways (which is discussed in greater detail later in this section) was intended to enhance plan comparability for consumers navigating the plan selection process. We stated that, theoretically, requiring issuers to offer plans with standardized cost sharing parameters would facilitate the plan selection process by reducing the number of factors that consumers must consider when evaluating all available plan options—since a certain subset of plans would have the same cost sharing parameters. We stated that as a result of having access to plans with standardized cost sharing parameters, consumers would theoretically have the ability to shift their focus to other important plan attributes, such as premiums, benefit coverage, provider networks, formularies, and quality ratings, during the plan selection process.
However, we stated (91 FR 6387) that based on our 4 plan years of experience (PY 2023 through PY 2026) administering these standardized and non-standardized plan option policies, we have found that in practice, given that standardized plan options continue to be offered alongside non-standardized plan options, whether a particular plan offering was a standardized or non-standardized plan option served as yet another variable that consumers must consider during the plan selection process, adding an additional layer of complication. Furthermore, we noted that in our experience, we have found when consumers are faced with a large number of heterogeneous plan options, they continue to rely primarily on premiums, networks, and issuer brand—meaning that standardizing cost sharing parameters by itself (especially when doing so only for a subset of all available plan options) fails to meaningfully reduce decision complexity for consumers.
In the proposed rule (91 FR 6387), we also considered more recent literature examining the effects of offering standardized plan options alongside non-standardized plan options. We highlighted a 2024 study demonstrating that the introduction of “Simple Choice” plans in PY 2017 and PY 2018 was associated with a reduction in gross premiums.[293]
Although we acknowledged that these findings contribute to a broader understanding of how plan standardization may influence issuer pricing behavior under certain market conditions, we emphasized that the authors caution against extrapolating these effects beyond the specific context in which they arose. In particular, we noted that the study period coincided with a period of pronounced market instability, characterized by significant issuer exits, rapidly increasing market concentration, and the defunding of cost-sharing reduction payments. The authors concluded that observed premium effects were likely attributable, in part, to issuer uncertainty during this volatile period and stated that similar policies implemented in more stable environments would have likely yielded smaller effects.
We also noted (91 FR 6387) that the study further documented that premium impacts dissipated following the discontinuation of the policy after PY 2018, with no evidence of persistent effects in subsequent years—suggesting that plan standardization, absent continued market disruption or policy-induced uncertainty, did not result in durable structural changes to issuer pricing behavior. We considered this lack of persistence particularly relevant when evaluating the continued necessity of standardized plan option requirements and associated non-standardized plan option limits within the current market context—especially with the increased burden, inhibition of issuer innovation, and constrained consumer choice associated with these policies.
Beyond this more recent literature, we noted (91 FR 6387) that for each plan year since these requirements were introduced in PY 2023, there has consistently been a comparatively low uptake of standardized plan options relative to corresponding non-standardized plan options. In fact, we noted that only 20 percent of total enrollment in the FFEs and SBE-FPs was in standardized plan options in PY 2023, 33 percent in PY 2024, and 33 percent in PY 2025, even with the reduction in non-standardized plan option offerings due to the introduction of the non-standardized plan option limit of four in PY 2024 and its reduction to two in PY 2025.[294]
Relatedly, we noted (91 FR 6387) that 25 percent of total plan offerings were standardized plan options in PY 2023, 28 percent in PY 2024, and 31 percent in PY 2025.[295]
Thus, we stated that total
( printed page 29713)
enrollment in standardized plan options was lower compared to what would be expected based on the total proportion of plans that are standardized plan options in PY 2023 and only increased to be approximately equal with what would be expected as the non-standardized plan option limit was introduced in PY 2024 and reduced in PY 2025. We stated that the consistently low proportion of consumers enrolled in standardized plan options over the years suggests that these plans fail to appeal to consumers compared to corresponding non-standardized plan options—or at the very least that consumers are unable to perceive a meaningful difference between standardized and non-standardized plan options.
Moreover, we noted (91 FR 6387) that even among active plan selections (which includes both consumers currently enrolled in a QHP that are making a new plan selection as well as consumers who are enrolling in any QHP offered through an FFE or SBE-FP for the first time, but excludes consumers who are auto-reenrolled in their current QHP from one year to the next), only 18 percent of consumers in the FFEs and SBE-FPs actively selected standardized plan options in PY 2023, 26 percent in PY 2024, and 18 percent in PY 2025.[296]
We stated that this comparatively lower than expected rate of active plan selections for standardized plan options further suggests that these plans have consistently failed to appeal to consumers—or at the very least that it is difficult for consumers to meaningfully distinguish standardized from non-standardized plan options or ascertain the benefits of enrolling in such plans.
We noted (91 FR 6387) that this consistently low uptake of standardized plan options by FFE and SBE-FP consumers for the last several plan years, as measured by both the proportion of total enrollment in as well as active selections of these plans, has occurred despite the fact that a full suite of differential display features visually distinguishes these plans from corresponding non-standardized plan options on both
HealthCare.gov
and the DE pathways, in accordance with the differential display requirements at §§ 155.205(b)(1), 155.220(c)(3)(i)(H), and 156.265(b)(3)(iv).
We stated (91 FR 6387) that under the present form of differential display on
HealthCare.gov
(and the corresponding forms of differential display on the DE pathways), standardized plan options are labelled “easy pricing” plans, and an accompanying icon visually distinguishes these plans from non-standardized plan options. We noted that accompanying hover text also explains both the benefits and distinctive features of these plans and how these plans differ from non-standardized plan options. We also noted that an additional “quick tip” feature provides greater detail regarding the benefits of standardized plan options—including that these plans contain pre-deductible coverage and that they are easier to compare because they have the same MOOP values, deductibles, and cost sharing within their respective health plan categories. Finally, we noted that consumers have the option to select a filter to view only standardized plan options among all available plan options—which excludes non-standardized plan options from the list of search results.
We stated (91 FR 6388) that even with this full suite of differential display features that visually distinguishes standardized plan options from non-standardized plan options on
HealthCare.gov
and the DE pathways, non-standardized plan options are consistently the more popular option for consumers, with a greater proportion of total enrollment in and active plan selections of non-standardized plan options each plan year since these requirements were introduced in PY 2023. We noted that without this full suite of differential display features that visually distinguishes standardized plan options from non-standardized plan options, standardized plan options would likely constitute an even lower proportion of both total enrollment and active plan selections, further suggesting that these plans have consistently failed to appeal to consumers compared to non-standardized plan options.
Furthermore, we stated (91 FR 6388) that total enrollment in and active selections of standardized plan options would be conceivably lower without the progressively more stringent non-standardized plan option limits (since there would have been a greater number of non-standardized plan options for consumers to select from). We stated that given the consistently low proportion of total enrollment in and active selections of standardized plan options each plan year since these requirements were introduced in PY 2023, we no longer believe that the benefits of requiring issuers to offer these plans outweighs the burden of requiring them doing so—especially since employing this strategy has failed to achieve our originally articulated objectives.
Specifically, we stated (91 FR 6388) that the burden of requiring issuers to offer these plans includes creating new plans that have cost sharing parameters that conform with the designs specified by HHS in annual rulemaking, the burden for both issuers and HHS in certifying a greater number of plans during QHP certification each year (standardized plan options as well as non-standardized plan option limit exceptions process plans), and the burden on issuers correspondingly adjusting portfolios of plan offerings (non-standardized plan options).
We noted (91 FR 6388) that in addition to enhancing the consumer experience, increasing consumer understanding, and simplifying the decision-making process for consumers purchasing coverage through the Exchanges, as we stated in the 2023 Payment Notice (87 FR 27311), another original objective of requiring FFE and SBE-FP QHP issuers to offer these standardized plan options was combatting discriminatory benefit designs. We stated that we attempted to achieve this objective in our approach to the design of these plans.
In particular, we noted (91 FR 6388) that each plan year since we introduced standardized plan options in PY 2023, in our design of these plans, we exempted the following frequently utilized benefit categories from the deductible at every metal level: primary care visits, specialist visits, mental health and substance use outpatient office visits, speech therapy, physical and occupational therapy, and generic drugs—with an increasing number of benefit categories being exempted from the deductible at higher metal levels. We stated that we adopted this approach since exempting benefits from the deductible reduces barriers to access for these services and makes it easier (that is, less expensive) for consumers to obtain these health care services. We noted that we also attempted to combat discriminatory designs by requiring flat copayments as the form of cost sharing instead of coinsurance rates for a greater number of benefit categories. We stated that we incorporated this plan design feature to enhance consumer certainty and reduce the risk of unexpected financial costs when obtaining health care.
We stated (91 FR 6388) that we continue to recognize that subjecting additional benefit categories to the deductible and including coinsurance rates as the form of cost sharing instead of flat copayments may make it more difficult for consumers to obtain the
( printed page 29714)
corresponding health care services. However, we acknowledged that these design features (specifically, pre-deductible benefit coverage and flat copayments for the aforementioned benefit categories) are routinely included for the corresponding benefit categories in many non-standardized plan option offerings, and with similar cost sharing amounts. We stated that this is because, as we stated in the 2023 Payment Notice (87 FR 27319), we design these standardized plan options to mirror the most popular plan design features of QHPs offered through the FFEs and SBE-FPs in previous plan years.
More specifically, regarding the methodology we employ to design these plans, we noted (91 FR 6388) that in the 2024 Payment Notice (88 FR 25848), we stated that we design these standardized plan options by selecting the most popular cost sharing type for each benefit category (which is a copayment or coinsurance rate that is either subject to or exempt from the deductible); selecting enrollee-weighted median cost sharing values for each of these benefit categories (as well as for the annual limitation on cost sharing and deductible values) based on refreshed cost sharing and enrollment data; modifying these plans to be able to accommodate State cost sharing laws; and decreasing the AVs for these plan designs to be at the floor of each AV
de minimis
range, primarily by increasing deductibles.
We stated (91 FR 6388) that employing this methodology in the annual design of these standardized plan options has resulted in these plans being comparable in many respects to corresponding non-standardized plan options that millions of consumers are already enrolled in. We noted that this further means that pre-deductible benefit coverage and flat copayments as the form of cost sharing instead of coinsurance rates are design features that are not exclusive to standardized plan options. We stated that, instead, these plan design features largely reflect market consensus and do not substantially deviate from this consensus. We also stated that the fact that these plan design features are already routinely included in many non-standardized plan options means that we could combat discriminatory plan designs (another originally articulated objective for reintroducing the requirement for issuers to offer standardized plan options) without subjecting both issuers and HHS to the increased burden of requiring issuers to offer and submit certification applications for these plans that largely reflect market consensus and existing offerings.
Furthermore, we stated (91 FR 6388) that we believe incorporating coinsurance rates as the form of cost sharing for particular benefits instead of flat copayments can serve an important role in plan design—by promoting greater engagement on behalf of consumers in evaluating health care options and by providing issuers additional levers to control costs, thereby helping to manage rising premiums. We further stated that we believe incorporating coinsurance rates as the form of cost sharing promotes greater engagement on behalf of consumers by encouraging consumers to more comprehensively research the full costs for particular services from different providers. We thus stated that we believe employing coinsurance rates instead of flat copayments as the form of cost sharing for particular benefits is not in itself necessarily discriminatory in nature and is an important factor in controlling costs and by extension counteracting increasing premiums.
Additionally, we stated (91 FR 6388) that the combination of standardized plan option requirements as well as non-standardized plan option limits has increasingly constrained issuers' ability to offer a sufficiently broad range of plans for several plan years. We stated that this includes plans with tiered provider networks, plans with separate medical and drug deductibles (as opposed to integrated medical and drug deductibles), plans with separate medical and drug MOOPs (as opposed to integrated medical and drug MOOPs), HSA-eligible high-deductible health plans (HDHPs), and plans with more than four tiers of prescription drug coverage. We noted that issuers have not been able to offer plans with these design features as standardized plan options since doing so would deviate from the required cost sharing parameters specified by HHS in rulemaking. Thus, we stated that removing this suite of requirements would grant issuers additional flexibility to once more vary plans along these parameters, which would enhance issuer innovation in plan design and consumer choice.
e. Plan Discontinuations
However, we stated in the proposed rule (91 FR 6389) that we recognize that some issuers and consumers may still find certain features of these plan designs valuable. We stated that this is why we were not proposing to require issuers to discontinue their standardized plan option offerings altogether. Instead, we stated that under the proposed approach, FFE and SBE-FP QHP issuers would be permitted to choose whether to discontinue these offerings altogether or to continue offering them with either the same or modified cost sharing, while we simultaneously discontinue the differential display of these plans on
HealthCare.gov
and the DE pathways.
We stated (91 FR 6389) that under our proposed approach, if issuers wished to discontinue their standardized plan option offerings altogether, they would be permitted to do so, and enrollees in these plans would be crosswalked to a different plan in accordance with the crosswalk hierarchy at § 155.335(j). Additionally, we stated that if issuers wished to continue offering these standardized plan options with the same cost sharing, they would also be permitted to do so, and enrollees in these plans would continue to be auto-reenrolled in these plans from one plan year to the next. However, we noted that these plans would no longer be visually distinguished as standardized plan options on
HealthCare.gov
or the DE pathways. Finally, we stated that if issuers wished to continue offering these standardized plan options but also wished to modify these plans' cost sharing structures, they would be permitted to do so, but these issuers would continue to be subject to the requirements under the definition of “plan” at § 144.103 and to the uniform modification requirements at § 147.106.
We noted (91 FR 6389) that in most scenarios where an issuer modifies the cost sharing structure of one of its standardized plan option offerings, the newly modified plan that was formerly the standardized plan option would be considered a new plan and would therefore require a new plan ID. We stated that in this scenario, enrollees would be crosswalked from the discontinued plan to another plan in accordance with the crosswalk hierarchy at § 155.335(j). We stated that these enrollees could be crosswalked into the newly modified plan that was formerly the standardized plan option, or an entirely different plan altogether, depending on the unique circumstances in each county.
However, we stated (91 FR 6389) that under the definition of “plan” at § 144.103, a State may permit issuers to make greater changes to a plan's cost sharing while still permitting that plan to be considered the same plan—thus maintaining the same plan ID. Furthermore, we stated that under § 147.106(e)(3)(iv), as long as the variation in cost sharing is solely related to changes in cost and utilization of medical care, or to maintain the same
( printed page 29715)
metal tier level (and other applicable requirements under § 147.106(e) are met), the modifications could be considered uniform (thus, a viable exception to guaranteed renewability).
We stated (91 FR 6389) that in the scenario where an issuer modifies what was formerly a standardized plan option's cost sharing structure while maintaining the same plan ID, enrollees in the plan would be auto-reenrolled from one plan year to the next. We stated that in either case, whether the modification of a former standardized plan option's cost sharing results in that plan being considered the same or a different plan, enrollees would be crosswalked in accordance with the crosswalk hierarchy at § 155.335(j), and that plan would no longer be differentially displayed as a standardized plan option on
HealthCare.gov
or the DE pathways. We stated that adopting this approach would effectively remove the standardization component of this suite of policies while minimizing the risk of disruption for consumers enrolled in and issuers of these plans.
We stated (91 FR 6389) that, altogether, we believe that employing this suite of policies for the last several plan years has failed to achieve the originally articulated objectives of enhancing the consumer experience, increasing consumer understanding, and combatting discriminatory benefit designs. We stated that this failure is demonstrated by exacerbated plan proliferation in PY 2023 and the comparatively low uptake of these standardized plan options despite the full suite of differential display features that visually distinguishes these plans from corresponding non-standardized plan options. Finally, we noted that these standardized plan options reflect market consensus and incorporate the most popular plan design features of many existing non-standardized plan option offerings, meaning these plan design features are not exclusive to standardized plan options.
We stated (91 FR 6389) that given that imposing these requirements has increased burden for both issuers and HHS (for example, by requiring issuers to create and submit certification applications for additional plans) and unnecessarily constrained issuers in plan design while failing to achieve our originally articulated objectives, we no longer believe that the advantages of employing this strategy outweigh the disadvantages of doing so. We stated that we therefore believe that discontinuing the full suite of standardized plan options policies (in conjunction with discontinuing non-standardized plan option limits and exceptions, discussed in section III.E.9. of the proposed rule) would reduce issuer and HHS burden and provide more flexibility for issuers to innovate in plan design.
Accordingly, we stated (91 FR 6389) that the proposal would remove the following from our regulations effective beginning PY 2027: the definition of “standardized option” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b), as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv). We stated that the proposal would also entail the cessation of the annual design and publication of these plans in the applicable Payment Notice rulemaking for each plan year.
We sought comment (91 FR 6389) on this proposal. We also sought comment on potential regulatory alternatives that would allow us to achieve the same goals of simplifying the plan selection process and reducing burden without discontinuing this suite of policies in its entirety. In particular, we sought comment on continuing to require issuers to offer standardized plan options only at particular metal levels, such as the bronze and silver metal levels (instead of at every metal level at which they offer non-standardized plan options). We also sought comment on requiring issuers to offer standardized plan options only in certain service areas in which they offer a certain number of non-standardized plan options. We also sought comment on transitioning from requiring issuers to offer these standardized plan options to once more allowing issuers to voluntarily offer them—as was the approach with the previous iteration of the policy—while we continue to maintain the differential display of these plans on
HealthCare.gov
and the DE pathways.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal to discontinue the full suite of standardized plan option policies below.
Comment:
Many commenters supported the proposal to discontinue these standardized plan option policies. These commenters stated that requiring issuers to offer standardized plan options (especially while simultaneously limiting the number of non-standardized plan options they can offer) has increasingly constrained issuers' ability to design and offer plans that reflect evolving market conditions and consumer preferences. These commenters cited plans with tiered provider networks, HSA-eligible HDHPs, plans with separate medical and drug MOOPs and deductibles (compared to integrated medical and drug MOOPs and deductibles), plans with more than four formulary tiers, plans that reduce cost sharing for virtual visits, and individual coverage health reimbursement arrangements (ICHRAs) as examples of benefit designs that have been increasingly constrained by these standardized plan option policies. These commenters thus stated that discontinuing these standardized plan option policies would greatly enhance the degree of consumer choice.
Commenters who supported discontinuing the requirement to offer standardized plan options also emphasized that plans with standardized cost sharing can still differ significantly in other important dimensions, such as in terms of benefit coverage, cost sharing for benefit categories outside those specified by HHS in annual rulemaking, provider networks, formularies, and utilization management practices. These commenters subsequently stated that formally designating plans that conform with the required cost sharing parameters specified by HHS in rulemaking as standardized plan options (along with differentially displaying these plans on
HealthCare.gov
and DE platforms) could therefore be considered misleading and can be confusing for consumers who are led to believe that these plans are completely standardized in all regards.
Commenters who supported discontinuing the requirement for issuers to offer standardized plan options further agreed that standardized plan options have failed to meaningfully simplify consumer choice as was originally intended—especially since standardized plan options continue to exist alongside non-standardized plan options. These commenters stated that contrary to the original intention of employing these standardized plan option policies—simplifying the plan
( printed page 29716)
selection process—whether a particular plan offering is a standardized or non-standardized plan option in practice serves as yet another variable that consumers must consider during the plan selection process, introducing an additional layer of complexity.
Commenters further stated that the failure of these standardized plan option policies to meaningfully simplify the plan selection process is evinced by the fact that the total number of plan offerings remains similar to the total number of plan offerings before the imposition of these requirements. Specifically, these commenters highlighted that the weighted average total number of plans available per enrollee was only reduced from 108 in PY 2022 to 100 in PY 2025—despite imposing multiple layers of novel requirements for several consecutive years, which substantially increased issuer burden and caused considerable market disruption in the form of plan discontinuations.
In contrast, several commenters opposed the proposal to discontinue the requirement to offer standardized plan options. These commenters stated that standardized plan options improve consumers' ability to make informed plan selections by facilitating more meaningful comparisons across plans. These commenters stated that standardizing cost sharing enhances transparency and allows consumers to more meaningfully evaluate other important plan attributes, such as provider networks, formularies, and quality ratings rather than relying on premium differences alone. Several commenters thus stated concern that removing standardized plan options would increase complexity for consumers and make plan selection more difficult, particularly for individuals with limited health insurance literacy.
Commenters further stated that standardized plan options promote more predictable and consumer-friendly cost sharing, including the use of copayments in place of coinsurance rates and the coverage of certain services before the deductible. Relatedly, several commenters emphasized that standardized plan options help mitigate the risk of potentially discriminatory benefit designs by reducing issuers' ability to structure benefits or formularies in ways that discourage enrollment by individuals with chronic and high-cost conditions. Several commenters stated concern that eliminating standardized plan options could increase opportunities for risk segmentation (for example, by allowing issuers greater leeway in designing plans in such a manner to encourage the enrollment of healthier and lower risk consumers while simultaneously discouraging the enrollment of less healthy and higher risk consumers), potentially leading to less stable risk pools and greater premium volatility.
Commenters who supported continuing requiring issuers to offer standardized plan options also highlighted that enrollment in and active selection of standardized plan options has increased in recent years and now represents a substantial share of total enrollment in the FFEs and SBE-FPs. Some commenters further pointed to the experience of State Exchanges that have adopted standardized plan option requirements, stating that these approaches have improved affordability, access, and consumer understanding. Finally, several commenters raised concerns about potential disruption to current enrollees, stating that discontinuing standardized plan options could force consumers to transition to new plans that may not meet their existing health care needs, potentially resulting in changes to provider networks, covered benefits, or prescription drug coverage.
Response:
For the reasons stated earlier in this section of this final rule, we agree with commenters who stated that requiring issuers to offer standardized plan options has constrained issuers' ability to design plans that reflect evolving market conditions and consumer preferences. For the reasons stated earlier in this section of this final rule, we also agree that these standardized plan option policies have constrained issuers' flexibility to develop innovative benefit designs. This includes plans with tiered provider networks, HSA-eligible HDHPs, plans with separate medical and drug MOOPs and deductibles (compared to integrated medical and drug MOOPs and deductibles), plans with more than four formulary tiers, plans that reduce cost sharing for virtual visits, and ICHRAs. Accordingly, we believe that discontinuing the requirement for issuers to offer standardized plan options will foster innovation, permit issuers to more readily adapt to evolving market dynamics, and ensure that consumers continue to retain a sufficient degree of choice in plan selection.
We also agree with commenters that standardized plan options may still differ across other important dimensions, such as in terms of benefit coverage, cost sharing for benefit categories not specified by HHS in rulemaking, provider networks, formularies, and utilization management practices. We therefore agree that designating these plans as standardized plan options despite these significant differences can be potentially misleading and confusing for consumers.
We also agree that contrary to the original intention of our standardized plan option policies—simplifying the plan selection process—whether a particular plan offering is a standardized or non-standardized plan option in practice serves as yet another variable that consumers must consider during the plan selection process, introducing an additional layer of complexity. This additional variable that consumers must consider in turn complicates the plan selection process and subsequently increases the risk of suboptimal plan selection.
We also agree that the total number of plan offerings remaining similar to the total number of plan offerings before the imposition of these requirements demonstrates that these standardized plan options failed to achieve our intended result. Specifically, we note that that the weighted average total number of plans available per enrollee was only reduced from 108 in PY 2022 to 100 in PY 2025. This is despite imposing multiple layers of novel requirements for several consecutive years, which substantially increased issuer burden and caused considerable market disruption in the form of plan discontinuations. The market disruption and plan discontinuations that occurred subsequent to the imposition of these requirements is discussed in greater detail in section III.E.9. of this final rule.
We acknowledge that standardized cost sharing may facilitate more direct comparisons between some subset of all available plan offerings, especially when supplemented with the differential display features for these plans on
HealthCare.gov
and DE platforms (such as by filtering to view only standardized plan options), which may benefit consumers with limited health insurance literacy, but we do not believe that this limited benefit warrants imposing substantial burden, inhibiting issuer innovation, constraining consumer choice, and causing considerable market disruption in the form of plan discontinuations. We further believe that consumers consider multiple factors beyond cost sharing, including premiums, provider networks, formularies, and total expected out-of-pocket costs. Standardizing cost sharing alone (especially if only for a subset of all benefit categories and for a subset of all plan offerings) does not ensure meaningful comparability for all
( printed page 29717)
available plan options for consumers—and contrary to the original intention of enacting these standardized plan option policies, complicates the plan selection process by introducing another variable that consumers must consider.
Furthermore, we believe that there are more effective and less burdensome alternatives for simplifying the plan selection process than continuing to require issuers to offer standardized plan options. In particular, we believe that making enhancements to plan display, choice architecture, decision-support tools, and other forms of consumer assistance on
HealthCare.gov
and DE platforms, rather than relying on restrictive plan design requirements, is an approach better suited to supporting informed consumer choice—and that such an approach avoids the negative consequences associated with standardized plan options, such as increased burden, inhibited issuer innovation, constrained consumer choice, and continued market disruption in the form of plan discontinuations. We therefore note that we will continue to research enhancements to plan display, choice architecture, decision-support tools, and other forms of consumer assistance on
HealthCare.gov
and encourage issuers and other DE partners to do the same.
We further considered comments stating that standardized plan options promote more predictable cost sharing, including the use of copayments and pre-deductible coverage. We do not believe it is necessary to require issuers to offer standardized plan options to achieve these outcomes. This is because issuers continue to retain the flexibility to incorporate these features into plan designs absent standardization requirements and frequently do so. As we stated in the proposed rule, we designed these plans to incorporate the most popular plan design features of many existing non-standardized plan option offerings—meaning many of these plan design features largely reflect market consensus, are not exclusive to standardized plan options, and are already frequently included in many standardized plan options currently offered through the FFEs and SBE-FPs.
For example, since the reintroduction of these standardized plan option policies in PY 2023, we finalized every annual iteration of plan designs with pre-deductible copayments as the form of cost sharing for the primary care visit benefit category at every metal level. When we initially created the plan designs for PY 2023, we based these plan designs on FFE and SBE-FP cost-sharing and enrollment data from PY 2021, which was the most recent available data at that time. In PY 2021, 91 percent of FFE and SBE-FP consumers were enrolled in plan offerings with pre-deductible copayments as the form of cost sharing for the primary care visit benefit category at the standard silver metal level. Furthermore, in the FFEs and SBE-FPs in PY 2021, the weighted average pre-deductible copayment amount for the primary care visit benefit category at the standard silver metal level was $37, while the copayment amount for this benefit category in our plan design at the standard silver metal level for PY 2023 was $40—a difference of only $3. Taken altogether, this means that this plan design feature was not exclusive to standardized plan options and was already incorporated into the vast majority of non-standardized plan option offerings—as is true for many other plan design features.
We also considered comments stating that standardized plan options help mitigate discriminatory benefit designs and reduce opportunities for risk segmentation. We note that existing nondiscrimination requirements, including those at §§ 156.125 and 156.200(e), as well as other FFE and SBE-FP QHP issuer monitoring and compliance mechanisms, continue to apply and prohibit discriminatory benefit designs. These requirements and mechanisms include, as part of Exchange QHP certification reviews, reviews for discriminatory language (which prohibit issuer marketing materials and benefit descriptions from containing language or content that discriminates against or discourages enrollment by individuals based on protected characteristics); cost-sharing outliers (which identify plans with unusually high or potentially discriminatory cost sharing relative to other plans to prevent the inclusion of plan attributes that could discourage enrollment by individuals with significant health needs); and various treatments under the treatment protocol calculator (which evaluate whether issuer utilization management policies (such as prior authorization and step therapy) are applied in a clinically appropriate and non-discriminatory manner to prevent practices that could inappropriately restrict access to medically necessary care or discourage enrollment by individuals with significant health needs). Due to their comprehensive scopes and well-established review processes, we believe that these existing protections are sufficient to address these concerns without requiring issuers to offer standardized plan options.
We further considered comments expressing concern that eliminating standardized plan options could negatively affect risk pool stability and increase premium volatility. We do not believe that continuing to require issuers to offer standardized plan options is necessary to maintain stable risk pools—especially since risk pools were relatively stable prior to the introduction of the requirement to offer these plans beginning in PY 2023. Additionally, since we designed standardized plan options to reflect and incorporate the most popular plan design features of QHPs offered in the FFEs and SBE-FPs, many non-standardized plan options that continued to be offered have these same plan design features. Thus, the discontinuation of the requirement for issuers to offer these plans would largely reflect a return to the status quo from several years ago with respect to risk pool stability and premium volatility.
Furthermore, other program features, including risk adjustment requirements (such as those under part 153) and rating rules (such as those at § 147.102) will help ensure that this discontinuation does not destabilize risk pools and does not encourage adverse selection (namely, issuers designing plans in such a manner to encourage the enrollment of healthier and lower risk consumers and discourage the enrollment of less healthy and higher risk individuals).
We also considered comments citing increasing enrollment in standardized plan options and the experience of State Exchanges that have adopted standardized plan requirements. While we acknowledge that a significant number of consumers have actively selected and enrolled in standardized plan options, we do not believe that this fact alone justifies maintaining these requirements—especially since these standardized plan options reflect the most popular plan design attributes of existing offerings and are thus largely duplicative of non-standardized plan options.
We further note that active selection of and enrollment in standardized plan options would be substantially lower without differential displaying these plans on
HealthCare.gov
and DE platforms as well as concurrently limiting the number of non-standardized plan options that issuers can offer—both of which have had the effect of actively steering consumers into standardized plan options but, despite this, have not resulted in overwhelming enrollment in standardized plan options. We also
( printed page 29718)
reiterate that these policies significantly constrained issuer innovation in plan design and the degree of consumer choice while simultaneously imposing substantial burden and causing a considerable degree of market disruption.
We also note that State Exchanges continue to retain the flexibility to adopt and implement State standardized plan option requirements, and this policy does not constrain their ability to do so. We further note that while requiring issuers to offer standardized plan options may be appropriate in those particular States, the nature of the markets in the FFEs and SBE-FPs differs substantially from the nature of the markets in those States (such as the markets in Connecticut, Massachusetts, and Vermont). Namely, the consumer populations (and by extension the unique health care needs) within the FFEs and SBE-FPs are significantly more heterogeneous in nature, and it is therefore difficult to impose an effective, uniform approach to plan design across all these States.
Finally, we acknowledge commenters' concerns regarding potential disruption to current enrollees, and we acknowledge that some enrollees may be required to transition to different plan offerings if issuers discontinue their existing standardized plan options. That said, as previously stated, standardized plan options were designed to largely reflect industry consensus on numerous fronts, and therefore we do not expect the discontinuation of standardized plan options to cause systematic disruption. Further, we expect that issuers will continue to offer a range of plans that meet consumer needs—including with plan design features previously incorporated into standardized plan options, since standardized plan options were designed to reflect the most popular plan design features in the FFEs and SBE-FPs.
In addition, as explained earlier in this section of this final rule, existing enrollment and crosswalk processes, such as those at § 155.335(j), are designed to support consumers during transitions and minimize disruption. We further reiterate that we are not requiring issuers to discontinue their standardized plan options. Instead, we are simply discontinuing the requirement for issuers to offer these plans as well as the differential display of these plans on
HealthCare.gov
and DE platforms.
Comment:
Several commenters stated that the proposal to discontinue these standardized plan option policies is arbitrary and capricious under the Administrative Procedure Act. These commenters cited prior rulemaking and
City of Columbus,
which included the vacatur of the 2019 policy to discontinue the designation of certain plans as “standardized options.”
These commenters stated that HHS failed to adequately justify its departure from longstanding findings in the 2017, 2018, and 2023 through 2025 Payment Notices, in which HHS concluded that standardized plan options enhance consumer understanding and simplify plan comparisons by reducing variation in cost sharing. These commenters further stated that HHS did not sufficiently explain why these previously identified benefits are now afforded less weight. These commenters stated that reliance on findings of only “marginal” reductions in plan counts is insufficient, particularly given evidence that even modest improvements in plan comparability can improve consumer outcomes.
Commenters also cited research indicating that excessive plan choice can lead to consumer confusion and suboptimal plan selection due to difficulty processing complex health insurance information and fatigue—which may lead to unnecessary spending and unexpected financial harm for consumers.[297 298]
These commenters further stated that HHS' conclusion that standardized plan options are ineffective in improving consumer experience is not adequately supported. Finally, these commenters stated that the proposal is internally inconsistent. They noted that, while HHS expresses concern regarding consumer experience and potential choice complexity, it simultaneously proposes to eliminate both standardized plan options and limits on non-standardized plan options. Commenters stated that this approach could increase the number of available plans and exacerbate consumer confusion, undermining the rationale for the policy change.
Response:
We do not agree with commenters' points. In the proposed rule, we expressly acknowledged the history of standardized plan option policies and stated that, based on more recent experience administering and operationalizing these policies, we thoughtfully reassessed their efficacy and have concluded that adopting these standardized plan option policies was an ineffective approach for improving the plan selection process. We offered ample evidence for this shift.
For example, as we explained in the proposed rule (91 FR 6385 through 6389), the requirement to offer standardized plan options increased both the weighted average number of total plans available per enrollee and the weighted average number of total plans offered per issuer in PY 2023; introduced another variable that consumers must consider during the plan selection process; yielded comparatively low enrollment in and active selection of standardized plan options despite the differential display of these plans as well as concurrent limits on the number of non-standardized plan options; and duplicated the most popular plan design features of plans offered through the FFEs and SBE-FPs—while simultaneously inhibiting issuer innovation in plan design, constraining the degree of consumer choice, imposing substantial burden, and causing significant market disruption.
We also do not agree that the proposal failed to address prior findings regarding the potential benefits of standardized plan options. While prior rulemaking identified potential benefits related to consumer understanding and plan comparison, we stated in the proposed rule (91 FR 6385 through 6389) that these benefits have not materialized to a sufficient degree in practice to justify continuing to require issuers to offer standardized plan options and limiting the number of non-standardized plan options.
Specifically, we found that the marginal net reductions in the weighted average number of total plans available per enrollee and per issuer associated with these standardized plan option and non-standardized plan option limits and exceptions policies were modest and likely indiscernible to consumers during the plan selection process. In particular, in PY 2022, the year before introduction of the standardized plan option policies, there was a weighted average number of 108 total plans available per enrollee and a weighted average number of 16.9 total plans offered per issuer. Whereas in PY 2025 (after several consecutive years imposing novel layers of requirements), these same measures were 100 and 13.7, respectively. For the reasons stated in the proposed rule and earlier in this section of this final rule, we concluded that these marginal net reductions do not warrant the ongoing regulatory complexity, increased issuer burden, limitations on issuer flexibility
( printed page 29719)
in plan design, and constraints on consumer choice associated with the current framework.
We further do not agree that the proposal fails to explain why prior findings are now afforded less weight, and we do not agree that prior findings are indeed “afforded less weight.” The proposed rule explains (91 FR 6387) that standardized plan options have operated alongside non-standardized plan options and, even when combined with limits on non-standardized plan options, have not meaningfully reduced overall plan complexity. Based on this experience, we concluded that standardized plan options are not an effective mechanism for achieving the intended goals of improving consumer experience and simplifying plan selection.
We acknowledge commenters' references to research on consumer decision-making and choice overload. However, we do not believe maintaining standardized plan option requirements is the most effective means of addressing concerns about improving consumer experience. We believe the standardized plan option policies inhibited issuer innovation in plan design, constrained the degree of consumer choice, and imposed substantial burden. As discussed earlier in this section, we believe that making improvements to choice architecture, transparency, and consumer decision-support tools are better suited to supporting informed plan selection without imposing prescriptive plan design constraints. We reiterate that we intend to continue researching such enhancements and that we encourage issuers and other DE partners to do the same.
Further, we do not agree that there is an internal inconsistency in discontinuing both standardized plan options and non-standardized plan option limits and exceptions. We determined that both the requirement to offer standardized plan options as well as imposing restrictive non-standardized plan option limits were ineffective tools for achieving their distinct intended objectives and simultaneously imposed unnecessary burden and constraints. Given that standardized plan options are offered alongside non-standardized plan options, whether a particular plan offering is a standardized or non-standardized plan option serves as yet another variable that consumers must consider during the plan selection process. This is contrary to the original intent of simplifying the plan selection process and introduces an additional layer of complexity.
Finally, the fact that eliminating these policies may result in marginal changes to the total number of available plan offerings per consumer and issuer does not render the policy arbitrary where, as here, HHS has reasonably stated its rationale for moving away from this regulatory approach and proposed, with evidence, a more effective approach for enhancing the consumer experience, increasing consumer understanding, and simplifying the decision-making process for consumers on the Exchanges.
Comment:
Several commenters supported continuing the meaningful difference standard under § 156.201(c) (which currently only applies to standardized plan options) and expanding it to apply to non-standardized plan options. These commenters stated concern that, absent a meaningful difference requirement, especially if standardized plan options and non-standardized plan option limits are discontinued, issuers would be permitted to offer numerous plans with only minor or difficult-to-discern differences in cost sharing, benefit designs, or plan marketing conventions.
These commenters stated that this could in turn increase plan proliferation and make it more challenging for consumers to identify coverage that best meets their unique health care and financial needs. These commenters thus suggested that differences in key plan design features, such as MOOPs, deductibles, benefit coverage, provider networks, or formularies should be required for plans to be considered meaningfully different from one another (and thus be permitted to be offered through the FFEs and SBE-FPs). In addition, these commenters recommended continuing monitoring plan offerings to ensure that any meaningful difference standard effectively prevents excessive plan proliferation and reduces consumer confusion.
Response:
We do not agree with commenters' concerns that, absent a meaningful difference requirement, particularly in combination with the discontinuation of standardized plan options and non-standardized plan option limits and exceptions, issuers will offer plans with only minor or difficult-to-discern differences, which could potentially contribute to plan proliferation and make it more challenging for consumers to identify coverage that meets their unique health care needs. In large part, this is because there were only a handful of instances of such duplicate plans out of hundreds of total plan offerings in the FFEs and SBE-FPs in PY 2026 that issuers needed to modify to conform with the standard at § 156.201(c). We expect the number of such duplicative plans to continue to be minimal in future plan years, even without such a standard being in place.
Further, we do not believe that maintaining or expanding a meaningful difference standard to apply to non-standardized plan option offerings (which we also did not propose to do) is the most appropriate or effective mechanism to address these concerns at this time. We believe that such requirements would impose additional operational burdens on issuers (such as by being forced to modify a plan's benefit coverage, cost sharing, MOOP, deductible, provider network, or formulary solely to conform to such a standard—which could also cause disruption to consumers enrolled in those plans).
We also believe that such requirements would fail to consistently yield differences that are meaningful or relevant from a consumer perspective—especially based on our experience administering the meaningful difference standard that was previously codified at § 156.298 from PY 2015 through PY 2018. In fact, when we discontinued the previous version of the meaningful difference standard, we stated (83 FR 17027) that removing the meaningful difference standard would not substantially increase the number of materially similar plans from the same issuer. This is because with the standard—similar to our experience with the standard at § 156.201(c)—there were only a handful of instances of such duplicate plans out of hundreds of total plan offerings in the FFEs and SBE-FPs that had to be modified to conform with the standard at § 156.298.
We are further concerned that such imposing requirements could further constrain issuers' flexibility to design plan offerings that respond to local market conditions and consumer preferences, similar to our concern about the impact of non-standardized plan option limits, discussed in section III.E.9. of this final rule, which is contrary to our current approach. We further acknowledge commenters' recommendations that HHS continue monitoring plan offerings to prevent excessive plan proliferation and consumer confusion. We intend to continue to monitor plan offerings and consumer experience. We further note that improvements to plan display, consumer decision-support tools, and transparency on
HealthCare.gov
and DE platforms will more effectively address concerns related to consumer understanding and plan selection without the unnecessary burden and
( printed page 29720)
constraints of an expanding meaningful difference standard.
Comment:
Several commenters addressed the role of enhancing choice architecture on
HealthCare.gov
and the DE platforms to simplify the plan selection process. These commenters stated that HHS has existing and emerging tools that could be leveraged to better support consumers in navigating plan choices, particularly in the absence of standardized plan options, non-standardized plan option limits, an expanded meaningful difference standard, or other plan design constraints.
These commenters suggested improvements such as more robust filtering capabilities, side-by-side plan comparisons, utilization-based recommendations, and targeted educational prompts to help consumers differentiate among plan options. Some commenters also recommended enabling consumers to more easily identify and filter plans based on specific characteristics, such as disease-specific offerings. Several commenters noted that emerging technologies, including tools that allow consumers to describe their health care needs in natural language and receive personalized cost projections, may facilitate the plan selection process more meaningfully than the suite of standardized plan option policies—and without the disadvantages of this approach.
In addition, several commenters emphasized the importance of clear and accessible plan information, including transparent presentation of provider network participation and cost-sharing obligations for key services such as hospital care. Commenters stated that improving the clarity and usability of plan information would better enable consumers to make informed decisions.
Response:
We agree with commenters that enhancing choice architecture on
HealthCare.gov
and DE platforms is an important component of improving the consumer experience, particularly as the landscape of plan offerings continues to evolve. We also agree that HHS has existing and emerging tools that can support consumers in navigating plan choices and making informed enrollment decisions. For example,
HealthCare.gov
already currently allows consumers to filter search results by a range of plan design features (such as monthly premium, metal level, maximum yearly deductible network type, insurance company, HSA eligibility, medical provider, and prescription drug) and compare up to three plans simultaneously.
We also appreciate commenters' specific recommendations to enhance consumer decision-support tools on
HealthCare.gov
and DE platforms, including through more robust filtering capabilities, improved side-by-side plan comparisons, utilization-based recommendations, and targeted educational prompts. We believe that these types of capabilities (several of which are already supported, including filtering capabilities, side-by-side comparisons, and targeted educational prompts) can help consumers better differentiate among plan options and select coverage that aligns with their needs. We will continue to consider opportunities to enhance these tools, and we encourage issuers and other DE partners to do the same.
We also agree that such tools have the potential to more meaningfully facilitate the plan selection process than employing these standardized plan option policies—and without the disadvantages of this approach. This is because consumers would have an enhanced degree of choice in terms of diverse plan offerings (with issuers no longer being constrained by these standardized plan option policies), and the search results of all available plan offerings on
HealthCare.gov
and DE platforms could then be tailored to unique consumer preferences and health care needs.
We further agree with commenters on the importance of clear, accurate, and accessible plan information, including transparent presentation of provider network participation and cost-sharing obligations for key services. This information is included on
HealthCare.gov
for every available plan option and is presented in a clear and understandable manner. In particular, details regarding each plan's premium, metal level, product network type, provider network, quality rating, estimated total yearly cost, deductible, MOOP, cost sharing, and prescription drug coverage are included in each plan's display card. This information is also accompanied by concise definitions of key terms. Ultimately, we agree that improving the clarity and usability of plan information is critical to enabling consumers to make informed decisions. We will continue to evaluate ways to enhance the presentation of this information, and we encourage issuers and other DE partners to do the same.
Comment:
Several commenters requested clarification on whether plans that were previously designated as standardized plan options in PY 2026 that issuers voluntarily choose to continue offering with either the same or modified cost sharing in PY 2027 are required to adopt any particular plan marketing name and whether it is permissible to continue to use phrases such as “standardized” or any other such similar language in the plan marketing name for these plans.
Response:
Issuers have not been subject to any specific plan marketing name requirements for standardized plan options since the introduction of the requirement to offer these plans in PY 2023, other than the requirements at § 156.225. Instead, issuers have retained the discretion to adopt the plan marketing names that they desire for these plans since PY 2023, subject to the existing requirements at § 156.225. Issuers continue to retain this discretion if they choose to continue offering plans that were previously designated as standardized plan options in PY 2026 with either the same or modified cost sharing in PY 2027. Issuers may also choose to continue including phrases such as “standardized” or any other such similar language in the plan marketing name for these plans, provided those plans names comport with the requirements at § 156.225.
9. Non-Standardized Plan Option Limits (§ 156.202)
In the 2027 Payment Notice proposed rule (91 FR 6390), we proposed to exercise our authority under sections 1311(c)(1) and 1321(a)(1)(B) of the Affordable Care Act to discontinue non-standardized plan option limits and exceptions at § 156.202 effective beginning in PY 2027. Section 1311(c)(1) of the Affordable Care Act directs the Secretary to establish criteria for the certification of health plans as QHPs. Section 1321(a)(1)(B) of the Affordable Care Act directs the Secretary to issue regulations that set standards for meeting the requirements of title I of the Affordable Care Act, which includes section 1311, for, among other matters, the offering of QHPs through such Exchanges.
In the 2023 Payment Notice proposed rule (87 FR 27345 through 27347), we solicited comment on choice architecture and preventing plan choice overload. In this comment solicitation, we noted that although we continued to prioritize competition and choice on the FFEs and SBE-FPs, we were concerned about plan choice overload, which can result when consumers have too many choices in plan options. We referred to a 2016 report by the RAND Corporation reviewing over 100 studies which concluded that having too many health plan choices can lead to poor enrollment decisions due to the difficulty consumers face in processing complex health insurance coverage
( printed page 29721)
information.[299]
We also referred to a study of consumer behavior in Medicare Part D, Medicare Advantage, and Medigap that demonstrated that a choice of 15 or fewer plans was associated with higher enrollment rates, while a choice of 30 or more plans led to a decline in enrollment rates.[300]
With this concern in mind, in the 2023 Payment Notice proposed rule (87 FR 27345 through 27347), we stated that we were interested in exploring possible methods of improving choice architecture and preventing plan choice overload. We stated interest in exploring the feasibility and utility of limiting the number of non-standardized plan options that QHP issuers could offer through the FFEs and SBE-FPs as one option to reduce the risk of plan choice overload and to further streamline and optimize the plan selection process for consumers on the FFEs and SBE-FPs.
Accordingly, we sought comment on the impact of limiting the number of non-standardized plan options that issuers can offer through the FFEs and SBE-FPs, on effective methods to achieve the goal of reducing the risk of plan choice overload and to further streamline and optimize the plan selection process for consumers on the FFEs and SBE-FPs, the advantages and disadvantages of these methods, and if there were alternative methods not considered. We also sought comment on evidence-based approaches to enhancing choice architecture within the FFEs and SBE-FPs.
In response to this comment solicitation, in the 2023 Payment Notice (87 FR 27345 through 27347), we highlighted many commenters' specific recommendations regarding modifying choice architecture to enhance the consumer shopping experience. We also noted that several commenters supported limiting the number of QHPs that could be offered through the FFEs and SBE-FPs, explaining that adopting such an approach could lower costs for consumers, set standards for plan quality, and foster robust competition among issuers seeking entry into the FFEs and SBE-FPs. Conversely, we noted that several commenters opposed limiting the number of QHPs that could be offered through the FFEs and SBE-FPs, explaining that doing so would limit issuer flexibility to design plans based on consumer preferences and needs. We also noted that several commenters supported resuming an updated version of the meaningful difference standard, which was previously codified at § 156.298.
In the 2024 Payment Notice (88 FR 25855 through 25865), at § 156.202, we introduced limits on the number of non-standardized plan options that issuers of QHPs can offer through FFEs and SBE-FPs to four non-standardized plan options per product network type (as described in the definition of “product” at § 144.103), metal level (excluding catastrophic plans), and inclusion of dental and/or vision benefit coverage, in any service area for PY 2024, and two for PY 2025 and subsequent plan years.
In the 2024 Payment Notice (88 FR 25856 through 25857), we stated that we introduced non-standardized plan option limits for several reasons. We stated that there had been a sizeable increase in the weighted average number of total QHPs on the FFEs and SBE-FPs available per enrollee and plans offered per issuer in recent years. We stated that with this continued plan proliferation, we believed that limiting the number of non-standardized plan options that FFE and SBE-FP issuers of QHPs could offer through the FFEs and SBE-FPs would greatly enhance the consumer experience on
HealthCare.gov.
We further stated that we made several enhancements to the consumer experience and choice architecture on
HealthCare.gov
in conjunction with introducing non-standardized plan option limits.
We stated that we believed that adopting both of these measures (in conjunction with requiring issuers to offer standardized plan options) would be the most effective method to streamline the plan selection process and to reduce the risk of plan choice overload for consumers on
HealthCare.gov.
We also stated that we believed that directly limiting the number of non-standardized plan options that issuers could offer through the FFEs and SBE-FPs was a more effective approach in reducing the risk of choice overload than reinstituting a revised version of the meaningful difference standard, which had previously demonstrated limited efficacy.
In the 2025 Payment Notice (89 FR 26362 through 26375), we introduced an exceptions process allowing issuers to offer additional non-standardized plan options exceeding the limit of two per product network type, metal level, inclusion of adult dental benefit coverage, pediatric dental benefit coverage, and adult vision benefit coverage, and service area for PY 2025 and subsequent plan years, if issuers demonstrate that these additional non-standardized plans have specific design features that would substantially benefit consumers with chronic and high-cost conditions. As part of this exceptions process, each issuer must demonstrate how cost sharing pertaining to the treatment of the chronic and high-cost condition would be reduced by 25 percent or more relative to that issuer's other non-standardized plan option offerings in the same product network type, metal level, inclusion of adult dental benefit coverage, pediatric dental benefit coverage, and adult vision benefit coverage, and service area.
In the 2025 Payment Notice (89 FR 26366), we stated that we introduced this exceptions process for several reasons. Specifically, we noted that several commenters stated that reducing the non-standardized plan option limit from four in PY 2024 to two in PY 2025 would cause FFE and SBE-FP issuers to discontinue non-standardized plans with lower enrollment, which would likely be plans with designs that are attractive to a smaller number of enrollees who have relatively less common and high-cost health care needs. Commenters further stated that many of the plans that would likely be discontinued would be those that benefit consumers with chronic and high-cost conditions. Commenters stated that permitting issuers to offer additional non-standardized plan options that would provide targeted coverage specifically for medically complex populations with chronic and high-cost conditions would allow for more targeted innovation by issuers while still achieving the reduction in plan proliferation HHS has sought.
In the proposed rule, we stated (91 FR 6391) that under our proposed approach, issuers would no longer be subject to the non-standardized plan option limit of two per product network type, metal level, inclusion of adult dental benefit coverage, pediatric dental benefit coverage, and adult vision benefit coverage, in any service area at § 156.202(a) through (c), for PY 2027 and subsequent years. We also stated that issuers would similarly no longer be required to utilize the non-standardized plan option limit exceptions process at § 156.202(d) through (e) to offer additional non-standardized plan options given that they would no longer be limited in the number of non-standardized plan options they may offer. We stated that we would correspondingly remove § 156.202 from our regulations.
( printed page 29722)
Similar to our proposal to discontinue the requirement for issuers to offer standardized plan options (as well as the differential display of these plans) but not to require issuers to discontinue these existing offerings altogether, in the proposed rule, we proposed to discontinue the non-standardized plan option limits and exceptions process but not require issuers to discontinue these existing offerings altogether (91 FR 6391). We stated that, instead, under the proposal, issuers would be permitted to choose whether to discontinue the chronic and high-cost condition plans originally offered through the non-standardized plan option limit exceptions process altogether or continue offering them with either the same or modified cost sharing.
We stated (91 FR 6391) that under this proposed approach, if issuers wished to discontinue the chronic and high-cost condition plans originally offered through the non-standardized plan option limit exceptions process altogether, they would be permitted to do so, and enrollees in these plans would be crosswalked to a different plan in accordance with the crosswalk hierarchy at § 155.335(j). Additionally, we stated (91 FR 6391) that if issuers wished to continue offering the chronic and high-cost condition plans originally offered through the exceptions process with the same cost sharing structures, they would also be permitted to do so, and enrollees in these plans would continue to be auto-reenrolled in these plans from one plan year to the next. Finally, we stated that if issuers wished to continue offering the chronic and high-cost condition plans originally offered through the exceptions process but also wished to modify these plans' cost sharing structures, they would be permitted to do so, but these issuers would continue to be subject to the requirements under the definition of “plan” at § 144.103 and to the uniform modification requirements at § 147.106.
We also stated (91 FR 6391) that in most scenarios where an issuer modifies the cost sharing structure of one of its chronic and high-cost condition plans originally offered through the exceptions process, the newly modified plan that was formerly the exceptions process plan would be considered a new plan and would therefore require a new plan ID. In this scenario, enrollees would be crosswalked from the discontinued plan to another plan in accordance with the crosswalk hierarchy at § 155.335(j). We stated that these enrollees could be crosswalked into the newly modified plan that was formerly the exceptions process plan, or an entirely different plan altogether, depending on the unique circumstances in each county.
However, we noted (91 FR 6391) that under the definition of “plan” at § 144.103, a State may permit issuers to make greater changes to a plan's cost sharing while still permitting that plan to be considered the same plan—thus maintaining the same plan ID. Furthermore, we noted that under § 147.106(e)(3)(iv), as long as the variation in cost sharing is solely related to changes in cost and utilization of medical care, or to maintain the same metal tier level (and other applicable requirements under § 147.106(e) are met), the modifications could be considered uniform (thus, a viable exception to guaranteed renewability).
We stated (91 FR 6391) that in the scenario where an issuer modifies what was formerly an exceptions process plan's cost sharing structure while maintaining the same plan ID, enrollees in the plan would be auto-reenrolled from one plan year to the next. We stated that in either case, whether the modification of a former exceptions process plan's cost sharing results in that plan being considered the same or a different plan, enrollees would be crosswalked in accordance with the crosswalk hierarchy at § 155.335(j), including reenrollment, if applicable.
In the proposed rule, we proposed this approach for several reasons. As discussed earlier in this section and in the section of the proposed rule addressing proposed updates to § 156.201 (91 FR 6391), for the last several plan years, we have employed a multi-faceted strategy in an attempt to streamline the consumer experience. This strategy entailed requiring issuers to offer standardized plan options, requiring these plans to meaningfully differ from one another, differentially displaying these plans, making additional enhancements to choice architecture on
HealthCare.gov,
limiting the number of non-standardized plan options that issuers can offer through the FFEs and SBE-FPs, and permitting issuers to offer additional non-standardized plan options beyond this limit if issuers demonstrate that these plans would substantially benefit consumers with chronic and high-cost conditions.
As we noted (91 FR 6391) in the preamble section of the proposed rule addressing the proposed removal of § 156.201, we have accumulated 4 plan years of experience (PY 2023 through PY 2026) administering this strategy (91 FR 6385). We stated that this cumulative experience provides us with a comprehensive and nuanced perspective regarding weighing both the advantages and disadvantages of employing this strategy, whether this strategy has aligned with our originally articulated objectives, and whether this strategy has yielded the intended results.
Similar to our view on the ineffectiveness of employing standardized plan option requirements, we stated in the proposed rule (91 FR 6391) that based on this experience, we have concluded that imposing non-standardized plan option limits and permitting exceptions to this limit for chronic and high-cost condition plans is an ineffective strategy in counteracting plan proliferation and enhancing the consumer experience on
HealthCare.gov,
the originally articulated objectives of employing our non-standardized plan option limits and related exceptions process policies.
We stated (91 FR 6392) that this is because requiring issuers to offer additional plans in the form of standardized plan options increased the weighted average number of total plans available per enrollee from 108 in PY 2022, the year before the introduction of the requirement to offer standardized plan options, to 114 in PY 2023, the year in which this requirement was introduced, with most of this increase in plans being comprised of standardized plan options. Furthermore, we noted that plan proliferation as measured by the weighted average number of total plans offered per issuer (which is derived by dividing the weighted average number of total plans available per enrollee by the weighted average number of total issuers per enrollee) increased from 16.9 in PY 2022 to 17.3 in PY 2023—meaning each issuer on average tended to offer a higher number of plans after the imposition of the requirement to offer standardized plan options than the year before this requirement was made effective.[301]
Furthermore, we stated (91 FR 6392) that even with the introduction of the non-standardized plan option limit of four in PY 2024 and its reduction to two as well as the introduction of the exceptions process in PY 2025, the net impact of both the requirement to offer standardized plan options as well as the subsequent imposition of non-standardized plan option limits and exceptions on the weighted average number of total plans available per enrollee and the weighted average number of total plans offered per issuer (including both standardized and non-
( printed page 29723)
standardized plan options) was marginal—despite the substantially increased regulatory complexity and the associated burden of creating and submitting certification applications for new plans (standardized plan options) and correspondingly adjusting existing portfolios of plan offerings (non-standardized plan options).
Specifically, we noted (91 FR 6392) that the weighted average number of total plans available per enrollee was reduced from 114 in PY 2023 to 100 in PY 2024 (when the non-standardized plan option limit of four was introduced) and remained constant at 100 in PY 2025 (when the limit was reduced to two and the non-standardized plan option limit exceptions process was introduced). Relatedly, we noted that the weighted average number of total plans offered per issuer decreased from 17.3 in PY 2023 to 14.7 in PY 2024 and 13.7 in PY 2025. Thus, we noted that in PY 2022, the year before this suite of policies was introduced, there was a weighted average number of 108 total plans available per enrollee and a weighted average number of 16.9 total plans offered per issuer, whereas in PY 2025 (after several consecutive years of imposing new layers of requirement), these same measures were 100 and 13.7, respectively.
We stated (91 FR 6392) that we do not believe that the marginal net reductions in the weighted average number of total plans available per enrollee and the weighted average number of total plans offered per issuer achieved by introducing this suite of standardized plan option and non-standardized plan option limit and exceptions requirements warrant imposing additional burden, impeding issuer innovation in plan design, and constraining consumer choice—especially given that these reductions are largely indiscernible to consumers during the plan selection process. We stated that this is especially true given that these metrics continue to remain significantly elevated compared to only several plan years ago. Specifically, we noted that in PY 2020, the weighted average number of total plans available per enrollee was 39, and the weighted average number of total plans offered per issuer was 11.1.
Thus, we stated (91 FR 6392) that the primary metric by which we have evaluated plan proliferation (the weighted average number of total QHPs available per enrollee in the FFEs and SBE-FPs) has remained relatively constant despite the imposition of multiple layers of requirements from PY 2023 to PY 2025 (specifically, the requirement to offer standardized plan options in PY 2023, non-standardized plan option limits in PY 2024, and the reduction of this limit and the introduction of the exceptions process in PY 2025). Further, we stated that the imposition of these requirements substantially increased burden for both issuers and HHS (that is, the burden associated with issuers creating and submitting certification applications for additional plans that would otherwise not be created and offered, and HHS reviewing and certifying these additional plans). We stated that this suite of policies creates additional fixed costs for issuers, introducing market inefficiencies. Finally, we stated that the imposition of these requirements caused a significant degree of market disruption—as reflected by the substantial number of plan discontinuations and the high number of enrollees impacted by these discontinuations, as is discussed in greater detail later in this section.
We referred readers (91 FR 6392) to the section III.E.8. of the proposed rule addressing the proposal to discontinue standardized plan options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv)) for a detailed discussion of relevant literature we also considered in our approach to the proposal to discontinue non-standardized plan option limits and exceptions.
Relatedly, we stated (91 FR 6392) that the strategy of requiring issuers to offer standardized plan options, differentially displaying these plans on
HealthCare.gov
and the DE pathways, and limiting the number of non-standardized plan options that issuers can offer was intended to enhance plan comparability for consumers navigating the plan selection process. We further stated that, theoretically, requiring issuers to offer plans with standardized cost sharing parameters would facilitate the plan selection process by reducing the number of factors that consumers must consider when evaluating all available plan options—since a certain subset of plans would have the same cost sharing parameters. We stated that as a result of having access to plans with standardized cost sharing parameters, consumers would theoretically have the ability to shift their focus to other important plan attributes, such as premiums, benefit coverage, provider networks, formularies, and quality ratings, during the plan selection process.
However, we stated (91 FR 6392) that in practice, given that standardized plan options continue to be offered alongside non-standardized plan options, whether a particular plan option was a standardized or non-standardized plan option served as yet another variable that consumers must consider during the plan selection process. Furthermore, we stated that in our experience, we have found when consumers are faced with a large number of heterogeneous plan options, they continue to rely primarily on premiums, networks, and issuer brand—meaning that standardizing cost sharing parameters alone (especially when doing so only for a subset of all available plan options) fails to meaningfully reduce decision complexity for consumers.
In addition, we stated (91 FR 6392) that we believe the fact that the consistently high proportion of total FFE and SBE-FP enrollment in as well as active selections (which includes both consumers currently enrolled in a QHP who are making a new plan selection as well as consumers who are enrolling in any QHP offered through the FFEs and SBE-FPs for the first time, but excludes consumers who are auto-reenrolled in their current QHP from one year to the next) of non-standardized plan options reflects the fact that consumers value the full range of choice within these plan offerings.
Specifically, we noted (91 FR 6393) that 80 percent of all consumers in the FFEs and SBE-FPs were enrolled in non-standardized plan options in PY 2023, 67 percent in PY 2024, and 67 percent in PY 2025. Furthermore, we noted that non-standardized plan options constituted 82 percent of FFE and SBE-FP active selections in PY 2023, 74 percent in PY 2024, and 82 percent in PY 2025.[302]
Relatedly, we noted that 75 percent of total plan offerings were non-standardized plan options in PY 2023, 72 percent in PY 2024, and 69 percent in PY 2025.[303]
Thus, we stated (91 FR 6393) that total enrollment in non-standardized plan options was higher compared to what would be expected based on the total proportion of plans that were non-standardized plan options in PY 2023 and within the expected range of deviation for PY 2024 and PY 2025. Furthermore, we stated that active plan selections for non-standardized plan options were higher compared to what would be expected based on the total proportion of plans that were non-standardized plan options in PY 2023, PY 2024, and PY 2025.
( printed page 29724)
We stated (91 FR 6393) that the consistently low proportion of consumers enrolled in standardized plan options over the years suggests that these plans fail to appeal to consumers compared to corresponding non-standardized plan options—or at the very least that consumers are unable to perceive a significant difference between standardized and non-standardized plan options. We further stated that this is despite the full suite of differential display features for standardized plan options on
HealthCare.gov
and the DE pathways that visually distinguish standardized plan options from non-standardized plan options and effectively steer consumers into standardized plan options and away from corresponding non-standardized plan options in accordance with §§ 155.205(b)(1), 155.220(c)(3)(i)(H), and 156.265(b)(3)(iv).
We stated (91 FR 6393) that without this full suite of differential display features that visually distinguishes standardized plan options from non-standardized plan options, the proportion of FFE and SBE-FP total enrollment in and active selections of non-standardized plan options would likely be considerably higher. This is because those visual markers have the effect of steering consumers to standardized plan options. We stated that we believe consumers' demonstrated preference for non-standardized plan options (as measured by both total enrollment and active plan selections) is in large part due to the fact that there is a greater degree of choice and variety in these plan offerings compared to standardized plan options.
Indeed, as we noted in the proposed rule (91 FR 6393), in the 2024 Payment Notice (88 FR 25860), many commenters who opposed imposing non-standardized plan option limits emphasized the importance of permitting issuers to maintain a diverse range of plan offerings as a mechanism to maximize the degree of consumer choice. These commenters specifically stated that imposing non-standardized plan option limits would force issuers to drastically reduce the unique plan designs they have thoughtfully developed to best serve their members' health care needs, which would in turn force consumers into a “one-size fits all” benefit offering.
Relatedly, we stated (91 FR 6393) that the combination of standardized plan option requirements as well as non-standardized plan option limits has increasingly constrained issuers' ability to offer a sufficiently broad range of plans for several plan years. We stated that this includes plans with tiered provider networks, plans with separate medical and drug deductibles (as opposed to integrated medical and drug deductibles), plans with separate medical and drug MOOPs (as opposed to integrated medical and drug MOOPs), HSA-eligible high-deductible health plans (HDHPs), and plans with more than four tiers of prescription drug coverage.
We stated (91 FR 6393) that issuers have been constrained by these requirements since they have been forced to discontinue offerings to comply with the non-standardized plan option limit. We noted that the plans that issuers have discontinued have generally been those with lower enrollment—which has often been plans with the aforementioned design features. Thus, we stated that removing this suite of requirements would grant issuers additional flexibility to once more vary plans along these parameters, which would enhance consumer choice. We further stated that removing this suite of requirements would also simultaneously reduce the issuer burden associated with creating and submitting additional QHP certification applications as well as HHS burden in reviewing and approving these applications.
Regarding market disruption that arose from issuers discontinuing plans to conform to the non-standardized plan option limit, we acknowledged (91 FR 6393) that there is a baseline rate of routine plan discontinuations on the FFEs and SBE-FPs that occur for a range of reasons unrelated to the imposition of new requirements. We noted, for example, that in the FFEs and SBE-FPs from PY 2020 to PY 2021, 17 percent of plan-county combinations were discontinued, affecting 10 percent of enrollees.[304]
Additionally, we noted in the FFEs and SBE-FPs from PY 2021 to PY 2022, 22 percent of plan-county combinations were discontinued, affecting 13 percent of enrollees. Thus, we stated that based on measures from the 2 plan years immediately preceding the introduction of the standardized plan option requirements in PY 2023, the baseline rate of routine plan-county discontinuations in the FFEs and SBE-FPs ranged from 17 to 22 percent, while the corresponding baseline rate of enrollees impacted by these discontinuations ranged from 10 to 13 percent.
However, we noted (91 FR 6393) that from PY 2022 to PY 2023, when the requirement for FFE and SBE-FP QHP issuers to offer standardized plan options was introduced, 35 percent of plan-county combinations in the FFEs and SBE-FPs were discontinued, affecting 19 percent of enrollees. In addition, we noted that from PY 2023 to PY 2024, when the non-standardized plan option limit of four was introduced, 24 percent of plan-county combinations in the FFEs and SBE-FPs were discontinued, affecting 17 percent of enrollees. Finally, we noted from PY 2024 to PY 2025, when the non-standardized plan option limit was reduced from four to two, 24 percent of plan-county combinations in the FFEs and SBE-FPs were discontinued, affecting 15 percent of enrollees on the FFEs and SBE-FPs.
Thus, we stated (91 FR 6393) that employing these standardized plan option, non-standardized plan option limit, and non-standardized plan option limit exceptions process policies coincided with an increase in plan-county discontinuations of 18 percent and an increase in enrollees affected by these discontinuations of 9 percent compared to the years immediately preceding the introduction of these requirements (specifically between PY 2020 and 2021 and when the requirement to offer standardized plan options was introduced from PY 2022 to PY 2023). We stated that, ultimately, requiring issuers to discontinue other existing plans (to comply with the new non-standardized plan option limits) increased plan-county discontinuations and the number of enrollees affected by these discontinuations.
We acknowledged (91 FR 6394) that some portion of these plan discontinuations and the subsequent number of enrollees affected by these discontinuations is attributable to the narrowing of the AV
de minimis
ranges per §§ 156.140, 156.200, and 156.400 in PY 2023 (such as the narrowing the AV
de minimis
range for on-Exchange silver offerings from 66 percent through 72 percent to 70 percent through 72 percent—which required issuers to either discontinue or modify offerings within the 66 percent through 70 percent range to have an AV within the 70 through 72 percent range). However, we noted that the rates of plan-county discontinuations and the subsequent number of enrollees impacted by these discontinuations continued to remain elevated in PY 2024 and PY 2025 (as the non-standardized plan option limit was
( printed page 29725)
introduced and subsequently reduced) compared to baseline rates of plan-county discontinuations and the number of enrollees affected by these discontinuations in PY 2020 through PY 2022—implying that a substantial portion of these discontinuations was also attributable to the imposition of the requirement to offer standardized plan options as well as the introduction of the non-standardized plan option limit.
We stated (91 FR 6394) that, given this accumulation of data, we no longer believe that the advantages of imposing non-standardized plan option limits and exceptions (namely, a marginal net reduction in plan proliferation) outweigh the disadvantages of imposing these requirements (namely, increased burden, increased regulatory complexity, market disruption, inhibition of issuer innovation in plan design, and constrained consumer choice).
Altogether, we proposed (91 FR 6394) to discontinue non-standardized plan option limits under § 156.202(a) through (c) and the corresponding exceptions process under § 156.202(d) through (e), since we have concluded that adopting these measures (in conjunction with requiring issuers to offer standardized plan options) is an ineffective method of achieving our originally articulated objectives of employing this suite of policies to streamline the plan selection process, counteract plan proliferation, and reduce the risk of plan choice overload for consumers on
HealthCare.gov.
Furthermore, we stated that discontinuing these policies would decrease regulatory complexity, issuer burden, and the market disruption caused by plan discontinuations arising from the non-standardized plan option limit. Finally, we stated that discontinuing these policies would enhance consumer choice by supporting issuers' ability to innovate in plan designs.
We sought comment (91 FR 6394) on this proposal. After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposal to discontinue non-standardized plan option limits and exceptions below.
Comment:
Many commenters supported the proposal to discontinue non-standardized plan option limits. These commenters stated that discontinuing these limits would provide issuers with greater flexibility to design plans that better reflect evolving market conditions and consumer preferences. Several commenters further stated that discontinuing the limits would enable a wider range of plan offerings. These commenters specifically cited plans with tiered provider networks, HSA-eligible HDHPs, plans with separate medical and drug MOOPs and deductibles (compared to integrated medical and drug MOOPs and deductibles), plans with more than four formulary tiers, plans that reduce cost sharing for virtual visits, and ICHRAs as examples of plans that would no longer be constrained if the limit were to be discontinued. Several commenters also stated that issuers would also be able to more easily offer a broader range of plans that target chronic and high-cost conditions without being subject to the burden of submitting the justification documentation that is currently required under the non-standardized plan option limit exceptions process.
Commenters that supported discontinuing non-standardized plan option limits also stated that this policy failed to effectively achieve its intended goals—streamlining the plan selection process, counteracting plan proliferation, and reducing the risk of plan choice overload for consumers—while simultaneously increasing regulatory complexity, issuer burden, and market disruption. These commenters pointed to the marginal net reductions in the weighted average total number of plans available per enrollee and issuer from PY 2022 to PY 2025 as well as the substantially increased number of plan discontinuations that coincided with the introduction of the non-standardized plan option limit of four in PY 2024 and the reduction of this limit to two in PY 2025.
Response:
For the reasons we detail in the proposed rule (91 FR 6391 through 6394) and stated earlier in this section of this final rule, we agree with commenters who stated that discontinuing non-standardized plan option limits and exceptions will provide issuers with greater flexibility to design plans that reflect evolving market conditions and consumer preferences. We also agree that discontinuing these limits will allow issuers to offer a broader range of plan designs, including plans with tiered provider networks, HSA-eligible HDHPs, plans with separate medical and drug MOOPs and deductibles (compared to integrated medical and drug MOOPs and deductibles), plans with more than four formulary tiers, plans that reduce cost sharing for virtual visits, ICHRAs, and plans that target chronic and high-cost conditions.
We also agree with commenters that stated that this policy failed to effectively achieve its intended goals—streamlining the plan selection process, counteracting plan proliferation, and reducing the risk of plan choice overload for consumers—while simultaneously increasing regulatory complexity, issuer burden, and market disruption. We further agree with these commenters that this failure is evinced by the marginal net reductions in the weighted average total number of plans available per enrollee and issuer from PY 2022 to PY 2025 as well as the substantially increased number of plan discontinuations that coincided with the introduction of the non-standardized plan option limit of four in PY 2024 and the reduction of this limit to two in PY 2025.
Comment:
Several commenters opposed the proposal to discontinue non-standardized plan option limits. These commenters stated that these limits prevent excessive plan proliferation and reduce the risk of consumer choice overload while encouraging issuers to offer plans that are meaningfully distinct from one another. Several commenters stated concern that removing these limits could significantly increase the number of plans offered through the FFEs and SBE-FPs, making it more difficult for consumers to meaningfully evaluate all available plan options and select a plan that best meets their unique health care needs.
Commenters also cited research demonstrating that FFE and SBE-FP enrollees experience difficulty comparing plans, including challenges understanding differences in provider networks, benefit coverage, cost sharing, and premiums.[305]
These commenters noted that increasing the total number of plans available to consumers could exacerbate these challenges and lead to poorer decision-making and increase the risk of suboptimal plan selection and unexpected financial costs. Several commenters also raised concerns about broader market impacts, stating that discontinuing these limits would increase opportunities for adverse selection (namely, by allowing issuers to design plans in such a manner to encourage the enrollment of healthier and lower risk consumers and discourage the enrollment of less
( printed page 29726)
healthy and higher risk individuals), potentially destabilizing risk pools and increasing premium volatility.
Other commenters warned that discontinuing these limits would enable issuers to offer duplicative plans to increase visibility in FFE and SBE-FP displays and dominate search results—a noncompetitive strategy which could distort plan selection dynamics and lead to fluctuations in market share. In addition, several commenters noted that non-standardized plan option limits and exceptions have only recently been implemented and that HHS has had insufficient time to fully evaluate their effects. These commenters urged continued monitoring before making significant policy changes.
Response:
We acknowledge commenters' belief that non-standardized plan option limits may play a role in preventing excessive plan proliferation and reduce the risk of consumer choice overload. We also acknowledge the research that commenters cited regarding consumer difficulty comparing plans and the potential for poorer decision-making outcomes in the presence of an overwhelming number of plan options. Still, in our experience operating the FFEs and SBE-FPs, placing limits on non-standardized plan options has failed to achieve the originally intended results of implementing these policies.
In particular, instead of streamlining the plan selection process, counteracting plan proliferation, and reducing the risk of plan choice overload for consumers (as was originally intended), we received feedback, and observed, that these non-standardized plan option limits increased regulatory complexity, issuer burden, and market disruption; inhibited issuer innovation in plan design; constrained the degree of consumer choice; only had a marginal net impact on plan proliferation; and in conjunction with the standardized plan option policies, complicated the plan selection process by introducing another variable that consumers must consider in the plan selection process.
For the reasons explained in the proposed rule (91 FR 6391 through 6394) and stated earlier in this final rule, while we acknowledge these concerns, we believe that consumers benefit from having access to a wider range of plan designs that better reflect diverse needs and preferences, that any theoretical advantages of employing these non-standardized plan options limits are outweighed by the significant disadvantages (such as inhibited issuer innovation in plan design and constrained consumer choice), and that these concerns would be best addressed by discontinuing non-standardized plan option limits.
We further do not believe that non-standardized plan option limits are the sole nor the most effective, least burdensome, or least disruptive mechanism to address these concerns. Instead, as was discussed in greater detail in section III.E.8. of this final rule, we believe that making enhancements to choice architecture, plan display, and consumer decision-support tools on
HealthCare.gov
and the DE platforms are better suited to helping consumers navigate a broad and diverse range of plan options and make informed decisions—while avoiding unnecessarily inhibiting issuer innovation and constraining consumer choice. This is because under this approach, consumers would have an enhanced degree of choice in terms of diverse plan offerings (with issuers no longer being constrained by these standardized plan option and non-standardized plan option limit and exception policies), and the search results of all available plan offerings on
HealthCare.gov
and DE platforms could then be tailored to unique consumer preferences and health care needs.
We also disagree with commenters who stated that discontinuing non-standardized plan option limits could increase the risk of adverse selection and contribute to premium volatility. We note that the non-standardized plan option limit of four was introduced in PY 2024 (with the limit being reduced to two the following year in PY 2025). Given that no such limits were in place prior to PY 2024 (and during that time, there was no evidence to suggest increased risks of adverse selection or premium volatility even when there were no limits in place), discontinuing these limits in PY 2027 would represent a return to the status quo in PY 2023 in terms of risk pool stability and premium volatility. We further note that other program features, including risk adjustment requirements (such as those under 45 CFR part 153) and rating rules (such as those at 45 CFR 147.102), are designed to mitigate adverse selection and promote market stability. Thus, we do not believe that maintaining these limits is necessary or even conducive to achieve these objectives.
We acknowledge commenters' concerns that discontinuing these limits could potentially enable issuers to offer duplicative plans to increase visibility in FFE and SBE-FP displays and dominate search results. However, we note that we do not anticipate such an occurrence at a sufficient scale to warrant the continuation of this policy. In large part, this is because there were only a handful of instances of such duplicate plans out of hundreds of total plan offerings in the FFEs and SBE-FPs in PY 2026 that issuers needed to modify to conform with the meaningful difference standard for standardized plan options at § 156.201(c).
Instead, we anticipate a return to the weighted average total number of plans available per enrollee and issuer to approximate what these metrics were before these limits were introduced in PY 2024 (since these limits only yielded marginal reductions in the first place). We also note that we will continue to monitor FFE and SBE-FP plan offerings and display practices during the annual QHP certification process and through other existing avenues through which consumers regularly submit complaints (such as the Health Insurance Casework System).
We further note that making additional enhancements to plan display and sorting methodologies on
HealthCare.gov
and the DE platforms would help alleviate these concerns without necessarily imposing restrictive limits on plan offerings. This is because consumers will have an enhanced degree of choice in terms of diverse plan offerings (with issuers no longer being constrained by these standardized plan option and non-standardized plan option limit and exception policies), and the search results of all available plan offerings on
HealthCare.gov
and DE platforms could then be tailored to unique consumer preferences and health care needs. We note that we continue to research such enhancements and encourage issuers and other DE partners to do the same.
We also considered comments stating that non-standardized plan option limits have only recently been implemented and that additional time may be needed to more comprehensively evaluate their effects. While we acknowledge that these policies were introduced several years ago, we believe that the considerations discussed above support discontinuing these limits at this time to reduce regulatory burden and increase flexibility. Our four years of cumulative experience administering these standardized plan option and non-standardized plan option limit and exception policies has provided us with a comprehensive and nuanced perspective regarding weighing both the advantages and disadvantages employing this strategy. After careful consideration, we have concluded that this strategy had failed to yield the originally intended results, as discussed throughout this section. We further believe that these concerns are better
( printed page 29727)
addressed by enhancing choice architecture and plan display on
HealthCare.gov
and DE platforms—as discussed throughout this section.
Comment:
Several commenters opposed discontinuing the non-standardized plan option limit exceptions process. These commenters stated concern that eliminating the exceptions process would reduce the availability of plans designed to meet the needs of individuals with chronic or high-cost conditions. In particular, commenters noted that plans previously approved through the exceptions process include targeted benefit designs that reduce cost sharing for condition-specific services or prescription drugs. These commenters stated that allowing issuers to discontinue these plans or modify them without being subject to the constraints of the exceptions process (such as demonstrating a substantial reduction in out-of-pocket costs for the treatment of a particular chronic and high-cost condition) could limit access to affordable and comprehensive coverage options for individuals with specific health care needs, including those managing chronic conditions such as diabetes.
Response:
We do not agree with concerns that eliminating the non-standardized plan option limit exceptions process could reduce the availability of plans designed to meet the needs of individuals with chronic or high-cost conditions. To the contrary, discontinuing non-standardized plan option limits will increase the ability of issuers to offer plans designed to meet the needs of individuals with chronic or high-cost conditions as well as other potential innovative plan designs. As such, we do not agree that maintaining a formal exceptions framework is necessary or helpful to support the continued availability of such plans.
Under our approach, issuers will have increased flexibility to design and offer a broader and more diverse array of plan options, including those with targeted benefit structures for individuals with chronic and high-cost conditions, without the need to obtain formal approval through the currently required exceptions process. We thus believe that discontinuing the exceptions process removes administrative barriers and will allow issuers to continue offering such plan designs with decreased burden. Further, nothing in this approach requires issuers to discontinue plans that are currently offered through the non-standardized plan option limit exceptions process.
10. Deferral of Network Adequacy Reviews to States With an Effective Provider Access Review Program (§§ 156.230 and 155.1050)
In the 2027 Payment Notice proposed rule (91 FR 6394), we proposed to exercise our authority under sections 1311(c)(1)(B) and 1321(a)(1)(B) of the Affordable Care Act to defer reviews of network adequacy to FFE States, including States performing plan management, provided the State elects to conduct such reviews, and demonstrates sufficient authority and the technical capacity to conduct network adequacy reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d)(2) through (d)(4). We proposed to revise § 156.230 to clarify that HHS would continue to conduct network adequacy reviews using standards described at § 156.230(a)(2) through (a)(4) for QHP issuers that use a provider network in FFE States that do not elect to conduct their own provider access reviews, or that HHS has determined do not satisfy applicable criteria to be considered to have an Effective Provider Access Review Program, as described at proposed § 155.1050(d).
Section 1311(c)(1)(B) of the Affordable Care Act requires the Secretary to establish minimum criteria for provider network adequacy that a health plan must meet to be certified as a QHP. Section 1321(a)(1)(B) of the Affordable Care Act directs the Secretary to issue regulations that set standards for meeting the requirements of title I of the Affordable Care Act, which includes section 1311, for, among other matters, the offering of QHPs through such Exchanges.
In the Exchange Establishment Rule (77 FR 18418), we set forth minimum network adequacy standards that plans must satisfy to be certified as QHPs at § 156.230. The Exchange Establishment Rule (77 FR 18409 through 18420) provided that an issuer of a QHP that uses a provider network must maintain a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible to enrollees without unreasonable delay. In the 2016 Payment Notice (80 FR 10830 through 10833), we revised § 156.230(a) to clarify that network adequacy requirements only apply to QHPs that use a provider network, defining such networks as networks comprised only of providers that are contracted as in-network. For PYs 2015 through 2017, the FFEs conducted network adequacy reviews of proposed QHPs for compliance with network adequacy time and distance standards.
The 2017 Market Stabilization final rule (82 FR 18346) initially deferred reviews of network adequacy for QHPs to States that HHS determined to have a sufficient network adequacy review process, an approach that was reiterated in the 2019 Payment Notice (83 FR 16930). Specifically, we deferred these reviews to States that possessed sufficient authority to enforce network adequacy standards that were at least equal to the reasonable access standard defined in § 156.230 and that had the means to assess the adequacy of plans' provider networks. In States without the authority or means to conduct network adequacy reviews, we relied on an issuer's accreditation (commercial, Medicaid, or Exchange) from an HHS-recognized accrediting entity—specifically, either The National Committee for Quality Assurance (NCQA), URAC, or Accreditation Association for Ambulatory Health Care (AAAHC). Any unaccredited issuers were required to submit an access plan to demonstrate that the proposed QHP's provider network met the requirement in § 156.230(a)(2) to demonstrate that an issuer had standards and procedures in place to maintain an adequate provider network consistent with the National Association of Insurance Commissioners' (NAIC's) Health Benefit Plan Network Access and Adequacy Model Act. To provide additional support to States, we further coordinated with States to monitor network adequacy through consumer complaint tracking and resolution.
On March 4, 2021, the United States District Court for the District of Maryland issued its decision in City of Columbus v. Cochran, which addressed a challenge to the policy of outsourcing network adequacy reviews.[306]
The court specifically vacated the portion of the 2019 Payment Notice's deferral of network adequacy reviews of QHPs offered through the FFEs to States with the authority and means to conduct sufficient network adequacy reviews, first finalized in rulemaking in the Market Stabilization final rule (83 FR 17024 through 17026). While the decision held that our policy of deferring network adequacy reviews to the States was not contrary to law, the court vacated the policy as an arbitrary and capricious agency action, holding that HHS did not meaningfully respond
( printed page 29728)
to comments and evidence in the record.
Comments and evidence in question centered around assessment of States' ability to meaningfully conduct network adequacy reviews, and the use of accreditation as a basis for determining QHP issuers' satisfaction of provider network adequacy standards. Commenters stated that States' and accrediting entities' review processes do not do enough to ensure enrollees have adequate access to necessary care. In particular, the decision raised concerns about HHS' position that States' network adequacy review procedures are adequate simply because States have State-specific regulations without explaining what these entail or why they are comparable to review under Federal standards. The court also raised concerns about comments stating that State review procedures are often not adequate, have no quantitative standards for network adequacy in place, and, in many States, are complaint driven rather than preemptive, as well as comments that in some States, requirements only apply to certain types of plan designs. Comments expressing concern about relying on accreditation as a determination of network adequacy standard satisfaction stated that accreditation standards are not public, accreditors do not have regulatory authority over plans, and accreditors are not in a position to monitor network adequacy via consumer complaints or other means.
In the 2023 Payment Notice (87 FR 27322), we finalized that we would evaluate the adequacy of QHP provider networks offered through the FFEs, or of plans seeking certification as FFE QHPs, except for FFEs in States performing plan management that elect to conduct network adequacy reviews, so long as the State applies and enforces quantitative network adequacy standards that are at least as stringent as the Federal network adequacy standards established for QHPs under § 156.230 (that is, Michigan, New Hampshire, South Dakota, and West Virginia) beginning with the 2023 QHP certification cycle. Additionally, in the 2023 Payment Notice (87 FR 27322), we adopted time and distance standards at § 156.230(a)(2) to assess whether plans seeking to be certified as QHPs in all FFE States meet network adequacy time and distance requirements.
In the 2024 Payment Notice (88 FR 25740), we revised network adequacy standards at § 156.230(a)(2) to establish appointment wait time standards starting in PY 2025. We also required all individual market QHPs, including individual market SADPs, and all SHOP QHPs, including SHOP SADPs, across all Exchanges to use a network of providers that complies with the network adequacy standards, and removed the exception that these requirements do not apply to plans that do not use a provider network. A limited exception was finalized at § 156.230(a)(4) for certain SADP issuers that sell plans in areas where it is prohibitively difficult for the issuer to establish a network of dental providers.
In the 2025 Payment Notice (89 FR 26218), we finalized § 155.1050(a)(2)(i)(A) to require that State Exchanges and SBE-FPs establish and impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs under § 156.230. We also finalized § 155.1050(a)(2)(i)(B) which required that, for plan years beginning on or after January 1, 2026, State Exchanges and SBE-FPs conduct quantitative network adequacy reviews to evaluate a plan's compliance with network adequacy standards under § 156.230(a)(1)(ii), (a)(1)(iii), and (a)(2)(i)(A) prior to certifying any plan as a QHP, while providing QHP certification applicants the flexibilities described under § 156.230(a)(2)(ii) and (a)(3) and (4).
To implement the requirements for FFEs that were in place from PY 2023 and subsequent years outlined above, we published in the 2023 Final Letter to Issuers in the Federally-facilitated Exchanges [307]
a list of provider types and facility types, developed consistent with industry standards, alongside the time and distance standard for each provider or facility specialty type for each county type designation which are based on population size and density parameters (Large Metro, Metro, Micro, Rural, and Counties with Extreme Access Considerations). All FFE QHP issuers were required to submit a Network Adequacy (NA) template during the QHP certification period which is populated with their in-network provider and facility information (for example, NPI, specialty type, address(s) of their practice(s)). We used that information to conduct geocoding analyses for compliance with network adequacy standards.[308]
This is an iterative process during QHP certification, with issuers informed of their review results and encouraged to contract with more providers to meet the standards if appropriate. Though there was no requirement for issuers to contract with a third-party vendor to assist with populating network adequacy templates, we are aware of some issuers that opt to outsource this work to vendors that have access to their claims data to assist in populating the template with providers with which the issuer is actively contracted.
Additionally, beginning January 1, 2025, QHP issuers in the FFEs were required to meet appointment wait time standards established in the 2023 Letter to Issuers.[309]
The 2025 Final Letter to Issuers on the Federally-facilitated Exchanges established the requirement for QHP issuers to contract with a third-party entity to administer secret shopper surveys on a sample of in-network providers to determine their level of compliance with appointment wait time standards for two provider types; [310]
specifically, the requirement that enrollees would be able to schedule an appointment at least 90 percent of the time within 15 business days for routine primary care, within 10 business days for behavioral health providers, and within 30 business days for routine specialty providers. We use the final Network Adequacy templates submitted by FFE issuers during QHP certification to generate the Provider Population Files for QHP issuers and their third-party entity to develop the Appointment Wait Time Secret Shopper Survey Samples as outlined in the Appointment Wait Time Secret Shopper Survey Technical Guidance.
In the proposed rule, we stated that the preceding years of conducting reviews of QHP issuer provider network adequacy, including analyzing issuer submitted data and through discussions with States, issuers, and other various interested parties around diverse market conditions, have demonstrated that a one-size-fits all approach to provider network adequacy review is not satisfactory. We noted, for example, that issuers have highlighted to us persistent challenges in locating and contracting with enough providers of various specialties (for example, allergy and immunology, behavioral health, gastroenterology) in remote or difficult
( printed page 29729)
to access areas of a State. We further noted that States have brought to our attention various geographic constraints that impact QHP issuers' ability to satisfy time and distance requirements and have made suggestions to assess a QHP issuer's ability to meet a time or a distance standard individually, rather than requiring it to meet a standard that assesses time and distance together, which may be insurmountable due to a topographical constraint such as a body of water or navigating roads in mountainous terrain.[311]
In addition, we stated that partnerships with States performing plan management, who have elected to conduct their own network adequacy reviews, have also highlighted for us how States may innovate in their approach to conducting network adequacy reviews that are sensitive to conditions and capacity in the State. For example, we stated that we are aware of States performing plan management that assess network adequacy based on access to services rather than provider types. We stated that deferring network adequacy reviews to FFE States that demonstrate sufficient authority and the technical capacity by satisfying the criteria to demonstrate they have an Effective Provider Access Review Program would empower these States to similarly innovate and mold their network adequacy standards to the needs of consumers in their individual States. We noted, for example, that a State may find it is in the interest of their consumers to assess network adequacy using a time or a distance standard individually rather than assessing whether a QHP issuer meets a time and distance standard, make adjustments to time and distance standards that account for more remote areas or more urban areas, assess network adequacy in different ways such as through provider-enrollee ratios, expand or change the provider types they assess, and implement other innovative, State-specific approaches to identify and address the systemic issues that result in many issuers being unable to meet the network adequacy standards described at § 156.230(a)(2). We stated that a State, with its more intimate knowledge of its own demographics, topography, quantity, and density of providers, is often best positioned to evaluate local provider networks and market conditions and tailor network adequacy standards in a more nuanced way than Federal requirements.
Thus, in recognition of the crucial role States have in developing and enforcing network adequacy standards and because we believe that States are often best positioned to evaluate local provider networks and market conditions, we proposed at § 155.1050(d), for PY 2027 and subsequent years, to allow FFE States, including States that perform plan management, to conduct reviews for provider access for issuers' plans that use and do not use a provider network, provided that we determine the State has sufficient authority and the technical capacity to conduct the reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program as described at proposed § 155.1050(d)(2) through (d)(4) and the State elects to conduct these reviews. Concurrently, we proposed, for plan years beginning on or after January 1, 2027, to amend § 156.230, including by (1) revising the section heading to state, “Provider access standards for network plans”; (2) revising § 156.230(a)(1) to remove the requirement that a QHP must use a provider network and clarify that the standards described in § 156.230(a)(1)(i), (ii), and (iii) apply to a QHP that uses a network of providers; (3) revising § 156.230(a)(2)(i) and (ii) to clarify that requirements for issuers of QHPs to meet time and distance standards and appointment wait time standards at § 156.230(a)(2) only apply in States that do not elect to conduct their own provider access reviews or States that we have determined do not do not satisfy the criteria to be considered to have an Effective Provider Access Review Program as described at proposed § 155.1050(d); (4) revising the exception at § 156.230(a)(3) to clarify that it applies only when HHS is conducting network adequacy reviews; and (5) revising § 156.230(a)(4) to conform with proposed revisions to § 156.230(a)(1).
Additionally, in recognition of the traditional role that all State Exchanges and SBE-FPs have in developing and enforcing network adequacy standards and to align with proposed changes for FFE States detailed in section III.D.18 of the proposed rule, we proposed to remove the requirements under § 155.1050(a)(2)(i) and (ii) for State Exchanges and SBE-FPs to establish and impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs under § 156.230 and to no longer require State Exchanges and SBE-FPs to conduct quantitative network adequacy reviews to evaluate a plan's compliance with network adequacy standards under § 156.230(a)(1)(ii), (a)(1)(iii), and (a)(2)(i)(A) prior to certifying any plan as a QHP. Instead, we proposed to restore § 155.1050(a)(2) to a pre-PY 2025 policy and require that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets standards specified in § 156.230(a)(1)(ii) and (iii) for network plans, or proposed § 156.236(a) for non-network plans, as applicable. This proposal is discussed in more detail in section III.D.18 of the proposed rule and this final rule.
In addition, as we stated in section III.E.12. of the proposed rule, we also now believe that there are alternative administrable regulatory standards that can ensure satisfaction of provider sufficiency requirements by QHPs that do not use traditional contracted networks of providers and that, especially in light of efforts to improve health care price transparency, an expanded definition of how to achieve sufficient access to providers would allow for innovations in plan design. Our proposal to allow for QHP certification of plans without a provider network is described in detail in section III.E.12. of the proposed rule.
Our proposed revisions to §§ 156.230(a)(2)(i) and (ii) and (a)(3) reflect our proposed change in policy at § 155.1050(d) to defer network adequacy reviews to FFE States that elect to perform such reviews, and that demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4), while also retaining Federal standards for HHS to utilize in conducting network adequacy reviews, including time and distance and appointment wait time standards, in States that do not elect to conduct such reviews or do not demonstrate they have sufficient authority and the technical capacity to conduct these reviews.
As we stated in the proposed rule, network adequacy analyses are often highly data-intensive. We stated that because the FFE has economies of scale
( printed page 29730)
in the collection and analysis of various forms of network adequacy data, including time and distance data and appointment wait time data, under our proposal, we would continue collecting this data from all FFE issuers, either to use to conduct Federal network adequacy reviews in FFE States that do not elect to do so or do not demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4), or with a view to make it available in a standardized format to States that are determined to have an Effective Provider Access Review Program, to assist them in their network adequacy analysis. We stated that we have extensive tools to standardize data, including a network adequacy template, other supporting document templates, manual data validation resources, and FAQs. We stated that the continuation of the aforementioned activities would support consumer protection as HHS would maintain an ability to utilize the collected data to research and address consumer or other complaints, provide continuity for States that may need time to expand their technical capacity and seek to rely on our infrastructure, and prevent any gaps in awareness as FFE States expand and fortify their own reviews. We further stated that this aspect of our proposal primarily seeks to support States that do not presently have sufficient authority or the technical capacity to conduct reviews and States that demonstrate sufficient authority and the technical capacity but seek to capitalize on HHS' data collection and analysis to supplement their provider access review programs. We stated that we believe this approach appropriately balances State and Federal responsibilities as it seeks to empower States that elect to conduct network adequacy reviews but also utilizes Federal systems to provide support to States, maximizing consumer protection and taking advantage of State expertise in developing and enforcing provider network adequacy requirements.
We stated that we would consider a State to have sufficient authority and the technical capacity to conduct network adequacy reviews if the State meets criteria set forth at proposed § 155.1050(d)(2) through (4) (discussed at section III.D.18. of the proposed rule). The proposal also clarified that if States are not determined to have an Effective Provider Access Review Program, then HHS would continue to perform provider access certification reviews consistent with § 156.230(a)(1) through (a)(4) for network plans and proposed § 156.236 for non-network plans.
We stated that, as proposed at § 155.1050(d)(2), an FFE State with an Effective Provider Access Review Program would be required to ensure that a QHP issuer that uses a network of providers ensures that its network of providers, as available to all enrollees, includes ECPs in accordance with § 156.235, and maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay, and is consistent with the rules for network plans of section 2702(c) of the PHS Act. We proposed at § 155.1050(d)(3) that an FFE State with an Effective Provider Access Review Program must ensure that a QHP issuer that does not use a network of providers (a non-network plan) provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay.
We further stated (91 FR 6397) that under our proposal at § 155.1050(d)(4), a State operating an FFE that elects to conduct its own provider access reviews would be considered to have an Effective Provider Access Review Program by satisfying the following requirements:
(1) The FFE State has established provider access standards that are set forth in State statute or regulation which are consistent with provider access standards as set forth in § 156.230(a)(1)(ii) and (iii), and reports to HHS whether the State has delegated authority to some entity other than the State Department of Insurance to perform any or all provider access review activities;
(2) The FFE State's provider access review process includes reporting systems for State-required provider access metrics and documentation of methodology and the State provides descriptions of all data collection systems, resources, templates, and methodologies used by the State or the State's delegated entity to collect and review provider access data; and the State receives from issuers data and documentation in connection with provider access standards that are sufficient to conduct the examination;
(3) The FFE State's provider access review process includes procedures to ensure full and ongoing compliance with State provider access standards and enforcement frameworks applicable to issuers that fail to meet provider access standards so that those issuers come into compliance with State provider access standards, including standardized processes to assess efforts the issuer is pursuing to come into compliance with State provider access standards, and implementing any justification and exception processes for issuers that have not yet or cannot meet provider access requirements;
(4) The FFE State establishes and maintains clear procedures and timeline requirements for regular provider access reviews, including processes that ensure reviews occur prior to each plan year's QHP certification cycle;
(5) The FFE State has a process for monitoring and addressing consumer-related provider access complaints to ensure sufficient access to providers consistent with section 1311(c)(1)(B) of the Affordable Care Act and as set forth in State statute; and
(6) The FFE State has a process to collect and review information sufficient to show that non-network plans provide access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full.
We proposed at § 155.1050(d)(5) that we would determine whether a State has an Effective Provider Access Review Program based on information available to us that demonstrates whether the program meets the criteria described at proposed § 155.1050(d)(4). We proposed at § 155.1050(d)(6) that we may also grant an exception to these criteria if we determined that making such an exception is in the interests of qualified individuals in the State or States in which such Exchange operates. We also proposed at § 155.1050(d)(7) that we would notify the FFE State electing to conduct provider access certification reviews of our decision in writing regarding whether the State is determined to have an Effective Provider Access Review Program and can therefore conduct its own provider access certification reviews. We proposed that we would also reserve the right at any time to evaluate whether, and to what extent, a State's circumstances have changed such that it has established, or no longer has, an Effective Provider Access Review Program under § 155.1050(d). We proposed that these evaluations may result in HHS assuming provider access review responsibilities or transitioning such responsibilities back to the State.
( printed page 29731)
We also proposed that a State would need to demonstrate that it meets applicable criteria for both network plans and non-network plans under § 155.1050(d), if it decides to certify such plans, to receive the designation to have an Effective Provider Access Review Program. We stated that this would mean that a State would not be permitted to elect to conduct provider access certification reviews for only network plans and not non-network plans, if it certifies such plans, or vice versa. We stated that we believe this is important, as some QHP issuers may choose to offer both network and non-network plans, and centralizing reviews to a single entity, whether the FFE State or HHS, for the same issuer would reduce administrative inefficiencies that may result if the FFE State and HHS have to coordinate provider access certification review results across a range of network and non-network plans. We stated that we also believe that review authority being limited to a single entity, either the FFE State or HHS, would allow both network and non-network plans to undergo consistent, standardized reviews conducted by the same reviewing entity. We further stated that we believe this would ensure similar requirements and methodologies would be applied fairly across network and non-network plans and reduce potential differences in provider access review results. We stated that, overall, just as with network plans, non-network plans would be required to ensure sufficient access to a range of providers in a manner consistent with section 1311(c)(1)(B) of the Affordable Care Act.
We stated in the proposed rule that rather than specifying the detailed methodology and standards States would be expected to use to determine sufficient access to providers, the proposed factors focus on processes to ensure a State has sufficient authority and the technical capacity to conduct network adequacy reviews. We further stated that the approach, as set forth at proposed § 155.1050(d), would provide for more than a perfunctory review of authority, but rather would thoroughly investigate States' ability to ensure provider access sufficiency in line with § 156.230(a)(1)(ii) and (iii). We stated that this proposed approach would allow States more flexibility in defining network adequacy standards that reflect their local markets, provider availability, geographic considerations, and demographics. We further stated that we would evaluate if the network adequacy review program in the State has established network adequacy standards that are set forth in State statute and regulation that are consistent with those set forth in § 156.230(a)(1)(ii) and (iii).
The first proposed criterion for evaluation requires that the State has established provider access standards that are set forth in State statute or regulation, which are consistent with provider access standards as set forth in § 156.230(a)(1)(ii) and (iii), and reports to HHS whether the State has delegated authority to some entity other than the State Department of Insurance to perform any or all provider access review activities. We stated that this criterion would be crucial as it addresses whether or not the State has sufficient authority to conduct provider access reviews. We noted that it would also be important for a State to report to us whether the State has delegated authority to some other entity to perform provider access review activities so we understand how the State is handling provider access review data and to whom it entrusts such data.
The second proposed criterion states that the State's provider access review process includes reporting systems for State required provider access metrics and documentation of methodology and the State provides descriptions of all data collection systems, resources, templates, and methodologies used by the State, or the State's delegated entity, to collect and review provider access data; and the State receives from issuers data and documentation in connection with provider access standards that are sufficient to conduct the examination. We stated that this information would be important for us to understand processes a State has in place to appropriately assess provider access. We stated that under our proposal, we would evaluate whether the State's provider access data, documentation, and analysis practices are sufficient to ensure it can conduct provider access reviews.
The third proposed criterion provides that the State's provider access review process includes procedures to ensure full and ongoing compliance with State provider access standards and enforcement frameworks applicable to issuers that fail to meet provider access standards so that those issuers come into compliance with State provider access standards, including standardized processes to assess efforts the issuer is pursuing to come into compliance with State provider access standards, and implementing any justification and exception processes for issuers that have not yet or cannot meet provider access requirements. We stated that this information would be important for reasons similar to the previously discussed proposed factor. We also noted that ensuring that adequate compliance processes exist would bolster the robustness of any network adequacy review to ensure sufficient provider access.
The fourth proposed criterion requires that the State establish and maintain clear procedures and timeline requirements for regular provider access reviews, including processes that ensure reviews occur prior to each plan year's QHP certification cycle. We stated that we believe that it would be important for States to have clearly established procedures for network adequacy review that are not reactive but are preemptive to ensure that plans being offered on an Exchange provide sufficient access to providers and so that consumers shopping for a plan have that guarantee.
The fifth proposed criterion requires the State to have a process for monitoring and addressing consumer-related provider access complaints to ensure sufficient access to providers consistent with section 1311(c)(1)(B) of the Affordable Care Act and as set forth in State statute. We stated that this criterion would be important because provider access can change often during the year. We stated that for plans using a provider network, contracts may be executed or terminated throughout a plan year for various reasons. We stated that any inaccuracies or out-of-date information contained in provider directories can create confusion or be misleading to consumers. Additionally, we noted that consumers may have trouble actually making appointments with network providers due to lack of availability of appointments. We further stated that for plans without a provider network, we anticipate that providers that accept a benefit amount as payment in full may also change frequently depending on market conditions, negotiations, and competition.
The sixth proposed criterion requires the State to have a process to collect and review information capable of demonstrating whether non-network plans provide access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full. We stated that this criterion would be important to ensure that, should a State offer non-network plans, these plans also ensure sufficient access to providers.
We stated that while these proposed criteria for assessing whether a State has an Effective Provider Access Review Program are comprehensive, we believe this approach would provide ample flexibility to States to determine the best
( printed page 29732)
methodology to assess network adequacy within the State. We anticipated each State's approach would be dependent on available resources (for example, technical infrastructure, budget, staffing), topographical considerations, and population needs unique to each State, and we proposed to empower States to utilize these factors to evaluate overall State processes that ensure sufficient consumer protection. We further stated that our proposal also does not dictate the precise network adequacy review methodology which may reasonably differ from State to State.
We stated that under our proposed approach, we would seek to work in partnership with States and would provide numerous resources to States to utilize as they see fit to further develop and enhance their network adequacy review capabilities. We stated that, for example, we would offer extensive resources originally developed for Federal network adequacy review during the annual QHP certification cycle as States may work to further develop network adequacy standards and review methods that best suit the conditions of their distinct consumer populations and needs. We stated that these tools, including a network adequacy template, other supporting document templates, manual data validation resources, and FAQs, could provide support to interested States as States continue to develop and implement processes to standardize any issuer-submitted data during their reviews, leveraging HHS' extensive experience in identifying efficient data formats and validation processes. We noted that this comprehensive support system would be available to States as States continue to develop and implement individualized network adequacy standards and review processes that are most appropriate and protective for their own consumers.
In summary, we proposed, for plan years beginning on or after January 1, 2027, to amend § 156.230, including (1) revising the section heading to state, “Provider access standards for network plans”; (2) revising § 156.230(a)(1) to remove the requirement that a QHP must use a provider network and clarify that the standards described in § 156.230(a)(1)(i), (ii), and (iii) apply to a QHP that uses a network of providers; (3) revising § 156.230(a)(2)(i) and (ii) to clarify that requirements to meet time and distance standards and appointment wait time standards at § 156.230(a)(2) only apply to States that we have determined do not satisfy the criteria to be considered to have an Effective Provider Access Review Program or that do not elect to conduct their own provider access reviews of issuers as described at proposed new § 155.1050(d); (4) revising exceptions to the aforementioned requirements at § 156.230(a)(3) to apply only when HHS is conducting network adequacy reviews; and (5) revising § 156.230(a)(4) to conform to revisions to § 156.230(a)(1). We stated that through these proposed changes, we would defer provider access reviews, for network and non-network plans, to FFE States, including States performing plan management, provided the State elects to conduct such reviews, and demonstrates it has sufficient authority and the technical capacity to conduct network adequacy reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program, as detailed at proposed § 155.1050(d)(2) through (4).
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy with minor modifications. We are modifying § 155.1050(a)(1) to differentiate between FFE States with an Effective Provider Access Review program and FFE States without an Effective Provider Access Review Program. We are revising § 155.1050(d)(1) to add a phrase clarifying that if States do not elect to conduct provider access reviews, CMS will continue to conduct reviews of QHP issuer provider access consistent with requirements under § 156.230 for network plans and, for plan years beginning on or after January 1, 2028, under § 156.236 for non-network plans and to acknowledge the delay in implementation of the policy, as finalized in this rule, allowing certification of non-network plans as QHPs beginning on or after January 1, 2028. Additionally, we are modifying § 155.1050(d)(4)(iv) to clarify that, to have an Effective Provider Access Review Program, the FFE State must establish and maintain clear procedures and timeline requirements for regular provider access reviews, including processes that ensure reviews occur prior to “completion of” each plan year's QHP certification cycle. We are also modifying § 155.1050(d)(4)(vi) to require that the State have a process to collect and review information described under § 156.236(b)(4) through (b)(9) from non-network plans. We are modifying § 155.1050(d)(5) to clarify that CMS will determine whether a State has an Effective Provider Access Review Program based on information that demonstrates whether the program meets criteria described under § 155.1050 (d)(2) through (d)(4).
We summarize and respond below to public comments received on this proposal.
Comment:
Several commenters stated support for the proposal and importance of recognizing FFE State flexibility, noting that States possess deep expertise in their local health care markets and are well-positioned to conduct meaningful network adequacy reviews. They stated that States understand local market dynamics, provider supply, and the specific needs of their populations in ways that Federal reviewers may not. Commenters noted that allowing FFE States to tailor their review processes to local conditions enables more responsive and effective oversight. Commenters noted that many States already have robust network adequacy requirements in place that are comparable to, and in some cases more stringent than, Federal requirements. They noted that these existing frameworks demonstrate that States are capable of conducting rigorous reviews without duplicative Federal oversight. Commenters stated the proposed approach appropriately balances State flexibility with consumer protections through clearly defined criteria FFE States must meet to conduct provider access reviews. Commenters also stated support for maintaining Federal network adequacy reviews as a backstop, ensuring that a Federal safety net remains in place for States that may lack the capacity or infrastructure to conduct robust reviews independently. A few commenters, while supportive of the policy, stated operational concerns and requested that we delay implementation of this policy to allow issuers that operate in multiple FFE States to adapt to potential variability in provider access reviews across FFE States.
Response:
We appreciate the support stated by commenters for the proposed approach and will be finalizing the policy as proposed, without delayed implementation, but with minor modifications for clarity which we described above. In particular, we agree that States are uniquely positioned to understand the health care markets within their jurisdictions and that leveraging State expertise can lead to more effective and efficient network adequacy oversight. We also agree that many States have developed sophisticated network adequacy frameworks that reflect a deep understanding of local provider landscapes and consumer needs and we seek to facilitate and support any FFE
( printed page 29733)
States that choose to elect to conduct provider access reviews.
We recognize that duplicative Federal and State review processes can create administrative burden for issuers without commensurate benefit to consumers. By allowing States that meet clearly defined criteria to conduct network adequacy reviews, we aim to reduce this duplication while preserving consumer protections. We believe this approach appropriately balances the goals of State flexibility and Federal oversight.
We also affirm our commitment to maintaining Federal network adequacy reviews as the default and to continued provider data collection, including collection of time and distance and appointment wait time (AWT) data for all FFE States, including States that elect to conduct provider access reviews and are determined to have an Effective Provider Access Review Program. This provider data will be available to States determined to have an Effective Provider Access Review Program, in a standardized format, to assist them in their network adequacy analysis. States that do not meet criteria described at § 155.1050(d)(2) through (d)(4), or that choose not to conduct their own reviews, will continue to be subject to Federal oversight. This ensures that consumers in all States benefit from a baseline level of protection, regardless of the State's capacity, authority, or approach to network adequacy oversight.
With regard to the request to delay implementation due to operational concerns, while we acknowledge the risk that some issuers operating in multiple FFE States may experience an increased administrative burden and are mindful of the potential operational implications for them, we will not be delaying implementation of this proposal. We reiterate that that the default status will be for the continuation of Federal network adequacy reviews and we anticipate most issuers will not experience much change operationally as it relates to network adequacy reviews in PY 2027 compared to PY 2026. In the event an FFE State elects to conduct provider access certification reviews and subsequently meets the criteria to be considered to have an Effective Provider Access Review Program for PY 2027, we will promptly communicate with issuers in that FFE State to inform them that the State is determined to have an Effective Provider Access Review Program for PY 2027. We also encourage issuers to communicate concerns with any States in which they operate and request guidance regarding expectations should the State elect to conduct provider access reviews for PY 2027.
Comment:
Many commenters stated general opposition to allowing FFE States to elect to conduct provider access reviews if they are able to demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the criteria to be considered to have an Effective Provider Access Review Program. The most common concern raised by commenters included that allowing FFE States with Effective Provider Access Review Programs to have more flexibility in developing provider access standards, which may be different than the Federal time and distance standards, may result in implementation of provider access reviews with “relaxed” time and distance standards or removal of time and distance standards altogether. Commenters were concerned that this may result in negative impacts in rural areas, such as longer wait times, reduced access to specialty care, including mental health and substance use disorder services, or the removal of certain specialties from their standards entirely; and generally narrower networks compared to those in FFE States where we will continue to conduct provider access reviews. Many commenters stated concern over a lack of an explicit requirement for FFEs to implement quantitative time and distance and appointment wait time standards, and recommended that CMS continue to require the Federal time and distance standards under § 156.230(a)(2(i)(A) and (B) apply as a requirement for an FFE State to be determined to have an Effective Provider Access Review Program. One commenter specifically requested quantitative requirements for access to mental health and substance use disorder services. Commenters stated that prior changes to Federal network adequacy standards have made meaningful progress in reducing network adequacy-related lawsuits and consumer complaints, and stated concern that the proposed changes would reverse this trend.
Response:
We acknowledge the concerns stated by commenters related to how FFE States may choose to implement provider access reviews in instances where they elect to conduct such reviews and are determined to have sufficient authority and the technical capacity to conduct the reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program. We acknowledge commenters' concerns about rural access, specialty care, and the potential for narrower networks, though we believe that many of these concerns are tied to larger systemic issues such as a lack of practicing providers in a particular geographic area and issuer/provider contracting complexities that will not be ameliorated or otherwise impacted significantly by any standardized set of time and distance standards. We want to highlight that under § 155.1050(d)(2), to demonstrate they have an Effective Provider Access Review Program, the FFE State must ensure that a QHP issuer that uses a network of providers ensures that the in-network providers, as available to all enrollees, include essential community providers (ECPs) in accordance with § 156.235, and maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay. So, while an FFE State with an Effective Provider Access Review Program could choose to implement standards that differ from the Federal review standards and hypothetically opt to remove a specialty type (for example, pulmonology) from the provider specialty list their FFE State reviews for time and distance, that in no way prevents QHP issuers from continuing to contract with that provider type in an effort to better serve their enrollees. One of the intentions of this policy is to recognize that FFE States are aware of the complexities and challenges present in their local markets and have their consumers' best interests in mind as they develop and enforce network adequacy standards. Additionally, State regulators are, in many respects, better positioned to address these concerns, and through providing them more flexibility to implement standards and reviews that may or may not differ from Federal reviews, they can tailor provider access reviews to the specific needs of their markets and populations.
We recognize that these concerns, including concerns regarding a lack of baseline quantitative standards and concerns that proposed changes would reverse trends in the reduction of network adequacy-related lawsuits and consumer complaints, reflect a broad apprehension about the absence of baseline quantitative requirements, including time and distance standards, that would apply uniformly to FFE States electing to conduct their own reviews. We acknowledge that quantitative standards can serve an important function in supporting
( printed page 29734)
network adequacy reviews that are measurable, enforceable, and meaningful for consumers. For the reasons stated earlier in this final rule, however, we believe that the qualification criteria established in this proposal under § 155.1050(d)(2) through (d)(4) provide a meaningful framework for ensuring that States conducting their own reviews maintain a level of rigor consistent with the Federal goals of ensuring sufficient access to providers, including providers that specialize in mental health and substance use disorder services. We discuss the importance of these criteria earlier in this final rule in detail. Furthermore, the Federal review for network adequacy is still the default for States that do not elect to conduct provider access reviews, and those that do not meet the criteria to be considered to have an Effective Provider Access Review Program.
We are also committed to working in partnership with FFE States that elect to conduct provider access reviews and are determined to have an Effective Provider Access Review Program by providing technical assistance and support, including through continued network adequacy data collection and through maintaining the requirement that all QHP issuers in all FFE States conduct AWT Secret Shopper Surveys. This empowers us to provide additional resources to FFE States as well as to retain the ability to continue to compare and monitor QHP issuer performance.
Additionally, there is also nothing barring FFE States from adopting Federal time and distance and appointment wait time standards, in whole or part, if the State determines this is in the best interest of consumers in their State. We have seen this approach in practice as some States that have transitioned from FFEs to State Exchanges have outright adopted or mirrored our current quantitative time and distance standards. For example, as of PY2027 Georgia continues to implement the network adequacy standards, including time and distance standards and appointment wait time standards, established by CMS.[312]
Because the provider data analysis we will offer FFE States uses Federal time and distance standards, FFE States with an Effective Provider Access Review Program may be more likely to adopt Federal network adequacy standards, in whole or part.
Comment:
Several commenters specifically stated concern that the proposed policy to allow FFE States to conduct provider access reviews, should they elect to conduct these reviews and be determined to have an Effective Provider Access Review Program, will result in geographic inequities, stating that a consumer's ability to access an adequate network of providers should not depend on where they live. These commenters noted a belief that broad discretion for States to develop network adequacy standards could produce standards that vary widely from State to State, and the potential for a lack of consumer transparency could make it difficult to assess whether the standards being applied are truly effective at measuring network adequacy.
One commenter specifically noted that requiring uniform standards would better support consumers in understanding their plans and assessing whether those plans are in compliance with network adequacy requirements, particularly for appointment wait times.
In this context, many commenters, including those that acknowledged support for State flexibility, called on CMS to maintain clear baseline Federal standards to address common challenges across jurisdictions, and to preserve confidence in the QHP certification process.
Response:
We acknowledge commenters' call for consistent, transparent, and comparable standards across States and acknowledge concerns about the potential for variability in provider access reviews across FFE States, including the stated preference for uniform quantitative standards that are applicable to all FFE States, even those that conduct provider access reviews. While FFE States which elect to conduct provider access reviews and are determined to have Effective Provider Access Review Programs will have flexibility around the specific provider access standards and reviews they implement, we are confident, for the reasons stated earlier in this final rule, that the criteria the FFE State must meet to be determined to have the authority and the technical capacity to conduct provider access reviews, as described at § 155.1050(d)(4), will ensure a high bar to conduct provider access reviews and a baseline level of consistency across FFE States. In particular, under § 155.1050(d)(4)(i), the FFE State must establish provider access standards that are set forth in State statute or regulation, meaning they are publicly available, and are consistent with the Federal provider access standards described at § 156.230(a)(1)(ii) and (iii). Additional, non-exhaustive examples of criteria that will ensure a level of consistency and consumer confidence in provider access across FFE States include requirements that the FFE State share its provider access review process with us, including reporting systems, access metrics, and methodology; that the review processes include procedures around ongoing compliance and enforcement of provider access standards; that clear review timelines be established with reviews completed prior to QHP certification; and that processes be in place for monitoring and addressing consumer complaints.
However, uniform policy requiring identical time and distance standards across all FFEs that elect to conduct provider access reviews and are determined to have an Effective Provider Access Review Program would not appropriately capture the realities of local provider availability, provider willingness to contract with issuers, and various geography. The needs of consumers in Alaska, for example, are fundamentally different from those of consumers in Florida, due to differences in geography, population size and distribution, and age of the States' populations.
We reiterate that we do not believe a one-size-fits all approach is satisfactory, as evidenced through our experience in conducting network adequacy reviews, and through discussions with States, issuers, and other various interested parties around diverse market conditions. As we noted in the proposed rule (91 FR 6458), for example, issuers have highlighted to us persistent challenges in locating and contracting with enough providers of various specialties (for example, allergy and immunology, behavioral health, gastroenterology) in remote or difficult to access areas of a State. We further noted that States have brought to our attention various geographic constraints that impact QHP issuers' ability to satisfy time and distance requirements and have made suggestions to assess a QHP issuer's ability to meet a time or a distance standard individually, rather than requiring it to meet a standard that assesses time and distance together, which may be insurmountable due to a topographical constraint such as a body of water or navigating roads in mountainous terrain. In these instances, variability in reviews has the potential to work to the benefit of the consumers, and the closer proximity of State regulators will work to support robust reviews in their own States as State regulators have intimate knowledge of
( printed page 29735)
their local markets, provider availability, geographic considerations, and demographics.
We reiterate that we believe the criteria established under § 155.1050(d)(2) through (d)(4) for an FFE State to demonstrate it has an Effective Provider Access Review Program serves as robust means to ensure States have sufficient authority and the technical capacity to conduct provider access reviews. We discuss the importance of these criteria earlier in this final rule in detail. Additionally, our continued network adequacy data collection from issuers in these States will allow us to continue to monitor QHP issuer performance and provide support to States. The State could then use this network adequacy data to supplement their reviews, according to needs of their State's consumers. There is also nothing barring FFE States from adopting Federal time and distance and appointment wait time standards under § 156.230, in whole or part, if the State determines this is in the best interest of their consumers.
Comment:
Many commenters noted that patients, specifically those seeking mental health and substance use disorder services, in areas with fewer in-network providers already face disproportionately higher out-of-pocket costs and stated concern that any loosening of standards would reduce access to affordable coverage, destabilize safety net providers, and expose consumers to even greater financial burden. These concerns were closely linked to broader worries about the proliferation of narrow networks, with commenters citing existing deficiencies in Exchange plans where consumers have had difficulty accessing needed mental health providers due to those providers being out-of-network or lacking available appointments.
Response:
We acknowledge the meaningful concerns about narrow networks and the negative impacts on consumers, including those seeking mental health services and substance use disorder services, which are specialties with known, frequent provider supply shortages and exclusion from issuer networks. Additionally, we recognize that many of the access concerns stated by commenters are tied to multiple systemic factors including provider availability and the complex relationship between issuers and providers. We want to reiterate that Federal provider access reviews will remain the default approach and FFE States will not automatically be allowed to conduct provider access reviews. Rather, we intend to ensure that if an FFE State elects to conduct provider access reviews, they have sufficient authority, technical capacity, and standards in place that ensure compliance with the requirements outlined under § 155.1050(d)(2) through (d)(4), which includes the requirement that FFE States that conduct their own provider access reviews establish provider access standards that are consistent with those for FFE States where we continue to conduct provider access reviews.
Comment:
Several commenters raised procedural and legal objections to the proposal. Commenters also raised concerns rooted in prior litigation, noting a court case in which a court stated concern about CMS' failure to provide a substantive response to allegations that States were not adequately conducting network adequacy reviews, and stating that little has changed, with more recent analyses continuing to find many States lacking in enforcement actions related to network adequacy. Commenters pointed out that the court had raised concerns about the adequacy of State review procedures and the absence of quantitative standards for network adequacy, deficiencies that commenters stated are not remedied by this proposal, which similarly does not impose quantitative requirements on States. Commenters also stated doubt about our assertion that issuers have identified challenges in contracting with sufficient numbers of providers and stated that in such a case, alternative methods to address provider shortages or provider reluctance to contract should be considered before reducing Federal oversight.
One commenter further stated that monitoring network adequacy is part of the Secretary's statutory duty and that Congress had an explicit intent to require uniform standards applicable to all Exchanges throughout the country.
Response:
We appreciate the legal and procedural concerns raised by commenters and take them seriously. As to the commenter's assertion that monitoring network adequacy is part of the Secretary's statutory duty and that Congress intended that uniform standards apply to all Exchanges throughout the country, we believe the approach finalized in this rule is consistent with the statutory framework detailed in section 1311(c)(1)(B) of the Affordable Care Act for the reasons stated earlier in this final rule. We also note that the language in the statute does not specify that the Secretary must define network adequacy standards in detail or create uniform standards that apply across all States. We also note that this policy maintains CMS as the default reviewer of network adequacy and will not result in a blanket deferral of network adequacy reviews to FFE States. The policy does not require FFE States to elect to conduct such reviews if they are satisfied with HHS continuing to conduct Federal provider access certification reviews of QHP issuers in their State consistent with requirements under § 156.230 for network plans and, for plan years beginning on or after January 1, 2028, under § 156.236 for non-network plans.
The policy we are finalizing in this rule is very different than the previous policy which deferred network adequacy reviews to FFE States. It establishes a structured, criteria-based pathway through which FFE States may elect to conduct provider access reviews while retaining CMS as the default review entity. and this policy also preserves meaningful Federal oversight, as we will continue to require QHP issuers in all FFE States to continue to submit network adequacy data prior to QHP certification and to conduct AWT Secret Shopper Surveys, regardless of whether we or the FFE State is conducting provider access reviews. This policy recognizes the unique capability of States to address the specific needs of their own consumers in a way that can be much more nimble, targeted, and flexible than is possible at a Federal level. We reiterate that a State, with its more intimate knowledge of its own demographics, topography, quantity, and density of providers, is often best positioned to evaluate local provider networks and market conditions and tailor network adequacy standards in a more nuanced way than Federal requirements. We discuss this in greater detail earlier in this final rule.
The network adequacy policy vacated in the
City of Columbus
case in 2021 allowed for the blanket deferral of network adequacy reviews to States. By contrast, under the policy we are finalizing in this rule, we will remain the default reviewing entity and FFE States will be the reviewing entity only if the FFE State elects to do so and only if the FFE State demonstrates it has sufficient authority and the technical capacity through meeting specific criteria described under § 155.1050(d)(2) through (d)(4). For the reasons stated earlier in this section of this final rule, we are confident that the criteria the FFE State must meet to be determined to have the authority and the technical capacity to conduct provider access reviews set a high bar for FFE States to demonstrate they are adequately prepared to conduct these reviews, otherwise we will continue to conduct reviews of QHP issuer provider
( printed page 29736)
access consistent with requirements under § 156.230 for network plans and, for plan years beginning on or after January 1, 2028, under § 156.236 for non-network plans. Specifically, under § 155.1050(d)(2), the FFE State must ensure a QHP issuer that uses a network ensures that the in-network providers, as available to all enrollees, include essential community providers (ECPs) in accordance with § 156.235, and maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay. The QHP issuer's provider network consisting of in-network providers, as available to all enrollees, must be consistent with the rules for network plans of section 2702(c) of the PHS Act. Under § 155.1050(d)(3), the FFE State must ensure that a QHP issuer that does not use a network of providers (a non-network plan) provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay.
Additionally, we are confident, for the reasons stated earlier in this final rule, that the criteria the FFE State must meet to be determined to have sufficient authority and the technical capacity to conduct provider access reviews, as described at § 155.1050(d)(4), will ensure a high bar to conduct provider access reviews and a baseline level of consistency across FFE States. In particular, under § 155.1050(d)(4)(i), the FFE State must establish provider access standards that are set forth in State statute or regulation, meaning they are publicly available, and are consistent with the Federal provider access standards described at § 156.230(a)(1)(ii) and (iii). Additional, non-exhaustive examples of criteria that will ensure a level of consistency and consumer confidence in QHP certification across FFE States, that were not present in the previously vacated policy, include requirements that the FFE State share its provider access review process with us, including reporting systems, access metrics, and methodology; that the review processes include procedures around ongoing compliance and enforcement of provider access standards; that clear review timelines be established with reviews completed prior to QHP certification; and that processes be in place for monitoring and addressing consumer complaints.
This policy seeks to empower FFE States that elect to conduct these reviews and are able to demonstrate sufficient authority and the technical capacity to do so with a level of flexibility intended to allow them to implement review programs that best fit their consumer needs, market conditions, and resource availability. This may include implementing reviews that are different from our quantitative time and distance review and reviews that are potentially more qualitative in nature, however, for the reasons stated earlier in this final rule, we believe we have developed a robust, comprehensive set of criteria that must be met and thus are confident FFE States that elect and that are determined to have Effective Provider Access Review Programs will conduct provider access reviews that are of a high quality and protect consumers.
Additionally, another difference in this policy is that we will continue to collect provider data from all QHP issuers in all FFE States, regardless of who is conducting the review, to maintain a level of awareness of QHP issuer provider networks and an ability to be responsive to consumer and interested parties complaints. All QHP issuers in all FFE States will also continue to conduct Appointment Wait Time Secret Shopper Surveys during the plan year using the provider data submitted to us during QHP certification. For the reasons stated earlier in this section of this final rule, we are confident that this policy will ensure a baseline level of consumer protection and access to care while empowering FFE States to innovate and invest in improving access for consumers through addressing concerns more locally and through the ability to make adjustments in standards and compliance requirements in a nimbler and more informed way than we are able.
Comment:
A number of commenters raised concerns about the capacity and consistency of State oversight under the proposed approach. Commenters questioned whether States have the resources, infrastructure, and capacity to conduct rigorous network adequacy reviews, and noted that the administrative burden of conducting such reviews would be shifted onto States that may not be equally vigilant in ensuring compliance. These concerns were reinforced by commenters who cited reports documenting wide variation in State network adequacy review practices, noting that many States rarely take enforcement actions and rely primarily on consumer complaints as their primary source of oversight data. Commenters stated concern that this historical variability and inconsistency in State oversight would be perpetuated, and potentially amplified under the proposed approach, resulting in reduced accountability and inconsistent protections for consumers across States. A few commenters urged CMS to delay the policy, citing the large number of policies proposed across the rule and the need for additional time to adapt to State network adequacy standards and to develop detailed compliance mechanisms.
Response:
We appreciate the concerns raised by commenters regarding the capacity and consistency of State oversight under the proposed approach and take these concerns seriously. We reiterate that the policy we are finalizing in this rule maintains CMS as the default reviewing entity unless an FFE State elects to and demonstrates sufficient authority and the technical capacity to conduct these reviews through meeting specific criteria described under § 155.1050(d)(2) through (d)(4). This policy is not a blanket deferral to all FFE States and does not require them to conduct these reviews if they do not wish to absorb the administrative burden and are satisfied with CMS conducting reviews of QHP issuer provider access or if the FFE State elects to but is unable to meet the criteria to demonstrate they have the authority and the technical capacity to conduct these reviews. In such cases, we will continue to conduct reviews consistent with requirements under § 156.230 for network plans and, for plan years beginning on or after January 1, 2028, under § 156.236 for non-network plans. This policy establishes a structured, criteria-based pathway through which only those FFE States that elect to conduct provider access reviews and can demonstrate sufficient authority and the technical capacity to conduct such reviews by satisfying criteria to be considered to have an Effective Provider Access Review program will be permitted to do so. The qualification criteria, discussed in detail in earlier in this final rule, are specifically designed to address the concerns commenters raised by ensuring that FFE States that take on this responsibility have demonstrated, to our satisfaction, that they wish to absorb the administrative burden of review and are equipped to conduct provider access reviews.
We acknowledge the commenter concerns regarding the wide variation in network review practices across States, the assertion that States rarely take
( printed page 29737)
enforcement action, and the reliance on consumer complaints to drive enforcement action. However, we are confident the requirements an FFE State must meet to demonstrate sufficient authority and the technical capacity to have an Effective Provider Access Review Program adequately address these concerns. While this policy is intended to allow flexibility in how FFE States conduct provider access reviews, the requirements described under § 155.1050(d)(2) through (d)(4) are designed to ensure that we will not approve an FFE State to conduct reviews unless they demonstrate sufficient authority and the technical capacity to do so. Specifically, § 155.1050(d)(iii) requires that the State's provider access review process includes procedures to ensure full and ongoing compliance with State provider access standards and enforcement frameworks applicable to issuers that fail to meet provider access standards so that those issuers come into compliance with State provider access standards. Additionally, § 155.1050(d)(4)(v) requires that the State have a process for monitoring and addressing consumer-related provider access complaints.
Regarding a call to delay implementation of this policy, we will be finalizing the policy as proposed for PY 2027. We acknowledge the operational concerns issuers may have in the event an FFE State they operate in elects to and is determined to meet the criteria to have an Effective Provider Access Review Program, but we believe that some FFE States may already be prepared to conduct these reviews. For example, some FFE States performing plan management have already elected to conduct network adequacy reviews in prior plan years. These States have already demonstrated sufficient authority and technical capacity in prior plan years to conduct provider access reviews, and may therefore already be positioned to meet the criteria to have an Effective Provider Access Review Program in PY 2027 and subsequent years. In our partnerships with these States, they have also highlighted how States may innovate in their approach to conducting network adequacy reviews that are sensitive to conditions and capacity in the State. We also want to reiterate that there is no requirement for FFE States to take on provider access reviews for PY 2027. If FFE States wish to elect to conduct provider access reviews, we encourage—and would require—them to take the time necessary to ensure they have established an Effective Provider Access Review Program that meets HHS standards. We will also notify issuers in FFE States if their State elects to conduct provider access reviews and is determined to have an Effective Provider Access Review Program. We encourage issuers and other interested parties to communicate and work directly with their State, if they have concerns surrounding when an FFE State may elect to conduct provider access reviews and any processes and expectations surrounding the way FFE States will conduct these reviews. We are also committed to providing necessary guidance and technical assistance to support States and issuers as they navigate this process. We will continue collecting network adequacy data, including time and distance and appointment wait time data from all FFE issuers, including FFE States determined to have an Effective Provider Access Review Program, with a view to make it available in a standardized format to assist them in their network adequacy analysis. We also offer extensive resources originally developed for Federal network adequacy review during the annual QHP certification cycle as States may work to further develop network adequacy standards and review methods that best suit the conditions of their distinct consumer populations and needs. These tools, including a network adequacy template, other supporting document templates, manual data validation resources, and FAQs, provide support to interested States as States continue to develop and implement processes to standardize any issuer-submitted data during their reviews, leveraging our extensive experience in identifying efficient data formats and validation processes.
Comment:
We received one comment recommending, we also remove the requirement that FFE States that conduct plan management ensure that QHP issuers follow quantitative time and distance network adequacy standards that are at least as stringent as standards for QHPs on the FFEs.
Response:
We acknowledge the commenter's request to adjust network adequacy requirements for FFE States performing plan management. For FFE States performing plan management, as with other FFE States, the current default is that CMS conducts network adequacy reviews of QHP issuer provider access consistent with requirements under § 156.230 for network plans and, for plan years beginning on or after January 1, 2028, under § 156.236 for non-network plans. However, we note that in the 2023 Payment Notice, we clarified that FFE States performing plan management could elect to perform their own network adequacy reviews, but that these reviews must be at least as stringent as Federal network adequacy standards established for QHPs under § 156.230. We have since previously approved a limited number of FFE States performing plan management to conduct network adequacy reviews in their State, who have elected to conduct such reviews, provided the State conducts network adequacy reviews in a manner as stringent as Federal network adequacy reviews.
We have made clear in this proposal, that should the four FFE states performing plan management functions that currently conduct their own network adequacy reviews also elect to conduct provider access reviews and be determined to have an Effective Provider Access Review Programs, they can tailor network adequacy standards to reflect State-specific needs, just as any other FFE State with an Effective Provider Access Review will be able to. This will allow this group of FFE States the flexibility, to tailor network adequacy standards to best reflect the needs of their State. We also clarify that we will work closely with FFE States that conduct plan management functions that have been previously approved to conduct their own network adequacy reviews in previous plan years to assist in a smooth transition to determine if they have Effective Provider Access Review Program in place if they elect to continue to conduct provider access reviews.
Comment:
One commenter requested clarification on operational details regarding the Effective Provider Access Review Program and inquired as to why instructions regarding submission of an attestation for having an Effective Provider Access Review Program were not mentioned when it was detailed in the proposal for an Effective ECP Review Program. The commenter also requested why HHS did not propose to codify the regulatory text to include a requirement to submit an attestation for having an Effective Provider Access Review Program. The commenter also noted that the Effective ECP Review Program proposal outlined a process by which, after an FFE State has been determined to have an Effective ECP Review Program, in subsequent years, HHS would reach out to the FFE State to confirm that the State wishes to continue conducting their own ECP reviews and verify if any circumstances had changed that may affect the State's authority and technical capacity to continue conducting such reviews. They questioned why this detail was not also
( printed page 29738)
included in the Effective Provider Access Review Program proposal.
Response:
We appreciate the commenter raising these additional questions. The regulatory text concerning the process FFE States must follow to elect to conduct their own provider access reviews is located under § 155.1050(d)(1), (5), and (7). We did not address the attestation process or the process for FFE States to confirm they will continue conducting provider access reviews in subsequent plan years because we believe these details are more operational in nature and intend to address these considerations through other guidance including communications sent directly to FFE States. However, we refer the commenter to the discussion in the proposed rule concerning the attestation form and related operational matters in the section of the rule discussing the Effective ECP Review Program (91 FR 6405) and clarify that we will require an attestation from FFE States that elect to conduct provider access reviews just as an attestation will be required of FFE States that elect to conduct ECP reviews. After the publication of this final rule, we intend to notify FFE States about their flexibility to conduct provider access reviews and provide FFE States with instructions on how to do so, including by providing an attestation form to FFE States. We will provide FFE States that elect to conduct provider access reviews time to complete the form, and after an FFE State completes this form, we will begin the determination process to assess if the FFE State meets all applicable criteria under § 155.1050(d)(2) through (4) to be considered to have an Effective Provider Access Review Program. Afterwards, we will send notice of our decisions to FFE States on a rolling basis. The detailed timeline for the entirety of this process, including the deadline to submit the attestation form, and our targeted timeframe for completing our determination process, will be communicated to FFE States through additional guidance. If an FFE State elects to conduct provider access reviews and is identified as having an Effective Provider Access Review Program, we will permit the FFE State to immediately begin conducting provider access certification reviews and will coordinate with the FFE State to communicate to issuers that the State will complete provider access certification reviews. We also will, in subsequent years, confirm with FFE States already determined to have an Effective Provider Access Review Program that they wish to continue to conduct such reviews and whether any circumstances have changed that may affect the State's authority and technical capacity to conduct provider access reviews.
Comment:
We received several comments that included recommendations for the Effective Provider Access Review Program. These included recommendations to remove the exceptions process entirely, to develop an appeal process for States that are determined to not meet the criteria for an Effective Provider Access Review Program, phasing out provider data collection, developing standard definitions to describe provider specialties and county designations, developing a common methodology to measure access, and requirements for FFE States to conduct oversight of provider availability throughout the plan year. Additionally, a few commenters recommended we publicly disclose all information submitted by the State to us, our written determinations, decisions to re-evaluate States that may newly qualify or cease to qualify, and requiring States to submit an annual report on their network adequacy review activities and standardized network adequacy metrics. Finally, one commenter provided a recommendation that CMS verify network adequacy through its own audits and subject States to a corrective action plan or revoke their ability to be solely responsible for their own network adequacy reviews when States perform poorly on network adequacy metrics.
Response:
We appreciate the thoughtful feedback regarding the Effective Provider Access Review Program requirements. At this time, we are not going to finalize any additional requirements, but we will consider these modifications in future rulemaking, as appropriate.
We will retain the exceptions process as it provides flexibility to accommodate FFE States who may be developing innovative methods to assess for provider access but may be, for example, temporarily not clearly meeting a criterion to be determined to have sufficient authority and the technical capacity to conduct provider access reviews and retains room for potential methods and scenarios beyond what we have explicitly described in § 155.1050(d)(2) through (4), which may ultimately benefit consumers in those States. Additionally, while we may consider an appeals process in future rule making, we are not developing an appeals process at this time, but do view the exceptions process as a route that provides comparable flexibility to an appeals process in that if an FFE State is electing to conduct provider access reviews but is aware of criteria they may or will not meet, the exceptions process retains flexibility and offers an open line of communication between the FFE State and HHS to determine if an exception is appropriate and the FFE State can otherwise be determined to have sufficient authority and the technical capacity to conduct provider access reviews.
We are choosing to retain provider data collection requirements for all QHP issuers in all FFE States as we believe this allows us to remain responsive to consumer and other interested parties complaints while providing additional support to FFE States with an Effective Provider Access Review Program. We want to reiterate that QHP issuers in FFE States with an Effective Provider Access Review Program will not be reviewed by us for compliance with our network adequacy standards.
As to the request to develop standard definitions to describe provider specialties and county designations, we believe that these are not necessary as there is already a level of standardization around provider specialty definitions and county type designations. We will not be requiring a common methodology to measure access or requirements for FFE States to conduct oversight of provider availability throughout the plan year as we believe this runs counter to the goals of this policy to allow FFE States flexibility in developing methodologies that are most responsive to specific needs of the State. However, we do want to highlight that to be determined to have sufficient authority and the technical capacity to have an Effective Provider Access Review Program, an FFE State must meet the requirements listed at § 155.1050(d)(4)(ii) which includes a requirement to submit a description of its methodology to us, and these FFE States must also comply with the requirement at § 155.1050(d)(4)(iv) which requires that FFE States conduct reviews prior to the completion of QHP certification. The latter requirement does not prevent the FFE State from additionally conducting mid-year reviews.
As it relates to the request that we publicly disclose all information submitted to us by the State, including our written determinations and decisions to re-evaluate States, and require States to submit an annual report on their network adequacy review activities and standardized network adequacy metrics, we will not be including these as requirements as it may risk disclosing QHP issuer confidential business information,
( printed page 29739)
including contracting details and network development strategies. While we will consider these suggestions for future policymaking, we highlight that in no way are we preventing the FFE State from publicly disclosing the items mentioned above and we encourage interested parties to work with their FFE State that is determined to have an Effective Provider Access Review Program to proactively make these items publicly available to consumers in their States.
As it relates to the comment requesting that we audit FFE States with Effective Provider Access Review Programs, at this time we will not include any additional requirements or develop timelines or processes for proactive audits, but we will consider it for future plan year rulemaking. Due to the nascent state of the policy and the expectation that it may take a few plan years before we see many FFE States electing to conduct and satisfy the criteria to have Effective Provider Access Review Programs, we believe that, currently, the addition of a proactive audit would be an unneeded additional burden on States that are or will be the process of initial qualification. Though, we will consider this for future rule-making we feel we first must gain a clear understanding of the number of FFE States who elect to conduct provider access reviews, receive their initial submission of the contents of their Effective Provider Access Review Programs, and understand how they intend to conduct these reviews before we can begin to develop an auditing process. In the meantime, we also view the continued collection of provider data from all QHP issuers, including those in FFE States determined to have an Effective Provider Access Review Program, as a means of maintaining awareness of provider access relative to our Federal time and distance standards, should complaints arise from interested parties.
Comment:
Several commenters called for transparency efforts and opportunity for public comment on an FFE State's ability to implement and maintain an Effective Provider Access Review Program. These include requests for public facing documentation of an FFE State's network adequacy standards, publishing issuer deficiencies and any justifications and exceptions granted, information around consumer complaints, information on inaccuracies in provider directories, and notification of any proposed timelines for an FFE to demonstrate that it will meet standards for becoming an Effective Provider Access Review Program.
Response:
While we will continue to consider commenters' points, at this time, we will not include additional requirements concerning FFE State transparency as it relates to their election, application, development, or operation of an Effective Provider Access Review Program. Regarding requests for the publishing of issuer deficiencies, justifications, exceptions, and consumer complaints, we believe that requiring public disclosure of this information may risk disclosing confidential business information, including contracting details and network development strategies, which would be inappropriate. We also believe that publishing this information may lack context, for example, it may not always be obvious or clear when deficiencies or complaints are due to geographic limitations or provider availability outside of an issuer's control. Additionally, any remediation efforts to resolve outstanding deficiencies or complaints may not be made easily clear and may risk disclosure of confidential business information. Regarding inaccurate provider directories, we note that provider directory information is highly dynamic and changes frequently and believe that public reporting of provider directory inaccuracies may pose significant operational burden. Any public reporting of inaccuracies that is not updated in near-real time could become a source of misinformation in and of itself.
Regarding requests for public facing documentation of an FFE State's network adequacy standards, we believe that the criteria described under § 155.1050(d)(4) that an FFE State must meet to be determined to have an Effective Provider Access Review Program, specifically the requirement that the State have its provider access standards set forth in statute or regulation, satisfies this request. We would refer FFE States with an Effective Provider Access Review Program to our Network Adequacy QHP Certification web page as a model for items to make publicly available regarding provider access reviews. Regarding notifications of and updates on any proposed timelines for an FFE State to demonstrate that it will meet standards to become an Effective Provider Access Review Program, we note that numerous factors may influence a State's timeline that may cause frequent revision, which may ultimately cause more confusion for the public. However, we plan to publicly share a list of States that have been determined to have an Effective Provider Access Review Program once that determination has been made. We will continue to evaluate the appropriate scope and format of any necessary public disclosures and highly encourage interested parties to engage with their State regulators to achieve a level of transparency that all parties find satisfactory.
11. Essential Community Provider Standards for Network Plans (§ 156.235) and Implementation of the Effective Essential Community Provider Review Program (§ 155.1051)
In the 2027 Payment Notice proposed rule (91 FR 6399), for PY 2027 and subsequent plan years, we proposed changes to QHP certification requirements for essential community providers (ECPs) included within a network plan issuer's provider network. First, we proposed to reduce the minimum percentage requirement (also referred to as the “ECP thresholds” or “ECP threshold requirements”) from 35 to 20 percent. (The minimum percentage requirement specifies a minimum percentage of participating ECPs that must be included within a network plan issuer's provider network based on the total available ECPs within the issuer's service area). Second, we proposed to change the narrative justification regulation text at § 156.235(a)(3) and (b)(3) to be consistent with systems changes and existing issuer ECP data submission requirements as part of ECP certification reviews. Third, as further discussed in this section, we proposed at new § 155.1051 to allow FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of QHP issuers' plans provided that the State has sufficient authority and the technical capacity to conduct these reviews, demonstrated by satisfying applicable criteria established by HHS to be considered an Effective Essential Community Provider (ECP) Review Program.
Section 1311(c)(1)(C) of the Affordable Care Act directs the Secretary to establish by regulation certification criteria for QHPs, including criteria that require QHP issuers to include ECPs within health insurance plan networks. ECPs include providers that serve predominantly low-income and medically underserved individuals, such as health care providers described in section 340B(a)(4) of the PHS Act and section 1927(c)(1)(D)(i)(IV) of the Act. We first implemented the above statutory provisions of the Affordable Care Act and codified ECP standards at § 156.235 in the Exchange Establishment Rule (77 FR 18310).
( printed page 29740)
These standards help ensure medical QHPs and SADP issuers include in their provider networks a sufficient number and geographic distribution of ECPs, where available, as a requirement to receive certification as a QHP.
a. Reduction of the Minimum Percentage (or Threshold) Requirement From 35 to 20 Percent
Sections 156.235(a)(2)(i) and (b)(2)(i) stipulate that a plan applying for QHP certification to be offered through an FFE has a sufficient number and geographic distribution of ECPs if it demonstrates, among other criteria, that its provider network includes as participating providers at least a minimum percentage, as specified by HHS, of available ECPs in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B). As stated in § 156.235(a)(2)(i) and (b)(2)(i), for purposes of satisfying this minimum percentage requirement, also known as the ECP threshold requirement, multiple providers at a single location count as a single ECP toward both the available ECPs in the plan's service area and the contracted ECPs included in the issuer's network for calculating the threshold.
The minimum percentage requirements have been modified over the years (for example, 20 percent, 30 percent, 35 percent) to accomplish different policy and operational priorities, such as to reduce regulatory burden (82 FR 18373, 83 FR 17025), to align with market conditions (82 FR 18373, 83 FR 17025), to expand access to care for consumers (87 FR 27336, 88 FR 25882), and to promote broader networks (87 FR 27336, 88 FR 25882). For example, for QHP certification for PY 2018, we reduced the minimum percentage requirement from 30 to 20 percent to substantially reduce the regulatory burden on issuers (due to issuers needing to submit less data on provider contracts with ECPs to demonstrate satisfaction of the ECP standard under § 156.235), while still requiring issuers to include a sufficient number and geographic distribution of ECPs in their networks (82 FR 18373). These minimum percentage requirements have been set at 35 percent since PY 2023 (87 FR 27336). In the 2024 Payment Notice (88 FR 25882), we also began to apply these minimum percentage requirements separately to two existing types of ECP categories that comprise more than 60 percent of all facilities on the HHS ECP List: FQHCs and family planning providers, in accordance with revisions to § 156.235(a)(2)(i) and (b)(2)(i).[313]
At a high level, to meet the ECP threshold requirements under § 156.235, issuers have been required to contract with at least 35 percent of available ECPs in each plan's service area to participate in the plan's network (that is, the overall ECP threshold requirement), at least 35 percent of available FQHCs that qualify as ECPs in the plan's service area (that is, the FQHC threshold requirement), and at least 35 percent of available family planning providers that qualify as ECPs in the service area (that is, the family planning provider threshold requirement).
To reduce administrative burden for QHP issuers, we proposed (91 FR 6399) to reduce the overall threshold, FQHC threshold, and family planning provider threshold requirements from 35 to 20 percent for both medical QHP and SADP issuers in FFE States, including States performing plan management, for PY 2027 and thereafter. We stated that we would consider medical QHP and SADP issuers to have satisfied the overall threshold requirement if these issuers contract with at least 20 percent of available ECPs in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B) to participate in the plan's provider network. Additionally, we stated that medical QHP issuers would be considered to have satisfied the separate FQHC and family planning provider threshold requirements by contracting with at least 20 percent of available FQHCs that qualify as ECPs in the plan's service area and at least 20 percent of available family planning providers that qualify as ECPs in the plan's service area, respectively. We also stated that SADP issuers would be considered to have satisfied the separate FQHC threshold requirement by contracting with at least 20 percent of FQHCs offering dental services in the plan's service area. We stated that the calculation methodology for determining if an issuer meets the threshold requirements would be consistent with previous years.[314]
We noted that while we proposed to lower the requirements for each of these three thresholds, we recognized that issuers have the flexibility to continue to choose to exceed the proposed minimum percentage requirement within their provider networks. We further noted that each plan year, ECP certification data consistently indicate that the majority of issuers on the FFE, including States performing plan management, exceed each of the minimum percentage requirements,[315]
and in prior years when the minimum percentage requirement was reduced (for example, from 30 to 20 percent during PY 2018), many FFE issuers continued to choose to exceed minimum percentage requirements.
In the proposed rule (91 FR 6400), we stated that we believe reducing the overall threshold, FQHC threshold, and family planning provider threshold requirements from 35 to 20 percent would provide additional flexibility for QHP issuers to build provider networks that comply with the ECP Standard under § 156.235. We further stated that we believe reverting to the previous 20 percent minimum percentage that issuers were accustomed to at the establishment of the FFE in PY 2014 and during PYs 2018 through 2022 would minimize disruptions for issuers in adjusting to meet the threshold requirements. We stated that in the past, several commenters on the Market Stabilization final rule (82 FR 18373) supported our proposals to decrease ECP threshold requirements, commenting that the lower threshold requirement would reduce the administrative burden on issuers, especially for those issuers in rural areas or States with few ECPs. We welcomed comments on if the proposed threshold percentage would still enable enrollees to access ECPs in rural areas and would not impose barriers to entry for issuers in rural areas by discouraging issuers from expanding into such areas (91 FR
( printed page 29741)
6400). Similarly, we stated that we expect these proposed changes would continue to reduce the regulatory and administrative burden on QHP issuers, such as by reducing the number of resources expended to secure and negotiate additional provider contracts and potential compliance related costs associated with submitting additional ECP data on provider contracts to meet the ECP standard under § 156.235. We further stated that this may provide issuers with more resources and flexibilities while still ensuring that a meaningful number of ECPs are included within an issuer's provider network consistent with the requirements of section 1311(c)(1)(C) of the Affordable Care Act. We also solicited comment on whether there is an alternative threshold percentage that is more effective and appropriate, including threshold percentages that may be targeted to specific geographic areas where issuers may require additional flexibilities to meet threshold requirements, and a percentage that strikes the appropriate balance between issuer flexibility and enrollee access. Furthermore, we stated that we understand that network participation negotiations are an important tool that issuers use to manage costs; therefore, fewer provider contracts needed to comply with threshold requirements may free up financial resources that issuers may leverage for other activities, such as innovating plan offerings to meet the diverse needs of consumers or passing on savings to consumers through lower premium rates that may especially benefit low-income and underserved populations.
Lastly, we stated that we continue to recognize concerns shared previously by commenters related to potential access to care barriers when reducing ECP threshold requirements in the past (82 FR 18373). We noted that when ECP threshold requirements were set at or reduced to 20 percent in previous years (PY 2014, PYs 2018 through 2022), we expanded efforts to ensure continued access to care to ECPs within an issuer's provider network. We continuously monitored potential issues raised by consumers and escalated any ECP access concerns identified through monitoring efforts by performing direct outreach to QHP issuers, as appropriate, including as part of post-certification monitoring and compliance efforts. Similarly, we stated that we would continue to monitor potential issues and undertake efforts to ensure consumers maintain adequate access to ECPs, and we would address any concerns through future guidance and/or possible rulemaking, as appropriate.
We sought comment on this proposal to reduce the overall threshold, FQHC threshold, and family planning provider threshold requirements from 35 to 20 percent. We received many comments from a variety of commenters that represent issuers, provider-based advocacy organizations, ECPs, and consumers.
After considering these comments and for the reasons outlined in the proposed rule and this final rule, we are not finalizing this proposal. Accordingly, HHS will retain the existing threshold requirements at 35 percent. We summarize and respond to public comments received on this proposal below.
Comment:
We received many comments in response to this proposal. The majority of commenters, such as consumers, advocacy groups representing providers, and ECPs (for example, FQHCs, family planning providers, Ryan White Providers, dental health centers, hemophilia treatment centers, cancer hospitals, etc.) opposed the proposed reduction of threshold requirements from 35 to 20 percent.
Commenters raised an array of concerns regarding access to care and other downstream impacts to safety-net providers that such a reduction in threshold requirements may perpetuate, especially for low-income and medically underserved individuals that rely on ECPs. Commenters believed this would weaken one of the few statutory safeguards within the Affordable Care Act that is intended to protect access to safety-net providers. Commenters stated that lowering threshold requirements would narrow and destabilize provider networks, affecting a consumer's reliable access to ECPs as participating providers in their issuer's provider network. Some commenters noted that this may widen existing gaps in provider networks between “theoretical network coverage” and “practical access,” which are influenced by providers no longer accepting new patients or an issuer's plan, or even “ghost networks” [316]
; thus, commenters stated even if an issuer includes 20 percent of ECPs within their service area, some ECPs listed as in-network by the issuer could be inaccessible for other reasons, such as not having the bandwidth or resources to accept all the issuer's enrollees at one given time.
Commenters further stated that if issuers include fewer ECPs within their provider networks as in-network providers due to this proposal, then consumers may experience disruptions in established relationships with existing ECPs, which may push some consumers to change providers. Other commenters noted that reducing the number of in-network providers may further limit enrollee choice, increase waiting times, cause families to travel farther for care, make consumers forgo needed services, or necessitate that consumers switch plans to stay with their provider of choice.[317]
In addition, commenters added that disruptions in continuity of care could affect quality of care and health outcomes if fewer in-network ECPs cause delays in seeking preventive services and routine screenings, regular chronic disease management, behavioral health services, and specialty care, which may increase avoidable emergency department visits.
In contrast, some commenters, including issuers, supported the proposal to reduce the threshold requirement from 35 to 20 percent. These commenters reasoned that this would reduce contracting burden while still maintaining meaningful inclusion of ECPs within an issuer's network. One commenter stated that a minimum percentage of 35 percent may force plans to include any willing ECP regardless of their quality or cost-efficiency to meet regulatory requirements, and reducing the minimum percentage may allow plans to focus on curating a network of higher-quality ECPs. Lastly, one commenter stated that they would support a proposed reduction in the threshold requirement, provided issuers continue to ensure at least one ECP category per county in the issuer's service area is included in their networks.
Response:
The commenters raised valid points about the proposal negatively affecting access to care by potentially disrupting enrollees' established relations with ECPs and limiting enrollee choice by incentivizing issuers to narrow networks, potentially disrupting continuity of care and risking negative health outcomes. We continue to prioritize consumers' adequate access to ECPs through their plans and do not intend to potentially harm consumer
( printed page 29742)
access through a reduced minimum percentage. We agree that ECPs provide valuable services to their communities (for example, preventive services, specialty care, etc.). Thus, we believe commenters' concerns warrant additional consideration and analysis, before finalizing a reduction in the threshold requirement, especially to safeguard low-income, medically underserved individuals that rely on ECPs as safety-net providers within their communities. For these reasons, we are not finalizing the proposal at this time.
In particular, we recognize the valid points that consumers raised regarding the existence of ghost networks or “theoretical networks” and the ECP threshold reduction potentially widening gaps in access already impacted by ghost networks, leading to no guarantee that all ECPs that an issuer contracts with are truly available and even more so if less ECPs are in-network with the issuer. We agree with commenters that these are important issues that need to be addressed, and that maintaining the existing threshold requirement could mitigate some of these effects while we conduct further analysis. While additional policy solutions would likely be required to address the specific issue of ghost or theoretical networks, which are beyond both the scope and purpose of this proposal, we appreciate the commenters' attention and feedback.
We also recognize concerns raised by commenters that reducing the number of in-network ECP facilities may further limit enrollee choice, and increase wait times, cost, and consumer burden due to the need to travel farther for care, potentially leading to consumers forgoing needed medically necessary services, including specialty care. We believe that retaining the existing minimum threshold would help stabilize the number of ECPs within current issuer networks at the current level, which would assist in addressing commenters' concerns that the threshold reduction would compromise enrollee choice and increase wait times and cost due travel time for specialized care.
Furthermore, we understand that some commenters believe that a specific minimum percentage may incentivize some issuers to contract with additional providers or facilities to meet requirements regardless of quality and that a lower minimum percentage may allow issuers to focus more resources on curating a network of higher quality ECPs. While it is possible that the specific minimum percentage could produce tradeoffs in the extent to which issuers consider the quality versus quantity of providers and facilities in their network, we believe that assuring consumers have more choice in the ECPs available within issuer's network and service area and adequate access should be prioritized. HHS can help facilitate this by setting a specific minimum percentage to ensure consumers have access to ECPs, but we do not currently set parameters on quality and cost-efficiencies for ECPs nor how issuers choose which qualified ECPs to include in their networks, as issuers are best equipped to consider these factors when deciding which providers are in their networks. Issuers retain the discretion to select among HHS-approved, qualified ECPs when curating their networks. The pool of eligible ECPs already reflects a baseline standard of eligibility and qualifications, as ECPs are reviewed and approved by HHS and other Federal partners [318]
to verify that covered entities meet all applicable statutory requirements prior to inclusion. Issuers therefore have the flexibility to prioritize ECPs within that qualified pool while still meeting the existing threshold.
Lastly, regarding the commenter who supported a threshold reduction if the category per county requirement was retained, we confirm that issuers must continue to offer a contract to at least one ECP category per county in the issuer's service area and networks, as we did not propose to remove this requirement.
Comment:
Commenters raised several potential cost impacts to consumers, ECPs, and issuers resulting from a reduction in the threshold requirement from 35 to 20 percent. Specifically, some commenters stated that if finalized, this proposal would cause issuers to choose to include fewer ECPs as in-network providers, and this may raise consumer out-of-pocket costs unless consumers can find other in-network ECPs. Multiple commenters also stated that if issuers contract with fewer ECPs, then ECPs would lose an important source of revenue from network contracts which could be financially destabilizing when ECPs already face declining margins, a disproportionate share of uncompensated care, and low reimbursement rates, further increasing existing risks of facility closures. Commenters that are ECPs further added that this may impact their ability to use Federal ECP requirements as leverage during contract negotiations with QHP issuers since these issuers would face less pressure to offer contracts to include additional facilities with almost a 50-percent reduction in the stringency of the threshold percentage requirement, if finalized.
However, commenters in support of the proposal stated that a reduction in threshold requirements may help lower costs for consumers with savings from a decrease in administrative costs, if issuers have more flexibility to evade contracts with higher-cost providers that increase premiums. These commenters also reasoned that lower threshold requirements would allow issuers more resources to account for other variables in their network designs, such as workforce shortages and improving care coordination, while still ensuring consumers have access to ECPs. One commenter believed there was little evidence to prove that the previous 20 percent threshold harmed access to care when in effect; though, many commenters opposing this proposal stated that reducing administrative burden is an insufficient reason to reduce threshold requirements, which increase the risk of impacting patient care.
Response:
We thank commenters for sharing different perspectives on this issue. We continue to believe that the affordability of plans through the FFE remains important, and that lowering a consumer's out-of-pocket costs helps serve this purpose. We do not intend to increase consumer out-of-pocket costs through a lower threshold requirement, rather we stated in the proposed rule that a lower threshold requirement could potentially decrease premiums. However, we believe that consumers raise important points on how a lower threshold requirement could potentially increase out-of-pocket costs if consumers cannot identify alternative in-network ECPs within their service area if an issuer ceases contracts with their preferred ECP, which becomes an out-of-network provider. We recognize that when ECPs become out-of-network, this could result in out-of-pocket costs for consumers continuing to see these ECPs. We understand that ECPs serve low-income, medically underserved individuals that may be less equipped to assume additional out-of-pocket costs, including those who often receive expensive specialty care services (for example, cancer care, HIV/AIDs treatment, etc.) from ECPs, which could serve as a significant barrier to accessing needed and/or critical services. Thus, we believe that these cost-related concerns and risks to the financial stability of ECPs warrant additional consideration and analysis before
( printed page 29743)
finalizing any possible reduction in the threshold requirement to safeguard access.
Additionally, we believe commenters raised important concerns regarding the financial stability of ECPs, including the financial strain of declining margins, disproportionate shares of uncompensated care, and low reimbursement rates. These cost-related concerns and risks to the financial stability of ECPs warrant additional consideration and analysis before finalizing any reduction in the threshold requirement. We remain open to understanding more directly from ECPs how specific minimum percentages influence an ECPs' ability to successfully negotiate contracts with QHP issuers.
Furthermore, in response to comments that supported reducing threshold requirements due to lower administrative costs for issuers and greater flexibility in network design, we understand that a reduced threshold requirement may reap these benefits, but we remain more concerned about the impact of this policy on ECP financial stability and consumer out-of-pocket costs. While one commenter stated that there is no substantive evidence that the previous 20 percent threshold negatively impacted access to care, we believe the potential for harm to vulnerable populations warrants a particularly cautious approach. Lastly, we hope that recent HHS initiatives to reduce issuer administrative burden and costs during QHP certification will further mitigate these concerns; for example, MPMS enhancements to allow issuers to import ECP data from their previous year's QHP application, filter options to only display applicable ECPs meeting specific ECP requirements, and a new ECP calculation workspace that provides direct feedback to issuers on performance and how to close gaps.
We will continue to monitor ECP inclusion trends and may revisit the threshold requirements in future rulemaking if evidence supports a revision. In the meantime, we reiterate that as crucial safety-net providers, ECPs must continue to treat patients on a sliding fee schedule and regardless of ability to pay; thus, regardless of the specific minimum percentage, ECPs should continue to serve low-income, medically underserved individuals regardless of insurance status and not subject individuals to excessive out-of-pocket costs far beyond their ability to pay. Thus, in this way, we agree with commenters that it is important to ensure low-income, medically underserved individuals receiving care at ECPs are not exposed to significant out-of-pocket costs.
Comment:
Many commenters deliberated on the appropriate, specific ECP minimum percentage that HHS should require. Most commenters believed that HHS should maintain the ECP minimum percentage at 35 percent. Commenters reasoned that since the majority of current QHP issuers exceed the 35 percent threshold, they were not convinced that issuers currently struggle to meet existing ECP threshold requirements enough to justify a reduction, and reasoned that some plans demonstrate even more capacity to maintain broader networks as evidenced by issuers that have exceeded the current 35 percent threshold. A few commenters added that the minimum percentage should not be lowered if issuers currently prove the existing minimum percentage is achievable, and that the purpose of a minimum percentage is to function as a guardrail for plans that are outliers due to poorer performance on ECP thresholds. Commenters pointed to HHS' progress in expanding protections for populations served by ECPs through current ECP requirements under § 156.235, as evidenced by higher compliance amongst issuers achieving ECP threshold requirements, and some commenters noting they have noticed fewer legal disputes and consumer complaints related to ECP access likely due to current ECP requirements. Commenters were concerned that if HHS were to proceed with reducing the ECP minimum percentage, this may reverse current progress if issuers reduce participating ECPs in their networks, and consequently, cause networks to narrow over time. Furthermore, many commenters did not believe enough empirical evidence (for example, through geographic modeling, network-composition analysis, literature, etc.) exists to demonstrate that HHS could reduce the ECP threshold without affecting access to care, and thus, encouraged HHS to share more data to support that a 20 percent minimum percentage would ensure meaningful access for low-income, medically underserved individuals.
Commenters also responded to HHS' comment solicitation on whether there is an alternative threshold percentage that is more effective and appropriate, including threshold percentages that may be targeted to specific geographic areas where issuers may require additional flexibilities to meet threshold requirements, and a percentage that strikes the appropriate balance between issuer flexibility and enrollee access. Specifically, some commenters recommended maintaining the threshold requirement at 35 percent or an alternative threshold between 20 and 35 percent until CMS can publish additional data to evaluate enrollee access to ECPs and impact on premiums. One commenter believed the existing 35-percent threshold is too low and should be increased. A few commenters suggested that CMS at least maintain the FQHC threshold requirement at 35 percent, create a new threshold requirement for ECPs that treat serious illnesses (for example, Cancer Hospitals, Ryan White Providers, Community Mental Health Centers, etc.), or require issuers that seek to include in their network around 20 percent of available ECPs in the issuer's service area to demonstrate that ECP access for underserved populations will be maintained.
Response:
Due to the concerns raised regarding the empirical evidence present to justify this proposal in particular, we agree that it is not appropriate to finalize a reduction in ECP threshold requirements until we conduct additional data analysis, including leveraging geographic modeling or network-composition analyses to ensure a threshold reduction would not adversely affect access to care. We are currently expanding data analysis efforts by utilizing geographic and composition analysis methods to analyze access to ECPs, including ECP category types, within certain geographic areas and according to different demographics. As part of these efforts, we also seek to understand the impact of specific ECP threshold percentages, such as if issuers are more likely to experience barriers in meeting ECP threshold requirements within certain geographic areas. Thus, we may consider this data along with these comments and make modifications to the ECP threshold requirements, as appropriate, through future rulemaking. We will also take into careful consideration the range of alternative threshold recommendations offered by commenters when examining if modifications to the threshold requirements are needed after supplemental analyses (for example, an interim threshold between 20 and 35 percent, maintaining at least the FQHC threshold at 35 percent or creating a new threshold category for ECPs that treat serious illnesses, and/or requiring documentation for issuers scoring between 20 and 35 percent).
We thank commenters who highlighted our progress in expanding protections for populations served by ECPs, as evidenced by higher rates of issuer compliance due to most issuers
( printed page 29744)
achieving threshold requirements across a range of service areas and market conditions, and a reduction in legal disputes and consumer complaints related to ECP access. We do not intend to potentially reverse this progress by creating conditions in which issuers have less incentive to maintain robust ECP participation. Thus, we are maintaining the existing minimum percentage at the attainable 35 percent, while identifying if additional approaches exist that promote issuer flexibility and maintain robust access to ECPs.
Comment:
Multiple commenters raised concerns that a reduction in the overall ECP threshold may decrease the number of ECPs within categories of services that are encompassed under the overall ECP threshold but do not currently have their own categorical threshold requirements like FQHCs and family planning providers. For example, commenters that represented Inpatient Hospitals, Ryan White Providers, Specialized Cancer Centers, Mental Health Facilities, and Hemophilia Treatment Centers were concerned that if the overall ECP threshold requirement were reduced further, fewer of these specialized facility types would be included in issuers' provider networks since there are no standalone categorical threshold requirements for these ECP category types. Commenters stated that less representation of these facility types in the overall ECP threshold could affect access to quality and comprehensive HIV care, chronic disease management, bleeding disorder care, pediatric specialty care, oncology services, and treatment for rare and complex conditions, which could impose additional costs to consumers.
Response:
We appreciate the concerns raised by commenters representing specialized ECP categories (such as Inpatient Hospitals, Ryan White Providers, Specialized Cancer Centers, Mental Health Facilities, Hemophilia Treatment Centers) regarding the potential downstream effects of reducing the overall ECP threshold for facility types that do not currently have their own standalone categorical threshold requirements. We understand the concerns stated by these commenters that a reduction in the overall ECP threshold could affect the representation of these specialized facility types within issuer networks, given that they are not independently protected by categorical threshold requirements in the same manner as FQHCs and family planning providers. We also recognize that these providers and facilities furnish services that often have limited alternatives within a given service area, and believe commenters raise important concerns that if the reduction in the overall threshold reduces the number of specialized facility types as in-network providers, consumers may face greater costs if receiving these services out-of-network, or may forgo needed care altogether due to cost or access barriers. We do not intend to create differential access to certain categories of ECPs through a proposed reduction in minimum percentage requirements, nor do we intend to signal that issuers should contract with one type of ECP category over another to meet the overall ECP threshold requirement. We continue to believe that all ECP categories should be represented within an issuer's provider network, which is why we continue to maintain the current ECP category per county requirements under § 156.235(a)(2)(ii)(B), so that issuers include in their network at least one ECP per each ECP category per county. Nevertheless, since we do not have sufficient data at this time to prove issuers would retain specialty care providers if there were a reduction in the overall ECP threshold, we believe it is not appropriate to finalize this proposal at this time until we understand these concerns in more depth through subsequent data analyses. We may also consider whether additional categorical threshold requirements or other targeted protections for ECPs providing specialty care may be warranted to better safeguard access for enrollees with complex, chronic, or rare conditions.
Comment:
Many commenters stated concerns specific to the FQHC threshold and family planning provider threshold. Commenters that represented community health centers, or FQHCs, shared specific concerns on potential impacts of reducing the FQHC threshold requirement from 35 to 20 percent and that FQHCs should not be treated interchangeably with other ECP categories. Commenters stated that FQHCs operate greater than 17,000 sites nationwide and serve more than 52 million patients annually, such as by providing comprehensive primary and behavioral health care services, care coordination, and reproductive health care. Commenters stated that FQHCs serve as the backbone of care to predominately low-income, medically underserved individuals, those in rural communities, people of color, individuals living with disabilities, and pregnant woman. Commenters shared that health center patients are four times more likely to have an income at or below the Federal Poverty Level (FPL) and twice as likely to have an income under 200 percent of the FPL compared to the U.S population.[319]
Thus, commenters stated that reducing the FQHC threshold may further risk that issuers include fewer FQHCs in their networks, potentially impacting access to essential services for enrollees if FQHCs become out-of-network and making contractual terminations financially destabilizing when FQHCs are currently experiencing declining margins.
Commenters further shared additional implications that a reduction in the FQHC threshold may have on dental services. Multiple commenters that represent dental health centers shared that FQHCs serve as crucial dental safety-net providers that provide dental care and treat severe dental infections for enrollees who often face financial, geographic, and insurance-related barriers to accessing routine dental care. These commenters were concerned that the reduction of the FQHC threshold may have a compounding disadvantage for safety-net dental providers alongside broader proposals to reinstate the prohibition on coverage of routine non-pediatric dental services as an essential health benefit.
Furthermore, some commenters were similarly concerned over the proposed reduction in the family planning provider threshold. Commenters reasoned that family planning providers serve as the safety-net for sexual and reproductive health care, women preventive care and screening, and counseling, and that these providers have relied on the family planning provider thresholds as points of leverage during contract negotiations with Exchange insurers. Commenters added that family planning providers have experienced significant, increasing financial pressure and operational strains in recent years to serve patients due to funding disruptions, thus losing additional revenue from contracts with insurers may further disrupt timely access to care and worsen maternal health outcomes.
Response:
We agree with commenters that FQHCs and family planning providers continue to serve as important safety-net providers within their community and provide an array of services to cater to a variety of health needs. This is why we established separate categorical threshold requirements for FQHCs and family planning providers to expand access to these provider types, and why we also require issuers to offer a contract to an FQHC and family planning provider
( printed page 29745)
within each county consistent with category per county requirements under § 156.235(a)(2)(ii)(B). Additionally, we understand commenters' concerns that FQHCs and family planning providers currently face significant financial strain, and we agree that these are important issues to address. Therefore, after consideration of these comments, we are not finalizing this proposal. We also take note of the concerns raised by commenters that a reduction in the FQHC threshold, considered alongside broader proposals affecting dental benefits, could have a disproportionate and compounding disadvantage for dental providers and the populations they serve.
In addition, we take note of the concerns raised by commenters that family planning providers have experienced significant financial pressures and operational strains in recent years due to funding disruptions, and the concern that a reduction in the threshold requirement would potentially correspond to the loss of revenue from insurer contracts if issuers do not renew contracts with ECPs due to lower threshold requirements. Not finalizing this proposal would allow us to further examine these concerns in more depth. Additionally, we will continue monitoring consumer access to FQHC and family planning provider, and consider potential future revisions to these threshold requirements as needed.
Comment:
Commenters addressed HHS' comment solicitation on if the proposed threshold percentage would still enable enrollees to access ECPs in rural areas and would not impose barriers to entry for issuers in rural areas by discouraging issuers from expanding into such areas. Commenters highlighted that rural residents currently face high premiums, fewer plan choices, long travel distances to access care, rural hospital closures, provider shortages, and poorer health outcomes compared to urban populations. Commenters also added that even having rural providers in-network does not guarantee these providers are accessible due to geographic and transportation barriers, and that reducing even a small number of safety-net providers can materially affect access to care and further narrow networks of rural providers. One commenter suggested that HHS conduct a rural impact analysis, while closely looking at access to rural hospitals.
Response:
We appreciate the concerns raised by commenters regarding the potential impact of reducing the ECP threshold requirement on enrollee access to ECPs in rural areas. We agree with the commenters' suggestion that we should consider conducting a rural impact analysis, especially with greater focus on rural hospitals, and believe this is a critical area that we can include as part of future data analysis initiatives. We understand that rural areas currently face significant provider supply shortages, which is why we are engaging rural providers as part of upcoming provider outreach initiatives, to recruit more eligible, qualified rural providers to HHS' ECP List, which would expand access to these ECPs. We also appreciate commenters for sharing specific barriers to care that rural residents regularly face, and we do not intend to risk further exacerbating disparities in access to care in rural areas where geographic and transportation barriers inherent to rural areas already make seeing in-network providers challenging, and where provider density is already limited and few alternative in-network options may be available. We intend to take all these comments into account to ensure that existing and future threshold requirements do not adversely affect access to care for rural enrollees.
Comment:
One commenter recommended that if HHS were to finalize a reduction in ECP threshold requirements from 35 to 20 percent, that HHS should require State Exchanges and issuers offering plans through State Exchanges to report data on in-network, contracted ECPs within each plan's service area and demographical data (for example, diagnoses, disability status, race/ethnicity, sex, etc.) on consumers seeking care from these ECPs.
Response:
We appreciate the commenter's suggestion. We would welcome the opportunity to collaborate with both States and issuers to better understand broader trends in access to ECPs within issuer's networks across State Exchange types, along with more details on consumers that typically receive care from ECPs. However, we did not propose or intend to impose any ECP-related threshold requirements on State Exchanges as a part of this proposal, and we do not currently require State Exchanges to submit ECP data collected from QHP issuers to HHS. Thus, we do not believe it is appropriate to finalize this recommended requirement at this time. Lastly, we believe this requirement could impose additional burden on both issuers in State Exchanges and States that do not currently report data to HHS, and issuers would have to implement new processes and expend resources to comply with ECP data reporting requirements.
Comment:
One commenter stated that if HHS were to finalize a reduction in ECP threshold requirements, this would require additional effort for States that currently rely on the medical QHP and SADP ECP Review Tools. Some States, especially State Exchanges, currently utilize these tools as part of State certification review processes by having QHP issuers in their State utilize the tools to calculate the total number of ECPs included in each plan's network within a service area to determine a threshold percentage of participating ECPs. The commenter was concerned that the State would need to perform additional data analyses if the State does not have a 20 percent threshold requirement.
Response:
We thank the commenter for sharing their concern as it relates to the reduction in the ECP threshold requirement and how States rely on the medical QHP and SADP ECP Review Tools. We want to clarify that, regardless of the Federal ECP minimum threshold percentage, State Exchanges, State-based Exchanges on the Federal platform, and issuers in these Exchanges that utilize the QHP and SADP ECP Review Tools would continue to have access to these ECP resources. We intend to continue developing and maintaining these tools and resources for States for PY 2027. Furthermore, the ECP Review Tools are already designed with flexibility to accommodate varying threshold requirements across States. Specifically, the tools allow users to modify the ECP threshold percentage within the tool to align threshold percentage requirements applicable in their respective State, including for State Exchanges that have established a different ECP threshold standard than the Federal minimum percentage. As such, States that maintain a threshold requirement that differs from the Federal minimum would retain the ability to configure the tools accordingly, without the need for additional data analyses outside of the existing tools.
b. Modifications to Narrative Justification Requirements at §§ 156.235(a)(3) and 156.235(b)(3)
Additionally, we proposed to change the narrative justification regulation text at § 156.235(a)(3) and (b)(3) to be consistent with system changes, current HHS operational processes, and existing issuer ECP data submission requirements as part of ECP certification reviews.[320]
The regulations at
( printed page 29746)
§ 156.235(a)(3) and (b)(3) currently state that if a plan applying for QHP certification to be offered through an FFE does not satisfy the ECP standard (under § 156.235(a)(2) for the General ECP Standard and § 156.235(b)(2) for the Alternate ECP Standard), the issuer must include as part of its QHP application a narrative justification describing how the plan's provider network provides an adequate level of service for low-income enrollees or individuals residing in Health Professional Shortage Areas within the plan's service area and how the plan's provider network will be strengthened toward satisfaction of the ECP standard prior to the start of the benefit year.
However, as we stated in the proposed rule, since beginning to collect this narrative justification information in PY 2014, we have instituted multiple refinements and modernizations to this process in recent years, including through innovations and standardizations to ECP data collection by implementing the ECP User Interface (UI) [321]
in the Marketplace Plan Management System (MPMS). MPMS allows us to collect the same type of information previously obtained from the narrative justification without having to actually require issuers to fill out the narrative justification. We have integrated the ECP data collection into MPMS such that issuers can easily submit their ECP data, including justification related information previously collected through written narratives and pre-populated Excel templates, without having to again explain or describe how the plan's provider network provides an adequate level of ECPs prior to the start of the benefit year.
In the proposed rule, we stated that due to these technical enhancements, along with other process efficiencies and resources provided to issuers (for example, Final Plan Year ECP Lists, outreach activities, and change reports), we have been able to efficiently obtain relevant quality data to adequately perform ECP certification reviews while reducing the time and resources required by issuers to submit supporting information, including the narrative justifications required by § 156.235(a)(3) and (b)(3). The ECP data obtained by issuers during the QHP certification process details which qualified ECPs have contracts executed with the issuer within each of the issuer's provider networks and service areas, which allows us to calculate an issuer's satisfaction of the ECP standard. This ECP data also identifies opportunities to alleviate gaps in an issuer's network and service area to ensure reasonable and timely access to ECPs by identifying additional ECPs an issuer may contract with to meet the ECP standard, while also highlighting different contract negotiation statuses that may explain why an issuer has not yet executed a contract with a specific provider.
Therefore, we proposed to modify and simplify this regulatory language at § 156.235(a)(3) and (b)(3) to remove the narrative justification and description requirement so that the regulatory language simply requires that an issuer include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. As stated above, we believe that continuing to collect contract negotiation status data from issuers is essential for performing ECP certification reviews. We stated that not only does this data allow us to monitor an issuer's progress toward contracting with a specific ECP and learn the rationale for why an issuer has yet to offer a contract with a specific ECP, the type of contract negotiation status an issuer selects for an ECP also determines whether the issuer will receive credit for that ECP toward satisfaction of the threshold, category per county, and Indian health care requirements under the ECP Standard. For example, if an issuer designates that an ECP rejected their contract offer in MPMS as part of their QHP application, the issuer will receive credit towards their efforts to offer a contract despite it being rejected as part of the calculations for the category per county and Indian health care requirements under § 156.235(a)(2)(ii), but will not receive credit as part of the calculations for the threshold requirements under § 156.235(a)(2)(i) and (b)(2)(i), which require that contract offers be fully executed with an ECP to receive credit. We stated that overall, collecting these contract statuses within the ECP UI in MPMS has allowed us to conduct ECP certification reviews that are as fulsome as certification reviews informed by narrative justifications, since the same information previously collected through narrative justifications is still received within MPMS but submitted by issuers in a simplified format through pre-populated contract status options that reduces issuer burden without written narratives required.
Moreover, we stated that this data had previously been collected through ECP narrative justifications, but the ECP UI enhancement now allows us to gather this information from issuers in a simplified and standardized format through various pre-populated fields, which eliminates the need for issuers to provide open-ended written descriptions that may be more time consuming for issuers that are continuing to work toward satisfaction of the ECP standard. In the ECP UI, this data is mainly collected from the status of contract negotiations. For example, the issuer could designate in its QHP application the contract negotiation status with an ECP for its networks by selecting if a contract was executed, a contract offer was made and awaiting a response, or a contract was not offered due to no response following issuer outreach, as some of the available standardized options.[322]
To reflect collecting this type of information as part of ECP certification reviews, we proposed to revise the regulations at § 156.235(a)(3) and (b)(3) to state that a network plan applying for QHP certification to be offered through a FFE must include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. We noted that since issuers have already been including this information as part of their QHP applications since PY 2025, there would be no substantive operational changes as a result of this proposal to the ECP data submission process as part of QHP certification.
Additionally, we noted that issuers are not required to designate the contract negotiation status for all available ECPs within their service area in their QHP application. We stated that we understand the total number of ECPs
( printed page 29747)
for which a contract negotiation status is selected within each network and service area is variable among issuers for multiple factors, including the size of the issuer's service area, the number of qualified ECPs available in the service area, the number of ECPs the issuer has contacted and/or engaged in contract discussions with, resources required by the issuer to initiate contract discussions with all qualified ECPs in their service area, if an issuer finds evidence that an ECP may no longer be eligible to qualify as an ECP, and the number of ECPs an issuer must contract with to achieve each of the requirements of the ECP standard. For these reasons, we proposed to additionally clarify at § 156.235(a)(3) and (b)(3) that a network plan does not need to report on the status of contract negotiations for all available ECPs in their service area, but must at least report on the status of contract offers for all ECPs which the issuer has either included in its network plan or offered a contract to be included in its network plan within each service area.
We sought comment on this proposal to modify the existing narrative justification requirement to be consistent with current ECP data submission requirements as part of QHP certification.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on this proposal below.
Comment:
Overall, commenters provided mixed opinions on our proposal to remove the narrative justification requirement. Issuers agreed with our proposal since the proposed modifications to the regulation text to instead designate that an issuer should include as part of its QHP application the status of contract offers to qualified ECPs would be more consistent with current ECP data submission processes within MPMS. However, multiple commenters stated concerns that modifying this requirement would remove pathways to ensure issuers justify how the plan's network would protect access to care and provide an adequate level of service for low-income enrollees or individuals in Health Professional Shortage Areas, leading to diminished transparency and accountability mechanisms, less meaningful enforcement, and would allow certification of plans that do not actually meet ECP requirements. Furthermore, commenters stated that narrative justifications compel issuers to articulate an access strategy that would provide regulators qualitative data regarding whether their network design meaningfully serves low-income, medically underserved populations, which may not be captured through contract statuses.
Response:
We thank commenters for sharing their concerns with removing the narrative justification requirement to instead collect the status of contract offers. As we previously stated, MPMS allows us to collect the same type of information previously obtained from the narrative justification, such that issuers can easily submit their ECP data, including justification-related information previously collected through written narratives and pre-populated Excel templates. During QHP certification, issuers input additional information such as contract offer dates, point of contact information, and sources pertaining to a provider's potentially changed status if applicable, and can use additional notes to indicate why the issuer did not fully execute or offer a contract to an ECP. Thus, we do not agree with commenters that we would lose important data needed to meaningfully enforce ECP requirements, and we have taken steps to directly engage issuers to ensure their network design provides meaningful access to care to populations served by ECPs. Specifically, we have expanded outreach activities to issuers before, during, and post-certification through various informational QHP certification webinars, calls to issuers that require additional assistance, and compliance activities to ensure certain QHP issuers are actively taking steps to remedy any identified deficiencies in ECP requirements. These outreach efforts have been important to gather justification information by communicating directly with issuers that share any barriers to meeting ECP requirements and how the plan's provider networks provide an adequate level of service for low-income enrollees or individuals residing in Health Professional Shortage Areas within the plan's service area, while disseminating information on ECP certification requirements and providing targeted assistance to issuers in overcoming common barriers in developing networks to meet the ECP standard.
In addition to outreach efforts and MPMS modifications to collect justification-related information from issuers, we have implemented more widespread supports and resources that have effectively assisted issuers in meeting ECP requirements and reduced the number of issuers who have needed to submit detailed narratives for not meeting the ECP requirements under § 156.235. When we first codified narrative justification requirements at § 156.235(a)(3) and § 156.235(b)(3) in the 2016 Payment Notice (80 FR 10838), we stated that “[w]e expect the need for issuers to submit such [narrative] justifications to decrease over time as issuers further develop their networks in adherence to HHS standards.” Since then, we launched our ECP Annual Application and Renewal Form (formerly called “ECP Petition Site”) initiative on December of 2015 to allow providers the opportunity to request to be added to the HHS ECP List and update their provider data on the ECP List. We have actively maintained and strengthened the HHS ECP List since the establishment of this initiative by ensuring the list more actively reflects the universe of qualified available ECPs in each service area, conducting outreach to providers to verify their information, and confirming prospective providers satisfy certain criteria prior to receiving a qualified ECP status. These efforts have provided issuers with a useful resource to identify providers that qualify for inclusion in an QHP issuer's plan network toward satisfaction of the ECP standard under § 156.235, which has assisted more QHP issuers in meeting the ECP standard and decreasing the number of QHP issuers needing to submit narrative justifications. Therefore, we continue to believe that the proposed modifications to § 156.235(a)(3) and § 156.235(b)(3) are appropriate, and we are finalizing these modifications so that the regulatory language simply requires that an issuer include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area.
c. Implementation of an Effective Essential Community Provider (ECP) Review Program (§ 155.1051)
To align with proposals in sections III.D.18 and III.E.10 of the proposed rule that would provide FFE States with additional flexibilities to conduct their own network adequacy reviews of QHP issuers operating in their States as long as they have sufficient authority and the technical capacity to conduct these reviews, demonstrated by satisfying criteria established by HHS to be considered an Effective Provider Access Review Program, we proposed to adopt new flexibilities for FFE States to conduct ECP certification reviews of QHP issuers' plans in their States provided that the State is determined by HHS to have an Effective ECP Review Program, as discussed later in this section. In proposing flexibilities for
( printed page 29748)
FFE States to conduct ECP certification reviews, we proposed to exercise our authority under section 1311(c)(1)(C) of the Affordable Care Act, which provides the Secretary authority to establish QHP certification criteria related to ECPs, and our authority under section 1321(a)(1)(B) of the Affordable Care Act, which grants HHS general rulemaking authority to issue regulations related to offering QHPs through the Exchanges.
Thus, beginning with PY 2027, we proposed to provide the opportunity for FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of QHP issuers' plans provided that the State demonstrates it has sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria established by HHS to have an Effective ECP Review Program to ensure reasonable and timely access to ECPs for low-income, medically underserved individuals. We set forth this proposal at new § 155.1051.
Over the years, we have deferred network adequacy reviews of QHPs to FFE States that were determined to have a sufficient network adequacy review process (82 FR 18346, 83 FR 16930). In determining whether it was appropriate to defer network adequacy reviews to FFE States, we considered a States' legal authority to enforce network adequacy standards and conduct network adequacy reviews, the means to conduct assessments on the adequacy of plans' provider networks, and the ability of States to enforce minimum access standards established by HHS (for example, reasonable access standards defined under § 156.230). In contrast, we have not historically deferred ECP certification reviews wholly to FFE States, in part due to the complexity of conducting ECP certification reviews, which require sufficient technical capacity and resources that may not be readily available to States. However, as we stated in the proposed rule, given the prior experience of many FFE States in reviewing issuer submitted network adequacy data and some FFE States in reviewing ECP data (for example, States performing plan management), we believe it is appropriate to reconsider a FFE State's desire, legal authority, and technical capability to effectively conduct ECP certification reviews. We noted that some States performing plan management have experience conducting ECP certification reviews prior to PY 2026 due to previous data integration and system limitations that prevented HHS from being able to conduct these reviews before we implemented the ECP UI in MPMS, which eventually allowed us to effectively conduct these reviews for issuers operating in States performing plan management.
In the proposed rule, we recognized that States possess unique knowledge on local factors related to ECP reviews, such as on market conditions, geographic constraints, areas in the State with limited economic resources, provider shortages, workforce issues, and population demographics. We stated that the States' unique knowledge of these various local factors, in particular, could strengthen ECP certification reviews, which often involve identifying low-income areas and geographic areas with health professional shortages. We further stated that a State's local knowledge of low-income areas and geographic areas with health professional shortages within the State could effectively help locate facilities in these areas that may qualify as ECPs to both measure access to ECPs across the State and for possible inclusion of these ECPs within an issuer's network towards satisfaction of the ECP standard under § 156.235. Lastly, we stated that a State's unique knowledge of local factors may allow States to innovate their approach to conduct ECP certification reviews that are more sensitive and tailored to local conditions and provider capacity in the State. We noted, for example, that a State may choose to implement additional or alternative access standards for mental health facilities, a type of ECP, and consider these standards during ECP certification reviews if the State is experiencing many Mental Health Professional Shortage Areas that necessitate tailored approaches to ensure consumers have increased access to mental health facilities within their networks.
Additionally, we stated that we believe several States already have robust ECP requirements in place, including quantitative measures to oversee the number or percentage of ECPs included in an issuer's network operating in their State. We noted, for example, that a Government Accountability Office (GAO) report in 2022 found evidence that approximately 19 States reported having a quantitative standard for ECPs when reviewing individual and group plans.[323]
The example given in the report of a quantitative standard is that multiple States require that 35 percent of ECPs in a service area must be included in the plan's network, which is consistent with the current Federal ECP threshold requirement. Furthermore, we noted that we have developed and expanded resources over the years that have familiarized some States with our ECP certification review process and methodologies, including various ECP review tools and templates, the Final Plan Year ECP List which captures qualified ECPs in each State, sub-regulatory guidance published on the QHP certification website (for example, Frequently Asked Questions, QHP Application Materials for the ECP section), and webinars and office hours with States. We also stated that we discovered through interested party engagement and communications throughout the years that some States utilize the aforementioned ECP certification resources as a foundation for their State ECP List and/or State ECP requirements.
Lastly, we noted (91 FR 6402) that States have stated interest in the past for us to grant them with additional flexibility to conduct reviews of ECP data. For example, in response to our proposal in the 2026 Payment Notice proposed rule (90 FR 4506) to allow HHS to conduct ECP certification reviews of QHP issuers in States performing plan management, one State that operates a State Exchange stated that each State's market demands tailored approaches to meet their unique needs, which may be more effectively addressed through State-level decision making and reviews of issuer-submitted ECP data.
For all these reasons, we stated that we believe FFE States may have the legal authority, technical capacity, expertise, and interest to conduct their own ECP certification reviews. Thus, beginning PY 2027 and thereafter, we proposed to allow FFE States, including States performing plan management, to elect to perform their own State reviews of issuer-submitted ECP data provided the State demonstrates sufficient authority and technical capacity by meeting the applicable criteria, as determined by HHS, to have an Effective ECP Review Program. We stated that an FFE State would be granted an Effective ECP Review Program designation if we determine it meets all applicable requirements described for this program under proposed § 155.1051. We stated that we believed establishing applicable requirements under proposed § 155.1051 for FFE States to demonstrate they have an Effective ECP Review Program is necessary to ensure States have the authority and technical capacity to conduct these ECP certification reviews in a way that
( printed page 29749)
continues to ensure consumers have adequate access to ECPs through their plans. We stated that if we determined that an FFE State does not have an Effective ECP Review Program, then we would continue to perform ECP certification reviews consistent with § 156.235 for network plans.
We stated that we continued to believe that HHS should continue to primarily conduct ECP certification reviews as the default approach for issuers' plans applying for certification to be offered as QHPs through an FFE, including States performing plan management, except if an FFE State elects to conduct ECP certification reviews and is determined to have sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective ECP Review Program. We stated that we believed Federal ECP certification reviews are highly valuable for several reasons.
First, we noted (91 FR 6403) that ECPs serve predominately low-income, medically underserved individuals, and these populations often experience higher rates of illness and are less equipped to field high out-of-pocket costs; additionally, the services furnished by ECP facilities are often more highly specialized with greater levels of acuity and expense,[324]
such as cancer care at Free-Standing Cancer Centers, Black Lung Disease treatment at Black Lung Clinics, tuberculosis treatment at Tuberculosis Clinics, hemophilia treatment at Hemophilia Treatment Centers, HIV/AIDs treatment with Ryan White Providers, and more. We stated that altogether, centralized Federal ECP certification reviews are continuously valuable to perform complex analyses that aim to protect these more vulnerable populations and decrease potential disparities in access across States.
Second, we stated that while we were aware of many States that have qualitative and/or quantitative network adequacy regulatory standards that are comparable to standards under § 156.230 (including with respect to time and distance and appointment wait time requirements) and experience conducting such reviews, less is known about to what extent States may have different and separate requirements for ECPs, integrate ECP and network adequacy requirements together under one standard, or do not have standalone ECP requirements at all. For this reason, we stated that we believed HHS retaining primary responsibility over conducting ECP certification reviews as the default approach is appropriate, at least until we learn additional information from FFE States on their ECP requirements as part of the Effective ECP Review Program determination process. To broaden knowledge on this issue, we solicited comments on different ways that FFE States, including States performing plan management, currently implement State-specific requirements for ECP standards and how these requirements may be comparable to or different from ECP requirements implemented at § 156.235.
Third, we stated that through interested party engagement throughout the years, we are also aware that some State Departments of Insurance may have limited resources and bandwidth to conduct ECP certification reviews, which are highly complex and data intensive. We stated that in the past, these State Departments of Insurance supported HHS conducting ECP certification reviews due to State resource limitations. We further stated that we have expanded our data collection capabilities and means to efficiently and adequately conduct ECP certification reviews over the years, such as through the development of the ECP List [325]
and ECP data collection in MPMS. The ECP List has helped us identify the exact geographic location and distribution of ECPs to highlight specific ECPs that may be available within an issuer's service area and available for contracting with the issuer to satisfy ECP requirements under § 156.235. And, use of the ECP List simultaneously ensures that the full range of different ECP categories defined in section 340B(a)(4) of the PHS Act and, for network plans, providers described in section 1927(c)(1)(D)(i)(IV) of the Social Security Act, are adequately represented and available to consumers in an issuer's network. We noted that this ECP List has been embedded within the ECP UI in MPMS, so QHP issuers can select specific ECPs from this list that are contracted with the issuer and included in their network within a particular service area, which allows us to calculate an issuer's satisfaction toward the ECP threshold, ECP category per county, and ECP Indian health care requirements. Based on our experience conducting ECP certification reviews, we maintained that having adequate and accurate data on available ECPs in a geographic area, sufficient tools to collect and calculate issuer submitted ECP data, and sound methodologies to quantitatively assess this data to determine reasonable and timely access to ECPs in accordance with section 1311(c)(1)(C) of the Affordable Care Act is crucial for any FFE State to demonstrate the technical capacity to conduct their own ECP certification reviews. We noted that outside of a couple of State Exchanges that have reached out annually to inquire about our ECP List and a couple of States that have shared that they keep their own State-specific list of available ECPs, it is unknown how many States can develop and maintain a similar State-specific list of qualified ECPs or utilize HHS' ECP List that can be applied to conduct their own ECP certification reviews of issuer-submitted ECP data. We further noted (91 FR 6404) that it is also unknown what tools States may currently utilize to collect issuer submitted ECP data and methodologies States apply to assess this data to demonstrate reasonable and timely access to ECPs. For these reasons, too, we stated we believe it is appropriate that HHS retain primary responsibility over conducting ECP certification reviews as the default approach, at least until we learn additional information from FFE States as part of the Effective ECP Review Program determination process. We stated that this additional information would include whether FFE States have a process to identify qualified ECPs “where available” that may be included within a network plan's provider network, tools to collect issuer-submitted ECP data, and methodologies to assess the adequacy of an issuer's network of ECPs. Additionally, to broaden our knowledge in this area, we sought comment to learn which States have their own ECP List or other related process to identify qualified ECPs that may be utilized for certification purposes.
Accordingly, we proposed to set forth the criteria for an Effective ECP Review Program by adding § 155.1051 to part
( printed page 29750)
155, subpart K. Under § 155.1051(a), we proposed that FFE States may elect to conduct their own ECP certification reviews of issuers' plans applying for certification to be offered as QHPs through an FFE, including States performing plan management, provided that the State demonstrates sufficient authority and technical capacity to conduct these reviews by satisfying the applicable criteria in proposed § 155.1051. We proposed that if FFE States do not satisfy the criteria established in proposed § 155.1051, then we would continue to perform ECP certification reviews consistent with § 156.235 for network plans.
In alignment with the proposal in section III.E.12. of the proposed rule to allow plans that do not use a network (non-network plans) to receive QHP certification, we stated that we would also provide additional flexibilities to FFE States to conduct ECP certification reviews of non-network plans if they are determined to have an Effective ECP Review Program. We further stated that, similar to the approach for network plans, we would perform ECP certification reviews for non-network plans under proposed § 156.236 if FFE States do not satisfy criteria for having an Effective ECP Review Program. We stated that an FFE State would need to demonstrate that it meets applicable criteria for both network plans and non-network plans (under proposed § 155.1051(b) through (c)), and the sufficient authority and technical capacity to conduct reviews of such plans (as assessed under proposed § 155.1051(e)), if they decide to certify non-network plans, to receive a designation as having an Effective ECP Review Program. We also stated that this would mean an FFE State would not be permitted to elect to conduct ECP certification reviews for only network plans and not non-network plans, if they certify non-network plans, or vice versa. However, we stated that if an FFE State notifies us that it does not intend to certify non-network plans within their State and consequently does not offer these plans to consumers on the FFEs operating in their State altogether (regardless of if the State or HHS would conduct ECP certification reviews), then we would continue to review whether an FFE State meets all applicable criteria for only network plans during the Effective ECP Review Program determination process. For additional details regarding the criteria for the Effective ECP Review Program under proposed § 155.1051 and how these criteria would pertain to reviews of non-network plans in FFE States electing to conduct ECP certification reviews, we referred readers to the discussion under sections III.D.19 and III.E.12.e of the proposed rule.
Furthermore, to ensure that issuers in FFE States continue to meet ECP requirements issued under section 1311(c)(1)(C) of the Affordable Care Act, and consistent with § 156.235 for network plans, we proposed in § 155.1051(b) that FFE States with an Effective ECP Review Program must ensure that a QHP issuer with a provider network includes in its provider network a sufficient number and geographic distribution of ECPs, where available, to ensure reasonable and timely access to a broad range of such providers for low-income individuals or individuals residing in Health Professional Shortage Areas within the QHP's service area, in accordance with the Exchange's network adequacy standards. Furthermore, we stated that we continue to believe that to protect low-income, medically underserved populations, and to ensure that enrollees in all FFEs have a minimum standard for consumer protections on reasonable access to providers and that disparities in access are minimized across FFE States, issuers in FFE States with an Effective ECP Review Programs must continue to demonstrate that they meet State requirements to ensure reasonable and timely access to ECPs that are consistent with requirements of the ECP Standard under § 156.235. Thus, we proposed in § 155.1051(c) that FFE States with an Effective ECP Review Program must have established ECP requirements that are set forth in State statute or regulation. We stated that FFE States must demonstrate that these established ECP requirements ensure that issuers with a provider network in their State meet all of the following requirements that promote a sufficient number and geographic distribution of ECPs: the minimum percentage requirements under § 156.235(a)(2)(i), the Indian health care provider requirement under § 156.235(a)(2)(ii)(A), and the category per county requirements for each of the eight ECP category types described under § 156.235(a)(2)(ii)(B). In this manner, we stated that we believe that FFE States having ECP requirements consistent with the three aforementioned requirements would help maintain access to ECPs.
However, we recognized that FFE States may have alternative, distinct ECP requirements to ensure a sufficient number and geographic distribution of ECPs are included within an issuer's network to address various local conditions unique to each State. We stated, for example, some FFE States may have time and distance requirements that issuers must satisfy for enrollees to access certain types of ECPs; some FFE States may have different minimum percentage requirements than those described under § 156.235(a)(2)(i),[326]
such as minimum percentages for rural health providers, mental health facilities, or other types of ECP facilities; and some FFE States may have ECP facility to enrollee ratio requirements, which may require an issuer to contract with a certain number or categories of ECPs based on the number of enrollees enrolled in their plan (for example, 1 FQHC per 1,000 enrollees). We acknowledged (91 FR 6404) that there could be numerous quantitative and qualitative methods beyond these aforementioned examples that States may use to analyze access to ECPs, which may especially be influenced by factors unique to each State. We stated that, for these reasons, FFE States with alternative ECP requirements would be required to demonstrate how these requirements would promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs, and an adequate level of service for low-income enrollees or individuals residing in Health Professional Shortage Areas under § 155.1051(d). We further stated that to assess an FFE State's satisfaction of the requirements in proposed § 155.1051(d), we would require FFE States to submit a written description of their alternative ECP requirements, an explanation of how the State collects ECP data from issuers to measure compliance with the alternative ECP requirement, and a detailed explanation of how the State uses this ECP data to analyze access to ECPs within an issuer's network.
In addition, we stated that for an FFE State to conduct ECP certification reviews, under our proposal, the FFE State would need to first express its interest to HHS and submit an attestation for having an Effective ECP Review Program. We stated that an FFE State would have the choice to submit an attestation for an Effective ECP Review Program, Effective Provider Access Review Program (described in section III.E.10. of the proposed rule), or both. We further stated that this means that an FFE State can elect to conduct their own ECP certification reviews, provider access certification reviews, or
( printed page 29751)
both reviews provided the State demonstrates that it has sufficient authority and the technical capacity by satisfying the applicable criteria for the applicable review program depending on which review(s) it wishes to conduct. We proposed that if an FFE State does not directly communicate to HHS its interest in conducting its own ECP certification reviews, then we would assume the FFE State prefers that we continue conducting these reviews. We also stated that FFE States with an interest in conducting their own ECP certification reviews would need to submit their attestation that the State has an Effective ECP Review Program prior to the start of the QHP certification cycle for the first plan year it wishes to assume responsibility to conduct ECP certification reviews. We stated that we would review information submitted by the FFE State to ensure the State has the authority and technical capacity to conduct effective, timely reviews of ECP data submitted by an issuer prior to each plan year's QHP certification cycle. We noted that in our review, we would consider whether the FFE State receives adequate issuer data and documentation sufficient to conduct an examination of ECP requirements described in § 156.235 for network plans. For additional details regarding the proposed criteria for the Effective ECP Review Program under proposed § 155.1051 and how these criteria would pertain to reviews of non-network plans in FFE States electing to conduct ECP certification reviews, we referred readers to the discussion under sections III.D.19 and III.E.12.e of the proposed rule. We proposed in § 155.1051(e)(1) through (10) that we would consider the following factors in our review to determine if an FFE State has an Effective ECP Review Program: [327]
(1) The State's legal authority to review whether plans applying for QHP certification meet ECP requirements, including relevant State regulations and statutes;
(2) Evidence that the State's requirements are consistent with ECP requirements under proposed § 155.1051(c)(1) through (c)(3) that promote a sufficient number and geographic distribution of ECPs, or the State's explanation of how its alternative ECP requirements promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs;
(3) A description of the State's definition of an ECP, if different from the definition under § 156.235(c), including relevant categories and eligibility criteria that the State uses to determine whether a facility qualifies as an ECP;
(4) Whether the State utilizes the Federal ECP List or has a process it uses to identify qualified ECPs that may be included within a network plan's provider network;
(5) Whether the State utilizes the Federal ECP List or has a process it uses to identify qualified ECPs that may accept a non-network plan's benefit amount as payment in full;
(6) A description of data collection systems, resources, templates, or methodologies used by the State to collect and review ECP data;
(7) Whether the State generally collects information from QHP issuers regarding the status of contract offers for network plans or offers of benefit amounts as payment in full to an ECP for non-network plans;
(8) Whether the State has delegated authority to some other entity other than the State Department of Insurance to perform ECP any or all review activities;
(9) Whether the State has compliance reviews, follow-up procedures, and enforcement frameworks applicable to issuers that demonstrate inadequate networks of ECPs so that those issuers come into compliance with State ECP requirements, including standardized processes to assess efforts the issuer is pursuing to come into compliance with State ECP requirements and any justification and exception processes for issuers that have not yet or cannot meet ECP requirements;
(10) Whether the State has a process for monitoring and addressing consumer-related complaints regarding access to ECPs to ensure sufficient access to ECPs consistent with section 1311(c)(1)(C) of the Affordable Care Act and set forth in State statute.
The first proposed factor under § 155.1051(e)(1) requires that the FFE State has established ECP requirements that are set forth in State statute or regulation. We stated (91 FR 6405) that this factor is crucial since it identifies whether the FFE State has sufficient legal authority to issue regulations to establish ECP requirements, and that it has the authority to conduct ECP certification reviews to ensure QHP issuers meet such requirements.
The second proposed factor under § 155.1051(e)(2) requires evidence that the FFE State's ECP requirements are consistent with ECP requirements under proposed § 155.1051(c)(1) through (c)(3) that promote a sufficient number and geographic distribution of ECPs, or the FFE State provides a rationale to describe how its alternative State ECP requirements promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs. We stated that this factor is important to ensure that an FFE State's requirements are consistent with those under § 156.235 for network plans and under proposed § 156.236 for non-network plans, so that these requirements continue to maintain access to ECPs especially if they differ from those ECP requirements under § 156.235 and proposed § 156.236.
The third proposed factor under § 155.1051(e)(3) considers the FFE State's definition of an ECP, if different from the definition under § 156.235(c), and relevant categories and eligibility criteria that the FFE State uses to determine whether a facility qualifies as an ECP. We stated that this factor acknowledges that FFE States may have different categories of ECPs compared to those described under § 156.235(c), including that some FFE States may have chosen to expand the categories of facilities that may qualify to be an ECP in the State. We stated that an understanding of the FFE State's definition of an ECP is necessary to ensure the State satisfies statutory requirements under section 1311(c)(1)(C) of the Affordable Care Act which requires the Secretary to issue regulations to ensure QHPs include within their networks certain categories of ECPs, such as those specified in section 340B(a)(4) of the PHS Act and entities described in section 1927(c)(1)(D)(i)(IV) of the Act.
The fourth and fifth proposed factors under § 155.1051(e)(4) and (e)(5) evaluate an FFE State's process to identify qualified ECPs that may be included within a network plan's provider network, or qualified ECPs that accept a non-network plan's benefit amount as payment in full, respectively; or whether it utilizes the Federal ECP List to identify qualified ECPs. As stated in the discussions above, we stated that we believe it is critical for the FFE State to have a process to identify qualified ECPs, “where available.” We stated that understanding whether the FFE State utilizes the Federal ECP List or has its own process to identify qualified ECPs is crucial to evaluate the FFE State's satisfaction of the requirements under section 1311(c)(1)(C) of the Affordable Care Act which requires the Secretary to issue regulations to ensure QHP issuers include within health insurance plan networks those ECPs, “where available,” that serve predominately low-income, medically underserved individuals. We also stated that an FFE State implementing a process to identify qualified ECPs, or even the FFE State's
( printed page 29752)
utilization of the Federal ECP List, would allow the State to identify the exact geographic location and distribution of ECPs to highlight specific ECPs that may be available within an issuer's service area and available for contracting with the issuer to satisfy ECP requirements. And we stated that if the FFE State identifies the category of services an ECP provides when identifying the qualified ECP, it can simultaneously ensure that the full range of different ECP categories defined in section 340B(a)(4) of the PHS Act and providers described in section 1927(c)(1)(D)(i)(IV) of the Social Security Act is adequately represented and available to consumers in an issuer's network.
The sixth proposed factor under § 155.1051(e)(6) considers if the FFE State has data collection systems, resources, templates, or methodologies to collect and review ECP data. We stated that this information would be important for HHS to understand processes a FFE State has in place to efficiently collect large, complex amounts of an issuer's ECP data and their ability to meaningfully leverage that data to apply assessment methodologies to measure access to ECPs across the State. We also stated that this information would offer additional evidence to demonstrate an FFE State's technical capacity by indicating the different documentation, resources, and expertise it has developed to have the means to conduct an effective, timely examination of ECP data.
The seventh proposed factor under § 155.1051(e)(7) considers if the FFE State collects information from QHP issuers regarding the status of contract offers for network plans or offers of benefit amounts as payment in full to an ECP for non-network plans. We stated that we believe this type of ECP data is important for an FFE State to collect from QHP issuers during its assessment of the adequacy of an issuer's network of ECPs or during its assessment to ensure access to a sufficient choice of ECPs that would accept a non-network plan's benefit amount in full. We stated that an FFE State collecting this type of data would demonstrate that it has the technical capacity to validate a QHP issuer's progress towards contracting with ECPs, which allows the FFE State to track an issuer's effort in pursuing to build a sufficient network of ECPs so that consumers in network plans have reasonable and timely access to a broad range of ECPs. Similarly, we stated that an FFE State collecting data from QHP issuers with non-network plans regarding the status of offering benefit amounts as payment in full to ECPs would allow the State to assess the issuer's commitment to facilitating access to a sufficient number of ECPs that an enrollee can access in their service area without needing to pay charges in excess of the benefit amount for an array of services. We stated that these contract statuses would serve as important metrics during an FFE State's assessment of ensuring access to ECPs, where available, including by allowing States to measure an issuer's compliance with the minimum threshold percentage, category per county, and Indian health care requirements under proposed § 156.236(b)(1) through (b)(3), which would be evaluated based on measurements of contracts offered or executed, and benefit amounts as payment in full that were offered to or accepted by an ECP.
The eighth proposed factor under § 155.1051(e)(8) considers whether the FFE State has delegated authority to some other entity other than the State Department of Insurance to perform any or all ECP review activities. We stated that it would be important for an FFE State to report to us any delegated authority to other entities to perform ECP review activities, so we understand how the FFE State is handling ECP review data and to whom it entrusts such data. In addition, we stated that it is important to review whether entities conducting such reviews have sufficient expertise to competently handle ECP reviews and that these entities would be able to conduct ECP reviews in such a way that would allow the FFE State to still satisfy all applicable criteria in proposed § 155.1051 as part of having an Effective ECP Review Program.
The ninth proposed factor under § 155.1051(e)(9) considers whether the FFE State has compliance reviews, follow-up procedures, and enforcement frameworks applicable to issuers that demonstrate inadequate networks of ECPs or inadequate access to ECPs that accept benefit amounts as payment in full, so that those issuers come into compliance with State ECP requirements. We stated that this factor would also consider whether the FFE State has standardized processes to assess efforts the issuer is pursuing to come into compliance with State ECP requirements and any justification and exception processes for issuers that have not yet or cannot meet ECP requirements. We explained that we believe the existence of these processes is critical for an FFE State to demonstrate sufficient enforcement authority, while maintaining the ability to evaluate the integrity and outcome of ECP certification reviews, which aims to ensure that low-income, medically underserved populations traditionally served by ECPs have sufficient access to these ECPs through their plans, where available. We stated that overall, these processes would ensure an FFE State has the ability to require that QHP issuers continue to meet state ECP requirements and comply with ECP statutory requirements under section 1311(c)(1)(C) of the Affordable Care Act.
The tenth proposed factor under § 155.1051(e)(10) considers whether the FFE State has a process for monitoring and addressing consumer-related complaints regarding access to ECPs to ensure sufficient access to ECPs consistent with section 1311(c)(1)(C) of the Affordable Care Act and as set forth in State statute. We stated that this factor is important since it would indicate the FFE State has a process to continuously monitor access to ECPs and ensure that State ECP requirements aimed to promote access to ECPs have their intended effect among consumers. We noted that access to ECPs can change during the year for a multitude of factors, including due to facility closures, network terminations, changes in services offered by ECPs, financial stability and funding reductions, and staffing shortages. We further noted that for plans using a provider network, contracts may be executed or terminated throughout a plan year for various reasons. Also, we stated that any inaccuracies or out-of-date information contained in provider directories can create confusion or be misleading to consumers. Additionally, we stated that consumers may have trouble making appointments with network providers due to lack of availability of appointments. We also stated that for plans without a provider network, we anticipate that ECPs that accept a benefit amount as payment in full could change depending on market conditions, negotiations, and competition, or that consumers may require additional assistance in understanding how to utilize plan benefit amounts to meet their health care needs in such a way that does not increase out-of-pocket costs beyond the plan's benefit amount.
Lastly, in § 155.1051(f), we proposed that we would notify the FFE State electing to conduct ECP certification reviews of our decision in writing prior to the start of the QHP certification cycle whether the FFE State is determined to have an Effective ECP Review Program and can therefore conduct its own ECP certification reviews for the plan year. We stated that in subsequent years and prior to the
( printed page 29753)
start of the QHP certification cycle each year, we would reach out to FFE States with an Effective ECP Review Program designation to confirm if the FFE States wish to continue conducting their own ECP certification reviews for the upcoming plan year and to verify if any circumstances have changed that may affect an FFE State's authority and technical capacity to continue conducting effective, timely reviews of ECP data. We proposed that we would reserve the right to evaluate the FFE State at any time to determine whether, and to what extent, the FFE State's circumstances have changed such that it has begun to or has ceased to satisfy the criteria established by HHS under proposed § 155.1051, and consequently no longer has an Effective ECP Review Program. We noted that we often complete an annual environmental scan of State authorities to maintain situational awareness of changing authorities across FFE States, and stated that the same would apply to this proposal to ensure FFE States with an Effective ECP Review Program continue to satisfy all applicable Federal requirements.
Additionally, we clarified that we would be available to provide technical assistance to FFE States on any issues related to the Effective ECP Review Program. We stated that we remain open to assisting FFE States at any point of the process, from electing to conduct their own ECP certification reviews to performing ECP certification reviews as an Effective ECP Review Program State, to ensure an FFE State's ECP requirements and certification review process continue to protect access to ECPs for low-income, medically underserved populations. We further stated that we would also continue to make ECP resources publicly available, including for those FFE States that are determined to have an Effective ECP Review Program and wish to utilize these resources as part of their ECP certification reviews. We noted that these resources include the Final Plan Year ECP List and Rolling Draft ECP List, medical QHP and SADP ECP tools, the Available ECP Write-in List, the Plan Validation workspace in MPMS, and guidance on the QHP certification website.[328]
We stated that we believe these supporting documents and tools are widely used across many States and among many issuers, serving as important resources for both identifying ECPs nationally to potentially include in a plan's network and assisting issuers in meeting ECP requirements.
We further stated (91 FR 6407) that in addition to the aforementioned resources and technical assistance that we would provide to FFE States, we would continue collecting ECP data from FFE issuers in FFE States with an Effective ECP Review Program, similar to the proposed approach for network adequacy in section III.E.10. of the proposed rule. We stated that we believe this data would provide additional insight to assess how QHP issuers are performing across the FFE, including in FFE States with an Effective ECP Review Program, to consistently compare issuer performance. We further stated that collecting this data would also provide us with the ability to continue to monitor consumer access to ECPs across the FFE. We also stated that the data would also be available in a standardized format to FFE States with an Effective ECP Review Program, which could be utilized to inform their ECP certification reviews and to perform additional analyses to analyze access to ECPs across the State. We stated that we believe this proposed approach would support FFE States in their capacity to conduct these complex ECP reviews.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy with modifications. Specifically, as discussed in section III.E.12. of this final rule, we are delaying implementation of QHP certification of non-network plans to PY 2028, which means that we will also delay implementation of the provisions allowing FFE States with an Effective ECP Review Program to conduct ECP certification reviews for non-network plans under § 155.1051. Also, in response to comments, we are finalizing adding § 155.1051(e)(11) to state that, in our review to determine if an FFE State has an Effective ECP Review Program, we will consider whether the FFE State collects the information described under § 156.236(b)(4) through (b)(9) from non-network plans, which issuers of non-network plans must submit to the FFE for a determination that the plan provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full. We refer readers to section III.E.12.e. of this final rule where we discuss and respond to a comment regarding QHP certification of non-network plans and ECP certification reviews of non-network plans by FFE States with an Effective ECP Review Program.
In the sections below, we summarize and respond to public comments received on the proposals above to allow FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of QHP issuers' plans provided that the State demonstrates it has sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria established by HHS to have an Effective ECP Review Program under § 155.1051.
Comment:
Commenters stated different perspectives on whether HHS should allow FFE States to conduct their own ECP certification reviews. Multiple commenters stated concerns that allowing FFE States to conduct their own ECP certification reviews would create inconsistency and variability in the application and enforcement of ECP requirements across FFE States, leading to a “patchwork” of varying ECP criteria, especially if FFE States are permitted to establish different ECP requirements. Some commenters stated that States may lack the resources and ability to establish their own review processes, and that CMS has much greater ECP data collection and analytical capacity than States, including to ensure compliance with section 1311(c)(1)(C) of the Affordable Care Act. One issuer recommended that CMS continue to perform ECP certification reviews since shifting these reviews to additional reviewing entities (for example, State Departments of Insurance) could increase administrative complexity for issuers and necessitate additional resources for issuers to manage varying Federal and State processes and timelines. Another commenter requested that, since ECP certification reviews are data-intensive and complex, HHS should not finalize this proposal and revisit this topic when more information can be gathered regarding the existing landscape of ECP requirements across States, including existing FFE State authority and technical capacity.
In contrast, multiple commenters stated that States are best positioned to assess access to ECPs within an issuer's network, and that States possess special insight on local markets, community needs, provider availability, and geographic conditions relevant to performing ECP certification reviews. Commenters also noted that proximity makes States best suited to design ECP requirements that address the specific needs of consumers; and that geographic distribution of ECPs varies significantly across States, so States have the expertise to evaluate whether issuers are
( printed page 29754)
meeting the needs of low-income, medically underserved individuals within their jurisdictions. Lastly, commenters supported HHS continuing to conduct ECP certification reviews for FFE States that do not elect to conduct their own reviews, or for those that do not satisfy all requirements under proposed § 155.1051.
Nevertheless, the majority of commenters agreed that if FFE States are permitted to conduct ECP certification reviews, it would be essential to ensure Federal oversight of FFE States conducting ECP reviews and to establish clearly-defined, minimum requirements that FFE States must satisfy to demonstrate having an Effective ECP Review Program, which would promote consistent access to ECPs across FFE States and preserve consumer protections. These commenters stated that this Federal oversight includes HHS determining that FFE States demonstrate sufficient authority and the technical capacity to have an Effective ECP Review Program. One commenter noted that States being well-suited to now conduct ECP certification reviews as an Effective ECP Review Program is rooted in the establishment of Federal ECP requirements that have been strengthened through years of rulemaking and refined implementation. The commenter stated that the establishment of robust Federal ECP requirements over time has provided an acceptable model for States to understand best practices for formulating ECP requirements and ensuring that issuers meet these requirements, now setting States up for success to have autonomy over ECP certification reviews. The commenter further added that State flexibility, combined with a defined, minimum Federal standard are complementary, not incompatible.
Response:
We thank commenters for providing valuable feedback on this proposal. We understand commenters' concerns regarding the potential for inconsistency and variability in the application and enforcement of ECP requirements across FFE States if FFE States conduct their own ECP certification reviews, which could cause differential access to ECPs across FFE States. However, we do not believe a one-size-fits all approach, by solely implementing HHS' review processes and standards, is the most effective approach to ensure access to ECPs; rather, some variability in FFE State requirements and certification review processes are valuable. FFE States with an Effective ECP Review Program will have flexibility under our policy as finalized in this rule to tailor their ECP review processes to address local ECP access by taking into account various conditions unique to each FFE State during reviews to maximize consumer impact, including geographic constraints, areas in the State with limited economic resources, provider shortages, workforce issues, and population demographics. For example, an FFE State that has numerous rural counties with significant Mental Health Professional Shortage Areas may consider adding additional types of mental health ECP facilities to its definition of mental health facilities to incentivize issuers to add more mental health facility types to their network to satisfy ECP requirements (including category per county requirements for mental health facilities).
In response to commenters that remain concerned about a “patchwork” of ECP requirements across the FFE if FFE States implement alternative ECP requirements, we believe that our proposal establishes a Federal floor of baseline ECP requirements that apply across the FFE to ensure reasonable consumer access across FFE States, even if FFE States have different ECP certification review processes or requirements. In particular, we remind commenters that under § 155.1051(c) through (e), during HHS' evaluation of whether an FFE State has an Effective ECP Review Program, HHS will closely examine whether FFE State ECP requirements and processes differ from those on the Federal level, and analyze whether identified differences will continue to promote a sufficient number and geographic distribution of ECPs or even strengthen access to ECPs. In addition, to help reduce potential variability in ECP access across FFE States if FFE States conduct ECP certification reviews, we proposed to continue collecting ECP data from issuers in FFE States with an Effective ECP Review Program. As we stated, this would help ensure we can continue to compare QHP issuer performance across the FFE, so that we can monitor consumer access to ECPs across the FFE and take additional actions if disparities emerge that could endanger consumer access.
Additionally, we recognize commenters' concerns that not all FFE States may possess the resources and ability to conduct ECP certification reviews. If we were to find during the Effective ECP Review Program determination process that an electing FFE State does not demonstrate sufficient authority and technical capacity to conduct ECP reviews due to insufficient resources and processes, then we would not permit the FFE State to conduct its own ECP certification reviews.
Furthermore, regarding concerns that this proposal may create additional administrative complexity and burden among issuers, we will continue to collaborate with FFE States approved to conduct their own ECP certification reviews to promptly communicate important information to QHP issuers and make resources widely available to facilitate a less burdensome, clear, and seamless QHP certification process. To help mitigate this burden, we will also continue to make MPMS available to FFE States should they wish to utilize the ECP UI in MPMS for their ECP certification reviews, which may reduce issuer burden if issuers submit ECP data through a centralized platform.
Lastly, in regard to commenters' suggestion to revisit this proposal once more information is gathered from FFE States on their authority and technical capacity to conduct ECP certification reviews, we do not believe there is a risk to consumers if HHS finalizes this proposal with a PY 2027 effective date. This is because HHS will only allow FFE States to conduct ECP certification reviews if they satisfy all the requirements under proposed § 155.1051 to demonstrate they have an Effective ECP Review Program with the sufficient authority and the technical capacity needed to ensure access to ECPs is maintained or expanded for consumers enrolled in QHPs in the State. Also, we believe that the Effective ECP Review Program determination process will provide HHS a unique opportunity to learn more in-depth information from FFE States when electing States submit information to HHS to demonstrate having an Effective ECP Review Program, since this detailed information will provide HHS insight into the FFE States' ECP requirements and processes to enforce these requirements. In addition, we acknowledged in the proposed rule (91 FR 6402) that we had evidence to believe several States already have robust ECP requirements and review processes, and this was one of the reasons that we proposed to allow FFE States flexibility to conduct ECP certification reviews if determined to have an Effective ECP Review Program.
Furthermore, we agree with the majority of commenters that Federal oversight combined with a minimum, clearly defined Federal ECP baseline would be essential to ensure consistent access to ECPs across FFE States if FFE States were permitted to conduct their own ECP certification reviews. In fact, this proposal would effectively establish a robust Federal floor for minimum
( printed page 29755)
requirements across the FFEs that are consistent with existing Federal ECP requirements under § 156.235 and that FFE States must meet prior to conducting their own ECP certification reviews (consistent with § 155.1051(b) through (e)). Collectively, these requirements, in particular, would help ensure reasonable consumer access to ECPs across FFE States, and ensure that FFE States use similar well-founded and reliable processes for conducting ECP reviews.
Comment:
One commenter urged HHS to require FFE States conducting their own ECP certification reviews to incorporate relevant Indian health care provider requirements at § 156.235(a)(2)(ii)(A) that would require FFE States to establish ECP requirements that require issuers to offer contracts to all available Indian health care providers in the service area. In addition, this commenter stated concerns over HHS suggesting that it would provide FFE States with flexibility to develop alternative ECP requirements under proposed § 155.1051(d), especially if such alternative ECP requirements may not require QHP issuers to offer contracts to all Indian health care providers within the service area. The commenter was concerned that this may reduce consumer protections for American Indian/Alaskan Native enrollees and cause disparities in access across States. For this reason, the commenter requested that HHS modify § 155.1051(d) to include that FFE States with an Effective ECP Review Program cannot propose alternatives to the Indian health care provider requirement under § 156.235(a)(2)(ii)(A) for network plans and under § 156.236(b)(3) for non-network plans.
Response:
We agree with commenters that access to Indian health care providers must be maintained if FFE States conduct their own ECP certification reviews, as Indian health care providers are an important ECP facility category that provide essential services to tribal populations, including American Indian/Alaskan Native Exchange enrollees. Indian health care providers are one of the types of ECPs included under section 340B(a)(4) of the PHS Act and section 1927(c)(1)(D)(i)(IV) of the Social Security Act, as required under section 1311(c)(1)(C) of the Affordable Care Act. In this regard, FFE States must also comply with Federal statutory requirements to ensure access to Indian health care providers within a QHP issuer's provider network. Accordingly, we are finalizing the proposed requirement at § 155.1051(c)(2) that FFE States with an Effective ECP Review Program must have established ECP requirements set forth in State statute or regulation that ensure network plans meet Indian health care requirements under § 156.235(a)(2)(ii)(A) and non-network plans meet Indian health care requirements under § 156.236(b)(3).
Furthermore, in response to the concern that an FFE State's alternative ECP requirements may not require issuers to offer contracts to all available Indian health care providers in the service area, consistent with proposed § 155.1051(d), we assure the commenter that if FFE States do have alternative ECP requirements to those described under § 155.1051(c)(1) through (c)(3), including requirements that ensure network plans meet Indian health care requirements under § 156.235(a)(2)(ii)(A) that require issuers to offer contracts to all available Indian health care providers in the service area, FFE States must submit additional information to HHS. FFE States would need to describe these alternative ECP requirements, explain how the FFE State collects ECP data from issuers to measure compliance with the alternative ECP requirements, and include a detailed explanation of how the FFE State uses this ECP data to analyze access to ECPs within an issuer's network. During this review, we would assess how this alternative ECP requirement compares to existing Federal ECP requirements, especially as it relates to maintaining access to care for tribal populations. If we identify during this review that the FFE State possesses an alternative ECP requirement related to Indian health care providers, we will not consider the FFE State to have an Effective ECP Review Program if the alternative requirement does not promote a sufficient number and geographic distribution of Indian health care providers and is not adequate to at least maintain or strengthen access to Indian health care providers. If the FFE State is determined to have an Effective ECP Review Program and is permitted to conduct its own ECP certification reviews while also having alternative ECP requirements, we will continue to collect ECP data from QHP issuers in these FFE States. This ECP data will quantitatively assess that a QHP issuer offers contracts to all available Indian health care providers in its service area. If HHS were to identify trends that issuers in the FFE State have poorer performance related to ensuring access to Indian health care providers, HHS may determine that the FFE State has ceased to satisfy criteria under proposed § 155.1051(d) and, under § 155.1051(f), revoke its prior determination that the FFE State has an Effective ECP Review Program. While we do not intend to adopt the commenter's proposed regulation text modification at this time, if we identify disparities in access to Indian health care providers within an FFE State that has an alternative ECP requirement for Indian health care providers, we will consider additional actions to remedy these disparities, which could include future rulemaking, as applicable.
Comment:
One commenter urged HHS to strengthen its oversight of the FFE States' ECP review processes, including by ensuring these processes prioritize that vulnerable populations can depend on consistent, access to care.
Response:
We agree with the commenter that FFE States must ensure their ECP certification review processes ensure that vulnerable populations, such as low-income, medically underserved individuals typically served by ECPs, have a sufficient number and geographic distribution of ECPs within their plans to provide reasonable and timely access to care. For this reason, under § 155.1051(e)(6), we proposed that during our review to determine if an FFE State has an Effective ECP Review Program, we would consider the FFE State's description of data collection systems, resources, templates, or methodologies used by the State to collect and review ECP data. We believe that finalizing this factor will address the commenter's request to strengthen Federal oversight, as it will allow us to collect information from FFE States to ensure FFE States have sufficient ECP certification review processes, which we do not currently collect from FFE States. This factor is important for us to understand processes an FFE State has in place to efficiently collect large, complex amounts of an issuer's ECP data and its ability to meaningfully leverage that data to apply assessment methodologies to measure access to ECPs across the State. Lastly, we remind the commenter that we will continue to collect ECP data from issuers in FFE States with an Effective ECP Review Program. If upon analyzing this data, we observes inadequate access to ECPs within issuers' networks across the FFE State, we may re-examine the FFE State's review processes to determine if the State's assessment and data collection methodologies no longer effectively ensure that issuers maintain adequate access to ECPs in their networks.
Comment:
A few commenters requested clarifications related to operations associated with the Effective
( printed page 29756)
ECP Review Program determination process. Specifically, one commenter was unclear why HHS did not propose to codify regulatory text to explicitly state that an FFE State must submit an attestation for having an Effective ECP Review Program. The same commenter requested clarity on when HHS will make determinations on if an FFE State has an Effective ECP Review Program and when HHS will inform the FFE State. In addition, the same commenter wanted more information regarding the process for Effective ECP Review Program determinations, including if the FFE State may appeal HHS's decision if HHS determines the FFE State does not have an Effective ECP Review Program, if HHS can clarify circumstances that may cause HHS to conclude that an FFE State no longer has an Effective ECP Review Program, and if HHS can share an example of the attestation form for electing to have an Effective ECP Review Program.
Response:
We appreciate the commenter asking these additional questions. The regulatory text concerning the review process and applicable criteria FFE States must satisfy to have an Effective Essential Community Provider Review Program to conduct their own ECP reviews is at new § 155.1051, and we refer the commenter to the discussion in the proposed rule concerning the attestation form and related operational matters (91 FR 6405). Furthermore, after the publication of this final rule, we intend to notify FFE States about their flexibility to conduct ECP certification reviews and will provide FFE States with ample instructions on how to do so, including by providing an attestation form to FFE States through the Plan Management State Coordination email. We will provide FFE States time to complete the form, and after an FFE State completes this form, we will begin the determination process to assess if the FFE State meets all applicable criteria under § 155.1051 to be considered to have an Effective ECP Review Program. Afterwards, we will send notice of our decisions to FFE States on a rolling basis. The detailed timeline for the entirety of this process, including the deadline to submit the attestation form, and our targeted timeframe for completing our determination process will be communicated to FFE States through additional guidance. If an FFE State is identified as having an Effective ECP Review Program, we will permit the FFE State to immediately begin conducting ECP certification reviews and will coordinate with the FFE State to communicate to issuers that they will complete ECP certification reviews.
We do not intend to establish a formal appeal process at this time. We may consider this recommendation for future plan years, especially if FFE States state a need for an appeal process during the first plan year for PY 2027. Since we will remain available to FFE States throughout the determination process should the FFE State reach out to us for further assistance, we do not see a need to adopt an appeals process at this time. We will provide technical assistance to the FFE State should the State require more tailored feedback on how to expand its authority and technical capacity to demonstrate having an Effective ECP Review Program. If we determine that an FFE State did not adequately demonstrate having an Effective ECP Review Program, the FFE State may request to meet with us to request additional feedback. The FFE State may resubmit an updated attestation form to us to elect to conduct ECP certification reviews during the following plan year's QHP certification cycle. Prior to the beginning of the following plan year's QHP certification cycle, we will communicate information to FFE States to assess if FFE States conducting ECP certification reviews wish to continue conducting these reviews and will provide a timeline for the Effective ECP Review Program determination process for the upcoming plan year to newly electing FFE States.
Furthermore, as we proposed under § 155.1051(f), we reserve the right to evaluate at any time whether, and to what extent, an FFE State's circumstances have changed such that it has begun to or has ceased to satisfy the criteria established by us and consequently no longer has an Effective ECP Review Program. For example, these circumstances may include significant changes in the FFE State's authority and technical capacity to conduct ECP certification reviews such that it no longer can do so in a timely and effective manner, or if we identify data (after collecting issuer data from FFE States with an Effective ECP Review Program) indicating that consumers in the FFE State have inadequate access to ECPs, consistent with § 155.1051(f).
Comment:
One commenter questioned the need for continued data collection from QHP issuers in FFE States with an Effective ECP Review Program who must still submit ECP data to HHS, which HHS would evaluate to see if these QHP issuers would meet Federal ECP requirements. The commenter did not see the meaning of collecting this data when FFE States conducting ECP certification reviews may have different ECP requirements than under § 156.235. Some commenters requested additional information on how HHS plans to release ECP data to QHP issuers in FFE States with an Effective ECP Review Program. Lastly, one commenter requested that HHS phase out issuer ECP data collection in FFE States that elect to conduct their own ECP certification reviews.
Response:
We appreciate these questions from commenters about ECP data collection from QHP issuers in FFE States with an Effective ECP Review Program. As we have stated in the proposed rule (91 FR 6407) and within this final rule, continuing to collect issuer ECP data will allow us to continue to compare QHP issuer performance across the FFE, so that we can monitor consumer access to ECPs across the FFE, including to address other commenters' concerns on the potential for inconsistency and variability in the application and enforcement of ECP requirements across FFE States if FFE States conduct their own ECP certification reviews. Accordingly, we do not plan to phase out ECP data collection from QHP issuers in FFE States with an Effective ECP Review Program. Lastly, we plan to release ECP data to QHP issuers in FFE States with an Effective ECP Review Program directly within the ECP UI in MPMS. QHP issuers in FFE States with an Effective ECP Review Program will still validate and submit ECP data within the ECP UI in MPMS and respond to data related errors, if applicable. After successful ECP data submission, QHP issuers may download their ECP results directly in the calculation workspace within the ECP UI.
Comment:
One commenter recommended that HHS establish a standardized, national ECP data submission template with detailed data descriptions aligned to HHS' existing ECP data submission processes, develop uniform review timelines, and create a single data submission pathway usable regardless of whether HHS or the FFE State conducts the review to promote consistency and streamline ECP data transfers.
Response:
We appreciate the commenter's unique suggestion to maximize efficiencies and reduce issuer burden within the QHP certification data submission process. Due to current timing constraints with the upcoming QHP certification window for PY 2027, we cannot implement this suggestion at this time and believe such a solution would require coordination and agreement among multiple interested
( printed page 29757)
parties, including FFE States and other QHP issuers. We also recognize that multiple factors exist that may prohibit uniform review timelines across HHS and FFE States, including different rulemaking cycles on the State versus Federal level, differences in resources and data collection systems, conflicting deadlines to complete certification review processes, and issuer volume. In the meantime, we will continue to make MPMS available to FFE States should they wish to utilize issuer ECP data submitted through the ECP UI in MPMS for their ECP certification reviews, which may reduce issuer burden if issuers submit ECP data through this centralized platform. We will provide technical assistance to FFE States should they wish to utilize the ECP UI in MPMS as part of State ECP certification processes, to reduce issuer burden.
Comment:
One commenter encouraged HHS to require FFE States with an Effective ECP Review Program to publicly report participating ECPs within an issuer's network by ECP category type, appointment availability, and wait times at ECPs, and publicly identify issuers who have been found by the State to have ghost networks.
Response:
Currently, we do not intend to require FFE States to publicly report issuer ECP data on ECP category type, appointment availability, and wait times at ECPs. Our intention in proposing the Effective ECP Review Program and its associated requirements under § 155.1051 was to effectively create a robust Federal floor of minimum requirements that an FFE State must meet to conduct its own ECP certification reviews. These minimum requirements are consistent with existing Federal ECP requirements and certification review procedures under § 156.235. Since HHS does not currently publicly disseminate issuer ECP data submitted to HHS as part of QHP certification due to the data being market-sensitive and proprietary, imposing this additional reporting requirement on FFE States would be more stringent than existing Federal requirements and review procedures and not consistent with the goals of establishing a Federal floor for ECP certification reviews and processes. However, we welcome FFE States to transparently share this data with HHS or the public as they desire and see fit.
Regarding the commenters' suggestion to require FFE States to report issuer data on ECP category type, we will continue to collect issuer ECP data from those QHP issuers operating in FFE States with an Effective ECP Review Program. Thus, HHS already has the analytic capability to identify individual ECP category types that may be included within a QHP issuer's network of ECPs, which diminishes the necessity to require FFE States to provide this to HHS or the public. HHS plans to make this data available in a standardized format to FFE States with an Effective ECP Review Program, which FFE States may utilize to perform additional analyses to analyze access to ECPs across the State (including by category). We hope that providing issuer ECP data to FFE States with an Effective ECP Review Program in this manner will foster Federal and State collaboration and promote data exchange between HHS and FFE States, which may naturally allow us to receive additional data on individual ECP category types included within a QHP issuer's network of ECPs that were not identified by HHS.
HHS also does not intend to require FFE States to publicly report issuer ECP data on appointment availability and wait times to HHS, since we do not currently require issuers to separately meet these requirements and report associated data on ECP appointment availability and wait time requirements under § 156.235. For FFE States to publicly report this issuer ECP data, they would need to collect this data directly from issuers as part of ECP certification reviews. To facilitate this data collection, HHS would likely have to impose an additional requirement for FFE States to collect this data on appointment availability and wait times at ECPs to ensure it can be reported by FFE States. Overall, imposing these additional requirements on FFE States that are inconsistent with existing Federal ECP requirements and review processes would conflict with the goals of establishing a Federal floor of minimum standards for ECP certification reviews. However, if FFE States have ECP appointment availability and wait time requirements, these would constitute alternative ECP requirements compared to threshold, category per county, and Indian health care requirements (under § 155.1051(c)(1) through (c)(3)) that States must describe to us, consistent with requirements at § 155.1051(d). That is, the FFE State must disclose these alternative ECP requirements in its attestation form when electing to conduct ECP certification reviews. If the FFE State is determined to have an Effective ECP Review Program and conducts their own ECP certification reviews, at the minimum, the FFE State should communicate these alternative ECP requirements to issuers so issuers understand the types of ECP data that must be submitted to meet these requirements. The FFE State then has discretion to publicly disseminate this data, as appropriate.
Lastly, for the reasons above regarding the need to establish a Federal floor consistent with ECP requirements and review processes under § 156.235, we do not believe it would be appropriate to require FFE States to highlight issuers with found ghost networks. While we agree that this type of information could be useful to the public, we believe HHS would first need to understand different initiatives and processes FFE States are currently taking to address issuer ghost networks within their State prior to HHS considering any additional requirement related to ghost networks. We also believe this specific requirement is beyond the scope of this proposal and would be more appropriate to contemplate through potential future rulemaking along with other policy solutions related to ghost networks.
Comment:
A few commenters recommended that HHS delay implementation of this proposal to a PY 2028 effective date. Commenters raised concerns that FFE States likely do not have enough time to make any necessary changes in State ECP requirements or operations that may be required to demonstrate having an Effective ECP Review Program, or if an FFE State wishes, to make modifications to State ECP requirements and associated processes (for example, legislation, rulemaking, review methodologies) to hold QHP issuers to more stringent ECP requirements than those currently reflected under § 156.235. The commenter also stated that this could affect QHP issuers as well, if additional contracting is needed to meet more stringent requirements. Another commenter shared additional implementation concerns, recommending that HHS require FFE States to give advance notice to and partner with QHP issuers in developing any new ECP requirements.
Response:
We recognize that some FFE States may not currently be in the position to elect to conduct ECP certification reviews and undergo the Effective ECP Review Program determination process at this time. If this is the case, these FFE States still have an ability to elect to conduct ECP certification reviews and submit an attestation for PY 2028, as we are also providing this flexibility for FFE States for future plan years, not just for PY 2027. Thus, if an FFE State does not have the ability at this time to conduct ECP certification reviews and submit
( printed page 29758)
information to HHS as part of the Effective ECP Review Program determination process, then we will continue to conduct ECP certification reviews and encourage the FFE State to submit an attestation in future plan years. We also believe that it is possible some FFE States would be in the position to elect to conduct ECP certification reviews beginning PY 2027, which reduces the need to delay implementation of this proposal to PY 2028. For example, some States performing plan management have experience conducting ECP certification reviews prior to HHS assuming responsibility of these reviews after we expanded capacity to conduct ECP certification reviews of issuers in States performing plan management through implementation of the ECP UI in MPMS; so, it is possible some of these States may be ready to elect to conduct ECP certification reviews. Lastly, if the FFE State were to impose more stringent ECP requirements than those currently under § 156.235, we believe that this would likely be consistent with existing State law and authority, independent of the Effective ECP Review Program determination process. Overall, if an FFE State is approved to conduct ECP certification reviews, we recommend that QHP issuers coordinate with their State to understand State ECP requirements (especially to learn if the FFE State has more stringent ECP requirements than under § 156.235) and ECP data submission processes.
Lastly, in response to the commenter that requested HHS require FFE States to coordinate with QHP issuers in developing any new ECP requirements, we believe finalizing this requirement would interfere with State-specific rulemaking procedures and outreach processes which are beyond the scope or intention of our proposal, which aims to set a pathway for an FFE State to conduct their own ECP certification reviews. Nevertheless, we believe that any new ECP requirements issued at the State level would likely require some coordination with QHP issuers that would need to submit ECP data and documentation to demonstrate meeting such requirements during certification. We would encourage FFE States that are approved to conduct ECP certification reviews as an Effective ECP Review Program to communicate State-specific ECP requirements to QHP issuers and consider QHP issuers' feedback on those requirements.
Comment:
A State operating as an SBE-FP noted that it is not currently possible for some States to evaluate plans' compliance with ECP requirements under the current configuration of the MPMS. The commenter stated that, currently, when users with the State Reviewer role download the network adequacy template from MPMS, the ECP facility tab remains blank and the State experiences issues with the ECP data being imported. The commenter believed that this potential system limitation could affect the ability of an FFE State with an Effective ECP Review Program to leverage Federal infrastructure (such as MPMS) to conduct their own reviews of issuer-submitted ECP data.
Response:
We thank the State for providing their experience with MPMS as it relates to ECP data submission and States conducting ECP reviews. First, we clarify that we did not propose to apply the Effective ECP Review Program under § 155.1051 to SBE-FPs, as SBE-FPs already conduct their own ECP certification reviews. Rather, we proposed to allow FFE States, including States performing plan management, to elect to conduct ECP certification reviews. SBE-FPs, FFE, States performing plan management, and FFE States with an Effective ECP Review Program should be able to effectively view and download issuer submitted ECP data through the ECP UI in MPMS. We do not believe that FFE States with an Effective ECP Review Program would be limited in utilizing MPMS to conduct their own ECP certification reviews. We remains available to provide technical assistance to all States that utilize MPMS and/or HHS provided certification tools, thus we welcome further coordinating with the State during the QHP certification process to address this issue.
Altogether, we summarize below our finalized policies under this section related to ECP requirements. We are not finalizing our proposal to reduce ECP minimum percentage requirements for the overall ECP threshold, family planning provider threshold, and FQHC threshold from 35 to 20 percent. Thus, the minimum percentage requirement will remain 35 percent. We are finalizing our proposal to amend narrative justification requirements at § 156.235(a)(3) and (b)(3) to be consistent with current ECP data submission requirements as part of QHP certification, which require issuers to include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. Lastly, we are finalizing under § 155.1051 our proposal to allow FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of QHP issuers, with or without a network, provided that HHS determines the FFE State has sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria be considered to have an Effective ECP Review Program. However, consistent with our decision to delay implementation of our finalized policy (as discussed in section III.E.12. of this final rule) to permit certification of non-network plans as QHPs to PY 2028, FFE States that we determine to have an Effective ECP Review Program will be permitted to conduct ECP certification reviews of non-network plans effective beginning PY 2028. Lastly, we will also continue to collect ECP data from all FFE issuers for monitoring purposes and remain available to provide technical assistance and publicly available ECP resources to all States.
12. QHP Certification of Non-Network Plans (§§ 155.1050, 155.1051, 156.230, 156.235, 156.236, 156.275, and 156.810)
In the 2027 Payment Notice proposed rule (91 FR 6407), we proposed a number of revisions to parts 155 and 156 to allow plans that do not use a network (non-network plans) to receive QHP certification beginning in PY 2027 by demonstrating that they ensure a sufficient choice of providers in a manner consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act. In addition, to ensure that non-network plans are subject to similar requirements as network plans, we proposed that (1) FFE States that elect to conduct provider access certification reviews and are determined by HHS to have an Effective Provider Access Review Program under proposed § 155.1050(d) would be permitted to perform provider access reviews of non-network plans if the State satisfies all applicable criteria under § 155.1050(d); and (2) FFE States that elect to conduct ECP certification reviews and are determined by HHS to have an Effective ECP Review Program under proposed § 155.1051 would be permitted to perform ECP certification reviews of non-network plans if the State satisfies all applicable criteria under § 155.1051. For additional details on how the Effective Provider Access Review Program and Effective ECP Review Program proposals would apply to FFE States conducting reviews of non-network plans, we referred readers to these discussions in section III.E.12.d and section III.E.12.e of the proposed rule.
( printed page 29759)
a. Previous Rulemaking Related to Non-Network Plans
Together, section 1311(c)(1), 1311(c)(1)(B), and 1311(c)(1)(C) of the Affordable Care Act directs HHS to establish by regulation certification criteria for QHPs, which include (but are not limited to) criteria that require QHPs to ensure a sufficient choice of providers, provide information to enrollees and prospective enrollees on the availability of in-network and out-of-network providers, and include within health insurance plan networks those ECPs, where available, that serve predominantly low-income, medically-underserved individuals. We have historically implemented these provisions through our network adequacy and ECP requirements for network plans at § 156.230 and § 156.235, respectively.[329]
In the Exchange Establishment Rule (77 FR 18310), we finalized the minimum network adequacy criteria that plans, including medical plans and SADPs, must meet to be certified as QHPs at § 156.230. In the 2016 Payment Notice (80 FR 10749), we revised § 156.230(a) to specify that network adequacy requirements apply only to QHPs that use a provider network (network plans) to deliver services to enrollees and that a provider network includes only providers that are contracted as in-network. We also revised § 156.235(a) to state that the ECP criteria apply only to QHPs that use a provider network. In part 1 of the 2022 Payment Notice (86 FR 6138), we added paragraph (f) to § 156.230 to clarify that a plan for which an issuer seeks QHP certification or any certified QHP that does not use a provider network (or non-network plan) is not required to comply with the network adequacy standards at paragraphs (a) through (e) of § 156.230 to qualify for certification as a QHP. Unlike network-based plans, non-network health plans do not rely on a contracted set of providers that agree in advance to specific terms and negotiated payment rates, nor do they condition or differentiate benefits to enrollees based on whether the issuer has a network participating agreement with a provider that furnishes covered services. Instead, these plans set specific benefit amounts for covered services and communicate those benefit amounts to enrollees who may then seek covered services from any provider. The plan may determine the benefit amount based on an established methodology such as a percentage of a publicly available benchmark, a reference-based pricing structure, or another reimbursement standard (that is, Medicare or private payor rates, etc.).
In the 2024 Payment Notice (88 FR 25872 through 25879), we exercised the authority delegated to us by section 1311(c)(1) of the Affordable Care Act to establish criteria for the certification of health plans as QHPs to revise §§ 156.230 and 156.235 to require all individual market QHPs and SADPs and all SHOP QHPs across all Exchanges to utilize a network of providers that complies with the standards described in §§ 156.230 and 156.235. In doing so, we acknowledged that we had previously stated that “nothing in [the Affordable Care Act] requires a QHP issuer to use a provider network” because there is no explicit standalone network requirement (88 FR 25872 (quoting 84 FR 6154)). But we still stated concerns over whether a plan without a network would be able to comply with Affordable Care Act section 1311(c)(1)(C)'s requirement that plans “shall, at minimum . . . include within health insurance plan networks those essential community providers, where available, that serve predominately low-income, medically-underserved individuals,” which we read to imply that access to ECPs would be provided “within health insurance networks” (88 FR at 25873). We also solicited comment on alternative administrable regulatory standards under which non-network plans could “ensure a sufficient choice of providers” consistent with section 1311(c)(1)(B) of the Affordable Care Act. At the time, neither commenters to the 2024 Payment Notice nor HHS had enough information to devise such an administrable regulatory standard to enable non-network plans to demonstrate a sufficient choice of providers to receive QHP certification. On these bases, in the 2024 Payment Notice (88 FR 25876), we finalized the requirement that all QHPs (except certain SADPs) [330]
must use a network of providers. As a result of this, non-network plans are currently unable to meet all of the minimum certification criteria at § 155.1000(c), which means Exchanges cannot currently certify non-network plans as QHPs and consumers cannot enroll in non-network plans through the Exchanges.
b. The Basis for Reconsidering Our Existing Prohibition on Non-Network Plans as QHPs
As a preliminary matter, in the proposed rule (91 FR 6408), we first explained why we were revisiting our existing blanket prohibition of non-network plans as QHPs, including our approach to ensure non-network plans meet requirements to ensure a sufficient choice of providers in a manner consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act. We stated that one justification for revisiting our existing prohibition of non-network plans as QHPs is that circumstances have changed: when we finalized our blanket prohibition of non-network plans as QHPs, we had not developed an effective, administrable approach at the time we adopted the prohibition through which we could adequately measure whether non-network plans could ensure a “sufficient choice of providers” under section 1311(c)(1)(B) of the Affordable Care Act, or include ECPs through their plans, where available, under section 1311(c)(1)(C) of the Affordable Care Act. We stated that we continue to believe that consumers shopping on the Exchanges must be assured of the ability of every QHP to provide a sufficient choice of providers under section 1311(c)(1)(B) of the Affordable Care Act, and that a non-network plan should not be given a “pass” on demonstrating that it provides access to a sufficient choice of providers because it does not utilize a provider network. As described further below and in the next subpart, we proposed a new approach to measuring a non-network plan's compliance with section 1311(c)(1)(B) and (C) of the Affordable Care Act, which addresses our prior concerns. In doing so, we also revisited our original interpretation of section 1311(c)(1)(C) of the Affordable Care Act, including how our proposed approach would mitigate prior concerns over non-network plans being able to provide access to ECPs in a manner consistent with this provision.
First, we acknowledged that provider networks serve as a critical cost control tool, which has downstream impacts on a consumer's out-of-pocket costs that are important to consider when devising an alternative regulatory standard to continue to ensure broader access to care. We noted that insurers with a provider network often have different cost-sharing requirements depending on if an enrollee sees a provider that is in-network versus out-of-network. We stated that a traditional network plan typically contracts with a certain number of providers (but rarely all) in each area who agree to accept the plan's negotiated rates as payment in full for covered services, ensuring that enrollees have reasonable access to a certain number of providers who will render services at specified costs; and often,
( printed page 29760)
these specified costs are lower if an enrollee sees an in-network provider since enrollees often have to pay more when seeking care from providers with whom the issuer did not contract.
We stated that, in contrast, a non-network plan sets specified benefit amounts for covered services and communicates those benefit amounts to its enrollees in advance. We stated that non-network plan enrollees use this benefit amount as a reference price for how much they should expect to pay for the receipt of covered services under the plan. We further stated that with it, they can choose any provider for their care and compare and negotiate prices among available providers to find a provider who will accept the plan's benefit amount as payment in full, such that the provider will not balance bill the enrollee for additional amounts beyond the plan's benefit amount. We noted that this interaction between the enrollee and provider before services are rendered could limit the enrollee from incurring additional unforeseen out-of-pocket costs, particularly if the enrollee decides to pursue care with the provider at a cost below or equal to the plan's benefit amount. Thus, we stated that both plan models are capable of providing a pathway for enrollees to limit out-of-pocket costs. We stated that non-network plans are capable of providing an opportunity for individual enrollees to participate in efforts to lower their health care costs through individualized price comparisons and negotiations, while network plans rely heavily on health insurers to do so.
However, we stated that while enrollees in a non-network plan can receive some benefit for covered services from virtually any provider, there is no guarantee that the plan's benefit amounts are actually sufficient to cover the provider's full charges, and there is no requirement imposed by the non-network plan on providers to accept the plan's benefit amount as payment in full. We stated that as a result, if or when these benefit amounts are too low, non-network plans can leave enrollees with additional out-of-pocket costs that make certain providers, as a practical matter, unavailable. We further stated that can be problematic for services that an enrollee could not have reasonably anticipated needing to negotiate for in advance. And we noted that it can have a particular impact on low-income, medically underserved populations who may face disproportionate challenges in paying for large out-of-pocket costs.
Furthermore, we stated that if a non-network plan's benefit amount for a covered service is so low that virtually no providers in a particular area accept the benefit amount as payment in full, the non-network plan cannot credibly claim to provide a sufficient choice of providers of those services, and the non-network plan does not provide access to a sufficient choice of providers under section 1311(c)(1)(B) of the Affordable Care Act. Conversely, we noted that if the benefit amount is sufficient such that many providers in the area accept the benefit amount as payment in full, enrollees may choose between providers in their area who will accept the non-network plan's benefit amount as payment in full without incurring additional out-of-pocket costs. We stated that in this case, a non-network plan may be able to provide access to a sufficient choice of providers for those services. In other words, we stated that the set of providers in the applicable area that would accept the plan's benefit amount as payment in full is like a network plan's network. We stated that so long as that set of providers is adequate, a non-network plan can comply with requirements to ensure a sufficient choice of providers, and we described our proposed method to measure that compliance in the next section.
As we stated in the discussions above, we raised concerns in the 2024 Payment Notice regarding the ability of a non-network plan to comply with section 1311(c)(1)(C) of the Affordable Care Act, due to our understanding that access to ECPs should be provided “within health insurance networks.” We inferred from Affordable Care Act section 1311(c)(1)(C)'s use of the word “network” that the statute meant that Exchanges could certify, as QHPs, only plans that have a contractual network of providers, not inclusive of non-network plans. Though, we recognized that the term “network” is never defined in the statute. And, as we have consistently noted, we stated that Congress never imposed a standalone requirement that QHPs structure their plans via contracts with providers nor was Congress specific on the requirements needed to constitute a network. We stated that we now interpret the statute to offer broad flexibility governing the status of a contractual relationship between a plan and provider as a precondition to constitute a network under section 1311(c)(1)(C) of the Affordable Care Act. In this regard, we stated that we believe that so long as non-network plans provide sufficient access to ECPs, where available, that serve predominately low-income, medically underserved individuals, a non-network plan could comply with requirements under section 1311(c)(1)(C) of the Affordable Care Act. We stated that this may be accomplished through a non-network plan demonstrating access to ECPs within their service area that would accept the plan's benefit amount as payment in full.
Furthermore, we stated that we have evaluated traditional networks to ensure enrollees have access to a sufficient choice of providers, consistent with section 1311(c)(1)(B) of the Affordable Care Act, and to promote access to ECPs, where available, for low-income, medically underserved individuals, consistent with section 1311(c)(1)(C) of the Affordable Care Act. To that effect, we noted that networks facilitate a multitude of different relationships between providers, insurers, and enrollees to ensure sufficient access to care, which can still be maintained through non-network plans through their greater focus on enrollees more directly participating in lowering the price of their care. Specifically, we stated that a non-network plan's “network” consists of the providers in the applicable area that would accept the plan's benefit amount as payment in full. We further stated that by establishing payment amounts that providers can choose to accept as payment in full, non-network plans are capable of creating a
de facto
network of providers or suppliers even without formal contractual relationships.
Thus, we stated (91 FR 6409) that a non-network plan can comply with section 1311(c)(1)(C) of the Affordable Care Act by ensuring that a sufficient number of ECPs accept the plan's benefit amounts as payment in full. However, we noted that a non-network plan would not satisfy that requirement if its benefit amount is so low that many ECPs would not accept the benefit amount as payment in full from enrollees, because section 1311(c)(1)(C) of the Affordable Care Act would still require an Exchange to consider the practical availability of services from ECPs before certifying a QHP, including ECPs, where available. We stated that it would not be sufficient for an Exchange to simply conclude that a non-network plan provides access to providers in a manner consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act because the plan provides some benefit amount for covered services rendered by any provider. Thus, we stated that the availability of providers in a particular area that accept the benefit amount as payment in full is important to constitute a sufficient choice of providers consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act.
( printed page 29761)
Moreover, we stated that there are additional reasons for our reconsideration of our blanket prohibition of non-network plans as QHPs. Specifically, we stated that recent efforts to improve health price transparency and its implementation across the health care system present an opportunity to reshape how health care services are delivered, and when enrollees have easier access to health care pricing information, market forces can and often do drive down costs through increased competition among providers.[331]
We noted that because enrollees directly negotiate the cost of care in non-network plans, non-network plans can more naturally leverage price transparency principles compared to network plans. We stated that by incentivizing patient involvement in health cost comparison, these plans have potential to reduce overall health care costs by empowering their enrollees to shop for and potentially negotiate lower prices. We further stated that such efforts could lead to a more efficient market where network formation becomes less critical for ensuring affordable health care access. We also stated that because providers are not bound by pre-negotiated network agreements, enrollees in such plans may face different pricing dynamics than in network-based plans, including the need to compare costs more proactively and, in some cases, negotiate payment amounts directly with providers. We stated that this model places greater emphasis on enrollee engagement and transparency but can also offer increased flexibility and broader provider choice while maintaining predictable plan liability through the use of clear and consistently applied reimbursement formulas.
We further stated that overall, non-network plans have great potential to reduce overall health care costs. First, we stated that they can empower enrollees to use price information on benefit amounts, when available, to shop for lower prices and negotiate directly with providers, fostering increased competition and potentially driving down prices across the market. When enrollees have access to accurate, timely health care pricing information, they can make informed decisions about their health care spending and actively seek the best value for medically necessary services. We anticipated that this consumer-driven approach would create a more competitive marketplace where providers would need to consider their pricing strategies more carefully to attract and retain patients. Additionally, we stated that as more enrollees engage in shopping and direct price negotiations, providers may be incentivized to proactively offer more competitive rates to maintain their market share, potentially leading to broader market-wide price reductions that benefit many enrollees.
Second, we stated (91 FR 6410) that non-network plans eliminate substantial administrative overhead associated with traditional network management, which in turn can result in lower premiums. We stated that the administrative cost savings are realized through four key areas, based on our internal research into existing non-network plans: (1) the elimination of provider contract management costs (including legal fees, staff, and provider relationship development and maintenance); (2) the removal of provider credentialing expenses and directory maintenance; (3) reduction in claims processing complexity and network-specific prior authorization requirements; and (4) streamlined organizational structure with resources redirected to consumer support tools and education.
c. Proposed Alternative Regulatory Standard for Non-Network Plans (§ 156.236)
Based on these legal principles, in the proposed rule (91 FR 6410), we proposed the following regulatory standards for non-network plans to demonstrate that they provide access to a sufficient choice of providers (including ECPs) to ensure compliance with section 1311(c)(1)(B) and, as relevant, section 1311(c)(1)(C) of the Affordable Care Act. First, we proposed to add a new section to part 156, § 156.236, that contains the provider access sufficiency standards (including ECP access) specific to non-network plans, and to revise §§ 156.230 and 156.235 to make clear that those sections address the provider access sufficiency standards (including ECP access) for network plans.
We proposed to add § 156.236(a) to state that a non-network QHP must ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that services will be accessible without unreasonable delay. Additionally, as discussed in sections III.D.18., III.D.19., III.E.10., and III.E.11.c of the proposed rule, we proposed to allow FFE States, including States performing plan management, to conduct their own provider access and/or ECP certification reviews provided the State demonstrates sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program (for provider access reviews) and/or an Effective ECP Review Program (for ECP reviews). We stated that FFE States that elect to conduct provider access certification reviews and are determined by HHS to have an Effective Provider Access Review Program under proposed § 155.1050(d) would be permitted to perform such reviews of non-network plans if the State satisfies all applicable criteria. Similarly, we stated that FFE States that elect to conduct ECP certification reviews and are determined by HHS to have an Effective ECP Review Program under proposed § 155.1051 would be permitted to perform such reviews of non-network plans if the State satisfies all applicable criteria. For additional detail on the applicability of the proposed Effective Provider Access Review Program and Effective ECP Review Program to non-network plans under proposed § 156.236, we referred readers to the discussions in sections III.D.18., III.D.19., III.E.10., and III.E.11.c. of the proposed rule.
Furthermore, under § 156.236(b), we proposed that a non-network plan applying for certification to be offered as a QHP through an FFE must report the following information to the FFE for the FFE's determination whether a non-network plan provides a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full (including ECPs and providers that specialize in mental health and substance use disorder services) to ensure that services will be accessible without unreasonable delay:
(1) The non-network plan's assessed percentage of available providers in each plan's service area that accept the plan's benefit amount as payment in full; and for ECPs, whether the non-network plan meets at least a minimum percentage, as specified by HHS, of available ECPs that accept the plan's benefit amount as payment in full in each plan's service area, collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B), and at least a minimum percentage of available ECPs that accept the plan's benefit amount as
( printed page 29762)
payment in full in each plan's service area within certain individual ECP categories, as specified by HHS;
(2) For ECPs, whether the non-network plan offers the benefit amount as payment in full to at least one ECP in each of the eight ECP categories per county in the plan's service area described in § 156.235(a)(2)(ii)(B);
(3) For ECPs, whether the non-network plan offers the benefit amount as payment in full to all available Indian health care providers in the plan's service area;
(4) The non-network plan's strategy for conducting continuous outreach to available providers (including ECPs) in the plan's service area to determine whether they would accept the plan's benefit amount as payment in full;
(5) The non-network plan's strategy for making benefit amounts available to the public, including plan enrollees, potential enrollees, and providers (including ECPs), in an easily accessible and understandable format;
(6) The non-network plan's methodology for determining benefit amounts;
(7) The non-network plan's strategy for providing consumer-friendly and public information about potential balance billing scenarios and expected out-of-pocket costs, including historical data on actual out-of-pocket costs incurred by its enrollees while accessing providers (including ECPs) in the area;
(8) The availability of an exceptions process under the non-network program for enrollees who cannot find providers (including ECPs) willing to accept the benefit amount as payment in full; [332]
and
(9) The non-network plan's strategy for providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers (including ECPs) in their area who will accept the plan's benefit amount as payment in full.
We stated that these are among the factors that we have historically found useful in considering whether a non-network plan provides access to a sufficient choice of providers, including ECPs, to warrant the certification of non-network plans for the FFEs. We noted that HHS, as operator of the FFEs, considered the QHP application submitted by a non-network plan for PYs 2021 and 2022 in Ohio. In assessing whether the plan was in the interests of qualified individuals on the FFE in Ohio (under § 155.1000(c)), we used similar factors to assess whether the non-network plan provided protection against additional out-of-pocket costs for EHB in a manner consistent with § 156.130, and we believe this was appropriate because these factors provide a more complete picture of how well a non-network plan actually limits enrollees' out-of-pocket costs.
We stated that the first proposed factor, the non-network plan's assessed percentage of available providers in each plan's service area that accept the plan's benefit amount as payment in full and, for ECPs, whether the non-network plan meets separate minimum percentage requirements of available ECPs that accept the plan's benefit amount as payment in full in each plan's service area, is an important indicator of how generous the non-network plan's benefit amounts actually are. We stated that it would provide an Exchange greater assurance that enrollees can actually access a sufficient number of providers, including ECPs, who will not seek additional payment from the enrollee after receiving the benefit amount from the plan. We further stated that requiring the non-network plan to have assessed the anticipated percentage of providers in the area who would accept the plan's benefit amount as payment in full also would provide Exchanges with assurance that the non-network plan issuer performed sufficient research and analysis in advance to determine sufficient benefit amounts for a relevant area. We stated that this would help ensure benefit amounts are generally sufficient to limit unanticipated additional out-of-pocket costs for enrollees.
We stated (91 FR 6411) that the second proposed factor, whether the non-network plan offers its benefit amount as payment in full to at least one ECP in each of the eight ECP categories per county in the plan's service area described in § 156.235(a)(2)(ii)(B), is an important indicator of the plan's ability to cater to enrollee needs across a wide array of priority health needs and socioeconomic factors, which is required by the Affordable Care Act as a condition of QHP certification. Section 1311(c)(1)(C) of the Affordable Care Act requires access to ECPs, where available, that serve predominately-low income, medically underserved individuals, such as health care providers defined in section 340B(a)(4) of the PHS Act and providers described in section 1927(c)(1)(D)(i)(IV) of the Act. We stated that to demonstrate that non-network plans comply with section 1311(c)(1)(C) of the Affordable Care Act and accordingly provide access to ECPs, where available, such as those under sections 340B(a)(4) of the PHS Act and 1927(c)(1)(D)(i)(IV) of the Act, Exchanges must be assured that the plan's benefit amounts are sufficient enough such that at least one ECP in each of the eight ECP categories per county within the plan's service area would accept the plan's benefit amount as payment in full.
We stated that the third proposed factor, whether the non-network plan offers its benefit amount as payment in full to all available Indian health care providers in the plan's service area, is an important indicator of the plan's ability to ensure Indian enrollees are able to receive applicable cost-sharing reductions for the plan variations described at §§ 156.420(b)(1) and (2) without incurring additional out-of-pocket costs. Additionally, we noted that Indian health care providers are among the providers described under section 340B(a)(4) of the PHS Act, which plans must demonstrate access to under § 156.235(a)(2)(ii), (b)(2)(ii), and (c), consistent with section 1311(c)(1)(C) of the Affordable Care Act.
We stated that the fourth proposed factor (91 FR 6411), the non-network plan's strategy for conducting outreach to available providers (including ECPs) in a particular area to determine whether they would accept the plan's benefit amount as payment in full, is an important indication of the non-network plan's recognition that whether any particular provider will accept a benefit amount as payment in full is a moving target. We noted that providers that are not under contract to accept a non-network plan's payment as payment in full are generally not bound by any contract or law in setting prices. We also noted that they may choose to change their charges for their services based on any multitude of factors, including changes in their operating expenses, changes in medical advancement, competitive pressure, or for no particular reason at all. And, they may choose to change this amount at any time. We stated that, as a result, it is imperative that a non-network plan have in place a strategy for conducting continuous outreach to available providers (including ECPs) in a particular area to determine whether they would accept the plan's benefit amount as payment in full, so that the plan can make adjustments to its benefit amounts to ensure that enrollees can access a sufficient number of providers.
We stated that the fifth proposed factor, the non-network plan's strategy
( printed page 29763)
for making benefit amounts available to the public, including plan enrollees, potential enrollees, and providers (including ECPs), in an easily accessible and understandable format, is an important indicator of the non-network plan's ability to effectively communicate the plan's benefit amounts. We stated that making this information widely available to providers would give notice to providers that charge more than the plan's benefit amount that their charges may be too high and they should consider lowering them to attract plan enrollees. We also stated that non-network plans work best when information between the plan, the enrollee, and the provider is shared transparently; and noted that, after all, an enrollee cannot be expected to shop for care if they do not understand what the plan will actually pay the provider.
We stated that the sixth proposed factor (91 FR 6411), the non-network plan's methodology for determining benefit amounts, is an important indicator that the non-network plan is not setting arbitrary benefit amounts for covered services; and, that the benefit amounts are well-informed through various analyses and research, so that the amounts reasonably cover costs associated with a particular service.
We stated that the seventh proposed factor, the non-network plan's strategy for providing consumer-friendly information to plan enrollees and potential enrollees about potential balance billing scenarios and expected out-of-pocket costs, including historical data on actual out-of-pocket costs incurred by its enrollees while accessing ECPs in the area, is an important indicator of the plan's ability to educate its enrollees about the plan's expectations on how the plan may be best utilized to minimize additional out-of-pocket costs. We noted that non-network health plans do not currently exist in the individual and small group market, and are less commonly offered in the large group market and as excepted benefits products, so the plan design may not be immediately intuitive to enrollees. We stated that, as such, it would be imperative that non-network plans have in place a cohesive strategy for providing consumer-friendly information about how the plan may be most effectively used to limit out-of-pocket costs and the impact of seeking care from providers who charge more than the plan's benefit amount.
We stated that the eighth proposed factor, the availability of an exceptions process under the non-network plan for enrollees who cannot find providers (including ECPs) willing to accept the benefit amount as payment in full, is an important indicator of the plan's commitment to be flexible for enrollees who have little choice in providers. We stated that the provision of such an exceptions process would recognize that there may be some circumstances where a non-network plan may be unable to adequately protect consumers against out-of-pocket costs in circumstances where large numbers of providers refuse the plan's payment as payment in full. We stated that in recognition of this possibility, such an exceptions process would be able to shift the burden of paying any unavoidable, additional out-of-pocket costs from the enrollee to the non-network plan.
We stated that the ninth proposed factor, the non-network plan's strategy for providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers (including ECPs) in their area who will accept the plan's benefit amount as payment in full, is another important indicator of the plan's ability to educate its enrollees about the plan's expectations on how the plan may be best utilized to minimize additional out-of-pocket costs.
We stated (91 FR 6412) that under this proposal, non-network plans would be subject to and allowed to demonstrate that they meet all the general certification criteria at § 155.1000(c), which would allow Exchanges the ability to certify non-network plans as QHPs. These general certification criteria include the minimum certification requirements outlined in subpart C of part 156,[333]
which include the requirement that each QHP must comply with benefit design standards as defined in § 156.20, which requires the provision of the EHB package. Thus, we stated that under this proposal, non-network plans would be required to provide this EHB package as a condition of QHP certification, which includes the provision of EHB in accordance with § 156.115, the cost-sharing requirements at § 156.130, and the levels of coverage requirement at § 156.140. We further stated that this requirement to provide the EHB in accordance with § 156.115 would mean that the non-network plan would, among other things, provide benefits that are substantially equal to the relevant State's EHB-benchmark plan. We stated that this would require the non-network plan to ensure that any covered benefits under the plan that are not EHB in the State are not treated as EHB under the plan. We also stated that non-network plans that do not comply with these minimum certification requirements would be subject to denial of certification in accordance with § 155.1000(e) and decertification in accordance with § 155.1080(c).
In addition, we stated that non-network plans that are applying for QHP certification or are QHPs would also be required to structure their plans so that they provide all the consumer protections that apply to individual and small group health coverage including, but not limited to, those specified in PHS Act title XXVII parts A through D, as all other plans applying for QHP certification are subject to providing. We also stated that under this proposal, a non-network plan would not be able to claim exemption from such protections merely because it does not enter into contracts with providers. We stated that failure to offer these protections would also result in denial of certification in accordance with § 155.1000(e) and decertification in accordance with § 155.1080(c), even though they are not explicitly included in the minimum certification requirements outlined in subpart C of part 156. We noted that under section 1311(e)(1)(B) of the Affordable Care Act and § 155.1000(c)(2), Exchanges have broad discretion to determine whether a plan is in the interest of qualified individuals and qualified employers, regardless of whether the plan meets other minimum certification requirements consistent with § 155.1000(c)(1). We confirmed that an Exchange may use this authority to deny certification to a non-network plan that is not structured in a manner that provides all the consumer protections that apply to individual and small group health insurance coverage including, but not limited to, those specified in PHS Act title XXVII parts A through D. We stated, for example, that the breadth of an Exchange's authority to deny certification under the interest standard extends to determinations that a non-network plan's benefit structure fails to provide protections against surprise medical bills in a manner similar to a network plan.[334]
We noted that the certification criteria at § 155.1000(c)(2) include the requirement that the Exchange determine that making the health plan
( printed page 29764)
available is in the interest of the qualified individuals and qualified employers. We stated that this proposal would not require States to approve non-network plans for sale nor would it require Exchanges to certify such plans. We stated that we have long maintained that Exchanges are free to exercise the authority at section 1311(e)(1) of the Affordable Care Act (as implemented at § 155.1000(c)(2)) to refuse certification to a plan if it determines that making available such health plan through such Exchange is not in the interests of qualified individuals and qualified employers in the State,[335]
even if the plan otherwise meets all other QHP certification requirements. We noted that in the Exchange Establishment Rule (77 FR 18405), we stated that an Exchange may want to choose among one of several strategies for making this determination: (1) an Exchange may choose to utilize an “any qualified plan” strategy for certifying QHPs in its Exchange, such that an Exchange certifies all health plans as QHPs that meet and agree to comply with minimum QHP certification requirements; (2) an Exchange could undertake a competitive bidding or selective contracting process and limit QHP participation to only those plans that ranked highest in terms of certain Exchange criteria; (3) an Exchange may also choose to negotiate with health insurance issuers on a case-by-case basis and could request that an issuer, upon meeting the minimum certification standards, amend health plan offerings to further the interest of qualified individuals and qualified employers served by the Exchange; or (4) an Exchange may implement selection criteria beyond the minimum certification standards in determining whether a plan is in the interests of the qualified individuals and employers.[336]
We reaffirmed these flexibilities under this proposal; we stated (91 FR 6412) that Exchanges would be able to require non-network plans to meet additional criteria beyond those described in the approach outlined above to be certified as QHPs, and they may determine that such plans are not in the interests of qualified individuals and qualified employers in the State, regardless of whether the non-network plan otherwise meets the certification criteria at § 155.1000(c)(1), and refuse them certification.
We sought comment regarding the PY 2027 effective date of this proposal. We noted that this includes comments from any QHP issuers that may be interested in submitting non-network plans for QHP certification for PY 2027, or whether PY 2028 may be the soonest that any QHP issuer could realistically consider submitting non-network plans for QHP certification.
We stated that, in connection with this proposal, we had not identified any barriers to non-network plans' participation in the HHS-operated risk adjustment program. However, we stated that because these plans are not under contractual relationships with providers, we recognize that they may have difficulty obtaining medical records from providers for the purposes of HHS-RADV, which is a requirement for risk adjustment covered plans under § 153.630. We noted that EDGE-reported diagnoses for which no medical record can be obtained are considered to be non-validated diagnoses in the HHS-RADV process and would result in higher error rates and higher HHS-RADV adjustments. As such, we sought comment on considerations for non-network plans in the HHS-RADV process.
d. Effective Provider Access Review Program Requirements for Non-Network Plans
Under sections III.D.18. and III.E.10. of the proposed rule, we proposed to allow FFE States, including States performing plan management, to elect to conduct their own provider access certification reviews of issuers' plans applying for certification as a QHP through an FFE, provided the State determines it has sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d)(2) through (d)(4), as determined by HHS. We proposed that in FFE States that do not elect to conduct provider access reviews or that we determine do not have an Effective Provider Access Review Program, we would continue to conduct provider access certification reviews consistent with § 156.230 for network plans.
To ensure that non-network plans would be held to similar requirements as network plans in meeting regulatory requirements to provide sufficient choice of providers under section 1311(c)(1)(B) of the Affordable Care Act, in the proposed rule (91 FR 6413), we also proposed to apply the Effective Provider Access Review Program to FFE States, including States performing plan management, that wish to conduct provider access reviews of non-network plans. We stated that this means that if an FFE State elects to conduct their own provider access certification reviews of issuers' plans applying for certification to be offered as a QHP through an FFE and we determine that the State has satisfied all the applicable criteria to be considered to have an Effective Provider Access Review Program, then the State would have the ability to conduct provider access certification reviews of non-network plans. We also stated that an FFE State would need to demonstrate that it meets applicable criteria for both network and non-network plans under proposed § 155.1050(d)(2) through (d)(4) prior to HHS determining that a State has an Effective Provider Access Review Program. We stated that this would mean an FFE State would not be permitted to elect to conduct provider access certification reviews for only network plans and not non-network plans, if they certify both such plans, or vice versa. However, we noted that should an FFE State notify us that it chooses not to certify non-network plans, and so does not offer non-network plans through the FFE operating in their State (regardless of if the State or HHS conducts the review), then we would determine whether it satisfies applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d)(2) through (d)(4) for network plans only. We sought comment on this approach. Additionally, we stated that similar to the approach for network plans, if we determine FFE States do not satisfy applicable criteria to be considered to have an Effective Provider Access Review Program, then we would conduct provider access certification reviews for non-network plans under new standards proposed at § 156.236.
We proposed (91 FR 6413) that an FFE State would need to demonstrate that it meets applicable criteria for both network plans and non-network plans under proposed § 155.1050(d)(2) through (d)(4), if they decide to certify such plans, to receive the designation to have an Effective Provider Access
( printed page 29765)
Review Program. We stated that this would mean that an FFE State would not be permitted to elect to conduct provider access certification reviews for only network plans and not non-network plans, if they certify such plans, or vice versa. We stated that we believe this is important, as some QHP issuers may choose to offer both network and non-network plans and centralizing reviews to a single entity, whether the FFE State or HHS, for the same issuer, would reduce administrative inefficiencies that may result if the FFE State and HHS have to coordinate provider access certification review results across a range of network and non-network plans. We also stated that we believe review authority being limited to a single entity, either the FFE State or HHS, would allow both network and non-network plans to undergo consistent, standardized reviews conducted by the same reviewing entity. We stated that we believe this would ensure similar requirements and methodologies would be applied fairly across network and non-network plans and reduce potential differences in provider access review results. We noted that this may also reduce variabilities in access across the FFE State between enrollees in non-network plans versus network plans that may result if these plans undergo different levels and types of provider access certification reviews by separate review entities, and it could make it more difficult to effectively compare provider access review results between network and non-network plans during certification if alternative review methods are applied within the same FFE State. We stated that, overall, just as with network plans, non-network plans must ensure sufficient access to a range of providers in a manner consistent with section 1311(c)(1)(B) of the Affordable Care Act.
We proposed to implement requirements for non-network plans that were similar to the requirements for network plans under the Effective Provider Access Review Program at proposed § 155.1050(d). We stated that an FFE State must demonstrate it has sufficient authority and the technical capacity to conduct provider access certification reviews for non-network plans by satisfying all applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d)(2) through (d)(4), including criteria specific to non-network plans. We also stated that, just as with network plans, an FFE State determined to have an Effective Provider Access Review Program would be expected to ensure sufficient access to providers under non-network plans. We stated that in this case, the FFE State would need to ensure that a QHP would be required to ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that services will be accessible without unreasonable delay.
We also stated that, under our proposal, as with network plans, a State operating an FFE that elects to conduct its own provider access reviews, and which deems to certify non-network plans, must demonstrate it has established provider access standards that are set forth in State statute or regulation which are consistent with provider access standards set forth in § 156.230(a)(1)(ii) and (iii) and are relevant to non-network plans. We stated that the FFE State would also need to demonstrate that the State's provider access review process includes reporting systems for State required provider access metrics related to non-network plans as well as documentation of methodology associated with non-network plan review; and that the State provides descriptions of all data collection systems, templates and methodologies used by the State, or the State's delegated entity, to collect and review provider access data for non-network plans and that this data and documentation received is sufficient to conduct an examination of non-network plans. We noted that the FFE State would also be required to establish and maintain clear procedures and timeline requirements for regular provider access reviews related to non-network plans, including processes that ensure reviews occur prior to each plan year's QHP certification cycle.
Additionally, we stated that the FFE State would be required to have a process for monitoring and addressing consumer-related provider access complaints for non-network plans to ensure sufficient access to providers consistent with section 1311(c)(1)(B) of the Affordable Care Act and as set forth in State statute. We further stated that the FFE State would also be required to have a process to collect and review information capable of demonstrating whether non-network plans provide access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full. We stated that we sought to understand whether the FFE State has a process for collecting and analyzing this information to demonstrate technical capacity during Effective Provider Access Review Program determinations. Additionally, we considered enumerating the information that non-network plans must submit to the FFE listed at § 156.236(b)(4) through (b)(9) within § 155.1050(d)(4)(vi) as requirements for FFE States with an Effective Provider Access Review Program to review non-network plans to ensure they are in alignment with HHS' proposed approach in an effort to further support consumer protectiveness in this novel plan design. We noted that these factors would include assessing a non-network plan's strategy for conducting outreach to providers in their area, making benefit amounts public to enrollees, methodologies for determining benefit amounts, strategy for publishing consumer-friendly information on balance billing and potential out-of-pocket costs, availability of exceptions processes for enrollees unable to locate providers who accept benefit amounts as payment in full, and customer services resources. However, we stated that, as HHS is seeking to broadly restore flexibilities to FFE States as a part of some QHP certification reviews and empower FFE States who understand their consumer needs and local conditions best, we opted in this proposal to provide deference to FFE States in how they will review non-network plans for a sufficient choice of providers who accept the plans benefit amount as payment in full in accordance with information listed at § 156.236(b)(4) through (b)(9). We sought comment on whether HHS should better align the reviews of non-network plans for QHP certification as described above.
We stated that while these factors for assessing whether a State has an Effective Provider Access Review Program, as related to non-network provider access reviews, are comprehensive, we believe this approach would provide ample flexibility to States to determine the best methodology to assess provider access under non-network plans within the State. We anticipated that each State's approach would be dependent on available resources and population needs unique to each State and that these proposed factors would serve to appropriately evaluate overall State processes for review of non-network plans to ensure sufficient consumer protection.
e. Effective Essential Community Provider Review Program Requirements for Non-Network Plans
Under sections III.D.19 and III.E.11.c. of the proposed rule, we proposed to allow FFE States, including States
( printed page 29766)
performing plan management, to elect to conduct their own ECP certification reviews of issuers' plans applying for certification as a QHP through an FFE provided the State demonstrates sufficient authority and the technical capacity to conduct these reviews by meeting the applicable criteria, as determined by HHS, to be considered to have an Effective ECP Review Program under proposed § 155.1051. Additionally, as discussed in section III.E.11.c of the proposed rule, we proposed that if we determine an FFE State does not have an Effective ECP Review Program, we would continue to conduct ECP certification reviews consistent with § 156.235 for network plans. To ensure that non-network plans would be held to similar requirements as network plans in meeting regulatory requirements to ensure reasonable and timely access to ECPs for low-income, medically underserved individuals, we proposed (91 FR 6414) to also apply the Effective ECP Review Program under § 155.1051 to FFE States, including States performing plan management, that wish to conduct ECP certification reviews of non-network plans. That is, we stated that under this proposal, if FFE States elect to conduct their own ECP certification reviews of issuers' plans applying for certification to be offered as a QHP through an FFE and the State is determined by HHS to have satisfied all the applicable criteria to be considered to have an Effective ECP Review Program, then States would have the ability to conduct ECP certification reviews of non-network plans. We stated that an FFE State would need to demonstrate that it meets applicable criteria for both network plans and non-network plans under proposed § 155.1051(b) through (c), and demonstrate it has the sufficient authority and technical capacity to conduct reviews of such plans (as assessed by HHS under § 155.1051(e)), prior to HHS determining that a State has as an Effective ECP Review Program. We stated that this would mean an FFE State would not be permitted to elect to conduct ECP certification reviews for only network plans and not non-network plans, if they certify such plans, or vice versa. However, we noted that if an FFE State notifies us that it does not deem to certify such non-network plans, and consequently not offer these plans altogether through the FFE operating in their State (regardless of if the State or HHS conducts the review), then we would continue to review whether a State meets all applicable criteria for only network plans during the Effective ECP Review Program determination process. We sought comment on this approach. Lastly, we stated (91 FR 6414) that similar to the approach for network plans, if FFE States do not satisfy criteria for having an Effective ECP Review Program, then we would perform ECP certification reviews for non-network plans under the proposed standards for non-network plans at § 156.236 discussed in section III.E.12.c. of the proposed rule.
Furthermore, we stated that we believe HHS should primarily conduct ECP certification reviews as the default approach for issuers with non-network plans applying for certification as a QHP to be offered through an FFE, including States performing plan management, except if an FFE State elects to conduct ECP certification reviews and is determined to have an Effective ECP Review Program. We stated that we believe this is valuable for most of the same reasons that we proposed to adopt this same approach for network plans under section III.E.11.c. of the proposed rule. In addition, as we stated in discussions above describing various characteristics of non-network plans, we stated that there is no guarantee that a non-network plan's benefit amount is actually sufficient to cover the provider's full charges, which can leave enrollees with additional out-of-pocket costs that may disproportionately challenge low-income, medically underserved populations. We noted that these populations typically served by ECPs are often at a greater risk for lower health insurance coverage literacy and an increased risk for illness,[337]
which may make it more difficult for these populations to understand how to use non-network plans to meet their needs. Additionally, we noted that the health care services furnished by ECPs are much more specialized and can be very expensive for enrollees, for example, HIV/AIDs treatment furnished by Ryan White program providers, cancer care furnished by Free-standing Cancer Centers, tuberculosis treatment furnished by Tuberculosis Clinics, hemophilia treatment furnished by Hemophilia Treatment Centers, and more.[338]
Thus, we stated that if a non-network plan's benefit amount is not sufficient to cover these expensive, specialized services often furnished by ECPs, then these enrollees could potentially face larger out-of-pocket costs that are more regressive for low-income, medically underserved populations. We stated that this necessitates some minimum standard to ensure these plans are as consumer protective as possible for the low-income, medically underserved populations traditionally served by ECPs, including criteria under proposed § 155.1051 to ensure FFE States have the authority and technical capacity to conduct these ECP certification reviews in a such a way that continues to ensure low-income, medically underserved populations have adequate access to ECPs through non-network plans.
Additionally, we stated that based on our experience conducting ECP certification reviews of network plans, we believe having adequate and accurate data on available ECPs in a geographic area, sufficient tools to collect and calculate issuer submitted ECP data, and sound methodologies to quantitatively assess this data to ensure access to ECPs in accordance with section 1311(c)(1)(C) of the Affordable Care Act would be crucial for any FFE State to demonstrate the technical capacity to also conduct their own ECP certification reviews of non-network plans. We stated that this would include
( printed page 29767)
having data collection capabilities and structured analyses to measure the adequacy of a non-network plan in providing access to a sufficient number and geographic distribution of ECPs in their service area that accept the plan's benefit amount as payment in full. We noted that while existing resources (for example, the Federal ECP List, MPMS, etc.) at the Federal level can be leveraged to efficiently conduct ECP certification reviews of non-network plans, it is unknown what tools FFE States may utilize to collect ECP data from non-network plans or to assess adequate access to ECPs within these plans. Further, we stated that it is especially unclear to what extent FFE States may already have experience in conducting reviews of non-network plans and what existing requirements States may have in place to ensure these plans provide reasonable and timely access to ECPs. Thus, to broaden our knowledge in this area, we solicited comment on whether FFE States, including States performing plan management, have experience conducting reviews of non-network plans; and we welcomed any information on current State-specific requirements that would ensure these plans provide reasonable and timely access to ECPs to medically underserved and low-income populations, including those ECPs that would accept a non-network plan's benefit amount as payment in full.
Moreover, we proposed that an FFE State would need to demonstrate that it meets applicable criteria for both network plans and non-network plans under proposed § 155.1051(b) through (d), and the sufficient authority and technical capacity to conduct reviews of such plans (as assessed by HHS under § 155.1051(e)), to receive a designation as having an Effective ECP Review Program under proposed § 155.1051, as they decide to certify such plans. We stated that this would mean that an FFE State would not be permitted to elect to conduct ECP certification reviews for only network plans and not non-network plans, or vice versa. We stated that we believe this is important for several reasons. We stated that some QHP issuers may choose to offer both network and non-network plans and centralizing the reviews to either the FFE State or HHS for the same issuer would reduce administrative inefficiencies that may result when FFE States and HHS have to coordinate ECP certification review results across a range of plans that may be offered by the same issuer.
Additionally, we stated (91 FR 6415) that we believe delegating reviews of both network and non-network plans to either the FFE State or HHS would allow both plan types to undergo consistent, standardized reviews conducted by the same reviewing entity, so that similar requirements and methodologies are applied fairly across all plan types to reduce differences in ECP certification review results. We stated that this may also reduce variabilities in access across the FFE State between enrollees in non-network plans versus network plans that may result if these plans undergo different levels and types of ECP certification reviews by separate review entities, and it could make it more difficult to effectively compare ECP review results between network and non-network plans during certification if alternative review methods are applied within the same FFE State. We noted that under our proposal, non-network plans must still ensure sufficient access to ECPs in a manner consistent with section 1311(c)(1)(C) of the Affordable Care Act and must be held in parity with network plans to provide reasonable and timely access to ECPs.
Accordingly, we proposed requirements at § 155.1051 that an FFE State must meet to be considered to have an Effective ECP Review Program and conduct ECP certification reviews of non-network plans. We proposed that an FFE State must demonstrate that it has sufficient authority and the technical capacity to conduct ECP certification reviews of non-network plans by meeting all the applicable criteria to be considered to have an Effective ECP Review Program under § 155.1051, including criteria specific to non-network plans. We stated that we continue to believe that to protect low-income, medically underserved populations, and to ensure that enrollees in all FFEs are provided a minimum standard of consumer protection for reasonable access to providers and that disparities in access are minimized across States, Effective ECP Review Program States must continue to demonstrate that issuers without a network of providers applying for certification as a QHP through the FFE operating in their State meet various requirements described in this section. We proposed under § 155.1051(b) that FFE States with an Effective ECP Review Program must ensure that a non-network plan applying for certification to be offered as a QHP through an FFE demonstrates that it provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full to ensure that services will be accessible without unreasonable delay. We stated that in lieu of the requirements for network plans that are based on contracts executed with and/or offered to an ECP, non-network plans would instead be required to indicate benefit amounts as payment in full that were accepted by and/or offered to an ECP, as reflected under proposed § 156.236(b)(1) through (b)(3). Thus, under § 155.1051(c), we proposed that FFE States with an Effective ECP Review Program must also demonstrate that their ECP requirements are comparable to ECP requirements under proposed § 156.236 for issuers' plans without a provider network so that plans: meet the minimum percentage requirements under proposed § 156.236(b)(1) for non-network plans; meet the Indian health care provider requirement under proposed § 156.236(b)(3) for non-network plans; and meet the category per county requirements under proposed § 156.236(b)(2) for non-network plans. Similarly, we stated that our proposal under § 155.1051(d) would also apply to non-network plans. Specifically, we proposed that FFE States with an Effective ECP Review Program that have alternative ECP requirements, including ECP requirements specific to non-network plans, compared to those requirements described under proposed § 155.1051(c)(1) through (c)(3), must demonstrate how their requirements would continue to promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs, and an adequate level of service for low-income enrollees or individuals residing in Health Professional Shortage Areas. We stated that we understand that due to the newness of these plans, if this proposal were finalized, many FFE States would still be in the earlier stages of implementing new requirements for these plans. Thus, we stated that we would continue to work with FFE States to provide technical assistance to ensure any State ECP requirements (including alternative requirements) for non-network plans continue to ensure reasonable and timely access to ECPs across the State before and after making an Effective ECP Review Program determination.
Furthermore, consistent with the discussion in section III.E.11.c. of the proposed rule for network plans, we stated that we would review information submitted by the FFE State to ensure the State receives adequate issuer data and documentation to conduct an examination of ECP requirements described in proposed
( printed page 29768)
§ 156.236 for non-network plans to demonstrate it has the authority and technical capacity to conduct effective, timely reviews of a non-network plan's ECP data. Under §§ 155.1051(e)(1) through (10), as described in section III.E.11.c of the proposed rule, we proposed factors that we would consider in our review to determine if an FFE State has an Effective ECP Review Program, including factors related to a State's legal authority, State ECP requirements compared to ECP requirements under § 156.235 and proposed § 156.236, definition of an ECP, process for identifying qualified ECPs, data collection systems and methodologies to collect and review ECP data, delegation of ECP review to other entities, compliance and enforcement mechanisms, and consumer assistance. We stated that we would still consider all these criteria when determining if an FFE State has sufficient authority and the technical capacity to conduct ECP certification reviews including for non-network plans.
However, we noted that there are several additional criteria we would consider during our review of FFE States specific to only non-network plans. First, we proposed under § 155.1051(e)(5) that we would consider if the FFE State utilizes the Federal ECP List or has a process they use to identify qualified ECPs that may accept a non-network plan's benefit amount as payment in full. We stated that we believe it is essential to have a means to identify the exact geographic location and distribution of ECPs that may be available within an issuer's service area that may accept a non-network plan's benefit amount as payment in full; we noted that this would ensure issuers fulfill statutory requirements under section 1311(c)(1)(C) of the Affordable Care Act to include ECPs “where available” so that enrollees have sufficient access to ECPs through their plans. Additionally, we proposed to consider under § 155.1051(e)(7) whether the FFE State collects information from issuers regarding the status of offers of benefit amounts as payment in full to an ECP. We stated that we believe this type of data is an important metric to assess an issuer's compliance with the minimum percentage, category per county, and Indian health care requirements under proposed § 156.236(b)(1) through (b)(3), which would be evaluated based on measurements of benefit amounts as payment in full that were offered to or accepted by an ECP.
Moreover, as we stated under section III.E.11.c of the proposed rule, we noted that States possess unique knowledge on local factors that could strengthen ECP reviews, such as on market conditions, geographic constraints, areas in the State with limited economic resources, provider shortages, workforce issues, and population demographics, and we stated that we believe States can leverage this same knowledge on local factors when conducting ECP reviews of non-network plans. However, we considered enumerating the information that non-network plans must submit to the FFE listed at § 156.236(b)(4) through (b)(9) as requirements for FFE States with an Effective ECP Review Program to review non-network plans to ensure they are in alignment with HHS' proposed approach in an effort to further support consumer protectiveness in this novel plan design. We stated that information described under proposed § 156.236(b)(4) through (9) is specific to non-network plans and reflect additional safeguards to ensure these plans maintain access to providers without traditional network arrangements. We noted that these factors would include assessing a non-network plan's strategy for conducting outreach to ECPs in their area and for making benefit amounts public to enrollees, methodologies for determining benefit amounts, strategy for publishing consumer-friendly information on balance billing and potential out-of-pocket costs, availability of exceptions processes for enrollees unable to locate providers who accept benefit amounts as payment in full, and customer services resources. We stated that these reflect more qualitative measures that would likely require different data collection methods compared to the more quantitative measures of minimum percentage, category per county, and Indian health care requirements under proposed § 156.236(b)(1) through (b)(3). We further stated that, as HHS is seeking to broadly restore flexibilities to FFE States as a part of ECP certification reviews and empower FFE States who understand their consumer needs and local conditions best, we opted to defer to FFE States in how they wish to review non-network plans for this type of information, as applicable. Though, we sought comment on whether HHS should better align the reviews of non-network plans across the FFE, regardless of whether HHS or an FFE State is conducting ECP certification reviews, by enumerating the factors under §§ 156.236(b)(4) through (b)(9).
Altogether, in addition to the proposal to revise §§ 156.230 and 156.235, and add §§ 156.236 and 155.1051, we proposed revisions to §§ 155.1050 (including its section heading), 156.275, and 156.810 to clarify that provisions within these sections would apply to the certification of non-network plans in the same manner that they apply to network plans.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy with a modification to delay implementation of this proposal to PY 2028. We are also modifying § 156.236(b)(5) to include the non-network plan's strategy for regularly updating any changes to benefit amounts, § 156.236(b)(7) to include the non-network plan's strategy for providing information on navigating episodes of care with multiple benefit amounts (including for ancillary providers and services), and § 156.236(b)(9) to include the non-network plan's strategy to assist plan enrollees in receiving real-time cost estimates prior to care being furnished, as information non-network plans must submit to the FFE for a determination that it provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full.
Lastly, we clarify that the finalized non-network plan requirements under § 156.236 are applicable to issuers with non-network plans seeking QHP certification to be offered on the FFE. We are not requiring FFE States to offer non-network plans on the FFE within their State, nor are we requiring States operating their own Exchanges to certify and offer these plans. States retain full discretion and authority to determine whether non-network plan designs are appropriate for their markets, consistent with applicable State laws and regulations. The requirements under § 156.236 lay out a clear regulatory framework that HHS will apply to conduct certification reviews of issuers with non-network plans seeking to be certified as a QHP on the FFE. States operating their own Exchanges (State Exchanges and SBE-FPs) are welcome to use the principles of this framework but have flexibility to determine the specific parameters for non-network plan certification requirements within their State, provided they ensure issuers provide sufficient access to providers consistent with standards under § 156.236(a). While HHS is delaying implementation of allowing non-network plans to receive QHP certification to be offered as QHPs through the FFE beginning PY 2028,
( printed page 29769)
SBEs and SBE-FPs retain full discretion and authority to determine the appropriate implementation timeline for their States if allowing non-network plans to be offered through State Exchanges. Accordingly, and consistent with finalized requirements under § 155.1050(a)(2), State Exchanges and State-based Exchanges on the Federal Platform may allow non-network plans to be offered through the Exchange for plan years beginning on or after January 1, 2027, if such plans are allowed to be offered through the Exchange, as applicable.
Comment:
Multiple commenters stated support for the proposal, including an issuer that offers non-network plans, multiple consumers currently enrolled in non-network plans outside of the Exchange, and employers that offer non-network plans to their employees. These commenters believe non-network plans provide Americans an opportunity to benefit from greater provider choice, transparency, affordability, and additional innovative plan design options through the FFE. They commended HHS for revisiting the existing prohibition of non-network plans and proposing a thoughtful regulatory framework under § 156.236 that addresses core statutory provisions while fostering required consumer protections. These commenters supported the proposed regulatory standard and stated the nine proposed factors (under § 156.236(b)(1) through (b)(9)) under which non-network plans would be assessed for QHP certification were reasonable, comprehensive, and appropriate.
Current non-network plan enrollees shared their positive experiences in relation to finding and receiving care under their plans. These commenters appreciated that their plan offered choice of any provider without referrals and prior authorization requirements as well as transparent information on the cost, quality ratings, availability, and location of providers to support cost-conscious, informed decision-making. Some commenters shared positive experiences utilizing their non-network plans to receive specialty care (for example, cancer care), including the receipt of specialized treatments and medications without delay, denial, or restriction contingent on provider network participation. Some commenters pointed to non-network plans as a viable solution to the current limitations of existing provider networks, including narrow networks and inaccuracy in provider directory information.
Response:
We thank commenters for their support and current enrollees of non-network plans for sharing their experiences.
Comment:
The majority of commenters stated significant opposition to the proposal to allow non-network plans to receive QHP certification, especially if HHS does not finalize additional, enforceable consumer protections beyond those proposed under § 156.236. Commenters were skeptical that a non-network plan could truly offer the comprehensive coverage required for QHP certification as a QHP. They were concerned these plans function to only discount health services, resulting in illusionary coverage that instills additional uncertainty and distrust among consumers. Some commenters stated that removing HHS' existing prohibition on non-network plans would stray from Congress' original intentions in drafting access to care provisions in the Affordable Care Act, weakening its core protections, undermining program integrity, risking market instability, and shifting additional risks to patients and providers.
Furthermore, several commenters stated that suggested savings from price transparency efforts and related policies would be small, as limited evidence demonstrates uptake of price transparency efforts by consumers and compliance against providers is limited in practice, and other systemic issues exist in the health care system that reduce the effectiveness of price transparency efforts. Commenters suggested that HHS focus on other activities to address these issues. For example, commenters urged HHS to develop stronger price transparency guidelines on “Good Faith Estimates” under the No Surprises Act and improve how providers display standard charges which often reflect an average of negotiated prices, so that price transparency information can be trusted. Commenters also urged HHS to develop a Federal all-payer claims database, so that nationwide price transparency information would be accessible across markets and to consumers enrolled in different plan types. Commenters also supported stronger legal requirements that target barriers limiting cross-data exchange on pricing information between billing departments at the provider and insurer level.
Response:
We do not agree that allowing certification of non-network plans as QHPs would stray from the Congress' intent in creating access to care provisions within the Affordable Care Act, and we refer readers to discussion earlier in this section explaining why. We believe that so long as non-network plans demonstrate a sufficient choice of providers consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act and satisfy all other applicable statutory and regulatory provisions, then non-network plans would not circumvent access to care provisions and the responsibility to provide comprehensive coverage. Under section 1311(e)(1) of the Affordable Care Act, Exchanges have broad discretion to deny certification of a health plan if the Exchange determines offering the plan is not in the interest of qualified individuals and qualified employers in the State or States in which such Exchange operates. We have previously clarified we would focus denials of certification in the FFEs based on cases involving the integrity of the FFEs and the plans offered through them (81 FR 12289). In the event a non-network plan meets certification requirements, but we determine that the plan is not in the interest of qualified individuals and employers or risks the integrity of the FFEs and the plans offered through them, we have authority to deny QHP certification of the non-network plan.
Lastly, we recognize that systemic issues exist in the health care system that currently could limit the full potential of price transparency initiatives. While we appreciate commenters' suggestions of other activities we could pursue to improve pricing information for consumers, these suggestions were outside the scope of this rulemaking as they do not relate to our specific proposal. However, we do believe a combination of various solutions would have the most systemic impact on price transparency, which we believe includes the availability of non-network plans. Since non-network plans often present transparent price information to their enrollees by making benefit amounts and providers' acceptance of those benefit amounts available, these plans can promote additional price transparency if plans compete by implementing more transparent price information to attract price-sensitive consumers. Non-network plans may further encourage providers to lower prices to attract enrollees shopping for care who would have access to compare providers' acceptance of benefit amounts and health care prices in their service area. Several factors relevant to the non-network plan regulatory framework promote an ecosystem which we believe will further encourage price transparency efforts, including those under § 156.236(b)(4) through (9) which include making benefit amounts publicly available, the methodology for determining benefit amounts, provider outreach to
( printed page 29770)
determine whether providers would accept the benefit amount as payment in full, the strategy for providing information about potential balance billing scenarios, including historical data on actual out-of-pocket costs incurred by enrollees, and providing adequate customer services to assist consumers in finding providers who will accept the plan's benefit amount as payment in full. Overall, these factors ensure non-network plans make the cost of care more transparent to consumers. We also believe that allowing non-network plans to be certified as QHPs on the FFEs, provided they meet all applicable requirements, would provide innovative plan options to consumers who value price transparency.
Comment:
One commenter suggested that instead of allowing non-network plans to be offered as QHPs, which allow the choice of any provider, HHS should strengthen network adequacy standards to ensure consumers have more choice of adequate providers through broader networks. Some commenters added that allowing these non-network plans would undercut long-standing initiatives to improve provider directory accuracy and hold issuers accountable for meeting provider network regulatory requirements. Commenters advocated for HHS to shift attention towards resolving these systemic issues instead.
Response:
We agree with commenters that network adequacy requirements and the accuracy of provider directories are important. While we appreciate and will consider commenters' suggestions to focus on these efforts, we do not believe there is a single solution to improve a consumer's choice of providers. Although a number of suggestions were outside the scope of this rulemaking, we appreciate commenters' attention and feedback. We will continue to pursue efforts to improve the adequacy of plan networks, including by finalizing network adequacy policies in this final rule that will allow FFE States to apply their superior knowledge of circumstances in their States to assess the adequacy of issuer networks, and maintaining existing ECP threshold requirements. For the reasons explained earlier in this final rule, we are of the view that allowing non-network plans to be certified as QHPs, provided they meet all applicable requirements, will promote more options in the types of plan designs offered through the FFE, especially for consumers who do not prefer traditional network plans.
Comment:
Commenters stated concern that non-network plans would unfairly shift administrative work from issuers to consumers—such as locating providers that accept benefit amounts as payment in full, negotiating prices, disputing charges, covering up-front costs, navigating reimbursements, handling prior authorization, and submitting supporting documentation for needed services—while issuers retain the financial benefits of reduced administrative costs that consumers assume. Commenters also were uncertain that online tools would be available to provide consumers information on locating providers and the full prices for their services.
Many commenters noted that consumers cannot predict all the medical services (for example, tests, procedures, referrals, drugs, etc.) they will need prior to the point of care, making it difficult to evaluate whether a non-network plan would meet their health care needs before enrolling in a non-network plan. Commenters explained that this uncertainty is particularly problematic for patients with serious, chronic, or disabling conditions, whose care is ongoing, expensive, and reliant on continuity of care with specific providers; and, these patients are unlikely to compare services from different providers while managing their illness.
Commenters also highlighted that the existing healthcare system is already complex, with many consumers—particularly those with language barriers, chronic conditions, low-income individuals, and caregivers—lacking health literacy and subsequently struggling to navigate covered benefits, formularies, diagnosis and procedure codes, claims processing and utilization management. They stated a non-network plan would add further confusion to an already burdensome system and risk consumers failing to understand the fundamental differences between network and non-network plans during plan selection.
Response:
While we appreciate commenters raising concerns related to potential burdens consumers may face in navigating non-network plans, this proposal neither discontinues network plans on the FFE nor encourages QHP issuers to cease offering them. We acknowledge that non-network plans may not suit every consumer and that many consumers will continue to prefer network plans. However, some consumers may prefer the flexibility of not being limited to a specific provider network and may wish to be more engaged in searching for and managing their care costs. This proposal is intended to expand plan design choices available on the FFE. As evidenced by commenters currently enrolled in and employers offering non-network plans, this plan design can offer meaningful transparency, choice, and quality for consumers, and, for those reasons and other reasons explained in this section of this final rule, should therefore be available as an option on the FFE.
Moreover, we support ensuring that clear information about non-network plans—including their benefits, risks, and how to utilize these plans to meet health needs—is available to consumers prior to enrollment. We aim to clearly identify and differentiate non-network plans during plan selection to support informed consumer decision-making and ensure consumers understand the administrative tasks they must take on should they choose to enroll in a non-network plan. To address commenters' concerns regarding the effort required to navigate these plans, potential confusion over this novel plan design, and uncertainty about meeting unpredictable medical needs, we are finalizing, with modifications, multiple provisions to promote adequate consumer support. These provisions require non-network plans to make benefit amounts for services publicly available, provide consumer-friendly and publicly-available information on expected out-of-pocket costs, make an exceptions process available to enrollees who cannot find providers willing to accept the benefit amount as payment in full, and provide adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers in their area who will accept the plan's benefit amount as payment in full. We further expect that non-network plans should provide consumers with relevant information related to claims submission, understanding costs, comparing price information, documentation requirements, and all other administrative processes consumers may expect when using a non-network plan consistent with information requested under § 156.236(b). As part of the QHP certification data submission process, non-network plan issuers will also be required to provide URLs that make benefit amounts publicly available, ensuring consumers have adequate information enabling them to understand the price of services and locate providers who will accept the plan's benefit amount as payment in full.
Comment:
Most commenters opposing this proposal raised concerns that non-network plans could impose additional out-of-pocket costs and balance-billing risks on consumers. Without provider networks and predetermined levels of
( printed page 29771)
cost-sharing for in-network providers, commenters reasoned that enrollees in non-network plans may face unforeseen out-of-pocket costs when a provider does not accept the plan's benefit amount as payment in full. One commenter stated that simply requiring non-network plans to provide information on potential balance billing scenarios and expected out-of-pocket costs does not protect against balance-billing. Another commenter added that consumers choosing plans on the FFE should not be expected to absorb such disclosures. Commenters were concerned these balance-billing risks would be high for those with complex medical needs, limited health literacy, those that rely on ECPs, and rural residents that may have a limited subset of providers accepting the benefit amount as payment in full.
Commenters further conveyed that unforeseen medical costs could be substantive for those receiving expensive specialty therapies, seeking emergency care, and those not accounting for additional charges of ancillary providers or services that may not accept the benefit amount as payment in full (for example, assistants, anesthesiologists, surgeons, pathologists, radiologists, diagnostic imaging, outside laboratories, laboratory tests, etc.). One commenter recommended that HHS require plans to ensure that the benefit amount as payment in full is accessed across all rendered services and providers involved in a covered episode of care, as long as the primary provider agreed to accept the benefit amount as payment in full.
Commenters also requested additional clarification on how non-network plans would satisfy applicable provisions of the No Surprises Act, and some posited that non-network plans may be incompatible with provisions of the No Surprises Act. However, one issuer that currently offers non-network plans stated that these plans are indeed subject to the No Surprises Act and comply with all applicable provisions, including provisions related to emergency and air ambulance services. The issuer stated that enrollees would not be subject to balance billing for these services and that providers would have access to independent dispute resolution processes.
Response:
We recognize there are situations where an enrollee may seek services from a provider that does not accept the benefit amount as payment in full, and to which the enrollee may be responsible for charges exceeding the benefit amount. These circumstances, however, are common in the individual insurance market in network plans, including if consumers knowingly receive services from out-of-network providers while receiving some benefits from their plan, in circumstances where the No Surprises Act does not apply. Nevertheless, non-network plans have a responsibility to provide sufficient resources to ensure enrollees understand out-of-pocket costs prior to receiving care to limit charges exceeding the benefit amount. We are finalizing, as proposed, that a non-network plan does not provide access to a range of providers by simply providing some benefit amount for covered services rendered by any provider without providing the Exchange any other contextual information. If a non-network plan does not offer access to range of providers that accepts the non-network plan's benefit amount as payment in full consistent with § 156.236(a), including due to insufficient benefit amounts that result in out-of-pocket costs exceeding the benefit amount, then the non-network plan would not meet all the necessary certification requirements.
In addition to this provision, we proposed multiple provisions under § 156.236 to ensure non-network plans provide adequate support to consumers, including by making benefit amounts publicly available (§ 156.236(b)(5)), providing consumer-friendly and public information on expected out-of-pocket costs (§ 156.236(b)(7)), making an exceptions process available to enrollees who cannot find providers willing to accept the benefit amount as payment in full (§ 156.236(b)(8)), and providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers in their area who will accept the plan's benefit amount as payment in full (§ 156.236(b)(9)). For the reasons stated earlier in this section of this final rule, we believe these additional provisions will ensure issuers provide clear information and resources so that enrollees understand potential out-of-pocket costs prior to receiving care and would be aware of any charges exceeding the benefit amount.
Furthermore, non-network plans that are applying for QHP certification will be required to structure their plans so that they provide all the consumer protections that apply to individual and small group health coverage including, but not limited to, those specified in PHS Act, title XXVII, parts A through D, as all other plans applying for QHP certification are subject to providing. A non-network plan will not be exempt from providing such protections to its enrollees merely because it does not contract with providers, and failure to offer these protections would result in denial of certification in accordance with § 155.1000(e) and decertification in accordance with § 155.1080(c). Additionally, as we have previously stated, HHS, as the operator of the FFE, has broad discretion to determine whether a plan is in the interest of qualified individuals and qualified employers, regardless of whether the plan meets other minimum certification requirements consistent with § 155.1000(c)(1). Thus, we believe our authority to deny certification of a non-network plan applying to be offered as a QHP on the FFE under the interest standard extends to determinations that a non-network plan's benefit structure fails to provide protections against surprise medical bills in a manner like a network plan.
Moreover, commenters requested additional clarification on how non-network plans would be required to comply with applicable provisions of the No Surprises Act. The Departments of Health and Human Services, Labor, and the Treasury have previously issued guidance stating that the surprise billing provisions of the No Surprises Act apply to plans and issuers that do not have a network of providers with respect to emergency services and air ambulance services.[339]
The Departments stated that the provisions that limit cost sharing for out-of-network emergency services apply if a plan or issuer provides or covers any benefits for emergency services and the services are provided by a nonparticipating provider or nonparticipating emergency facility. Similarly, the provisions that limit cost sharing for out-of-network air ambulance services apply if a plan or issuer provides or covers any benefits for air ambulance services and those services are provided by a nonparticipating provider of air ambulance services. The Departments explained that the definitions of nonparticipating provider or nonparticipating emergency facility (as provided in 45 CFR 149.30), and the protections afforded to participants, beneficiaries, or enrollees related to emergency services and air ambulance services, are not dependent on whether the group health plan or group or
( printed page 29772)
individual health insurance coverage has a network of providers.
However, provisions of the No Surprises Act that prohibit balance billing and limit cost sharing for non-emergency services apply only to services provided by a non-participating provider with respect to a visit to a participating health care facility. A participating health care facility is health care facility that has a contractual relationship with a plan or issuer, directly or indirectly, setting forth the terms and conditions upon which the relevant item or service is furnished to the participant, beneficiary, or enrollee under the plan or coverage.[340]
Therefore, the provisions that limit cost sharing and prohibit balance billing for non-emergency services provided by nonparticipating providers with respect to a visit to certain types of participating facilities would never be triggered if a plan or coverage does not have a network of participating facilities and thus no contractual relationship with such facilities.[341]
However, we note that all non-network plans must provide all the same consumer protections that apply to individual and small group health insurance, including those in PHS Act title XXVII parts A through D. These protections include the exceptions and appeals processes for non-covered services and benefit determinations.
Nevertheless, we believe that the concerns raised by commenters require additional consideration. For example, the concerns stated by commenters pertaining to episodes of care that may trigger multiple benefit amounts that consumers could not reasonably anticipate prior to receiving care warrants additional consideration. This includes care by ancillary providers (for example, diagnostic services, laboratory services, radiology, pathology, anesthesiology, etc.). We believe that it is a common occurrence that when a consumer visits a provider for a health concern or complaint, ancillary services may be required in the recommended course of treatment. A consumer being able to recognize the need for ancillary services likely requires a level of advanced medical knowledge that is more appropriate for providers. The selection of ancillary providers and services are often determinations made during a clinical episode and driven by real-time clinical decision making and medical necessity (for example, a surgical patient utilizing anesthesia or pathology services during an operation). In this example, the patient may be unable to assess if the anesthesiologist and pathologist accepted the benefit amount as payment in full prior to or during the surgery. Therefore, it would not be reasonable for a patient to anticipate ancillary providers and services as these are often determined by the provider (for example, the surgeon) and not known in advance. For this reason, we are finalizing additional language at § 156.236(b)(7) to promote additional consumer protection by ensuring non-network plans have a strategy for providing consumer-friendly information to enrollees on navigating episodes of care with multiple benefit amounts (including for ancillary providers and services). This information is important so that non-network plans can assist enrollees in avoiding balance billing and additional out-of-pocket costs beyond their control when receiving care that may trigger multiple benefit amounts that could not be reasonably anticipated. However, considering the novelty of these plan types, and the related complexity associated with potential out-of-pocket costs and balance billing scenarios, we will continue to consider if additional regulatory refinements around consumer protections are necessary and welcome recommendations.
Comment:
Commenters raised additional concerns regarding the potential impact of non-network plans on providers, including rural and safety net providers (such as ECPs), hospitals, emergency departments, and independent physician practices. Commenters believed that providers may face pressure to accept benefit amounts from enrollees of non-network plans without the ability to negotiate directly with the plan, especially in markets where Exchange enrollment represents a large share of patient volume. Commenters stated that this may then lead to increased uncompensated care, financial assistance spending, and downstream public costs. Commenters also stated that rural hospitals and clinics already operate on thin margins, and independent physician practices lack the support of larger systems that can cross-subsidize losses, thus risking facility closures.
In addition, commenters stated that without direct insurer-provider exchanges within a non-network plan, providers would experience less predictability and fewer estimates on patient volume in advance. Some commenters also stated concerns that if patients, especially those in need of specialty care, cannot regularly locate providers willing to accept the plan's benefit amount as payment in full, then more care could shift to safety-net providers and emergency departments that are obligated to treat patients regardless of insurance status or ability to pay. Some commenters shared concerns that, over time, a non-network plan could impact trust between providers and consumers if such plans lead to disputes (including disputes in court) between patients and providers on billing, eligibility, payment sufficiency, and coverage; and that these disputes could be mitigated through provider and insurer contracting.
In contrast, an insurer currently offering a non-network plan stated that providers had positive experiences with the plan due to increased freedom to treat patients without restrictions caused by prior authorization, step-therapy protocols, and formulary restrictions, along with the prompt payment upon rendering services.
Response:
Commenters raised important concerns; however, many of these issues, such as provider financial pressure due to plan payment amounts, uncertainty in patient volume, and billing disputes between providers and patients, are already well-documented systemic issues across plan types and are not specifically tied to non-network plans. For example, safety net providers and independent practices already face disproportionate financial strain, including higher levels of uncompensated care and risk for closure, influenced by broader payment structures across public and private payers and not necessarily by network design.[342]
And, disputes already exist between patients and providers influenced by poor good faith estimates, incorrect coding, and balance billing.
We acknowledge the concerns from providers that they may be influenced to accept the benefit amount as payment in full without an ability to directly negotiate with the non-network plan, and the impacts this may have on rural and safety net providers. However, it is our understanding that non-network plans perform comprehensive research prior to setting benefit amounts, as would any other network plan prior to negotiating payment rates. This includes directly gathering pricing information from providers, leveraging both Medicare and private payor rates, utilizing publicly available data, identifying regional factors to adjust for health care prices, and reviewing
( printed page 29773)
existing medical codes. Thus, we believe non-network plans' benefit amounts would be developed in a way that takes the current market and health care prices accepted by providers into consideration, such that benefit amounts are developed so enrollees can reasonably access providers in their service area that accept the benefit amount as payment in full.
We cannot require that providers accept a network agreement from an issuer; likewise, we cannot require that providers accept a non-network plan's benefit amount as payment in full. If there is not a sufficient choice of providers, including specialty care, available in an enrollee's service area that agree to accept the benefit amount as payment in full, then a non-network plan could not reasonably satisfy the proposed regulatory requirements under § 156.236, in which case we would not certify a non-network plan as a QHP to be offered through the FFE. Likewise, State Exchanges and SBE-FPs allowing non-network plans to be offered on their Exchanges may deny QHP certification to a non-network plan in this circumstance for not meeting requirements under § 156.236(a) to ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full consistent with § 155.1050(a)(2). We also acknowledge concerns that providers would experience less predictability and fewer estimates on patient volume in advance without direct insurer-provider interactions in non-network plans but remind commenters that the existence of non-network plans in their area by no means precludes the existence of network plans. As most plans have traditionally operated with a provider network, and these plans are likely most familiar to consumers, we expect many consumers will continue to enroll in network plans, and providers may continue to contract with network plans as they see fit, which may provide more certainty regarding expected patient volume for providers for whom this is a concern. We also understand concerns providers may have in potential erosion of trust with consumers over potential billing disputes. If a provider understands a consumer is enrolled in a non-network plan, we recommend that the provider communicate expected costs clearly with consumers, as they would with self-pay or uninsured individuals.
Though we acknowledge provider concerns with our proposal, there are also potential benefits to providers related to non-network plans, including increased freedom to treat patients without restrictions caused by prior authorization, step-therapy protocols, and formulary restrictions, along with the prompt payment upon rendering services, as verified by the one commenter providing non-network plans and based on our research into non-network plans. We believe some of these benefits may also reduce billing disputes experienced between providers and issuers when services are not covered and impact treatment due to these restrictions.
Comment:
Several commenters shared feedback on whether non-network plans would reduce health care costs, including administrative costs. Some commenters did not believe non-network plans would reduce overall health care costs, stating that providers may be incentivized to charge any payment amount for services without the safeguards of network contract agreements whereby providers and insurers agree in advance to negotiated, pre-determined rates that make care the least expensive for consumers seeing in-network providers. Commenters were uncertain that a non-network plan's benefit amounts would actually be sufficient, and that providers may not necessarily be obligated to accept the non-network plan's benefit amount and could change prices at any time, absent a contract with a plan. Other commenters shared that non-network plans would not meaningfully reduce health care costs but offload costs and responsibility to providers and patients, while allowing non-network plans to potentially evade accountability to secure access to care and control costs for consumers. Though, a different commenter did not believe a non-network plan would avoid administrative costs, since they would need to implement processes to verify a benefit amount as payment in full was accepted by providers and identify new solutions to monitor claims submitted by providers that they do not contract with. Commenters also stated concerned that non-network plans may drive patients into more expensive, less appropriate care settings that lead to avoidable spending and an inefficient use of taxpayer dollars that maximize the insurer's financial return via collected premiums and subsidies.
However, one consumer enrolled in a non-network plan shared that they switched to a non-network plan after previously experiencing an increase in premiums within a network plan, leading to a reduction in premium costs within the non-network plan. Another commenter thought both patients and providers would experience administrative cost savings resulting from no network limitations or prior authorization, leading to care that is not subject to administrative delays. In contrast, another commenter did not believe a non-network plan would produce enough administrative cost savings that would allow for enrollees to receive larger premium reductions.
Response:
We understand that commenters may be concerned with the potential for providers to set higher payment amounts without the influence of a network plan's pre-negotiated payment rates. However, we cannot dictate rates providers must accept or set. For the reasons stated earlier in this final rule, we believe that the structure of non-network plans, in which consumers are “shopping” for health care and potentially negotiating costs directly with providers, has potential to create a more competitive environment for health care services and discourage providers from setting unreasonably high payment amounts. If a certain provider were to set higher payment amounts due to the existence of non-network plans in their service area, an enrollee may choose to see a different provider with lower payment amounts that would accept the benefit amount as payment in full. In addition, non-network plans would be required to make benefit amounts publicly available and accessible to enrollees who can utilize these benefit amounts to compare prices among available providers as they seek care from providers who will accept the plan's benefit amount as payment in full. And, if there were a significant number of providers in an enrollee's service area that do not accept the plan's benefit amount as payment in full (for example, because of setting higher payment amounts for non-network enrollees), the non-network plan would not be able to demonstrate access to a range of providers that accepts the non-network plan's benefit amount as payment in full, which is needed to satisfy requirements under § 156.236. In such a case, the non-network plan would be denied QHP certification by HHS. Likewise, State Exchanges and SBE-FPs allowing non-network plans to be offered on their Exchanges may deny QHP certification to a non-network plan in this circumstance for not meeting requirements under § 156.236(a) to ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full consistent with § 155.1050(a)(2).
While a non-network plan may reduce administrative costs associated with provider network management, we do not believe a non-network plan would evade responsibility to ensure access to care, as again, the non-network plan
( printed page 29774)
must provide sufficient access to providers that accept the non-network plan's benefit amount as payment in full. These plans will be required to establish processes to set reasonable, data-driven benefit amounts and conduct outreach to providers to prove there is a sufficient number of providers that accept the plan's benefit amount as payment in full, as required under the proposed certification requirements. These plans will also be required to provide ample resources to assist enrollees in locating providers who will accept the plan's benefit amount as payment in full consistent with § 156.236(b)(9), and an exceptions process for enrollees who cannot provide providers consistent with § 156.236(b)(8). We also agree with the one commenter stating a non-network plan would not necessarily avoid all administrative costs. This is because non-network plans maintain claims processing technology to track care received by enrollees and reimburse enrollees and/or providers with benefit amounts for covered services, as supported by our preliminary research of existing non-network plans. Lastly, while it is true that non-network plans may save financial resources in not contracting with providers, providers may also benefit from administrative cost savings stemming from not needing to pursue contract negotiations with issuers of non-network plans or to provide documentation to justify the medical necessity of services rendered to enrollees in a non-network plan as part of prior authorization processes as verified by the one commenter currently providing non-network plans and based on our research into non-network plans. In addition, we believe that the reduced administrative costs associated with network contracting activities may be passed on to consumers in the form of reduced premiums, as evidenced by comments shared by current consumers in non-network plans and issuers of non-network plans.
Lastly, while we appreciate commenters expressing concerns that a non-network plan may drive patients to more expensive care settings, we do not believe there is substantive evidence of this claim at this time. Again, we reiterate that we believe the structure of non-network plans, in which consumers are “shopping” for health care and potentially negotiating costs directly with providers, will encourage thoughtful use of health care services by consumers and potentially create a more competitive environment for healthcare services. However, we will monitor consumer complaints from individuals enrolled in these plans to ensure enrollees have access to a range of providers as required under § 156.236(a) and, if appropriate, decertify the plan under § 155.1080(c) or deny certification to the plan under § 155.1000(c)(1).
Comment:
Many commenters conveyed the need to have guaranteed access to providers with certainty. Commenters believed that provider networks with contracted providers offer stable, predictable health coverage at reduced rates for enrollees. Commenters reasoned those guaranteed contracts with providers provide extra financial protection and limit risk at the point of care from potential balance billing. One commenter also stated that without a quantifiable network of providers, access to providers within non-network plans may be difficult to enforce, and consumers need certainty before enrolling in a QHP that a given provider will treat them at the plan's benefit amount. The commenter stated that this certainty is critical, so patients do not enroll in a plan with opaque pricing, ad-hoc provider acceptance, and billing disputes after services are already rendered. Overall, commenters were concerned that allowing certification of non-network plans may take away the incentive for current issuers to sign long-term, stable contracts that may affect overall market stability.
Response:
We agree with commenters that network plans provide both stability and value to enrollees through providers contracted with the network plan that agree to furnish health care services to enrollees at negotiated rates. For this reason, we do not intend to sway consumers towards non-network plans if consumers are satisfied with the benefits a network plan provides. As we have previously stated, we understand that the non-network plan design may not suit every consumer enrolling in a QHP offered through the FFE. Instead, our intention is to offer more choices to consumers in the plan design options available on the FFE, especially since each consumer may have different needs and expectations for their plans. However, we do not believe that network plans necessarily provide guaranteed access to providers for covered services with certainty, as it is common for in-network providers to transition out-of-network without a consumer's awareness or consumers may struggle to find in-network providers within a reasonable time, especially due to provider availability.
For the reasons explained earlier in this section of this final rule, we believe that non-network plans do provide a certain level of guarantee that enrollees can choose a provider of their choice and receive publicized benefit amounts for covered services. So long as non-network plans set benefit amounts in such a way that consumers have access to a sufficient choice of providers within their service area that accept the benefit amount as payment in full, then consumers should be able to locate necessary care while limiting out-of-pocket costs. Non-network plans are also required to make information available regarding exceptions processes for consumers who cannot find providers willing to accept the benefit amount as payment in full, under § 156.236(b)(8) and provide adequate customer service supporting consumers in finding providers who will accept the plan's benefit amount as payment in full under § 156.236(b)(9). We acknowledge commenters' concerns regarding worries that issuers may be disincentivized from signing long-term, stable contracts that may affect overall market stability. However, we do not believe that non-network plans will wholly replace network plans. Many consumers are familiar with, and will prefer to remain in network plans, and issuers will likely continue to offer network plans with contracted providers. Network plans do offer valuable benefits to consumers and should continue to be available through the FFE. However, we will continue to monitor the market for any potential effects on stability. Under § 155.1000(c)(2), like network plans, non-network plans, could be denied QHP certification if it is determined that making available such health plans through such Exchange is not in the interests of qualified individuals and qualified employers in the State. This also applies if non-network plans affect the integrity of plans offered through the FFE, including the availability of network plans.
Comment:
Commenters shared both support and concern for HHS' proposed general requirement under § 156.236(a) that a non-network plan must ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that services will be accessible without unreasonable delay. A few commenters raised concerns that this approach is not enforceable, and that HHS would not be able to verify adequate access until consumers are already enrolled. Commenters believe that this “theoretical access” framework relies on issuers' representations of sufficient access, rather than objective metrics and
( printed page 29775)
verifiable commitments based on provider contracts. Several commenters encouraged HHS to consider including other metrics to measure access to providers under a non-network plan, such as a combination of provider acceptance data, historical claims, binding participation agreements with providers, and other objective indicators showing that enrollees can obtain services within reasonable timeframes and geographic distances. One commenter reasoned that collecting real provider participation data would better measure access to providers rather than HHS requiring non-network plans to demonstrate access to providers through an attestation process. Another commenter requested HHS clarify how the agency will monitor access on an ongoing basis. Overall, commenters believed these alternative measurement approaches would improve the proposed regulatory requirement under § 156.236(a) and strengthen consumer protections to maintain reliable access to providers.
In contrast, an issuer currently offering a non-network plan supported the requirement that non-network plans utilize benefit amounts to indicate enrollees have access to a sufficient range of providers who will accept the benefit amount as payment in full. The commenter added that benefit amounts are currently utilized by non-network plans and that benefit amounts are informed by real-world pricing data, including cash prices, commercial rates, and Medicare fee schedules, to ensure enrollees can access care that is fully covered by the plan.
A few commenters shared that requiring a non-network plan to ensure access to a range of providers, such as providers that specialize in mental health and substance use disorder services, that accept the non-network plan's benefit amount as payment in full would help expand access to behavioral health. Commenters noted that many mental health and substance use disorder providers choose not to contract with insurers, often due to inadequate reimbursement rates or only accept a small number of patients at a lower rate paid by the insurer while reserving the remainder of their appointments for those who pay a much higher cash rate. Another commenter stated that health plans often do not display payment rates for behavioral health providers, thus enrollees may lack information to make an informed choice on which plan may best suit their behavioral health needs.
Response:
We appreciate these comments, including the alternative approaches shared by commenters to improve ways to measure access to care within non-network plans. We continue to believe that measuring access within non-network plans based on providers that accept the plan's benefit amount as payment in full is an acceptable and reasonable data point, supported by the other factors in place for assessing non-network plans and not a purely theoretical framework that cannot verify adequate access until consumers are already enrolled. Under our proposal, to be certified as a QHP on the FFEs, non-network plans must provide information about its assessed percentage of providers that accept the non-network plan's benefit amount as payment in full and whether it meets a minimum percentage of available ECPs that accept the plan's benefit amount as payment in full. It also must detail its methodology for determining benefit amounts and for providing adequate customer service, among other information about the plan's structure that we believe promotes sufficient access to care. It is our understanding, as shared by an issuer offering a non-network plan in the public comments received, that non-network plans have set benefit amounts for covered services informed by various data sources (for example, direct provider engagement, Medicare and private payor rates, regional factors, etc.), and consumers utilize the benefit amount as a reference point for how much they should expect to pay for the receipt of services under the plan.
Regarding concerns about insurers reporting lower payment reimbursement rates compared to actual charges received by consumers for their care, it is our understanding that non-network plans must have a process in place to assess whether a benefit amount was accepted by a particular provider when their enrollee seeks care, and that non-network plans build a repository over time of such providers accepting the benefit amount based on an enrollee's claims, which can inform non-network plans decisions to adjust or increase benefit amounts. To help reinforce this process, we proposed under § 156.236(b)(4) that non-network plans must report their strategy for conducting continuous outreach to available providers in a particular area to determine whether they would accept the plan's benefit amount as payment in full. Thus, we believe that non-network plans should be able to quantify the set of available providers in an applicable service area that accept the plan's benefit amount as payment in full. And by collecting this quantitative data as part of data submission requirements during QHP certification, we can measure access within a non-network plan's “network” consisting of the providers in the applicable area that would accept the plan's benefit amount as payment in full, even without formal contractual relationships.
We further clarify that we will not be requiring issuers to merely attest that their non-network plan has sufficient access to providers that accept the plan's benefit amount as payment in full. We will be collecting quantitative data from issuers that provide additional information regarding sufficient access to providers with non-network plans, including a numerical assessed percentage of providers that accept the plan's benefit amount as payment in full, and specific ECPs that have accepted the plan's benefit amount as payment in full. We also believe that the other information that non-network plans are required to submit work in concert to ensure sufficient access to providers that access the non-network plan's benefit amount as payment in full, including the strategy for making benefit amounts publicly available, methodology for determining benefit amounts, strategy for providing consumer-friendly and public information regarding costs, availability of exceptions processes, and strategy for providing adequate customer service to assist enrollees and potential enrollees in finding providers in their area who will accept the plan's benefit amount as payment in full. Together, we believe these factors constitute a framework that will ensure sufficient access to providers as they provide additional qualitative information on how the non-network plan has structured the plan, determines benefit amounts, and ensures consumers have sufficient access to care.
However, commenters raised valid recommendations on other data metrics to consider to measure provider access under a non-network plan, including a combination of provider acceptance data, binding provider acceptance agreements, historical claims data, and other objective indicators showing that enrollees can obtain services within reasonable timeframes and geographic distances. It is unclear to us how a provider acceptance agreement (a written agreement between the provider and non-network plans that the provider will accept a benefit amount as payment in full) may differ from traditional network contract agreements under a network plan. An explicit requirement to have provider acceptance agreements in place may also run counter to the premise underlying a non-network plan that distinguishes itself by not having formal agreements with providers. Part
( printed page 29776)
of the benefit of non-network plans, as verified by the one commenter currently providing non-network plans and based on our research into non-network plans, includes increased freedom on the part of providers to treat patients without restrictions caused by prior authorization, step-therapy protocols, and formulary restrictions, along with the prompt payment upon rendering services. In the proposed rule, we sought comment on the PY 2027 effective date on this proposal and whether PY 2028 would be more appropriate (91 FR 6413). We believe that delaying implementation of this policy until PY 2028 would be appropriate to allow HHS further time to consider if these alternative metrics and proposed modifications would improve access to providers within a non-network plan, as needed, in future rulemaking.
In response to the commenter requesting clarification on how we will monitor access on an ongoing basis, we will monitor potential issues raised by consumers on the FFEs and escalate any identified access concerns by performing direct outreach to QHP issuers with non-network plans, as appropriate. We will also consider additional outreach initiatives, including conducting consumer focus groups with enrollees of non-network plans. If we were to identify that a non-network plan cannot meet all certification requirements under § 156.236, we would consider decertification of such plan. Likewise, if a State Exchange or SBE-FP that allows non-network plans on their Exchange finds that a non-network plan no longer meets standards under § 156.236(a) and State requirements for non-network plans to provide access to providers, as applicable, then the State Exchange or SBE-FP may choose to decertify the non-network plan.
Lastly, we appreciate commenters' support that non-network plans may provide meaningful coverage for behavioral health providers that often do not contract with network plans.
Comment:
Many commenters shared concerns as well as recommendations regarding HHS' proposed general requirement under § 156.236(b)(1) that a non-network plan must submit information on an assessed percentage of providers in each plan's service area that accepts the plan's benefit amount as payment in full. Commenters questioned if HHS would require non-network plans to report the actual percentage of providers that agree to accept the benefit amount as payment in full and why HHS did not establish a specific minimum percentage.
Moreover, commenters stated concerns regarding whether a reported assessed percentage of providers in each plan's service area that accepts the plan's benefit amount as payment in full would allow the non-network plan to adequately determine how many providers would be sufficient to ensure services will be accessible without unreasonable delay. Commenters encouraged HHS to define how this assessment must be conducted, and to establish additional guidance regarding acceptable verification methodologies, required documentation, reassessment frequency, cadence for re-reporting the assessed percentage during the plan year, and required updates when provider acceptance declines. Another commenter recommended that HHS require non-network plans to conduct regular, independent, and transparent audits of how many providers accept the benefit amounts as payment in full, including behavioral health providers and to make the results of such audits publicly available prior to being certified as a QHP each year. This same commenter recommended the establishment of behavioral health provider availability thresholds for non-network plans to ensure sufficient access to behavioral health providers. Lastly, commenters opposing this proposal stated concern that an assessed percentage of providers in each plan's service area that accepts the plan's benefit amount as payment in full would function only as a point-in-time estimate that is subject to change, as there is no obligation that a provider would continuously accept the plan's benefit amount.
Response:
We appreciate these comments. We will require non-network plans to report an assessed percentage of providers that agree to accept the benefit amount as payment in full as part of data submission during the QHP certification cycle. We did not propose a specific minimum assessed percentage of providers that must accept the plan's benefit amount as payment in full as we intend to learn more about this novel plan type during QHP certification. We believe non-network plans may rely on various strategies to determine benefit amounts and different ways to analyze whether providers in a particular area will accept a benefit amount as payment in full and we first seek to understand in greater detail and intend to analyze these strategies after collecting this information from non-network plans during QHP certification. Thus, we plan to first collect the quantitative assessed percentage consistent with § 156.236(b)(1), as well as additional supporting information, including strategies to determine benefit amounts and the providers that will accept them consistent with § 156.236(b)(4) and § 156.236(b)(6), to supplement data analyses we will conduct prior to considering any data-driven selection of a specific minimum assessed percentage that we may address through future rulemaking. We do not believe it is appropriate to set a specific minimum percentage at this time until we are certain such a percentage would be effective and reasonable to promote access to a sufficient choice of providers that accept the benefit amount as payment in full. In addition, we do not agree with commenters that a non-network plan reporting an assessed percentage of providers accepting the plan's benefit amount as payment in full would mean that the issuer wholly decides what constitutes sufficient access, as the issuer must report this measure in good faith after a thorough analysis of providers available in their service area along with other data as part of its QHP application, so that we (and not the issuer) can make the determination if a non-network plan provides access to a sufficient choice of providers. In addition, the non-network plan's assessed percentage of providers that accept the plan's benefit amount as payment in full is not the only data point that we will utilize to determine whether a plan provides access to a sufficient choice of providers. Proposed language at § 156.236(b) indicates that that the determination as to whether a non-network plan provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full would be based on all the required information submitted to us consistent with that requested under § 156.236(b)(1) through (b)(9).
In addition, we acknowledge commenters' concerns that an assessed percentage of providers that accept the plan's benefit amount as payment in full could potentially represent only a point-in-time estimate that could change if a provider no longer accepts the plan's benefit amount as payment in full. Though, we believe that this issue is common in the existing health care market and is not only unique to a non-network plan, as issuers with network plans and providers may decide to terminate a contract during the plan year or a provider may change payment rates to adapt to shifts in health care prices outside of our purview. Nevertheless, this is one reason that we require plans to re-submit data each year as part of a new certification cycle,
( printed page 29777)
so we can identify changes in an issuer's data, including changes in a non-network plan's assessed percentage of providers that could result if a provider no longer accepts the non-network plan's benefit amount as payment in full. In the meantime, non-network plans would be required under revised § 156.236(b)(5) to regularly publicly update changes in benefit amounts, including if providers no longer accept benefit amounts so enrollees are aware and can make informed health care decisions.
Moreover, we appreciate commenters' request for additional information on how to perform a reasonable assessment of the assessed percentage of providers that accept the plan's benefit amount as payment in full, such as acceptable methodologies, reassessment frequencies, and documentation requirements. Similar to the reasons that we seek to learn more about the methodologies non-network plans utilize to determine an assessed percentage of providers prior to potentially establishing a minimum assessed percentage, we likewise believe it is premature to disseminate additional guidance on acceptable assessment methodologies until we gather more information on effective methodologies. We also believe that collecting more information on a non-network plan's assessed percentage of providers is important prior to considering establishing minimum thresholds for behavioral health providers or other specialty types. Collecting more information first would allow us to establish more evidence-based minimum thresholds that effectively promote access to providers, including in geographic areas that lack access to various specialty types. We also believe establishing separate thresholds for specific specialty types that must accept the non-network plan's benefit amount as payment in full would benefit from notice and comment rulemaking, just as we have historically done for proposing new provider-specific requirements and expanding provider types for network adequacy (under § 156.230) and ECP (under § 156.235). This would allow the public an opportunity to provide feedback on specific threshold percentages proposed by HHS and to assess if appropriate specialty type categories are adequately represented in a way that would promote access. However, for the reasons stated earlier in this section of this final rule, we believe the other information requested under § 156.236(b)(1) through (b)(9) works together to ensure a sufficient choice of providers in non-network plans, despite no specified minimum percentage being designated at this time.
As we learn more information prior to PY 2028, including after interested party engagement activities, we will consider commenters' suggestions to issue any additional guidance that may be necessary to provide to issuers offering non-network plans prior to implementation in PY 2028. While we do not intend to prescribe specific methods a non-network plan may use, we encourage non-network plans to consider a variety of methods, including, but not limited to, provider outreach, historical claims data, public data sources on available providers within the plan's service area, and other payor data.
We also acknowledge commenters' suggestion to require non-network plans to conduct regular, independent audits of how many providers accept the plan's benefit amounts as payment in full. However, we do not intend to require non-network plans to conduct audits and make this information publicly available at this time. We do not currently publicly report similar issuer certification review results as part of network adequacy and ECP reviews. If we determine that additional information is necessary to verify how many providers accept a non-network plan's benefit amount as payment in full beyond the information the issuer and HHS collect, then we may consider proposing this additional requirement through future rulemaking.
Comment:
A few commenters supported HHS' proposed requirements for non-network plans related to ECPs under § 156.236(b)(1) through 156.236(b)(3). These commenters agreed that non-network plans should be able to demonstrate that they provide access to a sufficient number and geographic distribution of ECPs, including Indian health care providers. One commenter requested HHS to clarify how HHS plans to measure and enforce these requirements and ensure that ECPs accept the non-network plan's benefit amount as payment in full.
Response:
We appreciate commenters' support for these ECP requirements that non-network plans must meet as part of obtaining QHP certification. To measure and enforce these requirements under § 156.236(b)(1) through 156.236(b)(3), we will require non-network plans to submit ECP data within MPMS during the annual QHP certification cycle to designate specific ECPs within their service area that have accepted the benefit amount as payment in full. Non-network plans will be required to select from a list of ECPs in the MPMS, that include qualifying ECPs that we approved for inclusion on the Final Plan Year ECP List.[343]
For each ECP selected by the issuer, non-network plans will be required to append a facility status (for example, accepted benefit amount as payment in full, rejected offer for benefit amount as payment in full, or did not offer a benefit amount as payment in full) to enable us to determine the issuer's satisfaction of each of the ECP requirements during certification reviews. Based on the facility statuses selected, we will be able to calculate whether the issuer meets minimum percentage requirements under § 156.236(b)(1), category per county requirements under § 156.236(b)(2), and Indian health care requirements under § 156.236(b)(3). For additional operational information, we refer commenters to the forthcoming 2027 Final Letter to Issuers and earlier discussion in this section of this final rule.
Comment:
Multiple commenters shared concerns as well as recommendations regarding HHS' proposed requirement under § 156.236(b)(4) that would require non-network plans to submit information on their strategy for conducting continuous outreach to available providers in a particular area to determine whether they would accept the plans' benefit amount as payment in full. Some commenters did not believe requiring non-network plans to report an outreach strategy would be sufficient, since there is still the potential that enrollees may be subject to additional out-of-pocket costs for charges exceeding the benefit amount even if a non-network plan conducts outreach to providers to inform benefit amounts. Commenters requested additional clarification on what constitutes adequate outreach, how frequently adequate outreach must occur, required documentation during outreach, and how HHS would evaluate the sufficiency of these outreach efforts. Another commenter questioned how outreach would work in practice, as it is possible providers may lack the incentive to provide price information to non-network plans that they do not contract with as they are often busy, under no formal contract with the issuer, and may not see the benefit in doing so.
( printed page 29778)
Response:
We appreciate commenters raising these concerns. We intend to collect qualitative data from issuers with non-network plans as part of data submission requirements during the annual QHP certification cycle, in which non-network plans would need to sufficiently describe these continuous outreach efforts. We disagree with commenters that did not believe requiring non-network plans to report information on their strategies for outreach would be sufficient since there is still the potential that enrollees may be subject to additional out-of-pocket costs. For reasons discussed earlier in this section, we believe that all the factors under § 156.236(b)(1) through (b)(9) collectively assist us in obtaining information to comprehensively assess whether a non-network plan pursues actions to limit out-of-pocket costs and ensure that there are sufficient choice of providers that accept the non-network plan's benefit amount as payment in full. Also, as discussed earlier in this section, relevant No Surprises Act provisions apply to non-network plans to limit costs associated with surprise billing for certain services. We also do not agree with commenters' assertion that collecting information on outreach efforts would not be sufficient. It is critical to understand a non-network plan's outreach efforts since these efforts would help us assess whether a non-network plan receives real-world data directly from communicating with providers to understand how many providers in the area will accept their benefit amount as payment in full. This effort is important to help the non-network plan set benefit amounts that providers would accept in practice to ensure that there is sufficient access to providers that accept the non-network plan's benefit amount as payment in full, so that consumers can avoid additional out-of-pocket costs. We are aware of at least one non-network issuer who is already performing provider outreach to inform the selection of benefit amounts. Requiring non-network plans to submit this information is crucial to understand if non-network plans provide sufficient choice of providers, as it will assist us in understanding how that information is provided and to ensure the benefit amount as payment in full remains relevant.
We believe that adequate outreach may consist of, but is not necessarily limited to, direct outreach to providers within the issuer's service area by utilizing multiple communication channels (for example, email, phone, in-person), collecting pricing information on a variety of different services from a meaningful sample of different provider types across various geographical areas, maintaining detailed documentation on the outcomes of such outreach (including verbal acceptance from providers that they accept benefit amounts as payment in full), and conducting this outreach at least annually to ensure that benefit amounts are routinely updated and current. Through engagement with issuers, these are common strategies that issuers with network plans conduct to ensure access to providers, thus we believe these strategies would also be appropriate to non-network plans. As an example, we will not consider it sufficient if the issuer were to only contact a single provider that accepts a benefit amount as payment in full and base any subsequent rates based on that single provider. Overall, we believe that conducting outreach is an essential tool along with other data sources (for example, claims, private payor rates, etc.) to assess acceptance of a non-network plan's benefit amount by providers.
Lastly, while it could be true in some cases that providers may not provide price information to non-network plans that they do not contract with, as they often are handling significant patient volumes and administrative processes, under no formal contract with the issuer, and may not see the benefit in doing so, we do believe that some providers may be incentivized to provide this information to attract new consumers. This may especially occur if non-network plans appropriately communicate the potential benefits of these plans to providers, including those mentioned by some providers currently accepting non-network plans, such as no need for prior authorization, step therapy protocols, and prompt payment upon services provided that often serve as barriers to providers furnishing care. We also believe that in practice, providers may already be required to disclose some price information since consumers have a right to request advance cost estimates for their services due to existing Federal price transparency requirements under the No Surprises Act and due to patients seeking to pay cash for services.
Comment:
Commenters stated both support and concern and shared recommendations regarding HHS' proposed requirement under § 156.236(b)(5) that non-network plans must report their strategy for making benefit amounts publicly available in an easily accessible and understandable format. Commenters supported transparent benefit amount information, stating that issuers offering non-network plans should maintain verified, current data on which providers accept the plan's benefit amount as payment in full. A few commenters suggested that HHS standardize the manner in which non-network plans display their benefit amounts, such as by requiring non-network plans to use recognizing billing codes (for example, CPT, HCPCS, or DRG codes). These commenters further recommended that the benefit amounts be made available through machine-readable formats, which would both allow researchers and consumers to more easily compare prices, and assist HHS in understanding how these benefit amounts compare to other negotiated rates. Lastly, one commenter stated that benefit amount information should be updated regularly to reflect current prices for services. An issuer currently offering a non-network plan shared that benefit amounts are reviewed and updated by the non-network plan at least quarterly to account for inflation, market changes, and enrollees access patterns and made available to enrollees.
Response:
We appreciate the feedback shared by commenters, especially from commenters confirming the importance of ensuring that benefit amounts are publicly available and accessible to consumers. We believe that issuers offering non-network plans must ensure that benefit amounts remain current, as this is essential to ensure that consumers can rely on the accuracy of price information prior to seeking care from providers, so consumers have certainty that they can access a provider that will accept the benefit amount as payment in full. For this reason, and with additional context received that non-network plans do regularly update their benefit amounts, we are finalizing additional language at § 156.236(b)(5) to reflect that a non-network plan must report their strategy for making benefit amounts publicly available in an easily accessible and understandable format and for regularly updating any changes to benefit amounts.
Lastly, we appreciate commenters' suggestions on ways to improve the standardization of benefit amounts. However, consistent with our interpretation of our statutory authority under section 1311(c)(1)(B) and (c)(1)(C) of the Affordable Care Act, we do not believe it would be appropriate to dictate specific billing codes a non-network plan must utilize, even for the purposes of standardization. Given their expertise in this area, we also believe specific billing codes plans should use are more appropriately determined jointly by issuers and providers. Lastly,
( printed page 29779)
we acknowledge requests to make benefit amounts available in a machine-readable format, however we believe it would be premature to standardize the format and structure for machine readable reporting at this time. We will consider these requests for future plan years.
Comment:
Commenters shared concern as well as recommendations regarding HHS' proposed requirement under § 156.236(b)(7) that a non-network plan must report their strategy for providing consumer-friendly and public information about potential balance billing scenarios and expected out-of-pocket costs, including historical data on actual out-of-pocket costs incurred by its enrollees while accessing providers (including ECPs) in the area. Commenters advocated for balance billing protections, such as through the implementation of clear, consumer disclosures with plain language. Specifically, commenters suggested that HHS utilize clear, standardized disclosure so enrollees understand how a non-network plan works, including how benefit amounts are determined, the percentage of providers in a service area that accept the plan's benefit amount, how to find providers that would accept the benefit amount as payment in full, potential out-of-pocket costs, and how to access consumer assistance resources. Commenters believed that disclosures specifying this type of information are necessary to prevent consumer confusion, limit the risk that consumers enroll in plans without fully considering risks versus benefits of the plan, and further protect against balance billing risks. Some commenters requested clarity regarding how HHS intends to display or “label” non-network plans.
Moreover, one commenter stated that requiring a non-network plan to report the strategy for providing consumer-friendly information about balance-billing scenarios is not a substitute for protecting against these balance-billing scenarios. Many commenters raised concerns that many medical interactions pose significant balance-billing risks, including in ways that may violate provisions of the NSA, due to consumer uncertainty regarding what medical services a patient will actually need since most consumers lack detailed medical knowledge. Thus, commenters shared that consumers need more information beyond potential out-of-pocket costs.
Response:
We appreciate commenters raising these important points related to balance-billing and the implementation of clear disclosures for consumers. We agree that clear disclosures are essential to communicate important information on non-network plans. This is why we proposed under § 156.236(b)(7) to require non-network plans to provide information on their strategy for providing consumer-friendly and public information about potential balance billing scenarios and expected out-of-pocket costs, including historical data on actual out-of-pocket costs incurred by enrollees while accessing providers in the area. We will utilize this information to determine whether a non-network plan adequately provides clear discourses to consumers on balance billing risks and out-of-pocket costs. Particularly due to the novelty of this innovative network design, we agree that consumers should have accessible information about the structure of these plans, the use of benefit amounts and how to apply these benefit amounts, potential balance-billing risks, and other consumer assistance resources. As we have previously stated in this section of this final rule, we understand that a non-network plan may not necessarily fit every consumer. These plans may be more suitable for consumers who wish to take an active role in searching for and negotiating prices with providers, and less suitable for those who do not wish to “shop around” and navigate additional administrative processes associated with their care, but rather prefer to enroll in a plan with contracted providers who have set, negotiated rates. Thus, it is important for issuers to communicate vital information about non-network plans to consumers so consumers understand their structure and how to utilize the plan, so consumers can make well-informed decisions prior to enrollment and confidently select a plan that best suits their needs. For that reason, we will ensure non-network plans are clearly differentiated from network plans during plan selection on
HealthCare.gov
and ensure clear information about these plans is accessible to consumers, including information regarding the lack of a traditional network, links to the public benefit amounts on the issuer's website, potential balance billing risks, and the availability of other consumer resources.
Furthermore, and as stated in the discussions above, we understand that commenters have concerns about the ability of enrollees to predict all the required health services they will need during an episode of care, prior to receiving services. Many medical interactions result in the need for additional ancillary services that a consumer may not be able to reasonably predict, including diagnostic and laboratory tests, imaging tests, and recommendations for necessary services from ancillary providers such as pathologists, anesthesiologists, and radiologists. As we previously stated in discussions above, consumers should not be expected to understand and anticipate all the ancillary providers and services their provider may recommend during their episode of care, as this anticipation likely requires a level of advanced medical knowledge that is more appropriate for providers. And, the selection of ancillary providers and services are often determinations made during a clinical episode by providers (not patients) and are driven by real-time clinical decision making and medical necessity. When we proposed this factor in the proposed rule, we stated that this factor is important to ensure non-network plans have in place a cohesive strategy for providing consumer-friendly information about how the plan may be most effectively used to limit out-of-pocket costs and the impact of seeking care from providers who charge more than the plan's benefit amount, since this plan design may not be immediately intuitive to enrollees (91 FR 6411). An enrollee receiving additional ancillary services and care from ancillary providers would likely impose additional out-of-pocket costs, especially if the enrollee initially proceeded with care due to a benefit amount wholly accepted by the primary provider. But, the enrollee did not foresee the care furnished by ancillary providers and ancillary services costing more than the plan's benefit amount when selecting the primary provider, which would constitute additional out-of-pocket costs. Thus, we are finalizing additional language in § 156.236(b)(7) to ensure non-network plans have a strategy for providing consumer-friendly information to enrollees on navigating episodes of care with multiple benefit amounts (including for ancillary providers and services). We believe modifying this factor to reflect consumer-friendly information on costs associated with ancillary providers and services would be consistent with our expectation when initially proposing this factor that plans should provide information about how the plan may be most effectively used to limit out-of-pocket costs and the impact of seeking care from providers who charge more than the plan's benefit amount. This type of information would be required to be disseminated to consumers along with other information on potential out-of-pocket costs and balance-billing
( printed page 29780)
scenarios, to support expected needs of most consumers using these plans and in order for non-network plans to meet the requirements under § 156.236(b)(7).
Comment:
Commenters shared both support and concern as well as recommendations regarding HHS' proposed requirement under § 156.236(b)(8) that a non-network plan must describe the availability of an exceptions process under the non-network plan for enrollees who cannot find providers (including ECPs) willing to accept the benefit amount as payment in full. Specifically, commenters believed that the proposed regulatory language should be more detailed in how it defines standards for an acceptable exceptions process to meet § 156.236(b)(8) and that the existence of an exceptions process does not prevent out-of-pocket costs. A few commenters stated that the language only addresses “unavoidable” out-of-pocket costs, which does not provide ample consumer protections. One commenter requested that HHS establish minimum standards for exceptions processes, timelines for resolving gaps in access to care, payment adjustments if the provider does not accept a benefit amount as payment in full, and “consumer rights if access failures occur.” Another commenter stated that network plans are subject to important consumer protections such as appeal and exception rights, which allow enrollees to appeal for coverage of services provided by out-of-network providers when no in-network providers are available; thus, the commenter requested clarification on whether non-network plans would be required to have similar protections.
An issuer currently offering a non-network plan described that the plan's exceptions process ensures that enrollees have access to care at or below the plan's benefit amount, or the non-network plan would increase the benefit amount to fill gaps in access to care. The commenter stated that diligent adjustments of the benefit amount help promote consumer protections.
Response:
We appreciate commenter's feedback. We do not agree with commenters that stated the language currently under § 156.236(b)(8) only addressed “unavoidable” out-of-pocket costs, since this language is not explicitly in the proposed regulation text. Rather, the proposed regulation text requires non-network plans to disclose information regarding an exceptions process for enrollees who cannot find providers willing to accept the benefit amount as payment in full. For the reasons we explain earlier in this section of this final rule, we expect the non-network plan to provide broad information on their exceptions processes such that we can determine if it adequately protects consumers in the event the consumer is unable to find care at or below the plan's benefit amount.
As we previously stated (91 FR 6411), it is important that the non-network plan remains flexible for enrollees who have little choice in providers and cannot locate providers willing to accept the benefit amount as payment in full. If a non-network plan cannot protect consumers against out-of-pocket costs in situations where many providers refuse to accept the plan's benefit amount as payment in full, an effective exceptions process should be able to shift the burden of paying any unavoidable, additional out-of-pocket costs from the enrollee to the non-network plan. We expect that the non-network plan's exceptions process can appropriately assist consumer's in limiting out-of-pocket costs if assisting the consumer in locating additional providers that accept the plan's benefit amount, increasing the benefit amount so that providers in the consumer's service area accept the benefit amount as payment in full, or by some other means. As these plans become available through the FFEs, we will consider whether additional requirements may be needed as part of an exceptions process including if complaints from non-network plan enrollees are identified through regular HHS monitoring that can be mitigated by proposing more requirements on a non-network plan's exceptions process. We may also assess exceptions processes that may potentially be adopted by State Exchanges and SBE-FPs offering non-network plans through their Exchanges to consider the application of these processes on the Federal level.
Overall, we appreciate commenters' suggestions to mandate more prescriptive standards surrounding the exceptions process. We believe that well-established exceptions processes that already exist for enrollees in network plans to receive coverage for an out-of-network provider when an in-network provider is not available, should also be extended to enrollees in non-network plans when enrollees cannot locate a provider that will accept the benefit amount as payment in full. For example, just as issuers with network plans must provide access to covered services when in-network providers are unavailable, non-network plans must maintain an exceptions process to ensure that enrollees are able to obtain covered services at or below the plan's benefit amount when there is not sufficient access to providers accepting the plan's benefit amount as payment in full.
Lastly, in response to commenters that advocated for more guidelines on the exceptions and appeals processes to promote more consumer protections, we affirm that non-network plans must provide all the same consumer protections that apply to individual and small group health insurance coverage, including, but not limited to, those specified in PHS Act title XXVII parts A through D, as all other plans applying for QHP certification are subject to providing. These consumer protections that non-network plans must provide include both an exceptions processes for non-covered services by providers, and formal appeal processes to allow enrollees to appeal coverage and benefit determinations. Lastly, we note that the requirement under § 156.236(b)(8) under which non-network plans must submit information to HHS regarding whether the plan has an exceptions process for enrollees who cannot find providers willing to accept the benefit amount as payment in full, does not exempt non-network plans from also ensuring their enrollees have access to formal appeals processes consistent with consumer protections specified in PHS Act title XXVII parts A through D.
Comment:
Commenters stated both support and concern as well as shared recommendations regarding proposed § 156.236(b)(9) that would require a non-network plan to report the plan's strategy for providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers (including ECPs) in their area who will accept the plan's benefit amount as payment in full. Commenters supported directories of providers that have been determined to accept the plan's benefit amount as payment in full. Commenters stated that the list of these providers should be routinely updated, including at least monthly and verified at least every 90 days. Commenters stated that this information would be important so that enrollees have current information and can avoid getting care from providers who may no longer accept the plan's benefit amount as payment in full.
Additionally, some commenters stated that consumers need more customer service resources, such as tools to provide enrollees real-time information on the cost of care, so consumers fully understand their financial liabilities before services are furnished or at the point of service. One commenter stated that medical technology has expanded, such that
( printed page 29781)
real-time pricing infrastructure systems are becoming more accessible. The commenter stated these systems can consider benefit amounts and provider charges, while calculating full payment determinations by accounting for “eligibility verification, benefit computation, cost-sharing calculations, and coordination of benefits.” An issuer currently offering a non-network plan added that the plan provides online tools, so enrollees have real-time information on local providers, anticipated costs, and benefit amounts so consumers may make informed decisions. The commenter shared that in cases where a provider's total cost exceeds the plan's benefit amount, the enrollee receives that information and should they continue to seek care from the provider, they do so knowingly.
Response:
We thank commenters for this information. We agree that non-network plans should have accessible provider directory assistance resources so enrollees can easily locate providers willing to accept the plan's benefit amount as payment in full, thus we intend to finalize this requirement so that non-network plans report to us their strategy for providing these resources to enrollees.
Additionally, we understand the importance for consumers to understand potential costs associated with receiving care prior to the point of service, especially since a single episode of care could trigger multiple benefit amounts that consumers may not be able to sufficiently anticipate. We appreciate commenters noting that technology to provide consumers that real-time information is becoming more accessible, and that non-network plans have already implemented efforts to provide these services to consumers, as the issuer currently offering non-network plans shared that the plan provides online tools so consumers have real-time information on local providers, anticipated costs, and benefit amounts. Therefore, we are finalizing additional language at § 156.236(b)(9) to ensure non-network plans have a strategy to assist enrollees in receiving real-time cost estimates prior to care being furnished. We believe this would further address commenters' concerns about balance-billing risks and unanticipated out-of-pocket costs, as outlined in discussions above, as it would help enrollees more appropriately determine healthcare costs in advance of seeking care so a consumer can make an informed decision on seeing a provider after evaluating a real-time cost estimate. And, we believe it is feasible as one issuer with a non-network plan confirmed the plan already has online tools to perform these real-time cost estimates to inform consumers. In addition, there is robust evidence that real-time cost estimate technology has already been widely adopted by both issuers and providers, thus we maintain that this requirement is reasonable for non-network plan issuers to meet.[344]
Comment:
One commenter recommended that individuals enrolling in non-network plans be permitted to access a special enrollment period to switch plans mid-year if they are unable to access care from providers willing to accept the plan's benefit amount as payment in full.
Response:
While we may consider this issue in future rulemaking, we do not believe it is appropriate at this time. Again, we reiterate that we believe that information requested by us under § 156.236(b)(1) through (b)(9) works together to ensure non-network plans provide a sufficient choice of providers that accept the plan's benefit amount as payment in full, including the availability of an exceptions process for enrollees who cannot find providers willing to accept the benefit amount as payment in full (under § 156.236(b)(8)) and the non-network plan's strategy for providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers in their area who will accept the plan's benefit amount as payment in full (under § 156.236(b)(9)). If we identify during the plan year that a non-network plan no longer provides access to providers willing to accept the plan's benefit amount as payment in full, the non-network plan may no longer meet certification requirements under § 156.236 and is subject to decertification in accordance with § 155.1080(c). We also note that there is currently no special enrollment period exception for individuals enrolled in network plans if their plans no longer cover their preferred in-network providers, and we did not discuss the applicability of special enrollment periods within the proposed rule.
Comment:
One commenter requested that HHS require non-network plan issuers to provide consumers with maximum binding cost commitments prior to service delivery, including for services such as scheduled imaging, laboratory panels, and preventive screenings, to ensure a cost for a specific service would not exceed a maximum amount.
Response:
We believe that non-network plans must provide consumers with transparent benefit amount information, so that consumers can make informed decisions about their care. We understand that services such as imaging, laboratory services, and preventive screenings may constitute additional costs that consumers cannot always anticipate prior to seeking care. While we cannot dictate specific payment obligations to non-network plans related to specific services, we finalized a modification at § 156.236(b)(7) to ensure non-network plans have a strategy for providing consumer-friendly information to enrollees on navigating episodes of care with multiple benefit amounts (including for ancillary providers and services). We believe these ancillary services would be inclusive of imaging, laboratory services, and preventive screenings, and thus a non-network plan providing resources to consumers on how to navigate these services would help limit potential out-of-pocket costs associated with such services combined with public benefit amount information.
Comment:
Many commenters stated concern regarding how HHS plans to operationalize the proposals and the implementation timeline. Specifically, commenters were concerned with HHS assessing compliance with non-network plan standards under § 156.236(b)(4) through (b)(9) based on an issuer's “yes” or “no” attestations. Commenters feared it would be too easy for these attestations to be given in bad faith. Commenters advocated for HHS to disseminate clear sub-regulatory guidance, including before the QHP certification cycle, so issuers can better understand requirements under § 156.236 and build infrastructure to capture benefit amounts.
Lastly, a large portion of commenters recommended that HHS delay implementation of this proposal to PY 2028, and some encouraged separate notice-and-comment rulemaking or a request for information (RFI) on non-network plans. One commenter suggested phasing in certification of non-network plans over time. Commenters reasoned that after the finalization of this payment notice, there would be a short turnaround time
( printed page 29782)
for plans to prepare for the upcoming QHP certification cycle. Commenters also believe that delaying finalization would allow HHS time to further strengthen the proposed regulatory requirements, evaluate potential impacts to market stability, analyze the intersections of non-network plans with other policy areas, and gather interested party input.
Response:
We acknowledge commenters' concerns regarding attestations that may be answered in bad faith. Issuers are responsible for answering truthfully regarding any attestations made during the QHP certification process and risk QHP certification denial if they do not answer truthfully. In our experience certifying QHPs, we have found issuer's attestation responses to be done in good faith and generally found to be truthful. To address commenters' concerns with providing more certainty that non-network plans provide consumer protections, and to collect better qualitative data on non-network plans, we will require issuers to provide additional information to support compliance with requirements under § 156.236(b)(4) through (b)(9). Specifically, issuers with non-network plans will be required to provide written descriptions to describe how the plan satisfies each of the factors under § 156.236(b), and submit additional supporting documentation (for example, empirical data, methodology for setting benefit amounts, resources provided to consumers, evidence of publicly available benefit amounts, etc.) to validate these responses. We believe requiring this additional information would provide more detail to us than “yes” or “no” responses to each of the factors that do not explain how and why an issuer meets or does not meet requirements, so that we have more information during determinations on whether a non-network plan provides adequate consumer protections.
Moreover, we recognize that commenters may need additional time to learn about this novel plan type (especially consumers) and to adequately prepare infrastructure for the entry of these plans. We also believe that commenters have raised valid concerns in response to this proposal that warrant further consideration and analysis—principally, concerns on consumer out-of-pocket costs, impact of non-network plans on providers, risk-adjustment, and alternative methods to measure access to providers within non-network plans. For this reason, we agree that it is appropriate to delay implementation of this proposal until PY 2028. We remain open to further engaging interested parties to discuss potential concerns with non-network plans and modifications to finalized policies under § 156.236 to ensure these plans provide meaningful access to care to enrollees enrolled in QHPs on the FFE.
Comment:
One commenter recommended that HHS develop a uniform set of reporting metrics applicable across non-network plan issuers, encompassing measures such as provider acceptance rates, out-of-network utilization rates, complaint categories, and complaint resolution timelines, and reports on how often a non-network plan's payment amounts are challenged by providers using the independent dispute resolution (IDR) process that exists under the No Surprises Act. Another commenter pointed to the availability of third-party quality measurement tools as viable mechanisms to provide consumers and enrollees with sufficient information to make well-informed decisions about their health care and coverage.
Response:
We appreciate commenters' recommendations regarding data reporting and metrics that could be valuable tools for consumers or used to assess a non-network plan's compliance with law. At this time, we decline to finalize such data reporting metrics as we believe instituting these requirements would benefit from separate notice and comment rulemaking, so that we can better understand if specific metrics are consistent with data collected by non-network plans and whether these metrics are realistic for plans to report to us. Not finalizing these requirements at this time will also allow us additional time to consider whether a uniform set of reporting metrics could be adopted and standardized for both network and non-network plans. In addition, much of the data reporting metrics requested by commenters is consistent with data that we already intend to collect, including an assessed percentage of providers that accept the plan's benefit amount as payment in full (for example, provider acceptance rates) under § 156.236(b)(1), and an exceptions process for enrollees who cannot find providers willing to accept the plan's benefit amount as payment in full (for example, complaint resolution) under § 156.236(b)(8). We also respect that State Exchanges and SBE-FPs have broad authority to develop reporting metrics and related requirements that will allow them to assess a non-network plan's access to care. HHS, as operator of the FFEs, will take these suggestions into consideration as we learn more about the possible variations of non-network plans and as we further develop policy in this area and encourage State Exchanges and SBE-FPs to do the same.
Comment:
Many commenters questioned how non-network plans would intersect with other existing policy areas, such as the Mental Health Parity and Addiction Equity Act (MHPAEA), transparency in coverage requirements, EHB requirements, coverage of preventive services, advanced explanation of benefits reporting, medical necessity, utilization requirements, and continuity of care requirements.
Commenters also requested additional clarity on how non-network plans would need to demonstrate coverage of each EHB, including coverage of preventive services without cost sharing and additional costs beyond the plan's benefit amount. One commenter stated concern that if non-network plans cannot guarantee access to preventive services without cost sharing, enrollees may be disincentivized from seeking preventive services. Another commenter questioned how a non-network plan would comply with non-quantitative treatment limitation requirements under MHPAEA, so that non-network plans do not impose more restrictive non-quantitative treatment limitations on mental health and substance use disorder services than on medical/surgical services.
Response:
We thank commenters for raising these important questions. Non-network plans will not be exempt from market requirements applicable to network plans and must provide all the same consumer protections that apply to individual and small group health insurance coverage. These requirements include, but are not limited to, those specified in PHS Act title XXVII parts A through D, including MHPAEA and advanced explanation of benefits reporting requirements, and the requirement to provide coverage for preventive services consistent with section 2713(a) of the PHS Act and § 147.130, including by demonstrating a sufficient choice of providers that accept the plan's benefit amount as payment in full for all the required categories of preventive services (for example, immunizations for routine use, evidence-informed preventive care and screenings, etc.). Regarding the commenter's question on how a non-network plan would comply with non-quantitative treatment limitation requirements under MHPAEA, since MHPAEA is included under PHS Act title XXVII part A, non-network plans must comply with these requirements and would not be permitted to impose more restrictive non-quantitative
( printed page 29783)
treatment limitations on mental health and substance use disorder services than on medical/surgical services.
Furthermore, to receive certification as a QHP, a non-network plan must provide the EHB package in accordance with § 156.115, and comply with benefit design standards defined in § 156.20, the cost-sharing requirements at § 156.130, and the levels of coverage requirement at § 156.140. The requirement to provide EHB in accordance with § 156.115 means that the non-network plan must, among other things, provide benefits that are substantially equal to the relevant State's EHB-benchmark plan. As part of QHP certification, non-network plans must submit the Plans and Benefits Template as any other network plans, which will allow us to ensure all EHBs are covered.
Additionally, it is our understanding that non-network plans currently do not place restrictions on medical necessity, nor do they require prior authorization for covered services, as verified by the one commenter currently providing non-network plans and based on our research into non-network plans. A non-network must provide consumers appropriate information on the plan's benefit amount for covered services, whether a provider would accept the plan's benefit amount, and information on a consumer's out-of-pocket costs. Overall, we believe delaying implementation of this proposal until PY 2028 will provide time for us to conduct additional analysis on these thoughtful questions about how non-network plans intersect with other policy areas more fully and how non-network plans would demonstrate compliance with requirements, including through additional guidance.
Comment:
Some commenters requested additional information from HHS on the structure of a non-network plan design, including if these plans have deductibles, maximum out-of-pocket limits, cost-sharing such as coinsurance and copayments, and traditional formularies. Commenters questioned if non-network plans have annual and lifetime limits, maximum out-of-pocket limits, and deductible limits. Commenters sought more information on cost sharing, including how the annual limitation on cost sharing would apply to non-network plans when applicable provisions are often defined in terms of in-network benefits. Commenters also requested that HHS address how the annual out-of-pocket maximum limit would function for non-network plans, including how benefit amounts would be addressed within this limit when the limit is often calculated with negotiated rates for in-network providers. Commenters urged HHS to establish clear cost-sharing standards, including by considering that all providers under a non-network plan should count as being in-network.
Commenters also questioned a non-network plan's compatibility with the AV Calculator, with some commenters requesting that HHS require non-network plans to demonstrate compliance with metal level actuarial value (AV) requirements using the existing AV Calculator. Some commenters sought to understand how non-network plans would calculate AV when the AV Calculator uses in-network benefits. One commenter reasoned that since non-network plans set benefit amounts for a particular service, the structure of the AV Calculator may need to be modified to appropriately capture the value of benefits in absence of a non-network plan inputting coinsurance and copayment amounts. One commenter reasoned that if HHS did not require non-network plans to utilize the existing AV Calculator, the non-network plan type may appear affordable to consumers, while lacking adequate coverage.
Response:
We acknowledge that non-network plans represent a novel plan offering and there are open questions regarding how these non-traditional plans will comply with various standards that may be applicable to individual market coverage. We are finalizing clear requirements under which non-network plans must comply with the market reforms and consumer protections under the Affordable Care Act. Based on our internal preliminary research into existing non-network plans, it is our understanding that most non-network plans currently have deductibles, premiums, and maximum out-of-pocket limits. We believe there are some non-network plans available that do not have traditional coinsurance and copayment structures; rather, these plans utilize benefit amounts (or set payment rates) for covered services. Thus, an enrollee seeking care from a provider that does not accept the plan's benefit amount as payment in full may experience excess charges as out-of-pocket costs. Nevertheless, non-network plans must comply with the cost-sharing requirements at § 156.130.
In addition, non-network plans must comply with the levels of coverage requirement at § 156.140 as a condition of QHP certification similar to network plans. Regarding use of the AV Calculator, we maintain that a non-network plan will still be required to meet Federal standards for AV calculation for determining level of coverage, per § 156.135. We may consider additional refinements to AV calculation requirements under § 156.135 and alternative methodologies for a non-network plan to estimate AV through future rulemaking, as appropriate. The Affordable Care Act's MOOP requirement under section 1302(c)(1) does not set forth a specific exception for non-grandfathered, non-network plans.[345]
Additionally, it is our understanding that non-network plan types do not have traditional formularies, rather they apply benefit amounts for certain covered drugs under the plan, as identified by our internal preliminary research into existing non-network plans. Nevertheless, due to the novelty of this plan design, it is possible other variants of non-network plans currently exist in the market that apply these elements, such as how they structure drug coverage, in different ways.
While we understand the need for consumers to understand the applicability of benefit amounts to various elements of plan design in more detail, we believe this would require additional clarifications on how benefit amounts would fit within the Federal definition of cost sharing, which is beyond the scope of this final rule. However, the Departments have previously addressed the application of MOOP requirements pertaining to reference-based pricing arrangements in Affordable Care Act Implementation FAQs (Part XIX and Part XXI).[346]
Specifically, the guidance states that the Departments would not consider a plan or issuer as failing to comply with the annual limitation on cost sharing requirements of PHS Act section 2707(b) because the plan or issuer treats providers that accept the reference amount as the only in-network providers, as long as the plan or issuer uses a reasonable method to ensure that it offers adequate access to quality providers, including maintaining an
( printed page 29784)
exceptions process and appropriate consumer protections. The Departments subsequently provided additional guidance as to what constituted a reasonable method within these aforementioned FAQs.
Comment:
Commenters stated concerns over non-network plans having lower premiums and potentially becoming the second lowest cost silver plan in areas they are sold. Consequently, commenters were concerned that due to the second lowest cost silver plan being tied to APTCs, this may reduce premium tax credits raising out-of-pocket costs for consumers not even enrolled in these plans. One commenter requested HHS to consider prohibiting non-network plans from setting the APTC benchmark. Commenters were further concerned that if a non-network plan has lower administrative costs, they may offer lower premiums that attract consumers who do not fully grasp the plans' complexity and despite premium savings, may ultimately expend more resources to navigate benefit amounts, locating providers, and negotiating prices.
Response:
We acknowledge commenters' concerns regarding potential impacts non-network plans may have on the overall market, especially to the extent that these plans end up affecting the costs for consumers not enrolled in these plans. We have never prevented a plan from becoming the second lowest cost silver plan and believe it would be premature to break that precedent based on assumptions that non-network plans will have significantly lower premiums without us first receiving this data directly from non-network plans during QHP certification. We reiterate that our goal with this proposal is to encourage innovation and competition in the Exchange. However, commenters raise valid concerns that we will continue to monitor to identify if non-network plans produce downstream impacts on costs to consumers across the individual market. Should we have concerns regarding market stability, as we have previously stated, under § 155.1000(c)(2), Exchanges have broad discretion to determine whether a plan is in the interest of qualified individuals and qualified employers, regardless of whether the plan meets other minimum certification requirements consistent with § 155.1000(c)(1). We have long maintained [347]
that Exchanges are free to exercise the authority at section 1311(e)(1) of the Affordable Care Act (as implemented at § 155.1000(c)(2)) to refuse certification to a plan if they determines that making available such health plan through such Exchange is not in the interests of qualified individuals and qualified employers in the State,[348]
even if the plan otherwise meets all other QHP certification requirements. We will consider these issues in future rulemaking to determine if exercising this “interest standard” is appropriate.
We also acknowledge concerns related to consumers who may be attracted by lower premiums who do not fully understand the plan. To this extent, we reiterate we intend to ensure non-network plans are clearly differentiated from network plans during plan selection on
HealthCare.gov
and ensure clear information about these plans is accessible to consumers, including information regarding the lack of a traditional network, links to the benefit amounts, potential balance billing risks, and the availability of other consumer resources.
Comment:
Many commenters stated concerns over a non-network plan's potential to attract healthier, more-price sensitive consumers due to lower premiums, while concentrating higher-cost enrollees with greater health needs in network-based plans with higher premiums. Commenters noted their belief that this may lead to risk segmentation by significantly altering risk pools, including across various metal tiers, and destabilize the risk adjustment program, including by suppressing statewide average premiums used in risk adjustment calculations. Overall, commenters shared concerns that these effects would affect long-term market stability.
In addition, a few commenters responded to HHS' comment solicitation on considerations for non-network plans in the HHS-RADV process. One commenter raised concerns that if a non-network plan was not able to report diagnoses with claims as part of the risk adjustment process, this may result in “significant risk adjustment payables, and potentially very large RADV transfer adjustments.” The commenter stated concern that if the non-network plans would not be able to financially cover these transfer amounts, then other plans would not receive the risk adjustment amounts they are owed. The commenter did not believe it would be appropriate to exempt non-network plans from HHS-RADV, as it could incentivize plans to avoid covering individuals with greater health needs.
A different commenter recommended that HHS consider flexibility in the data sources utilized for the HHS-operated risk adjustment program and HHS-RADV, including direct payment to providers via invoices, medical records, cash-pay transactions, encounter data, or third-party data to submit verified diagnosis information. The commenter also requested HHS to allow the use of centralized, independent data integrators or aggregators that can make objective determinations of enrollee risk across all issuers by utilizing data already available through data-exchanges and other Federal sources. The commenter noted their belief that this recommended approach would more fairly support newer plans entering the market that do not have the resources and data aggregation capabilities that larger health plans may have developed to maximize risk adjustment payments by using sophisticated data methods to increase the number of diagnostic codes summitted through issuers' EDGE servers.
Response:
We agree with commenters that non-network plans should not be exempt from participation in HHS-RADV. Participation in HHS-RADV is a critical element of maintaining program integrity by validating issuers' risk under the HHS-operated risk adjustment program. For the purposes of the HHS-operated risk adjustment program, we believe that the approach to gathering diagnoses through a standardized claim-data format best ensures that HHS risk adjustment transfers under the State payment transfer formula are based upon the most reliable data possible. For the purposes of HHS-RADV, we continue to believe medical record review to be the best approach for validating the diagnoses submitted through issuers' EDGE servers.
349
Therefore, we did not propose and are not finalizing any changes to the risk
( printed page 29785)
adjustment data submission process or HHS-RADV to incorporate additional data flexibilities for non-network plans nor are we allowing issuers to use alternative data sources for risk adjustment and HHS-RADV. In accordance with §§ 153.700 through 153.740, we will continue to collect enrollee-level plan enrollment data, enrollee claims data, and enrollee encounter data from issuers' EDGE servers for the purposes of calculating HHS risk adjustment transfers under the State payment transfer formula. Furthermore, in accordance with § 153.630(b)(7), we will continue to use relevant medical record documentation to validate enrollee health status through review of all relevant paid/positively adjudicated pharmacy claims, validating medical records according to industry standards for coding and reporting, and having a senior reviewer confirm any enrollee risk adjustment error discovered during the initial validation audit to validate the demographic and risk score of enrollees in HHS-RADV. We also note that non-network plans may opt out of participation in HHS-RADV in favor of being assessed a default data validation charge (DDVC) as described in § 153.630(b)(10).
We appreciate the comments regarding non-network plans' potential impacts on the HHS-operated risk adjustment program. We acknowledge commenters' concern that non-network plans are likely to attract healthier enrollees. However, we do not believe this will have the impact of suppressing the statewide average premium used in the State payment transfer formula. The statewide average premium is a weighted average based on enrollment in each plan in a State market risk pool. If non-network plans offer lower premiums and attract healthier enrollees away from other plans, the statewide average premium should remain around the same value, assuming roughly the same population of enrollees remain enrolled statewide. Nevertheless, it would be likely that under such a scenario, non-network plans, if they attract healthier enrollees, would generally owe risk adjustment charges to other issuers in the relevant State market risk pool. We therefore caution issuers considering offering non-network plans to carefully weigh the impact of risk adjustment in their rating decisions.
Comment:
Overall, commenters had mixed reactions to the proposal to allow FFE States the flexibility to conduct provider access or ECP certification reviews of non-network plans provided the FFE State elects to conduct such reviews and satisfies applicable criteria to be considered to have an Effective Provider Access Review Program under proposed § 155.1050(d) and/or an Effective ECP Review Program under proposed § 155.1051.
One issuer currently offering a non-network plan shared that States generally possess unique knowledge of local market conditions, geographic constraints, provider availability, and population demographics which may make States well positioned to review non-network plans. A few commenters noted that some FFE States may already have existing regulatory frameworks or experience reviewing non-network plans. For example, one commenter shared that Ohio has experience in reviewing non-network plans, which could be leveraged by HHS and Exchanges to inform the development of effective review processes for non-network plans. However, some commenters cautioned that some FFE States currently may not be equipped to conduct their own reviews without more specific guidance from HHS regarding processes and assessment methodologies for evaluating a sufficient choice of providers under a non-network plan.
Response:
We agree that FFE States possess unique knowledge of local factors affecting consumers' ability to access a full range of providers, which can adapt certification reviews of both network and non-network plans to address local needs. We also agree that some FFE States may not be equipped to conduct reviews of non-network plans in time for the upcoming PY 2027 QHP certification cycle, since some FFE States may need to develop new regulations and operational processes to review non-network plans. Consistent with our decision to delay implementation of the proposal to permit certification of non-network plans as QHPs to PY 2028, we also will delay to PY 2028 implementation of the provisions allowing FFE States with an Effective Provider Access Review Program and/or Effective ECP Review Program to conduct certification reviews for non-network plans under § 155.1050 and § 155.1051, respectively. Specifically, we are finalizing modifications to § 155.1050(d)(1) and § 155.1051(a) such that they will be applicable to non-network plans for plan years beginning on or after January 1, 2028. We intend to issue further guidance and provide technical assistance to FFE States to help them develop their own technical capacity and processes to evaluate non-network plans for QHP certification.
Comment:
Commenters provided specific recommendations on how HHS should apply the Effective ECP Review Program to non-network plans. Commenters recommended clear, specific, and verifiable standards that issuers offering non-network plans must meet to demonstrate they provide access to ECPs under an Effective ECP Review Program prior to a non-network plan receiving certification as a QHP. For example, commenters recommended allowing issuers offering non-network plans to demonstrate that they provide access to ECPs via contracts or participation agreements with ECPs that accept the issuer's benefit amount as payment in full. Another recommendation included a more quantitative, data-driven approach that would incorporate an analysis of an issuer's benefit amounts that would then be compared to other data sources of ECP service charges in the same service area; the commenter stated that this could be accomplished by HHS defining a methodology that includes a specific percentile threshold that benefit amounts must meet, while performing additional analyses to reduce geographic disparities in access to ECPs.
Response:
In the proposed rule, we proposed that an FFE State with an Effective ECP Review Program must ensure that issuers offering non-network plans meet specific ECP requirements. Specifically, we stated at proposed § 155.1051(b) that FFE States with an Effective ECP Review Program must ensure that a non-network plan applying for certification to be offered as a QHP through an FFE demonstrates that it provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full to ensure that services will be accessible without unreasonable delay. We appreciate commenters recommending ways that non-network plans could demonstrate reasonable and timely access to ECPs. First, we do not believe it is appropriate to require FFE States to collect data from non-network plans on contracts with ECPs because non-network plans do not typically contract with providers. We also believe that our proposed requirements for an FFE State with an Effective ECP Review Program under § 156.236(b)(1) through (3) would address the commenters' request to demonstrate an ECP's acceptance of benefit amounts as payment in full. We also proposed under § 155.1051(e)(7) that we would consider whether the State collects information from issuers with non-network plans regarding the status of offers of benefit amounts as payment in full to ECPs; this would
( printed page 29786)
allow HHS to assess the State's ability to collect verifiable data that can be utilized to quantitatively assess an issuer's compliance with minimum percentage, category per county, and Indian health care requirements under § 156.236(b)(1) through (3), which can be evaluated based on benefit amounts as payment in full that were offered to or accepted by an ECP.
Additionally as part of this proposal, we intended to propose an regulatory framework for non-network plans to demonstrate a sufficient choice of providers consistent with section 1311(c)(1)(B) and (c)(1)(C) of the Affordable Care Act that is distinct from existing provider access and ECP requirements for network plans under § 156.230 and § 156.235, but also complementary to these existing requirements by proposing an alternative methodology to measure access to providers without traditional provider networks. Thus, we do not intend to prescribe billing and payment requirements by defining benefit amount percentiles that non-network plans must meet relative to an ECPs' service charges. Rather, we aim to capture facility-level data (and not service charge data from ECPs) on the number of ECPs that accept the non-network plan's benefit amount as payment in full, similar to how we currently collect how many ECPs in an issuer's network and service area accepted or were offered a contract. And, since for the reasons stated earlier in this final rule we believe it is appropriate to establish a Federal floor of baseline ECP requirements that apply across the FFE through the Effective ECP Review Program under § 155.1051, we do not intend to create more stringent requirements for FFE States than proposed Federal ECP requirements for non-network plans at this time. However, we are not limiting an FFE State's ability to create more stringent requirements than those under § 155.1051 or limiting an FFE State's ability to require a non-network plan to submit this type of data. Commenters sharing these various ways that non-network plans may demonstrate reasonable and timely access to ECPs affirms our decision to not be prescriptive in setting these requirements. We are implementing these requirements beginning in PY 2028. Additional details about these ECP requirements related to non-network plans will be detailed in the 2027 Final Letter to Issuers.
Comment:
One commenter supported HHS' approach to require that FFE States meet applicable criteria for reviewing both network and non-network plans to demonstrate having an Effective Provider Access Review Program and/or Effective ECP Review Program. While the commenter recognized that some FFE States may not yet have the expertise to review non-network plans, the commenter stated that requiring the FFE State to demonstrate the ability to review for both plan types is essential to prevent FFE States from selectively electing to only conduct reviews of network plans and choosing not to invest in or develop capacity to conduct reviews for non-network plans. Overall, the commenter believed that FFE States should accept the responsibility to conduct reviews for the full range of plan types, and that if FFE States are not prepared to do so, then FFE States should defer to HHS to conduct reviews for non-network plans.
Response:
We appreciate the commenter's support for the requirement that FFE States demonstrate the capacity to review both network and non-network plans as part of our determination of whether an FFE State has an Effective Provider Access Review Program or Effective ECP Review Program, assuming the FFE State permits non-network plans to be certified as QHPs. We also intend to conduct outreach to FFE States over the coming year to assess their current capacity and readiness to review non-network plans in advance of the PY 2028 implementation date of this policy.
Finally, while we understand commenter's desire for a State not to limit the types of plans it allows (network vs. non-network plans), we affirm that we will not require FFE States to offer non-network plans in their State. We believe that States, that know their population and local markets best, should be able to make a final determination about whether or not non-network plans are appropriate for their State. Should an FFE State choose not to allow these plans, a State would only be required to demonstrate sufficient authority and the technical capacity to review network plans to be determined to have an Effective Provider Access Review Program or an Effective ECP Review Program.
Comment:
Some commenters encouraged HHS and FFE States to publicly disclose details of non-network plan certification review processes. Some commenters recommended public disclosure of the criteria utilized to evaluate non-network plans and the outcomes of such reviews. Commenters reasoned that this reporting would promote consistency across the FFE to ensure that consumer protections are applied consistently.
Response:
We appreciate commenters' suggestions. We have laid out the criteria under which we would review non-network plans to be certified as QHPs on the FFE under § 156.236(b)(1) through (9). Additional operational details regarding non-network plan data submission for PY 2028 will be detailed in the 2027 Final Letter to Issuers with subsequent guidance anticipated in the 2028 Final Letter to Issuers. Issuers and the public can also learn more about non-network plan review processes on the QHP certification website in the Application Instructions section.[350]
However, we believe the suggested approach to publicize the outcomes of non-network reviews, which would be inconsistent with current network adequacy and ECP review procedures which do not currently publicize the outcomes of network adequacy or ECP reviews for network plans, would be inappropriate because private, market proprietary information may be published in the process. A number of public use files (PUFs) are made available to the public as part of the QHP certification process, and the Plan Attributes PUF will reflect plan attributes for non-network plans, including data originating from the issuer's Plans and Benefits Template which the issuer submits to detail plan data, including information about benefit packages, cost-sharing, and EHBs. Information on what is included in the Plan Attributes PUF can be found at the Health Insurance Exchange Public Use Files website.[351]
Lastly, since application of both the Effective Provider Access Review Program and Effective ECP Review Program would establish a Federal floor of minimum criteria that FFE States must demonstrate to adequately review non-network plans, we believe these minimum requirements will help promote a level of consistency in how non-network plans are reviewed across the FFEs. Based on our experience administering the FFEs, if non-network plans undergo consistent, standardized reviews across the FFE, this will likely facilitate consistent application of consumer protections.
Comment:
One commenter responded to HHS's request for comment on whether HHS should clarify the information FFE States with an Effective Provider Access Review Program or an Effective ECP Review Program must
( printed page 29787)
review when evaluating non-network plans to ensure alignment with HHS' approach under § 156.236(b)(4) through (b)(9). This commenter supported enumerating the information these FFE States must review to promote consistency across the FFEs and ensure non-network plan enrollees receive similar consumer protections regardless of whether HHS or the FFE State is conducting the certification review.
Response:
We appreciate the commenter supporting the clarification of the information that non-network plans must submit to the FFE listed at § 156.236(b)(4) through (b)(9) as requirements for FFE States with an Effective Provider Access Review Program and/or an Effective ECP Review Program to review non-network plans for certification. For the reasons stated earlier in this final rule, we believe these factors will yield important information that an FFE State with an Effective Provider Access Program or an Effective ECP Review Program would need to collect to ensure it has sufficient authority and the technical capacity to review non-network plans.
In response to the commenter's support for enumerating the information these FFE States must collect to promote consistency across the FFE in how non-network plans are reviewed, we are adding an additional factor related to the Effective ECP Review Program under § 155.1051(e)(11) and modifying an existing factor related to the Effective Provider Access Review Program under § 155.1050(d)(4)(vi) to indicate the State has a process to collect and review information described under § 156.236(b)(4) through (9) from non-network plans, which the non-network plan must submit for a determination that it provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full. We believe adding these additional factors is crucial to ensure safeguards are in place across the FFE so that non-network plans remain consumer protective, regardless of the entity (HHS or the FFE State) conducting the review. Requirements described under § 156.236(b)(4) through (9) are specific to non-network plans and reflect additional safeguards to ensure these plans maintain access to providers without traditional network arrangements. These requirements include assessing a non-network plan's strategy for conducting outreach to providers in their area, making benefit amounts public to enrollees, methodologies for determining benefit amounts, publishing consumer-friendly information on balance billing and potential out-of-pocket costs, the availability of exceptions processes for enrollees unable to locate providers who accept benefit amounts as payment in full, and customer services resources. As evidenced in the discussions above related to public comments received on these specific factors, it is important that non-network plans across the FFEs consistently report this information so that we and/or the FFE State can assess whether the non-network plan: (1) provides a sufficient choice of providers; (2) executes the necessary steps to effectively set data-driven benefit amounts that providers would accept in full to limit enrollee out-of-pocket costs; and (3) disseminates all the resources enrollees need to leverage non-network plans to meet their health needs.
Comment:
One commenter encouraged HHS to adopt standards for non-network plans that provide enough flexibility to accommodate innovative plan models (including related to network design) that are not purely reference-based pricing models, such as hybrid models which may blend a contracted network of providers and reference-based pricing models.
Response:
We appreciate the commenter's suggestion regarding additional variations of non-network plan design that could be supported by this policy. Encouraging innovation in plan design is the goal in which this proposal is rooted. We welcome continued engagement on ways this policy might be implemented to support variations on plan designs that do not fully rely on a contracted network to ensure access to essential community providers in accordance with HHS regulations and access to sufficient numbers and types of providers to ensure all services will be accessible without unreasonable delay, including services from providers that specialize in mental health and substance use disorders.
Comment:
Several commenters raised concerns that allowing non-network plans to be certified as QHPs as early as the PY 2027 would not allow sufficient time for States to build oversight capacity or for Federal and State regulators to coordinate regarding the approval of non-network plans seeking QHP certification. One commenter stated concern that the proposed rule does not adequately address how States will monitor whether non-network plans maintain a sufficient number of providers willing to accept the plan's benefit amount as payment in full, particularly given the absence of a mechanism to ensure that providers will continue to accept that reimbursement amount for the duration of a consumer's plan year. Another commenter raised concerns regarding the operational burden imposed by the late release of the proposed rule, leaving little time for issuers, States, and other interested parties to understand, adjust to, and implement non-network plans for the upcoming plan year.
Several commenters also recommended that HHS work with States and NAIC to ensure that non-network plans remain financially stable and that their issuers understand financial obligations associated with QHP participation. They also requested that States retain full plan approval authority, with a number of States commenting that they were grateful that HHS was not requiring States to offer non-network plans and stating that they would assess interested party interest before making any determination on whether or not they would offer non-network plans in their State. Commenters also encouraged greater coordination among CMS, State insurance regulators, and Exchanges to identify and establish realistic, actionable policies to address concerns related to non-network plans. One commenter also recommended that we extend requirements for non-network plans under § 156.236(b) to State Exchanges and SBE-FPs.
Response:
We appreciate the detailed feedback from commenters regarding State oversight capacity, implementation timelines, financial oversight, and the need for Federal and State coordination for non-network plans. We affirm that we are not requiring States to allow certification of non-network plans in their markets, including FFE States, State Exchanges, and SBE-FPs. Our proposal did not aim to interfere with whether States choose to offer these plans in general, rather we aimed to establish a clear regulatory standard that non-network plans must meet to be offered as QHPs through the FFE. State Exchanges and SBE-FPs retain full discretion and authority to determine whether non-network plan designs are appropriate for their markets, subject to § 156.236(a), if allowing non-network plans to be offered as QHPs through State Exchanges and SBE-FPs and consistent with applicable State laws and regulations. To provide more clarity, we are finalizing a clarification under § 155.1050(a)(2) to suggest these States may allow non-network plans to be offered through the Exchange “
if such plans are allowed to be offered through the Exchange
” to preserve the State's authority to determine whether non-network plans are appropriate for their markets.
( printed page 29788)
We also acknowledge the concerns raised regarding the ability of States to monitor ongoing provider availability in non-network plans, especially in the absence of a mechanism to ensure that providers will continue to accept the non-network plan's benefit amount for the duration of a consumer's plan year. We recognize that the absence of traditional network contracting structures presents unique oversight challenges and that we are not able to dictate what a provider charges for services. Providers may choose to modify charges for their services based on any number of factors, including changes in their operating expenses, changes in medical advancement, competitive pressure, or for no particular reason at all. And, they may choose to change this amount at any time. We stated that, consistent with § 156.236(b)(4), it is imperative that a non-network plan have in place a strategy for conducting continuous outreach to available providers (including ECPs) in a particular area to determine whether they would accept the plan's benefit amount as payment in full, so that the plan can make adjustments to its benefit amounts to ensure that enrollees can access a sufficient number of providers. Additionally, for the reasons stated earlier in this section of this final rule, we are confident that all the factors laid out under § 156.236(b)(1) through (b)(9) provide a means to appropriately determine if a non-network plan is providing sufficient access to providers (including ECPs), whether HHS or an FFE State is conducting the review.
Regarding the recommendation that we apply the requirements under § 156.236(b) to State Exchanges and SBE-FPs, we are declining to do so to remain consistent with the proposal to restore aspects of network adequacy authority back to these Exchanges. As we discuss in more detail in section III.D.18 of this final rule, State Exchanges and SBE-FPs have significant experience conducting provider access reviews and are well-positioned to account for the unique needs of their specific populations and markets. Accordingly, while we continue to require that State Exchanges and SBE-FPs provide sufficient access to providers in a manner that meets standards under § 156.230(a)(1)(ii) and (iii) for network plans, and under § 156.236(a) for non-network plans, as applicable, we are affording these Exchanges the flexibility to determine the specific parameters for meeting these requirements.
Regarding implementation challenges raised by commenters, we sought comment regarding the effective date of this proposal in the proposed rule, requesting comments from QHP issuers that may be interested in submitting non-network plans for QHP certification for PY 2027 or whether PY 2028 may be the soonest that any QHP issuer could realistically consider submitting non-network plans for QHP certification. We acknowledge the implementation challenges raised by commenters, especially considering the timing of the release of this final rule and the time it takes for States and issuers to develop and design plans to be submitted to us for consideration for QHP certification. In recognition of these comments that pushed for delayed implementation, and to allow States, issuers, and other interested parties sufficient time to prepare for potential certification of non-network plans as QHPs across the FFEs, we are delaying implementation of this non-network plan certification proposal to PY 2028. We believe this will allow additional, sufficient time for issuers to fully consider the finalized policies and make adequate preparations for the next QHP certification cycle to meet regulatory requirements, including but not limited to modifications to plan design, additional outreach to providers regarding benefit amounts, and developing consumer-facing materials. States would also have an additional year to consider whether they wish to allow non-network plans in their State and if any State-level legislative or regulatory actions are required before non-network plans can enter State markets. It will further provide us more time to conduct additional analyses on more complex issues raised by commenters in this final rule and engage interested parties to boost operational readiness and incorporate additional feedback prior to implementation of non-network plans. We are committed to working with States, issuers, and other interested parties during this period through interested parties outreach to support successful implementation in a manner that minimizes operational burden and reduces the risk of adverse outcomes for consumers and systems operations.
Lastly, while HHS is delaying implementation of this policy to allow non-network plans to receive certification to be offered as QHPs through the FFE beginning PY 2028, HHS is not requiring State Exchanges or SBE-FPs to also delay implementation of allowing non-network plans to be offered as QHPs through their Exchanges beginning PY 2028. Rather, State Exchanges and SBE-FPs retain full discretion and authority to not only assess whether non-network plan designs are appropriate for their markets, but also to independently determine the appropriate implementation timeline for their States if allowing non-network plans to be offered through their Exchanges. Consistent with discussions in this final rule to restore aspects of network adequacy back to State Exchanges (see section III.D.18 of this final rule), both State Exchanges and SBE-FPs have unique knowledge on local factors (for example, market conditions, geographic constraints, provider shortages, etc.) that have been consistently leveraged to conduct their own network adequacy certification reviews, which can also be utilized to conduct reviews of non-network plans. Thus, we believe these States may already possess the knowledge and expertise to begin conducting reviews of non-network plans and offering these plans through State Exchanges or SBE-FPs. For this reason, we do not desire to limit these States in proceeding with offering these non-network plans if States already allow these plans in State Exchanges or SBE-FPs or are well-positioned to begin doing so effective PY 2027. Accordingly, we are finalizing under § 155.1050(a)(2) that State Exchanges and SBE-FPs must ensure that each QHP provides sufficient access to providers in a manner that meets standards under § 156.236(a) for non-network plans for plan years beginning on or after January 1, 2027, if such plans are allowed to be offered through the Exchange, as applicable. State Exchanges and SBE-FPs still have autonomy to target implementation dates after PY 2027, if they desire.
13. Strengthening HHS' Oversight of the Administration of Advanced Payments of the Premium Tax Credit, Cost-Sharing Reductions, and User Fee Programs and Clarifying HHS' Compliance Review Authority (§ 156.480)
In the 2027 Payment Notice proposed rule (91 FR 6417), we proposed two proposals related to § 156.480. First, we proposed to modify § 156.480 to clarify HHS' authority to audit or conduct a compliance review of an issuer that offers a QHP through an Exchange for the purposes of administering and providing oversight of the APTC, CSR, and user fee programs. Specifically, we proposed to amend § 156.480(c) to provide that HHS or its designee may audit or conduct a compliance review to assess compliance with all requirements related to APTC, CSR, and user fee programs applicable to issuers offering a QHP in an Exchange, rather than only
( printed page 29789)
the requirements of 45 CFR subpart E and § 156.50, as is currently provided. For consistency, we also proposed to make conforming changes to § 156.480(c)(6) to provide that in instances where HHS enforces compliance with any requirements related to the APTC, CSR, and user fee programs for QHP issuers participating in State Exchanges or SBE-FPs, HHS may do so in accordance with § 156.805. Second, we proposed to clarify that HHS may conduct a compliance review to assess issuers' compliance with requirements related to these programs under § 156.480(c) as needed or on an annual basis rather than only on an ad hoc basis, as previously stated in the preamble to part 2 of the 2022 Payment Notice (86 FR 24244 through 24247).
To explain our first proposal, in the 2014 Payment Notice (78 FR 65078), we established HHS' authority at § 156.480(c) to assess issuers' compliance with requirements in 45 CFR part 156, subpart E through audits to ensure the appropriate use of Federal funds related to the APTC and CSR programs. After several years of experience with operating the Exchanges, in part 2 of the 2022 Payment Notice (86 FR 24244, 24246), we expanded HHS' oversight tools at § 156.480(c) to include the authority for HHS to conduct compliance reviews, in addition to audits, and expanded the scope of such audits and compliance reviews to include requirements in § 156.50 related to the user fee program, in addition to those previously referenced in part 156, subpart E. We also provided that compliance reviews conducted under this oversight authority would follow the standards set forth in § 156.715. In the proposed rule, we considered additional clarifications to HHS' authority on compliance reviews under § 156.480.
Currently, § 156.480(c) provides that in conducting APTC, CSR, and user fee audits or compliance reviews, HHS may assess an issuer's compliance with the requirements in 45 CFR part 156, subpart E and § 156.50. The regulatory text does not currently reference assessment of an issuer's compliance with other Exchange requirements related to administration of the APTC, CSR, and user fee programs that are outside of subpart E and § 156.50. For example, it does not include the assessment of grace period requirements at § 156.270(g), located in part 156, subpart C, which mandates that an issuer terminate an enrollee's enrollment after not receiving payments for any outstanding premium balance, or an amount within an issuer-established premium payment threshold, within the 3-month grace period. Noncompliance with this, and other enrollment and payment requirements, can result in an issuer receiving APTCs on behalf of an enrollee who is not eligible for APTC due to nonpayment of premiums. To prevent these improper payments, we stated in the proposed rule that it follows that HHS' administration and oversight of the APTC program should include assessment of issuers' compliance with these requirements.
To further explain, we have historically interpreted section 1313(a)(5) of the Affordable Care Act, which states that the Secretary shall implement any measure or procedure that the Secretary has authority to implement in title I of the Affordable Care Act or any other Act, to protect against fraud and abuse, and section 1321(c) of the Affordable Care Act to provide HHS with broad authority to implement oversight activities to assess compliance with all Exchange standards issued in accordance with section 1321(a)(1) of the Affordable Care Act. For example, compliance reviews conducted in accordance with § 156.715 as part of HHS' financial integrity oversight of QHP issuers in the FFE, and under the authority of Affordable Care Act section 1321(c), are not limited in scope to a set of listed regulatory requirements. Instead, § 156.715(a) identifies the scope of such compliance reviews as tools to generally ensure “ongoing compliance with Exchange standards applicable to issuers offering QHPs in a Federally-facilitated Exchange.” Audits and compliance reviews conducted as part of HHS' oversight of the APTC, CSR, and user fee programs, which ensure fiscal responsibility of issuers and compliance with the requirements for QHP issuers, fall under this same broad statutory authority. We stated in the proposed rule that while requirements related to the APTC, CSR, and user fee programs are concentrated in § 156.50 and subpart E, it was an unintended limitation to confine the scope of audits and compliance reviews conducted in accordance with § 156.480(c) to only these requirements. We noted that HHS has issued regulations that impact administration of these programs in other regulatory sections. For example, noncompliance with the premium payment requirements established in subpart C of part 156 may result in an issuer's receipt of improper APTCs on behalf of ineligible enrollees.
We stated in the proposed rule that as we continue to conduct audits and compliance reviews, we want to ensure that we are clear on our authority to assess and enforce compliance with requirements related to the APTC, CSR, and user fee programs that are outside subpart E and § 156.50. Therefore, to provide this clarity, we will revise the introductory text in § 156.480(c) and make conforming revisions to paragraph (c)(6) to state that HHS may audit or conduct compliance reviews and enforce issuer compliance with all applicable requirements related to the APTC, CSR, and user fee programs.
To explain our second proposal, we proposed to revise our current position in the preamble of part 2 of the 2022 Payment Notice (86 FR 24244 through 24247), stating that HHS conducts compliance reviews on an ad hoc basis, to provide that HHS may conduct compliance reviews as needed, including on an annual basis based on HHS' assessment of noncompliance with the applicable requirements and any identified issues related to noncompliance.
In part 2 of the 2022 Payment Notice (86 FR 24244 through 24247), we stated that compliance reviews would be conducted on an ad hoc basis to provide HHS with a mechanism to address situations where a systemic error or issue is identified during an audit, and if HHS suspects similarly situated issuers may have experienced the same systemic error or issue but were not selected for audit in the year in question. However, we stated in the proposed rule that we have found that this approach is insufficient. We noted, for example, that annual APTC, CSR, and user fee program audits of issuers in State Exchanges often identify data inaccuracies in issuers' enrollment and payment data that resulted in APTC over- or underpayments. While annual, these audits are conducted on benefit year data after the close of the 3-year window for resolution of payment inaccuracies described in § 156.1210(c).[352]
We stated that annual compliance reviews would provide issuers with an opportunity to proactively correct these data inaccuracies prior to the scheduled audits, which would ensure better compliance with APTC and other related requirements and, in turn, more quickly resolve any APTC over- or
( printed page 29790)
underpayments. We stated that with compliance reviews only occurring on an ad hoc basis, we are unable to regularly and fully address these issues prior to the audit process. As a result, we proposed to revise our position such that HHS may conduct compliance reviews as needed, including on an annual basis, based on its assessment of identified issues related to noncompliance. We stated that we were not seeking to make amendments to regulation text at § 156.480(c) to address this; rather, we were proposing to clarify in the preamble of this final rule that the compliance review authority would allow us to conduct compliance reviews on an annual or as needed basis.
In summary, we proposed to add language to the introductory text of § 156.480(c) which states that HHS may audit or conduct a compliance review of an issuer offering a QHP through an Exchange to assess its compliance with the applicable requirements related to administration of the APTC, CSR, and user fee programs. We also proposed to add conforming language to § 156.480(c)(6) to state that in instances where HHS enforces compliance with any requirement related to APTC, CSR, and user fee programs for QHP issuers participating in State Exchanges or SBE-FPs, HHS may do so in accordance with § 156.805. Finally, as discussed above, we proposed to revise our position on the frequency of compliance reviews such that HHS would conduct compliance reviews as needed, including on an annual basis based on its assessment of identified issues related to noncompliance; however, we did not propose amendments to regulation text at § 156.480(c) to address this.
We sought comment on these proposals.
After consideration of comments, and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these policies as proposed. We summarize and respond below to public comments received on the proposed clarification that HHS may audit or conduct a compliance review of an issuer offering a QHP through an Exchange to assess its compliance with the applicable requirements related to administration of the APTC, CSR, and user fee programs, and the proposal that HHS may conduct compliance reviews on an as needed or annual basis, rather than just on an ad hoc basis.
Comment:
Several commenters generally supported HHS strengthening the oversight of the APTC, CSR, and user fee programs, and some of these commenters also supported clarifying HHS' authority to audit or conduct compliance reviews to assess compliance with these programs. Another commenter recommended that to prevent increased administrative burden, when conducting audits, HHS should allow issuers to consolidate multiple audits into a single audit across HIOS IDs under common company control.
Some commenters were concerned that if compliance reviews occur on an as needed or annual basis, the reviews may place significant administrative burdens on issuers. Several commenters provided recommendations for how HHS should conduct compliance reviews to prevent administrative burdens on issuers. One commenter encouraged HHS to consider operational impacts and ensure that the timing, scope, and frequency of reviews remain predictable and risk-based to avoid administratively and financially burdening issuers. Another commenter recommended that HHS establish a predictable, risk-based audit cadence every three years while preserving targeted review authority in response to certain data inaccuracies, complaints, or identified compliance risks. Another commenter noted that between existing statutory safeguards, current CMP authority, and State insurance oversight, there are multiple layers of oversight and that expanding review frequency or adding duplicative Federal audit processes would increase administrative burden and costs, since it would divert resources from other activities, and recommended that HHS reconsider the scope of these proposed enforcement expansions to ensure they align with the Administration's commitment to reducing unnecessary regulatory complexity.
Response:
We are finalizing these proposals as proposed. We appreciate commenters' recommendations on how best to conduct audits and compliance reviews while preventing increased administrative burdens on issuers. We intend to work with issuers to identify additional efficiencies to prevent undue burden as we follow the audit procedures described under § 156.480(c).
In terms of compliance reviews, we believe that it is important that we safeguard Federal funds, and conducting compliance reviews on an as needed or annual basis is an important part of these safeguards. By conducting compliance reviews on an as needed or annual basis, we are ensuring that issuers resolve data inaccuracies on a timely basis, which may result in over- or underpayments of Federal funds, such as APTC, on behalf of enrollees to issuers. Compliance reviews, alongside audits and other enforcement mechanisms such as CMPs, are a necessary oversight tool to aid both issuers and HHS in ensuring compliance with the applicable APTC, CSR, and user fee program requirements. Further, we do not believe that compliance reviews occurring on an annual or as needed basis will create additional burdens on issuers.
Moreover, as discussed in the proposed rule (91 FR 6418), experience with past audits that occur after the close of the 3-year window for resolution of payment inaccuracies described in § 156.1210(c) are still finding systemic errors and numerous data inaccuracies. For example, annual APTC, CSR, and user fee program audits of issuers in State Exchanges often identify data inaccuracies in issuers' enrollment and payment data that resulted in APTC over- or underpayments. Therefore, we believe that it is in the best interest of the issuer, State, and HHS to conduct compliance reviews on an annual or as needed basis, to provide timely reporting to issuers and States and allow the issuer to proactively resolve data inaccuracies or any issues of noncompliance resulting from systemic errors prior to the annual audit process (and the 3-year cutoff after which issuers would not receive additional APTCs as a result of data inaccuracies). We also believe that conducting compliance reviews on an as needed or annual basis and providing issuers and States information to resolve payment inaccuracies within the 3-year window will help to reduce many burdens that arise during the audit process. We will work with States and issuers during compliance reviews, which will be conducted annually or as needed, to conduct the reviews efficiently and without undue administrative burden. As with audits, issuers will have an opportunity to provide feedback that HHS considers to improve future compliance reviews and ensure that the process is not overly burdensome.
14. Factors Considered in Determining the Amount of CMPs and HHS' Authority To Impose CMPs Against Issuers in State Exchanges and SBE-FPs (§ 156.805)
In the 2027 Payment Notice proposed rule (91 FR 6418), we proposed two proposals related to § 156.805. First, we proposed to amend § 156.805(b) to reiterate what factors HHS considers when determining the amount of CMPs as enforcement remedies against QHP issuers in Exchanges. Specifically, to
( printed page 29791)
increase transparency in how HHS calculates the amounts of CMPs imposed against QHP issuers for violations described in § 156.805(a), including but not limited to substantial noncompliance with Exchange standards under parts 153 and 156 of title 45, we proposed to reiterate in § 156.805(b) that in determining the amount of CMPs, in addition to the factors HHS takes into account when determining a CMP amount listed in § 156.805(b)(1) through (3), HHS would identify the lawful purpose or purposes of the CMP amount. As discussed in section III.A.1. of the proposed rule, to align with these proposed amendments to § 156.805(b), we also sought to clarify the factors considered in determining the CMP amount and the purpose of the CMP in § 150.317.
Second, we proposed to amend § 156.805(f) to clarify the authority HHS has to impose CMPs against issuers in State Exchanges or SBE-FPs for identified violations. Specifically, we proposed to amend § 156.805(f) to clarify that HHS' authority to impose CMPs against issuers in State Exchanges or SBE-FPs includes the authority to impose CMPs for identified violations of any Exchange requirements and standards applicable to issuers offering a QHP in an Exchange, when a State notifies HHS that it is not enforcing these requirements or HHS determines that a State is failing to substantially enforce these requirements. As detailed further below, we did not propose any other changes to the legal bases for imposing CMPs against issuers in FFEs nor the circumstances in which HHS may exercise its enforcement authority against issuers in State Exchanges or SBE-FPs.[353]
Under the first proposal, sections 2723(b)(2), 2718(b)(3), and 2761(b) of the PHS Act and section 1321(c)(2) of the Affordable Care Act authorize the Secretary to impose CMPs when a QHP issuer fails to meet the required standards.[354]
In prior rulemakings (78 FR 54121; 79 FR 15240, 15242 through 15243; 79 FR 30240, 30264; 81 FR 12204, 12313 through 12314; and 81 FR 61538, 61581), to implement these statutory provisions, we established provisions at § 156.805 to govern the bases and process for imposing CMPs against QHP issuers in Exchanges when HHS has reasonably determined that the issuer has engaged in one or more of the enumerated actions listed in § 156.805(a)(1)-(7), including noncompliance with issuer standards and requirements under 45 CFR parts 153 and 156. Further, in part 2 of the 2022 Payment Notice (86 FR 24242 through 24243), we set forth the framework for HHS' enforcement of the applicable Federal APTC, CSR, and user fee standards in situations where State authorities fail to substantially enforce those standards for the QHP issuers participating in State Exchanges and SBE-FPs, and HHS' authority to impose associated CMPs.
Since 2014, Exchange regulations have imposed standards and requirements on issuers offering QHPs participating in Exchanges, including, but not limited to, standards and requirements under 45 CFR subtitle A, subchapter B, parts 153 and 156,[355]
such as compliance with premium payment policies in part 156. Historically, to facilitate QHP issuers' compliance with Exchange standards and requirements, HHS conducted audits, the results of which played a critical role in ensuring that Federal funds are appropriately safeguarded. However, we exercised enforcement discretion and did not seek to impose CMPs to enforce the findings in such audits, to give issuers time to acclimate to a new market and learn the regulatory scheme, and relied instead on other mechanisms available, such as recouping overpayments, decertification of QHP issuers for egregious violations, and corrective action plans.[356]
But, as we stated in the proposed rule, as the markets have matured, HHS audits consistently reveal that in practice, issuers implement inconsistent policies, even after we have provided such issuers with guidance and recommendations to cure identified noncompliance. We stated that continued violations put HHS at risk of making improper payments, such as APTC payments for enrollees with noncompliant effectuations or continued enrollments that should have been cancelled or terminated. We further stated that violations may be identified long after an improper payment is made,[357]
and retroactive changes often involve loss of eligibility for APTC, disenrollment of coverage, and reversal of paid claims, which together can cause enrollees outsized financial harm. We noted, for example, that if we were to find that an issuer maintained an enrollee's coverage in violation of an enrollment or payment requirement and directed the issuer to retroactively terminate the enrollee's coverage to correct the noncompliance, the enrollee would lose their APTC for the months they were covered, which may have tax implications, and the enrollee could be liable for claims costs previously covered under their plan which might, as a practical matter, be difficult for a QHP issuer to recover. We stated that to minimize these needless harms to enrollees and QHP issuers alike and bolster compliance with HHS standards and requirements applicable to issuers offering QHPs participating in Exchanges, HHS oversees QHP issuer compliance in this area.
We proposed to amend § 156.805 to reiterate that HHS would identify the lawful purpose or purposes of the CMP when calculating CMP amounts. As noted above, section 2723(b)(2) of the PHS Act and section 1321(c)(2) of the Affordable Care Act authorize HHS to impose CMPs to enforce Exchange standards and requirements applicable to issuers offering QHPs participating in Exchanges. Section 2723(b)(2)(C)(i) of the PHS Act caps the amount of the CMP at $100 (as adjusted annually under the Federal Civil Penalties Inflation Adjustment Act Improvements Act of 2015 and other relevant laws)
358
for each day for each individual for which an entity fails to comply with a relevant statutory or regulatory requirement. Further, when assessing a CMP, section 2723(b)(2)(C)(ii) of the PHS Act requires HHS to consider the previous record of compliance of the entity with the applicable legal provisions and the gravity of the violation.
As discussed in the proposed rule, that broad delegation of enforcement authority can encompass several traditional purposes of monetary
( printed page 29792)
remedies. For example, in some circumstances, when consistent with these provisions and applicable law, HHS might impose a CMP to penalize a QHP issuer when an audit reveals that it failed to comply with an applicable law in prior years and thereby collected payments for some period despite not being entitled to those payments under a public benefits program the government runs. In other circumstances, HHS might impose a CMP to bring a currently noncompliant QHP issuer into compliance with relevant laws, such as if HHS discovers that a QHP issuer is currently refusing to comply with particular laws. And in still other circumstances, HHS might impose a CMP to try to make a wronged party whole for harm caused by the QHP issuer's conduct, such as if HHS discovers violations that cost the public money and HHS is able to make the Government whole through its CMP authority.
We stated that these purposes for which HHS imposes CMPs related to enforcement of Exchange standards and requirements applicable to issuers offering QHPs participating in Exchanges are not mutually exclusive. To increase transparency in how HHS calculates the amounts of CMPs imposed against QHP issuers for violations described in § 156.805(a), including but not limited to substantial noncompliance with Exchange standards under parts 153 and 156 of title 45, we proposed to clarify that HHS will identify the underlying lawful purpose or purposes of a CMP when calculating the relevant amount.
We stated that QHP issuers have been on notice of possible CMPs for noncompliance since the inception of the Exchange, through regulations, and directly through subsequent HHS communications. We noted, for example, that in the 2019 CMS Program Integrity letter to FFE issuers,[359]
we stated that CMPs may be imposed against QHP issuers for violations of applicable regulatory requirements identified through FFE audits of APTCs and user fees beginning for benefit year 2020. We added similar language to APTC and user fee audit reports for FFE issuers for benefit years 2016-2019,[360]
and we restated that we may begin imposing CMPs starting with 2020 benefit year APTC and user fee audits of FFE (and SBE-FP) issuers in a Fall 2023 webinar for all FFE and SBE-FP issuers.[361]
In the proposed rule, we noted that QHP issuers now have over a decade of experience implementing applicable Exchange standards and requirements. We stated that given the duty to safeguard Federal funds, ongoing concerns with QHP issuers' inconsistent premium payment policies, and in light of ongoing audit observations and findings of noncompliance,[362]
HHS plans to proactively monitor and enforce compliance with the Exchange standards and requirements applicable to issuers offering QHPs participating in Exchanges, including through the imposition of CMPs, as warranted.
Second, we proposed to clarify the authority that HHS has to impose CMPs against issuers in State Exchanges or SBE-FPs when a State notifies HHS that it is not enforcing the applicable requirements or HHS determines that a State is failing to substantially enforce these requirements. Specifically, we proposed to amend § 156.805(f) to clarify that HHS' authority to impose CMPs against issuers in State Exchanges or SBE-FPs includes authority to impose CMPs for identified violations of the requirements applicable to the noncompliant actions described in § 156.805(a) that are applicable to issuers offering a QHP in a State Exchange or SBE-FP, including substantial noncompliance with issuer standards and requirements under parts 153 and 156 of title 45, as opposed to just those requirements in subpart E or § 156.50, as currently written. We also proposed a conforming change to § 156.800.
In prior rulemaking (86 FR 24248 through 24252), we set forth the framework, consistent with section 2723(b) of the PHS Act and section 1321(c)(2) of the Affordable Care Act, for HHS' authority to enforce applicable Exchange standards for QHP issuers participating in State Exchanges and SBE-FPs. We further clarified that this enforcement authority arises when a State authority notifies HHS that it is not enforcing these standards or HHS determines that a State has failed to substantially enforce these standards, and that if HHS has this enforcement authority, HHS could impose a CMP. However, as we stated in the proposed rule, when establishing this framework, we inadvertently limited the scope of HHS' authority under § 156.805(f) to enforcement of only those requirements in subpart E of part 156 or in § 156.50.
To align with HHS' statutory authority, we proposed to amend § 156.805(f) to expressly provide that when appropriately triggered, HHS has the authority to enforce the requirements applicable to the noncompliant actions described in § 156.805(a) that are applicable to issuers offering a QHP in a State Exchange or SBE-FP, as well as the authority to impose CMPs against a QHP issuer in a State Exchange or SBE-FP on the same grounds for which it can impose CMPs for QHP issuers in a FFE under § 156.805. We further stated that amending the language to expressly address HHS' enforcement authority for these requirements would help to ensure that HHS can hold all issuers accountable for violations of requirements that result in improper APTC payments.
We stated that this proposed amendment would not usurp the States' power to enforce these requirements in their own Exchanges. As previously established in prior rulemaking, the process for imposing CMPs must either require that the State notify HHS that it is failing to enforce the requirements of subpart E or § 156.50 or that HHS make its own determination, following the standards in § 150.201,
et seq.,
that the State is failing to substantially enforce these requirements.
In summary, we proposed to amend § 156.805(b) to reiterate that in determining the amount of CMPs, in addition to the factors HHS takes into account when determining a CMP amount listed in § 156.805(b)(1) through (3), HHS would identify the lawful purpose or purposes of the CMP amount. We also proposed to amend § 156.805(f) to provide that when appropriately triggered, HHS would enforce the requirements applicable to the noncompliant actions described in § 156.805(a) that are applicable to issuers offering a QHP in a State Exchange or SBE-FP, and has the authority to impose CMPs against a QHP issuer in a State Exchange or SBE-FP on the same grounds for which it can impose CMPs for QHP issuers in an FFE.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing the amendments to § 156.805(b) and (f) as proposed. We
( printed page 29793)
summarize and respond below to public comments received on the proposed reiteration in § 156.805(b) that in determining the amount of CMPs, in addition to the factors HHS takes into account when determining a CMP amount, HHS would identify the lawful purpose or purposes of the CMP amount, and the proposed amendments to § 156.805(f) to clarify HHS' authority to impose CMPs against issuers in State Exchanges and SBE-FPs.
Comment:
Several commenters supported the proposal to reiterate that when HHS determines the amount of a CMP, HHS would identify the lawful purpose or purposes of the CMP. One of these commenters recommended that if the proposal is finalized, HHS should minimize unintended disruption to consumers receiving ongoing coverage, and such actions could include enrollment protections and transition safeguards where enforcement actions affect issuer participation or plan operations.
Response:
We appreciate comments on the proposed revisions to §§ 150.317 and 156.805(b) and are finalizing these provisions as proposed. As for concerns about the unintended disruption of consumers' ongoing coverage, we note that the audits and CMPs discussed in this section do not typically occur until after the benefit year has closed, and therefore, we do not expect these provisions to retroactively impact enrollee coverage for the benefit year. However, CMPs should promote future compliance by issuers in their participation or plan operations to ensure that enrollee coverage is appropriate and compliant with all applicable Exchange requirements, such as premium payment requirements.
Comment:
Other commenters recommended clarifications regarding when a CMP would be imposed. One commenter stated the proposed language for § 156.805(b) would expand enforcement authority without defining the nature or severity of conduct which would result in the imposition of a CMP and recommended the adoption of specific and measurable criteria for violations, including safe harbors for good faith compliance efforts. The commenter also recommended that HHS articulate factors considered, such as issuer size, duration of violation, and consumer harm, to help ensure that CMP amounts are proportional to the nature of the violation and issuer size. Another commenter urged HHS to clarify that CMPs will be imposed only for actions solely within an issuer's control. The commenter stated that many administrative functions are performed by Exchanges and are outside of issuers' control; therefore, issuers should not be subject to CMPs that result from operational failures or determinations that are an Exchange's responsibility, and rather than imposing CMPs, actions attributed to an Exchange should be addressed through appropriate oversight of the Exchange.
Response:
HHS' audit processes and regulations for imposing CMPs provide issuers with information on whether a CMP will be imposed and describe what factors HHS takes into consideration when determining the CMP amount. Under § 156.805(a), if there is credible evidence, HHS may impose CMPs if there is a determination that an issuer has engaged in certain actions. Such actions include when there is misconduct or substantial noncompliance by the issuer with Exchange standards and requirements applicable to QHP issuers, which include requirements and issuer standards under 45 CFR parts 153 and 156. If HHS seeks to impose a CMP, when determining the CMP amount, along with considering the lawful purpose of the CMP, HHS may also take into account the factors under § 156.805(b)(1)-(3), which we did not propose to change in this rule. HHS may consider the level of the violation, as determined in part by the frequency of the violation, taking into consideration whether any violation is an isolated occurrence, represents a pattern, or is widespread. HHS may also consider any aggravating or mitigating circumstances or other such factors as justice may require. Therefore, if factors such as volume of violations, which may correlate with issuer size based on the volume of policies, duration of violations, financial impact, and good faith compliance efforts fall within the factors described in § 156.805(b)(1)-(3), then HHS may take those factors into consideration when determining the CMP amount.
Additionally, in accordance with regulations at § 156.480(c), HHS conducts entrance and exit conferences for audits (including those which may result in CMPs) and provides issuers with documentation such as preliminary [363]
and final audit reports, which provide information on HHS' reasoning for proposing a CMP and the CMP amount. During audit entrance and exit conferences and in these audit reports, HHS will continue to work collaboratively with issuers to ensure they are directly informed of the process and methodology for the CMP determination and CMP amount.
Further, as discussed above, HHS may impose CMPs if an issuer has engaged in actions where there is misconduct or substantial noncompliance with Exchange standards and requirements applicable to QHP issuers, which includes requirements and standards for QHP issuers under 45 CFR parts 153 and 156. HHS has discretion in determining whether to impose a CMP. As described in § 156.805(b)(3), HHS may consider any aggravating or mitigating circumstances or other such factors as justice may require. Conduct outside of the issuer's control could be considered a mitigating circumstance that HHS could consider when determining the CMP amount.
Comment:
A few commenters supported the proposal to clarify that when appropriately triggered, HHS has the authority to impose CMPs against issuers in State Exchanges and SBE-FPs for identified violations of requirements described in § 156.805(a). One commenter supported the clarification and stated that it reinforces the consequences for failing to comply with requirements and will help to restore accountability for issuers, as well as encourage better State performance and help to maintain accountability across all Exchanges without overriding State roles in routine cases. Another commenter supported the clarification and HHS' active enforcement to safeguard individual and government spending (that is, premiums and APTC) against issuer noncompliance. One commenter, although supportive, raised concerns that an expansion in authority may create conflicts with the Exchange's implementation and recommended working with State Exchanges to address compliance concerns. One commenter stated that enforcement must account for variability in State regulatory authorities, respect State roles in regulating their Exchanges, and avoid unintentional Federal preemption of valid State requirements.
Several commenters opposed the proposal, stated concerns about expanding HHS' enforcement authority beyond statutory limits, and stated that the proposed clarification encroaches upon State authority. One commenter noted that it would be contrary to section 1321 of the Affordable Care Act to penalize issuers for failing to comply with State guidance or for violations stemming from State Exchange failures, recommending that HHS refrain from expanding its CMP authority. Another
( printed page 29794)
commenter stated that because HHS enforcement authority is limited to specific enumerated circumstances tied to the APTC, CSR, and user fee programs, expanding HHS' authority would encroach into areas reserved for the States by Congress, going against the Affordable Care Act's Federal-State framework. Another commenter stated the current regulations already appropriately respect the role of States in regulating their Exchanges, and further stated the proposed amendments deviate from constitutional norms and usurp States' constitutional roles as regulators within their own borders. Another commenter opposed the clarification and stated that HHS intervention should be limited to only when the State explicitly notifies HHS it is not enforcing requirements. Another commenter opposed the clarification because State Exchange issuers would be exposed to substantial financial penalties in circumstances where they are complying with State requirements, creating conflicting and duplicative enforcement.
A few commenters recommended that, if these proposals are finalized, HHS defer the applicability of these provisions to give State Exchanges, SBE-FPs, and issuers time to make necessary adjustments. One commenter recommended allowing a safe-harbor period of 1 year to allow time for State Exchanges, SBE-FPs, and issuers to address any changes in regulatory scope and obligations. Another commenter recommended deferring enforcement of CMPs against issuers in State Exchanges or SBE-FPs for 6 months following the applicability date for these provisions to allow issuers time to update compliance processes, seek appropriate guidance, and align internal controls to avoid the risk of inadvertent noncompliance.
One commenter recommended publishing implementation guidance and considering implementing phase-in periods for the new enforcement procedures to allow time for issuers, agents, and brokers to adapt their operational processes and internal compliance systems.
Response:
We appreciate these comments and are finalizing these provisions as proposed. We agree that the clarification that HHS can assess compliance with any applicable Exchange requirements helps to ensure issuer accountability, appropriately safeguard Federal funds, and ensure that there is accountability for Exchange standards across every Exchange.
As stated above, we did not propose any changes to the circumstances in which HHS may exercise its enforcement authority against issuers in State Exchanges or SBE-FPs. We are not expanding HHS' enforcement authority beyond statutory limits and are merely reiterating current authority governing when HHS can take enforcement actions against issuers in State Exchanges and SBE-FPs. In the proposed rule (91 FR 6420), we stated that this proposed amendment would not usurp States' power to enforce these requirements in their own Exchanges and therefore, this proposal would align with section 1321 of the Affordable Care Act. As previously established in prior rulemaking (86 FR 24248 through 24252), HHS may not impose CMPs unless either the State notifies HHS that it is failing to enforce Exchange requirements or HHS makes its own determination, following the standards in § 150.201,
et seq.,
that the State is failing to substantially enforce these requirements. Therefore, we disagree that the finalized provisions will encroach upon States' authority and that HHS is improperly expanding its enforcement authority beyond statutory limits.
When developing the State-Federal regulatory framework for CMPs, we set forth the framework to be consistent with section 2723(b) of the PHS Act and section 1321(c)(2) of the Affordable Care Act, which allows the Secretary to implement Exchange standards in a State when directly authorized to do so. The PHS Act and Affordable Care Act authorize the Secretary to do so when a State has failed to substantially enforce provisions for health insurance issuers in the State. This authority includes imposing CMPs for issuers' failure to comply with Exchange requirements, such as APTC, CSR, and user fee program requirements. Additionally, the regulatory framework takes into consideration States' powers to regulate their own Exchanges, as HHS is unable to impose CMPs against issuers in State Exchanges or SBE-FPs unless specific statutory and regulatory requirements are met, and noncompliance is identified for requirements enforceable by HHS under § 156.805(f). As such, we do not believe that there is conflicting or duplicative enforcement.
For the comments suggesting HHS delay the applicability date of HHS enforcing requirements in State Exchanges or SBE-FPs, we do not agree. This policy only clarifies current HHS authority and is not making any changes to the Exchange requirements with which issuers are required to comply. Issuers and States have been on notice prior to this rulemaking [364]
that HHS can enforce in instances in which a State Exchange or SBE-FP informs HHS that it is not enforcing these requirements or HHS determines that the State Exchange or SBE-FP is not substantially enforcing these requirements.
Lastly, we are finalizing HHS' authority under § 156.805(f), which allows for the imposition of CMPs against QHP issuers for certain actions. We note that the comment regarding guidance and an implementation phase for agents and brokers to adapt their operational processes and internal systems is out of scope of this final rule because it does not relate to our proposal—these amendments will impact issuers and not agents and brokers. However, we appreciate the commenter's attention and feedback.
Comment:
Commenters provided additional recommendations on determinations for when State Exchanges or SBE-FPs are not enforcing requirements. One commenter recommended that HHS publish a list of Exchange requirements that details what State Exchanges or SBE-FPs have informed HHS they are not enforcing the requirements or when HHS has determined that the State Exchange or SBE-FP substantially failed to enforce Exchange requirements. Another commenter noted that the current authority for HHS to enforce requirements in subpart E of part 156 or in § 156.50 against issuers participating in State Exchanges and SBE-FPs rests on questionable statutory authority, as this commenter believed that there is no clear statutory authority allowing this, and recommended that HHS clearly articulate the parameters of its authority. The commenter also recommended that HHS provide clear notice to regulated parties that responsibility has shifted to HHS to enforce requirements, so that issuers are not subject to conflicting regulatory directives. Another commenter recommended that HHS issue further rules detailing circumstances in which HHS will deem a State Exchange's or SBE-FP's enforcement activities insufficient and that HHS should further establish procedures in advance via notice and public comment in cases of intended enforcement.
Commenters also provided recommendations on how to best implement a framework for imposing CMPs against issuers in State Exchanges or SBE-FPs. One commenter
( printed page 29795)
recommended that HHS work closely with States on developing and implementing a CMP framework for issuers and that HHS should prioritize aligning any Federal penalty framework with State oversight efforts to ensure it does not disrupt a State's regulation of its Exchange. Another commenter stated that enforcement must account for variability in State regulatory authorities, respect State roles in regulating their Exchanges, and avoid unintentional Federal preemption of valid State requirements.
Response:
We will not impose CMPs against QHP issuers in State Exchanges and SBE-FPs unless we determine that HHS is responsible for enforcing Exchange requirements, which occurs when HHS is notified by a State Exchange or SBE-FP that the Exchange is not enforcing these requirements or HHS follows the processes under § 150.201
et seq.
and determines the State Exchange or SBE-FP is not substantially enforcing these requirements. We intend to provide notification to State Exchange or SBE-FP issuers if HHS is responsible for enforcement and may impose CMPs against issuers in these Exchanges. For example, we could provide notification through audit processes, such as the preliminary or final audit reports.
Additionally, as discussed above, HHS' authority comes from statutory provisions which grant it enforcement authority over Exchange requirements, including those related to the APTC, CSR, and user fee programs, when a State does not substantially enforce them. Further, regardless of whether a State Exchange or SBE-FP is responsible for enforcing requirements against issuers within its Exchange or HHS is responsible for such enforcement, the requirements do not change; rather, it is merely the entity responsible for enforcement that would change. Further, section 1321(d) of the Affordable Care Act provides that there would be no interference with State regulatory authority. Therefore, there would not be any conflicts between State and Federal law if HHS is responsible for enforcement, as the requirements would be applied equally, just as they would be if the State is enforcing the requirements.
15. Administrative Review of QHP Issuer Sanctions (§§ 156.903 and 156.935)
In the 2027 Payment Notice proposed rule (91 FR 6420), to improve the accuracy of hearing decisions and increase hearing efficiency, we proposed to amend the review process that governs administrative appeals of QHP issuer sanctions imposed under § 156.800, including QHP decertification actions and CMPs imposed against QHP issuers for, among other actions, violations of Exchange standards. First, under § 156.903, we proposed to allow an administrative law judge (ALJ) who presides over an administrative appeal of a QHP issuer sanction imposed in accordance with § 156.800 to issue subpoenas, upon his or her own motion or at the request of a party, if the subpoenas are reasonably necessary for the full presentation of a case. Second, to expedite the process of appeals and limit duplication, we proposed to amend § 156.935 so that the discovery provisions set forth therein do not apply to administrative appeals of proposed CMPs for violations identified through audits of the APTC, CSR, or user fee programs conducted in accordance with § 156.480(c). We stated that if finalized as proposed, these amendments would apply to appeals filed on or after the effective date of the final rule.
In the 2014 Payment Notice (78 FR 65079), we codified the administrative appeals process for QHP issuers in an FFE to challenge the imposition of a sanction, as described in § 156.800. These procedures include the opportunity for a hearing before an ALJ of the HHS Departmental Appeals Board (DAB). In part 2 of the 2022 Payment Notice (86 FR 24253), we further amended these procedures to affirm that the process applies to appeals of sanctions imposed against QHP issuers participating in any Exchange and to align with the DAB's internal practices for administrative hearings to appeal CMPs.
The DAB's internal practices include procedures that ALJs and parties must follow for appeals and administrative hearings, and ALJs and parties must also follow any relevant agency's administrative hearing procedures as prescribed by the agency through regulation for the agency's programs.[365]
The DAB's procedures currently allow parties to request subpoenas, and they allow ALJs to issue a subpoena if the ALJ is authorized by law to issue a subpoena and applicable regulatory requirements are met.[366]
However, currently, 45 CFR part 156, subpart J does not provide the authority for the ALJ to issue subpoenas in hearings requested by parties to appeal the imposition of a QHP issuer sanction, as defined in § 156.800. We stated in the proposed rule that having the option to issue a subpoena would help the ALJ obtain necessary documentation, information, and potential testimony from witnesses to fully develop a case before issuing a decision, which could streamline hearing processes and improve the accuracy of DAB decisions, benefiting both parties. We further stated that granting ALJs the authority to issue a subpoena would also align with other similar programs.[367]
Therefore, to further align HHS administrative appeal procedures with the DAB's procedures and improve the speed and accuracy of the hearing process, we proposed to add the ability to issue a subpoena in the ALJ's current authority under § 156.903.
As part of this provision, we also proposed that a party must file a written request for a subpoena with the ALJ at least 5 calendar days before the date set for the hearing and that the request must identify the witness(es) or documents to be produced, describe their address(es) or location(s) with sufficient particularity to permit them to be found, specify the pertinent facts the party expects to establish by the witness(es) or documents, and indicate why those facts could not be established without use of a subpoena. We stated that establishing these requirements in regulation would provide structure to the subpoena request, thereby increasing the efficiency with which ALJs can exercise the proposed subpoena authority. We further stated that these requirements would also ensure that parties requesting subpoenas provide ALJs with all relevant information ALJs will need to determine if the subpoena is reasonably necessary for full presentation of the case.
Second, to expedite the process of appeals and limit duplication, we proposed to amend § 156.935 to ensure that the discovery provisions set forth therein do not apply to administrative appeals of notices of proposed CMP assessments for violations identified through audits of the APTC, CSR, or user fee programs conducted in accordance with § 156.480(c). To explain, current audit processes under § 156.480(c)(3) require that HHS (1) conduct an audit entrance conference with each issuer selected for audit to discuss the scope of the audit, (2) provide issuers with preliminary audit
( printed page 29796)
findings and an opportunity to refute the preliminary findings prior to receiving the final audit report, and (3) provide issuers with an opportunity to discuss final audit findings during an exit conference. In addition, audits are collaborative, meaning that at any point during the audit, issuers can ask questions of the auditors or seek clarification on the information or documentation needed. Further, in conjunction with these audit processes and in accordance with § 156.806, when imposing a CMP, HHS must provide written notice to the issuer that describes the potential violation(s), provides 30 days from the date of the notice to respond and provide additional information to refute the allegations, and states that a CMP may be assessed if the allegations are not refuted as determined by HHS.
During the established audit processes, HHS makes available to issuers relevant information that HHS relies on in making final audit determinations, including written audit procedures, and provides issuers with multiple opportunities to ask HHS questions about the audit procedures and audit findings. Should HHS determine that a CMP is appropriate, HHS would also make relevant information that HHS relied on to determine the CMP amount available to the issuer during the audit process. Therefore, as we stated in the proposed rule, under these established audit processes, issuers are able to develop an extensive record that can inform a CMP appeal. For these reasons, we stated that we believe issuers would not need to rely on the time-consuming process of discovery for information to develop a record for an administrative appeal of a notice of proposed CMP assessment for violations identified through audits of the APTC, CSR, or user fee programs.
Similarly, we stated that these established audit procedures already allow HHS to obtain information necessary to inform final audit findings from the issuer during the audit process, limiting the need for discovery of information. Therefore, to prevent duplicative efforts for gathering documentation and information and to reduce burden on both parties to an appeal, we proposed adding a new paragraph to § 156.935 which would exclude appeals of CMPs resulting from audits at § 156.480(c) from the process of discovery.
In summary, we proposed to add a new paragraph to § 156.903 which provides the ALJ with the authority to issue subpoenas, upon his or her own motion or at the request of a party, if they are reasonably necessary for the full presentation of a case for an administrative appeal brought under § 156.805 or § 156.810. We also proposed to add a new paragraph to § 156.935 to ensure that the discovery provisions set forth therein do not apply to appeals of proposed CMPs imposed under § 156.805 resulting from audits at § 156.480(c). We stated that, if finalized as proposed, these amendments would apply to appeals filed on or after the effective date of the final rule.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond below to public comments received on the proposed additions to § 156.903 to grant ALJs the authority to issue subpoenas and the proposed additions to § 156.935 to ensure that the discovery provisions set forth therein do not apply to appeals of proposed CMPs imposed under § 156.805 resulting from audits at § 156.480(c).
Comment:
Several commenters opposed the proposal that provides that the discovery provisions do not apply to appeals of proposed CMPs under § 156.805 resulting from audits under § 156.480(c). Commenters noted this proposal raises due process concerns, as the removal would limit issuers' due process protections. One commenter noted that discovery is essential to the determination of the reasonableness of a CMP and the removal of discovery violates statutory requirements for administrative decisions to be made on a full record. Other commenters noted the removal of discovery could result in issuers not being able to develop a full record and present a case. One commenter stated that eliminating discovery would limit access to necessary information, making it difficult for the issuer to understand the basis for the enforcement action and assemble a complete record which includes complex factual and technical evidence, and recommended that issuers have the ability to retain adequate tools and time to prepare effective responses, particularly where sanctions carry significant financial or operational consequences. Another commenter recommended that discovery should be retained as the proposal would require issuers to develop their defense from their audit record alone, which would preclude an issuer's ability to compel necessary information to develop a full defense.
Response:
We acknowledge these comments but are finalizing § 156.935 as proposed, as discovery for appeals of proposed CMPs under § 156.805 resulting from audits under § 156.480(c) is redundant and unnecessary. The audit procedures under § 156.480(c) and the CMP imposition process provide both issuers and HHS with necessary documentation and ample opportunities to disclose necessary and pertinent information. The audits conducted under § 156.480(c) are collaborative, where HHS works with issuers to ensure they have several opportunities to provide information and evidence to address any findings of noncompliance.
Audit procedures under § 156.480(c)(1) and (3) require that HHS conduct an audit entrance conference with each issuer selected for audit to discuss the scope of the audit and provide issuers with preliminary audit findings and an opportunity to refute the preliminary findings prior to receiving the final audit report. Issuers are also provided with an opportunity to discuss final audit findings during an exit conference. In addition to these opportunities, HHS provides issuers with documentation throughout the audit, including the audit sampling and extrapolation methodology, audit notification letters, entrance conference slides, instructions for completing the audit, a discrepancy process to provide additional documentation or justification of findings, the Notice of Noncompliance Preliminary Findings Audit Report (which includes the methodology for determining CMP amounts), and the Final Findings Audit Report (which includes written responses to refutations). For example, under § 156.806, prior to imposing CMPs, if there is a potential violation identified under § 156.800 which may result in a CMP, HHS provides the Noncompliance Preliminary Findings Audit Report. This report includes the methodology for determining CMP amounts; describes each violation, including the issuer's explanation of the circumstances surrounding the violation; provides the issuer with 30 days to refute the violation; and notifies the issuer that CMPs may be assessed if violations are not refuted. Therefore, throughout the audit, issuers receive the administrative record and have ample opportunities to both share information with HHS and request information from HHS to better understand why HHS has identified violations due to noncompliance and why a CMP may be assessed, allowing issuers to develop a full case to present in front of the DAB and ALJ if necessary. Thus, the removal of discovery will not prevent issuers from having a fair opportunity to
( printed page 29797)
present a full case. Additionally, regulations for other programs, such as the appeal and CMP regulations for Medicare Advantage at 42 CFR part 422, for example, do not have any provisions for discovery.
Comment:
Several commenters recommended that HHS clarify the scope and limits of the proposed subpoena authority and include sufficient procedural safeguards to protect fairness so that issuers have the fair opportunity to present a case. One commenter recommended that the ALJs' subpoena authority be narrowly tailored to prevent disruption of issuer operations and to ensure the authority to subpoena would address relevant issues.
Response:
We appreciate these comments and are finalizing this provision as proposed. The ALJ's subpoena authority will allow the ALJ to issue subpoenas either upon his or her own motion or upon the request of a party, and having the option to issue a subpoena will help the ALJ obtain necessary documentation, information, and potential testimony from witnesses to fully develop a case before issuing a decision. HHS intends that this provision will streamline hearing processes and improve the accuracy of DAB decisions, benefiting both parties. Under this process, the ALJ must follow certain regulatory procedures when issuing subpoenas, thereby ensuring the authority is not broad and is tailored to the case. Also, this authority under § 156.903 will provide the scope of what information subpoena requests are required to include and ensure that the requested subpoena seeks information that will address relevant issues in the case. Additionally, other regulations for other programs, such as the appeal and CMP regulations for Medicare Advantage at 42 CFR part 422, for example, provide the ALJ with the authority to issue subpoenas.
In the 2027 Payment Notice proposed rule (91 FR 6421), we proposed to require QHP issuers to submit quality improvement strategies (QISs) addressing any two of the five topic areas listed in section 1311(g)(1) of the Affordable Care Act, without mandating which specific topic areas a QHP issuer would be required to address to meet the QIS statutory certification requirement beginning with PY 2027.
In accordance with section 1311(c)(1)(E) of the Affordable Care Act, QISs described in section 1311(g)(1) of the Affordable Care Act must be implemented across Exchanges as a QHP certification requirement. Section 1311(g)(1) of the Affordable Care Act defines a QIS as a payment structure that provides increased reimbursement or other market-based incentives for implementing activities related to five health care topic areas identified in statute: improving health outcomes of plan enrollees, preventing hospital readmissions, improving patient safety and reducing medical errors, promoting wellness and health, and reducing health and health care disparities. Under § 156.1130(a), an issuer participating in an Exchange for two or more consecutive years must implement and report on a QIS, including a payment structure that provides increased reimbursement or other market-based incentives in accordance with the health care topic areas in section 1311(g)(1) of the Affordable Care Act, for each QHP offered in an Exchange, consistent with the guidelines developed by HHS under section 1311(g) of the Affordable Care Act. In the 2016 Payment Notice (80 FR 10844 through 10848), we established a phase-in approach for QIS implementation standards and reporting requirements to provide QHP issuers time to understand the populations enrolling in a QHP offered through the Exchange and to build quality performance data on their respective QHP enrollees. In the 2023 Payment Notice (87 FR 27341 through 27345), we finalized a guideline to require QHP issuers to address health and health care disparities as a specific topic area within their QIS, in addition to at least one other topic area described in section 1311(g)(1) of the Affordable Care Act, beginning in 2023.
We proposed to modify the approach finalized in the 2023 Payment Notice (87 FR 27208) to instead require QHP issuers to submit QISs addressing any two of the five topic areas listed in section 1311(g)(1) of the Affordable Care Act, without mandating which specific topic areas a QHP issuer would be required to address to meet the QIS statutory certification requirement. We did not propose any amendments to the regulatory text outlined in § 156.1130.
We stated in the proposed rule that we believe this proposal would align with current Administration priorities, provide increased flexibility and reduced burden for QHP issuers that are required to submit QISs, and would better allow these QHP issuers to define the health outcome needs of their enrollees, set goals for improvement, and provide increased reimbursement to their providers or other market-based incentives to reward achievement of those goals, as initially described in the 2015 Payment Notice (79 FR 13744) when establishing the QIS program. Specifically, we stated that by allowing QHP issuers to select the two topic areas most relevant to their population and operational context, the proposal would empower issuers to focus resources on areas with the greatest potential for meaningful improvement, rather than adhering to a one-size-fits-all approach. We stated that this targeted flexibility would support innovative strategies for improving patient outcomes, encourage adoption of best practices across diverse settings, and help ensure that incentives are aligned with measurable progress on priority health outcomes, consistent with the objectives articulated in the 2015 Payment Notice (79 FR 13744) when establishing the QIS program.
We stated that we continue to believe that improving health care quality and outcomes for all is important. We stated that QHP issuers have a critical role in promoting high quality health care by designing QISs that tie provider payments or other market-based incentives to measures of performance, such as when providers meet quality indicators or when enrollees make certain choices associated with improved health. We further stated that for each QIS topic area, issuers may select quality measures, such as those from the Marketplace Quality Rating System, or other performance targets based on their programmatic goals and the needs of their enrollee populations, to monitor QIS progress.
We stated that although QHP issuers would no longer be required to submit a QIS that addresses health and health care disparities as a specific topic area within their QIS under this proposal if finalized, they would be permitted to continue to choose this topic area as one of the two topic areas they address in their QIS. We further noted that health and health care disparities may relate to various factors such as geographic, economic, educational, disability status, and other factors that impact high quality health care for all.
We sought comment on this proposal.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy as proposed. We summarize and respond to public comments received on the proposed requirement that QHP issuers submit QISs addressing any two of the five topic areas described in section 1311(g)(1) of the Affordable Care Act, without mandating that issuers address health and health care disparities as a specific topic area below.
( printed page 29798)
Comment:
Some commenters supported the proposal to allow QHP issuers to select any two of the five statutory QIS topic areas described in section 1311(g)(1) of the Affordable Care Act to address in their QISs. These commenters stated that increased flexibility would allow QHP issuers to better tailor their QISs to enrollee needs and local market conditions, and to focus resources on areas with the greatest potential impact. Several commenters also noted that the proposal would reduce administrative burden by removing prescriptive requirements.
Many commenters opposed or stated concerns regarding the proposal to no longer require QHP issuers to address health and health care disparities as a specific topic area within their QISs. These commenters emphasized that maintaining a required focus on health and health care disparities is critical to advancing health equity across QHP issuers. Several commenters stated that making this topic area optional could reduce prioritization of health and health care disparity-related activities, lead to variability in QHP issuer implementation of QIS activities addressing health and health care disparities and weaken alignment with broader health equity goals. A few commenters recommended retaining the requirement to address health and health care disparities as a specific topic area within a QIS or establishing alternative mechanisms to ensure continued focus on health and health care disparities.
Response:
We appreciate commenters' support for this proposal and agree that the proposal would reduce administrative burden and increase flexibility, allowing QHP issuers to better tailor their QISs to enrollee needs and local market conditions and focus resources on areas with the greatest potential impact. We acknowledge commenters' concerns that making the health and health care disparities topic area optional could reduce prioritization of health and health care disparity-related activities. However, we continue to believe that allowing QHP issuers to select any two of the five statutory QIS topic areas under section 1311(g)(1) of the Affordable Care Act provides appropriate flexibility to address the most pressing needs of their enrollee populations and supports more targeted and effective quality improvement efforts. We also reiterate that QHP issuers may continue to select health and health care disparities as one of their QIS topic areas. We do not agree that this flexibility diminishes the importance of strategies to address health and health care disparities. Rather, it is intended to support more effective and context-specific implementation of quality improvement strategies, including those that directly address health and health care disparities. In addition, issuers retain the ability to select reducing health and health care disparities as one of their QIS topic areas, ensuring that flexibility is available for issuers to focus their quality improvement efforts on chosen areas of disparities.
For commenters' recommendations to retain the requirement to address health and health care disparities as a specific topic area within a QIS or establish alternative mechanisms to ensure continued focus on reducing health and health care disparities, we are not adopting those recommendations at this time. We believe that continued flexibility is maintained for issuers to choose to address health and health care disparities in quality improvement efforts. Through educational webinars and technical guidance, we will ensure continued focus on reducing health and health care disparities, along with other QIS topic areas.
Comment:
Several commenters opposed the proposal more broadly, expressing concern that removing prescriptive requirements could weaken the effectiveness of the QIS program, reduce consistency across QHP issuers, and diminish alignment with broader quality goals. A few commenters stated that the current requirement to address health and health care disparities as a specific topic area within a QIS provides important structure and accountability.
Several commenters requested additional clarity to support consistent implementation, while other commenters recommended that CMS monitor the effects of the policy change, including impacts on quality and health equity outcomes.
Response:
We acknowledge commenters' concerns. As discussed in the proposed rule (91 FR 6421), we believe that allowing QHP issuers to select the two statutory QIS topic areas most relevant to their populations and operational contexts supports more targeted and meaningful quality improvement efforts while reducing unnecessary burden. We proposed to remove the prescriptive topic area requirements to afford QHP issuers greater flexibility in designing QIS programs that are tailored to the specific needs of their enrolled populations while continuing to advance meaningful quality improvement objectives. This approach is consistent with the statutory framework under sections 1311(c)(1)(E) and 1311(g)(1) of the Affordable Care Act and the original intent of the QIS program as established in the 2015 Payment Notice (79 FR 13744).
For commenters' concerns that removing prescriptive requirements could reduce consistency across QHP issuers and weaken QIS program effectiveness, we note that QHP issuers remain subject to the QIS requirements under § 156.1130, which require issuers to implement and report on strategies that include a payment structure tied to performance and quality improvement incentives. As discussed in the proposed rule, we believe that the statutory framework under sections 1311(c)(1)(E) and 1311(g)(1) of the Affordable Care Act, as implemented at § 156.1130, continues to provide a foundation for accountability and quality improvement regardless of which topic areas an issuer selects.
Regarding commenters' concerns about the removal of health and health care disparities as a specifically enumerated topic area and potential implications for alignment with broader quality goals, we reiterate that QHP issuers may continue to select health and health care disparities as a topic area under the revised framework, and we further encourage issuers to tailor their QIS activities as appropriate to the needs of their enrolled populations, which may appropriately include a focus on health and health care disparities where relevant. We continue to believe that providing issuers flexibility to determine how best to address the needs of their enrollees is consistent with the intent of the QIS program as established in the 2015 Payment Notice (79 FR 13744) and as subsequently modified in the 2023 Payment Notice (87 FR 27341 through 27345). This flexibility supports more targeted and effective quality improvement by enabling issuers to align QIS activities with population-specific needs and local performance data.
The QIS statutory framework under sections 1311(c)(1)(E) and 1311(g)(1) of the Affordable Care Act, as implemented at § 156.1130, provides a foundation for this approach by requiring issuers to implement and report on QISs that include a payment structure tied to performance and quality improvement incentives. This reporting requirement creates a mechanism for accountability in that CMS and Exchange authorities are able to review QHP issuer submissions to assess whether QHP issuers are actively implementing strategies designed to improve the quality of care and health outcomes for their enrollees.
( printed page 29799)
Specifically, because QHP issuers must document and report on their QIS activities, including the topic areas they have selected and the performance-based payment structures they have established, there is a transparent record of QHP issuer efforts that is subject to oversight and review. Where we identify deficiencies in a QHP issuer's QIS submission, we may require the issuer to remediate those deficiencies, thereby providing an additional layer of accountability and oversight. The requirement to tie payment structures to performance further ensures that QHP issuers have a financial incentive to achieve meaningful quality improvement outcomes, rather than merely satisfying a procedural reporting obligation. Accordingly, while this policy affords QHP issuers greater flexibility with respect to the topic areas they select to address in their QISs, the underlying structural requirements of § 156.1130—including implementation, performance-based payment, reporting, and deficiency review—continue to serve as the mechanisms through which QHP issuer accountability is maintained under the revised framework.
For commenters' requests for additional clarity to support consistent implementation, we note that the comments did not identify with specificity the aspects of the revised framework for which additional clarity was sought. To the extent interested parties have questions regarding implementation of the revised QIS requirements under § 156.1130, we will consider addressing these implementation questions through sub-regulatory guidance, as appropriate, to promote consistency across QHP issuers. We encourage issuers and other interested parties to submit specific implementation questions through established CMS channels so that we may consider addressing them in future guidance as appropriate and necessary.
Finally, regarding commenters' recommendations that CMS monitor the effects of this policy change, we agree that ongoing oversight is appropriate and consistent with CMS' broader quality improvement objectives. We will continue to monitor QHP issuer selection of QIS topic areas, QIS activities, and associated outcomes, including those related to health and health care disparities, and may consider future policy changes or refinements, as needed. We agree that clear implementation and ongoing oversight are important and will continue to oversee QIS implementation through established reporting and review processes, and provide technical assistance, as needed, consistent with our authority under section 1311(g)(2) of the Affordable Care Act to develop guidelines for QIS implementation.
17. Netting and Establishment of Debt Regulations To Include CMPs (§ 156.1215)
In the 2027 Payment Notice proposed rule (91 FR 6422), we proposed to amend the payment and collections processes set forth at § 156.1215. In particular, we proposed to amend § 156.1215(b) to provide that any CMPs assessed [368]
against health insurance issuers for violations of any applicable Exchange standards and requirements or PHS Act requirements applicable to health insurance issuers would be subject to netting as part of HHS' integrated monthly payment and collections cycle. We proposed to apply the netting provisions of the payment and collections process to CMPs assessed against health insurance issuers to allow the payment and collections process to evolve with the needs of the programs administered by HHS, ensure stability and consistency in the monthly payment and collections process, and improve HHS' ability to recover Federal debts by withholding funds payable by HHS to, or held by HHS for, health insurance issuers to satisfy a debt to HHS for CMPs assessed against health insurance issuers.
In the proposed rule, we stated that since finalizing the netting rules at the beginning of the Affordable Care Act financial management programs (79 FR 13817, 81 FR 12317 through 12318), the programs under title XXVII of the PHS Act have evolved, and existing Exchange programs have matured and stabilized. We noted that we have undertaken efforts to adapt our payment and collections process to fit the current needs of the Exchange and other programs administered by HHS. We stated that as we work to enhance enforcement of these maturing programs, we believe that the payment and collections process should reflect this change by further evolving to provide that CMPs assessed against health insurance issuers, for violations of any applicable Exchange standards and requirements or PHS Act requirements, including the No Surprises Act, applicable to health insurance issuers, are also subject to netting as part of HHS' integrated monthly payment cycle.
Accordingly, we proposed to amend § 156.1215(c) to provide that any amount owed to the Federal Government by an issuer and its affiliates for these unpaid CMP amounts due to the Federal Government from these issuers and their affiliates, after HHS nets amounts owed by the Federal Government under these programs, would be the basis for calculating the determination of the debt.
We stated in the proposed rule that HHS' current integrated monthly payment and collections cycle is designed to streamline payment processing for both health insurance issuers and HHS, and includes statements to health insurance issuers that reflect how payments have been netted in the monthly payment and collections cycle. We stated that the proposed changes, to provide for netting of CMPs assessed against health insurance issuers and their affiliates, would ensure stability and consistency in the monthly payment and collections process and support HHS' continued ability to recover Federal debts by withholding funds payable to (or held by HHS for) issuers to satisfy an outstanding balance due to HHS for CMPs. We further stated that netting supports HHS' integrated monthly payment and collections cycle by limiting the number of charges flowing back and forth between HHS and issuers, mitigates the need for additional steps for Federal debt collection when internal netting may resolve the outstanding balance due to HHS from a determined debt, and may prevent inappropriately enriching an issuer if a payment is made from HHS when the issuer has an outstanding CMP.
In summary, we proposed to amend § 156.1215(b) to add language which applies the netting provisions of the payment and collections process to CMPs assessed for violations of any applicable Exchange standards and PHS Act requirements applicable to health insurance issuers. We also proposed to amend § 156.1215(c) to add language which provides that any amount owed to the Federal Government by an issuer and their affiliates for unpaid CMP amounts due to the Federal Government, after HHS nets amounts owed by the Federal Government under these programs, is a determination of debt.
We sought comment on these proposals.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these policies as proposed. We summarize and respond below to public comments received on the proposed amendments to the payment
( printed page 29800)
and collections processes set forth at § 156.1215(b) to provide that any CMPs assessed against health insurance issuers for violations of any applicable Exchange standards and requirements or PHS Act requirements applicable health insurance issuers will be subject to netting as part of HHS' integrated monthly payment and collections cycle, and on the proposed amendment to § 156.1215(c) to provide that any amount owed to the Federal Government by an issuer and its affiliates for unpaid CMP amounts will be the basis for calculating the determination of the debt.
Comment:
One commenter stated that the netting of CMPs would allow immediate collection, offset, or withholding from issuer revenue streams and noted that issuers may not have sufficient revenue to offset potential CMPs, which creates a risk of insolvency. The commenter suggested there should be exceptions to netting CMPs in situations where there is a risk of issuer insolvency. Another comment stated that this proposal, in tandem with the proposal to limit discovery during proceedings for appeals of CMPs set forth in § 156.935, would expose issuers to heightened financial exposure.
Response:
HHS continuously monitors issuers' financial solvency and liquidation status, but we do not believe that an exception should be made to netting CMPs in situations where there is a risk of issuer insolvency. We believe that it is more important to ensure the most efficient method for recovering debts owed to the Federal government—netting—is being used. Specifically, prioritizing issuer solvency over penalty collection undermines the integrity of the Exchange and creates a shift of the financial risk of non-compliance onto the Federal Government and taxpayers. Furthermore, many factors contribute to an issuer's insolvency issues, so netting for CMPs alone would not likely be the sole reason for an issuer becoming insolvent. A legally enforceable debt is recorded on the issuers' books and would be part of the financial health evaluation performed by State and Federal regulators. To comply with Federal debt collection requirements, netting of these charges is appropriate. Further, HHS maintains working relationships with State regulators to monitor issuer solvency and has procedures in place to address situations of financial instability such as State supervision, rehabilitation, and liquidation.
Additionally, we do not believe that limiting discovery in proceedings for appeals of CMPs as set forth in § 156.935, in combination with this netting of CMPs as finalized in this rule, would further impact issuer insolvency, as the issuer will continue have the full administrative record from the audit even without discovery. For these reasons, we are finalizing these policies as proposed.
18. Technical Correction to Cross Reference (§ 156.1220(b)(1))
In the 2027 Payment Notice proposed rule (91 FR 6422), we proposed a technical correction to § 156.1220(b)(1) to update a cross-reference in the regulation text from paragraph (a)(5) to (a)(6). We noted that the process for administrative appeals consists of requests for reconsideration, described in § 156.1220(a), followed by informal hearings, described in § 156.1220(b). We stated that § 156.1220(b)(1) serves to explain the manner and timing of the request for an informal hearing, in the event that a request for reconsideration is not accepted by HHS. Currently § 156.1220(b)(1) references § 156.1220(a)(5), which is the scope of review of the reconsideration decision, and we proposed to correct this reference to § 156.1220(a)(6) on the reconsideration decision.
We sought comments on this technical correction.
We only received one comment that acknowledged the proposed technical correction to § 156.1220(b)(1) but did not express any support or opposition. After consideration of this comment and for the reasons outlined in the proposed rule and this final rule, we are finalizing this correction as proposed.
F. Part 158—Issuer Use of Premium Revenue: Reporting and Rebate Requirements
1. Comment Solicitation on Potential Adjustment to the MLR Standard for a State's Individual Market (Subpart C)
In the PY 2027 Payment Notice proposed rule (91 FR 6422), we sought comment on the impact of the Federal MLR standard on individual market stability, including the impact of MLR on costs and premiums and how such impact, if any, may affect individual market stability. We thank commenters for their feedback and will take these comments into consideration as we continue to consider potential adjustments to the Federal MLR standard for particular States' individual health insurance markets.+
G. Applicability Dates
In the 2027 Payment Notice proposed rule, we proposed that some policies, if finalized, would become applicable for plan years beginning on or after January 1, 2027.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing the applicability dates with the following modifications as provided in Table 13. We note that this rule is effective 30 days after publication in the
Federal Register
, and we provide further specificity where applicability dates of certain provisions may vary.
( printed page 29801)
( printed page 29802)
( printed page 29803)
( printed page 29804)
H. Comments Regarding the Public Comment Period
The 2027 Payment Notice proposed rule displayed at the
Federal Register
on February 9, 2026, and published in the
Federal Register
on February 11, 2026. The comment period closed on March 13, 2026, 32 days after the rule displayed and 30 days after it published in the
Federal Register
. We summarize and respond to the public comments received regarding the length of the public comment period below.
Comment:
A few commenters stated that a 30-day comment period was insufficient given the proposed rule's length and complexity, stating that it did not allow adequate time for researchers, practitioners, and the public to thoroughly read, analyze, and provide meaningful feedback on complex proposals. One comment letter alleged HHS withheld data relevant to understanding the proposals and that withholding this information denied the public a reasonable opportunity to comment. Commenters suggested that HHS either extend the comment period or set aside consideration of less-developed proposals in favor of expediting publication of the final rule and its standards affecting coverage requirements for PY 2027 and PY 2028 and implementing the WFTC legislation.
Commenters also raised concerns that the late publication of the proposed rule creates serious downstream implementation challenges, leaving State agencies, issuers, and other interested parties without enough time to address final rule policies before critical filing deadlines. One commenter stated that because the comment period would end just 2 months before the mid-May 2026 deadline for Affordable Care Act plans to file rates in their States, there would be little time for State insurance regulators to publish guidance for issuers that reflect the provisions of the final rule.
Response:
We disagree that interested parties had insufficient time to meaningfully consider and comment on the proposed rule. Thirty days has become the standard length of this annual rulemaking's comment period, setting an expectation which prepares commenters, especially in the individual market health insurance industry, to provide meaningful comments within the allotted time. We received over 5,029 comments addressing every substantive proposal in the 2027 Payment Notice proposed rule, including comments from individuals, State governments or entities, national professional organizations, issuers and issuer groups, providers/provider groups/provider associations, general advocacy groups, agents/brokers, disease advocacy groups, pharmaceutical companies and groups, tribal organizations, dental organizations, labor groups, and other organizations, and approximately 2,169 form letters. These comments demonstrate that individuals and organizations alike were able to submit meaningful comments within the comment period and do not support an extension of the comment period or assertions that the public lacked a meaningful opportunity to comment.
( printed page 29805)
Further, we did not withhold information on which the proposals in the proposed rule relied. As commenters acknowledged, the proposed rule referenced data relevant to the proposed policies, including data we previously made available through public use files and other publications. To the extent any interested parties had questions about data cited in the proposed rule or required any further information, the proposed rule invited parties to contact HHS during the comment period. Notably, no commenter suggested they sought data from HHS during the comment period and was denied. For this reason, we do not agree that HHS withheld data impeding the public's ability to meaningfully comment on the proposed rule.
We acknowledge the importance of finalizing this rule as soon as possible and prior to critical deadlines for submission of health insurance rates to Federal and State regulators. Rate setting and plan finalization for PY 2027 depends on the finalization of the policies set forth in this final rule (such as permissible cost sharing parameters and the submission of rate filing justifications). Consistent with comments outlining concerns about impending critical rate filing deadlines, if we were to extend the comment period, the publication of the final rule would be further delayed. To provide individual and small group market issuers sufficient time to develop and price plan offerings for PY 2027 and because it is imperative that these rules be finalized as soon as possible, we set a 30-day comment period for the proposed rule.
I. Severability
We stated in the proposed rule that, as demonstrated by the number of distinct programs addressed in that rulemaking and the structure of the proposed rule in addressing them independently, we generally intended the rule's provisions, if finalized, to be severable from each other. For example, the proposed rule outlines proposed payment parameters and provisions for the HHS-operated risk adjustment program and HHS-RADV, the 2027 user fee rate for issuers in the risk adjustment program, the 2027 FFE and SBE-FP user fee rates, and provisions related to administration of CMPs. We also proposed, among other proposals, to disallow APTC for individuals who are ineligible for Medicaid due to their immigration status and have income below 100 percent of the FPL for taxable years beginning after December 31, 2025, limit APTC eligibility among aliens lawfully present who are not “eligible aliens” effective January 1, 2027, and extend the removal of the 150 percent FPL SEP beyond PY 2026 to align with the WFTC legislation. We stated that in the proposed rule that we believe the proposed provisions, if finalized, are generally capable of functioning sensibly on an independent basis. We stated that it is our intent that if any provision of the proposed rule, if finalized, is held to be invalid or unenforceable by its terms, or as applied to any person or circumstance, the other provisions in the proposed rule shall be construed so as to continue to give maximum effect as permitted by law, unless the holding shall be one of utter invalidity or unenforceability. We stated that in the event a provision if finalized is found to be utterly invalid or unenforceable, we intend for that provision to be severable.
We sought comment on the severability of these provisions in the proposed rule and did not receive any comments in response. For the reasons outlined in the proposed rule and in this final rule, we are finalizing this policy as proposed.
IV. Collection of Information Requirements
Under the Paperwork Reduction Act of 1995, we are required to provide notice in the
Federal Register
and solicit public comment before a collection of information requirement is submitted to the Office of Management and Budget (OMB) for review and approval. To fairly evaluate whether an information collection should be approved by OMB, section 3506(c)(2)(A) of the Paperwork Reduction Act of 1995 requires that we solicit comments on the following issues:
The need for the information collection and its usefulness in carrying out the proper functions of the agency.
The accuracy of our estimate of the information collection burden, including the validity of the methodology and assumptions used.
The quality, utility, and clarity of the information to be collected.
Recommendations to minimize the information collection burden on the affected public, including automated collection techniques.
We solicited public comment on each of these issues for the following sections of this document that contain information collection requirements (ICRs). The public comments and our responses appear in this section, and in the applicable ICR sections that follow.
A. Wage Estimates
To derive wage estimates, we generally use data from the Bureau of Labor Statistics to derive labor costs (including a 100 percent increase for the cost of fringe benefits and overhead) for estimating the burden associated with the ICRs.[369]
Table 14 presents the median hourly wage, the cost of fringe benefits and overhead, and the adjusted hourly wage.
As indicated, employee hourly wage estimates have been adjusted by a factor of 100 percent. This is necessarily a rough adjustment, both because fringe benefits and overhead costs vary significantly across employers, and because methods of estimating these costs vary widely across studies. Nonetheless, there is no practical alternative, and we believe that doubling the hourly wage to estimate total cost is a reasonably accurate estimation method.
( printed page 29806)
We proposed to adopt an hourly value of time based on after-tax wages to quantify the opportunity cost of changes in time use for unpaid activities (91 FR 6424). This approach matches the default assumptions for valuing changes in time use for individuals undertaking administrative and other tasks on their own time, which are outlined in an Assistant Secretary for Planning and Evaluation (ASPE) report on “Valuing Time in U.S. Department of Health and Human Services Regulatory Impact Analyses: Conceptual Framework and Best Practices.” [370]
We start with a measurement of the usual weekly earnings of wage and salary workers of $1,206.[371]
We divide this weekly rate by 40 hours to calculate an hourly pre-tax wage rate of approximately $30.15. We adjust this hourly rate downwards by an estimate of the effective tax rate for median income households of about 17 percent, resulting in a post-tax hourly wage rate of approximately $25.02. We adopt this as our estimate of the hourly value of time for changes in time use for unpaid activities.
We sought comment on these burden estimates and assumptions.
We did not receive any comments in response to these proposed burden estimates. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
B. ICRs Regarding Rate Filing Justification—OMB Control Number 0938-1141 (§ 154.215)
1. ICR Regarding Estimating CSR Load Factor Using the Standard Methodology
In the proposed rule, we stated that under § 154.215(b)(1) through (3) and CMS' Unified Rate Review Instructions,[372]
issuers are required to submit a rate filing justification that consists of three parts: (1) the URRT; (2) a written description justifying any premium rate increase when a plan within a product has a rate increase that is subject to review; and (3) an Actuarial Memorandum when a plan within a product has a rate increase, regardless of the size of the increase, when a product contains a QHP, or when a State requires it (91 FR 6425). Section 156.80(d)(2)(i) specifies that the actuarially justified plan-specific factors by which an issuer may vary premium rates for a particular plan from its market-wide index rate include the actuarial value and cost-sharing design of the plan, including, if permitted by the applicable State authority, accounting for CSR amounts provided to eligible enrollees under § 156.410, provided the issuer does not otherwise receive reimbursement for such amounts.
As discussed in the proposed rule, CSR loading is a permissible practice if permitted by the State and the amounts are actuarially justified plan-level adjustments which issuers must report when they submit a rate filing to the State or CMS for review, to ensure compliance with the Federal rating rules, including § 156.80. To provide regulators with information to help determine whether CSR loads are actuarially justified, this rule finalizes our proposal that the actual CSR amount paid on behalf of eligible enrollees and the additional revenue collected from the previously applied CSR load be reported on the URRT and calculated using the most recent annual data that
( printed page 29807)
is available prior to the applicable filing year, using the standard methodology set forth in § 156.430(c)(2).
Assuming a cross-functional team, we estimate that issuers will incur an initial one-time cost and burden in 2026 to develop and implement a claim-level re-adjudication process using the standard methodology set forth in § 156.430 to produce the required values. We estimate that for each issuer it will require 2,400 hours (at an hourly rate of $120.94) for Actuaries to define the plan mappings and business rules and set reasonableness thresholds, 3,000 hours (at an hourly rate of $108.26) for Data Scientists to design the approach and data flows, prototype the logic, and validate results, 3,000 hours (at an hourly rate of $94.88) for Computer Programmers to develop and maintain the production code and workflows, automate runs, and ensure reliability and performance, 2,000 hours (at an hourly rate of $73.84) for Claims Specialists to assemble and interpret claims, eligibility, and accumulator data, and 1,000 hours (at an hourly rate of $96.88) for a Project Manager to coordinate timelines, handoffs, and deliverables to produce the experience-period actual CSR amount paid on behalf of eligible enrollees (using the most recent annual data available, generally 2 years before the upcoming plan year, using the CMS standard methodology set forth in § 156.430(c)(2)), the additional revenue collected from the previously applied CSR load from the most recent annual data available, the projection-period expected CSR amount to be paid on behalf of enrollees for the upcoming plan year, and the plan-level CSR load factor for the upcoming plan year, and additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year for URRT reporting, resulting in a total one-time burden of 11,400 hours, with an associated cost of approximately $1,144,236. For all 366 issuers, we estimate a total burden of 4,172,400 hours, with an associated cost of approximately $418,790,376.
In subsequent years, we assume that issuers will require targeted updates to ensure their systems are accurately calculating the required values using the most recent data. We estimate that for each issuer it will require 1,200 hours (at an hourly rate of $120.94) for Actuaries to update plan parameters and CSR-to-standard-plan mappings using the most recent annual data that is available prior to the applicable filing year, 1,500 hours (at an hourly rate of $108.26) for Data Scientists to update specifications, oversee execution, and review outputs, 1,500 hours (at an hourly rate of $94.88) for Computer Programmers to reload data, apply configuration and code updates, and run and monitor the processing, 1,000 hours (at an hourly rate of $73.84) for Claims Specialists to reconcile corrected claims, and 500 hours (at an hourly rate of $96.88) for a Project Manager to manage review and sign-off for the cycle, resulting in an annual ongoing burden of 5,700 hours, with an associated cost of approximately $572,118. For all 366 issuers, we estimate a total burden of 2,086,200 hours, with an associated cost of approximately $209,395,188.
Some issuers may incur a lower one-time cost if they currently have a system in place that is able to calculate the load factor and other required values using the standard methodology, or if their systems only require updates and minor changes to function properly. We also acknowledge that some issuers may incur higher costs if they are required to develop and build a new system to meet the proposed requirements and calculate the appropriate values. We further acknowledge that some issuers may incur higher or lower annual costs depending on their volume of CSR-eligible claims.
2. ICR Related to the Submission of Unified Rate Review Templates (URRTs)
As discussed in section III.C. of this final rule, this rule finalizes our proposal to change the instructions for the URRT so that issuers will enter the actual amount of CSRs they paid on behalf of eligible enrollees (using the most recent annual data that is available prior to the applicable filing year, generally two years prior to the upcoming plan year), the additional revenue collected from the previously applied CSR load, the amount of CSRs they expect to be paid on behalf of enrollees in the upcoming plan year, the CSR load factor for the upcoming plan year, and the additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year.
Issuers will incur ongoing burden to gather all the required CSR-related data
( printed page 29808)
elements and enter them into the URRT in their appropriate places. We estimate that for each plan an issuer will require 0.5 hours (at an hourly rate of $120.94) for Actuaries to collect all required CSR-related data elements (actual CSR amounts paid on behalf of eligible enrollees, additional revenue collected from the previously applied CSR load, expected CSR amounts to be paid on behalf of enrollees in the upcoming plan year, CSR load factor for the upcoming plan year, and additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year) and ensure the data is accurately entered into the URRT, resulting in an ongoing burden of 0.5 hours, with an associated cost of approximately $60 per plan. We estimate that each issuer will need to submit data for an approximate average of 7 plans [373]
that include CSR load factors and thus will incur an estimated burden of 3.6 hours, with an associated cost of approximately $430.[374]
For all 366 issuers, we estimate a total burden of 1,300 hours, with an associated cost of approximately $157,222.
3. ICR Related to the Submission of Actuarial Memorandum
As discussed in section III.C. of this final rule, this rule finalizes our proposal that information regarding CSR-related plan-level adjustments to the index rate should be provided in the URRT and also provided in the Actuarial Memorandum so that issuers provide numerical values in the URRT and explain how they reached those values in the Actuarial Memorandum.
Issuers will incur additional ongoing burden to develop, draft, and add the explanation of the methodology used to determine the load factor and an explanation of how the additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year compares to the amount of CSRs expected to be paid on behalf of enrollees for the same period. We estimate that for each plan an issuer will require 2 hours (at an hourly rate of $120.94) for Actuaries to develop, draft the required explanations (the methodology used to determine the CSR load factor for the upcoming plan year and an explanation of how the additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year compares to the amount of CSRs expected to be paid on behalf of enrollees for the same period), and add them to the Actuarial Memorandum for submission via SERFF and/or MPMS, resulting in an ongoing burden of 2 hours, with an associated cost of approximately $242 per plan. We estimate that each issuer will need to submit explanations for an average of 7 plans and thus would incur an estimated burden of approximately 14 hours, with an associated cost of approximately $1,718. For all 366 issuers, we estimate a total burden of 5,200 hours, with an associated cost of approximately $628,888.[375]
The information collection described in this section will be submitted as a revision to the currently approved PRA package CMS-10379 (OMB Control Number 0938-1141) for OMB review under the Paperwork Reduction Act.
Table 19 aggregates the burden and costs from Tables 15 through 18. The 2026 burden (11,418 hours per respondent) includes the one-time implementation (11,400 hours) plus ongoing URRT and Actuarial Memorandum submissions (18 hours total). The 2027-2028 burden (5,718 hours per respondent) includes annual system updates (5,700 hours) plus ongoing URRT and Actuarial Memorandum submissions (18 hours total). The three-year averages are calculated by summing the annual figures and dividing by three.[376]
( printed page 29809)
4. Cost to Federal Government Related to Review of URRT Reporting Requirements Related to CSR Estimates
In 2026 (for PY 2027 rate filings), the Federal Government will incur costs to review and evaluate the data and actuarial memoranda submitted by issuers into MPMS or SERFF. To conduct the review of all required CSR-related data elements and explanations submitted, the Federal Government, at a minimum, will require staff at GS-14 level (at an hourly rate of $154.76 for GS-14 step 5) 6 hours per plan to review the materials submitted by issuers. The Federal Government will incur a burden of 15,600 hours, with an associated estimated cost of $2,414,256 to review all URRT and actuarial memoranda related material related to CSR data and explanations.
We sought comment on these assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
C. ICRs Regarding Mandating HHS-Approved and -Created Consumer Consent Form (§ 155.220)
As discussed in the preamble of this final rule, we are finalizing amendments to § 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and consent documentation requirements. We are finalizing this policy with a modification that it will be effective beginning with PY 2028 instead of PY 2027. Accordingly, we are also finalizing the redesignation of current § 155.220(j)(2)(ii)(A)(2) as § 155.220(j)(2)(ii)(A)(3) and current § 155.220(j)(2)(iii)(C) as § 155.220(j)(2)(iii)(D). We are also finalizing corresponding changes to §§ 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to state that current documentation policies for eligibility application and review and consent are effective until PY 2028. Our finalized policy will eliminate the current broad allowances for meeting these requirements. The language in the regulation will also be changed to clarify what types of actions constitute “taking an action” to meet the regulatory requirements. As discussed in the proposed rule, the goal of this policy is to reduce confusion among agents, brokers, and web-brokers on what constitutes compliant eligibility application review documentation and what constitutes compliant consumer consent by ensuring objective standards, which ultimately protects consumers (91 FR 6427). These finalized policies will also greatly improve HHS' investigative abilities into agent, broker, and web-broker eligibility application review documentation and consumer consent documentation review by creating a clear and objective standard for all applications clearly outlining what HHS deems complaint.
We estimate there will be very minimal costs in time associated with this policy as agents, brokers, and web-brokers are already required to document and maintain eligibility application review documentation information and consumer consent documentation information. As a result, this policy will not add to those requirements, rather, it will only require that a specific form be used.
In the proposed rule, we stated that according to our records, as of September 18, 2025, there are a total of 105,988 agents, brokers, and web-brokers who have presently completed the FFE training who are registered to assist consumers on the Exchanges. Under our records, the percentage of agents, brokers, and web-brokers that currently submit only audio files for eligibility application review documentation and consumer consent documentation is approximately 24 percent, which equals 25,437 agents, brokers, and web-brokers who are utilizing this method. Additionally, per our records, the percentage of agents, brokers, and web-brokers that currently submit partial audio files in connection with eligibility application review documentation and consumer consent documentation is approximately 42 percent, which equals 44,514 agents, brokers, and web-brokers who are utilizing this method.
Regarding the costs related to requiring agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review
( printed page 29810)
documentation requirements and the consumer consent documentation requirements, we estimate it would take approximately 10 minutes of time for an enrolling agent, broker or web-broker to meet eligibility application review documentation requirements and to obtain consumer, or their authorized representative, affirmation of their consent. Using the current adjusted hourly wage rate of $58.04 [377]
for an insurance sales agent, each enrollment using the HHS-approved and -created consumer consent form would have approximately $9.87 (10 minutes, or 0.17 hours, at an hourly wage rate of $58.04) in additional cost associated with it based on the extra time commitment from these proposed policy changes. In PY 2024, agents submitted 9,800,000 policies. Based on this number of enrollments, the total annual burden is 1,666,000 hours (9,800,000 submitted policies × approximately 0.17 hours) with a total annual cost of $96,694,640 (1,666,000 hours × $58.04 per hour).
Under the finalized policy, HHS will require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and the consumer consent documentation requirements. The HHS-approved and -created consumer consent form can be submitted electronically, so there will be no costs associated with printing or mailing the HHS-approved and -created consumer consent form.
The estimated cost of requiring agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and the consumer consent documentation requirements is $96,694,640.
Because we are finalizing this proposal, the new information collection requirements discussed in this section will be submitted for OMB review and approval in a new PRA package.
We sought comment on these burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed and this final rule, we are finalizing these estimates with the modification to implement the policy effective PY 2028.
D. ICRs Regarding Misleading Marketing (§ 155.220)
As discussed in the preamble of this final rule, we are finalizing amendments to § 155.220(j), creating new standards of conduct section on marketing requirements, which would be housed in § 155.220(j)(3). These new regulations will prohibit agents, brokers, and web-brokers from engaging in misleading marketing, while adhering to the requirements in newly proposed § 155.220(j)(3)(iii), and require agents, brokers, and web-brokers to provide marketing materials to HHS upon request. We estimate costs that would be associated with this finalized policy are mainly those involved in responding to HHS' requests for documentation. Producing such documentation will require the submission of electronic documents to HHS upon request.
As discussed in the proposed rule, we do not anticipate many costs for the agents, brokers, or web-brokers we investigate for misleading marketing (91 FR 6428). Based on our current investigative methods and volume of misleading advertisements we have uncovered thus far, we currently only plan to send 70 notifications annually to agents, brokers, and web-brokers for misleading marketing. Based on analysis of existing enforcement outreach conducted on misleading marketing, about
2/3
of the notices we send would be part of our Technical Assistance (TA) enforcement workstream, only requires the agent, broker, or web-broker to indicate the ad(s) has been removed. The other
1/3
of the notices we send would be Notices of Intent to Terminate (NoITs). NoITs require the agent, broker, or web-broker to respond indicating (1) they removed the ad(s) in question and (2) they reviewed the marketing guidelines CMS sent them. Therefore, there would only be approximately 24 notifications sent annually that require agents, brokers, or web-brokers to submit documentation in response to HHS. We are finalizing our proposal to allow HHS to request and review advertisements in new § 155.220(j)(3)(iv). If HHS were to utilize this regulatory authority and request advertisements from an agent, broker, or web-broker, it would be part of our NoIT requirements and the same 24 agents, brokers, or web-brokers would be impacted.
We believe responding to HHS requests to provide confirmation they removed the ads and/or reviewed the marketing guidelines would not be overly time-consuming or burdensome. Our notifications to the agents, brokers, or web-brokers detail what response is required and provide hyperlinks to the noncompliant ad(s). We estimate it would take each agent, broker, or web-broker one hour to remove any noncompliant ad(s), and/or review the marketing guidelines, and respond to HHS via email. This estimate incorporates the potential of HHS asking these 24 agents, brokers, and web-brokers to provide advertisements for HHS' review. Using the hourly wage rate for an insurance sales agent from Table 14, this means the total burden of responding to HHS regarding misleading marketing would be 24 hours at a cost of $1,392.96 ($58.04 per hour × 1 hour × 24 responses), beginning in 2027.
We sought comment on these burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
E. ICRs Regarding State Exchange Enhanced Direct Enrollment (SBE-EDE) Option (§ 155.221)
We are not finalizing our proposal to add § 155.221(k) to establish a new State Exchange enhanced direct enrollment (SBE-EDE) option by which State Exchanges can leverage direct enrollment technology to transition primarily to private sector-focused enrollment pathways operated by QHP issuers, web-brokers, and agents and brokers, instead of or in addition to a centralized eligibility and enrollment website operated by an Exchange. In the proposed rule, we stated that current State Exchanges that elect to implement the SBE-EDE option will need to revise their Exchange Blueprint to notify HHS that the State proposes to implement the SBE-EDE option in compliance with related requirements (91 FR 6428). We sought comment on the burden associated with this activity but did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in section III.D.4. of this final rule, we are not finalizing these estimates as HHS is not finalizing this policy.
F. ICRs Regarding Limiting APTC Eligibility to “Eligible Noncitizens” (§§ 155.20, 155.305(f)(1), and 155.320)
1. Basic Health Program
The following changes will be submitted for review under OMB Control Number 0938-1218 for BHP. We explained in the proposed rule that because section 71301 of the WFTC legislation amended section 36B of the Code to provide that PTC is not allowed
( printed page 29811)
for the coverage of noncitizens who are lawfully present but not “eligible aliens,” this population is no longer allowed PTC for their coverage beginning January 1, 2027, and as such, States will no longer receive Federal payments associated with members of this population who are BHP enrollees effective January 1, 2027 (91 FR 6429). States that operate a BHP will need to modify enrollment data sent to CMS in accordance with this provision to enable CMS to accurately calculate the State's BHP funding.
We estimate that implementing this policy would require ongoing costs for States to submit additional enrollment data to CMS. We estimate that it would take a Business Operations Specialist 2.5 hours at $78.14 per hour and a General Manager 0.5 hours at $99 per hour to compile and submit additional quarterly estimated enrollment data. We estimate that it would take a Business Operations Specialist 25 hours at $78.14 per hour and a General Manager 2.5 hours at $99 per hour to compile and submit additional quarterly final enrollment data. For the three States and DC currently approved to operate a BHP in 2027 we estimate the total annual ongoing cost to be $39,133.60.
We sought comment on these burden estimates and assumptions.
We did not receive any comments in response to these proposed burden estimates. For the reasons outlined previously and in the proposed rule, we are finalizing these estimates as proposed.
2. Exchanges
The following changes will be submitted for review under OMB Control Number 0938-NEW for Exchanges and OMB Control Number 0938-1218 for BHP.
As discussed in section III.D.8. of this final rule, we are finalizing our proposal to align Exchange eligibility and verification rules with section 71301 of the WFTC legislation, which disallows PTC for the coverage of noncitizens other than “eligible aliens.” We are adding a new definition of “eligible noncitizen” at § 155.20 and updating our regulations at § 155.305(f)(1)(ii) to align with 26 CFR 1.36B-1(d) and § 155.305(f)(1)(ii)(C) to clarify that an Exchange must grant eligibility for APTC to individuals defined as “U.S. citizens, U.S. nationals, and eligible noncitizens,” provided the other APTC eligibility requirements are met. For BHP, we are finalizing our proposal to add a new definition of “eligible noncitizen” at 42 CFR 600.5 that cross-references to § 155.20. These changes are effective beginning in PY 2027 and will apply to the 22 State Exchanges expected to be operating in PY 2027, Exchanges on the Federal platform, and to the three States that are currently approved to operate a BHP (Minnesota, Oregon, and New York), as well as the District of Columbia.[378]
To implement these changes, in the proposed rule we stated that the Federal Data Services Hub would need to make updates to its Verify Lawful Presence (VLP) service, to enable Exchanges to accurately verify whether an individual is an eligible noncitizen (91 FR 6429). In addition, we also stated that Exchanges on the Federal platform and the 22 State Exchanges would need to update their eligibility and enrollment systems to collect applicant attestations regarding eligible noncitizen status, to correctly determine APTC and income-based CSR eligibility on the basis of such attestations, to determine whether such attestations can be considered verified, to set and process new inconsistencies in cases where such attestations cannot be verified. Exchanges would also need to ensure that current enrollees who would no longer be eligible for APTC or income-based CSRs as a result of this finalized policy have their APTC and CSR eligibility ended accordingly.
3. Implementation Costs
We estimate that implementing this policy will require one-time costs for the Federal Government to make technical updates to its system. Based on preliminary analysis, we estimate that it would take the Federal Data Services Hub (the “Hub”) 2,000 hours in 2026 to make these technical updates. Of the 2,000 hours for Hub updates, we estimate it would take a database and network administrator and architect 500 hours at $103.34 per hour and a computer programmer 1,500 hours at $94.88 per hour. Given this, to make Hub updates, we estimate that the Federal Government would incur a one-time burden in 2026 of $193,990 [(500 hours × $103.34 + (1,500 hours × $94.88)] to make these system updates.
We also estimate that it will take Exchanges on the Federal platform 7,000 hours to make the updates required to implement this provision. Of the 7,000 hours required to make updates for Exchanges on the Federal platform, we estimate that it would take a database and network administrator and architect 1,750 hours at $103.34 per hour and a computer programmer 5,250 hours at $94.88 per hour. Given this, Exchanges on the Federal platform would incur a one-time burden of $678,965 [(1,750 hours × $103.34) + (5,250 hours × $94.88)].
Similar to the one-time costs incurred by Exchanges on the Federal platform, we estimate that implementing this policy will require one-time costs for each State Exchange of 7,000 hours. Of these 7,000 hours, we estimate it would take a database and network administrator and architect 1,750 hours at $103.34 per hour and a computer programmer 5,250 hours at $94.88 per hour to make the changes. State Exchanges would therefore incur a one-time burden of $14,937,230 [(1,750 hours × $103.34) + (5,250 hours × $94.88)] × 22 State Exchanges) to implement these technical changes.[379]
4. Ongoing Burden Related to New DMI Type for “Eligible Noncitizens”
We anticipate that this finalized policy will not result in ongoing burden changes for Exchanges and individuals related to the creation of a new DMI type for “eligible noncitizens” because these individuals would already be required to submit documentation to verify their eligibility to enroll in a QHP.
The total estimated annual burden for these information collection requirements is $15,810,185, representing 163,000 hours of burden.
We sought comment on these assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined previously and in the proposed rule, we are finalizing these estimates as proposed.
G. ICRs Regarding the Prohibition of APTC for Individuals Who Are Ineligible for Medicaid Due to Their Immigration Status and Have Income Below 100 Percent of the FPL (§ 155.305(f)(2))
1. Exchanges
We estimate that implementing this finalized policy will require one-time costs for Exchanges to make technical updates to their eligibility systems related to both APTC and the BHP. We estimate that it would have taken the Exchanges on the Federal platform 2,500 hours and each State Exchange 2,000 hours in 2025 to make these technical updates. Of those 2,500 hours for Exchanges on the Federal platform, we estimate it would take a database and network administrator and architect
( printed page 29812)
625 hours at $103.34 per hour and a computer programmer 1,875 hours at $94.88 per hour. Of those 2,000 hours for State Exchanges, we estimate it would take a database and network administrator and architect 500 hours at $103.34 per hour and a computer programmer 1,500 hours at $94.88 per hour. Given this, we estimate that Exchanges on the Federal platform would have incurred a one-time burden in 2025 of $242,488 [(625 hours × $103.34) + (1,875 hours × $94.88)] to make these system updates. State Exchanges would have incurred a one-time burden of $4,073,790 [(500 × $103.34) + (1,500 × $94.88)] × 21 State Exchanges to implement these technical changes.[380]
2. Ongoing Burden Reduction—Medicaid Lawful Presence (MLP) and Annual Income (AI) Data Matching Issue (DMI) Processing
We anticipate that this finalized policy will result in ongoing burden reduction for Exchanges on the Federal platform related to no longer generating Medicaid Lawful Presence (MLP) Data Matching Issues (DMIs) and for all Exchanges related to no longer generating annual income (AI) DMIs for those who attest to income under 100 percent of the FPL. We noted in the proposed rule that these DMIs are generated when an individual attests that they are a lawfully present noncitizen and have an attested household income under 100 percent of the FPL, but the Exchange is not able to verify promptly whether their immigration status disqualifies them from full Medicaid coverage or verify their attested annual household income with trusted data sources (91 FR 6430). We also stated that currently, Exchanges must require individuals to submit documentation to verify their attested application information when trusted data sources cannot verify.
3. Medicaid Lawful Presence (MLP) Data Matching Issue (DMI) Reduction
These inconsistencies are not generated by State Exchanges, so we do not estimate any change in burden to State Exchanges. Based on historical data from the FFE, we estimate a reduction of approximately 275,000 inconsistencies [381]
at the consumer level for the Exchanges on the Federal platform. The change would result in a decrease in burden on the Exchanges on the Federal platform. Once households have submitted the required verification documents, we estimate that it takes approximately 1 hour and 12 minutes (or 1.2 hours) for an eligibility support staff person (BLS occupation code 43-4061), at an hourly cost of $49.52,[382]
to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes. The revisions to § 155.305 would result in a decrease in annual burden for the Federal government of 330,000 hours (275,000 inconsistencies at the consumer level × 1.2 hours) with savings of $16,341,600 (330,000 hours × $49.52 hourly wage rate).
4. Annual Income (AI) Data Matching Issue (DMI) Reduction
Based on historical data from the FFE, we estimate that approximately 77,000 inconsistencies [383]
would not be generated at the household level for the Exchanges on the Federal platform. On the State Exchanges, we estimate this figure to be 54,000 inconsistencies.[384]
The change would result in a decrease in burden on Federal and State Exchanges. Once households have submitted the required verification documents, we estimate that it would take approximately 1 hour and 12 minutes (or 1.2 hours) for an eligibility support staff person (BLS occupation code 43-4061), at an hourly cost of $49.52,[385]
to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes. Therefore, removing these inconsistencies would result in a decrease in burden on the Federal Government of 92,400 hours (77,000 verifications × 1.2 hours per verification) with savings of $4,575,648 (92,400 hours × $49.52 per hour), and a decrease in burden on the State Exchanges of 64,800 hours (54,000 verifications × 1.2 hours per verification) with savings of $3,208,896 (64,800 hours × $49.52 per hour), and the cost decrease across all Exchanges would be approximately $7,784,544 (157,200 hours × $49.52 hourly cost of eligibility support staff person).
The total estimated annual reduction in burden for these information collection requirements, beginning in 2026, is $24,126,144 ($16,341,600 + $7,784,544), representing 487,200 (330,000 + 157,200) hours of burden across all affected entities.
We sought comment on these proposed burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined previously and in the proposed rule, we are finalizing these estimates as proposed.
H. ICRs Regarding Failure To File and Reconcile (§ 155.305)
We are finalizing our proposal to amend paragraph § 155.305(f)(4) so that in PY 2028 and beyond, all Exchanges may not determine a tax filer or their enrollee eligible for APTC if: (1) HHS notifies the Exchange that APTC were paid on behalf of the tax filer, or their spouse if the tax filer is a married couple, for one year for which tax data would be utilized for verification of household and family size, and (2) the tax filer did not comply with the requirement to file a Federal income tax return and reconcile APTC for that year (referred to as the “1-tax year FTR” process). We also are finalizing that at the option of the Exchange, an Exchange may choose to implement this policy earlier in PY 2027 if it has the resources and capability to adopt the 1-year FTR process or continue to follow the 2-year FTR process until PY 2028. Exchanges on the Federal platform intend to adopt the 1-year FTR process in PY 2027, as HHS has the resources possible to do so. As we noted in the proposed rule, section 71303(a)(6) of the WFTC legislation amended section 36B(c) of the Code such that term “coverage month” does not include, for any individual enrolled in a QHP through an Exchange, any month for which the Exchange does not meet the requirements of § 155.305(f)(4)(iii) as published in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074) for PY 2028 and beyond, where effectively Exchanges are required to find enrollees ineligible for APTC after they or their tax filer has failed to file and reconcile their APTC for 1-tax year (91 FR 6430). However, minimal changes to the language of the Exchange application questions for States served by
HealthCare.gov
will be necessary to obtain relevant information; as such, we anticipate that the amendment finalized in this rule will not impact the information collection burden for consumers. We anticipate that for some Exchanges, there will no longer be a 2-year FTR population for PY 2027, and thus the notices sent to the 1-year FTR population will be similar to the current 2-tax year FTR notices in inciting an urgency to act. Other Exchanges may
( printed page 29813)
choose to delay the change until PY 2028, but that all consumers with an FTR status will be in a 1-tax year FTR status for PY 2028. Due to this, we do not anticipate PRA impacts related to noticing requirements (OMB Control Number: 0938-1207).
We sought comment on these proposed burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
I. ICRs Regarding Income Verification When Data Sources Indicate Income Less Than 100 Percent of the FPL (§ 155.320(c)(3)(iii))
We are finalizing our proposal to update § 155.320(c)(3)(iii)(A) to extend the requirement for applicants to submit documentation when their attested household income is within the APTC range, but data sources indicate income less than 100 percent of the FPL. As finalized in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), Exchanges are required to generate income DMIs when a tax filer's attested annual household income would qualify the taxpayer as an applicable taxpayer according to 26 CFR 1.36B-2(b) and trusted data sources indicate that income is under 100 percent of the FPL only through PY 2026. In the proposed rule, we stated that we proposed to implement this policy as a new and permanent verification process within the Exchange, as detailed later (91 FR 6431).
We anticipate that extending this income verification requirement would result in approximately 1 hour of time spent by consumers to complete associated questions in the application or to submit supporting documentation for each year of operation. Based on historical data from the FFE, we estimate that approximately 340,000 inconsistencies would be generated at the household level for the Exchanges on the Federal platform annually starting in 2027. On the State Exchanges, we estimate this figure to be 208,000 inconsistencies annually starting in 2027. Therefore, adding these inconsistencies would increase burden on consumers by approximately 548,000 hours across all Exchanges. Using the estimate of the hourly value of time for changes in time use for unpaid activities calculated at $25.02 per hour in section IV.A. of this final rule, we estimate that the increase in cost for each consumer in 2027 would be approximately $25.02, and the cost increase for all consumers who would generate this income inconsistency in 2027 and onwards would be approximately $13,710,960 (548,000 hours × $25.02 cost of unpaid activities) per year.
Additionally, we estimate that adding this income verification requirement would result in an increase in burden on the Exchanges on the Federal platform. Once households have submitted the required verification documents, we estimate that it would take approximately 1 hour and 12 minutes (1.2 hours) for an eligibility support staff person (BLS occupation code 43-4061), at an hourly cost of $49.52,[386]
to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes. Therefore, adding these inconsistencies would result in an increase in annual burden on Exchanges on the Federal platform of 408,000 hours (340,000 verifications × 1.2 hours per verification) at a cost of $20,204,160 (408,000 hours × $49.52 per hour) starting in 2027, and an increase in annual burden on the State Exchanges of 249,600 hours (208,000 verifications × 1.2 hours per verification) at a cost of $12,360,192 (249,600 hours × $49.52 per hour) starting in 2027.
In addition to these administrative costs, we anticipate system expenses occurring in 2026 to establish this policy ahead of the effective date in 2027. These costs are to support updating technical systems, including the eligibility system. In the 2025 Marketplace Integrity and Affordability final rule (90 FR 27185), we estimated that it would take the Exchanges on the Federal platform and each State Exchange 8,000 hours in 2026 to make these updates and sunset the policy. Of those 8,000 hours, we estimated that it would take a database and network administrator and architect 2,000 hours at $103.34 per hour and a computer programmer 6,000 hours at $94.88 per hour. Given this, we estimate that Exchanges on the Federal platform would incur a one-time burden in 2026 of $775,960 (2,000 × $103.34 + 6,000 × $94.88) to make these eligibility system updates. State Exchanges would incur a one-time burden of $16,295,160 ((2,000 × $103.34 + 6,000 × $94.88) × 21). Because we are now finalizing this as a new and permanent verification process within the Exchange, we anticipate that many State Exchanges and the Federal Platform would incur the totality of these expenses to implement this policy as finalized.
We sought comment on these proposed burden estimates and assumptions.
We summarize and respond to public comments received on the burden estimates proposed policy in section V.C.14. of this final rule. For reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
J. ICRs Regarding Removal of the Requirement To Accept Attestations of Household Income When Tax Data Is Unavailable (§ 155.320(c)(5))
We are finalizing our proposal to remove § 155.320(c)(5), which will allow Exchanges to continue the income verification process when IRS is successfully contacted but IRS returns no data rather than accepting an applicant's annual household income attestation. We are implementing this policy as a new permanent verification procedure, and we are presenting these estimates as costs inherent to implementing the policy as finalized in this final rule.
In the proposed rule, we stated that based on internal historical DMI data, we estimate that approximately 1,722,000 inconsistencies will be generated annually at the household level for Exchanges on the Federal platform, and 1,056,000 will be generated at the household level for State Exchanges due to this final policy (91 FR 6431). Once households have submitted the required verification documents, we estimate that it will take approximately 1 hour and 12 minutes (1.2 hours) for an eligibility support staff person (BLS occupation code 43-4061), at an hourly cost of $49.52,[387]
to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes. Therefore, the removal of § 155.320(c)(5) will result in an increase in annual burden for Exchanges on the Federal platform of 2,066,400 hours (1,722,000 verifications × 1.2 hours per verification) at a cost of $102,328,128 (2,066,400 hours × $49.52 per hour) starting in 2027 and an increase in annual burden on State Exchanges of 1,267,200 hours (1,056,000 verifications × 1.2 hours per verification) at a cost of $62,751,744 (1,267,200 hours × $49.52 per hour) starting in 2027.
In addition to the increased administrative burden on Exchanges, this change will increase the number of consumers who are required to submit documentation to verify their income. We estimate that consumers will each
( printed page 29814)
spend 1 hour to answer the associated question, or to submit documentation. Based on historical data from the FFE, we estimate that approximately 2,777,000 inconsistencies will be generated at the household level across all Exchanges yearly. Using the estimate of the hourly value of time for changes in time use for unpaid activities calculated at $25.02 per hour in section IV.A. of this final rule, we estimate that the increase in annual cost for each consumer starting in 2027 will be approximately $25.02 and that the finalized change will increase burden on consumers by 2,777,000 hours per year at an associated cost of $69,480,540 (2,777,000 hours × $25.02 per hour).
In addition to these administrative costs, we anticipate system expenses occurring in 2026 to establish this policy ahead of the effective date in 2027. We estimated that it will take Exchanges on the Federal platform and each State Exchange 9,000 hours in 2026 to implement this policy. Of those 9,000 hours, we estimated it will take a database and network administrator and architect 2,250 hours at $103.34 per hour and a computer programmer 6,750 hours at $94.88 per hour. Therefore, we estimated that Exchanges on the Federal platform will incur a one-time burden in 2026 of $872,955 (2,250 × $103.34 + 6,750 × $94.88) to make these eligibility system updates, and State Exchanges will incur a one-time burden total in 2026 of $18,332,055 ($872,955 × 21) associated with a total of 189,000 (9,000 × 21) burden hours. Because this finalized policy will be implemented as a new permanent verification procedure, we anticipate that the full costs described in this provision will be applied to the State Exchanges and Exchanges on the Federal platform prospectively.
We sought comment on these proposed burden estimates and assumptions.
We summarize and respond to public comments received on the burden estimates proposed policy in section V.C.15. of this final rule. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
K. ICRs Regarding Pre-Enrollment SEP Verification (§ 155.420(g))
In this final rule, we are finalizing the provision allowing the Federal Exchange to conduct pre-enrollment verification for SEPs other than Loss of Minimum Essential Coverage and adding the requirement that Exchanges on the Federal Platform conduct pre-enrollment verification for at least 75 percent of new enrollments.
In the proposed rule, we stated that we anticipate that maintaining this expansion of pre-enrollment verification for SEPs would result in approximately 1 hour of time spent by consumers to complete associated questions in the application or submit supporting documentation (91 FR 6432). Based on historical data from the FFE, we estimate that approximately 293,073 new SEP verification issues would continue to be generated at the household level for Exchanges on the Federal platform. Therefore, maintaining these inconsistencies would continue to increase burden on consumers by approximately 293,073 hours. Using the estimate of the hourly value of time for changes in time use for unpaid activities calculated at $25.02 per hour in section IV.A, we estimate that the cost increase for all consumers who generate this income inconsistency would be approximately $7,332,686 annually starting in 2027.
Additionally, we estimate that maintaining expanded pre-enrollment verification for SEPs would result in an increase in burden on Exchanges using the Federal platform. Based on historical FFE data, we anticipate that approximately 293,073 inconsistencies would be generated at the household level for Exchanges on the Federal platform. Once households have submitted the required verification documents, we estimate that it would take approximately 12 minutes (0.2 hours) for an eligibility support staff person (BLS occupation code 43-4061), at an hourly cost of $49.52,[388]
to review and verify submitted verification documents. Therefore, expanding verification would result in an increase in burden on Exchanges on the Federal platform of 58,615 hours (293,073 verifications × 0.2 hours per verification) at a cost of $2,902,615 (58,615 hours × $49.52 per hour) annually starting in 2027.
We sought comment on these proposed burden estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these burden estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates below.
Comment:
Several commenters stated concern that expanding SEPV would increase the burden on Exchanges using the Federal platform, which could potentially result in delayed coverage and discourage enrollment. Commenters also stated that the proposed estimates did not account for additional expenditures related to consumer communications, outreach, and assister training.
Response:
We agree that expanding SEPV will increase the burden on Exchanges using the Federal platform. Our estimates are based on historical data from the FFE, and we anticipate that the expansion of SEPV will result in an increase in annual labor burden on Exchanges using the Federal platform at an estimated cost of $2,902,615 annually.
L. ICRs Regarding Expansion of Hardship Exemption Eligibility (§ 155.605(d)(1))
Under this finalized policy, individuals who are ineligible for APTC or CSRs due to projected household income may apply for a hardship exemption to qualify for catastrophic coverage. While the FFE automatically grants these exemptions through the application system when consumers apply for catastrophic coverage, some consumers may submit paper applications for hardship exemptions.
In the proposed rule, we stated that the burden associated with this requirement includes the time for consumers to complete and submit paper hardship exemption applications, and the time for Exchanges to review and process these applications.[389]
This information collection is currently approved under OMB control number 0938-1191 (CMS-10440), which covers hardship exemption applications and related documentation.[390]
The finalized expansion of hardship exemption eligibility will not create a new information collection but will expand the scope of an existing collection to include a new category of eligible applicants.
Based on current FFE implementation, we estimate that it will continue to require consumers approximately 16 minutes to complete and submit a paper hardship exemption application.
The four State Exchanges that process their own exemptions—California,
( printed page 29815)
Connecticut, Maryland, and the District of Columbia—will experience an administrative burden associated with reviewing and processing hardship exemption applications under the expanded eligibility criteria. We estimate that Exchange staff will require approximately 19 minutes to manually review and process each paper hardship exemption application. Using the adjusted hourly wage of $49.52 for Eligibility Interviewers, Government Programs (occupation code 43-4061), we estimate the cost per application to be $15.75 [(19 minutes ÷ 60 minutes) × $49.52/hour].
Based on the FFE implementation data and accounting for the enrollment share of the four State Exchanges that process their own exemptions (estimated at approximately 10 percent of total Exchange enrollment), we estimate these four State Exchanges will collectively process approximately 1,072 applications annually under the expanded hardship exemption eligibility criteria. Using the per-application manual processing cost of $15.75, we estimate the total annual cost burden for these four State Exchanges in total to be approximately $16,884 (1,072 applications × $15.75 per application). Individual State burden would depend on each State Exchange's enrollment volume and the proportion of consumers who fall into the expanded hardship exemption category. States with larger enrollment volumes and higher proportions of consumers with income below 100 percent FPL or above 250 percent FPL may experience higher application volumes than States with smaller enrollment or different demographic characteristics.
We note that the burden estimates presented previously may not reflect the actual burden on both consumers and Exchanges. The FFE experience demonstrates that automated exemption processing significantly reduces the need for manual paper application review. Exchanges may implement similar automated systems that grant hardship exemptions automatically when consumers ineligible for APTC or CSRs due to income apply for catastrophic coverage, thereby eliminating the need for separate exemption applications in most cases. Additionally, State Exchanges currently processing their own exemptions may choose to delegate exemption processing to HHS, which would eliminate the direct administrative burden on the State while ensuring consumers have access to the expanded hardship exemption eligibility. This delegation option is available under existing regulations and would result in zero additional burden to the delegating States.
We sought comment on these assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
M. ICRs Regarding Modification of Exchange Network Adequacy Standards (§ 155.1050)
In the proposed rule, we stated that the burden associated with QHP issuers and States in State Exchanges and SBE-FPs in implementing changes for PY 2026 to meet time and distance standards at § 155.1050 is covered by the currently approved information collection (OMB Control Number: 0938-1341 (CMS-10592)/Expiration date: April 30, 2027) (91 FR 6433). We sought comment on these proposed burden estimates in the context of the changes at § 155.1050(a)(2) that we proposed in the proposed rule and are now finalizing in this final rule, discussed directly below.
We are finalizing our proposal to amend § 155.1050(a)(2) to eliminate, for plan years beginning on or after January 1, 2027, the requirements under § 155.1050(a)(2)(i) and (ii) for State Exchanges and SBE-FPs to establish and impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs under § 156.230; instead, we will require that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards specified in § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or, for plan years beginning on or after January 1, 2027, § 156.236(a) for non-network plans if such plans are allowed to be offered through the Exchange, as applicable. Many State Exchanges and SBE-FPs demonstrated to HHS that they have robust network adequacy standards and reviews in place beyond the requirements specified in § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or § 156.236(a) for non-network plans. This approach recognizes that States are often best positioned to evaluate local provider networks and market conditions.
We estimate there would be minimal increase in burden to issuers associated with the modification of this policy as it was in effect for only one plan year, and prior to PY 2026, each State Exchange and SBE-FP was evaluated by HHS to understand their current state of network adequacy reviews, with all States being deemed as either meeting the requirements described at § 155.1050(a)(2)(i) or were determined to have a network adequacy review in place that met the requirement for the exception described at § 155.1050(a)(2)(ii).
We previously estimated that the total annual burden associated with State Exchanges and SBE-FPs in establishing and conducting network adequacy reviews to be up to 900 hours, which we anticipate would still apply, as we do not anticipate State Exchanges or SBE-FPs would need to make changes to their systems or policies to support the restoration of flexibilities to conduct network adequacy. Assuming the compliance officer average hourly rate of $75.40,[391]
we estimate the cost of the data collection, operations, and maintenance pertaining to these finalized requirements on each State Exchange and SBE-FP would be $67,860 per year (900 hours × $75.40 per hour). In total, for the 22 State Exchanges and 1 SBE-FP anticipated to be operational in 2027, we estimate a burden of 20,700 hours (23 State Exchanges and SBE-FPs × 900 hours per Exchange) at an annual cost starting in 2027 of $1,560,780 (23 State Exchanges and SBE-FPs × 900 hours per Exchange × $75.40 per hour).
We sought comment on these proposed burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
N. ICRs Regarding General Program Integrity and Oversight Requirements (§ 155.1200)
We are finalizing our proposal to amend § 155.1200(d) to reduce duplication between the proposed SEIPM program described in proposed subpart Q and the annual independent external programmatic audit requirements and standards described at § 155.1200(c) and (d). We are adding § 155.1200(e) to permit a State Exchange to satisfy certain annual independent external programmatic audit requirements, as described at § 155.1200(d), by completing the required annual SEIPM program process finalized in this rule. As a result, we estimate that there would be a general burden reduction for State Exchanges related to the programmatic audit requirement under § 155.1200(c). In
( printed page 29816)
particular, the 22 State Exchanges that operate their own eligibility and enrollment platforms would incur lower costs for contracts with independent external auditors, since many requirements under subparts D and E would be addressed through completion of the SEIPM process for the applicable benefit year.
In the proposed rule, we stated that based on industry estimates of the average cost of contracting an auditor to perform an independent external programmatic audit, we project that the reduced audit scope would lower annual costs by approximately $45,000 for each State Exchange (91 FR 6433). This is based on an estimated average annual programmatic cost of $150,000. We anticipate the total cost annual reduction across 22 State Exchanges would be approximately $990,000 and that these savings could begin as early as 2027, coinciding with the submission of independent external audits for the PY 2026 SMART. However, we also noted that this change would also introduce a new burden associated with completing the SEIPM process, as discussed in the section below.
We sought comment on these proposed burden estimates and assumptions and specifically sought feedback from State Exchanges regarding the annual cost of the programmatic audit process.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
O. ICRs Regarding the State Exchange Improper Payment Measurement (SEIPM) (§§ 155.1600-155.1650)
As described in the preamble to § 155.1600, SEIPM is being finalized as proposed to replace the previous IPPTA program with requirements related to mandatory participation in SEIPM. SEIPM is designed as a process for HHS to review payments of APTC that were determined by State Exchanges to produce an estimate of improper payments.
In the preamble to § 155.1615(a)(1), we are finalizing our proposal that State Exchanges would provide to HHS: the State Exchange's Program Information which consists of policy, operational and technical documentation concerning business rules and calculations, entity relationships, data dictionaries, operating procedures, and system technology. This information is currently retained by State Exchanges in a digital format and can be electronically transmitted to HHS. We estimate that the burden associated with the collection and transfer of this information to HHS would be no more than 40 hours.
In the preamble to § 155.1615(a)(2), we are finalizing our proposal that State Exchanges would provide HHS with the universe of tax household information respective to the plan year being reviewed, that being a listing of the population of tax households that were enrolled in a QHP, where payments of APTC were made. The listing must include an identifier for each tax household, an identifier for each QHP policy within that tax household, the tax household size, the total payment amounts for each sampled unit for the benefit year, and information about the existence of an eligibility verification inconsistency associated with each sampled unit. The burden associated with the finalized collection of information includes the time it would take each State Exchange to meet with HHS to review the submitted information. We estimate that the burden associated with this data collection and transfer would be no more than 40 hours.
In the preamble to § 155.1615(a)(3), we are finalizing our proposal that State Exchanges would provide HHS with review unit data, that being the specific information that is required to review each of the sampled QHP tax household, which includes the following information at the tax household level:
Information pertaining to the calculation of the APTC benefits paid. This includes monthly enrollment premium amounts, monthly APTC payment amounts, monthly Second Lowest Cost Silver Plan Premium amounts, and monthly essential health benefit amounts.
Information provided by policy issuers relevant to enrollment reconciliation. This includes dates and amounts of effectuation payments, APTC and premium payment information, and policy start and end dates.
Information relevant to the determination of eligibility for an SEP (where applicable), this includes consumer attestations and representations, copies of documentary evidence submitted by applicants, electronic verification information, and timing information.
Information about timing of certification and coverage area of the associated QHP. This includes the coverage area of the QHP, timing of QHP certification or approval, and timing of QHP decertification or suppression.
For each person on the policy who is included in the APTC payment calculation:
Attestation and demographic information relevant to initial QHP. This includes the demographic information and consumer attestations and representations.
Information relevant to electronic eligibility verifications and payment determinations. These include the electronic source consulted, the timing of the verification, and the results of the verification.
Information relevant to QHP and APTC manual eligibility verifications and the resolution of electronic verification inconsistencies. This includes copies of documentary evidence submitted by applicants, the timing of submission, the timing of adjudication, and information about good faith extensions.
HHS would specify the manner in which the data is collected. HHS anticipates utilizing a standardized data request form with specific required fields for the collection of this information. The final collection instrument and methodology will be specified in subsequent guidance and would be designed to minimize burden while ensuring data quality and consistency across State Exchanges. HHS will provide State Exchanges with detailed specifications for data formatting, submission procedures, and technical requirements prior to implementation. We estimate that the burden associated with this data collection and transfer would be no more than 8 hours per sample. We anticipate each State Exchange would need to provide between 50 to 250 samples proportionate to the total amount of APTC payments processed by the State Exchange. At the aggregate level, a total sample size of approximately 2,000 tax households would be used to support improper payment measurement across all State Exchanges. In future periods, the total sample size may be adjusted based on factors such as observed error rates, statistical precision requirements, State Exchange participation levels, and available program resources, while ensuring compliance with OMB statistical sampling guidance for improper payment measurement.
The burden associated with completion and return of the required information would be the time it would take each State Exchange to meet with HHS to review the information being requested, analyze and design any database queries needed to produce the information, organize the information into a document or documents for the
( printed page 29817)
purposes of transmittal to HHS, electronically transmit the information to HHS, and meet with HHS to verify and validate the information.
We estimate that for each State Exchange, the total costs would range between $24,950 and $124,750 depending on the identified sample size. The calculation at the low end of the range was produced by multiplying 50 (the smallest number of samples that will be used in SEIPM) × $499 (the average cost per sampled record) = $24,950. The calculation at the high end of the range was produced by multiplying 250 (the largest number of samples that will be used in SEIPM) × $499 = $124,750.
The annual, aggregated burden for the total 22 State Exchanges to complete the SEIPM is estimated to be $1,097,800. This calculation was made by multiplying 2,200 (the total number of samples to be used in SEIPM) × $499 (the average cost per sample). This cost estimate encompasses the processes at the State Exchanges that includes but is not limited to the following: sampling procedures, data collection protocols, and analytical frameworks required to produce an annual improper payment estimate while maintaining statistical validity and regulatory compliance standards.
To compile our estimates, we utilized industry-standard burden estimation methodologies commonly employed for Federal data collection initiatives. We conducted a comprehensive task analysis to identify specific personnel roles and time requirements across all phases of the data collection process, including transition and SEIPM preparation, system setup and maintenance, materials preparation, tool and data preparation for review processes, pre-engagement activities, sampling procedures, review conduct, collaborative observations, and closeout activities. This systematic approach ensures our estimates reflect realistic operational requirements based on established Federal data collection practices.
Hourly wage rates vary across the occupational specialties necessary to perform the information collection and are as follows:
This establishes a mean hourly rate of $111.12 across all of the occupational specialties that would be needed for performing this collection.
While the initial burden estimate assumes 8 hours per sample as a baseline, HHS recognizes that State Exchanges would realize significant economies of scale when processing multiple samples within the same collection period. The initial sample requires the upfront costs in system setup, query development, staff training, and process establishment. However, subsequent samples within the same collection cycle will benefit from:
Established data extraction processes and validated database queries
Trained personnel familiar with HHS requirements and submission procedures
Streamlined workflows and standardized documentation templates
Reduced coordination overhead through established communication channels
These efficiencies typically reduce the per-sample burden for subsequent samples after the initial setup. The 8-hour baseline represents the maximum expected burden per sample, with actual burden decreasing as State Exchanges leverage established processes and systems for additional samples within the same collection period, equating to an average hourly burden per sample of 4.49 hours.
The calculations in this paragraph demonstrate how the cost estimates were derived for the data collection process across State Exchanges. The mean hourly rate of $111.12 was calculated by averaging the five adjusted median occupational wage rates ($99.00 + $164.62 + $97.30 + $99.80 + $94.88 = $555.60 ÷ 5 = $111.12). While the baseline estimate assumes 8 hours per sample initially, economies of scale reduce the average burden to 4.49 hours per sample as State Exchanges develop efficient processes for subsequent samples. The cost per sample is calculated by multiplying the average burden hours by the mean hourly rate (4.49 hours × $111.12 = approximately $499 per sample). Finally, the aggregate cost estimate of $1,097,800 across all 22 exchanges represents the total expected cost when these efficiencies are realized across the entire sample collection process, which works out to an average of approximately $49,900 per State Exchange, calculated with the premise that each State Exchange would submit on average 100 samples. In summary, the total cost of $1,097,800 is derived from multiplying the estimated average cost per sample ($499) times the total samples (2200) to be drawn across all the State Exchanges.
The costs associated with the SEIPM program will begin in 2027, coinciding with the effective date of the regulation as specified in § 155.1605(a). These are annual recurring costs that State Exchanges will incur each year as part of the ongoing SEIPM requirements. The annual nature of these costs reflects the ongoing data submission processes that State Exchanges must perform to support HHS' annual improper payment measurement and reporting obligations under the Payment Integrity Information Act of 2019.
We will request to account for the associated information collection burden under OMB control number: 0938-NEW/CMS-10942.
( printed page 29818)
Additionally, as described in the preamble to § 155.1535, we are finalizing that State Exchanges may be required to develop and implement corrective action plans (CAPs) following a completed SEIPM measurement designed to reduce improper payments as a result of eligibility determination errors, beginning in 2029. The burden associated with this requirement is the time and effort put forth by State Exchanges to develop and submit a CAP to HHS. We estimate that it would take each selected State Exchange up to 1,000 hours to develop a CAP. We estimate that the total annual burden associated with this requirement for up to 22 State Exchange respondents would be up to 22,000 hours. Assuming the management analyst average hourly rate of $97.30 per hour, we estimate that the cost of a corrective action plan per State Exchange could be up to $97,300, and for all 22 State Exchanges, up to $2,140,600. The burden related to this information collection will be submitted to OMB for approval after future rulemaking has been completed regarding the CAP process and requirements.
We sought comment on these proposed burden estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these burden estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates below.
Comment:
Several commenters stated concerns regarding the burden calculations associated with SEIPM. Most of these concerns pertained the anticipated increased cost for resources needed for the data processing and the manual effort needed for documentary evidence requirements. Some commenters shared specific burden calculations associated with IPPTA and stated that SEIPM burden will be significantly more. One commenter stated that HHS did not account for the hours and costs for State Exchanges to make modifications in the PRA estimations or the current ICR of the Proposed Rule. One commenter noted that the IPPTA work accounted for at least 400 staff hours to date. Other commenters stated that HHS underestimated the burden calculations due to the complexity and challenges experienced in IPPTA, which may transfer to SEIPM. Other commenters requested additional details on the sampling methodology, sample size estimates, and other information to accurately estimate State Exchange burden and costs associated with SEIPM.
Response:
We conducted a comprehensive analysis to identify specific personnel roles and time requirements across all phases of the data collection process, including transition and SEIPM preparation, system setup and maintenance, materials preparation, tool and data preparation for review processes, pre-engagement activities, sampling procedures, review conduct, collaborative observations, and closeout activities. We used the GSA labor category table to estimate burden on key occupational roles that we considered crucial in SEIPM while also using some of the early survey data provided by State Exchanges in Group A, although we received limited feedback centered on the burden concerns. While we received some IPPTA burden information from a couple of commenters, we did not receive information across all State Exchanges.
While some commenters stated that significant time and resources were required for IPPTA, we understand that there is variability across each state in terms of how much time and resources are required. The processes such as developing SQL scripts that were completed during IPPTA are intended to translate into the SEIPM process. The time and resources spent for developing those scripts and troubleshooting the output would not be experienced in SEIPM because the work will already have been completed. We clarify that we will allow flexibility in the data submission process to alleviate some of the administrative burden placed on the State Exchanges. We also intend to release sub-regulatory guidance to provide further details on SEIPM. For these reasons, HHS believes that the proposed estimations are sufficient for the State Exchanges to complete SEIPM.
Comment:
Many commenters stated concerns about SEIPM being duplicative of other audits such as the independent external programmatic audit.
Response:
We note that we have addressed duplication concerns in the General Program Integrity and Oversight Requirements of this final rule under § 155.1200 and SEIPM under § 155.1645. We also clarify that we intend to release sub-regulatory guidance to provide additional clarity.
P. ICRs Regarding the Discontinuation of Standardized Plan Options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv))
We are finalizing our proposal to remove the following from our regulations effective beginning in PY 2027: the definition of “standardized options” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b) as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv).
As stated in the proposed rule (91 FR 6435), under §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv), approved web-brokers and QHP issuers using a DE pathway to facilitate enrollment through an FFE or SBE-FP must differentially display standardized plan options in accordance with § 155.205(b)(1) in a manner consistent with how standardized plan options are displayed on
HealthCare.gov,
unless we approve a deviation. Any requests from web-brokers and QHP issuers seeking approval of an alternate differentiation format are reviewed based on whether the same or a similar level of differentiation and clarity is provided under the requested deviation as is provided on
HealthCare.gov.
The current information collection is
Non-Exchange Entities
(OMB Control Number: 0938-1329 (CMS-10666)/Expiration date: February 20, 2029). Given that we are finalizing our proposal to discontinue the full suite of standardized plan option policies from our regulations (including standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv)), we are also finalizing the discontinuation of this information collection—as these entities are no longer required to submit a request to deviate from the form of display on
HealthCare.gov.
( printed page 29819)
We sought comment on the proposal to discontinue this information collection. We did not receive any comments in response to the proposal to discontinue this information collection. For the reasons outlined in the proposed and final rules, we are finalizing the discontinuation of this information collection as proposed.
Q. ICRs Regarding Non-Standardized Plan Option Limits (§ 156.202)
We are finalizing our proposal to discontinue non-standardized plan option limits and exceptions at § 156.202. Because we are finalizing this policy as proposed, we are also finalizing our proposal to discontinue the corresponding information collection, which is Non-Standardized Plan Option Limit Exceptions (OMB Control Number: 0938-1461 (CMS-10878)/Expiration date: July 31, 2027), since issuers that seek to offer plans that are tailored to the treatment of chronic and high-cost conditions would be able to do so without submitting information that was formerly required under the exceptions process.
We sought comment on the proposal to discontinue this information collection. We did not receive any comments in response to the proposal to discontinue this information collection. For the reasons outlined in the proposed and final rules, we are finalizing this proposal as proposed.
R. ICRs Regarding Provider Access Standards for Network Plans (§ 155.1050 and § 156.230)
We are finalizing our proposal at § 155.1050(d), for PY 2027 and beyond, to allow FFE States, including States that perform plan management, that elect to do so, to conduct provider access reviews for issuers' plans that use and do not use a provider network, provided that the State has demonstrated sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program, as described at § 155.1050(d)(2) through (d)(4) as finalized in this rule. We will continue to conduct provider access reviews consistent with § 156.230 for QHP issuers that use a provider network and § 156.230 for QHP issuers that do not use a provider network in FFE States that do not elect to conduct such reviews, or in FFE States that do not demonstrate sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program, as described at § 155.1050(d)(2) through (d)(4) as finalized in this rule. Under this finalized policy, we will continue to collect network adequacy data, including time and distance and appointment wait time data. We will continue collecting this data from all FFE issuers, either to use to conduct Federal network adequacy reviews in FFE States that do not elect to do so, or do not demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4), or with a view to make it available in a standardized format to States that are determined to have an Effective Provider Access Review Program, to assist them in their provider access analysis. We stated in the proposed rule (91 FR 6436) that we do not believe this proposal would introduce new burdens associated with data collection, as we would continue to utilize the same systems, processes, and data requirements currently in place. We believe the ICRs associated with this finalized policy are assessed and are encompassed by the revised information collections for QHP certification and network adequacy data collection (Continuation of Data Collection to Support QHP Certification and other Financial Management and Exchange Operations (OMB Control Number 0938-1187 (CMS-10433)/Expiration date: June 30, 2025) and Essential Community Provider-Network Adequacy (ECP/NA) Data Collection to Support QHP Certification (OMB Control Number. 0938-1415 (CMS-10803)/Expiration date: December 31, 2027)). Overall, we expect any change in burden cost to be negligible under this finalized policy. We do expect the total burden cost associated with the provider access review process to decrease for QHP issuers in States with an Effective Provider Access Review Program, as outside of initial data submission and validation, these issuers would not be subject to review processes conducted by HHS. However, burden costs saved by QHP issuers on the Federal level may be lost at the State review level, depending on how a State implements provider access review processes. It is unknown how States will implement provider access data collection and certification reviews under this final policy and the number of States that will elect to conduct these reviews, thus the total burden associated with undergoing this provider access certification review process on the State-level is uncertain.
We sought comment on these proposed burden estimates and assumptions.
We did not receive any comments in response to the proposed burden estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
S. ICRs Regarding Essential Community Providers (§ 155.1051 and § 156.235)
In this final rule, we are not finalizing our proposal to reduce the minimum percentage requirements described under § 156.235(a)(2)(i) and (b)(2)(i) from 35 to 20 percent for the overall, FQHC, and family planning ECP thresholds, and will maintain the minimum percentage at 35 percent for each of the three aforementioned thresholds. We are finalizing our proposal to amend the narrative justification requirement language at § 156.235(a)(3) and 156.235(b)(3) to reflect current operations and data submission requirements as part of ECP certification reviews, as narrative justifications are no longer required for issuers not meeting the ECP standard because they input contract statuses directly into the ECP User Interface in the MPMS. Additionally, we are finalizing our proposal, with modification, to allow FFE States flexibility to elect to conduct ECP certification reviews. Specifically, as discussed in the preamble of this final rule, we are finalizing our proposal to allow FFE States flexibility to elect to conduct ECP certification reviews for network plans effective beginning PY 2027; however, we are modifying our proposal such that we will allow FFE States to conduct ECP certification reviews for non-network plans effective beginning PY 2028 under § 155.1051 due to the delayed implementation of the provisions allowing certification of non-network plans as QHPs. As noted in the proposed rule, the ICRs associated with QHP certification and ECP Data Collection to Support QHP Certification have already been assessed and are encompassed by the currently approved information collections (
Continuation of Data Collection to Support QHP Certification and other Financial Management and Exchange Operations
(OMB Control Number 0938-1187 (CMS-10433)/Expiration date: June 30, 2025) and
Essential Community Provider/Network Adequacy (ECP/NA) Data Collection to Support QHP Certification
(OMB Control Number. 0938-1415 (CMS-10803)/Expiration date: December 31, 2027)) (91 FR 6436).
( printed page 29820)
We note that the type of ECP data collected from issuers will remain the same; issuers will still be required to designate contracted ECPs included within their provider networks for each of their service areas to meet the ECP standard under § 156.235. Thus, we expect issuer burden to remain at least the same by maintaining existing ECP threshold requirements, or lower due to recent system enhancements within the ECP UI in MPMS that aim to minimize issuer burden. For example, MPMS system enhancements within the ECP UI include optimized filter options that display applicable ECPs relevant to meeting specific ECP requirements (including threshold requirements) if selected as contract executed or contract offered by issuers; prior year import functionality that enable issuers to import ECP data from their previous year's QHP application, including contracts executed with ECPs, which reduces time needed to re-enter details that are up to date; and an ECP calculation workspace that provides direct feedback on how issuers scored on each ECP requirement within each network and service area (for example, a met versus unmet status), and how many additional ECPs need to be included within their application to satisfy ECP requirements. However, issuers may not experience reductions in administrative costs due to the need to maintain existing contracts, including by re-negotiating contract renewals and/or pursuing additional contracts to continue to meet existing ECP requirements.
Based on an analysis of PY 2026 FFE plan data, the average threshold percentage for all FFE QHP issuers, including issuers in States performing plan management, was 71 percent for the overall ECP threshold requirement, 85 percent for the family planning provider threshold requirement, and 79 percent for the FQHC threshold requirement. Thus, many issuers continue to exceed current threshold requirements by more than 30 percent, so even if the threshold were reduced to 20 percent, the reduction may not have influenced issuer contracting behavior and associated administrative cost savings. Therefore, in this final rule, we are not finalizing our proposal to reduce the minimum percentage requirements, which will maintain the minimum percentage at 35 percent for the overall, FQHC, and family planning ECP thresholds.
Furthermore, according to an analysis of PY 2025 FFE plan data, 14 medical QHPs (including one dual QHP) and 8 additional SADPs would have been required to submit narrative justifications for not meeting the ECP standard under § 156.235 if these data requirement collections were still in place. In the justification Excel format used prior to PY 2025, the 22 issuers referenced previously would have spent on average an estimated minimum of at least 2 minutes per ECP inputting provider contact information and the status of negotiations. The modernizations to the ECP data collection process in the ECP UI implemented beginning for PY 2025 have contributed to burden reductions among these issuers, since the time spent reporting provider data will be reduced, with issuers easily importing their prior year's ECP data into their current year's application or selecting ECPs with pre-populated contact information from the list embedded in MPMS. Additionally, in lieu of providing information on particular ECPs and writing responses to questions pertaining to monitoring and mitigating measures for ECP network gaps in the Excel justification format, these issuers now designate the status of negotiations with particular ECPs by selecting from a drop-down list in MPMS, which averages an estimated minimum of at least 5 seconds per ECP. As a whole, these efficiencies to the justification process through the ECP UI MPMS modernizations have reduced issuer burden as part of ECP certification reviews through reductions in the amount of time issuers spend submitting ECP data because the data is mostly prepopulated within MPMS, there are drop-down options to quickly append the status of contract negotiations, and MPMS clearly identifies needed corrections and required fields for the issuer to complete a satisfactory justification to support their QHP certification. Therefore, we are finalizing our proposal to change the narrative justification regulation text at § 156.235(a)(3) and (b)(3) to be consistent with these system changes, current HHS operational processes, and existing issuer ECP data submission requirements as part of ECP certification reviews.
In addition, we are finalizing our proposal, with a minor modification, to allow FFE States, including States performing plan management, to elect to conduct their own ECP certification reviews of issuers plans' with or without a provider network provided the State demonstrates it has sufficient authority and the technical capacity to conduct these reviews by meeting the applicable criteria, as determined by HHS, to be considered to have an Effective ECP Review Program under § 155.1051. While we are finalizing, beginning PY 2027, the proposal for FFE States to conduct their own ECP certification reviews of issuers' plans with a provider network provided the State demonstrates it has sufficient authority and the technical capacity to conduct these reviews, we are modifying our proposal to delay application of this policy to ECP certification reviews of issuers' non-network plans until PY 2028 due to the delayed implementation of the provisions allowing QHP certification of non-network plans. An FFE State will need to first express its interest to HHS and submit an attestation, and it will be granted an Effective ECP Review Program designation after HHS determines it meets all applicable requirements described for this program under § 155.1051. An FFE must also demonstrate sufficient authority and technical capacity to review non-network plans seeking QHP certification beginning PY 2028, if the State deems to allow such plans to operate in the State. If we determine that an FFE State does not have an Effective ECP Review Program or an FFE State does not elect to conduct such reviews, then we will continue to perform ECP certification reviews consistent with § 156.235 for network plans and § 156.236 for non-network plans (effective PY 2028). We are revising the information collection currently approved under OMB Control Number 0938-1415 (CMS-10803) (Essential Community Provider-Network Adequacy (ECP/NA) Data Collection to Support QHP Certification to reflect new requirements finalized under § 155.1051 for the Effective ECP Review Program. Since we will perform ECP certification reviews for issuers in FFE States without an Effective ECP Review Program consistent with our current operations, processes, and data submission requirements as part of QHP certification, we do not believe this finalized policy will introduce any new burdens associated with data collection. In addition, for QHP issuers in Effective ECP Review Program States, we do expect the total annual hours and annual burden cost associated with the ECP certification review process to slightly decrease on the Federal level. While QHP issuers in FFE States with an Effective ECP Review Program will still need to submit ECP data to HHS, issuers will not be required to undergo the extensive ECP review process to address corrections identified by HHS by resubmitting data, if they instead go through this process in FFE States with an Effective ECP Review Program. However, burden costs saved by QHP
( printed page 29821)
issuers by not undergoing the extensive ECP certification review process on the Federal level may be offset at the State level if FFE States impose new, additional ECP certification data collection and review procedures for QHP issuers that do not already exist to comply with § 155.1051. It is unknown how FFE States will implement ECP data collection and certification reviews and the number of FFE States that will elect to conduct these reviews, thus the total burden associated with undergoing this ECP certification review process on the State level is uncertain.
We sought comment on these proposed burden estimates and assumptions, but we did not receive any comments in response to these proposed burden estimates related to ECP standards for network plans (§ 156.235) and the implementation of the proposed Effective ECP Review Program (§ 155.1051).
T. ICRs Regarding QHP Certification of Non-Network Plans (§§ 155.1050, 156.230, 156.235, 156.236, 156.275, and 156.810)
In this final rule, we are finalizing a number of revisions to Part 155 and Part 156 to allow plans that do not use a network (non-network plans) to receive QHP certification beginning with PY 2028 by demonstrating that they ensure a sufficient choice of providers in a manner consistent with section 1311(c)(1)(B) and (C) of the Affordable Care Act. We are finalizing our proposal to add new section § 156.236, that contains the provider access sufficiency standards (including ECP access) specific to non-network plans, and to revise §§ 156.230 and 156.235 to make clear that those sections address the provider access sufficiency standards (including ECP access) for network plans. Additionally, we clarify that non-network plans would be subject to and must be able to meet all of the general certification criteria at § 155.1000(c), which would allow Exchanges the ability to certify non-network plans as QHPs. Furthermore, we are finalizing our proposal effective beginning in PY 2028 to allow FFE States, including States performing plan management, to conduct provider access and/or ECP certification reviews provided the State elects to conduct these reviews and demonstrates it has sufficient authority and the technical capacity to conduct these reviews by meeting the applicable criteria, as determined by HHS, for each review program it wishes to administer; these review programs include the Effective Provider Access Review Program for provider access certification reviews under § 155.1050(d) and/or the Effective ECP Review Program for ECP certification reviews under § 155.1051. Accordingly, FFE States that elect to conduct provider access certification reviews, and are determined by HHS to have sufficient authority and the technical capacity to conduct these reviews by satisfying applicable criteria to be considered to have an Effective Provider Access Review Program under § 155.1050(d)(2) through (d)(4) will be permitted to perform such reviews of non-network plans, effective for non-network plans seeking QHP certification beginning PY 2028. Similarly, FFE States that elect to conduct ECP certification reviews, and are determined by HHS to have sufficient authority and the technical capacity to conduct these reviews by meeting applicable criteria to be considered to have an Effective ECP Review Program under § 155.1051 will be permitted to perform such reviews of non-network plans seeking QHP certification beginning PY 2028. The revision of the information collection currently approved under OMB Control Number 0938-1415 (CMS-10803) (Essential Community Provider-Network Adequacy (ECP/NA) Data Collection to Support QHP Certification) to reflect the finalized requirements under § 156.236 for non-network plans will be revised separately at a later date for OMB review and approval through the PRA renewal package process.
We believe that most of the current provider access data collection and submission requirements that apply to network plans would also apply to provider access reviews for non-network plans. Relevant to provider access reviews, under § 156.236(b)(1), non-network plans will be required to report their assessed percentage of providers in a service area that accept the plan's benefit amount as payment in full.
Additionally, to comply with § 156.236(b)(4) through (9), non-network plans will be required to submit supporting documentation and explain how they meet these regulatory requirements. Non-network plans will be required: to describe the processes and/or methodologies in place to conduct continuous outreach to available providers in a particular service area to determine whether they would accept the plan's benefit amount as payment in full; to identify how they make benefit amounts publicly available and accessible; to explain how benefit amounts are determined; to detail how they provide consumer-friendly and public information about potential balance billing scenarios and expected out-of-pocket costs; to validate that they offer an exceptions process for enrollees who cannot find providers (including ECPs) willing to accept the benefit amount as payment in full; and summarize how they provide adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers (including ECPs) in their area who will accept the plan's benefit amount as payment in full. It is uncertain approximately how many non-network plans will apply for QHP certification beginning PY 2028 to reasonably estimate the total annual burden cost and hours for completing these requirements. However, we expect the time for responding to questions to assess compliance with § 156.236(b)(4) through (9) and submitting supporting documentation for a single non-network plan will range between 20 to 40 minutes for each of the 6 attestation questions, if assuming a 500-word limit, likely requiring a maximum 2 to 4 hours total to complete.
Furthermore, we believe that many of the current ECP data collection and submission requirements that already apply to network plans would also apply to non-network plans. First, non-network plans applying for QHP certification would similarly use MPMS, which has extensively streamlined data collection and submission, reducing burden among issuers during QHP certification. The MPMS ECP UI only displays qualified and eligible ECPs in the issuer's State, reducing the burden of filtering through the entire ECP List for applicable facilities. Instead of spending time and effort inputting individual ECP data (such as facility name, facility address, ECP reference number, NPI, etc.) for each applicable facility in each of the plan's applicable network and/or service area, QHP issuers, including SADPs, are able to use MPMS to select prepopulated ECPs from a list of available and eligible ECPs within the user interface. MPMS is also updated regularly during QHP certification to remove ECPs that have closed or are no longer eligible such that issuers do not spend time entering in ECP data that is no longer valid or applicable to their QHP application.
Non-network plans must submit ECP data in MPMS to demonstrate they meet ECP related requirements at § 156.236(b)(1) through (3) such as: whether the non-network plan meets at least a minimum percentage, as specified by HHS, of available ECPs that accept the plan's benefit amount as payment in full in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B), and at least a minimum percentage of available ECPs
( printed page 29822)
in each plan's service area within certain individual ECP categories, as specified by HHS; whether the non-network plan offers the benefit amount as payment in full to at least one ECP in each of the eight ECP categories per county in the plan's service area described in § 156.235(a)(2)(ii)(B); and whether the non-network plan offers the benefit amount as payment in full to all available Indian health care providers in the plan's service area. Network plans currently satisfy data collection requirements by designating contract statuses, including whether a contract was offered or fully executed, with select ECPs within their application in MPMS. To satisfy § 156.236(b)(1) through (3), non-network plans will submit ECP data by similarly selecting ECPs within their application in MPMS, but instead of contract statuses, they will select modified statuses describing whether a select ECP was offered or accepted their benefit amount as payment in full. Thus, we do not believe the finalized ECP requirements under § 156.236(b)(1) through (3) for non-network plans would impose significantly new, additional information collections. Thus, we believe both total annual burden hours and cost of the new ECP requirements under finalized § 156.236(b)(1) through (3) would be negligible.
In summary, we will be revising the information collection currently approved under OMB Control Number 0938-1415 (CMS-10803) (Essential Community Provider-Network Adequacy (ECP/NA) Data Collection to Support QHP Certification) to reflect finalized requirements under § 156.236 for non-network plans at a later time through the OMB review and approval process for PRA renewal packages.
We sought comment on these proposed burden estimates and assumptions. However, we did not receive any direct comments in response to these proposed burden estimates for this policy, thus we are finalizing these estimates. As discussed in III.E.12. of this final rule, we are delaying the implementation of this finalized policy to PY 2028.
U. ICRs Regarding Quality Improvement Strategy (§ 156.1130)
There is no information collection associated with this policy and no changes were proposed to the QIS data collection requirements applicable to QHP issuers. QIS data collection from QHP issuers to the Exchange has been approved under OMB Control Number 0938-1286.
V. Summary of Annual Burden Estimates for
Finalized
Requirements
W. Submission of PRA-Related Comments
We have submitted a copy of this final rule to OMB for its review of the rule's information collection and recordkeeping requirements. These requirements are not effective until they have been approved by the OMB.
To obtain copies of the supporting statement and any related forms for the finalized collections discussed previously, please visit CMS' website at
www.cms.hhs.gov/PaperworkReductionActof1995,
or call the Reports Clearance Office at 410-786-1326.
V. Regulatory Impact Analysis
A. Statement of Need
This final rule includes payment parameters and provisions related to the HHS-operated risk adjustment and HHS-RADV programs, as well as 2027 benefit year user fee rates for issuers that participate in the HHS-operated risk adjustment program and the 2027 benefit year user fee rates for issuers offering QHPs through FFEs and SBE-FPs. This final rule also includes finalized revisions to the defrayal policy; removal of the requirement for a State to operate a SBE-FP before operation of a State Exchange; expanded
( printed page 29823)
marketing prohibition regulations and mandated use of the HHS-approved and created form for agents, brokers, and web-brokers; strengthened ability to take administrative actions against agents, brokers, and web-brokers; coordination of the new SEIPM process with existing independent external programmatic audit requirements; a prohibition on issuers from including routine non-pediatric dental services as an EHB; cost-sharing changes for catastrophic and bronze plans; clarifications for how catastrophic plans may have plan terms of up to 10 consecutive years; repeal of standardized plan options and non-standardized plan options limits and exceptions; revisions to network adequacy reviews; participation by QHPs that do not use a provider network; Essential Community Provider (ECP) standards and implementation of an Effective ECP Review Program; modification to allow QHP issuers to submit any two of five QISs topic areas listed in section 1311(g)(1) of the Affordable Care Act; imposition of CMPs against issuers in State Exchanges or SBE-FPs; revisions to rate filing justifications; changes to options for implementing premium payment thresholds; and income verification requirements. Finally, this final rule includes updates needed to align Exchange regulations with the WFTC legislation.
B. Overall Impact
We have examined the impacts of this final rule as required by Executive Order 12866, “Regulatory Planning and Review”; Executive Order 13132, “Federalism”; Executive Order 13563, “Improving Regulation and Regulatory Review”; Executive Order 14192, “Unleashing Prosperity Through Deregulation”; the Regulatory Flexibility Act (RFA) (Pub. L. 96-354); section 1102(b) of the Social Security Act; and section 202 of the Unfunded Mandates Reform Act of 1995 (Pub. L. 104-4); and the Congressional Review Act (5 U.S.C. 804(2)).
Executive Orders 12866 and 13563 direct agencies to assess all costs and benefits of available regulatory alternatives and, if regulation is necessary, to select those regulatory approaches that maximize net benefits (including potential economic, environmental, public health and safety, and other advantages; distributive impacts). Section 3(f) of Executive Order 12866 defines a “significant regulatory action” as any regulatory action that is likely to result in a rule that may: (1) have an annual effect on the economy of $100 million or more or adversely affect in a material way the economy, a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or State, local, territorial, or Tribal governments or communities; (2) create a serious inconsistency or otherwise interfere with an action taken or planned by another agency; (3) materially alter the budgetary impacts of entitlements, grants, user fees, or loan programs or the rights and obligations of recipients thereof; or (4) raise novel legal or policy issues arising out of legal mandates, or the President's priorities.
A regulatory impact analysis (RIA) was prepared for this final rule in keeping with Executive Order 12866. Based on our estimates, the Office of Management and Budget's (OMB) Office of Information and Regulatory Affairs (OIRA) has determined that this rulemaking is “significant” per section 3(f)(1). Under Subtitle E of the Small Business Regulatory Enforcement Fairness Act of 1996 (also known as the Congressional Review Act), OIRA has also determined that this is a major rule as defined by 5 U.S.C. 804(2).
We have prepared an RIA that, to the best of our ability, presents the costs and benefits of the rulemaking.
C. Impact Estimates of the Finalized Payment Notice Provisions and Accounting Table
This final rule implements standards for programs that will have numerous effects, including providing consumers with access to more affordable health insurance coverage, reducing the impact of adverse selection, and stabilizing premiums in the individual and small group health insurance markets and in Exchanges. We are unable to quantify all the benefits and costs of this final rule. The effects in Table 22 reflect qualitative assessment of impacts and estimated direct monetary costs and transfers resulting from the provisions of this final rule for Exchanges, health insurance issuers and consumers. The annual monetized transfers described in Table 23 includes changes to costs associated with the risk adjustment user fee paid to HHS by issuers.
( printed page 29824)
( printed page 29825)
( printed page 29826)
( printed page 29827)
1. HHS-RADV Error
Estimation Modification to Incorporate IVA Sampling Changes
In the 2026 Payment Notice, we finalized excluding enrollees with HCCs from IVA sampling beginning with benefit year 2025 HHS-RADV. As a consequence of this change to the IVA sampling methodology, we are now finalizing our proposal to add an additional scaling factor
ai
to the error estimation methodology to ensure that HCC-associated error rates continue to apply to only the proportion of total PLRSs that are associated with HCC components of EDGE risk scores. The additional scaling factor
ai
will serve to capture the proportion of an issuer's total population's risk that is associated with enrollees with HCCs.
In simulating the impact of the proposed additional scaling factor, we found that HHS-RADV adjustments to risk adjustment transfers decreased in magnitude by 11.7 percent in the individual market (going from $148 million to $139 million) and by 13.8 percent in the small group market (from $81 million to $69.8 million). Table 24 shows only the impact on positive HHS-RADV adjustments. Because HHS-operated risk adjustment, and HHS-RADV adjustments, are budget neutral, we anticipate the same impact on negative risk adjustment transfers (or risk adjustment charges), in that both will decrease in magnitude. When examining the impact of the additional finalized scaling factor on HHS-RADV adjustments over premium, we anticipate only a 0.01 percent change in positive HHS-RADV adjustments in both markets between results with no additional factor and results with the additional scaling factor. This corresponds with a percentage point (PP) change of − 0.02. This helps to contextualize the change in the magnitude of HHS-RADV adjustments. This finalized policy will more precisely assess the proportion of an issuer's population's risk that arises as a result of enrollees with HCCs.
We solicited comments on the estimated impacts of this proposal.
( printed page 29828)
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in this final rule, we are finalizing these estimates as proposed.
2. HHS Risk Adjustment User Fee for 2027 Benefit Year (§ 153.610(f))
For the 2027 benefit year, HHS will operate risk adjustment in every State and the District of Columbia. As described in the 2014 Payment Notice (78 FR 15416 through 15417), HHS' operation of risk adjustment under section 1343 of the Affordable Care Act on behalf of States is funded through a risk adjustment user fee. For the 2027 benefit year, we are finalizing our proposal to use the same methodology to estimate our administrative expenses to operate the HHS risk adjustment program as was used in the 2026 Payment Notice. As discussed previously in this final rule, risk adjustment user fee costs for the 2027 benefit year are expected to be similar to the prior 2026 benefit year budget estimates.
However, expected enrollment has deviated from the proposed rule to the final rule. Specifically, we have more recently available interim risk adjustment data for benefit year 2025, resulting in an increase to some of our enrollment estimates. Therefore, we anticipate that our revised enrollment projections will somewhat impact expected HHS risk adjustment user fee collections. For these reasons, we are finalizing a risk adjustment user fee rate of $0.18 PMPM for the 2027 benefit year, which is lower than the $0.20 PMPM for the 2026 benefit year. We expect the finalized HHS risk adjustment user fee for the 2027 benefit year will decrease the amount transferred from issuers of risk adjustment covered plans to the Federal Government by approximately $4 million.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates.
3. Submission of Rate Filing Justification (§ 154.215)
This rule finalizes our proposal to collect information on adjustments to the index rate as part of the rate filing justification to account for unreimbursed CSRs. As detailed in section III.C of this preamble, issuers will be required to report on the URRT actual CSR amounts paid on behalf of eligible enrollees and additional revenue collected from the previously applied CSR load (using the most recent annual data that is available prior to the applicable filing year, generally two years prior, using the standard methodology set forth in § 156.430(c)(2)), projected CSR amounts expected to be paid on behalf of enrollees in the upcoming plan year and the additional revenue expected to be collected from the applied CSR load factor for the upcoming plan year, and the CSR load factor for the upcoming plan year. This rule also finalizes our proposal to require issuers to provide an explanation in the Actuarial Memorandum of the methodology used to determine the load factor for the upcoming plan year and an explanation of how additional revenue expected to be collected from the applied CSR load factor compares to the amount of CSRs expected to be paid on behalf of enrollees for the same period.
The finalized provisions will primarily affect health insurance issuers offering qualified health plans in the individual market, Federal and State regulators in their review capacity, and indirectly, Marketplace enrollees who receive cost-sharing reductions. The enhanced CSR reporting will enable issuers to more accurately determine their CSR payment amounts and improve future projections for rate setting. This increase in accuracy and transparency may result in more appropriate premium levels if current CSR load factors are determined to be inaccurate or unreasonable, enabling issuers to better calibrate their load factors to adequately cover actual CSR costs, potentially leading to more stable and accurate premium pricing over time.
Issuers will incur a one-time cost, in 2026, of $418,790,376 to implement the standard methodology and generate the new URRT entries, followed by annual ongoing costs, beginning in 2027, of $209,395,188 to update their systems and recalculate the URRT values. Additionally, issuers will incur annual ongoing costs, beginning in 2026, of $157,222 to enter the finalized values in the URRT and $628,888 to provide an explanation in the Actuarial Memorandum of how the CSR load factor was determined. Costs might vary with issuer scale, data systems, and product complexity. These costs are expected to add approximately $2.00 PMPM or 0.25 percent of premium in administrative expenses for the 2027 plan year with that amount decreasing to approximately $1.00 PMPM or 0.13 percent of premium in later years. Additionally, the Federal Government will incur annual ongoing costs, beginning in 2026 (for PY 2027 rate filings), of $2,414,256 to review the additional information submitted. These costs are discussed in detail in the Collection of Information section IV.B of this final rule.
Enrollees can potentially experience changes in out-of-pocket costs as more accurate CSR reporting may lead issuers to adjust their load factors and premium pricing; the direction of these changes will depend on whether the current CSR load factors overestimate or underestimate actual CSR costs. If issuers have been overestimating actual CSR costs, they may decrease load factors and premiums, which could result in lower out-of-pocket costs for
( printed page 29829)
enrollees through decreased premiums. Conversely, if issuers have been underestimating CSR costs, load factors and premiums could increase.
Changes in CSR load calculations could result in corresponding adjustments to PTCs, as more accurate CSR load factors may increase or decrease silver plan premiums. If CSR loads decrease, silver plan premiums should decrease with corresponding Federal PTC outlays decreasing and offsetting changes in consumer net premiums. To the extent that improved estimates change plan pricing, there may also be distributional enrollment shifts among enrollees across metal levels on-Exchange and in silver plans offered off-Exchange.
We sought comment on these impacts and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates later.
Comment:
A few commenters supported the proposed CSR data collection, stating that they are in favor of increased transparency and standardized reporting to better understand CSR loading practices and ensure CSR loads align with actual costs. Many other commenters stated concern that the proposed CSR data reporting requirements would impose significant operational and financial burdens on issuers and may lead to higher premiums.
Response:
We acknowledge that issuers will incur operational and financial burdens because of these reporting requirements. However, as discussed in section III.C.1 of this preamble, collection of this information is an important program integrity measure that will help ensure that CSR loads are appropriate to recover lost CSR payments and are not inappropriately inflating Federal expenditures or undermining Federal rating rules. This information will also benefit State regulators by providing necessary data to determine if their issuers' CSR load amounts are actuarially justified plan-level adjustments to the index rate under § 156.80.
Comment:
Several commenters stated that implementation for PY 2027 is infeasible, noting that the final rule would arrive close to or after State filing deadlines and would require issuers to reconstruct 2025 claims data that was not consistently stored for this purpose. These commenters noted that the proposal compresses system design, vendor contracting, validation, and rate filing work into an unrealistically short window.
Response:
We acknowledge that implementation timing can affect both the operational feasibility and quality of initial data submissions. We recognize the substantial one-time and annual costs associated with implementing the standard methodology and that some issuers may incur additional costs associated with vendor contracting, data and systems validation, and reporting to meet the required reporting date. As discussed in section III.C.1 of this preamble, we do not agree that a delayed implementation date is warranted. The data collection process is intended to leverage the existing rate filing process by using the existing URRT and currently required actuarial memorandum.
Comment:
Many commenters stated that the standard methodology is especially burdensome because it effectively requires retrospective re-adjudication or double adjudication of claims, accumulator recalculation, pharmacy benefit manager (PBM) and vendor involvement, manual corrections, and ongoing audit work to produce credible data, and that the systems or staff needed to perform this work are no longer maintained in the form contemplated by the proposal.
Response:
We acknowledge the operational concerns raised regarding the standard methodology but continue to be of the view that obtaining standardized annual information is important to improving the accuracy of future CSR projections and supporting review of whether applied load factors are appropriately calibrated to expected unreimbursed CSR obligations. As discussed in section III.C.1 of this preamble, issuers were required to use the standard methodology to calculate CSRs paid on behalf of enrollees for the 2017 plan year and we believe it remains the most accurate method for such calculation. While issuers may need to update their systems to generate the actual value of CSRs provided, the actuarial memorandum should already include an explanation of the methodology used to determine the load factor; therefore, while issuers may incur some additional costs for actuarial analysis, the impact on issuers' system is limited.
Comment:
Several commenters stated that using recent experience to constrain or reshape CSR loading could reduce affordability for subsidized consumers by lowering benchmark silver premiums and therefore APTCs, shifting enrollment among metal levels, or increasing benchmark volatility. A few commenters emphasized that even modest premium or subsidy changes can have outsized effects in rural and limited-issuer markets where Tribal entities help finance coverage and depend on predictable APTC values.
Response:
As discussed in more detail in section V.C.3 of this final rule, we acknowledge that more accurate CSR reporting could either decrease or increase load factors and hence premiums, depending on whether current values overstate or understate an issuer's expected CSR costs and revenues. We do not assume a single directional market effect and recognize that impacts may vary across geographies and populations. As discussed in section III.C.1 of this preamble, we appreciate commenters' concern that such shifts in enrollment could negatively affect American Indian/Alaska Native populations and Tribal health programs. CMS affirms that it undergoes tribal consultation for all rulemaking and has worked with the appropriate parties to ensure that any such potential impact is mitigated.
Comment:
Several commenters stated that the RIA did not sufficiently explain why the new burden is warranted or quantify how the reporting requirement could affect premiums, premium tax credits (PTCs), or consumer affordability. A few requested HHS to analyze data already collected under the PY 2026 guidance before making the requirement recurring.
Response:
We acknowledge these concerns. As described in the RIA, we have tried to quantify the administrative costs of the reporting and analysis, and we recognize that issuers may pass on these costs to consumers in the form of increased premiums, which could have significant impacts on PTCs, and enrollment or retention of enrollees. We recognize that the effects of the CSR load reporting are uncertain, as outcomes depend on whether current load factors overstate or understate actual CSR obligations. As discussed in section III.C.1. of this preamble, the purpose of this data collection is to allow the State or CMS, as applicable, to determine whether the CSR load factor is actuarially justified and not excessive in relation to the amount expected to be paid for unreimbursed CSRs. We are concerned that excessive CSR loads on silver plans might lead to inflated premiums for silver plans, further distorting pricing for bronze and gold plans relative to silver plans, limit consumer choice, increase premium costs for unsubsidized enrollees, and significantly increase the cost of the second lowest cost silver plan, which in
( printed page 29830)
turn increases PTC amounts and Federal expenditures. The collection is intended to improve the evidentiary basis for future oversight and rate-review analysis.
Comment:
A few commenters stated that documentation and review of CSR loading could improve pricing signals, detect over-collection, and reduce subsidy distortions or unwarranted benchmark premium inflation, and viewed the reporting burden as justified given the size of Federal PTC exposure. Many commenters contended that the RIA understates the likelihood that issuer compliance costs will be passed through into premiums or will crowd out resources otherwise available for member services or care management emphasizing that a market-wide administrative burden in the hundreds of millions of dollars can itself create material pricing pressure.
Response:
As described in the RIA, the proposal aims to improve the alignment between pricing inputs and expected CSR obligations over time, not to predetermine a particular pricing outcome. We acknowledge that administrative costs may be passed on to consumers in the form of premium increases or potential changes in cost-sharing amounts. However, as discussed in section III.C.1.b. of this preamble, while we recognize that many issuers might have to update their systems to calculate the actual value of CSRs provided, we believe that issuers should already be calculating the actual CSRs paid for enrollees, as specified earlier in the PY26 Rate Filing Guidance. That guidance instructed issuers to report the actual CSRs paid for enrollees for PY 2024 in the actuarial memorandum submitted with the 2026 rate filing. Furthermore, as discussed in section III.C.1. of this preamble, the additional data collected will be used to ensure that CSR loads are actuarially justified to compensate for the amount of unreimbursed CSRs, which we believe serves the broader goal of protecting both consumers and Federal expenditures over time.
4. Approval of a State Exchange (§ 155.105)
We are finalizing our proposal to remove § 155.105(b)(4) to rescind a requirement made in the 2025 Payment Notice,[393]
such that for a State seeking to operate a State Exchange, it must first operate for at least one plan year an SBE-FP. The original amendment was intended to give States sufficient time to create, staff, and structure a State Exchange. However, HHS recognizes that requiring States to first operate as an SBE-FP for at least one plan year could potentially create unnecessary barriers and delays for States that are well-prepared to implement a State Exchange more immediately. Ultimately, a State must demonstrate its ability to operationalize State Exchange functional requirements through a well-established and robust review process with HHS. Whether a State first operates an SBE-FP does not change our review process for determining whether a State is ultimately prepared to implement a State Exchange The finalized changes therefore do not impose any new requirements on States in operating State Exchanges or SBE-FPs and instead returns flexibility to States regarding implementation of either a SBE-FP or State Exchange.
We sought comments on the practical utility of this data collection from potential users of this CSR amount data (for example, State regulators).
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
5. Approval of a State Exchange (§ 155.106)
We are finalizing our proposal to amend § 155.106(a)(2) to rescind a requirement made in the 2025 Payment Notice [394]
that, as part of a State's activities for its establishment of a State Exchange, the State must provide supporting documentation demonstrating progress toward meeting or implementing State Exchange Blueprint requirements. States recognize the need for HHS to request supplemental documentation in order for HHS to assess a State's readiness to operate a State Exchange, which assessment supports a State's successful State Exchange operation. States have provided such supplemental documentation upon HHS request similarly both before and after this requirement was originally finalized. The Blueprint Application already provides that we may require supporting documentation from a State as evidence of its progress toward meeting State Exchange Blueprint Application requirements, which is part of HHS' overall process for providing a State with approval to operate a State Exchange. The finalized changes do not impose any new requirements on States in establishing a State Exchange.
We sought comment on these impacts and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
6. Amending Requirements for State Exchanges To Operate a Centralized Eligibility and Enrollment Infrastructure (§§ 155.205(b) and 155.221(k))
a. Amending the Requirement for State Exchanges To Operate a Centralized Eligibility and Enrollment Consumer Interface on the State Exchange's Website (§ 155.205(b))
We are not addressing in this final rule our proposal to amend § 155.205(b) to specify that a State Exchange is not limited to operating a centralized eligibility and enrollment consumer interface on the State Exchange's website as the only model for supporting consumer eligibility application submission and QHP enrollment functionality. We stated in the proposed rule that we expected minimal, if any, financial impact to current State Exchanges and States in the process of establishing their own State Exchange.
For the reasons outlined earlier in section III.D.4. of this final rule, we will address this policy and related comments in the 2028 Payment Notice or another appropriate rulemaking.
b. SBE-Enhanced Direct Enrollment Option (§ 155.221(k))
We are not finalizing our proposal to add § 155.221(k) to establish a new State Exchange enhanced direct enrollment (SBE-EDE) option by which State Exchanges can leverage direct enrollment technology to transition primarily to private sector-focused enrollment pathways operated by QHP issuers, web-brokers, and agents and brokers, instead of or in addition to a centralized eligibility and enrollment website operated by an Exchange. In the proposed rule, we stated that State Exchanges can elect, subject to HHS approval, to implement the SBE-EDE option and that the impact of the new SBE-EDE option would depend on the number of States that take advantage of the new option. We also stated in the proposed rule that current State Exchanges that elect to implement the SBE-EDE option would be responsible for meeting certain requirements for approval, in particular revising their Exchange Blueprint under new § 155.221(k) to describe precisely how the State proposes to implement the SBE-EDE option. We stated that we believe that any costs of revising the Exchange Blueprint would be nominal,
( printed page 29831)
as this process involves logging into a CMS web interface that serves as the repository for all States' Exchange Blueprints to input additional information on the updated processes and controls the State would implement to manage its new Exchange EDE program. However, we sought comment on the burden associated with this activity, noting that the Exchange Blueprint is currently approved under the PRA under OMB Control Number 0938-1172.
We sought comment on the proposed impacts and assumptions, and did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the final rule, we are not finalizing these estimates as HHS is not finalizing this policy.
7. Additional Required Benefits (§ 155.170)
We are finalizing our proposal to amend § 155.170(a) to provide that any State-required benefits will be considered “in addition to EHB” (and thus not EHB) if they are: required by a State action taking place after December 31, 2011; applicable to the small group and/or individual markets; specific to required care, treatment, or services; and not required by State action for purposes of compliance with Federal requirements. Under this finalized policy, such State-required benefits will be considered in addition to EHB regardless of whether the mandated benefits are embedded in the State's EHB-benchmark plan. We are finalizing this policy with a modification that it will be effective beginning with PY 2028 instead of PY 2027. We also are finalizing revisions to § 156.115(a) to align with this policy and to have State and issuer responsibilities for State-required benefits appear in a more logical reading order in the CFR.
We believe that this revision will have a mixed effect on the cost to States and the Federal Government. We stated in the proposed rule that a small number of States and issuers have taken significant action based on current § 155.170, including some States having sought or seeking EHB-benchmark plan changes under § 156.111 to add certain State-required benefits as EHB with the understanding that the cost of these additions would not require defrayal by the State (91 FR 6447). We stated that, in such States, this proposal may frustrate such efforts should it become effective in PY 2027, as any State-required benefit that fulfills the four proposed conjunctive elements at § 155.170(a)(1)(i) through (iv) would require defrayal, regardless of whether the benefit is included in the State's EHB-benchmark plan. We note that this defrayal policy is being finalized in this rule at § 155.170(a)(2)(i) through (iv) for plan years on or after PY 2028.
In States that ceased defraying the cost of State-required benefits included in their EHB-benchmark plans beginning in PY 2025 under the previous regulation but will be required to defray the cost of State-required benefits beginning in PY 2028 under the provision finalized in this final rule, the percentage of premium attributable to coverage of EHB for purpose of calculating APTC may decrease. Under this finalized policy, in a State that enacts a mandate for a benefit that is currently covered in its EHB-benchmark plan, there will be a decrease to Federal Government expense as the benefit will no longer be permitted to be included in the percentage of premium attributable to coverage of EHB for purpose of calculating APTC. States should evaluate the overlap between mandates and benefits covered in the State's EHB benchmark-plans for benefits for which they will be required to defray the cost under this finalized policy. Specifically, a State that wants to avoid defrayal obligations for the cost of State-required benefits that are already in the State's EHB-benchmark will be able to do so by repealing the applicable State requirement as being applicable to QHPs. While we expect that there should not be any measurable operational implications or infrastructure changes needed for States to implement this provision, we sought comments from States on any administrative costs that would be incurred as a result of implementing this provision. We likewise recognize that States that opt to retain benefit-mandates that carry defrayal obligations will incur defrayal costs. The scale of these costs will depend on the cost attributable to the State-required benefit. We sought comments from States on such estimates where applicable. Issuers may have to make modifications to their plan designs and plan filings to reflect any possible changes in designation of benefits as EHB because of this finalized policy, in the regular course of updating those annual materials. Given variation in State legislative calendars and session timing, and the need for issuers to update their plan filings and rates to account for benefits that will be defrayed by the State, we solicited comment on finalizing an effective date for PY 2028 instead of PY 2027.
We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy, but with the modification to the final policy to delay the effective date to PY 2028. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Commenters broadly supported delaying the applicability of the proposed policy until at least PY 2028, with some commenters urging HHS to delay applicability until 2029 or 2030. Commenters explained that States need time to assess which benefits are now considered “in addition to” EHB under the new policy and coordinate with CMS and issuers, and align with legislative and rate filing timelines, which would not allow sufficient time for PY 2027 implementation of the proposed policy. Commenters also emphasized that State legislative calendars and budget processes (which both vary by State) require additional time to allow for States to consider legislative or regulatory changes and to secure appropriations for defrayal, if necessary. Some commenters stated concern that the proposed policy would create instability and uncertainty for States and issuers, undermining their ability to engage in long-term fiscal and operational planning. These commenters stated that changes to defrayal requirements could result in benefits previously considered EHB becoming subject to new defrayal obligations, creating a shifting regulatory landscape with moving targets for States and issuers.
Some commenters stated concern that because the proposal could effectively apply new defrayal obligations to past State actions taken under prior regulatory frameworks, States will be forced to make difficult financial decisions that place certain benefits at risk.
Response:
We acknowledge that providing States enough time to plan to effectuate the new defrayal requirements would be beneficial. To assist States in complying with their defrayal obligations and ensure they have sufficient time, we are extending the date by which States must be compliant with the finalized policy to PY 2028 to provide States ample time to comply. We believe that this revised timeline will help mitigate a number of the operational and fiscal concerns raised by commenters, including by providing States additional time to conduct benefit-by-benefit analyses, engage with issuers and legislative bodies, secure any necessary
( printed page 29832)
appropriations for defrayal, and communicate with consumers and other interested parties regarding changes to benefit classifications.
We also understand that a small number of States and issuers have taken significant action based on current § 155.170 requirements, including that some States have sought or are seeking EHB-benchmark plan changes under § 156.111 to add certain State-required benefits as EHB based on the understanding that such EHB additions would be effective indefinitely absent any further EHB-benchmark plan changes under § 156.111 and that the cost of these additions would not require defrayal by the State. As finalized, any State-required benefit that fulfills the four conjunctive elements at § 155.170(a)(2)(i) through (iv) would require defrayal, regardless of whether the benefit is included in the State's EHB-benchmark plan.
We believe finalizing a delayed effective date of PY 2028 provides sufficient time for States to make these determinations and take any necessary action.
Comment:
One commenter urged HHS to withdraw the proposal, stating that finalization would impose significant financial and operational burden on States, including the burden of reappealing State mandated benefits, conducting benefit-by-benefit analysis on benefits that are “in addition to EHB”, and engaging with issuers on defrayal payment modifications. The commenter further stated concern that the proposed policy would cause significant consumer confusion and create extra work for State agencies and lawmakers.
Response:
We acknowledge the financial and operational implications associated with the proposed policy. However, we note that HHS has historically required States to conduct defrayal analyses for State mandated benefits under previous policy interpretations of § 155.170, and ensure a developed processes for operationalizing defrayal. We believe States are equipped and have the established infrastructure and experience to implement the financial and operational aspects of compliance with the finalized policy. We also note that the extended applicability date of PY 2028 is intended to provide States and issuers with sufficient time implement changes to benefit classifications, thereby reducing the potential for consumer confusion. Further, we intend to continue to engage with States and provide technical assistance as needed to ensure States understand when a State-benefit requirement is in addition to EHB and requires defrayal.
8. Mandating the HHS-Approved and -Created Consumer Consent Form—Eligibility Application Review and Documenting Receipt of Consumer Consent (§ 155.220(j))
As discussed in the preamble of this final rule, we are finalizing amendments to §§ 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review requirements and consent documentation requirements. We are finalizing this policy with a modification that it will be effective beginning with PY 2028 instead of PY 2027. Accordingly, we are also finalizing the redesignation of current § 155.220(j)(2)(ii)(A)(2) as § 155.220(j)(2)(ii)(A)(3) and current § 155.220(j)(2)(iii)(C) as § 155.220(j)(2)(iii)(D). We are also finalizing corresponding changes to §§ 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to state that current documentation policies for eligibility application and review and consent are effective until PY 2028. Our finalized policy will eliminate the current broad allowances for meeting these requirements. The language in the regulation will also be changed to clarify what types of actions constitute “taking an action” to meet the regulatory requirements. The goal of this policy is to reduce confusion among agents, brokers, and web-brokers on what constitutes compliant eligibility application review documentation and what constitutes compliant consumer consent by ensuring objective standards, which protects consumers ultimately. These provisions also greatly improve HHS' investigative abilities into agent, broker, and web-broker eligibility application review and consumer consent review by creating a clear and objective standard for all applications clearly outlining what HHS deems complaint.
Given this finalized policy will require the usage of the HHS-approved and -created consumer consent form, agents, brokers, and web-brokers who had previously relied exclusively on text messaging, or other non-HHS-approved and -created consumer consent form methods will be particularly impacted by this change. Importantly, the HHS-approved and -created consumer consent form guarantees and ensures all regulatory requirements are in the documentation provided to the consumer, as well as making documentation review of potentially noncompliant agents, brokers, and web-brokers more streamlined and efficient. The HHS-approved and -created consumer consent form [395]
we are finalizing to become standard also went through a readability analysis, which entails a review of language to help make text easier to understand, especially with documentation that may contain industry terms of art, such as healthcare. Requiring that agents, brokers, and web-brokers use the HHS-approved and -created consumer consent form will help ensure consumers are reviewing documentation that has been reviewed to be consumer-friendly but still contains the regulatory requirements. Agents, brokers, and web-brokers will still be able to provide consumers with more details than what is listed on the documentation and answer specific questions a consumer may have about a plan, policy, or the enrollment process.
As estimated in section IV.C of this final rule, the estimated annual cost of requiring agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review requirements and the consumer consent documentation requirements is $96,694,640, beginning in PY 2028.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and this final rule, we are finalizing these estimates with the modification to implement the policy effective PY 2028.
9. Misleading Marketing (§ 155.220(j)(3))
As discussed in the preamble of this final rule, the finalized regulatory amendments will create a new standards of conduct section in § 155.220(j) describing marketing requirements. These requirements will list certain prohibited practices, provide HHS audit authority, and put agents, brokers, and web-brokers on notice that they are responsible for marketing created by their downstream entities. This finalized policy will allow HHS to increase its efforts to engage in compliance actions for misleading marketing by providing agents, brokers, and web-brokers notice of the types of activities that are prohibited, allowing HHS to review marketing materials for compliance, and ensure agents, brokers, and web-brokers are not able to push responsibility to third-parties. Creating a
( printed page 29833)
marketing standards of conduct section is necessary to protect consumers and maintain the integrity of the Exchanges.
The finalized provisions will provide instructive language agents, brokers, and web-brokers may utilize when creating Exchange marketing materials. This will help ensure agents, brokers, and web-brokers are creating compliant marketing from the beginning and will not be subject to enforcement actions.
As estimated in section IV.D, the estimated total cost for the burden of responding to HHS regarding misleading marketing will be $1,392.96, beginning in 2027.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
10. Removal of the Vendor Program (§ 155.222)
As outlined in the preamble of this final rule, we are finalizing our proposal to remove the vendor program requirements established at § 155.222, that allow for certain training and information verification functions to be provided by HHS-approved vendors. Removing these requirements will permit HHS to discontinue the vendor program.
Considering the lack of utilization of this program by agents and brokers, as well as dwindling interest on the part of potential vendors, as outlined in the preamble, we do not anticipate potential vendors, nor agents and brokers, to be substantially impacted by these proposals. Agents and brokers will continue to have the ability to complete the annual training and information verification requirements through the MLMS at no cost.
This finalized policy will additionally save the government approximately $300,000 each plan year beginning in 2027 by removing the contractual costs required to facilitate the program.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
11. Limiting APTC Eligibility to “Eligible Noncitizens” (§§ 155.20, 155.305(f)(1), and 155.320)
We estimate that there are currently 1,227,000 individuals receiving APTC through Exchanges who are lawfully present noncitizens, but who are not “eligible noncitizens,” and will therefore become ineligible for APTC and income-based CSRs beginning in PY 2027 under section 71301 of the WFTC legislation. This estimate is based on evaluating internal FFE data regarding “eligible noncitizen” enrollees and extrapolating that data to estimate the size of the impacted population in State Exchanges. Based on average monthly APTC expenditures of $656.89 per person, we project that this population becoming ineligible for APTC will reduce annual APTC expenditures by $9,672,048,360 (1,227,000 enrollees × $656.89 average APTC × 12 months), beginning in 2027.
We also anticipate that this change will result in costs to State Exchanges and the Federal Government to update eligibility systems in accordance with this finalized policy. As discussed further in section IV.F of this final rule, in aggregate we estimate $15,810,185 in PY 2026 in estimated one-time costs for implementation ($193,990 Federal government + $678,965 Exchanges on the Federal platform + $14,937,230 State Exchanges). For the three States and DC currently approved to operate a BHP beginning in 2027, we estimate the annual ongoing cost to be $39,133.60.
As some noncitizens will no longer be eligible for PTCs under this new provision, there are also individuals for whom the Federal Government will not make a payment if enrolled in a BHP. In Table 25, we provide our projections of BHP enrollment and spending prior to the impacts of the WFTC legislation. We have updated these projections to include New York's BHP, which is scheduled to restart effective July 1, 2026.
In 2025, we estimate there were about 138,100 BHP enrollees in 2 States based on the quarterly enrollment estimates that States submit to CMS. With DC starting a BHP in 2026 and New York restarting its BHP July 1, 2026, we project that enrollment would have increased by 479 percent in 2026 and by 83 percent in 2027, prior to any of the changes made by legislation and described in this final rule. We project enrollment will decrease in 2028 by 7.7 percent to 1,348,200 due to other legislative changes, and increase by 0.4 percent to 1,353,100 in 2029 and remain at that level through 2030.
We also estimate that the current Federal BHP payment in 2025 is about $644 per member per month, based on payments the Federal Government has made to the 2 BHP States last year. We project that these will increase by 25 percent in 2026 and to decrease 0.5 percent in 2027, with an average monthly payment of $803 in 2027 prior to changes made by legislation. These trends are heavily influenced by the restart of New York's BHP, which accounts for the majority of BHP enrollees and spending, and has a relatively higher average BHP payment per person. We project payments will increase at an average rate of about 5.2 percent after 2027.
We estimate that this provision will affect about 1.6 percent of BHP enrollees
( printed page 29834)
starting in 2027. These estimates are based on analysis of citizenship and residence status of enrollees in the health insurance exchanges. To develop these estimates, we reviewed the number of eligible noncitizens receiving PTCs through the Exchanges in 2025 using the Multidimensional Insurance Data Analytics System (MIDAS) database. We found about 1.6 percent of all individuals receiving PTC were lawfully present noncitizens who would not be considered “eligible noncitizens” under this section of the legislation. We multiplied projected BHP enrollment by this percentage, and then we multiplied the enrollment change by the projected average per member per year Federal BHP costs to develop the expenditure amounts. This change will impact about 16,100 individuals in 2027, somewhat fewer in 2028 and then an increasing number of individuals through 2030. The changes will also reduce Federal spending by about $149 million in 2027 (real 2026 dollars), with a somewhat smaller effect in 2028 and then an increasing amount through 2030. These impacts after 2027 are largely influenced by the overall trends in BHP enrollment and spending. The annual estimates are shown in Table 26.
We sought comments on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy with the modifications made previously. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Several commenters claimed that the estimates were inaccurate and that the figures presented in the proposed rule did not match their attempt to reproduce the results.
Response:
We believe that differences between the commenters' results and the estimates presented in the proposed rule may reflect differences in methodology or assumptions used to reproduce the analysis. These differences may also reflect rounding (where the figures in the proposed rule were generally rounded to the nearest thousand enrollees or the nearest million dollars), as well as differences between nominal and real dollar estimates. In the interest of presenting this analysis more clearly, we have updated this section of the impact analysis. We have also rounded enrollment estimates to the nearest hundred in these figures. In addition, we have updated the estimates with more recent data on enrollment and per member per month costs. These changes had minimal effects on the overall estimates. We have also included the effects for New York, which is restarting its BHP on July 1, 2026, and that change resulted in larger impacts than shown in the proposed rule.
12. Prohibition of APTC for Individuals Who Are Ineligible for Medicaid Due to Their Immigration Status and Have Income Below 100 Percent of the FPL (§ 155.305(f)(2))
As described in the Collection of Information Requirements in section IV.G of this final rule, we estimate that implementing this finalized policy will require one-time costs for Exchanges to make technical updates to their eligibility systems totaling $4,316,278 ($242,488 for Exchanges on the Federal platform + $4,073,790 for State Exchanges) in PY 2025. We also estimate that this finalized policy will result in a reduction of the amount of DMIs with a total estimated annual reduction in burden for these information collection requirements of $24,126,144 ($16,341,600 for removal of MLP DMIs for Exchanges on the Federal platform + $4,575,648 for removal of AI DMIs for Exchanges on the Federal platform + $3,208,896 for removal of AI DMIs for State Exchanges), beginning in 2026.
As of the end of the Open Enrollment period for 2025, there were 237,125 enrollees who were part of the population of consumers with an annual household income of less than 100 percent of the FPL, who were also ineligible for Medicaid due to their immigration status and were enrolled in Marketplace coverage with APTC on the FFE. We estimate the average monthly value of that APTC was $656.89. Through this finalized policy and subsequent elimination of APTC across all exchanges, we estimate $1,869,180,495 (237,125 enrollees × $656.89 average APTC × 12 months) in APTC savings per year, beginning in PY 2026. We estimated the impact of section 71302, which no longer allows PTC during periods of Medicaid ineligibility on BHP enrollment and spending. Prior to the enactment of the WFTC legislation, some noncitizens would have been eligible for Medicaid on the basis of income and other criteria except for the 5-year waiting period for lawful permanent residents (LPRs) to be allowed to enroll in Medicaid. For those individuals, they would have instead been eligible for PTC through enrolling in a QHP on the health insurance exchanges assuming they met all other criteria. Similarly, those individuals would have been included in Federal BHP calculations in States that had elected to operate a BHP. Generally, these are individuals with household incomes up to 100 percent of the FPL.
Under section 71302 of the WFTC legislation, these individuals will no longer be eligible for PTC, and therefore the Federal Government will not make a payment for these individuals if enrolled in a BHP. We reviewed current BHP enrollment data based on the quarterly enrollment estimates, and we estimate that in 2026 about 223,000 BHP enrollees will no longer be eligible for PTC under this section, and thus there will not be BHP payments made for these enrollees. These projections have been updated since the proposed rule to include New York's BHP, which is scheduled to restart on July 1, 2026. From 2027 through 2030, we estimate the number of affected individuals will be between 400,000 and 440,000 annually. We project Federal spending will be lower by $2,522 million in 2026 (real 2026 dollars), and between $4,300 million and $4,700 million lower annually between 2027 and 2030. The annual estimates are shown in Table 27.
( printed page 29835)
We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy with the modifications made previously. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Several commenters claimed that the estimates were inaccurate and that the figures presented in the proposed rule did not match their attempt to reproduce the results.
Response:
We believe that differences between the commenters' results and the estimates presented in the proposed rule may reflect differences in methodology or assumptions used to reproduce the analysis. These differences may also reflect rounding (where the figures in the proposed rule were generally rounded to the nearest thousand enrollees or the nearest million dollars), as well as differences between nominal and real dollar estimates. In the interest of presenting this analysis more clearly, we have updated this section of the impact analysis. We have also rounded enrollment estimates to the nearest hundred in these figures. In addition, we have updated the estimates with more recent data on enrollment and per member per month costs. These changes had minimal effects on the estimates. We have also included the effects for New York, which is restarting its BHP on July 1, 2026, and that change resulted in larger impacts than shown in the proposed rule.
13. Failure To File and Reconcile (FTR) (§ 155.305(f)(4))
We are finalizing our proposal to amend paragraph § 155.305(f)(4) so that in PY 2028 and beyond, all Exchanges may not determine a tax filer or their enrollee eligible for APTC if: (1) HHS notifies the Exchange that APTC were paid on behalf of the tax filer, or their spouse if the tax filer is a married couple, for one year for which tax data would be utilized for verification of household and family size, and (2) the tax filer did not comply with the requirement to file a Federal income tax return and reconcile APTC for that year (referred to as the “1-tax year FTR” process). We also are finalizing that, at the option of the Exchange, an Exchange may choose to implement this policy earlier in PY 2027 if they have the resources and capability to adopt the 1-year FTR process or continue to follow the 2-year FTR process until PY 2028. Exchanges on the Federal platform intend to adopt the 1-year FTR process in PY 2027, as HHS has the resources possible to do so. To conform with this finalized policy, we further are finalizing our proposal to amend the notice requirement at § 155.305(f)(4)(iii), which is where the notice requirements have been reorganized. Our changes are aimed at addressing the notice messaging for tax filers who are at risk for losing APTC under a 1-year FTR policy, either for the Exchanges that adopt this option in PY 2027, and for all Exchanges in PY 2028. Exchanges operating under a 1-year FTR policy should use the more urgent language currently contained in the second-year notice of the 2-year FTR policy notices to accurately convey to tax filers or their enrollees that they are at imminent risk of losing APTC if they do not file and reconcile.
This provision will align with the WFTC legislation starting in PY 2028, but we additionally are finalizing that Exchanges can choose to implement this as early as PY 2027.
In light of the finalized policy changes for FY 2027 and beyond, we estimate that it will take the Federal Government and each State Exchange, if they choose to implement the 1-year FTR policy for PY 2027, instead of PY 2028 as required by the WFTC legislation, approximately 10,000 hours in 2026 to develop and code changes to the eligibility systems to evaluate and verify FTR status under the revised FTR process, such that enrollees are found to be FTR after 1 tax year of failing to file and reconcile their APTC. Of those approximately 10,000 hours, we estimate it will take a database and network administrator and architect 2,500 hours at $103.34 per hour and a computer programmer 7,500 hours at $94.88 per hour based on our prior experience with system changes. In aggregate for the State Exchanges, we estimate a one-time burden in 2026 of 200,000 hours (20 State Exchanges × 10,000 hours) at a cost of $19,399,000 (20 States × [(50,000 hours × $103.34 per hour) + (150,000 hours × $94.88 per hour)]) for completing the necessary updates to State Exchange eligibility systems in 2026, if State Exchanges implement the 1-year FTR process for PY 2027. If Exchanges choose to implement the 1-year FTR process for PY 2028, these estimated costs will be delayed by one year to 2027. For the Federal Government, we estimate a one-time burden in 2026 of 10,000 hours at a cost of $969,950 ((2,500 hours × $103.34 per hour) + (7,500 hours × $94.88 per hour)). In total, the burden associated with all system updates to revert back to the 1-year policy will be 210,000 hours at a cost of $20,368,950.
We also estimate that by switching to the 1-year policy from the current 2-year policy in PY 2028 or at the Exchange's option in PY 2027, the Federal Government will save APTC from the population of 1-year FTR consumers who would otherwise have retained APTC eligibility for an additional coverage year under the 2-year FTR policy. We estimate that total enrollment for the Exchanges will decrease by approximately 725,000 to 1,800,000 individuals in PY 2026 as compared to PY 2025 due to the expiration of the enhanced APTC subsidies, the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), and the WFTC legislation. The resulting reduction in Exchange enrollment from these law and policy changes, will also affect the total amount of expected households in FTR status. For PY 2025, the total FTR 1-year population dropped from almost 1.5 million households prior to Open Enrollment to less than 400,000 households during FTR Recheck. The total FTR 2-year population dropped from approximately 350,000 households prior to Open Enrollment, to approximately 300,000 households at FTR Recheck, and then after the final
( printed page 29836)
check of IRS data, HHS terminated APTC for approximately 200,000 households. Under our finalized 2028 1-year policy with the option to early adopt in 2027, we expect to remove APTC from all households still in an FTR status in our final Recheck. Based on historical FTR data and expectations for Exchange population size due to changes from the 2025 Marketplace Integrity and Affordability final rule, expiration of enhanced APTC subsidies, and the WFTC legislation, we expect that the total amount of households that lose APTC could be approximately 28,500 on the Federal Exchanges. While we do not have any data regarding the impact of the FTR process on consumers served by State Exchanges, the State Exchange population is approximately 46 percent of the total population of consumers served by Exchanges on the Federal platform. Extrapolating that proportion, it is possible that approximately 13,100 consumers on State Exchanges could lose APTC in PY 2028 for failing to file and reconcile, assuming all State Exchanges choose to wait to adopt the 1-year policy until 2028. This is the population that will otherwise retain their APTC in a 2-year policy during PY 2028. The annual savings generated by removing their APTC based on 8 months of enrollment and the average amount of APTC removed per household of $784 per month is approximately $179 million. Depending on how many Exchanges elect to adopt the 1-year FTR policy in PY 2027, the savings could be achieved as early as PY 2027, as the Exchanges on the Federal platform plan to early adopt the 1-year FTR policy.
For the purposes of this RIA, we assume the scenario that Exchanges will comply with the policy in PY 2028 to align with the WFTC legislation. We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
14. Income Verification When Data Sources Indicate Income Less Than 100 Percent of the FPL (§ 155.320(c)(3)(iii))
In this final rule, we are amending § 155.320(c)(3)(iii)(A) to indefinitely extend the requirement for applicants to submit documentation when they attest to income that would qualify the taxpayer as an applicable taxpayer per 26 CFR 1.36B-2(b), but trusted data sources show income below 100 percent of the FPL starting in 2027.
As discussed further in section IV.I of this final rule, we estimate an approximate annual increase in burden costs of $20.2 million for Exchanges using the Federal platform and $12.4 million for State Exchanges starting in 2027 to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes for applicants below 100 percent of the FPL. The implementation of this finalized policy will result in a one-time cost of $775,960 to Exchanges on the Federal platform and approximately $16.3 million total State Exchanges in 2026 to update the eligibility systems and perform other technical updates to implement the additional verification of an applicant's annual household income attestation when tax data is returned that is under 100 percent of the FPL while the household's annual income attestation is at or above 100 percent of the FPL. Finally, we estimate an increase in burden of approximately $13.7 million across all Exchanges in 2027 and annually onwards for consumers to submit documentation to fulfill income verification requirements. We recognize the burden the continuation of policy may place on State Exchanges, and we sought comment from these and other impacted interested parties to inform this decision.
While there would be additional annualized budget impacts of this policy on State Exchanges and the Federal Platform, there may be some savings associated with an anticipated reduction in APTC for consumers. Based on our analysis of enrollment data from DMI generation numbers from when this DMI was previously in place, we estimate creating DMIs that require additional verification will reduce the number of people who receive APTC annually by 50,000 for Exchanges on the Federal platform. We estimate the annual reduction of people who receive APTC in the State Exchanges to be 31,000. Using an estimated average four months reduced APTC and an average monthly APTC rate of $656.89 per person, we estimate total APTC expenditures will be reduced by approximately $213 million per year starting in 2027 for the period in which we maintain this policy (50,000 × $656.89 × 4 + 31,000 × $656.89 × 4).
We sought comment on these impact estimates and assumptions. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed. We summarize and respond to public comments received on the burden estimates of the proposed policy to perform further income verification processes when the IRS returns income that is below 100 percent FPL but an applicant's attested projected annual household income would consider them an applicable taxpayer according to 26 CFR 1.36B-2(b) for the plan year for which coverage is requested, and is more than a reasonable threshold above the annual household income, below.
Comment:
Many commenters stated concerns about the costs and burdens for this proposal on Exchanges. Commenters mentioned that they believe the proposal would increase administrative costs, and that this would result in having to divert funds from other important eligibility and enrollment operations to implement and maintain. Many also stated that State Exchanges do not currently have appropriated funds or other resources to implement this change and are especially concerned given the expected upcoming costs associated with upcoming changes from the WFTC legislation. Some commenters stated skepticism that this would result in a net gain in saved APTC, with one commenter mentioning how if a consumer ends up in Medicaid after their income DMI expires it does not save the government money.
Response:
We acknowledge the costs associated with implementing this proposal. We are confident that the Exchanges on the Federal platform can implement this proposal by the rule's effective date and are not concerned with implementation operations. Additionally, we believe that the costs associated with implementing and operating this policy are justified, as this is a critical program integrity measure to ensure consumers who may not be eligible for APTC are not erroneously receiving APTC throughout the entire plan year. Because of that, while we understand State Exchanges are concerned about the implementation and ongoing costs, including any upcoming changes due to the passing of the WFTC legislation, we believe that the program integrity gains outweigh the potential costs to State Exchanges. Finally, we emphasize that while some consumers may end up in Medicaid and therefore, result in costs associated with that instead of APTC, we believe that it is important that consumers end up in the correct coverage for the scenario.
15. Removal of the Requirement To Accept Attestations of Household Income When Tax Data Is Unavailable (§ 155.320(c)(5))
In this final rule, we are finalizing our proposal to remove § 155.320(c)(5), which will allow Exchanges to continue the income verification process when IRS is successfully contacted but IRS returns no data rather than accepting an
( printed page 29837)
applicant's annual household income attestation.
As further discussed in section IV.J of the final rule, we estimate an increase in annual burden costs of approximately $102.3 million for Exchanges on the Federal platform and approximately $62.8 million total for State Exchanges starting in 2027 to receive, review, and verify submitted verification documents as well as conduct outreach and determine DMI outcomes for applicants whose tax return data is unavailable. The implementation of this finalized policy will result in a one-time cost of $872,955 to Exchanges on the Federal platform and approximately $18.3 million total State Exchanges in 2026 to update the eligibility systems and perform other technical updates to implement the additional verification of an applicant's annual household income attestation when tax data is unavailable. As also further discussed in section IV.J of this final rule, we also estimate an increase in annual burden of $69,480,540 for consumers in 2027 and beyond to submit documentation to fulfill income verification requirements associated with this finalized provision.
Based on our analysis of enrollment data from DMI generation numbers from when this DMI was previously in place, as well as historical enrollment data, we estimate creating DMIs that require additional verification will result in a decrease in APTC, potentially to zero, for 252,000 enrollees for Exchanges on the Federal platform and 155,000 enrollees on State Exchanges each year. Using an estimated average 4 months reduced APTC, as estimated based on internal 2016-2020 APTC data, with an average monthly APTC rate of $656.89 per person, we anticipate that this change could result in an annual reduction of $1,069 million (252,000 × $656.89 × 4 + 155,000 × $656.89 × 4) in APTC expenditures starting in 2027. We accepted comments on whether this number may be slightly less because of potential decreased enrollment if the enhanced PTC are no longer in effect.
We sought comment on these impact estimates and assumptions.
For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed. We summarize and respond to public comments received on the burden estimates proposed policy later.
Comment:
Most commenters oppose this proposal, stating that it will create barriers for vulnerable consumers and increase administrative costs. Commenters also stated this could destabilize the risk pool because these changes could increase adverse selection because less healthy individuals have greater incentive to put in the time and effort necessary to resolve income verification issues.
Response:
We acknowledge commenters' concerns around administrative burden and risk pool impacts. We believe eligible applicants would likely have documentation to verify their household income as readily available to them as the standard tax filer without an income DMI. Although reintroducing income verification for applicants with no tax return data would increase the burden on some applicants, we do not anticipate this burden would deter many eligible people from enrolling. An accurate household income estimate is a critical program integrity element of the Affordable Care Act's framework for verifying and determining eligibility for APTC. We acknowledge the concerns about the impact of this proposal on the risk pool and the agree about the importance of maintaining a healthy risk pool. However, we emphasize that having people improperly enrolled, especially for many without their knowledge, does not improve the risk pool. We believe that the positive impact to program integrity will outweigh any negative impacts.
16. Premium Payment Threshold (§ 155.400)
We are finalizing modifications to § 155.400(g) to remove paragraphs (2) and (3), which establish an option for issuers to implement a fixed-dollar and/or gross percentage-based premium payment threshold (if the issuer has not also adopted a net percentage-based premium threshold) beginning in the 2027 coverage year. Permanently removing the options for issuers to implement either a fixed-dollar and/or gross percentage will continue to help strengthen program integrity by ensuring that enrollees cannot remain enrolled in coverage for extended periods of time without paying any premium, increasing the likelihood that consumers who were improperly enrolled become aware of their enrollment.
We do not anticipate that there will be any costs for issuers going forward since issuers were not able to implement these thresholds in PY 2026 per the 2025 Marketplace Integrity and Affordability final rule (90 FR 27133), and we are extending this policy permanently in this final rule.
While we did not initially provide these estimates in the proposed rule, we did not receive any response to the proposed impact estimates for this policy when they were previously proposed in the 2025 Marketplace Integrity and Affordability rule (90 FR 27202). For the reasons outlined in this final rule, we are finalizing these estimates.
17. Extend the Removal of the 150 Percent FPL SEP Beyond Plan Year 2026 (§ 155.420)
We are finalizing our proposal to no longer “sunset” the prohibition on Exchanges offering the 150 percent FPL SEP, in alignment with section 71304 of the WFTC legislation. As explained in preamble in section III.D.15 of this final rule, section 71304 of the WFTC legislation prohibits APTC for plans enrolled in through the 150 percent FPL SEP, and therefore eliminates the SEP's ability to facilitate access to affordable coverage. We are therefore finalizing our proposal to no longer permit Exchanges to offer the 150 percent FPL SEP.
In the proposed rule, we stated that absent the WFTC legislation, and assuming that the prohibition on Exchanges offering the 150 percent FPL SEP had “sunset” on December 31, 2026, we assume that all Exchanges would have elected to begin offering the 150 percent FPL SEP again in PY 2027 (91 FR 6451). We stated that this assumption is based on past experience with the overwhelming majority of Exchanges choosing to offer this SEP. If all Exchanges offered the 150 percent FPL SEP beginning in PY 2027, we assumed that this would result in increased adverse selection, which will result in increases to premiums and APTC expenditures. As a result, we estimated that the proposed policy would reduce premiums by 3 to 4 percent, as a result of improvements to the risk pool as the removal of the SEP would limit consumers' ability to wait until they need services to enroll in coverage. We estimated that the reduced premiums would have resulted in an overall decrease in APTC expenditures of $3.4 to $4.5 billion per year, beginning in PY 2027. For the purposes of the RIA in the proposed rule, we used $3.8 billion as the estimated annual decrease in APTC expenditures, beginning in PY 2027.
We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates with the following modifications. We have reduced the estimated premium impact of this policy to 2 to 3 percent resulting in a decrease in APTC expenditures of $2.5 to $3.6 billion per year. For the purposes of the RIA, we used $3.1 billion as the estimated annual decrease
( printed page 29838)
in APTC expenditures, beginning in PY 2027. The previous estimates assumed a lack of program integrity would lead to abuse of this policy and create an environment where almost anyone could use this SEP to obtain coverage after becoming sick. We summarize and respond to public comments received on the proposed estimates below.
Comment:
Some commenters disputed the estimate that the elimination of the 150 percent FPL SEP would result in a 3 to 4 percent decrease in premiums. Commenters cited that section 71304 of the WFTC legislation, which was effective January 1, 2026, disallows individuals who enroll through an income-based SEP from accessing APTC. Because of this, commenters believe that the purported adverse selection effects of allowing Exchanges to offer the 150 percent FPL SEP were overstated. This is because even if HHS were to maintain its current regulatory posture and permit Exchanges to offer the SEP again beginning in PY 2027, section 71304 of the WFTC legislation prohibits enrollees using the SEP from accessing APTC. Enrollees utilizing the SEP would therefore be much less likely to be able to afford to enroll, and as a result, changing HHS' regulatory posture to prohibit the 150 percent FPL SEP would not have a significant impact on the risk pool or premiums.
Response:
We acknowledge that, if we were to permit Exchanges to offer the 150 percent FPL SEP, section 71304 of the WFTC legislation makes it much less likely that individuals would use the SEP to enroll, given that section 71304 prohibits APTC for their coverage. While affordability makes it less likely healthier individuals would enroll, it does not prevent adverse selection, as the cost of health insurance can be less expensive for individuals that become sick. We do agree the previous impact of 3 to 4 percent assumed a lack of program integrity that would allow for greater abuse of this SEP, so we have revised the impact to a 2 to 3 percent decrease in premiums.
Comment:
Some commenters disputed the estimate that the elimination of the 150 percent FPL SEP would result in a 3 to 4 percent decrease in premiums, given that section 71304 of the WFTC legislation eliminated the 150 percent FPL SEP. One commenter stated that HHS had advised Exchanges that section 71304 of the WFTC legislation was self-executing.
Response:
We clarify that section 71304 of the WFTC legislation does not prohibit Exchanges from offering income-based SEPs, including the 150 percent FPL SEP. Rather, it prohibits the availability of PTC, and therefore of APTC and CSRs, for individuals who enroll through such SEPs. We also clarify that we did not advise Exchanges that section 71304 of the WFTC legislation was self-executing; rather, we regulated to remove Exchanges' ability to provide the 150 percent FPL SEP in the Marketplace Affordability and Integrity Rule (90 FR 27074), which was finalized prior to the passage of the WFTC legislation.
18. Pre-Enrollment Special Enrollment Period Verification (§ 155.420(g))
In this final rule, we are finalizing the provision to allow Exchanges on the Federal Platform to continue to conduct pre-enrollment verification for SEPs other than Loss of Minimum Essential coverage and add the requirement that Exchanges on the Federal Platform conduct pre-enrollment verification for at least 75 percent of new enrollments.
We anticipate that revisions to § 155.420 will have a positive impact on program integrity by verifying eligibility for SEPs. Increasing program integrity through continuing this policy will reduce improper subsidy payments and could contribute to keeping premiums low and therefore, further protecting taxpayer dollars. This policy may deter enrollments among younger people at higher rates, which could worsen the risk pool and increase premiums. However, we expect any such deterrence will impact a very small number of young people and, therefore, have only a minimal impact on the risk pool and premiums. We estimate that the net effect of pre-enrollment verification will reduce premiums by approximately 0.5-0.8 percent and will maintain the reduction in APTC spending of approximately $105.4 million, beginning in PY 2027.[396]
We anticipate this policy will moderately increase the regulatory burden on Exchanges using the Federal platform. Based on past experience, we estimate that maintaining the expansion in pre-enrollment verification to most individuals seeking to enroll in coverage through all applicable SEPs offered through Exchanges on the Federal platform will result in an additional 293,073 individuals having their enrollment delayed or “pended” annually until eligibility verification is completed, although for the vast majority of individuals the delays would be less than 1-3 days. As mentioned in section IV.K of this final rule, we anticipate that maintaining the expansion of SEP verification will result in increased inconsistencies, with an associated cost increase for consumers of approximately $7,332,686 beginning in 2027. There will also be an increase in ongoing costs for Exchanges on the Federal platform due to an increase in the number of SEP enrollments for which they must conduct verification. We estimate that the total increase in ongoing processing costs to maintain compliance with this requirement for the FFE will be approximately $11.7 million annually (293,073 additional SVI × $40 cost per SVI). Furthermore, as mentioned in section IV.K, we anticipate that expanding verification will result in an increase in annual burden of labor costs on Exchanges on the Federal platform at a cost of $2,902,615 annually.
We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these burden estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Several commenters stated concern that expanding SEPV would increase the burden on Exchanges using the Federal platform, which could potentially result in delayed coverage and discourage enrollment. Commenters also stated that the proposed estimates did not account for additional expenditures related to consumer communications, outreach, and assister training.
Response:
We agree that expanding SEPV will increase the burden on Exchanges using the Federal platform. Our estimates are based on historical data from the FFE, and we anticipate that the expansion of SEPV will result in an increase in annual labor burden on Exchanges using the Federal platform at an estimated cost of $2,902,615 annually.
19. Expansion of Hardship Exemption Eligibility (§ 155.605(d)(1))
This final rule amends § 155.605(d)(1) to codify and expand hardship exemption eligibility to individuals who are ineligible for APTC or CSRs due to projected household income (below 100 percent or above 250 percent of the FPL). This expansion will allow these individuals to qualify for catastrophic coverage under section 1302(e) of the Affordable Care Act.
( printed page 29839)
Most State Exchanges currently delegate hardship exemption processing to HHS. However, four State Exchanges—California, Connecticut, Maryland, and the District of Columbia—currently process their own exemptions. Following HHS guidance published on September 4, 2025, this policy expansion has been implemented for consumers in all States that currently delegate exemption processing to HHS. This final rule will extend the same hardship exemption eligibility to consumers in the four State Exchanges that currently process their own exemptions, ensuring that consumers in all States have access to affordable coverage.
We assume the four State Exchanges that process their own exemptions will experience an administrative burden associated with processing hardship exemption applications under the expanded eligibility criteria. Based on previous experience, we estimate that Exchange staff will require approximately 19 minutes (0.32 hours) to review and process each hardship exemption application. Using the median hourly wage of $24.76 for Eligibility Interviewers, Government Programs (occupation code 43-4061), and adjusting for fringe benefits and overhead, we calculate an adjusted hourly wage of $49.52. Based on these figures, we estimate the cost per application to be $15.75, calculated as follows: (19 minutes ÷ 60 minutes) × $49.52/hour = $15.75 per application.
Based on our analysis of operational FFE data regarding existing hardship exemption requirements and the new requirement finalized in this rule, we estimate these four State Exchanges will collectively process approximately 1,072 applications annually under the expanded hardship exemption eligibility criteria when considering their combined share of approximately 10 percent of total Exchange enrollment.
Using the per-application manual processing cost of $15.75, we estimate the total annual cost burden for these four State Exchanges in total to be approximately $16,884 (1,072 applications × $15.75 per application). Individual State burden will vary depending on each State Exchange's enrollment volume and the proportion of consumers who fall into the expanded hardship exemption category. States with larger enrollment volumes and higher proportions of consumers with income below 100 percent FPL or above 250 percent FPL may experience higher application volumes than States with smaller enrollment or different demographic characteristics.
We note that the actual burden may be lower over time than estimated if State Exchanges implement automated exemption processing similar to the FFE's system. The FFE experience demonstrates that automated processing significantly reduces the need for manual paper application review, as the system automatically grants hardship exemptions for consumers ineligible for APTC due to income when they apply for catastrophic coverage. State Exchanges that adopt similar automated systems will experience reduced administrative burden while ensuring consumers have seamless access to hardship exemptions and catastrophic coverage.
To estimate the cost of developing an automated exemption processing system, we analyzed personnel and time requirements across three major phases: system development, testing and quality assurance, implementation and training. The hour estimates presented later are illustrative examples intended to demonstrate the general magnitude of costs that might be associated with automated system development.
We estimate that Computer Systems Analysts will need approximately 400 hours at an adjusted hourly wage of $99.80, resulting in a cost of $39,920. Computer Programmers will require the most substantial time investment, with an estimated 600 hours at an adjusted rate of $94.88 per hour, totaling $56,928. Database and Network Administrators will need approximately 200 hours at $103.34 per hour to configure the necessary data infrastructure and system architecture, costing $20,668. A Project Manager will oversee the development effort for approximately 160 hours at $96.88 per hour, adding $15,501 to the total. The combined system development cost will be approximately $133,017, requiring 1,360 total staff hours.
Following initial development, the system will require comprehensive testing to ensure accuracy, compliance with Federal regulations, and proper integration with existing Exchange systems. Computer Systems Analysts will conduct approximately 120 hours of testing at $99.80 per hour, costing $11,976. Compliance Officers will review the system for regulatory compliance for approximately 80 hours at $75.40 per hour, adding $6,032. The total testing and quality assurance cost will be approximately $18,008, requiring 200 staff hours.
The final phase will involve deploying the automated system and training staff on any residual manual processes or system monitoring requirements. Management Analysts will coordinate the implementation for approximately 80 hours at $97.30 per hour, costing $7,784. Eligibility Interviewers will require approximately 40 hours of training at $49.52 per hour to understand the new automated processes and handle any exceptions, totaling $1,981. The implementation and training phase will cost approximately $9,765, requiring 120 staff hours.
Combining all three phases, the total estimated one-time cost in PY 2026 to develop an automated exemption processing system will be approximately $160,790, so in total $643,160 for four State Exchanges. This estimate represents 1,680 total staff hours across multiple occupational categories and assumes a standard development timeline and complexity level.
We recognize that this cost estimate could vary significantly depending on several factors. States with more modern and flexible existing system infrastructure may experience lower development costs due to easier integration. Conversely, States with legacy systems may face higher costs. State-specific requirements, customizations, or additional compliance considerations could also increase costs.
We sought comment on these burden estimates, including the estimated number of applications, time required for consumers to complete applications, and time required for Exchanges to process applications. We also sought comment on opportunities to further reduce burden through automation or other streamlined processes.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in this final rule, we are finalizing these estimates as proposed.
20. Modification of Exchange Network Adequacy Standards (§ 155.1050)
We are finalizing our proposal to amend § 155.1050(a)(2) to eliminate the requirements under § 155.1050(a)(2)(i) and (ii) for State Exchanges and SBE-FPs to establish and impose quantitative time and distance network adequacy standards for QHPs that are at least as stringent as standards for QHPs participating on the FFEs under § 156.230; instead, we will require that State Exchanges and SBE-FPs ensure that each QHP provides sufficient access to providers in a manner that meets applicable standards specified in § 156.230(a)(1)(ii) and (a)(1)(iii) for network plans, or, for plan years beginning on or after January 1, 2027, § 156.236(a) for non-network plans if
( printed page 29840)
such plans are allowed to be offered through the Exchange, as applicable. State Exchanges and SBE-FPs have traditionally managed their respective network adequacy reviews, and many State Exchanges and SBE-FPs demonstrated to HHS that they have robust network adequacy standards and reviews in place beyond the requirements specified in § 155.1050(a)(2)(i) or were determined to have standards and reviews in place that satisfied the exception described at § 155.1050(a)(2)(ii). We recognize that State Exchanges and SBE-FPs are often best positioned to evaluate local provider networks and market conditions.
We anticipate this finalized policy will maintain the regulatory burden on the 22 State Exchanges and 1 SBE-FP we expect for PY 2027, providing them with more flexibility to regulate and review for network adequacy in a manner that best protects their respective consumers. We estimate this impact to be $1,560,780 beginning in PY 2027, as outlined in section IV.M of this final rule. We anticipate this provision might increase the administrative burden on issuers that operate in multiple States as they navigate varying regulatory frameworks and standards. The impact to consumers is not known at this time but there is a risk of potential decreased access to care for consumers if those State standards and their reviews are less consumer protective than the Federal network adequacy review framework.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed rule, we are finalizing these estimates as proposed.
21. General Program Integrity and Oversight Requirements (§ 155.1200)
We are finalizing our proposal to amend § 155.1200(d) to reduce duplication between the SEIPM program described in subpart Q and the annual independent external programmatic audit requirements and standards described at § 155.1200(c) and (d). We are finalizing our proposal to add § 155.1200(e) to permit a State Exchange to satisfy certain annual independent external programmatic audit requirements, as described at § 155.1200(d), by completing the proposed required annual SEIPM program process. As a result, we estimate that there will be a general burden reduction for State Exchanges related to the programmatic audit requirement under § 155.1200(c). In particular, the current 22 State Exchanges that operate their own eligibility and enrollment platforms will incur lower costs for contracts with independent external auditors, since many requirements under subparts D and E will be addressed through completion of the SEIPM process for the applicable benefit year.
Based on industry estimates of the average cost of contracting an auditor to perform an independent external programmatic audit, HHS projects that the reduced audit scope would lower annual costs by approximately 30 percent or $45,000 for each State Exchange. This is based on an estimated average annual programmatic audit cost of approximately $150,000 for a medium-size State Exchange. We anticipate the total cost annual reduction across 22 State Exchanges will be approximately $990,000 and expect that these savings could begin as early as 2027, coinciding with the submission of independent external audits for the PY 2026 SMART. However, this change would also introduce a new burden associated with completing the SEIPM and the related CAP process, as discussed in the section later. For an estimate of the burden created under SEIPM, please refer to section V.C.22.
We requested comment on the reduction in burden and specifically sought feedback from State Exchanges regarding the annual cost of the programmatic audit process.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
22. State Exchange Improper Payment Measurement (§§ 155.1600 Through 155.1650)
This policy will allow HHS to implement the Payment Integrity Information Act of 2019 (PIIA) requirements for State Exchanges. As described in the preamble earlier in this final rule, the PIIA requires that agencies measure the improper payments rate for programs susceptible to significant improper payments. HHS already undertakes annual measurements for Medicare, Medicaid, FFEs, and SBE-FPs. This final rule lays the groundwork to complete the Exchanges' measurement program by including State Exchanges and to enable HHS to estimate a comprehensive APTC improper payment rate as mandated by statute.
This policy will allow HHS to measure improper payments that are resultant from State Exchange operations related to the determination of eligibility and payment amounts for APTC and will require State Exchanges to provide Corrective Action Plans responsive to the findings of the measurement. Even slight decreases in this rate will accrue large taxpayer savings. To delineate the range of estimated burden across the State Exchanges, cost estimates were created at the State Exchange level using an average cost per sample of $499. State Exchanges with proportionally smaller amounts of APTC are planned to produce a sample size of 50 while the largest States are planned to produce a sample size of 250. Using these numbers multiplied by the average cost estimate per sample of $499, the SEIPM will incur a range of approximately $24,950.00-$124,750.00 in costs per respondent. As stated in the Information Collection in IV.O, the total costs for the State Exchanges to produce the information and to undergo the review process is estimated to be $1,097,800. Additionally, State Exchanges will incur a cost to develop and submit a corrective action plan (CAP) to HHS following an SEIPM cycle beginning in 2029. We estimate that it will take each State Exchange up to 1,000 hours or $97,300 to develop a CAP. We estimate that the total annual burden associated with this requirement for up to 22 State Exchange respondents will be up to 22,000 hours and $2,140,600. The burden related to this information collection will be submitted to OMB for approval after future rulemaking has been completed regarding the CAP process and requirements.
Additionally, we estimate that six Full Time Equivalents (FTEs) will be necessary to complete the activities associated with SEIPM and SEIPM contract management. This estimate is based upon our experience with staffing the Improper Payment Pre-Testing and Assessment (IPPTA) which has been operationalized in a similar manner and format as will be the SEIPM. The estimated annual cost per Full-Time Equivalent (FTE) is $376,075. This figure was derived by identifying the maximum salary for a Federal employee on the general pay table in the Baltimore area, which was $183,500 in 2023. To ensure conservative budgeting and sufficient funding, this salary was used as the base. The base salary was then multiplied by a factor of two to account for employee fringe benefits and overhead costs. Consequently, the total annual estimate per FTE is $376,075, leading to an aggregate annual cost of $2,256,450 for all FTEs.
( printed page 29841)
Finally, we anticipate total estimated annual contracting costs of $19.5 million incurred by HHS. These costs include but are not limited to: collecting the information from the State Exchanges, building and completing automated review systems, creating the statistical methodology and identifying the sample, appeal adjudication, estimating the improper payment rate, generating required reports, and IT support and infrastructure costs.
In summary, we expect total annual costs incurred across the State Exchanges to being $3.2 million, total HHS contracting costs to being $19.5 million, and total HHS staffing costs to being $2.3 million for a total cost of $24.8 million annually.
We believe that the potential benefits of this regulatory action justify the present costs. We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Some commenters stated the proposal does not accurately estimate the hours, costs, procedural requirements, and the hiring of additional full-time staff needed to complete SEIPM. Some commenters stated concern with operational and staff burden to complete data and documentation submission activities. One commenter stated that the proposed alternative data collection solution will still require significant mapping, validation, and reconciliation.
Response:
We appreciate these comments and recognize the operational and financial costs that will be incurred as a result of SEIPM activities. SEIPM addresses a critical gap in HHS' ability to comply with the Payment Integrity Information Act of 2019 (PIIA). Under PIIA, HHS is required to produce reliable and statistically valid estimates of improper payments and report those estimates through the Agency Financial Report (AFR). We believe that the long-term benefits of improved program integrity, including identification and reduction of improper payments, justify the associated operational investment. We acknowledge the incurred operational and financial burden by the State Exchanges and intend to provide ongoing technical support and additional operational information through sub-regulatory guidance to support State Exchange planning and preparation.
We conducted a comprehensive analysis to identify specific personnel roles and time requirements across all phases of the data collection process. We used the GSA labor category table to estimate burden on key occupational roles that we considered crucial in SEIPM while also using some of the early survey data provided by State Exchanges in Group A. While we received some burden data from a couple of commenters, we did not receive information across all State Exchanges. We noted that some States during IPPTA were able to provide the required information with minimal challenges.
While some commenters stated that significant time and resources were required for IPPTA, we understand that there is variability across each State in terms of how much time and resources are required. The processes such as developing SQL scripts that were completed during IPPTA are intended to translate into the SEIPM process. The time and resources spent for developing those scripts and troubleshooting the output would not be experienced in SEIPM because the work will already have been completed. We also clarify that we will allow flexibility in the data submission process to alleviate some of the administrative burden placed on the State Exchanges. We also intend to release sub-regulatory guidance to provide further details on SEIPM. For these reasons, HHS believes that the proposed estimations are sufficient for the State Exchanges to complete SEIPM. Accordingly, we are finalizing § 155.1600 as proposed.
23. FFE and SBE-FP User Fees (§ 156.50)
We are finalizing an FFE user fee rate of 1.9 percent of premiums for the 2027 benefit year, which is less than the 2.5 percent FFE user fee rate finalized for the 2026 benefit year. We are also finalizing an SBE-FP user fee rate of 1.5 percent of premiums for the 2027 benefit year, which is less than the 2.0 percent SBE-FP user fee rate we finalized for the 2026 benefit year.
Because we are decreasing the FFE and SBE-FP user fee rates for the 2027 benefit year from the current 2026 benefit year rates, we are estimating that this reduction in FFE and SBE-FP user fee rates will reduce transfers from issuers to the Federal Government by approximately $130 million for benefit year 2027 compared to the prior benefit year. We expect that available user fee collections will be sufficient to fund Exchange operations through 2027 at the finalized 2027 benefit year user fee rates.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy.
For the reasons outlined in the proposed rule and this final rule, we are finalizing these estimates as described in this section.
24. Provision of EHB (§ 156.115(d))
We are finalizing our proposal to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB. We do not anticipate any immediate costs to the Federal Government, States, issuers, or enrollees because of this finalized policy. This finalized policy will once again prohibit issuers from covering routine non-pediatric dental services as an EHB, which avoids the potential imposition of premium increases associated with these services. However, we do not expect that the removal of routine non-pediatric dental services as an EHB will have a significant impact on premium reduction, as all benefits a State adds to their EHB-benchmark plan are subject to the typicality standard at § 156.111(b)(2)(ii), which limits how generous the updated plan would be. For example, if a State added routine non-pediatric dental services as an EHB under the existing policy, as we explained in the 2025 Payment Notice final rule (89 FR 26348), they may have needed to consider removing and/or adjusting other benefits to make room for the non-pediatric dental services to ensure the scope of benefits falls within the typicality range.
Additionally, this finalized change only has a premium impact to the extent States already updated their EHB-benchmark plans to include routine non-pediatric dental services under the policy finalized in the 2025 Payment Notice that allows States to add routine non-pediatric dental services as an EHB beginning with PY 2027. Since no State has taken this action, this finalized policy has no premium impact. Finalized as proposed, this policy to prohibit coverage of routine non-pediatric dental services as an EHB will be effective upon the effective date of this final rule, preventing any future premium impact from the former policy.
Consistent with our note in the 2025 Payment Notice final rule (89 FR 26409), which acknowledged that removing the prohibition on routine non-pediatric dental services as an EHB may increase costs for issuers who may need to expand their networks to cover these services, this policy may avoid cost increases for issuers that would have needed to expand their networks
( printed page 29842)
to cover these new required services, although issuers could have contracted with a dental vendor to administer the routine non-pediatric dental EHB if such a benefit was adopted by a State as an EHB. As we also noted in the 2025 Payment Notice final rule, the size of non-pediatric dental networks varies by State, therefore, some States would have been affected by the need to build a new network of dental providers (or contract with dental vendors) more than others. Therefore, by reinstating the prohibition at § 156.115(d), this policy will avoid these potential network expansion costs.
While this finalized policy may limit potential premium increases for enrollees and cost increases for issuers related to network expansion, we acknowledge that this policy may impact long-term health outcomes and associated medical costs. As we explained in the proposed 2025 Payment Notice (88 FR 82597-98), oral health and overall health are inextricably linked; untreated oral health conditions can increase risk for and complicate the management of chronic conditions.[397]
As we also noted in the 2025 Payment Notice final rule (89 FR 26348), improving access to non-pediatric dental services would reduce health care costs by yielding downstream savings in overall health care expenditures and reducing costly emergency room department visits for dental care. However, as we mentioned in preamble of this final rule, we clarify that this prohibition on including routine non-pediatric dental services as an EHB does not prevent States from addressing non-pediatric oral health and overall health outcomes—and associated medical costs—through alternative policy mechanisms. For example, as we mentioned earlier in this final rule, States could mandate coverage of routine non-pediatric dental services as a non-EHB and defray the cost associated with that benefit. We believe ensuring better alignment of the regulatory requirements at § 156.115(d) with section 1302(b)(2)(A) of the Affordable Care Act regarding the EHB typicality standard outweighs these other policy considerations.
We solicited comment on the impact of our proposal to revise § 156.115(d) to prohibit issuers from including routine non-pediatric dental services as an EHB and whether other impacts should be considered.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy as proposed. We summarize and respond to public comments received on the proposed estimates below.
Comment:
Several commenters stated concerns regarding the downstream cost impacts of this proposal, particularly in regard to increased emergency department (ED) visits as a result of a lack of dental coverage and access to preventative care. At least one commenter urged CMS before implementing this proposal to consider how reinstating the prohibition of non-pediatric dental in EHB will impact local communities and shift costs to States. As an example, one commenter explained that data shows the long-term impact of the elimination of Medicaid adult dental benefits has been increased costs to States and overburdened local health care systems when individuals without access to dental coverage resort to ED visits to receive treatment for non-traumatic dental conditions (NTDC).[398]
This commenter cited data showing that ED visits for NTDCs cost States $3.9 billion in 2022, driven by a 29 percent increase in the mean cost of an ED visit for dental conditions, which was significantly higher than the average cost of a dental visit.[399]
This commenter also noted that increased costs are especially pronounced for individuals managing chronic conditions such as diabetes and coronary artery disease, and that the long-term impact of eliminating adult dental coverage has historically been increased costs to States and overburdened local health care systems.
Response:
We appreciate commenters' concerns regarding downstream cost impacts and cost-shifting to States. We recognize that oral health and overall health are inextricably linked. However, as we noted in the preamble, this prohibition does not prevent States from addressing non-pediatric oral health outcomes and associated costs through alternative policy mechanisms, including mandating coverage of routine non-pediatric dental services as a non-EHB benefit and defraying the associated costs. Additionally, as we noted previously, since no State has updated its EHB benchmark plan to include routine non-pediatric dental services under the policy finalized in the 2025 Payment Notice, this finalized policy has no immediate premium or cost impact. We believe that achieving better alignment with section 1302(b)(2)(A) of the Affordable Care Act regarding the EHB typicality standard outweighs these other policy considerations.
25. Multi-Year Terms for Catastrophic Plans To Improve Health (§§ 156.130 and 156.155)
Under current regulations, catastrophic plans, like all QHPs offered through the Exchanges, have annual contract periods that require re-enrollment each year during the open enrollment period. The finalized regulation will provide consumers who are eligible for catastrophic coverage with the potential of more predictable multi-year coverage arrangements, with a term of multiple consecutive plan years not to exceed 10 years, compared to annual re-enrollment, though premiums may be adjusted during the contract term in accordance with applicable requirements. As finalized, other than the fact that a multi-year catastrophic plan could have a term of up to 10 consecutive plan years for individuals who qualify for such plans upon enrollment, and coverage could be provided before the deductible is met for certain VBID benefits to be specified in future guidance, there would be no material differences between the regulatory requirements for such plans and 1-year catastrophic plans. This may potentially reduce premium volatility and administrative burden while maintaining the EHB and consumer protections required under the Affordable Care Act. This finalized policy aims to enhance market stability for a segment of consumers who may benefit from longer-term coverage arrangements. The finalized regulation will be effective for plan years and policy years beginning on or after January 1, 2027.
We sought comments on issuer participation, State and State Exchange operational impacts, and market segmentation effects.
The finalized regulation is anticipated to deliver benefits for eligible consumers and participating issuers. Consumers who enroll in multi-year catastrophic plans may benefit from more predictable multi-year coverage, with a term of multiple consecutive plan years not to exceed 10 years, reduced need to navigate annual open
( printed page 29843)
enrollment periods, and decreased risk of coverage gaps due to missed enrollment deadlines. Issuers offering multi-year catastrophic plans may experience reduced administrative burden associated with annual re-enrollment activities and lower operational expenses related to annual plan document preparation and filing. The extended contract periods may also promote continuous coverage among individuals. Even though premiums may be adjusted during the contract term in accordance with applicable requirements, issuers may price plans conservatively to account for uncertainty, potentially resulting in higher initial premiums. Additionally, there is uncertainty about how multi-year catastrophic plans might affect risk selection, including whether healthier individuals would disproportionately select multi-year plans. We note that there is currently no available evidence on these potential effects and data that could help understand the potential unintended consequences.
Issuers may incur costs related to developing multi-year catastrophic plans, such as developing new pricing models. States and the Federal Government will face costs associated with reviewing and approving multi-year catastrophic plan filings. We sought comments on costs and data that could be used to quantify these impacts.
The availability of multi-year catastrophic plans may result in transfer effects impacting consumers, issuers, States, and the Federal Government, with the magnitude dependent on uptake rates. We sought comments on transfer effects, premium impacts, Federal PTC expenditures, and data that could be used to quantify these impacts.
Given that this will be a new option for consumers, there is uncertainty regarding consumer demand for multi-year catastrophic plans. There is also uncertainty regarding how premiums will be structured for multi-year catastrophic plans, including the methodology and frequency of adjustments (such as annual adjustments tied to inflation or other factors) permitted under applicable requirements. Additionally, there is uncertainty about how consumers enrolled in multi-year catastrophic plans will respond if their health status changes and what implications this may have for consumers. We sought comment on these uncertainties and requested data that could help quantify the potential impacts of multi-year catastrophic plans on enrollment patterns, premium levels, and Federal expenditures.
As discussed in section III.E.6. of this final rule, after consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing this policy with the following modifications. We are finalizing § 156.155(a)(6) with minor revisions to refer to “plan years” instead of “years” for greater clarity and precision. We are also finalizing § 156.155(a)(6) to state that multi-year catastrophic plans may utilize value-based insurance designs to provide benefits before reaching the deductible, under guidelines issued by the Departments. We are also finalizing a conforming amendment at § 156.155(a)(3), providing that catastrophic plans provide no benefits before the annual limitation on cost sharing is reached, except as provided in paragraph (a)(6). We are not finalizing the proposed conforming amendments to § 156.155(a)(1), as multi-year catastrophic plans, like other catastrophic plans, must meet all applicable requirements for health insurance coverage in the individual market. We are not finalizing the proposed addition of § 156.130(c) which provided that in the case of a multi-year catastrophic plan, the annual limitation on cost sharing for the initial plan year of the contract may apply on an annual basis, or on average over the life of the contract. We summarize and respond to public comments received on the proposed impact estimates for this policy later.
Comment:
A few commenters supported the proposal, contending that multi-year catastrophic plans could create lower-premium or more predictable coverage options for people who are not well served by current offerings, reduce churn, improve continuity, expand HSA use, and strengthen incentives for issuers to invest in preventive care and other long-run health management activities. A few of these commenters also viewed added flexibility for pre-deductible preventive services as a meaningful improvement over current catastrophic plan design. Several commenters contended that the proposal's claimed benefits are either unproven or unlikely to materialize in the individual market. These commenters stated that multi-year catastrophic plans would not meaningfully reduce churn, lower premiums, or reduce administrative burden, particularly once new pricing, oversight, and systems costs are taken into account. Some commenters noted that the RIA does not treat premium reductions, administrative savings, or improved long-term health outcomes as quantified results; rather, it identifies them as potential effects and these commenters noted that they believed this approach to be appropriate given the novelty of the product type but did not provide any specific usable data.
Response:
We appreciate the comments received on this topic. We acknowledge commenters who noted that multi-year catastrophic products could improve continuity of coverage, reduce repeated enrollment friction, and better align issuer incentives with long-term prevention and care management. As discussed in section III.E.6. of this final rule and this RIA, we are of the view that those are among the potential benefits of finalizing the proposed requirements under which issuers of catastrophic coverage may enroll individuals for multiple plan or policy year terms with periods of up to 10 years. We acknowledge commenters who stated that these benefits are uncertain or may not materialize in practice and we recognize that the benefits discussed in this rule, given the uncertainties regarding State, issuer, and consumer reaction to the finalized provisions, may not materialize to the degree anticipated. We agree with those commenters that noted that they believed our approach to qualitatively describe the potential benefits of this provision to be appropriate given the novelty of the product type. We did not receive any data or additional information from commenters that would assist in our ability to quantify the potential effects of this provision. Regarding those commenters that stated that multi-year catastrophic plans would not meaningfully reduce churn or lower premiums, as discussed in more detail in section III.E.6. of this final rule, we agree that medical costs and other factors cause premiums to increase; however, we believe that reductions in marketing and administrative cost associated with multi-year catastrophic plans could help moderate premium increases. We recognize that any realized benefit will depend heavily on actual issuer uptake, plan offers and features, retention, and implementation costs.
Comment:
A few commenters stated support for the proposal to the extent that structures that spread cost-sharing out monthly or otherwise, together with additional pre-deductible value-based design for preventive service benefits, could reduce upfront financial shock, improve access to preventive and chronic care management, and make catastrophic coverage more usable for some enrollees than under current annual cost-sharing structures. As
( printed page 29844)
discussed in section III.E.6. of this final rule, many commenters stated concern that long-duration catastrophic products could leave enrollees effectively “locked into” inadequate coverage as their health, income, employment, family, or geographic circumstances change. These commenters emphasized that consumers who develop chronic conditions (for example, cancer, kidney disease, diabetes, multiple sclerosis, and behavioral health conditions) could end up stuck in plans with very high cost-sharing and limited practical value. Other commenters warned that front-loaded or variable MOOP/deductible structures could result in enrollees incurring significant medical debt, worsen instances of underinsurance, and increase uncompensated care (especially in rural markets). Additionally, these commenters noted that, given the overall lack of medical literacy, these products could be confusing enough that some consumers would underestimate their true liability at enrollment.
Response:
We acknowledge and appreciate the comments received. We acknowledge commenters who observed that spreading cost-sharing or allowing additional pre-deductible preventive benefits could, in theory, reduce abrupt out-of-pocket costs and encourage timely use of high-value care. However, as discussed in greater detail in section III.E.6. of this final rule, we are finalizing the VBID provision, with modifications, to permit multi-year catastrophic plans to utilize value-based insurance designs to provide benefits before reaching the deductible, under guidelines issued by the Departments. Regarding commenters who stated that individuals could be “locked into” multi-year catastrophic plans, as further noted in section III.E.6. of this final rule, enrollees may terminate coverage at any time without penalty and may also enroll in other coverage during open or special enrollment periods. Therefore, they are not locked into these plans. We acknowledge that certain benefit designs may create incentives to remain enrolled, and we expect issuers to disclose those features. An example of how benefit design differences can incentivize voluntary enrollment over a longer term can be found in Germany, where the German population has many publicly subsidized insurance plans with indefinite coverage terms from which to choose, and only 5 percent of the population switches plans in a given year despite the ability to do so annually.[400]
We also recognize the substantial concern that multi-year catastrophic products could expose enrollees to potential unexpectedly high initial out-of-pocket costs and the possibility of being underinsured if their health needs change after enrollment, if the enrollee is unaware of the policy terms. As discussed in section III.E.6. of this final rule, we are not finalizing the provision that would have permitted the annual limitation on cost sharing to apply on an average basis over the life of the contract, and we note that section 1302(e) of the Affordable Care Act requires that, for each 12-month plan year within a multi-year catastrophic plan, the plan must comply with the Federal annual limitation on cost sharing that applies for that plan year, and the limitation on cost sharing for each plan year of a catastrophic plan must equal the applicable maximum annual limitation on cost sharing for that plan year and cannot vary by disease or other health status, thereby limiting the risk of the front-loaded or variable MOOP/deductible structures that commenters warned could result in significant medical debt and underinsurance. Further, as discussed in this RIA, we recognize and note this as a potential unintended consequence, which could be exacerbated if there are instances of potential reduced flexibility to switch plans in response to changing health needs or life circumstances. As discussed in section III.E.6. of this final rule, we encourage all individuals, including those enrolled in a multi-year catastrophic plan, to review their coverage options regularly and select the option that best suits their needs and budget.
Comment:
A few commenters stated that multi-year catastrophic plans could improve the risk pool by keeping healthier unsubsidized consumers in the Affordable Care Act market rather than uninsured, and, if implemented carefully, the product flexibility could attract issuer participation without necessarily destabilizing the market. Many commenters stated an opposing view noting that healthier or more price-sensitive individuals would disproportionately select multi-year catastrophic plans, worsening the morbidity of remaining metal-tier risk pools resulting in increased premiums for more comprehensive coverage. Many commenters also stated that if healthier individuals enroll in multi-year catastrophic plans, any resulting adverse selection could lead to increases in benchmark premiums and PTC expenditures, or otherwise shift costs toward consumers who need more comprehensive coverage. Many commenters, including providers, safety-net organizations, and State regulators, stated concern that shifting enrollment toward high-deductible multi-year catastrophic coverage would increase uncompensated care, bad debt, or charity-care burdens for hospitals, rural providers, emergency departments, and community health centers because more patients would be unable to meet large deductibles or cost-sharing obligations.
Response:
We appreciate and agree with those commenters that stated, if implemented carefully, multi-year catastrophic plans could retain healthier unsubsidized individuals in the risk pool as opposed to remaining or becoming uninsured and the flexibilities could increase issuer participation. We also acknowledge commenters who warned that longer-term catastrophic plans could worsen adverse selection in metal-tier products. We recognize that given current market conditions, that both outcomes are a possibility and could result in additional changes in market dynamics. As discussed in section V.C.25 of this RIA, due to the current lack of data and information on the potential effects of multi-year catastrophic plans and how they would be structured, we note the uncertainty in potential changes in market dynamics. Further, as discussed in section III.E.6. of this final rule, we are not finalizing a provision that would extend the multi-year plan standards to metal level plans in this final rule. For those commenters stating that adverse selection could lead to increases in premiums and PTC expenditures, we acknowledge the potential effect on premiums, PTC expenditures, and additional transfer effects which would ultimately depend on actual uptake, the mobility of those who enroll, and whether consumers who become higher risk remain in or discontinue these products. However, we also are of the view that, because multi-year catastrophic plans remain part of the individual market risk pool, if uninsured individuals that are healthier enroll in these types of plans, rather than remain uninsured, they could lead to improvements in the risk pool and thus an overall reduction in premiums. Similarly, provider spillovers will depend on realized cost-sharing burdens and enrollee churn.
Comment:
Many commenters stated that pricing multi-year catastrophic products is materially more difficult than annual rating. They highlighted
( printed page 29845)
uncertainty around medical trends, utilization, regulatory changes, changes in benefit mandates, and consumer behavior over multi-year periods. Commenters noted that these uncertainties could either result in higher initial premiums or create material solvency and mispricing risk, including the possibility of product withdrawal or issuer distress. As noted in section III.E.6. of this final rule, several commenters recommended delay, phased implementation, or a shorter initial pilot—often two years rather than up to 10 years—together with more detailed actuarial and State review guidance before allowing broad rollout.
Response:
We appreciate the comments received on this topic and recognize the significant actuarial concerns raised. Pricing any new insurance product requires assumptions about expected claims, utilization, and retention, and those uncertainties materially increase as the pricing horizon lengthens. However, as discussed in more detail in section III.E.6. of this final rule, for rate setting, rate calculations for multi-year plans will be determined each year, as they are for a 1-year plan that renews each year. Thus, rate increases for the whole term will not be set at the initial filing, and enrollees will not progress through the age curve each year. Therefore, we are of the view that this will decrease the likelihood that issuers may ultimately either load premiums for this uncertainty, which could result in higher premiums, or risk inadequate rate setting that could result in financial distress. With regard to comments suggesting that the applicability date should not be imminent, while we are finalizing the proposal to be applicable starting in PY 2027, we will provide additional guidance or rulemaking, as necessary, to address certain aspects of this policy.
Comment:
Many commenters stated concern that the evidentiary basis for the proposal is limited. These commenters stated that insufficient empirical information exists regarding consumer demand, enrollment persistence, premium effects, market segmentation, transfer effects, State operational costs, and Federal spending to support conclusions. Several commenters specifically noted that the agency had not provided sufficient detail, analysis, or data for commenters to fully evaluate the proposal's likely effects on the individual market dynamics, consumers, providers, and other affected entities.
Response:
We acknowledge that the evidentiary record for this novel policy option is limited. Nevertheless, we also reiterate that, as stated previously, Germany offers an example of how the availability of plans with terms that exceed 1 year has potential to reduce churn. Although many different public health insurance plans are offered with indefinite term lengths in Germany, and despite the fact that enrollees can switch plans annually, 39 percent never switch plans in their lifetime.[401]
As discussed in V.C.25. of this RIA, we recognize that available evidence and data on potential effects is lacking and we requested comment and additional data that could help us quantify the impacts multi-year catastrophic plans might have on enrollment patterns, premium levels, Federal expenditures, and operational costs. However, we did not receive any actionable data or information that would assist in further analyzing these issues.
26. Cost-Sharing for Bronze and Catastrophic Plans (§§ 156.136 and 156.155)
To address an issue that has arisen in the implementation of section 1302(c) through (e) of the Affordable Care Act, we are finalizing our proposal adding new § 156.136 to change the permissible cost-sharing parameters for bronze plans and revisions to § 156.155(a)(3) for updated requirements for catastrophic plans with modifications.
We are finalizing changes to the cost-sharing requirements at § 156.155(a)(3) for catastrophic plans in the individual market to address an irreconcilable conflict between section 1302(c) through (e) of the Affordable Care Act. Specifically, we are finalizing our proposal to permit some individual market bronze plans to exceed the maximum annual limitation on cost sharing beginning in PY 2027, but we are modifying to require these bronze plans not to exceed 130 percent of the standard annual limitation on cost sharing, rounded down to the next lowest multiple of 50 dollars, and to achieve an AV within the standard bronze
de minimis
variation at § 156.140(c). We are finalizing our proposal to allow individual market issuers the option to offer one or more increased annual limitation on cost sharing plans only if they offer at least one bronze plan that meets the annual limitation on cost sharing (that is, does not have an increased annual limitation on cost sharing). We are also finalizing our proposal, effective beginning PY 2028, to require catastrophic plans to provide no benefits for any plan year (except as provided in § 156.155(a)(4), (b), and (c)) until an amount equal to 130 percent of the annual limitation on cost sharing is reached. As finalized, we expect that this would incentivize enrollment in bronze plans if issuers can offer these bronze plans at lower premiums than they are currently able under the current annual limitation on cost sharing restriction. This, in turn, would raise the expected out-of-pocket costs by up to 30 percent for enrollees in these additional plans who incur health care costs in excess of the current annual limitation on cost sharing. We also believe that this would provide consumers with additional choice of bronze plans, including the potential for plan designs with lower deductibles and lower premiums.
We sought comment on these impact estimates and assumptions.
After consideration of comments and for the reasons outlined in the proposed rule and this final rule, including our responses to comments, we are finalizing these impact estimates for this policy with the following modifications: to require that the higher MOOP limit which is permitted for some bronze plans not exceed the calculation of 130 percent of the annual limitation on cost sharing; to make a correction to the calculation of 130 percent of the annual limitation; and to delay the implementation of the requirement to calculate the catastrophic annual limitation on cost sharing as 130 percent of the standard annual limitation cost sharing until PY 2028. We summarize and respond to public comments received on the proposed estimates later.
Comment:
Several commenters stated that we failed to consider that raising MOOPs would worsen affordability, delay care, increase medical debt, and potentially contribute to bankruptcy. Many comments noted that providers and hospitals would face increasing uncompensated care when enrollees would not be able to afford their out-of-pocket contribution in such a plan. Many comments stated concern about wider shifts in risk, premium, and enrollment due to the required higher MOOP limits for catastrophic plans, as potentially splitting the population into plans according to their health and level of subsidy, with healthier, richer enrollees selecting catastrophic plans, and only the sicker remaining enrollees remaining in metal tier coverage. Chronic illness was often cited by commenters as making enrollees especially vulnerable to the higher costs possible under this proposal.
Response:
We acknowledge providers and hospitals may become responsible for an increased share of health costs
( printed page 29846)
when consumers are less shielded from the actual costs of services and treatments available through their health plan. However, we are skeptical that many issuers will utilize this enhanced MOOP flexibility for individual market bronze plans in PY 2027, and do not anticipate such widespread availability and enrollment that would require setting premiums responsive to this suspected shift in risk selection. We agree with comments that sicker enrollees may face higher cost sharing, but anticipate limited impact given that those with high medical expenses may generally not opt to purchase a catastrophic plan. We will monitor implementation to be informed of any unanticipated effects.
Comment:
Several comments requested we consider alternatives to altering the annual limitation on cost sharing for catastrophic and bronze plans other than increasing the annual limitation on cost sharing.
Response:
As we stated in the proposed rule, we believe the impasse was not the result of methodological decisions, and no administrable alternatives exist. This issue arises from incongruence between health care cost trends and statutory cost sharing provisions of the Affordable Care Act. In the end, we stated that we believe the differing rates of changes between the three major factors of AV calculation pose an insurmountable statutory problem created by the cost-sharing provisions of section 1302 of the Affordable Care Act. As this will eventually make it impossible for issuers to simultaneously comply with all of these provisions, it produces a result Congress could not have intended, including the eventual elimination of the bronze metal tier. As we previously described, we believe that the policy we are finalizing in this rule represents the best possible outcome since it ensures that meaningful difference be restored between catastrophic plans and bronze plans, attracts currently uninsured individuals who are not eligible for subsidies and deterred by the high premiums of metal tier plans, and will eventually improve the overall risk pool. The underlying actuarial problem—the gradual convergence of catastrophic and bronze plan designs and value—has been developing for several years, and we have been monitoring and discussing this issue since at least the 2017 Market Stabilization Rule. We do not believe that further delay would change the actuarial trajectory or the need for regulatory action, but we have chosen to delay implementation by 1 year to ease the impact of the catastrophic plan change on issuers, States, and Exchanges. We note again that offering catastrophic plans is optional for issuers, as is offering bronze plans. Nothing prevents issuers from conducting a risk assessment when deciding whether to offer these plans for PY 2027 and future plan years that are subject to the cost-sharing changes. Thus, of the various options we identified, the policy we finalize in this rule is one that meets the statutory requirements, considering the other options we identified would put us clearly out of compliance with AV requirements, including by requiring deviation from generally accepted actuarial principles, cause bronze plans to become non-viable more quickly, or both; and we previously described in greater detail how bronze plans becoming impossible to design would be outside of the outcomes clearly intended by Congress. In other words, although we could make adjustments to the AV Calculator methodology and its underlying data sources with the express purpose of preserving bronze plans, we are not convinced that such changes would comply with section 1302(d) of the Affordable Care Act and actuarial standards. Specifically, as we stated earlier in this rule and in the proposed rule, we are not aware of any administrable, actuarially sound regulatory alternatives that could mitigate this problem. We provided examples of alternatives that we considered but did not implement, such as trending the AV Calculator to account for changes in the standard population. However, we believe such a change would make the AV Calculator meaningless, and likely would be contrary to section 1302(d) of the Affordable Care Act. Therefore, we do believe that a real conflict exists, and that the best way to solve the conflict is to give issuers the flexibility, at their option, to offer bronze plans exceeding the standard annual limitation on cost sharing as long as they offer a bronze plan that meets the standard annual limitation on cost sharing. This resolution both ensures that plans meeting the standard annual limitation on cost sharing will be available and that all plans will meet the statutorily-created AV requirements.
27. Discontinuation of Standardized Plan Options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv))
We are finalizing our proposal to discontinue the full suite of standardized plan option policies effective beginning in PY 2027. Specifically, we are finalizing our proposal to remove the following from our regulations: the definition of “standardized options” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b) as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the authority to differentially display standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv). Finally, we are finalizing our proposal to cease the annual design and publication of these plans in the applicable Payment Notice for each plan year.
However, we recognize that some issuers and consumers may still find certain features of these plan designs valuable. This is why we did not propose to require issuers to discontinue their existing standardized plan option offerings altogether. Instead, under this finalized approach, issuers will be permitted to choose whether to discontinue these offerings altogether or to continue offering them with either the same or modified cost sharing, while we simultaneously discontinue the differential display of these plans on
HealthCare.gov
and the DE pathways.
Under this finalized approach, if issuers wished to discontinue their standardized plan option offerings altogether, they will be permitted to do so, and enrollees in these plans will be crosswalked to a different plan in accordance with the crosswalk hierarchy at § 155.335(j). Additionally, if issuers wished to continue offering these standardized plan options with the same cost sharing, they will also be permitted to do so, and enrollees in these plans will continue to be auto-reenrolled in these plans from one plan year to the next. However, these plans will no longer be visually distinguished as standardized plan options on
HealthCare.gov
or the DE pathways. Finally, if issuers wished to continue offering these standardized plan options but also wished to modify these plans' cost sharing structures, they will be permitted to do so, but these issuers will continue to be subject to the requirements under the definition of “plan” at § 144.103 and to the uniform modification requirements at § 147.106.
( printed page 29847)
In most scenarios where an issuer modifies the cost sharing structure of one of its standardized plan option offerings, the newly modified plan that was formerly the standardized plan option will be considered a new plan and will therefore require a new plan ID. In this scenario, enrollees will be crosswalked from the discontinued plan to another plan in accordance with the crosswalk hierarchy at § 155.335(j). These enrollees could be crosswalked into the newly modified plan that was formerly the standardized plan option, or an entirely different plan altogether, depending on the unique circumstances in each county.
However, under the definition of “plan” at § 144.103, a State may permit issuers to make greater changes to a plan's cost sharing while still permitting that plan to be considered the same plan—thus maintaining the same plan ID. Furthermore, under § 147.106(e)(3)(iv), as long as the variation in cost sharing is solely related to changes in cost and utilization of medical care, or to maintain the same metal tier level (and other applicable requirements under § 147.106(e) are met), the modifications could be considered uniform (thus, a viable exception to guaranteed renewability).
In the scenario where an issuer modifies what was formerly a standardized plan option's cost sharing structure while maintaining the same plan ID, enrollees in the plan will be auto-reenrolled from one plan year to the next. In either case, whether the modification of a former standardized plan option's cost sharing results in that plan being considered the same or a different plan, enrollees will be crosswalked in accordance with the crosswalk hierarchy at § 155.335(j), and that plan will no longer be differentially displayed as a standardized plan option on
HealthCare.gov
or the DE pathways.
Adopting this approach will effectively remove the standardization component of this suite of policies while simultaneously minimizing the risk of disruption for consumers enrolled in and issuers of these plans. This approach will also ensure that issuers of these plans that wish to continue offering them will be able to do so at their discretion. If issuers did choose to continue offering these plans, either with the same or modified cost sharing structures, they will be able to continue utilizing existing benefit packages, provider networks, drug lists, and formularies, including those paired with standardized plan options for PY 2026. This will further minimize burden for these issuers.
In addition, we have assumed the responsibility for differentially displaying standardized plan options on
HealthCare.gov
in accordance with § 155.205(b)(1), meaning that FFE and SBE-FP issuers have not been subject to this burden since the requirement to offer standardized plan options as well as the differential display of these plans were reintroduced in PY 2023. Thus, discontinuing the differential display of these plans on
HealthCare.gov
will not affect issuers or impose any additional burden in this regard.
However, we acknowledge that the discontinuation of the differential display requirements for the DE pathways at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv) will impose a degree of burden on approved web-broker and QHP issuer enrollment partners using a direct enrollment pathway to facilitate consumer enrollment through an FFE or SBE-FP, since these entities will be required to modify their own platforms in some manner. However, we anticipate that the burden of making these modifications will be minimal, as decommissioning existing functionalities (such as the differential display of standardized plan options, which will include the full suite of differential display features discussed in greater detail in the preamble to § 156.201 of this final rule) and reverting to the previous state of display will entail significantly lower burden than introducing novel features and functionalities.
Further, since differential display of standardized plan options on
HealthCare.gov
is operationally contingent on these plans having the required cost sharing parameters, and since we will no longer design and publish standardized plan options in the applicable Payment Notice for each plan year, no plans will technically meet the requirements to be considered standardized plan options, meaning no plans will differentially display on
HealthCare.gov
—even if we made no changes to the current functionality. The same will be true for approved web-broker and QHP issuer enrollment partners using a direct enrollment pathway to facilitate consumer enrollment through an FFE or SBE-FP, meaning the discontinuation of the differential display features could occur even without disabling the existing functionality to differentially display standardized plan options on their respective platforms.
We refer readers to the preamble section for the finalized policy to discontinue standardized plan options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv)) for a detailed discussion of relevant literature we considered in our approach to this finalized policy.
We sought comment on these impact estimates and assumptions. We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
28. Discontinuation of Non-Standardized Plan Option Limits and Exceptions (§ 156.202)
We are finalizing our proposal to discontinue non-standardized plan option limits and exceptions at § 156.202. However, we recognize that some issuers and consumers may still find certain features of the chronic and high-cost condition plans that were originally offered through the non-standardized plan option limit exceptions process valuable. This is why we did not propose to require issuers to discontinue these chronic and high-cost condition plans. Instead, under this finalized policy, issuers will be permitted to choose whether to discontinue the chronic and high-cost condition plans originally offered through the non-standardized plan option limit exceptions process altogether or continue offering them with either the same or modified cost sharing. Issuers will similarly be permitted to continue offering other non-standardized plan options not associated with the non-standardized plan option limit exceptions process.
Under this finalized approach, if issuers wish to discontinue the chronic and high-cost condition plans originally offered through the exceptions process (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process) altogether, they will be permitted to do so, and enrollees in these plans will be crosswalked to a different plan in accordance with the crosswalk hierarchy at § 155.335(j). Additionally, if issuers wish to continue offering the chronic and high-cost condition plans originally offered through the exceptions process (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process) with the same cost sharing structures, they will also be permitted to do so, and enrollees in these plans will continue to be auto-reenrolled in these plans from one plan year to the next. Finally, if issuers wish to continue offering the chronic and high-cost condition plans originally offered through the exceptions process (or other non-
( printed page 29848)
standardized plan options not associated with the non-standardized plan option limit exceptions process) but also wish to modify these plans' cost sharing structures, they will be permitted to do so, but these issuers will continue to be subject to the requirements under the definition of “plan” at § 144.103 and to the uniform modification requirements at § 147.106.
In most scenarios where an issuer modifies the cost sharing structure of one of its chronic and high-cost condition plans originally offered through the exceptions process (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process), the newly modified plan that was formerly the exceptions process plan (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process) will be considered a new plan and would therefore require a new plan ID. In this scenario, enrollees will be crosswalked from the discontinued plan to another plan in accordance with the crosswalk hierarchy at § 155.335(j). These enrollees could be crosswalked into the newly modified plan that was formerly the exceptions process plan, or an entirely different plan altogether, depending on the unique circumstances in each county.
However, under the definition of “plan” at § 144.103, a State may permit issuers to make greater changes to a plan's cost sharing while still permitting that plan to be considered the same plan—thus maintaining the same plan ID. Furthermore, under § 147.106(e)(3)(iv), as long as the variation in cost sharing is solely related to changes in cost and utilization of medical care, or to maintain the same metal tier level (and other applicable requirements under 45 CFR 147.106(e) are met), the modifications could be considered uniform (thus, a viable exception to guaranteed renewability).
In the scenario where an issuer modifies what was formerly an exceptions process plan's (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process) cost sharing structure while maintaining the same plan ID, those enrolled in the plan will be auto-reenrolled from one plan year to the next. In either case, whether the modification of a former exceptions process plan's cost sharing results in that plan being considered the same or a different plan, enrollees will be crosswalked in accordance with the crosswalk hierarchy at § 155.335(j).
Ultimately, adopting this approach will substantially reduce regulatory complexity and the burden associated with the non-standardized plan option limit and the corresponding exceptions process while simultaneously minimizing the risk of disruption to consumers enrolled in and issuers of the chronic and high-cost condition plans originally offered through the exceptions process (or other non-standardized plan options not associated with the non-standardized plan option limit exceptions process). If issuers did choose to continue offering these plans, either with the same or modified cost sharing structures, they will be able to continue utilizing existing benefit packages, provider networks, drug lists, and formularies, including those paired with what were formerly the exceptions process plans for PY 2026. This will further minimize burden for these issuers.
We refer readers to the preamble section for the finalized policy to discontinue standardized plan options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv)) for a detailed discussion of relevant literature we considered in our approach to the finalized policy to discontinue non-standardized plan option limits and exceptions.
We sought comment on these impact estimates and assumptions. We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
29. Provider Access Standards for Network Plans (§ 155.1050 and § 156.230)
We are finalizing our proposal at § 155.1050(d) to allow FFE States, including States that perform plan management, that elect to do so, to conduct provider access reviews for issuers' plans that use and do not use a provider network, provided that the State demonstrates it has sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4). This policy will apply effective beginning in PY 2027 for provider access certification reviews for issuers' plans that use a provider network and effective PY 2028 for provider access certification reviews for issuers' plans that do not use a provider network. HHS will continue to conduct network adequacy reviews consistent with § 156.230 for QHP issuers that use a provider network and, for plan years beginning on or after January 1, 2028, provider access reviews for QHP issuers that do not use a provider network in FFE States that do not elect to conduct such reviews, or in FFE States that do not demonstrate they have sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program, as described at § 155.1050(d)(2) through (d)(4). Under this finalized policy, we will continue to collect network adequacy data, including time and distance and appointment wait time data. We will continue collecting this data from all FFE issuers, either to use to conduct Federal network adequacy reviews in FFE States that do not elect to do so or do not demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4), or with a view to make it available in a standardized format to States that are determined to have an Effective Provider Access Review Program, to assist them in their network adequacy analysis.
The preceding years of conducting reviews of QHP issuer provider network adequacy, including analyzing issuer submitted data and discussions with States, issuers, and other various interested parties around diverse market conditions, have demonstrated that a one-size-fits-all approach to provider network adequacy review is not satisfactory. For example, issuers have highlighted to us persistent challenges in locating and contracting with enough providers of various specialties (for example, allergy and immunology, behavioral health, gastroenterology) in remote or difficult to access areas of a State. States have brought to our attention various geographic constraints that impact QHP issuer's ability to satisfy time and distance requirements and have made arguments to assess based on time or distance individually rather than being required to meet a time and distance standard that may be insurmountable due to a topographical constraint such as a body of water or navigating roads in mountainous terrain. Partnerships with States performing plan management, that have elected to conduct their own network adequacy reviews, have highlighted for us how States may innovate in their approach to conducting network adequacy reviews in ways that are sensitive to conditions and capacity in the State. These are among the factors
( printed page 29849)
that led us to revisit our previous approach to defer network adequacy reviews to States as we recognize that a State, with its more intimate knowledge of its own demographics, topographical considerations, and provider supply, is often best positioned to evaluate local provider networks and market conditions and can tailor network adequacy standards in a more nuanced way than the broader Federal Government requirements may. Thus, in recognition of the crucial role States have in developing and enforcing network adequacy standards and because we believe that States are often best positioned to evaluate local provider networks and market conditions, we are finalizing at § 155.1050(d) to allow FFE States, including States that perform plan management, that elect to do so, to conduct provider access reviews for issuers' plans that use and do not use a provider network, provided that HHS determines the State has sufficient authority and the technical capacity to conduct the reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4). As noted previously, this policy will be effective beginning PY 2027 for provider access reviews of network plans, and beginning PY 2028 for provider access reviews of non-network plans. In addition, we will continue collecting network adequacy data from all FFE issuers, either to use to conduct Federal network adequacy reviews in FFE States that do not elect to do so, or do not demonstrate they have sufficient authority and the technical capacity to conduct these reviews by satisfying the criteria to be considered to have an Effective Provider Access Review Program as described at § 155.1050(d)(2) through (d)(4), or with a view to make it available in a standardized format to States that are determined to have an Effective Provider Access Review Program, to assist them in their network adequacy analysis.
We do not anticipate any additional costs to the Federal Government as part of this finalized policy. While HHS still intends to collect data from QHP issuers in States with Effective Provider Access Review Programs, there is the potential for cost savings at the Federal level related to provider access reviews during QHP certification if HHS shifts these responsibilities to States that elect to conduct their own reviews. However, this may increase costs in States if they do not already possess capability and resources necessary to conduct sufficient provider access reviews, as well as ensure compliance and appropriate consumer protections. For QHP issuers, this finalized policy may have reduced administrative costs and efficiency gains. While HHS will still collect network adequacy data from issuers in these States, issuers will not have to undergo network adequacy certification reviews at the Federal level which often requires additional reporting to HHS to address corrections in network adequacy required to meet Federal standards. Additionally, many QHP issuers already have State specific network adequacy requirements with which they must comply to operate plans in the State. Thus, redirecting network adequacy review activities to States, that issuers already need to report to, could streamline the efficiency of the QHP certification process and reduce burden for issuers. However, requiring issuers to submit network adequacy data on both the State and Federal levels could potentially duplicate efforts and increase costs for issuers, though the extent of any administrative burden is uncertain as States may have different data collection and submission requirements, and it is not yet known how FFE States would implement or may change network adequacy data collection as part of an Effective Provider Access Review Program and if existing data collection processes already exist or need to be modified to support requirements under finalized § 155.1050(d).
Regarding Federalism implications of this finalized policy, the Affordable Care Act does not require States to establish and enforce network adequacy certification criteria and review programs for QHP issuers; if a State elects not to establish any of these programs or is not approved to do so, HHS must establish and operate the programs in that State. As part of this finalized policy, we will not require that States elect to conduct provider access certification reviews as part of an Effective Provider Access Review Program. Rather, we are finalizing our proposal to allow States flexibility to conduct provider access certification reviews, should they choose, provided they have sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria in § 155.1050(d)(2) through (d)(4).
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
30. Essential Community Provider Standards (§ 155.1051 and § 156.235)
In this final rule, we are not finalizing our proposal to reduce the minimum percentage requirements described under § 156.235(a)(2)(i) and (b)(2)(i) from 35 to 20 percent for the overall, FQHC, and family planning ECP thresholds, and will maintain the minimum percentage at 35 percent for each of the three aforementioned thresholds. We are finalizing our proposal to amend the narrative justification requirement language at § 156.235(a)(3) and 156.235(b)(3) to reflect current operations and data submission requirements as part of ECP certification reviews, as narrative justifications are no longer required for issuers not meeting the ECP standard as they input contract statuses directly into the ECP User Interface in the MPMS. Additionally, we are finalizing our proposal with modifications to allow FFE States flexibility to elect to conduct ECP certification reviews. Specifically, as discussed earlier in this final rule, we are finalizing our proposal to allow FFE States flexibility to elect to conduct ECP certification reviews for network plans effective beginning PY 2027; however, we are modifying our proposal that will allow FFE States to conduct ECP certification reviews for non-network plans effective beginning PY 2028 under § 155.1051 due to the delayed implementation of the provisions of allowing certification of non-network plans as QHPs.
ECP requirements under the General Standard at § 156.235(a)(2)(i) specify that a plan applying for QHP certification to be offered through a FFE must demonstrate in its QHP application that the issuer's provider network includes as participating providers at least a minimum percentage, as specified by HHS, of available ECPs in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B), and at least a minimum percentage of available ECPs in each plan's service area within certain individual ECP categories, as specified by HHS. Alternate Standard issuers must demonstrate similar minimum percentage requirements as described at § 156.235(b)(2)(i). For PY 2014, we set this minimum percentage at 20 percent and increased the minimum percentage to 30 percent for PY 2015. For QHP certification for PY 2018 and through the end of PY 2022, we returned to the percentage used in PY 2014, and to again consider the
( printed page 29850)
issuer to have satisfied the threshold requirement if the issuer contracted with at least 20 percent of available ECPs in each plan's service area to participate in the plan's provider network. We increased the minimum percentage to 35 percent starting in PY 2023 and required issuers to separately meet 35 percent minimum percentage requirements within two standalone ECP categories, FQHCs and family planning providers, as finalized in the PY 2024 Payment Notice. In this final rule, we are not finalizing our proposal to reduce the minimum percentage requirement from 35 to 20 percent, but we are instead retaining the minimum percentage requirement at 35 percent. Accordingly, medical QHP and SADP issuers will be considered to have satisfied minimum percentage requirements under § 156.235(a)(2)(i) and (b)(2)(i) if they contract with at least 35 percent of available ECPs in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B), they contract with at least 35 percent of available FQHCs that qualify as ECPs in each plan's service area, and they contract with at least 35 percent of available family planning providers that qualify as ECPs in the plan's service area (medical QHPs only) to participate in the plan's provider network. While we maintain that reducing the minimum percent to the previous 20 percent would have allowed additional flexibility for QHP issuers to build provider networks that comply with the ECP Standard under § 156.235, we believe the majority of issuers exceed the minimum percentage requirement within their provider networks and may not require this level of flexibility. For example, for PY 2026, the average threshold percentage for all FFE issuers, including issuers in States performing plan management, for the overall ECP requirement was 71 percent, for the family planning provider requirement was 85 percent, and for the FQHC requirement was 79 percent despite the minimum percentage being set at 35 percent. Thus, many issuers continue to exceed current threshold requirements by more than 30-percent, so even if the threshold were reduced to 20 percent, the reduction may not have influenced issuer contracting behavior and associated administrative cost savings.
We do not anticipate any major new impacts associated with maintaining the minimum ECP threshold percentage at 35 percent described under §§ 156.235(a)(2)(i) and (b)(2)(i), compared to previous plan years. Retaining existing requirements for network size may stabilize costs for consumers as issuers may have responded to reduced minimum percentage requirements by contracting with fewer ECPs, which could have increased out-of-pocket costs for consumers whose preferred ECPs transition out-of-network. Retaining the existing minimum percentage requirement will minimize additional costs from increased travel time and wait time for appointments or reductions in continuity of care for patients whose providers have been removed from their insurance networks. Issuers who maintain existing contracting levels to meet the 35-percent minimum percentage requirement will likely maintain any current costs.
We are finalizing our proposal to modify the narrative justification requirement under §§ 156.235(a)(3) and 156.235(b) to make the language more consistent with current operations and data submission requirements for ECP certification reviews. As part of the narrative justification requirements, an issuer applying for QHP certification that is not meeting the ECP standard under § 156.235 had to include as part of its QHP application a written open-ended narrative describing how the issuer's provider network as currently designed would provide an adequate level of service for individuals residing in low-income zip codes or Health Professional Shortage Areas within the plan's service area, and how the issuer would strengthen the plan's provider network in future years. We have instituted multiple refinements and modernizations to the justification process over time, and recently in PY 2025, leveraged information technology to embed justification related information (for example, contract statuses) into the new ECP User Interface (UI) in the MPMS. In alignment with this modernization that now allows issuers to easily select and report the contract status of ECPs included within their networks or who are being recruited into their networks, we are finalizing our proposal to modify §§ 156.235(a)(3) and 156.235(b) to instead designate that a network plan applying for QHP certification to be offered through a FFE must include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. A network plan will not need to report on the status of contract offers for all available ECPs in the network plan's service area but should at least report on the status of contract offers for all ECPs which the issuer has either included in its network plan or offered a contract to be included in its network plan within each service area.
We believe these changes to the narrative justification requirements at §§ 156.235(a)(3) and 156.235(b) will not have meaningful impacts to issuers since these amendments reflect current ECP data submission requirements that have been in place since PY 2025. Issuers will continue to upload ECP data into MPMS and complete required fields within the ECP UI, including selecting or importing ECPs included within their networks and designating the status of their contract offers. Although this finalized language does not modify current requirements as part of ECP certification reviews, it will reflect modernizations to the ECP data collection process that have introduced significant program efficiencies that have improved data quality, and effectively reduced the time, resources, and administrative costs required by issuers to submit supporting justification documentation for meeting the ECP standard under § 156.235.
Furthermore, we are finalizing our proposal with minor modifications to allow FFE States, including States performing plan management, to elect to perform their own State reviews of issuer-submitted ECP data provided the State demonstrates sufficient legal authority and the technical capacity to conduct these reviews by meeting the applicable criteria, as determined by HHS, to be considered to have an Effective ECP Review Program under § 155.1051. We are finalizing this policy for FFE States to conduct their own ECP certification reviews of issuers' plans with a provider network effective beginning in PY 2027, and we are modifying our proposal to be effective PY 2028 for ECP certification reviews for issuers' plans that do not use a provider network. We are finalizing that FFE States must ensure that a QHP with a provider network includes in its provider network a sufficient number and geographic distribution of ECPs, where available, to ensure reasonable and timely access to a broad range of such providers for low-income individuals or individuals residing in Health Professional Shortage Areas within the QHP's service area, in accordance with the Exchange's network adequacy standards. In addition, we are finalizing our proposal that FFE States must also ensure that a non-network plan applying for certification as a QHP to be offered through an FFE demonstrates that it provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full to ensure that services will be accessible without
( printed page 29851)
unreasonable delay. We also are finalizing that FFE States must have established ECP requirements that are set forth in State statute or regulation, and FFE States must demonstrate that these established ECP requirements ensure plans meet all the following requirements that promote a sufficient number and geographic distribution of ECPs: Minimum percentage requirements (under § 156.235(a)(2)(i) and § 156.236(b)(1)), Indian health care provider requirements (under § 156.235(a)(2)(ii)(A) and § 156.236(b)(3)), and category per county requirements (under § 156.235(a)(2)(ii)(B) and § 156.236(b)(2)). We are also finalizing that FFE States with alternative ECP requirements must demonstrate how those requirements would promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs. At § 155.1051(e), we also set forth factors that HHS would consider in its review to determine if an FFE State has an Effective ECP Review Program. Additionally, HHS will be available to provide technical assistance and various resources to FFE States, including that we will continue collecting ECP data from FFE issuers in FFE States with an Effective ECP Review Program with the goal of providing this data in a standardized format to FFE States that could inform additional assessments of access to ECPs across the State and assisting FFE States that may require additional support due to more limited resources.
We anticipate several potential impacts associated with these finalized changes to implement the Effective ECP Review Program provisions at § 155.1051. First, while we believe that predominately collecting and reviewing ECP data on the Federal level as part of QHP certification for issuers across the FFE has helped ensure that issuers include a sufficient number and geographic distribution of ECPs within their networks, we believe providing FFE States more flexibility and authority to conduct their own ECP certification reviews may deliver quality improvements to the review process. We acknowledge that States possess unique knowledge on local and contextual factors, such as on market conditions, geographic constraints, and areas in the State with limited economic resources, provider shortages, workforce issues, and population demographics. FFE States may incorporate these various factors to tailor their ECP certification reviews and apply ECP certification results to more directly address State-specific challenges for consumers as it pertains to ECP access, which is more difficult to accomplish at the Federal level with a one-size-fits all approach for all States. In addition, continuing to leverage Federal infrastructure to collect ECP data from issuers in FFE States with an Effective ECP Review Program will create opportunities for a State-Federal partnership where HHS could provide data in a standardized format to States to inform their ECP certification reviews and provide support to FFE States that require additional assistance.
Additionally, we presume there are several cost-related implications of this finalized policy. We do not anticipate any additional costs to the Federal Government as part of this finalized policy. While HHS still intends to collect data from QHP issuers in FFE States with Effective ECP Review Programs, there is still the potential for cost savings at the Federal level as it pertains to reviewing such ECP data during QHP certification and taking enforcement actions against QHP issuers after QHP certification as part of compliance if HHS shifts these responsibilities to FFE States that elect to conduct their own reviews of issuers as part of the Effective ECP Review Program. Though, in turn, this may increase costs among FFE States if they do not already possess the capability and resources to conduct complex, data-intensive ECP certification reviews and enforcement actions against issuers that neglect to meet ECP requirements. For QHP issuers, this finalized policy may have reduced administrative costs and efficiency gains. While HHS will still collect ECP data from issuers in these FFE States, issuers will not have to undergo intensive ECP certification reviews at the Federal level which often requires coordination with HHS to address corrections in ECP data until ECP requirements are met. Also, many QHP issuers already need to coordinate with FFE States to meet various requirements to operate plans in the State. Thus, redirecting ECP review activities to FFE States that issuers already need to coordinate with could further streamline the efficiency of the QHP certification process. However, requiring issuers to submit ECP data on both the State and Federal levels could potentially duplicate both effort and costs among issuers, but the extent of this administrative burden is uncertain as States likely have different data collection and submission requirements, and it is not yet known how FFE States will implement ECP data collection as part of the Effective ECP Review Program and if existing data collection processes already exist or need to be developed to support requirements under § 155.1051.
Lastly, as it pertains to Federalism implications of this proposal, the Affordable Care Act does not require FFE States to establish and enforce ECP certification criteria and review programs for QHP issuers; if an FFE State elects not to establish any of these programs or is not approved to do so, HHS must establish and operate the programs in that State. As part of this finalized policy, we will not require that FFE States elect to conduct ECP certification reviews as part of the Effective ECP Review Program. Rather, we are finalizing additional flexibilities to allow FFE States with the desire to conduct ECP certification reviews to have an opportunity to do so, provided they have sufficient authority and the technical capacity to conduct these reviews by meeting the applicable criteria in § 155.1051. Thus, FFE States that elect to perform their ECP certification reviews and undergo HHS' determination process for assessing if an FFE State has an Effective ECP Review Program will be willingly assuming this responsibility.
We sought comment on these impacts and assumptions.
We did not receive any comments in response to the proposed impact estimates for these policies as part of the regulatory impact analyses. However, several commenters raised general concerns on the potential cost impacts to consumers, ECPs, and issuers if the minimum percentage requirement is reduced to 20 percent. Please see our response to this discussion in section III.E.11.a. of this final rule. For the reasons outlined in the final rule, we are finalizing these estimates with modifications to reflect the impacts associated with not finalizing the proposed minimum percentage reduction. These modifications include no projected impacts due to retaining the minimum percentage at 35 percent on consumer's access to continuous care and out-of-pocket costs, and administrative costs to issuers.
31. QHP Certification of Non-Network Plans (§ 156.236)
We are finalizing a number of revisions to part 155 and part 156 to allow plans that do not use a network (non-network plans) to obtain QHP certification by demonstrating sufficient access to a broad range of providers in a manner consistent with sections 1311(c)(1)(B) and (C) of the Affordable Care Act. Non-network plans will be permitted to obtain QHP certification effective PY 2028, if satisfying all
( printed page 29852)
applicable certification requirements, including those under finalized § 156.236. This finalized policy will not require States to approve non-network plans for sale nor will it require Exchanges to allow such plans to operate on the Exchange in their State. States that do not approve non-network plans as QHPs will see no impact under this proposal. The following impact analysis applies only to States that decide to offer such plans as QHPs.
Non-network plans may typically attract healthier enrollees who are generally more willing and able to engage in a sufficient number of price negotiations with providers to benefit from the value a non-network plan can provide. Conversely, individuals requiring frequent care may prefer enrolling in network plans to avoid the need to conduct price negotiations for a greater volume of needed care. This, in turn, naturally leads to favorable risk selection in non-network plans. Consequently, under this finalized policy, non-network plans should anticipate and budget for risk adjustment transfers in their premium calculations, at least to the extent that the issuers of such plans do not already have sufficient reserves at hand to be able to pay an expected high risk adjustment transfer amount.
This dynamic also means that non-network plans may tend to have lower premiums than network plans, so we expect that they would tend to be among the least expensive plans in a particular area. This could affect premium tax credits to the extent that non-network plans are the lowest and/or second-lowest cost silver plan in that area.
We sought comment on these impact estimates and assumptions.
While commenters did not specifically comment on the proposed estimates within this section, commenters shared concerns consistent with this discussion regarding consumer out-of-pocket costs and balance billing risks, financial impacts on providers unable to negotiate benefit amounts with non-network plans, the likelihood for non-network plans to lower health care costs, non-network plans potentially affecting the benchmark for advanced premium tax credits, and the possibility for non-network plans to alter risk pools by attracting healthier enrollees. Please refer to our responses to these concerns in III.E.12. of this final rule. For the reasons outlined in the proposed and final rule, we are finalizing these estimates.
32. Strengthening HHS' Oversight of the Administration of the Advanced Payments of the Premium Tax Credit, Cost-Sharing Reductions, and User Fee Programs and Clarifying HHS' Compliance Review Authority (§ 156.480)
We are finalizing our proposal to modify § 156.480 to clarify HHS' authority to audit or conduct a compliance review to assess issuers' compliance with requirements related to the APTC, CSR, and user fee programs. Specifically, we are clarifying that under § 156.480(c), HHS or its designee may audit or conduct a compliance review to assess compliance with all requirements related to the APTC, CSR, and user fee programs applicable to issuers offering a QHP in an Exchange. For consistency, we are also finalizing our proposal to make conforming changes to § 156.480(c)(6) to provide that in instances where HHS enforces compliance with any requirements related to the APTC, CSR, and user fee programs for QHP issuers participating in State Exchanges or SBE-FPs, HHS may do so in accordance with § 156.805. We are further clarifying that the compliance review authority in § 156.480(c) allows for compliance reviews on an as needed or annual basis.
We estimate that the audits that we will conduct under this authority will not impose additional costs beyond what is already accounted for in the audit review process (86 FR 24140, 24281). We estimate that we will conduct compliance reviews under this authority to address systemic issues for approximately 150 issuers each year. We estimate that it will take a business operations specialist 10 hours (at a rate of $78.14 per hour) to compile and submit data and other information necessary for a compliance review. We estimate it will take a compliance officer (at a rate of $75.40 per hour) 4 hours to review and sign off on the submission. The cost per issuer to develop and submit the compliance information will be approximately $1,083.
The total annual cost to issuers undergoing compliance reviews will be approximately $162,450 ($1,083 × 150 issuers) beginning in 2026. However, conducting compliance reviews on an as needed or annual basis if determined appropriate by HHS to assess issuer compliance with requirements related to the APTC, CSR, and user fee programs may reduce the amount of APTC overpayments and result in HHS recouping those overpayments. Further, this additional information could assist issuers in correcting their data for APTC payments not received in advance of the 3-year window, after which HHS only recoups overpayments.[402]
While there will be some Federal costs to conduct the compliance reviews, we expect benefits of more accurate APTC reconciliation and payment adjustments to outweigh the costs.
We sought comment on the proposed impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates with modifications to update for the current adjusted hourly wage rates used in burden estimates provided in Table 14 of part IV.A.
33. Factors Considered in Determining the Amount of CMPs and HHS' Authority To Impose CMPs Against Issuers in State Exchanges or SBE-FPs (§ 156.805)
We are finalizing our proposal to amend § 156.805 to reiterate what HHS considers when imposing CMPs as enforcement remedies against QHP issuers in Exchanges. Specifically, we are amending § 156.805(b) to provide that HHS, in determining the amount of CMPs, will identify the lawful purpose or purposes of the CMP.
We are also finalizing our proposal to clarify the authority HHS has to impose CMPs against issuers in State Exchanges and SBE-FPs for identified violations. Specifically, we are amending § 156.805(f) to clarify that, when HHS' authority to enforce requirements in State Exchanges and SBE-FPs is triggered, HHS may impose CMPs against issuers in State Exchanges and SBE-FPs for violations of requirements described in § 156.805(a) that are applicable to issuers offering a QHP in a State Exchange or SBE-FP.
We do not believe that the finalized amendments will impose substantial additional costs to HHS beyond the costs that are already accounted for as part of the existing bases and process for imposing CMPs in the FFE, State Exchanges, and SBE-FPs. This is an existing policy that already applies broadly to those issuers participating on the Exchange, and since this amendment does not independently add
( printed page 29853)
any new requirements for any issuer in an Exchange, we believe that the burden associated with it is already covered by existing requirements in § 156.805. Therefore, we do not believe there will be additional burden to issuers under this finalized policy. The burden associated with these requirements is the time and effort necessary to draft and submit audit reports that form the basis for subsequent CMP assessments. While these requirements do impose burdens, data collection requirements associated with imposing CMPs on QHP issuers in an Exchange are exempt from PRA requirements in accordance with 44 U.S.C. 3518(c)(1)(B)(ii), as effectuated through 5 CFR 1320.4(a)(2), because this information would be collected during the conduct of an administrative action or investigation involving an agency against specific individuals or entities.
On balance, we anticipate that this finalized policy will streamline our compliance and enforcement processes and limit the administrative burden for evaluating Exchange standards and requirements applicable to issuers offering QHPs participating in Exchanges.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
34. Administrative Review of QHP Issuer Sanctions (§§ 156.903 and 156.935)
We are finalizing our proposal to amend to § 156.903 to provide that an ALJ presiding over an appeal of a sanction imposed in accordance with § 156.805 may issue subpoenas, upon his or her own motion or at the request of a party, if they are reasonably necessary for the full presentation of a case and to add procedures governing the process for issuing subpoenas. We are also finalizing our proposal to amend § 156.935 to ensure that the discovery provisions set forth therein do not apply to appeals of proposed CMPs to be assessed under § 156.805 that result from violations identified in audits under § 156.480(c).
We do not believe that the finalized amendments will impose additional costs to HHS beyond what is currently accounted for in appeals to the DAB. The DAB's procedures include subpoena procedures which follow the procedures established by a program's regulations. We also do not believe the finalized amendments to exclude appeals of CMPs to be assessed under § 156.805 that result from violations identified in audits under § 156.480(c) from discovery will impose additional costs on HHS or issuers, as both parties would be able to provide and obtain information during the audit and informal refutation process and obtain publicly available information that would help to develop a record for appeal.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
35. Quality Improvement Strategy (§ 156.1130)
As discussed in section IV.U of this final rule, there is no information collection associated with this finalized policy and no changes were proposed to the QIS data collection requirements applicable to QHP issuers.
We sought comment on this impact estimate and assumption.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
36. Netting and Establishment of Debt Regulations To Include CMPs (§ 156.1215)
We are finalizing our proposal to amend the payment and collections processes set forth at § 156.1215(b) to provide that any CMPs assessed against health insurance issuers for violations of any applicable Exchange standards and requirements or PHS Act requirements applicable health insurance issuers, will be subject to netting as part of HHS' integrated monthly payment and collections cycle. We also finalize our proposal to amend § 156.1215(c) to provide that any amount owed to the Federal Government by an issuer and its affiliates for unpaid CMP amounts, after HHS nets amounts owed by the Federal Government under these program affiliates, will be the basis for calculating the determination of the debt.
We do not believe that the finalized amendments will impose additional costs to HHS beyond costs that are already accounted for as part of the existing payment and collections process. The existing payment and collection process uses netting as one means to collect debts from health insurance issuers. The finalized amendments provide that HHS will use the existing process to collect unpaid amounts for CMPs assessed against issuers and their affiliates operating under the same tax identification number that are already subject to netting. This finalized policy also reduces the number of payments and charges flowing back and forth between HHS and issuers, allowing for more efficient collections.
Therefore, we anticipate this finalized policy will streamline the payments and collections processes and limit the administrative burden for operating our programs.
We sought comment on these impact estimates and assumptions.
We did not receive any comments in response to the proposed impact estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
37. Regulatory Review Cost Estimation
As discussed in the 2027 Payment Notice proposed rule, due to the uncertainty involved with accurately quantifying the number of entities that would review the rule, we assumed that the mid-point between the total number of unique commenters on the 2026 Payment Notice proposed rule (269) and the number of page views on the
Federal Register
website during the comment period for that rule (15,824) would be the approximate number of reviewers (8,046) of this final rule. We acknowledged that this assumption may understate or overstate the costs of reviewing this rule. It was possible that not all commenters reviewed last year's rule in detail, and it was also possible that some reviewers chose not to comment on the proposed rule. For these reasons, we thought that the mid-point of unique commenters and page views would be a fair estimate of the number of reviewers of this rule. We welcomed any comments on the approach in estimating the number of entities which would review the proposed rule. We also recognized that different types of entities are in many cases affected by mutually exclusive sections of the proposed rule, and therefore for the purposes of our estimate, we assumed that each reviewer reads approximately 50 percent of the rule. We sought comments on this assumption. Using the wage information from the BLS for medical and health service managers (Code 11-9111), we estimated that the cost of reviewing the proposed rule is $113.42 per hour, including overhead
( printed page 29854)
and fringe benefits.[403]
Assuming an average reading speed of 250 words per minute, we estimated that it would take approximately 6.5 hours for the staff to review half of the proposed rule. For each entity that reviewed the rule, the estimated cost is $741.77 (6.54 hours × $113.42). Therefore in the proposed rule, we estimated that the total cost of reviewing this regulation is approximately $5,968,281.42 ($741.77 × 8,046 reviewers).
We sought comment on these estimates and assumptions.
We did not receive any comments in response to the proposed estimates for this policy. For the reasons outlined in the proposed and final rules, we are finalizing these estimates with the following modifications. The mid-point between the actual number of comments received for the 2027 Payment Notice proposed rule (2,861) and the number of page views on the
Federal Register
website as of March 26, 2026 (25,723) would be the approximate number of reviewers (14,292) of this final rule. As noted previously, the estimated cost for each entity to review the rule is $741.77. Therefore, we finalize the regulatory review cost estimation as approximately $10,601,376.80 ($741.77 × 14,292 reviewers).
38. Overall Impact of the Proposed Payment Notice Individual Provisions
In the regulatory impact analysis of this final rule, we include impact analyses and estimates for each finalized policy separately, as we intend for each provision to be severable from the rest. Please see section III.I. of this final rule for a more detailed discussion on the severability of the provisions of this rule. However, we anticipate that the provisions of this final rule, while severable, may work in concert with each other and affect many of the same individuals seeking coverage through the individual health insurance market. Therefore, the overall impact of this final rule will likely be less than the simple accumulation of the individual provisions' impact analyses. To the best of our ability, we provide overall impact estimates of these provisions for enrollment, premiums, and APTC, that minimize the overlap of individuals affected.
The baseline starts with internal CMS data of enrollment by month, premiums, and APTCs, we summarize the data using average monthly amounts. These monthly averages are projected throughout the year using historical monthly patterns during a similar environment. For future years, the enrollment is trended by the projected growth in the under age 65 population, however, there is a decrease in 2028 enrollment due to the expected impact of the WFTC legislation which is expected to reduce the level of improper enrollments through additional eligibility verification standards. Spending amounts are trended using projected growth in NHEA less Medicare. While effectuated enrollment numbers are unavailable at this time, we have increased the 2026 average baseline enrollment by 1.151 million to 18.861 million compared to the 17.71 million baseline used in the proposed rule based on enrollee activity we have seen so far in 2026. Moreover, our 2027 baseline enrollment is 18.881 million compared to the 17.729 million in the proposed rule. We have also reduced the impact of the under 150 percent FPL SEP that was included in the proposed rule.
Based on the analysis presented thus far in this section, we expect average enrollment for 2027 to decrease between 1.2 and 2 million enrollees compared to baseline estimates. We expect average premium PMPMs to range from 1.2 percent to 1.8 percent lower compared to the baseline scenario before normal premium trends. Many enrollees will discontinue coverage when stronger eligibility verifications identify they are no longer eligible for subsidies, and we believe it is likely that healthier enrollees are more likely to discontinue coverage. The expected worsening of morbidity in the market is offset by protecting against adverse selection with pre-enrollment SEP verification, removal of the SEP for those under 150 percent FPL, and a reduction in exchange user fee charges.
We have estimated a 1.7 percent increase in premiums in the scenario where 1.2 million enrollees leave the market and a 2.4 percent premium increase if 2 million enrollees leave. These premium impact estimates assume the 1.2 million leaving enrollees have average claims expenses that are 75 percent of the average risk pool and the 2 million leaving enrollees have average claims expenses that are 80 percent of the average risk pool. If the average claims PMPM is 86 percent of the premium PMPM (0.86 × $764.28 = $657.28), we estimate the 1.2 million exiting enrollees have claims costs of $492.96 PMPM (0.75 × 657.28 = 492.96), and the remaining 17.681 million enrollees have an average claims cost of $668.44 (1.2/18.881 × 492.96 + 17.681/18.881 × 668.44 = 657.28). Comparing the new claims PMPM of $668.44 to the prior claims PMPM of $657.28 shows a 1.7 percent increase in average claims (668.44/657.28−1 = 0.017). Similarly, if 2 million enrollees leave the market, they are likely to be closer to the average claims cost of the market, so we estimate this population averages 80 percent of the average risk pool cost or $525.83 PMPM (0.80 × 657.28 = 525.83). If 2 million enrollees with average claims cost of $525.83 leave the risk pool, the remaining 16.881 million enrollees would have an average claims cost of $672.86 (2/18.881 × 525.83 + 16.881/18.881 × 672.86 = 657.28), which is 2.4 percent higher than the baseline claims PMPM. Assumptions regarding the relative health of the population leaving the market compared to the health of the average population were further informed considering various economic studies. Consistent with Tebaldi's (2023) research [404]
showing equilibrium in health insurance exchanges demonstrates younger people are more price sensitive and cheaper to cover, we focused on how friction impacts decisions for healthier enrollees. However, research by Deshpande and Li (2019) [405]
and Homonoff and Somerville (2019) [406]
suggest enrollment friction can be a barrier despite potential benefits to the enrollee, so it is not only the young and healthy we should expect to leave the market. Therefore, we reduced the role of health status in explaining how friction impacts enrollment.
These increases are offset by pre-enrollment SEP verification to improve the health of the risk pool from adverse selection by removing opportunities for unauthorized enrollment and plan switches. With loss of enhanced subsidies and an increase in the member shared responsibility payment, an enrollment option always being available encourages healthier individuals to forgo coverage and wait until they are sick to enroll in an
( printed page 29855)
Affordable Care Act plan. These policies help mitigate that risk. We originally assumed 3 to 4 percent premium savings due to eliminating the under 150 percent FPL SEP; however, after consideration of comments and the impact of additional income verifications in the rule that will proactively lower the amount of people determined eligible for this income-based SEP, we have reduced the estimated impact to 2 percent savings in the 1.2 million enrollment scenario and 3 percent savings in the 2 million enrollment scenario. We are also implementing pre-enrollment SEP verification that we estimate will lead to a 0.5 percent premium reduction in the 1.2 million enrollment scenario and a 0.8 percent premium reduction in the 2 million enrollment scenario beginning in 2027.
The FFE user fee is being reduced to 1.9 percent of monthly premiums, and the SBE-FP user fee rate is being reduced to 1.5 percent, so we reduce the premium estimate by 0.4 percent beginning in 2027. The 0.4 percent premium reduction was calculated using total premiums by State to weight the user fee reduction across all States to obtain an overall market premium impact for this change. Overall, after accounting for the market morbidity impact along with policies aimed at mitigating adverse selection, premiums are expected to be 1.2 percent lower in the 1.2 million enrollment scenario and 2.4 percent lower in the 2 million enrollment scenario in 2027 compared to the baseline scenario before normal premium trends.
For the 1.2 million enrollment scenario, premium trend is estimated to increase by 4.5 percent for 2027 and 4 percent the following years. Premium trend is estimated to increase by 6 percent for 2027 and 4.5 percent in the following years for the 2 million enrollment scenario. Starting with a 2026 premium PMPM of $736.36 and applying the adjustments mentioned previously, we arrive at estimated premium PMPMs of $760.66 in the 1.2 million enrollment scenario and $767.28 in the 2 million enrollment scenario [736.36 × (1 + 0.045 + 0.017-0.02-0.005-0.004) = 760.66 and 736.36 × (1 + 0.06 + 0.024-0.03-0.008-0.004) = 767.28]. We assume APTC PMPMs will be approximately 88.5 percent of premium PMPMs, leading to projected 2027 APTC PMPMs of $673.18 for the 1.2 million enrollment scenario and $679.05 for the 2 million enrollment scenario (760.66 × 0.885 = 673.18 and 767.28 × 0.885 = 679.05).
Future enrollment is expected to shrink by 2.3 percent for 2028 as these policies continue to take full effect. We estimate modest enrollment increases of 0.3 percent for 2029 and 0.03 percent for 2030.
While not specifically accounted for in these estimates, we further expect a decrease in average premiums and APTC payments resulting from better estimates of the CSR load factor. By providing guidance that the CSR load factor must be set to only collect expected unpaid CSR amounts and not inappropriately inflate Federal expenditures, the likely result will be reduced benchmark plan premiums in several states which will also cause a shift in metal tier enrollment distribution. These additional premium decreases will potentially lead to net reduction in premium under this final rule.
Comment:
We received comments that addressed the overall impacts of the finalized policies and the lower and upper bound analyses. Some commenters expressed concerns with the enrollment drops estimated in the proposed rule. Other commenters requested additional information on the assumptions that guide the baseline and the impact estimates, including the enrollment and premium impact trends. Some commenters believed that the year-over-year coverage losses should be higher starting in PY 2027 given the interactions of various eligibility provisions. Commenters also believed that the provisions in this rule would lead to increased adverse selection and premiums compared to what was estimated in the proposed rule. One commenter requested HHS to separately calculate premium impacts of each provision and release the underlying data that supports the impact analyses.
Response:
We have updated the overall impact of the finalized policies, including reducing the impact of the 150 percent FPL SEP. As mentioned above, we believe there is likely overlap in the populations affected by these policies, and that is reflected in the estimated enrollment decrease. We also expect the enrollment decreases will result in a morbidity increase to the individual market, leading to an additional 1.7 to 2.4 percent increase in claims and premium as described above.
( printed page 29856)
39. Regulatory Impact Considerations Regarding City of Columbus v. Kennedy
This final rule finalizes updates to policies that were previously finalized with an earlier effective date in the 2025 Marketplace Integrity and Affordability final rule (90 FR 27074), including § 155.305(f)(4) Failure to File and Reconcile (FTR), § 155.320(c)(3)(iii) Income Verification when Data Sources Indicate Income Less than 100 Percent of the FPL, § 155.320(c)(5) Income Verification When Tax Data is Unavailable, and § 155.420(g) Pre-Enrollment Special Enrollment Period Verification. Although these policies were initially finalized in the 2025
( printed page 29857)
Marketplace Integrity and Affordability final rule with a sunsetting at the end of PY 2026, they are currently stayed by the court.[407]
While we cannot postulate on active judicial proceedings, we have considered the regulatory impact if this stay was lifted and these provisions from the 2025 Marketplace Integrity and Affordability final rule became effective. If the stay is lifted in PY 2026, these provisions may become effective in PY 2026, but there still may be an operational delay in effectuating the policies. If the provisions become effective in PY 2026, the regulatory impacts that were estimated in the 2025 Marketplace Integrity and Affordability final rule would be in effect for PY 2026. From PY 2027, the ongoing regulatory impacts that are estimated in this final rule would be in effect. Any costs to sunset the provisions that were estimated in the 2025 Marketplace Integrity and Affordability final rule would be nullified if this final rule is finalized as proposed because the policies would continue beyond PY 2026. We do not anticipate additional impacts beyond what has been estimated in the 2025 Marketplace Integrity and Affordability final rule and this final rule. If the court stay is lifted after PY 2026 and this rule is finalized as proposed, we do not anticipate additional regulatory impacts from the court decision, as the policies in this final rule will be in effect, and we have estimated the regulatory impacts under the relevant provisions in this final rule.
Due to the uncertainties mentioned previously, we are unable to further quantify the impact regarding the active court proceedings. We sought comment on these estimates and assumptions.
We did not receive any comments in response to these proposed impact estimates. For the reasons outlined in the proposed and final rules, we are finalizing these estimates as proposed.
D. Regulatory Alternatives Considered
CMS created a Frequently Asked Questions (FAQ) document to help address the issue of what is considered “taking an action” as it relates to regulatory requirements for creating documentation related to eligibility application review and consumer consent, as per § 155.220(j)(2)(ii)(A) and (j)(3)(iii)(A), respectively. However, adding this language solely to sub-regulatory guidance, such as an FAQ, would not provide HHS with the necessary enforcement authority when we are reviewing documentation submitted by agents/brokers related to documenting consumer eligibility application requirements and consent documentation. Therefore, it was determined that updating the regulations in § 155.220 was necessary.
When developing the finalized proposal to expand the marketing regulations to improve our enforcement authority related to misleading marketing, we considered creating an FAQ document to notify agents, brokers, and web-brokers of certain prohibited behaviors related to marketing practices. However, adding this language solely to sub-regulatory guidance, such as an FAQ document, would not provide HHS with the necessary enforcement authority when we discover misleading marketing. Therefore, it was determined that updating the regulations in § 155.220 was necessary.
In developing the SEIPM policies contained in this final rule (§ 155.1600), we considered the lessons learned while implementing IPPTA. During IPPTA, HHS engaged with 19 State Exchanges to test measurement processes. We considered several data collection options and chose the primary option as that which provides the greatest amount of reliability and flexibility in providing the data that supports the payment decisions and calculations of APTC made by State Exchanges.
In regard to the finalized SEIPM, HHS considered several alternative approaches. For the implementation timeline, HHS considered alternative implementation timelines for SEIPM beyond the finalized January 1, 2027 effective date. Alternatives for extending the implementation timeline to 2028 or 2029 were considered as they would have provided HHS the window to evaluate all of the results from IPPTA as well as afford State Exchanges with additional preparation time. Delaying the implementation beyond 2027 would delay HHS' ability to meet PIIA requirements for comprehensive improper payment measurement across all APTC programs. The January 2027 effective date balances the need for adequate State Exchange preparation time with Federal statutory obligations, particularly given the foundational framework established through the IPPTA with the large bulk of operational processes associated with collecting information from the State Exchanges being completed. IPPTA will continue through the end of 2026 and we will continue to assess lessons learned for incorporation into the SEIPM implementation.
For the data collection requirements, HHS evaluated alternate approaches that would have required more limited data submissions from State Exchanges. One alternative considered was limiting data collection to only basic enrollment and payment information, which would have reduced State Exchange burden but would not have provided sufficient detail to conduct comprehensive improper payment reviews that meet PIIA standards. For sampling methodology, HHS considered alternative approaches to the proposed stratified random sampling methodology. One alternative considered was using a simple random sampling approach without stratification, which would have been easier to implement but would have been less efficient in detecting errors and would have required larger sample sizes to achieve the same level of statistical precision. HHS also considered implementing a static sample size approach that would have applied the same sample size across all State Exchanges regardless of their APTC volume or operational characteristics. While this approach would have simplified program administration and ensured consistent measurement effort across all participating Exchanges, it would have resulted in imprecise estimates for smaller State Exchanges and inefficient resource allocation for larger Exchanges, failing to optimize statistical precision relative to program risk and Federal investment. HHS also evaluated implementing more prescriptive enforcement mechanisms with automatic penalties for noncompliance but determined that the proposed graduated enforcement approach with due process protections and opportunities for corrective action better supports the collaborative relationship necessary for successful program implementation while maintaining appropriate accountability for State Exchange compliance with Federal oversight requirements.
Finally, in considering the SEIPM, we evaluated the option of publishing individual rates for each SBE, rather than an aggregate rate for all State Exchanges. Achieving an appropriate level of precision (that is, a margin of error less than +/−5 percent) for such an approach, however, would require doubling the sample sizes used which would incur an additional $25 million Federal and $1.5 million State cost annually. Therefore, we did not adopt this approach.
In considering modifications to the programmatic audit requirements under § 155.1200(c), HHS evaluated several alternatives. These included maintaining the existing audit requirement for State Exchanges that
( printed page 29858)
complete the SEIPM for a given benefit year, as well as allowing SEIPM to fully satisfy the audit requirement under § 155.1200. Maintaining the current audit requirement would have resulted in duplicative reviews and increased administrative burden for State Exchanges, while allowing SEIPM to replace the audit entirely would have reduced the comprehensiveness of oversight currently provided.
In developing this finalized policy to require issuers that make plan-level adjustments to account for unreimbursed CSRs to submit specified CSR data elements in the URRT and Actuarial Memorandum, HHS considered several alternative approaches. One alternative considered was to maintain the current policy as outlined in the 2025 Rate Filing Guidance, which would have continued to rely on reporting of CSR-related information in the Actuarial Memorandum without adding explicit URRT fields. However, this approach would not have achieved the policy goal of ensuring consistency and comparability across issuers and States in the reporting of CSR load methodologies and amounts. HHS also considered permitting issuers to use alternative or simplified methodologies for estimating CSR amounts paid on behalf of enrollees, leveraging existing internal calculations that may vary by issuer. While this approach could have reduced issuer burden, it would have resulted in inconsistent data and limited the ability of State and Federal regulators to assess whether CSR load adjustments are actuarially justified. Finally, HHS considered not requiring submission of CSR data at all, leaving such determinations entirely to State review processes. However, this would not have provided HHS and State regulators with standardized, plan-level information needed to ensure transparency and regulatory oversight of CSR loading practices. The finalized approach—requiring consistent data reporting through the URRT and Actuarial Memorandum using the standard methodology under § 156.430(c)(2)—balances the need for improved data comparability and regulatory oversight with the goal of minimizing additional issuer burden by leveraging existing data and familiar calculation methodologies.
We considered maintaining the vendor program, which would allow the opportunity for approved third-party vendors to facilitate agent and broker annual registration and training in addition to having the training and registration process available through the CMS Marketplace Learning Management System (MLMS), but determined the benefits of terminating the vendor program outweighs the costs of maintaining the existing policy with both programs. As such, we did not consider other regulatory alternatives, as removing § 155.222, which would allow HHS to sunset the vendor program, would maintain agent and broker accessibility to training and registration while reducing costs.
We provided examples of alternatives that we considered but did not implement when confronting the incongruence between section 1302(c) through (e) of the PPACA, such as trending the AV Calculator to account for changes in the standard population. However, we believe such a change would make the AV Calculator likely contrary to of the Affordable Care Act and generally accepted actuarial standards. Therefore, we do believe that a real conflict exists, and that the best way to solve the conflict is to give issuers the flexibility, at their option, to offer bronze plans exceeding the standard annual limitation on cost sharing as long as they offer a bronze plan that meets the standard annual limitation on cost sharing per § 156.136, and further differentiate catastrophic plans through a higher required annual limitation on cost sharing per § 156.155(3)(a)(ii).
We considered a range of regulatory alternatives for the finalized policy to discontinue the full suite of standardized plan options policies effective beginning in PY 2027. Under the finalized provision, we will remove the following from our regulations: the definition of “standardized option” at § 155.20; all requirements pertaining to standardized plan options at § 156.201 (the requirements for FFE and SBE-FP QHP issuers in the individual market to offer these plans at paragraphs (a) and (b) as well as the requirement for these plans to meaningfully differ from one another at paragraph (c)); the differential display of standardized plan options on
HealthCare.gov
at § 155.205(b)(1); and the corresponding standardized plan option differential display requirements for approved web-broker and QHP issuer enrollment partners using a DE pathway to facilitate consumer enrollment through an FFE or SBE-FP at §§ 155.220(c)(3)(i)(H) and 156.265(b)(3)(iv), and non-standardized plan option limits and exceptions at § 156.202. Finally, we are finalizing our proposal to cease the annual design and publication of these plans in the applicable Payment Notice rulemaking for each plan year.
We considered several regulatory alternatives that could potentially allow us to achieve the same goals of simplifying the plan selection process and reducing burden without discontinuing this suite of policies in its entirety. In particular, we considered continuing to require issuers to offer standardized plan options but only at particular metal levels, such as the bronze and silver metal levels (instead of at every metal level at which they offer non-standardized plan options). We also considered requiring issuers to offer standardized plan options only in certain service areas in which they offer a certain number of non-standardized plan options. We also considered transitioning from requiring issuers to offer these standardized plan options to once more allowing issuers to voluntarily offer them—as was the approach with the previous iteration of the policy—while we continue to maintain the differential display of these plans on
HealthCare.gov
and the DE pathways. We also considered resuming a revised version of the meaningful difference standard, which was previously codified at § 156.298.
However, based on our experience administering this suite of policies from PY 2023 through PY 2026, we have determined that this suite of policies has failed to meaningfully enhance the consumer experience, increase consumer understanding, and simplify the plan selection process—our originally articulated objectives. Furthermore, imposing these requirements has increased burden for both issuers and HHS (for example, by requiring issuers to create and submit certification applications for additional plans), impeded issuer innovation in plan design, unnecessarily constrained consumer choice, and caused significant market disruption. Additionally, based on our experience administering the previous iteration of this suite of policies from PY 2017 through 2019 (when standardized plan options were voluntary and when there was no non-standardized plan option limit), we do not believe it would be an effective approach to once more revert to making it voluntary for issuers to offer these plans. This is primarily because when there was no requirement for issuers to offer these plans, few issuers chose to offer them, and fewer consumers chose to enroll in them.
Furthermore, we do not believe HHS is positioned to impose a “one size fits all” approach standardized plan option designs for an environment as heterogenous as the FFEs (such as in terms of consumer demographics, health care needs, and preferences). We refer readers to the preamble section for the finalized policy to discontinue
( printed page 29859)
standardized plan options (§§ 155.20, 155.205(b)(1), 155.220(c)(3)(i)(H), 156.201, and 156.265(b)(3)(iv)) for a detailed discussion of relevant literature we considered in our finalized policy to discontinue the full suite of standardized plan option limits policies. Finally, given that we previously discontinued standardized plan options at a time when the individual market was considered to be at risk of destabilization, and given that there are a range of substantive changes in the present environment, we believe that now is not an appropriate time to once again add to that complexity.
We considered making the provisions requiring income verification when tax data is unavailable and income verification when trusted data sources indicate income less than 100 percent of the FPL optional for State Exchanges that demonstrate improper payment rates (that is, SEIPM) below the Federal rate (that is, FEIPM). Under the current finalized policy, we will impose these requirements on all Exchanges starting in PY 2027. We considered this regulatory alternative in light of the fact that some analysis [408]
has shown that erroneous or improper enrollments are less widespread in State Exchanges than in Exchanges on the Federal platform and due to the significant annual administrative costs (that is, a combined $75 million annually) that would be incurred by States in implementing these provisions. Under this regulatory alternative these provisions would be optional for State Exchanges so long as they maintained a SEIPM below the FEIPM in any given year. If a State Exchange's SEIPM meets or exceeds the FEIPM in any year then, under this regulatory alternative, these integrity provisions would be imposed on that State Exchange in the subsequent year and would remain in effect unless the State Exchange demonstrated a SEIPM below the FEIPM for three subsequent consecutive years (at which point these provisions would revert to being optional for the State Exchange). While this approach could strike a balance between the need to safeguard program integrity and mitigate administrative costs, the SEIPM will not be fully implemented until at least PY 2029. Additionally, we note that implementation of this regulatory alternative would be administratively burdensome and would require a doubling of sample sizes (resulting in an additional $25 million Federal and $1.5 million State costs annually) to ensure a sufficiently precise margin of error. Since this regulatory alternative would significantly delay implementation of these vital program integrity measures, would impose additional administrative cost and complexity, and would fail to fully address known program integrity issues, it was determined to impose these requirements on all Exchanges starting in PY 2027.
We considered taking no action regarding modifications to § 155.400(g), which would have allowed the FFE, SBE-FPs, and State Based Exchanges to allow issuers to adopt a fixed-dollar premium payment threshold and/or a gross premium-based percentage payment threshold. We also considered removing just the gross premium fixed-dollar threshold policy and allowing issuers the option to utilize the fixed-dollar premium threshold, since the gross premium percentage-based threshold could allow an enrollee with a larger gross premium to remain enrolled in coverage for a longer period of time and accumulate a higher amount of debt. However, given the continued numbers of improper enrollments and plan switches and other improper enrollment trends, both the fixed-dollar and gross-premium percentage-based thresholds present program integrity risks that may allow consumers (and Medicaid beneficiaries who are victims of dual improper enrollment into a QHP) to remain in coverage for a much longer or indefinite amount of time, after payment of the binder. Consumers who never wanted, or no longer need, QHP coverage could remain enrolled for longer than the 3-month grace period, accruing premium debt and potentially facing complications when they file their taxes. Issuers will still have the option to implement the existing net premium percentage-based policy to allow consumers who pay the majority of their premium to avoid being put into a grace period.
E. Regulatory Flexibility Act (RFA)
The RFA requires agencies to analyze options for regulatory relief of small entities, if a rule has a significant impact on a substantial number of small entities. The RFA generally defines a “small entity” as (1) a proprietary firm meeting the size standards of the Small Business Administration (SBA), (2) a not-for-profit organization that is not dominant in its field, or (3) a small government jurisdiction with a population of less than 50,000. Individuals and States are not included in the definition of a “small entity.”
1. Legislative and Regulatory Overview
Title I of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) added a new title XXVII to the PHS Act to establish various reforms to the group and individual health insurance markets. These provisions of the PHS Act were later augmented by other laws, including the Affordable Care Act. Subtitles A and C of title I of the Affordable Care Act reorganized, amended, and added to the provisions of part A of title XXVII of the PHS Act relating to group health plans and health insurance issuers in the group and individual markets. The term “group health plan” includes both insured and self-insured group health plans. For summarized sections of the PHS Act and Affordable Care Act, please see section II.A. of this final rule.
These finalized provisions revise current regulations, and HHS does not anticipate any duplication, overlap, or conflict with other rules and regulations associated with these rules.
2. Need for Regulatory Action and Objectives
For the purposes of the RFA, we believe the following provisions could impact smaller agent, broker, and web broker firms.
a. Mandating the HHS-Approved and -Created Consumer Consent Form—Eligibility Application Review and Documenting Receipt of Consumer Consent (§ 155.220(j))
We are finalizing amendments to §§ 155.220(j)(2)(ii)(A) and (j)(2)(iii)(A) to require agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review requirements and consent documentation requirements. Our finalized policy will eliminate the current broad allowances for meeting these requirements. The language in the regulation will also be changed to clarify what types of actions constitute “taking an action” to meet the regulatory requirements. The goal of this policy is to reduce confusion among agents, brokers, and web-brokers on what constitutes compliant eligibility application review documentation and what constitutes compliant consumer consent by ensuring objective standards, which protects consumers ultimately. These policies also greatly improve HHS' investigative abilities into agent, broker, and web-broker eligibility application review and consumer consent review by creating a clear and objective standard for all applications clearly outlining what HHS deems
( printed page 29860)
complaint. More information about this provision is available in section V.C.8. of this final rule.
b. Misleading Marketing (§ 155.220(j)(3))
The finalized regulatory amendments create a new standards of conduct section in § 155.220(j) describing marketing requirements. These requirements will list certain prohibited practices, provide HHS audit authority, and put agents, brokers, and web-brokers on notice that they are responsible for marketing created by their downstream entities. This finalized policy will allow HHS to increase its efforts to engage in compliance actions for misleading marketing by providing agents, brokers, and web-brokers notice of the types of activities that are prohibited, allowing HHS to review marketing materials for compliance, and ensure agents, brokers, and web-brokers are not able to push responsibility to third-parties. Creating a marketing standards of conduct section is necessary to protect consumers and maintain the integrity of the Exchanges. More information about this provision is available at section V.C.9. of this final rule.
For the purposes of the RFA, we believe the following provisions could impact smaller insurers.
c. Submission of Rate Filing Justification (§ 154.215)
The final rule will require issuers to report actual CSR amounts paid in the Market Experience section (2 years prior, using the standard methodology), projected CSR amounts in the current filing year in the Projections section, and CSR load factors in a new dedicated line item, among other proposed requirements. Issuers would also be required to provide an explanation of how these data points were used to determine the CSR load as part of the Actuarial Memorandum.
The finalized provisions will primarily affect health insurance issuers offering qualified health plans in the individual market, Federal and State regulators in their review capacity, and indirectly, Marketplace enrollees who receive cost-sharing reductions. The enhanced CSR reporting will enable issuers to more accurately determine their CSR payment amounts and improve future projections for rate setting. This could result in more appropriate premium levels if current CSR load factors are inaccurate or unreasonable, enabling issuers to better calibrate their load factors to adequately cover actual CSR costs, potentially leading to more stable and accurate premium pricing over time. More information is available at section V.C.3. of this final rule.
d. Amendments To Strengthen HHS' Oversight of the Administration of the Advanced Payments of the Premium Tax Credit, Cost-Sharing Reductions, and User Fee Programs and Clarifying HHS' Compliance Review Authority (§ 156.480)
We are finalizing our proposal to modify § 156.480 to clarify HHS' authority to audit or conduct a compliance review to assess issuers' compliance with requirements related to the APTC, CSR, and user fee programs. Specifically, we are clarifying that under § 156.480(c), HHS or its designee may audit or conduct a compliance review to assess compliance with all requirements related to APTC, CSR, and user fee programs applicable to issuers offering a QHP in an Exchange. For consistency, we also are finalizing conforming changes to § 156.480(c)(6) to provide that in instances where HHS enforces compliance with any requirements related to APTC, CSR, and user fee programs for QHP issuers participating in State Exchanges or SBE-FPs, HHS may do so in accordance with § 156.805. We also are clarifying that the compliance review authority in § 156.480(c) allows for compliance reviews as needed or on an annual basis. More information about this provision is available at section V.C.32. of this final rule.
3. Number of Affected Small Entities
For purposes of the RFA, we believe that health insurance issuers and group health plans would be classified under the North American Industry Classification System (NAICS) code 524114 (Direct Health and Medical Insurance Carriers) or possibly be classified in 621491 (HMO Medical Centers). Based on latest available Statistics of U.S. Businesses (SUSB) data, 1,071 and 146 total firms fall under NAIC codes 524114 and 621491, respectively.[409]
According to SBA size standards, entities with average annual receipts of $47 million or less would be considered small entities for NAICS code 524114 and $44.5 million or less for NAICS code 621491.[410]
SUSB data confirms there are no small firms within NAIC code 621491. However, we believe that few, if any, insurance companies underwriting comprehensive health insurance policies (in contrast, for example, to travel insurance policies or dental discount policies) fall below these size thresholds. Based on data from MLR annual report submissions for the 2023 MLR reporting year, approximately 84 out of 479 issuers of health insurance coverage nationwide had total premium revenue of $47 million or less.[411]
Furthermore, it should be noted that approximately 80 percent of these small issuers belong to larger holding groups based on the MLR data, and many, if not all, of these small companies are likely to have non-health lines of business that result in their revenues exceeding $47 million.[412]
Therefore, we assume approximately 20 percent, or 16, of the 84 potential small issuers are in fact small issuers for purposes of this analysis. We believe this is an overestimate, as many if not all of these small issuers are likely to have non-health lines of business that result in their revenues exceeding $47 million, but we use 16 small issuers for purposes of this analysis. We sought comment on these estimates.
For purposes of the RFA, the Department consider agents, brokers, and web brokers classified under NAICS code 524210 (Insurance Agencies and Brokerages) that have annual receipts of $15 million or less to be small entities. According to the 2022 Statistics of U.S. Businesses data,[413]
there are 120,434 firms in the Insurance Agencies and Brokerages industry, of which 119,114, or approximately 99 percent, had annual receipts below the $15 million size standard. Nearly all agents, brokers, and web brokers affected by this final rule would therefore be small entities.[414]
4. Regulatory Impacts and Alternatives
For the purposes of this RFA, the costs per agent, broker, and web broker summarized in sections V.C.8. and V.C.9. are expected to be representative of the average costs that would be incurred by small agents, brokers, and web brokers to comply with the provisions in this final rule. We outline
( printed page 29861)
those assumptions and estimates later in this section.
Regarding the costs related to requiring small agents, brokers, and web-brokers to use the HHS-approved and -created consumer consent form to meet the eligibility application review documentation requirements and the consumer consent documentation requirements, we estimate it would take approximately 10 minutes of time for an enrolling agent, broker or web-broker to meet eligibility application review documentation requirements and to obtain consumer, or their authorized representative, affirmation of their consent. Using the current adjusted hourly wage rate of $58.04 [415]
for an insurance sales agent, each enrollment using the HHS-approved and -created consumer consent form would have approximately $9.87 (10 minutes, or 0.17 hours, at an hourly wage rate of $58.04) in additional cost associated with it based on the extra time commitment from these finalized policy changes. The total cost for small agents, brokers, and web-brokers would be contingent on the number of policies enrolled by each small firm, with the upper bound estimate being 9.8 million policies estimated for all agents, brokers, and web brokers regardless of firm size. Please see sections IV.C. and V.C.8. of this final rule for more information.
As stated in IV.D of this final rule, we do not anticipate many costs for the agents, brokers, or web-brokers we investigate for misleading marketing. We believe responding to HHS requests to provide confirmation they removed the ads and/or reviewed the marketing guidelines would not be overly time-consuming or burdensome. Our notifications to the agents, brokers, or web-brokers detail what response is required and provide hyperlinks to the noncompliant ad(s). We estimate it would take each agent, broker, or web-broker one hour to remove any noncompliant ad(s), and/or review the marketing guidelines, and respond to HHS via email. This estimate incorporates the potential of HHS asking these agents, brokers, and web-brokers to provide advertisements for HHS' review. Using the hourly wage rate for an insurance sales agent from Table 14 in section IV.A. of this final rule ($58.04), the cost of responding to HHS would be $58.04 per response. The total cost for small agents, brokers, and web-brokers would be contingent on the number of responses from these smaller firms, with the upper bound estimate being 24 responses estimated for all agents, brokers, and web brokers regardless of firm size. Please see sections IV.D. and V.C.9. of this final rule for more information.
For the purposes of this RFA, the costs per issuer summarized in sections V.C.3. and V.C.32 of this final rule are expected to be representative of the average costs that would be incurred by small issuers to comply with the provisions in this final rule. We outline those proposed assumptions and estimates later in this section.
As discussed in section III.C. of this final rule, this rule is finalizing our proposal to change the instructions for the URRT so that issuers will enter the actual amount of CSRs they paid for enrollees (2 years prior), the amount of CSRs they expect to provide to enrollees, and add a new field to gather the “load amount.” Issuers will incur ongoing burden to gather the three required values and enter them into the URRT in their appropriate places. The annual cost and burden per issuer to update and run the standard methodology calculations is $572,118 at 5,700 hours. The annual cost and burden per issuer to provide CSR related information in the URRT is $429.47 at 3.6 hours. The annual cost and burden per issuer to provide CSR calculation explanations in the Actuarial Memorandum is $1,718.27 at 14.2 hours. The total annual ongoing cost for 16 small issuers is $9,188,251.84 at 91,488 hours. We estimate that each issuer will incur an initial one-time cost of $1,114,236 at 11,400 burden hours in 2026 to develop and implement a claim-level re-adjudication process using the standard methodology set forth in § 156.430 to produce the required values, which totals $17,827,776 at 182,400 for 16 small issuers. Please see sections IV.B. and V.C.3. of this final rule for more information.
In regard to modifying § 156.480 to clarify HHS' authority to audit or conduct a compliance review to assess issuers' compliance with requirements related to the APTC, CSR, and user fee programs, we estimate that the audits that we conduct under this authority will not impose additional costs beyond what is already accounted for in the audit review process (86 FR 24140, 24281). We estimate that it will take a business operations specialist 10 hours (at a rate of $78.14 per hour) to compile and submit data and other information necessary for a compliance review. We estimate it will take a compliance officer (at a rate of $75.40 per hour) 4 hours to review and sign off on the submission. The cost per issuer to develop and submit the compliance information would be approximately $1,083. The total cost for small issuers is contingent on the number of small issuers selected for a compliance review each year (out of the 150 estimated regardless of firm size in section V.C.32. of this final rule). Please see section V.C.32. of this final rule for more information.
We anticipate small issuers could be impacted by other provisions in this final rule. However, we are unable to quantify the impact of these changes on small issuers due to uncertainty regarding their market share, market participation, membership in larger holding groups, enrollment and risk mix, and APTC receipts. However, we anticipate that there would not be a significant change in revenue for issuers as a reduction in APTC payments would mean consumers would be responsible for the balance of the premium not covered by APTC. Yet, we also acknowledge that due to the reductions in enrollment anticipated to result from the policies in this final rule, including the potential reduction in APTC to consumers resulting in increased premiums and choosing not to maintain coverage due to affordability constraints, issuers may experience a reduction in premium revenue. However, we anticipate this could be balanced by a reduction in claims experience, and we are unable to quantify this impact on small issuers due to uncertainty.
The data and conclusions presented in this section, along with the rest of the RIA, amount to our final regulatory flexibility analysis under the RFA.
We sought comment on the estimates and assumptions.
Comment:
Some commenters noted concerns that small agencies may be disproportionately affected by the compliance burdens in the rule, which could operationally impact the small agencies, reduce small agent participation, and have downstream impacts on consumers such as potentially limiting consumer choice, increasing consumer confusion, longer wait times for assistance, and lower enrollment rates. One commenter requested HHS to evaluate the administrative burdens on small agencies.
Response:
We acknowledge the concerns noted by commenters that smaller entities may be disproportionately affected by the burdens in this final rule, which could ultimately impact consumers. Our impact estimates were calculated based on assumptions that would be
( printed page 29862)
applicable across firm sizes, and we do not anticipate disproportionate impact on smaller entities. Similarly, we do not anticipate disproportionate impact on consumers of small agencies as a result of provisions in this final rule. Where possible to quantitatively estimate, we have provided the regulatory impacts on small entities, including the administrative burdens, in V.E.4. of this final rule.
For the reasons outlined in the proposed and final regulatory flexibility analyses, we are finalizing the previous estimates.
As discussed in section V.C.37. of this final rule, we anticipate that entities such as issuers, including small issuers and agents/brokers, would face regulatory review costs as a result of needing to familiarize themselves with this final rule. The cost per entity to review this final rule is estimated to be $741.77. The total cost for 16 small issuers to review this rule is estimated to be $11,868.32. We anticipate that agents, brokers, and web brokers would also incur costs to review this final rule, however, we do not have reliable data on the number of agents, brokers, and web brokers that would review this rule and therefore do not estimate the total burden for these entities. We sought comment on the number of agents, brokers, and web brokers that may review this rule and the associated costs.
We did not receive any comments in response to our proposed regulatory review costs. Therefore, we are finalizing these estimates.
For regulatory alternatives considered regarding the provisions in this final rule, please see section V.D. of this final rule.
5. Impact on Small Rural Hospitals
In addition, section 1102(b) of the Act requires us to prepare a regulatory impact analysis if a rule may have a significant impact on the operations of a substantial number of small rural hospitals. This analysis must conform to the provisions of section 604 of the RFA. For purposes of section 1102(b) of the Act, we define a small rural hospital as a hospital that is located outside of a metropolitan statistical area and has fewer than 100 beds. While this final rule is not subject to section 1102 of the Act, we have determined that this rule would not affect small rural hospitals. Therefore, we anticipate this final rule would not have a significant impact on the operations of a substantial number of small rural hospitals.
F. Unfunded Mandates Reform Act (UMRA)
Section 202 of the Unfunded Mandates Reform Act of 1995 (UMRA) also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2026, that threshold is approximately $193 million. Although we have not been able to quantify all costs, we expect that this final rule would not impose a mandate that would result in the expenditure by State, local, and Tribal Governments, in the aggregate, or by the private sector, of more than $193 million in any 1 year.
G. Federalism
Executive Order 13132 establishes certain requirements that an agency must meet when it issues a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on State and local governments, preempts State law, or otherwise has Federalism implications.
In compliance with the requirement of E.O. 13132 that agencies examine closely any policies that may have Federalism implications or limit the policy making discretion of the States, we have engaged in efforts to consult with and work cooperatively with affected States, including participating in conference calls with and attending conferences of the NAIC, and consulting with State insurance officials on an individual basis.
While developing the proposed rule and this final rule, we attempted to balance the States' interests in regulating health insurance issuers with the need to ensure market stability. By doing so, we complied with the requirements of E.O. 13132.
Because States have flexibility in designing their Exchange and Exchange-related programs, State decisions would ultimately influence both administrative expenses and overall premiums. States are not required to establish an Exchange or risk adjustment program. For States that elected previously to operate an Exchange, those States had the opportunity to use funds under Exchange Planning and Establishment Grants to fund the development of data. Accordingly, some of the initial cost of creating programs was funded by Exchange Planning and Establishment Grants. After establishment, Exchanges must be financially self-sustaining, with revenue sources at the discretion of the State. Current State Exchanges charge user fees to issuers.
In our view, while this final rule will not impose substantial direct requirement costs on State and local governments, this regulation has Federalism implications due to potential direct effects on the distribution of power and responsibilities among the State and Federal Governments relating to determining standards relating to health insurance coverage that is offered in the individual and small group markets.
We have examined the federalism implications involved in finalizing our proposal to revise § 155.170(a) to provide that any State-required benefits would be considered “in addition to EHB” (and thus not an EHB) if they are: required by a State action taking place after December 31, 2011; applicable to the small group and/or individual markets; specific to required care, treatment, or services; and not required by State action for purposes of compliance with Federal requirements. While developing this finalized policy, we considered our longstanding engagement with States regarding their benefit mandates and the operation and impact of the statutory defrayal requirement, including discussions with State insurance officials over time about how State mandates affect affordability and Federal and State financial impacts. In developing this finalized policy, we sought to balance States' interests in regulating health insurance issuers with the need to promote market stability and affordability, and we believe this approach appropriately respects State authority while advancing the objectives of the Affordable Care Act. As finalized, we expect that there would be increased costs to any States that would have to defray the cost of benefits that would be considered “in addition to EHB.”
In addition, we believe this final rule does have Federalism implications due to system and operation costs associated with requiring the four State Exchanges that process their own hardship exemptions to process the additional hardship exemptions expected due to the amendment to § 155.605(d)(1) in this final rule. However, the Federalism implications are mitigated as this final rule would not preempt State law, as it provides States with flexibility to either process hardship exemptions themselves or delegate this function to HHS under existing regulatory provisions at § 155.605(d), thereby avoiding any Federalism implications that would trigger the requirements of Executive Order 13132.
Additionally, in this final rule, HHS finalizes new State flexibilities for provider access reviews and/or ECP certification reviews, which have
( printed page 29863)
federalism implications for FFE States, including States performing plan management. Specifically, CMS is finalizing that FFE States may elect to conduct their own provider access reviews and/or ECP certification reviews of issuers' plans, with a provider network in PY2027, and beginning in PY2028, plans without a provider network, that apply for QHP certification to be offered through an FFE (including States that perform plan management), provided that CMS determines the State has sufficient authority and the technical capacity to conduct such reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program for provider access certification reviews, and/or an Effective ECP Review Program for ECP certification reviews. An FFE State would have the choice to elect to conduct their own provider access certification reviews, ECP certification reviews, or both reviews provided the FFE State satisfies the applicable criteria for each respective effective review program it wishes to administer. For additional detailed information on the federalism impacts of these finalized policies, please reference the discussions in sections V.C.20. for Modification of Exchange Network Adequacy Standards, V.C.29 for Provider Access Standards for Network Plans, and V.C.30 Essential Community Provider Standards of this final rule.
Additionally, we believe this final rule also has Federalism implications for both policies related to income verification in cases where a consumer attests to an income at or above 100 percent of the FPL but the IRS returns data below 100 percent of the FPL as well as in cases where the IRS returns no income data for a household. Specifically, States will incur one-time implementation costs as well as annual operating costs for the policies, and, in the case of the below 100 percent FPL policy, requiring State Exchanges to set continue the income verification when IRS returns data below 100 percent of the FPL but households attest to income at or above 100 percent of the FPL. However, this is mitigated by no longer requiring Exchanges to accept attestations in cases where the IRS returns no income for a household. Additionally, the Federalism implications are mitigated by the benefits to ensuring Marketplace stability, particularly through addressing continued potential fraud.
We also believe this final rule has Federalism implications for the amendment of the failure to file and reconcile policy at § 155.305(f)(4) in this final rule. Specifically, States will incur one-time implementation costs as well as annual operating costs for their failure to file and reconcile policies. Federalism implications are mitigated by the benefits to the Marketplace by removing unauthorized enrollments and lessening the potential for consumers to generate potentially large tax liabilities.
In addition, we believe this final rule's provisions related to cost sharing for catastrophic plans at § 156.155(3)(a)(ii) and for some bronze plans at § 156.136 present implications for State authority and impact, but do not rise to the definition set in Executive Order 13132 because Section 1302(c)(1) of the Affordable Care Act establishes the annual limitation on cost sharing that applies to health plans offered in the individual and small group markets, and we are only reiterating that States may not set a different annual limitation on cost sharing than the limitation established under section 1302(c)(1) of the Affordable Care Act, nor may States set a different limit under existing statute. States may decline to certify plans designed with the flexibility we are finalizing to allow higher annual limitation on cost sharing than previously permitted. The optionality of the sale of these plans further shows that this this rule does not impose substantial direct compliance costs on State and local governments beyond those already required by the existing statutory framework, nor does it set a standard that would preempt State law. Rather, this rule provides additional flexibility within the boundaries Congress established, and it does not alter the fundamental statutory relationship between Federal and State authority for the annual limitation on cost sharing.
H. E.O. 14192, “Unleashing Prosperity Through Deregulation”
Executive Order 14192, entitled “Unleashing Prosperity Through Deregulation” was issued on January 31, 2025, and requires that “any new incremental costs associated with new regulations shall, to the extent permitted by law, be offset by the elimination of existing costs associated with at least 10 prior regulations.” This rule is exempt from otherwise-applicable requirements under E.O. 14192, per footnote 1 of OMB's Accounting Methods.[416]
I. Congressional Review Act
This final regulation is subject to the Congressional Review Act provisions of the Small Business Regulatory Enforcement Fairness Act of 1996 (5 U.S.C. 801et seq.) and has been transmitted to the Congress and the Comptroller General for review.
Mehmet Oz, Administrator of the Centers for Medicare & Medicaid Services, approved this document on May 11, 2026.
For the reasons set forth in the preamble, the Department of Health and Human Services and the Centers for Medicare & Medicaid Services amends 42 CFR part 600 and 45 CFR subtitle A, subchapter B, as set forth below:
( printed page 29864)
Title 42
PART 600—ADMINISTRATION, ELIGIBILITY, ESSENTIAL HEALTH BENEFITS, PERFORMANCE STANDARDS, SERVICE DELIVERY REQUIREMENTS, PREMIUM AND COST SHARING, ALLOTMENTS, AND RECONCILIATION
1. The authority citation for part 600 continues to read as follows:
Authority: Section 1331 of the Patient Protection and Affordable Care Act of 2010 (Pub. L. 111-148, 124 Stat. 119), as amended by the Health Care and Education Reconciliation Act of 2010 (Pub. L. 111—152, 124 Stat. 1029).
2. Section 600.5 is amended by adding the definition of “Eligible noncitizen” in alphabetical order as follows:
Factors CMS uses to determine the amount of penalty.
In determining the amount of any civil money penalty, CMS will identify the lawful purpose or purposes of the penalty, and take into account the following factors as appropriate to the circumstances of the case:
* * * * *
PART 155—EXCHANGE ESTABLISHMENT STANDARDS AND OTHER RELATED STANDARDS UNDER THE AFFORDABLE CARE ACT
5. The authority citation for part 155 continues to read as follows:
(2) Submit an Exchange Blueprint application for HHS approval at least 15 months prior to the date on which the Exchange proposes to begin open enrollment as a State Exchange.
(i)
Public notice.
Upon submission of an Exchange Blueprint application to operate a State Exchange, the State shall issue a public notice of its Exchange Blueprint application submission through its website and include a copy of the Exchange Blueprint application, a description of the Plan Year for which the State seeks to transition to a State Exchange, language indicating that the State is seeking approval from HHS to transition to a State Exchange, and information about when and where the State will conduct public engagements regarding the State's Exchange Blueprint application, as described in paragraph (a)(2)(ii) of this section.
(ii)
Public engagements.
After a State issues its public notice as described in paragraph (a)(2)(i) of this section and until HHS approves, or conditionally approves, the State's Exchange Blueprint application, a State must conduct at least one public engagement (such as a townhall meeting or public hearing) either in-person or virtually, regarding the State's Exchange Blueprint application progress, in a timeline and manner considered effective by the State and with HHS' concurrence. A State shall provide public notice of the public engagement. Such public engagement shall also provide interested parties the opportunity to learn about the State's progress in transitioning to a State Exchange and offer input on that transition. Following the initial public engagement described in this paragraph and until HHS approves or conditionally approves the State Exchange Blueprint application, a State shall conduct periodic public engagements, either in-person or virtually, in a timeframe and manner considered effective by the State.
* * * * *
9. Section 155.170 is amended by revising paragraph (a) to read as follows:
(a)
Additional required benefits.
(1) A State may require a QHP to offer benefits in addition to the essential health benefits. For plan years beginning before January 1, 2028, a benefit required by State action taking place on or before December 31, 2011, a benefit required by State action for purposes of compliance with Federal requirements, or a benefit covered in the State's EHB-benchmark plan is considered an EHB. A benefit required by State action taking place on or after January 1, 2012, other than for purposes of compliance with Federal requirements, that is not a benefit covered in the State's EHB-benchmark plan is considered in addition to the essential health benefits.
(2) For plan years beginning on or after January 1, 2028, a State may require a QHP to cover benefits in addition to the essential health benefits, which are any State-required benefits that are:
(i) Required by a State action taking place after December 31, 2011;
(ii) Applicable to the small group and/or individual markets;
(iii) Specific to required care, treatment, or services; and
(iv) Not required by State action for purposes of compliance with Federal requirements.
(3) A State must make payments in accordance with paragraph (b) of this section to defray the cost of any State-required benefits in addition to the EHB.
* * * * *
10. Section 155.205 is amended by revising paragraph (b)(1) introductory text to read as follows:
Ability of States to permit agents and brokers and web-brokers to assist qualified individuals, qualified employers, or qualified employees enrolling in QHPs.
* * * * *
(j) * * *
(2) * * *
(i) Provide consumers with correct information, without omission of material fact, regarding the Federally-facilitated Exchanges, QHPs offered through the Federally-facilitated Exchanges, and insurance affordability programs, and refrain from conduct that is misleading (including by having a direct enrollment website that HHS determines could mislead a consumer into believing they are visiting
HealthCare.gov), coercive, or discriminates based on race, color, national origin, disability, age, or sex;
(ii) * * *
(A) Documenting that eligibility application information has been reviewed by and confirmed to be accurate by the consumer or the consumer's authorized representative must require the consumer or their authorized representative to take an action that produces a record that can be maintained by the individual or entity described in paragraph (j)(1) of this section and produced to confirm the consumer or their authorized representative has reviewed and confirmed the accuracy of the eligibility application information. For enrollments for plan years ending prior to January 1, 2028, non-exhaustive examples of acceptable documentation include obtaining the signature of the consumer or their authorized representative (electronically or otherwise), verbal confirmation by the consumer or their authorized representative that is captured in an audio recording, a written response (electronic or otherwise) from the consumer or their authorized representative to a communication sent by the agent, broker, or web-broker, or other similar means or methods specified by HHS in guidance.
* * * * *
(
2) For enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j), all documentation required under paragraph (j)(2)(ii)(A) of this section must be collected by having the consumer or the consumer's authorized representative take an action to execute an HHS-approved and -created consumer consent form. The action the consumer or the consumer's authorized representative took to confirm the eligibility application information has been reviewed and confirmed to be accurate must be clear to HHS. This may include hand-written or electronic written signature or initials on the HHS-approved and -created consumer consent form, an email from the consumer or the consumer's authorized representative, or a recorded verbal conversation. A signature that is simply typed on the documentation or a filled-in check box does not clearly indicate the eligibility application information was reviewed and confirmed accurate by the consumer or the consumer's authorized representative.
* * * * *
(iii) * * *
(A) Obtaining and documenting the receipt of consent must require the consumer, or the consumer's authorized representative designated in compliance with § 155.227, to take an action that produces a record that can be maintained and produced by an individual or entity described in paragraph (j)(1) of this section to confirm the consumer's or their authorized representative's consent has been provided. For enrollments for plan years ending prior to January 1, 2028, non-exhaustive examples of acceptable documentation of consent include obtaining the signature of the consumer or their authorized representative (electronically or otherwise), verbal confirmation by the consumer or their authorized representative that is captured in an audio recording, a response from the consumer or their authorized representative to an electronic or other communication sent by the agent, broker, or web-broker, or other similar means or methods specified by HHS in guidance.
* * * * *
(C) For enrollments for plan years beginning on or after January 1, 2028, including enrollments under § 155.335(j), all documentation required under paragraph (j)(2)(iii)(A) of this section must be collected by having the consumer or the consumer's authorized representative take an action to execute an HHS-approved and -created consumer consent form. The action the consumer or the consumer's authorized representative took to provide consent must be clear to HHS. This may include hand-written or electronic written signature or initials on the HHS-approved and -created consumer consent form, an email from the consumer or the consumer's representative, or a recorded verbal conversation. A signature that is simply typed on the documentation or a filled-in check box does not properly indicate consent was provided by the consumer or the consumer's authorized representative.
* * * * *
(3)
Marketing requirements.
An individual or entity described in paragraph (j)(1) of this section must additionally:
(i) Comply with the standards of conduct under paragraph (j)(2) of this section; and
(ii) Provide consumers with correct information, without omission of material fact, regarding the Federally-facilitated Exchanges, QHPs offered through the Federally-facilitated Exchanges, and insurance affordability programs, and refrain from marketing that is misleading, materially inaccurate, coercive, or discriminates based on race, color, national origin, disability, age, or sex.
(iii) Examples of prohibited misleading marketing practices agents, brokers, and web-brokers may not include in their marketing of FFE plans include, but are not limited to:
(A) Providing cash, monetary rebates, gift cards, travel vouchers, or cash equivalents as an inducement for enrollment or otherwise.
(B) Offering gifts to consumers, unless the gifts are of nominal value, are offered to similarly situated consumers without regard to whether or not the consumers enroll, and are not in the form of cash or cash equivalents.
(C) Falsely asserting or suggesting that consumers will always qualify for zero-dollar insurance/zero-dollar premiums.
(D) Falsely using identical or facsimiles of government or other official logos and notations.
(E) Miscommunicating enrollment timelines and deadlines.
(F) Misconstruing legislation, regulations, or Executive Orders, including listing fake or incorrect references or citations.
(G) Utilizing the image or likeness and/or utilize a quote from a notable figure, such as a celebrity or politician, in an advertisement claiming that figure has endorsed you or your agency when that endorsement is not truthful.
(iv) An individual or entity described in paragraph (j)(1) of this section must produce any marketing material upon request, within the specified timeframe HHS mandates, in response to monitoring, audit, and enforcement
( printed page 29866)
activities conducted consistent with paragraphs (c)(5), (g), (h), and (k) of this section.
(v) An individual or entity described in paragraph (j)(1) of this section is responsible to ensure that all marketing-related materials created, written, released, or otherwise produced by the individual or entity or on their behalf adhere to the requirements of paragraphs (j)(3)(ii) and(iii) of this section, and to make all such marketing-related materials available upon request in accordance with paragraph (j)(3)(iv) of this section.
(ii) One or more applicants who is expected to be a member of the tax filer's family within the meaning of 26 CFR 1.36B-1(d) for the benefit year—
* * * * *
(C) He or she is a U.S. citizen, U.S. national, or an eligible noncitizen as defined in § 155.20.
* * * * *
(4)
Compliance with tax filing requirement—
(i)
APTC eligibility.
(A) For plan year 2027, an Exchange must implement one of two policies where it may not determine a tax filer eligible for APTC if the tax filer and their spouse, if the tax filer is married, has either failed to file and reconcile for 1 year, as described in paragraph (f)(4)(ii)(A) of this section (“1 tax year FTR policy”) or has failed to file and reconcile for 2 consecutive tax years, as described in paragraph (f)(4)(ii)(B) of this section (“2 tax-year policy”). Exchanges must apply any such policy uniformly to all tax filers (and their spouses, if married).
(B) For plan year 2028 and beyond, an Exchange must implement a 1-tax year FTR policy described in paragraph (f)(4)(ii)(A) of this section.
(ii)
Failure to file and reconcile.
For purposes of paragraph (f)(4)(i) of this section:
(A) A tax filer and their spouse, if the tax filer is married, is considered to have failed to file and reconcile for 1 tax year if HHS notifies the Exchange as part of the process described in § 155.320(c)(3) that APTC payments were made on behalf of either the tax filer or the tax filer's spouse, if the tax filer is a married couple, for the most recent year for which tax data would be utilized for verification of household income and family size in accordance with § 155.320(c)(1)(i), and the tax filer or the tax filer's spouse did not comply with the requirement to file an income tax return for that year as required by 26 U.S.C. 6011, 6012, and in 26 CFR chapter I, and reconcile APTC for that period.
(B) A tax filer and their spouse, if the tax filer is married, is considered to have failed to file and reconcile for 2 tax years if HHS notifies the Exchange as part of the process described in § 155.320(c)(3) that APTC payments were made on behalf of either the tax filer or the tax filer's spouse, if the tax filer is a married couple, for the 2 most recent consecutive tax years for which tax data would be utilized for verification of household income and family size in accordance with § 155.320(c)(1)(i), and the tax filer or the tax filer's spouse did not comply with the requirement to file an income tax return for those years as required by 26 U.S.C. 6011, 6012, and in 26 CFR chapter I, and reconcile APTC for that period.
(iii) Notice Requirements. For purposes of paragraph (f)(4)(ii) of this section, the following notice requirements apply.
(A) An Exchange that implements a 2-tax year FTR policy as described in paragraph (f)(4)(ii)(B) of this section must:
(
1) For tax filers failing to file and reconcile for 1 tax year as described in paragraph (f)(4)(ii)(A) of this section:
(
i) Send a notification to the tax filer, consistent with the standards applicable to the protection of Federal Tax Information, that informs the tax filer that the Exchange has determined that the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file and reconcile, and educate the tax filer of the need to file and reconcile or risk being determined ineligible for APTC if they fail to file and reconcile for a second consecutive tax year; or
(
ii) Send a notification to either the tax filer or their enrollee, that informs the tax filer or enrollee that they may be at risk of being determined ineligible for APTC in the future. These notices must educate tax filers or their enrollees on the requirement to file and reconcile, while not directly stating that the IRS indicates the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file and reconcile.
(
2) For tax filers failing to file and reconcile for 2 consecutive tax years as described in paragraph (f)(4)(ii)(B) of this section:
(
i) Send a direct notification to the tax filer, consistent with the standards applicable to the protection of Federal Tax Information, that explicitly informs the tax filer that the Exchange has determined that the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file their Federal income taxes and reconcile APTC, and educate the tax filer of the need to file and reconcile or risk being determined ineligible for APTC after 2 consecutive tax years of failing to file and reconcile; or
(
ii) Send an indirect notification to either the tax filer or their enrollee, that informs the tax filer or enrollee that they may be at risk of being determined ineligible for APTC after 2 consecutive tax years of failing to file and reconcile. These notices must educate tax filers or their enrollees on the requirement to file and reconcile, while not directly stating that the Internal Revenue Service indicates the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file and reconcile.
(B) An Exchange that implements 1-tax year FTR policy as described in paragraph (f)(4)(ii)(A) of this section must:
(1) Send a notification to the tax filer, consistent with the standards applicable to the protection of Federal Tax Information, that informs the tax filer that the Exchange has determined that the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file and reconcile of the need to file and reconcile, and of the risk of being determined ineligible for APTC if they fail to file and reconcile immediately; or
(2) Send a notification to either the tax filer or their enrollee, that informs the tax filer or enrollee that they may be at risk of being determined ineligible for APTC in the future. These notices must educate tax filers or their enrollees on the requirement to file and reconcile, while not directly stating that the IRS indicates the tax filer or the tax filer's spouse, if the tax filer is married, has failed to file and reconcile.
* * * * *
14. Section 155.320 is amended by—
a. Revising paragraphs (c)(3)(iii)(A) and (c)(3)(vi)(C)(2);
b. Removing the second occurrence of paragraph (c)(3)(viii);
c. Revising paragraphs (c)(3)(vii) and (viii);
d. Adding paragraph (c)(3)(ix); and
( printed page 29867)
Verification process related to eligibility for insurance affordability programs.
* * * * *
(c) * * *
(3) * * *
(iii) * * *
(A) Except as specified in paragraphs (c)(3)(iii)(B), (C), and (D) of this section, if an applicant's attestation to projected annual household income, as described in paragraph (c)(3)(ii)(B) of this section, would qualify the tax payer as an applicable taxpayer under 26 CFR 1.36B-2(b) for the plan year for which coverage is requested and is more than a reasonable threshold above the annual household income computed in accordance with paragraph (c)(3)(ii)(A) of this section, the data described in paragraph (c)(3)(ii)(A) of this section indicates that projected annual household income is under 100 percent of the FPL, and the Exchange has not verified the applicant's MAGI-based income through the process specified in paragraph (c)(2)(ii) of this section to be within the applicable Medicaid or CHIP MAGI-based income standard, the Exchange must proceed in accordance with § 155.315(f)(1) through (4). For the purposes of this paragraph, a reasonable threshold is established by the Exchange in guidance and approved by HHS, but must not be less than 10 percent, and can also include a threshold dollar amount.
* * * * *
(vi) * * *
(C) * * *
(2) If the data described in paragraph (c)(3)(vi)(A) of this section indicates that projected annual household income is under 100 percent of the FPL and the applicant's attestation to projected household income, as described in paragraph (c)(3)(ii)(B) of this section, would qualify the taxpayer as an applicable taxpayer according to 26 CFR 1.36B-2(b) for the plan year for which coverage is requested and is more than a reasonable threshold above the annual household income as computed using data sources described in paragraph (c)(3)(vi)(A) of this section, in which case the Exchange must follow the procedures specified in § 155.315(f)(1) through (4). The reasonable threshold used under this paragraph must be equal to the reasonable threshold established in accordance with paragraph (c)(3)(vi) of this section.
* * * * *
(vii)
Definition of household income.
For the purposes of paragraph (c)(3) of this section, “household income” means household income as specified in 26 CFR 1.36B-1(e).
(viii)
Definition of family size.
For purposes of paragraph (c)(3) of this section, “family size” means family size as specified in section 26 CFR 1.36B-1(d).
(ix) Verification of eligible noncitizen status. (A) Verification with the records of the Department of Homeland Security. For an applicant who has information or documentation of immigration status that can be verified through the Department of Homeland Security's Systematic Alien Verification for Entitlements (SAVE) program, and who attests to having an eligible noncitizen immigration status as defined at § 155.20, the Exchange must transmit information from the applicant or document to the Department of Homeland Security for verification.
(B) Inconsistencies and inability to verify information. For an applicant who attests to having an eligible noncitizen status as defined at § 155.20, and for whom the Exchange cannot verify such attestation through the Department of Homeland Security, the Exchange must follow the procedures specified in § 155.315(f)(1) through (4). The date on which the notice is received means 5 days after the date on the notice, unless the applicant demonstrates that he or she did not receive the notice within the 5 day period as described in § 155.315(b)(2).
(C) If, at the conclusion of the period specified in paragraph (c)(3)(ix)(B) of this section, the Exchange remains unable to verify the applicant's attestation, the Exchange must determine the applicant ineligible for advance payments of the premium tax credit and cost-sharing reductions, notify the applicant of such determination in accordance with the notice requirements specified in § 155.310(g), and discontinue any advance payments of the premium tax credit and cost-sharing reductions in accordance with the effective dates specified in § 155.330(f).
* * * * *
15. Section 155.400 is amended by revising paragraph (g) to read as follows:
(g)
Premium payment threshold.
Exchanges may, and the Federally-facilitated Exchanges and State-Based Exchanges on the Federal Platform will, allow issuers to implement, a premium payment threshold policy under which issuers can consider enrollees to have paid all amounts due if the enrollees pay an amount sufficient to maintain a percentage of total premium paid out of the total premium owed equal to or greater than a level prescribed by the issuer, provided that the level is reasonable and that the level and the policy are applied in a uniform manner to all enrollees. If an applicant or enrollee satisfies the premium payment threshold policy, the issuer may:
(1) Effectuate an enrollment based on payment of the binder payment under paragraph (e) of this section.
(2) Avoid triggering a grace period for non-payment of premium, as described by § 156.270(d) of this subchapter or a grace period governed by State rules.
(3) Avoid terminating the enrollment for non-payment of premium as, described by §§ 156.270(g) of this subchapter and 155.430(b)(2)(ii)(A) and (B).
* * * * *
16. Section 155.420 is amended by—
a. Removing paragraph (a)(4)(ii)(D);
b. Revising paragraph (a)(4)(iii) introductory text;
(iii) For the other triggering events specified in paragraph (d) of this section, except for paragraphs (d)(2)(i), (d)(4), and (d)(6)(i) and (ii) of this section for becoming newly eligible or ineligible for CSRs, and paragraphs (d)(8), (9), (10), (12), and (14) of this section:
* * * * *
(d) * * *
(13) At the option of the Exchange, the qualified individual provides satisfactory documentary evidence to verify his or her eligibility for an insurance affordability program or enrollment in a QHP through the Exchange following termination of Exchange enrollment due to a failure to verify such status within the time period specified in § 155.315.
* * * * *
(g)
Special enrollment period verification.
Beginning January 1, 2027, unless a request for modification is granted in accordance with § 155.315(h), Exchanges on the Federal platform must conduct pre-enrollment verification of new applicants' eligibility for special enrollment periods under this section. An Exchange meets this requirement if it verifies eligibility each plan year for the number of individuals newly
( printed page 29868)
enrolling in Exchange coverage through special enrollment periods that equals at least 75 percent of all special enrollments based on prior year enrollments. If the Exchange is unable to verify eligibility for individuals newly enrolling in Exchange coverage through a special enrollment period for which the Exchange requires verification, then such individuals are not eligible for enrollment through that special enrollment period. In accordance with § 155.505(b)(1)(iii), individuals have the right to appeal the eligibility determination.
17. Section 155.605 is amended by—
a. Removing “or” at the end of paragraph (d)(1)(ii)
b. Removing the period at the end of paragraph (d)(1)(iii) and adding “; or” in its place ; and
(iv) The applicant, or if the applicant is a tax dependent, the tax filer claiming the applicant as a dependent, has a projected household income that does not qualify them as an applicable taxpayer according to 26 CFR 1.36B-2(b) or does not qualify them for cost-sharing reductions according to 45 CFR 155.305(g)(1)(i)(C).
* * * * *
18. Section 155.1050 is amended by—
a. Revising the section heading and paragraphs (a)(1) and (2); and
Establishment of Exchange provider access standards.
(a) * * *
(1) A Federally-facilitated Exchange State without an Effective Provider Access Review Program (as defined in paragraph (d) of this section) must ensure that each QHP provides sufficient access to providers in a manner that meets the standards specified in § 156.230 for network plans, or, for plan years beginning on or after January 1, 2028, § 156.236 for non-network plans if such plans are allowed to be offered through the Exchange, as applicable. A State on the Federally-facilitated Exchanges with an Effective Provider Access Review Program (as defined in paragraph (d) of this section) must ensure that each QHP provides sufficient access to providers in a manner that meets the standards specified in § 156.230(a)(1) for network plans, or, for plan years beginning on or after January 1, 2028, § 156.236(a) for non-network plans if such plans are allowed to be offered through the Exchange, as applicable.
(2) State Exchanges and State-based Exchanges on the Federal Platform must ensure that each QHP provides sufficient access to providers in a manner that meets standards under § 156.230(a)(1)(ii) and (iii) for network plans, or, for plan years beginning on or after January 1, 2027, § 156.236(a) for non-network plans if such plans are allowed to be offered through the Exchange, as applicable.
* * * * *
(d)(1) FFE States may elect to conduct their own provider access certification reviews of issuers' plans, with or without a provider network, applying for certification as a QHP to be offered through a Federally-facilitated Exchange provided that the State has demonstrated sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Provider Access Review Program under paragraphs (d)(2) through (d)(4) of this section. This option applies to Federally-facilitated Exchange States, including States performing plan management. If States do not satisfy the criteria established under paragraphs (d)(2) through (d)(4) of this section, or do not elect to conduct such reviews, CMS will continue to conduct reviews of QHP issuer provider access in those States consistent with requirements listed under § 156.230 for network plans and under § 156.236 for non-network plans. Applicable requirements for non-network plans under this section are effective for plan years beginning on or after January 1, 2028.
(2) Federally-facilitated Exchange States with an Effective Provider Access Review Program must ensure that a QHP issuer that uses a network of providers ensures that the in-network providers, as available to all enrollees, include essential community providers (ECPs) in accordance with § 156.235, and maintains a network that is sufficient in number and types of providers, including providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay. The QHP issuer's provider network consisting of in-network providers, as available to all enrollees, must be consistent with the rules for network plans of section 2702(c) of the PHS Act.
(3) Federally-facilitated Exchange States with an Effective Provider Access Review Program must ensure that a QHP issuer that does not use a network of providers (a non-network plan) provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, including ECPs and providers that specialize in mental health and substance use disorder services, to ensure that all services will be accessible without unreasonable delay.
(4) A Federally-facilitated Exchange State that elects to conduct provider access reviews has an Effective Provider Access Review Program if it meets the following requirements:
(i) The State has established provider access standards that are set forth in State statute or regulation, which are consistent with provider access standards as set forth in § 156.230(a)(1)(ii) and (iii), and reports to CMS whether the State has delegated authority to some entity other than the State Department of Insurance to perform any or all provider access review activities.
(ii) The State's provider access review process includes reporting systems for State required provider access metrics and documentation of methodology and the State provides descriptions of all data collection systems, resources, templates, and methodologies used by the State, or the State's delegated entity to collect and review provider access data; and the State receives from issuers data and documentation in connection with provider access standards that are sufficient to conduct the examination.
(iii) The State's provider access review process includes procedures to ensure full and ongoing compliance with State provider access standards and enforcement frameworks applicable to issuers that fail to meet provider access standards so that those issuers come into compliance with State provider access standards, including standardized processes to assess efforts the issuer is pursuing to come into compliance with State provider access standards and implementing any justification and exception processes for issuers that have not yet or cannot meet provider access requirements.
(iv) The State establishes and maintains clear procedures and timeline requirements for regular provider access reviews, including processes that ensure reviews occur prior to completion of each plan year's QHP certification cycle.
(v) The State has a process for monitoring and addressing consumer-related provider access complaints to ensure sufficient access to providers consistent with section 1311(c)(1)(B) of the Affordable Care Act and as set forth in State statute.
( printed page 29869)
(vi) The State has a process to collect and review information described under § 156.236(b)(4) through (b)(9) from non-network plans, which non-network plans must submit to the FFE for a determination that it provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full.
(5) CMS will determine whether a State has an Effective Provider Access Review Program based on information available to CMS that demonstrates whether the program meets the criteria described under paragraphs (d)(2) through (d)(4) of this section.
(6) CMS may grant an exception to the requirements in paragraph (d) of this section if it determines that making such an exception is in the interests of qualified individuals in the State or States in which such Exchange operates.
(7) CMS will notify the FFE State electing to conduct provider access certification reviews of its decision in writing whether the State is determined to have an Effective Provider Access Review Program and can therefore conduct its own provider access certification reviews. CMS reserves the right to evaluate at any time whether, and to what extent, an FFE State's circumstances have changed such that it has begun to or has ceased to satisfy the criteria established by CMS under this section. Such evaluations may result in CMS assuming provider access review responsibilities or transitioning such responsibilities back to the State.
* * * * *
19. Add § 155.1051 to subpart K to read as follows:
Effective Essential Community Provider Review Program.
(a) FFE States may elect to conduct their own ECP certification reviews of issuers' plans with or without a provider network applying for certification as a QHP to be offered through a Federally-facilitated Exchange provided that the State demonstrates it has sufficient authority and the technical capacity to conduct these reviews by satisfying the applicable criteria to be considered to have an Effective Essential Community Provider Review Program under this section. This option applies to all FFE States, including States performing plan management. An FFE State must demonstrate it meets applicable criteria established under paragraphs (b) through (c) of this section for both network plans and non-network plans, and the sufficient authority and technical capacity to conduct reviews of such plans (as assessed by CMS under § 155.1051(e)), to be considered to have an Effective Essential Community Provider Review Program, if they decide to certify such plans. If FFE States do not satisfy the criteria established by CMS under paragraphs (b) through (e) of this section or do not elect to conduct such reviews, then CMS will continue to perform ECP certification reviews consistent with § 156.235 for network plans and § 156.236 for non-network plans. Applicable requirements for non-network plans under this section are effective for plan years beginning on or after January 1, 2028.
(b) FFE States with an Effective ECP Review Program must ensure that a QHP issuer with a provider network includes in their provider network a sufficient number and geographic distribution of ECPs, where available, to ensure reasonable and timely access to a broad range of such providers for low-income individuals or individuals residing in Health Professional Shortage Areas within the QHP's service area, in accordance with the Exchange's network adequacy standards. FFE States with an Effective ECP Review Program must also ensure that a non-network plan applying for certification to be offered as a QHP through a Federally-facilitated Exchange demonstrates that it provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full to ensure that services will be accessible without unreasonable delay.
(c) FFE States with an Effective ECP Review Program must have established ECP requirements that are set forth in State statute or regulation. FFE States must demonstrate that these established ECP requirements ensure that plans meet all the following requirements that promote a sufficient number and geographic distribution of ECPs:
(1) The minimum percentage requirements under § 156.235(a)(2)(i) for network plans, and under § 156.236(b)(1) for non-network plans.
(2) The Indian health care provider requirement under § 156.235(a)(2)(ii)(A) for network plans and under § 156.236(b)(3) for non-network plans.
(3) The category per county requirements, including for each of the eight ECP category types under § 156.235(a)(2)(ii)(B) for network plans and under § 156.236(b)(2) for non-network plans.
(d) FFE States with an Effective ECP Review Program that have alternative ECP requirements compared to those described under paragraph (c)(1) through (3) of this section must demonstrate how their requirements would continue to promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs, and an adequate level of service for low-income enrollees or individuals residing in Health Professional Shortage Areas.
(e) CMS will consider all the following factors in its review to determine if an FFE State has an Effective ECP Review Program:
(1) The State's legal authority to review whether plans applying for QHP certification meet ECP requirements, including relevant State regulations and statutes.
(2) Evidence that the State's requirements are consistent with ECP requirements under paragraph (c)(1) through (3) of this section that promote a sufficient number and geographic distribution of ECPs, or the State provides a rationale to describe how its alternative requirements promote a sufficient number and geographic distribution of ECPs to ensure reasonable and timely access to ECPs.
(3) A description of the State's definition of an ECP, if different from the definition under § 156.235(c), including relevant categories and eligibility criteria that the State uses to determine whether a facility qualifies as an ECP.
(4) Whether the State utilizes the Federal ECP List or has a process it uses to identify qualified ECPs that may be included within a network plan's provider network.
(5) Whether the State utilizes the Federal ECP List or has a process it uses to identify qualified ECPs that may accept a non-network plan's benefit amount as payment in full.
(6) A description of data collection systems, resources, templates, or methodologies used by the State to collect and review ECP data.
(7) Whether the State generally collects information from QHP issuers regarding the status of contract offers for network plans or offers of benefit amounts as payment in full to an ECP for non-network plans.
(8) Whether the State has delegated authority to some other entity other than the State Department of Insurance to perform any or all ECP review activities.
(9) Whether the State has compliance reviews, follow-up procedures, and enforcement frameworks applicable to issuers that demonstrate inadequate networks of ECPs or inadequate access to ECPs that accept benefit amounts as payment in full, so that those issuers come into compliance with State ECP requirements, including standardized processes to assess efforts the issuer is pursuing to come into compliance with State ECP requirements and any justification and exception processes for
( printed page 29870)
issuers that have not yet or cannot meet ECP requirements.
(10) Whether the State has a process for monitoring and addressing consumer-related complaints regarding access to ECPs to ensure sufficient access to ECPs consistent with section 1311(c)(1)(C) of the Affordable Care Act and set forth in State statute.
(11) Whether the State collects the information described under § 156.236(b)(4) through (b)(9) from issuers of non-network plans, which issuers of non-network plans must submit to the FFE for a determination that the plan provides reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full.
(f) CMS will notify the FFE State electing to conduct ECP certification reviews of its decision in writing whether the State is determined to have an Effective ECP Review Program and can therefore conduct its own ECP certification reviews. CMS reserves the right to evaluate at any time whether, and to what extent, an FFE State's circumstances have changed such that it has begun to or has ceased to satisfy the criteria established by CMS under this section, and consequently no longer has an Effective ECP Review Program.
20. Section 155.1200 is amended by revising paragraph (d) introductory text and adding paragraph (e) to read as follows:
General program integrity and oversight requirements.
* * * * *
(d)
External audit standard.
The State Exchange must ensure that independent audits of State Exchange financial activities and program activities under paragraph (c) of this section address the following requirements, unless a State Exchange is satisfying certain programmatic audit requirements for a given benefit year, as identified by HHS in sub-regulatory guidance, under paragraph (e) of this section:
* * * * *
(e)
State Exchange Improper Payment Measurement (SEIPM) program.
For a given benefit year, a State Exchange may satisfy certain requirements of the independent external programmatic audit, particularly the review of compliance with subparts D and E of this part, as identified by HHS in sub-regulatory guidance, as outlined in paragraph (d) of this section, by completing the SEIPM process established through 45 CFR part 155, subpart Q.
(a) This subpart sets forth the requirements of the State Exchange Improper Payment Measurement (SEIPM) program. SEIPM is an initiative through which HHS will measure improper payments of advance payment of the premium tax credit (APTC) that are administered by State Exchanges, as described in more detail in § 155.1610. HHS will use the SEIPM program results to produce an estimate of improper payments of APTC aggregated across State Exchanges.
(b) Unless otherwise specified by HHS, all State Exchanges must submit information on an annual basis that is necessary to support the SEIPM processes.
(c) HHS will publish in the Agency Financial Report an estimate of improper payments that is aggregated across all State Exchanges.
Annual Program Schedule
means the document issued by HHS to each State Exchange that prescribes the dates by which key program milestones must be met for each SEIPM Cycle.
Administrative Appeal
means the process by which a State Exchange may request HHS to review and reconsider a Difference Resolution Decision. The appeal is the second and last level for a State Exchange to contest findings of error or improper payment as it relates to APTC.
Administrative Appeal Decision
means the HHS final appeal decision resulting from a State Exchange's request for an appeal of one or more error or improper payment findings in a Sampled Unit Assessment Package.
Corrective Action Plan
(
CAP) means the plan a State Exchange develops in order to correct errors resulting in improper payments of APTC identified through SEIPM.
Difference Resolution
means the process by which a State Exchange may initially request HHS to reconsider one or more errors or improper payment findings documented in a Sampled Unit Assessment Package.
Difference Resolution Decision
means the HHS decision resulting from a State Exchange's request for a difference resolution of any Sampled Unit Assessment Package.
Error
means a finding by HHS that a State Exchange did not correctly apply a requirement of subparts D and E of this part related to:
(1) Eligibility for and enrollment in a Qualified Health Plan (QHP);
(2) Eligibility for APTC, and calculated amount of APTC;
(3) Redeterminations of eligibility during a plan year;
(4) Eligibility redeterminations for purposes of re-enrollment.
Measurement Year
means the calendar year in which the processes described in § 155.1625 are initiated. The Measurement Year immediately follows the Plan Year and is the second year of the SEIPM Cycle.
Reporting Year
means the calendar year in which HHS reports the improper payment rate for State Exchanges as required under § 155.1625(c), following completion of the measurement processes for the applicable Plan Year. The Reporting Year immediately follows the Measurement Year and is the last year of the SEIPM Cycle.
Sampled Unit Assessment Package
means the collection of findings and supporting documentation that HHS prepares in order to record errors at the tax household level using the process described in § 155.1625.
State Exchange Improper Payment Measurement or SEIPM
means the process for determining estimated improper payments of APTC that are administered by State Exchanges as required under the Payment Integrity Information Act of 2019, which includes a review of a State Exchange's APTC-related determinations regarding:
(1) Eligibility for and enrollment in a QHP;
(2) Eligibility for APTC, and calculated amount of APTC;
(3) Redeterminations of eligibility during a Plan Year;
(4) Annual eligibility redeterminations.
SEIPM Cycle
means the 3-year period consisting of the Plan Year, Measurement Year, and Reporting Year, during which the improper payment measurement process occurs for the Plan Year that is subject to review.
( printed page 29871)
Tax household
means the applicant, the applicant's spouse if the applicant is married and files a joint return, and all individuals who are dependents of the applicant or spouse as defined in 26 U.S.C. 152.
(a) HHS will issue an Annual Program Schedule to each State Exchange no later than January 5th of the Measurement Year. The Annual Program Schedule will specify the deadlines for all information submissions required under this section.
(b) On an annual basis, each State Exchange must submit or make available to HHS the following information:
(1)
Program documentation.
Policy, operational and technical documentation concerning business rules and APTC calculations that pertain to consumer eligibility and enrollment processes of the State Exchange as well as information that describes the data system architecture of the State Exchange such as entity relationship diagrams and data dictionaries.
(2)
Universe.
For the Plan Year being reviewed, a listing of the population of tax households that have associated QHP enrollments and payments of APTC. For each tax household within the universe, the State Exchange must submit the following information:
(xii) APTC amount paid over the duration of the benefit year.
(3)
Tax household Data.
For each of the sampled tax households and in a format specified by HHS:
(i) Information pertaining to the calculation of the APTC benefits paid that includes monthly enrollment premium amounts, monthly APTC payment amounts, monthly Second Lowest Cost Silver Plan Premium amounts, and the amount of each monthly premium that is attributable to essential health benefits.
(ii) Information relevant to enrollment that includes dates and amounts of effectuation payments, premium payment amount, and policy start and end dates.
(iii) Information relevant to the determination of eligibility for a special enrollment period (where applicable), which would include (where applicable) information collected by the State Exchange about consumer attestations and representations regarding special enrollment period eligibility criteria, copies of documentary evidence submitted by applicants, electronic verification information, and timing information.
(iv) Information about the timing of QHP certification or approval, the coverage area of the associated QHP, and the timing of any QHP decertification or suppression.
(v) To the extent applicable, for each person who is included in the APTC payment calculation:
(A) Information collected by the State Exchange about consumer attestations regarding QHP and APTC eligibility factors and demographic information relevant to initial QHP enrollment and eligibility.
(B) APTC eligibility and payment determinations which includes evidence of required data verifications, the electronic sources consulted, the timing of required verifications, and the results of the verification.
(C) Information relevant to QHP and APTC manual eligibility verifications and the resolution of electronic verification inconsistencies, which would include copies of documentary evidence submitted by QHP enrollees, the timing of submissions, the timing of adjudication, and information about good faith extensions.
(D) Information relevant to QHP and APTC eligibility redeterminations such as information about automatic annual redeterminations, the timing and results of periodic examinations of data sources, and policy or application changes initiated by the consumer and resultant electronic or manual eligibility verifications.
(vi) Any consumer submitted documents that were used to establish new or continued eligibility for enrollment in a QHP and APTC.
(a)
Sample size.
At the beginning of each SEIPM cycle, HHS will calculate a sample size in aggregate across all State Exchanges.
(1)
Statistical methodology.
The sample size will be calculated to estimate an improper payment rate.
(2)
State-specific sample sizes.
HHS will develop sample sizes specific for each State Exchange. HHS may take into consideration the following factors in determining each State Exchange's sample size for the current SEIPM cycle:
(i) Overall APTC expenditures associated with the State Exchange.
(ii) State-level precision goals for the current SEIPM cycle.
(iii) The improper payment rate from the State Exchange's previous SEIPM cycle.
(3)
Sample size parameters.
HHS will establish minimum and maximum sample sizes to ensure statistical validity while maintaining operational feasibility across State Exchanges of varying sizes.
(b)
Sample selection procedures.
On an annual basis, HHS will select samples of tax households from the data provided by each State Exchange as described in § 155.1615(b)(2).
(c)
State Exchange coordination and notification
—(1)
Sampled records notification.
Following receipt of the universe data from State Exchanges as described in § 155.1615(b)(2), HHS will notify each State Exchange of the specific records selected for review. This notification will include:
(i) The total number of sampled tax households selected for the State Exchange.
(ii) A unique identifier for each sampled tax household.
(iii) Any specific instructions or requirements that HHS determines are needed to facilitate HHS' review of the sampled records.
(2)
Timing of sampled records notification.
HHS will provide the sampled records notification described in paragraph (c)(1) of this section no later than 60 days after receipt of complete universe data from all State Exchanges.
(3)
Extension of sampling notification timeline.
(i) HHS may extend the 60-day timeline specified in paragraph (c)(2) of this section if:
(A) Technical issues prevent completion of the sampling process within the standard timeframe;
(B) Data quality issues require additional coordination with State Exchanges before sampling can be completed; or
(C) Other circumstances beyond HHS's control necessitate additional time to ensure accurate sampling methodology.
(ii) If HHS determines an extension is necessary, HHS will:
( printed page 29872)
(A) Notify all affected State Exchanges in writing of the extension and the revised notification date;
(B) Provide the reason for the extension; and
(C) Confirm the impact, if any, on subsequent SEIPM cycle timelines.
(a)
Review of records and error identification.
(1)
Systematic review process.
For each sampled record, HHS will conduct a comprehensive review of all information provided by the State Exchange using standardized review criteria.
(2)
Data sources.
HHS will conduct reviews using the tax household information provided under § 155.1615(b)(3), supplemented by any relevant consumer-submitted documents that were gathered by the State Exchange as part of the enrollment and eligibility process and provided to HHS.
(3)
Error identification.
The review will identify whether the State Exchange made any errors related to the following resulting in improper payments of APTC:
(i) Enrolling or re-enrolling a consumer into a QHP for which APTC was paid.
(ii) Consumer eligibility for APTC being paid on the consumer's behalf.
(iii) Calculating the APTC amount that was paid on the consumer's behalf.
(iv) Taking required actions upon changes to a consumer's status that would affect their APTC-related eligibility or payment amount.
(4)
Review standards and criteria.
HHS will apply consistent review standards based on the APTC-related determination requirements established in subparts D and E of this part, and other applicable provisions of this part.
(b)
Error evaluation.
HHS will evaluate each error to determine an improper payment amount. For each error identified, HHS will:
(1) Calculate the correct APTC amount based on the requirements of section 36B of the Internal Revenue Code and applicable implementing regulations.
(2) Determine an improper payment amount.
(3) Document the error and improper payment amount within a Sampled Unit Assessment Package and provide the Sampled Unit Assessment Package to the State Exchange.
(4) Extrapolate the identified improper payments from the sample to estimate the total improper payment amount for the State Exchange's entire universe of APTC payments, using statistically valid methodologies that comply with OMB guidance on improper payment estimation.
(c)
Reporting.
HHS will report annually in the Agency Financial Report, which is made available to the public:
(1) The estimated aggregate improper payment rate for Federal and State Exchanges combined.
(2) The estimated aggregate improper payment rate for State Exchanges, and;
(3) HHS will provide to each State Exchange a report that documents the State-specific improper payment rate and error analysis.
(a)
Difference Resolution.
(1) The State Exchange may make a written Difference Resolution request to HHS within 30 days after the issuance of the Sampled Unit Assessment Package to dispute HHS' error and improper payment findings.
(2) Upon receipt of a Difference Resolution request, HHS will do the following:
(i) Engage with the State Exchange in a collaborative process to examine the disputed findings and any additional documentation provided by the State Exchange.
(ii) Evaluate the disputed findings by applying the same protocol used in the original review while considering whether the State Exchange's position is supported by the existing or newly provided evidence.
(iii) Prepare the Difference Resolution Decision.
(3) The Difference Resolution Decision will be communicated to the State Exchange within 90 days of receipt of the written request for a Difference Resolution. The Difference Resolution Decision will include a summary of the analysis and rationale that informed the decision.
(b)
Administrative appeal.
(1) To dispute a Difference Resolution Decision, the State Exchange may make a written request for an administrative appeal within 15 business days after the issuance of the Difference Resolution Decision.
(i) The State Exchange may not submit new evidence; it may use evidence that was previously submitted during Difference Resolution.
(ii) The State Exchange may provide additional context regarding information that was submitted during Difference Resolution.
(2) Upon receipt of an appeal request, HHS will do the following:
(i) Assign the appeal request to one or more administrative appeal reviewers who were not involved in the original review;
(ii) Conduct a comprehensive review of the disputed findings using the administrative record established during the Difference Resolution process;
(iii) Independently evaluate the disputed findings by applying the same protocol used in the original review while considering whether the State Exchange's position is supported by the evidence; and
(iv) Prepare an appeal decision for the completed review based on a preponderance of the evidence.
(3) HHS will issue the appeal decision within 90 days of receipt of the written request for appeal. The appeal decision will include a summary of the analysis and rationale that informed the decision.
(c)
Difference Resolution and administrative appeal submission requirements.
All Difference Resolution and appeal requests must be filed in a form and manner specified by HHS and contain the following:
(1) A clear statement of the specific finding(s) being challenged.
(2) All factual and legal bases for filing the request.
(3) Evidence directly related to the finding(s), which may include:
(i) Clarifying information regarding data interpretation.
(ii) Legal citations supporting the State Exchange's position.
(d)
Timing of Difference Resolution and Administrative Appeal decisions.
(1) For Difference Resolution Requests or administrative appeals resolved in favor of the State Exchange during the current SEIPM cycle:
(i) HHS will adjust the affected improper payment rate calculations for the SEIPM cycle.
(ii) Updated aggregate rates will be reflected in current cycle reporting.
(2) For Difference Resolution Requests or administrative appeals resolved in favor of the State Exchange after completion of the SEIPM cycle:
(i) If Difference Resolution or administrative appeal decisions result in material changes to aggregate rates, HHS will publish amended aggregate improper payment rates in subsequent Agency Financial Reports or other appropriate public reporting mechanisms as well as notify affected State Exchanges of any amendments to previously published rates.
(ii) If HHS determines, at its discretion, that the Difference Resolution or administrative appeal decisions do not result in material changes to aggregate rates, no action will be taken to publish amended aggregated improper payment rates or notify affected State Exchanges.
(e)
Good cause exception.
For good cause, HHS may extend the timelines
( printed page 29873)
for accepting a Difference Resolution request or administrative appeal request or for issuing a Difference Resolution Decision or Administrative Appeal Decision. The failure of HHS to timely issue a Difference Resolution or Administrative Appeal decision does not indicate an acceptance of the State Exchange's position and is not a basis to decide in favor of the State Exchange.
(a)
CAP.
HHS may require the State Exchange to develop and submit a proposed CAP to correct errors resulting in improper payments.
(b)
Development of proposed CAP.
A State Exchange's proposed CAP must address errors that are included in the State Exchange improper payment report described in § 155.1625(c)(2) and must be developed in accordance with HHS requirements.
(1) In developing a proposed CAP, the State Exchange must conduct an error analysis such as reviewing causes, characteristics, and frequency of errors that are associated with improper payments. The State Exchange must review the findings of the analysis to determine the causes of the errors included in the State Exchange improper payment rate, if any, and to identify the root causes of the resulting improper payments.
(i) If a State Exchange has a pending Difference Resolution request or administrative appeal and HHS requests a CAP, HHS may provide a new timeline for CAP submission after the Difference Resolution or Administrative Appeal Decision and calculation of the final improper payment rate.
(2) The State Exchange must determine the corrective actions to be implemented to correct causes of the errors included in the State Exchange improper payment rate and to prevent them from occurring again.
(3) The proposed CAP must include measurable milestones, accountability mechanisms, regular monitoring and validation of progress, documentation of implemented corrective actions, and regular status updates. The CAP must include all the following for each identified error:
(i) The specific corrective action.
(ii) Status of the corrective action.
(iii) Scheduled or actual implementation date of the corrective action.
(iv) Key personnel responsible for implementing each corrective action.
(v) A plan for monitoring the effectiveness of the corrective action.
(c)
Implementation and evaluation of a CAP.
A State Exchange must develop an implementation schedule for its CAP, implement the plan in accordance with that schedule, and regularly evaluate whether the initiatives are effective at reducing or eliminating error causes. The State Exchange must provide updates on CAP implementation progress in a manner and frequency specified by HHS, but at least annually.
(d)
Failures in the CAP process.
If a State Exchange does not submit a CAP when one has been required, submits an incomplete CAP that does not address all the required parts of a CAP as specified in paragraph (b)(3) of this section, fails to follow the implementation schedule referenced in paragraph (c), or submits a CAP that is otherwise unacceptable following technical assistance from HHS, HHS may take actions consistent with § 155.1650.
(a) Any State Exchange in its first year of operation must participate in a 1-year SEIPM preparation phase prior to participating in SEIPM in the subsequent year.
(b) To satisfy the requirements of the SEIPM preparation phase, a State Exchange must:
(1) Complete the information submission requirements in § 155.1615(b)(1) and (3) using information from the most current Plan Year for a sample size not to exceed 10 unique tax households that address scenarios specified by HHS.
(2) Undergo the review procedures in § 155.1625(a) and (b).
(3) Participate in technical assistance activities provided by HHS, which may include:
(i) Training on SEIPM requirements and procedures;
(ii) System readiness assessments;
(iii) Data quality validation exercises; and
(iv) Process improvement recommendations.
(c) At the beginning of each calendar year, HHS will provide any State Exchange that meets the conditions in paragraph (a) of this section with a schedule that spans a 12-month period that specifies when the requirements of this section must be completed.
HHS will minimize potential duplicate requirements of the annual independent external programmatic audit described at § 155.1200(c) and (d) and SEIPM, such that, as determined by HHS, a State Exchange may be deemed to satisfy certain requirements of § 155.1200(c) and (d), particularly the review of compliance with subparts D and E, as identified in HHS sub-regulatory guidance, for a particular plan year by successfully completing the SEIPM process.
(a)
General principle.
For purposes of improper payment measurement under this subpart, HHS will classify APTC payments as improper when a State Exchange fails to provide adequate documentation demonstrating that such payments were made in accordance with applicable Federal requirements.
(b)
Determination of substantial noncompliance.
HHS will determine that a State Exchange has failed to substantially comply with this subpart if the State Exchange:
(1) Fails to submit required data or documentation within the timelines specified in the Annual Program Schedule.
(2) Submits data or documentation that is incomplete, inaccurate, or in a format that would reasonably prevent effective review.
(3) Fails to implement the CAP process as set out in § 155.1635(d).
(4) Demonstrates a pattern of more than five instances during a SEIPM cycle in which the State Exchange fails to respond within 30 calendar days, or provides a non-responsive answer, to HHS requests for clarification or additional information.
(c)
Notice and opportunity to cure.
Before implementing measures under paragraph (d) of this section, HHS will:
(1) Provide written notice to the State Exchange specifying the nature of the noncompliance and the potential consequences.
(2) Allow the State Exchange a reasonable opportunity, not less than 30 days, to cure the noncompliance or demonstrate that compliance has been achieved.
(d)
Remedial measures.
If a State Exchange fails to substantially comply with the data collection requirements, the CAP provisions contained in this subpart, or HHS requests for clarification or additional information, and HHS finds that such failures undermine or prohibit HHS's efficient administration of Exchange improper payment measurement activities, HHS may implement measures or procedures for:
(1) Enhanced monitoring and reporting.
(2) Mandatory implementation of specific operational procedures or controls.
(3) On-site visits to State Exchange facilities to assess operational procedures, data systems, and compliance with program requirements.
( printed page 29874)
(e)
Escalation procedures.
If a State Exchange continues to fail to comply after implementation of initial remedial measures under paragraph (d) of this section, HHS may initiate proceedings to revoke the State Exchange's authority to operate in accordance with applicable law.
PART 156—HEALTH INSURANCE ISSUER STANDARDS UNDER THE AFFORDABLE CARE ACT, INCLUDING STANDARDS RELATED TO EXCHANGES
22. The authority citation for part 156 continues to read as follows:
(2) Are required by a State action taking place on or before December 31, 2011.
* * * * *
(d) For plan years beginning before January 1, 2026, an issuer of a plan offering EHB may not include routine non-pediatric dental services, routine non-pediatric eye exam services, long-term/custodial nursing home care benefits, or non-medically necessary orthodontia as EHB. For plan years beginning on any day in calendar year 2026, an issuer of a plan offering EHB may not include routine non-pediatric dental services, routine non-pediatric eye exam services, long-term/custodial nursing home care benefits, non-medically necessary orthodontia, or specified sex-trait modification procedures (as defined at § 156.400) as EHB. For plan years beginning on or after January 1, 2027, an issuer of a plan offering EHB may not include routine non-pediatric dental services, routine non-pediatric eye exam services, long-term/custodial nursing home care benefits, non-medically necessary orthodontia, or specified sex-trait modification procedures (as defined at § 156.400) as EHB.
* * * * *
24. Section 156.130 is amended by revising paragraph (a)(2) to read as follows:
(2) Except as permitted in § 156.136 and § 156.155(a)(3)(ii), for a plan year beginning in a calendar year after 2014, cost sharing may not exceed the following:
* * * * *
25. Add § 156.136 to subpart B to read as follows:
For plan years beginning on or after January 1, 2027, if an issuer offers a bronze plan (as defined at § 156.140(b)(1)) in the individual market that complies with the cost-sharing requirements at § 156.130 and the levels of coverage requirements at § 156.140, the issuer may also offer within the same service area bronze plans that exceed the maximum annual limitation on cost sharing at § 156.130 by amounts in increments of 50 dollars in order to achieve an AV within the standard bronze de minimis variation at § 156.140(c), calculated as described in § 156.135 of this subpart, but not to exceed an amount equal to 130 percent of the annual limitation on cost sharing under section 1302(c)(1) of the Affordable Care Act.
(3)(i) For plan years beginning before January 1, 2028, provides coverage of the essential health benefits under section 1302(b) of the Affordable Care Act, except that the plan provides no benefits for any plan year (except as provided in paragraphs (a)(4), (b), and (c) of this section) until the annual limitation on cost sharing in section 1302(c)(1) of the Affordable Care Act is reached.
(ii) For plan years beginning on or after January 1, 2028, provides coverage of the essential health benefits under section 1302(b) of the Affordable Care Act, except that the plan provides no benefits for any plan year (except as provided in paragraphs (a)(4) and (6), (b), and (c) of this section) until an amount equal to 130 percent of the annual limitation on cost sharing in section 1302(c)(1) of the Affordable Care Act, rounded down to the next lowest multiple of 50 dollars, is reached.
* * * * *
(6) For plan years beginning on or after January 1, 2027, has a plan term of either 1 plan year, or of multiple consecutive plan years not to exceed 10 plan years. Such a plan with a plan term of at least 2 consecutive plan years may utilize value-based insurance designs to provide benefits before reaching the deductible, pursuant to guidelines issued by the Secretaries of Health and Human Services, Labor, and the Treasury under section 2713(c) of the Public Health Service Act.
29. Section 156.230 is amended by revising the section heading, paragraphs (a)(1) introductory text, (a)(2)(i) introductory text, (a)(2)(ii), and (a)(3) and (4) to read as follows:
(1) A QHP that uses a network of providers must ensure that the provider network consisting of in-network providers, as available to all enrollees, meets the following standards:
* * * * *
(2) * * *
(i)
Standards.
A QHP issuer in a Federally-facilitated Exchange in a State that CMS has not determined to have an Effective Provider Access Review Program as described in § 155.1050(d) must comply with the requirement in paragraph (a)(1)(ii) of this section by:
* * * * *
(ii)
Justification.
If a plan applying for QHP certification to be offered through a Federally-facilitated Exchange in a State that CMS has not determined to have an Effective Provider Access Review Program as described in § 155.1050(d) does not satisfy the network adequacy standards described in paragraphs (a)(2)(i)(A) and (B) of this section, the issuer must include as part of its QHP application a justification describing how the plan's provider network provides an adequate level of service for enrollees and how the plan's provider network will be strengthened and brought closer to compliance with the network adequacy standards prior to the start of the plan year. The issuer must provide information as requested by the FFE to support this justification.
(3) When CMS is conducting provider access reviews under paragraph (a)(2)(i)(A) and (B) of this section, the Federally-facilitated Exchange may grant an exception to the requirements in paragraphs (a)(2)(i)(A) and (B) of this section if the Exchange determines that
( printed page 29875)
making such health plan available through such Exchange is in the interests of qualified individuals in the State or States in which such Exchange operates.
(4) A limited exception to the requirement described under paragraph (a)(1) of this section is available to stand-alone dental plans issuers that sell plans in areas where it is prohibitively difficult for the issuer to establish a network of dental providers; this exception is not available to medical QHP issuers. Under this exception, an area is considered “prohibitively difficult” for the stand-alone dental plan issuer to establish a network of dental providers based on attestations from State departments of insurance in States with at least 80 percent of counties classified as Counties with Extreme Access Considerations (CEAC) that at least one of the following factors exists in the area of concern: a significant shortage of dental providers, a significant number of dental providers unwilling to contract with Exchange issuers, or significant geographic limitations impacting consumer access to dental providers.
* * * * *
30. Section 156.235 is amended by revising the section heading, and paragraphs (a)(1), (a)(2) introductory text, (a)(2)(i), (a)(2)(ii) introductory text, (a)(3) and (5), and (b) to read as follows:
Essential community provider standards for network plans.
(a) * * *
(1) A QHP issuer that uses a provider network consisting of in-network providers must ensure that the provider network of each of its QHPs includes a sufficient number and geographic distribution of essential community providers (ECPs), where available, to ensure reasonable and timely access to a broad range of such providers for low-income individuals or individuals residing in Health Professional Shortage Areas within the QHP's service area, in accordance with the Exchange's network adequacy standards.
(2) A network plan applying for QHP certification to be offered through a Federally-facilitated Exchange has a sufficient number and geographic distribution of ECPs if it demonstrates in its QHP application that—
(i) The QHP issuer's provider network includes as participating providers at least a minimum percentage, as specified by HHS, of available ECPs in each network plan's service area collectively across all ECP categories defined under paragraph (a)(2)(ii)(B) of this section, and at least a minimum percentage of available ECPs in each network plan's service area within certain individual ECP categories, as specified by HHS. Multiple providers at a single location will count as a single ECP toward both the available ECPs in the network plan's service area and the issuer's satisfaction of the ECP participation standard. For network plans that use tiered networks, to count toward the issuer's satisfaction of the ECP standards, providers must be contracted within the network tier that results in the lowest cost-sharing obligation. For network plans with two network tiers (for example, participating providers and preferred providers), such as many preferred provider organizations (PPOs), where cost-sharing is lower for preferred providers, only preferred providers will be counted towards ECP standards; and
(ii) The issuer of the network plan offers contracts to—
* * * * *
(3) A network plan applying for QHP certification to be offered through a Federally-facilitated Exchange must include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. A network plan does not need to report on the status of contract offers for all available ECPs in the network plan's service area, but must at least report on the status of contract offers for all ECPs which the issuer has either included in its network plan or offered a contract to be included in its network plan within each service area.
* * * * *
(5) A network plan that provides a majority of covered professional services through physicians employed by the issuer or through a single contracted medical group may instead comply with the alternate standard described in paragraph (b) of this section.
(b)
Alternate ECP standard.
(1) A network plan described in paragraph (a)(5) of this section must have a sufficient number and geographic distribution of employed providers and hospital facilities, or providers of its contracted medical group and hospital facilities, to ensure reasonable and timely access for low-income individuals or individuals residing in Health Professional Shortage Areas within the network plan's service area, in accordance with the Exchange's network adequacy standards.
(2) A network plan described in paragraph (a)(5) of this section applying for QHP certification to be offered through a Federally-facilitated Exchange has a sufficient number and geographic distribution of employed or contracted providers if it demonstrates in its QHP application that—
(i) The number of its providers that are located in Health Professional Shortage Areas or five-digit zip codes in which 30 percent or more of the population falls below 200 percent of the Federal poverty level satisfies a minimum percentage, specified by HHS, of available ECPs in each network plan's service area collectively across all ECP categories defined under paragraph (a)(2)(ii)(B) of this section, and at least a minimum percentage of available ECPs in each network plan's service area within certain individual ECP categories, as specified by HHS. Multiple providers at a single location will count as a single ECP toward both the available ECPs in the network plan's service area and the issuer's satisfaction of the ECP participation standard. For network plans that use tiered networks, to count toward the issuer's satisfaction of the ECP standards, providers must be contracted within the network tier that results in the lowest cost-sharing obligation. For network plans with two network tiers (for example, participating providers and preferred providers), such as many PPOs, where cost sharing is lower for preferred providers, only preferred providers would be counted towards ECP standards; and
(ii) The issuer's integrated delivery system provides all of the categories of services provided by entities in each of the ECP categories in each county in the network plan's service area as outlined in the general ECP standard, or otherwise offers a contract to at least one ECP outside of the issuer's integrated delivery system per ECP category in each county in the network plan's service area that can provide those services to low-income, medically underserved individuals.
(3) A network plan applying for QHP certification to be offered through a Federally-facilitated Exchange must include as part of its QHP application the status of contract offers to qualified ECPs available in the network plan's service area. A network plan does not need to report on the status of contract offers for all available ECPs in the network plan's service area, but must at least report on the status of contract offers for all ECPs which the issuer has either included in its network plan or offered a contract to be included in its network plan within each service area.
* * * * *
31. Add § 156.236 to subpart C to read as follows:
Provider access and essential community providers standards for non-network plans.
(a) A QHP that does not use a network of providers (a non-network plan) must ensure access to a range of providers that accept the non-network plan's benefit amount as payment in full, including essential community providers (ECPs) and providers that specialize in mental health and substance use disorder services, to ensure that services will be accessible without unreasonable delay. A non-network plan does not provide access to a range of providers in this manner by simply providing some benefit amount for covered services rendered by any provider without providing the Exchange any other contextual information.
(b) For plan years beginning on or after January 1, 2028, a non-network plan applying for QHP certification to be offered as a QHP through a Federally-facilitated Exchange must submit the following information to the Federally-facilitated Exchange for a determination that it provides access to a sufficient choice of providers that accept the non-network plan's benefit amount as payment in full, and reasonable and timely access to ECPs that accept the plan's benefit amount as payment in full:
(1) The non-network plan's assessed percentage of providers in each plan's service area that accepts the plan's benefit amount as payment in full; and for ECPs, whether the non-network plan meets at least a minimum percentage, as specified by HHS, of available ECPs that accept the plan's benefit amount as payment in full in each plan's service area collectively across all ECP categories defined under § 156.235(a)(2)(ii)(B), and at least a minimum percentage of available ECPs that accept the plan's benefit amount as payment in full in each plan's service area within certain individual ECP categories, as specified by HHS;
(2) For ECPs, whether the non-network plan offers the benefit amount as payment in full to at least one ECP in each of the eight (8) ECP categories per county in the plan's service area described in § 156.235(a)(2)(ii)(B);
(3) For ECPs, whether the non-network plan offers the benefit amount as payment in full to all available Indian health care providers in the plan's service area;
(4) The non-network plan's strategy for conducting continuous outreach to available providers (including ECPs) in a particular area to determine whether they would accept the plan's benefit amount as payment in full;
(5) The non-network plan's strategy for making benefit amounts publicly available, including to plan enrollees, potential enrollees, and providers (including ECPs), in an easily accessible and understandable format, and for regularly updating any changes to benefit amounts;
(6) The non-network plan's methodology for determining benefit amounts;
(7) The non-network plan's strategy for providing consumer-friendly and public information about potential balance billing scenarios and expected out-of-pocket costs, including historical data on actual out-of-pocket costs incurred by its enrollees while accessing providers (including ECPs) in the area, and information on navigating episodes of care with multiple benefit amounts (including for ancillary providers and services);
(8) The availability of an exceptions process under the non-network plan for enrollees who cannot find providers (including ECPs) willing to accept the benefit amount as payment in full; and
(9) The non-network plan's strategy for providing adequate customer service or online provider directory assistance resources to assist plan enrollees and potential enrollees in finding providers (including ECPs) in their area who will accept the plan's benefit amount as payment in full, and to assist plan enrollees in receiving real-time cost estimates prior to care being furnished.
(iv)
Provider access.
The provider access standards for accreditation used by the recognized accrediting entities must, at a minimum, be consistent with the general requirements for network plans codified in § 156.230(a)(2) and (3) and the general requirements for non-network plans codified in § 156.236(a).
* * * * *
34. Section 156.480 is amended by revising paragraph (c) introductory text and paragraph (c)(6) to read as follows:
Oversight of the administration of the advance payments of the premium tax credit, cost-sharing reductions, and user fee programs.
* * * * *
(c)
Audits and compliance reviews.
HHS or its designee may audit or conduct a compliance review of an issuer offering a QHP through an Exchange to assess its compliance with the applicable requirements related to administration of the advance payments of the premium tax credit, cost-sharing reductions, and user fee programs. Compliance reviews conducted under this section will follow the standards set forth in § 156.715.
* * * * *
(6)
Circumstances requiring HHS enforcement.
If HHS determines that the State Exchange or State-based Exchange on the Federal platform is not enforcing or fails to substantially enforce compliance with the applicable requirements related to administration of the advance payments of the premium tax credit, cost-sharing reductions, and user fee programs, then HHS may do so and may pursue the imposition of civil money penalties as specified in § 156.805 for noncompliance by QHP issuers participating in the State Exchange or State-based Exchange on the Federal platform.
35. Section 156.800 is amended by revising paragraph (b) to read as follows:
(b)
Scope.
Sanctions under subpart I are applicable for noncompliance with QHP issuer participation standards and other standards applicable to issuers offering QHPs in a Federally-facilitated Exchange. Sanctions under paragraph (a)(1) of this section are also applicable for noncompliance by QHP issuers participating in State Exchanges and State-based Exchanges on the Federal platform when HHS is responsible for enforcement of any of the requirements applicable to the actions identified in § 156.805(a) that are applicable to issuers offering a QHP in a State Exchange or State-based Exchange on the Federal platform.
* * * * *
36. Section 156.805 is amended by revising paragraphs (b) introductory text and (f) to read as follows:
Bases and process for imposing civil money penalties in Federally-facilitated Exchanges.
* * * * *
(b)
Factors in determining the amount of civil money penalties assessed.
In determining the amount of civil money
( printed page 29877)
penalties, HHS will identify the lawful purpose or purposes of the civil money penalty, and take into account the following factors as appropriate to the circumstances of the case:
* * * * *
(f)
Circumstances requiring HHS enforcement in State Exchanges and State-based Exchanges on the Federal platform.
(1) HHS will enforce the requirements applicable to the actions identified in paragraph (a) of this section that are applicable to issuers offering a QHP in a State Exchange or State-based Exchange on the Federal platform, if the State with enforcement authority over such Exchange notifies HHS that it is not enforcing these requirements or if HHS makes a determination using the process set forth at 45 CFR 150.201,
et seq.
that such State is failing to substantially enforce these requirements.
(2) If HHS is responsible under paragraph (f)(1) of this section for enforcement of the requirements applicable to the actions identified in paragraph (a) of this section that are applicable to issuers offering a QHP in a State Exchange or State-based Exchange on the Federal platform, HHS may impose civil money penalties on an issuer in such Exchange, in accordance with the bases and process for imposing civil money penalties set forth in this section.
37. Section 156.810 is amended by revising paragraph (a)(8) to read as follows:
Bases and process for decertification of a QHP offered by an issuer through a Federally-facilitated Exchange.
(a) * * *
(8) The QHP issuer substantially fails to meet the requirements under § 156.230 related to provider access standards for network plans, § 156.235 related to essential community provider access standards for network plans, or § 156.236 related to provider access and essential community providers standards for non-network plans, as applicable;
* * * * *
38. Section 156.903 is amended by adding paragraph (d) to read as follows:
Scope of Administrative Law Judge's (ALJ) authority.
* * * * *
(d) The ALJ, upon his or her own motion or at the request of a party, may issue subpoenas if they are reasonably necessary for the full presentation of a case.
(1) The party must file a written request for a subpoena with the ALJ at least 5 calendar days before the date set for the hearing.
(2) The request must:
(i) Identify the witnesses or documents to be produced;
(ii) Describe their addresses or location with sufficient particularity to permit them to be found; and
(iii) Specify the pertinent facts the party expects to establish by the witnesses or documents, and indicate why those facts could not be established without use of a subpoena.
(3) Subpoenas are issued in the name of the Secretary.
39. Section 156.935 is amended by adding paragraph (f) to read as follows:
(f) This section does not apply to appeals of civil money penalties imposed under § 156.805 for violations identified during audits or compliance reviews conducted in accordance with § 156.480(c).
40. Section 156.1215 is amended by revising paragraphs (b) and (c) to read as follows:
(b)
Netting of payments and charges for later years.
As part of its payment and collections process, HHS may net payments owed to issuers and their affiliates operating under the same tax identification number against amounts due to the Federal Government from the issuers and their affiliates under the same taxpayer identification number for advance payments of the premium tax credit, advance payments of and reconciliation of cost-sharing reductions, payment of Federally facilitated Exchange user fees, payment of State Exchanges utilizing the Federal platform user fees, HHS risk adjustment, reinsurance, and risk corridors payments and charges, administrative fees for utilizing the Federal Independent Dispute Resolution process in accordance with § 149.510(d)(2) of this subchapter, and civil money penalties assessed for violations of any applicable Exchange standards and requirements or Public Health Service Act standards and requirements applicable to issuers.
(c)
Determination of debt.
Any amount owed to the Federal Government by an issuer and its affiliates for advance payments of the premium tax credit, advance payments of and reconciliation of cost-sharing reductions, Federally-facilitated Exchange user fees, including any fees for State-based Exchanges utilizing the Federal platform, HHS risk adjustment, reinsurance, risk corridors, unpaid administrative fees for utilizing the Federal Independent Dispute Resolution process in accordance with § 149.510(d)(2), and civil money penalties assessed for violations of any applicable Exchange standards and requirements or Public Health Service Act standards and requirements applicable to issuers, after HHS nets amounts owed by the Federal Government under these programs, is a determination of a debt.
41. Section 156.1220 is amended by revising paragraph (b)(1) to read as follows:
(1)
Manner and timing for request.
A request for an informal hearing must be made in writing and filed with HHS within 30 calendar days of the date of the reconsideration decision under paragraph (a)(6) of this section. If the last day of this period is not a business day, the request for an informal hearing must be made in writing and filed by the next applicable business day.
* * * * *
Robert F. Kennedy, Jr.,
Secretary, Department of Health and Human Services.
Footnotes
1.
The Patient Protection and Affordable Care Act (Pub. L. 111-148) was enacted on March 23, 2010. The Healthcare and Education Reconciliation Act of 2010 (Pub. L. 111-152), which amended and revised several provisions of the Patient Protection and Affordable Care Act, was enacted on March 30, 2010. In this rulemaking, the two statutes are referred to collectively as the “Patient Protection and Affordable Care Act” or “Affordable Care Act.”
21.
Section 251A(6)(B) of the Balanced Budget and Emergency Deficit Control Act, 2 U.S.C. 901a(6)(B), as amended, requires sequestration of non-exempt direct spending programs, excluding Medicare, through fiscal year 2031 at a uniform percentage calculated by OMB to be necessary to meet certain deficit reduction targets in fiscal year 2021. That uniform percentage was calculated to be 5.7 percent in the OMB Report to the Congress on the Joint Committee Reductions for Fiscal Year 2021.
22.
The State payment transfer formula refers to part of the Federally certified risk adjustment methodology that applies in States where HHS is responsible for operating the program. The formula calculates payments and charges at the State market risk pool level (prior to the calculation of the high-cost risk pool payments and charges that apply beginning with the 2018 benefit year). See, for example, 81 FR 94080.
23.
For the 2017 through 2022 benefit years, there is a set of 11 binary enrollment duration factors in the adult models that decrease monotonically from 1 to 11 months, reflecting the increased annualized costs associated with fewer months of enrollments. See, for example, 81 FR 94071 through 94074. These enrollment duration factors were replaced beginning with the 2023 benefit year with HCC-contingent enrollment duration factors for up to 6 months in the adult models. See, for example, 87 FR 27228 through 27230.
24.
For the 2018 benefit year, there were 12 RXCs, but starting with the 2019 benefit year, the two severity-only RXCs were removed from the adult models. See, for example, 83 FR 16941.
27.
For unique State-specific plans, we apply the CSR adjustment factors that correspond to each plan's AV. See, for example, the 2025 Payment Notice, 89 FR 26252 through 26253. However, a different approach is taken for States whose State-specific plans take the form of Medicaid expansion plans offered on the Exchange (for example, Arkansas), because these Medicaid-expansion plans are identical in all their parameters, including AV and degree of plan liability, to other plans offered on the Exchange in those States and are differentiated from their comparable plans only in eligibility criteria, plan enrollment selection, and sources of funding.
Ibid.
Footnote 79 of the 2025 Payment Notice (89 FR 26253), erroneously stated that, “we would use the proposed CSR adjustment factor of 1.12 for Arkansas 94 percent AV Medicaid-expansion plans and the proposed CSR adjustment factor that corresponds to the silver metal level zero cost sharing variants (that is, the proposed 1.46 CSR adjustment factor for zero cost sharing variants) for Arkansas 100 percent AV Medicaid-expansion plans in the plan liability risk score calculation.” See
https://regtap.cms.gov/reg_librarye.php?i=4690.
Arkansas 100 percent AV Medicaid-expansion plan features remain more similar to the 94 percent silver plan variant than to the silver metal level zero cost sharing variant for AI/AN enrollees. Therefore, for both the 94 and 100 percent Medicaid-expansion plans in Arkansas, we use the same CSR adjustment factor of 1.12 used for the 94 percent silver plan variant CSR adjustment factor in the plan liability risk score calculation. We will continue to align the CSR adjustment factor for both the 94 and 100 percent Medicaid-expansion plans in Arkansas with the 94 percent silver plan variant CSR adjustment factor for the 2027 benefit year and beyond unless the AVs for these unique Arkansas-specific plans change. More information on the CSR factors used for CSR plan variants, including State program CSR variants, can be found in the applicable Risk Adjustment HHS-Developed Risk Adjustment Model Algorithm “Do It Yourself (DIY)” Software instructions, available at
https://www.cms.gov/marketplace/resources/regulations-guidance#Premium-Stabilization-Programs.
28.
Although we do receive the next year of enrollee-level EDGE data prior to the proposed rule, that data must go through several quality and analysis checks before it is useable for HHS risk adjustment model calibration.
30.
Because EDGE data do not generally account for drug rebates per the EDGE Server Business Rules (ESBR) (available at
https://regtap.cms.gov/reg_librarye.php?i=3765), for the purposes of risk adjustment recalibration, we also incorporate assumptions about drug rebates in our trending of prescription drug data.
31.
We note that we apply some standard data exclusions to all years of enrollee-level EDGE data for the purposes of risk adjustment recalibration. For example, enrollees with at least one capitated claim in EDGE are excluded from recalibration because we have some concerns that the methods for computing and reporting derived amounts from capitated claims could be inconsistent across issuers and would not provide reliable or comparable data. See, for example, the 2025 Payment Notice (89 FR 26252).
32.
To begin this transition for the 2026 benefit year HHS risk adjustment models, we applied the specialty drug trend to 1 year of trending Hepatitis C treatment costs (that is, the trend from 2025 to 2026) for all 3 years of enrollee-level EDGE data used (that is, 2020, 2021, and 2022 benefit year enrollee-level EDGE data) in 2026 benefit year HHS risk adjustment model recalibration. To continue this transition for the 2027 benefit year HHS risk adjustment models, we apply the specialty drug trend to 2 years of trending Hepatitis C treatment costs (that is, the trend from 2025 to 2026 and from 2026 to 2027) for all 3 years of enrollee-level EDGE data (that is, 2021, 2022, and 2023 benefit year enrollee-level EDGE data) proposed to be used in 2027 benefit year HHS risk adjustment model recalibration.
33.
Since the start of model calibration for the HHS risk adjustment models in benefit year 2014, the COVID-19 PHE and its potential impact on utilization and costs has been the only such situation to date. Other events and policy changes have not risen to the same level of uniqueness or potential impact.
34.
The current specification of the HCC-contingent enrollment duration factors was finalized in the 2023 Payment Notice (87 FR 27228 through 27230). Please note that the HCC-contingent enrollment duration factors only apply to adult HHS risk adjustment models. See footnote 46 of the HHS-Operated Risk Adjustment Technical Paper on Possible Model Changes, (CMS, 2021; available at
https://www.cms.gov/files/document/2021-ra-technical-paper.pdf). See also the 2021 Payment Notice (85 FR at 7103 and 7104).
40.
At the time of the publication of the proposed rule, the most recently available version was the January 23, 2026 version of the 2025 Benefit Year Risk Adjustment HHS-Developed Risk Adjustment Model Algorithm “Do It Yourself (DIY)” Software, available at
https://www.cms.gov/marketplace/resources/regulations-guidance.
Although not directly applicable to the 2027 benefit year, the 2025 benefit year software contains information that can be used to correctly filter and format enrollee-level data for the calculation of risk scores using the proposed 2027 benefit year HHS risk adjustment model coefficients that we are finalizing in this rule.
41.
As finalized in the 2020 Payment Notice (84 FR 17466 through 17468), we will maintain the high-cost risk pool parameters for the 2020 benefit year and beyond, unless amended through notice-and-comment rulemaking. We did not propose changes to the high-cost risk pool parameters for the 2027 benefit year. Therefore, we will maintain the $1 million threshold and 60 percent coinsurance rate for the 2027 benefit year.
42.
In the 2026 Payment Notice, we incorrectly stated that for RXC eligibility (including medically administered injectable claims), a professional or outpatient medical claim does not need to have a risk adjustment eligible service code or bill type code. We subsequently updated the January 2025 version of the 2024 Benefit Year Risk Adjustment DIY software instructions (
https://www.cms.gov/files/document/cy2024-diy-instructions-01072025.pdf) to reflect this erroneous statement. In the Final 2024 Risk Adjustment DIY software instructions updated April 9, 2025 (
https://www.cms.gov/files/document/cy2024-diy-instructions-04092025.pdf), we corrected this error and clarified that the HCPCS-level file for RXC assignment can only be sourced from institutional inpatient and outpatient claims with RA-eligible bill types. We expect ACFs related to prescription drugs will be sourced using the same criteria as RXCs. We will announce changes to HHS risk adjustment claims filtering with regard to RXC or ACF eligibility in future guidance documents or notice and comment rulemakings, as appropriate.
43.
Because there are no catastrophic plans in the small group market, separating the individual and small group markets would require the recalibration of 12 additional risk adjustment models, one for each metal level (except catastrophic) and age group (adult, child, infant). This would result in a total of 27 HHS risk adjustment models instead of the current 15.
44.
For a State-level summary of enrollment by market, see, for example, CMS. (2025). Summary Report On Individual And Small Group Market Risk Adjustment Transfers For The 2024 Benefit Year, Appendix A.
https://www.cms.gov/files/document/ra-report-by2024.pdf.
47.
GLP-1 drugs approved for the treatment of diabetes are presently included in RXC 7 (Anti-Diabetic Agents, Except Insulin and Metformin Only) to the extent that their positive predictive values (PPVs) with diabetes HCCs are high and do not indicate a large degree of over-prescribing. See, for example Table 10a of the 2025 Benefit Year risk Adjustment HHS-Developed Risk Adjustment Model Algorithm “Do It Yourself (DIY)” Software Technical Details, available at:
https://www.cms.gov/marketplace/resources/regulations-guidance.
49.
See, for example, Kautter, J., et al. (2014). The HHS-HCC Risk Adjustment Model for Individual and Small Group Markets under the Affordable Care Act.
Medicare & Medicaid Research Review (4)
3.
https://www.cms.gov/mmrr/Downloads/MMRR2014_004_03_a03.pdf.
See also the 2014 Payment Notice (77 FR 73127 through 73129).
51.
See, for example, Kautter, J., Pope, G.,C., Ingber, M., et al. (2014). The HHS-HCC Risk Adjustment Model for Individual and Small Group Markets under the Affordable Care Act.
Medicare & Medicaid Research Review, 4
(3).
https://www.cms.gov/mmrr/Downloads/MMRR2014_004_03_a03.pdf.
53.
See section 2701 of the Public Health Service Act (42 U.S.C. 300gg) as amended by section 1201 of the Affordable Care Act. See also the Market Rules and Rate Review final rule (78 FR 13406, 13411-13).
62.
See CMS. (2025).
Guidance on Hardship Exemptions for Individuals Ineligible for Advance Payment of the Premium Tax Credit or Cost-sharing Reductions Due to Income, and Streamlining Exemption Pathways to Coverage. https://www.cms.gov/files/document/guidance-hardship-exemptions.pdf.
We note that this final rule is also finalizing an amend to § 155.605(d)(1) to codify the expansion of hardship exemption eligibility in this guidance document to individuals who are ineligible for APTC or CSR due to projected household income below 100 percent or above 250 percent FPL.
63.
This guidance applies to consumers in FFE States and in SBE States that choose to have exemptions processed through the FFE, which currently include all SBEs except California, Connecticut, Maryland, and the District of Columbia. We note that in the 2027 Payment Notice proposed rule (91 FR 6353), we proposed to expand § 155.605(d)(1) to codify the expansion of hardship exemption eligibility to consumers ineligible for APTC or CSRs due to projected household income below 100 percent or above 250 percent FPL in all States.
65.
In other words, this will factor out the contribution of demographic factors, enrollee RXCs, HCC-RXC interaction factors, CSR adjustment factors, HCC-contingent enrollment duration factors, and interacted HCC counts factors towards the EDGE risk scores of enrollees with HCCs. As previously explained, these factors are not included in the calculation of the HCC-associated error rate during HHS-RADV error estimation. See Section 13.3.1.3.3 Calculate Error Rates of the BY24 HHS-RADV Protocols, available at
https://regtap.cms.gov/uploads/library/HHS-RADV_2024_Benefit_Year_Protocols_v1_5CR_060625.pdf.
67.
Although enrollees without HCCs will be excluded from IVA sampling beginning with 2025 benefit year HHS-RADV, enrollees without HCCs on EDGE will be categorized into stratum 10 for these operational purposes.
68.
Enrollees without HCCs may contribute to the PLRS through demographic factors, enrollee RXCs, and CSR adjustment factors. As previously explained, these enrollees are not included in the calculation of the HCC-associated error rate during HHS-RADV error estimation.
69.
While HHS-RADV also includes processes for validating RXCs and demographic and enrollment factors, any errors regarding these factors are treated as materially incorrect EDGE server data submissions. See 83 FR 16970 through 16971. Also see 84 FR 17501 and 85 FR 77002 through 77005.
70.
Enrollees without HCCs may contribute to the PLRS through demographic factors, enrollee RXCs, and CSR adjustment factors. As previously explained, these enrollees are not included in the calculation of the HCC-associated error rate during HHS-RADV error estimation.
71.
While HHS-RADV also includes processes for validating RXCs and demographic and enrollment factors, any errors regarding these factors are treated as materially incorrect EDGE server data submissions. See 83 FR 16970 through 16971. Also see 84 FR 17501 and 85 FR 77002 through 77005.
72.
Each benefit year of HHS-RADV, HHS releases the HHS-RADV Protocols, which provide details on the operations and workflows associated with HHS-RADV, including error estimation, and are available on REGTAP.
75.
We estimated that the total costs for HHS to operate the risk adjustment program on behalf of States for the 2026 calendar year would be approximately $65 million. See the 2026 Payment Notice (90 FR 4424 at 4448).
77.
See Letter from Acting HHS Secretary Eric Hargan to CMS Administrator Seema Verma Regarding Payments to Issuers for Cost-Sharing Reductions (CSRs) (Oct. 12, 2017), conveying legal opinion of Attorney General Jefferson B. Sessions III (Oct. 11, 2017). Available at
https://www.hhs.gov/sites/default/files/csr-payment-memo.pdf.
78.
For purposes of this preamble, we use the term “CSR loading” to refer to any rating practices to increase premiums to offset amounts of unreimbursed CSRs whether that is “silver loading” or “broad loading.”
86.
If the rate filing contains a proposed increase that meets or exceeds the threshold at § 154.200(a)(1) (currently 15 percent), then the State or CMS also reviews the proposed increase to determine if it is an unreasonable rate increase. Also see 45 CFR 154.205(a). When CMS reviews a rate increase subject to review under § 154.210(a), CMS will determine that the rate increase is an unreasonable rate increase if the increase is an excessive rate increase, an unjustified rate increase, or an unfairly discriminatory rate increase.
88.
Under § 156.80(d)(2)(i), an issuer may vary premium rates for a particular plan from its market-wide index rate for a relevant State market based on the actuarial value and cost-sharing design of the plan, including accounting for, if permitted by the applicable State authority, CSR amounts provided to eligible enrollees under § 156.410, provided the issuer does not otherwise receive reimbursement for such amounts. Therefore, if there is a valid appropriation such that HHS and the Department of the Treasury resume making advance payments of CSRs, issuers may not apply any CSR load to QHPs receiving advance CSR payments. In addition, in the event that advance payments of CSRs are made to issuers to reimburse them for CSRs provided, HHS will calculate these monthly advance payments using the formula finalized in the 2015 Payment Notice and using the standard methodology as set forth in 45 CFR 156.430(c)(2) for reconciliation of CSR amounts. See 79 FR 13804-13808. Also see 90 FR 4424, 4488.
93.
The information collection described in this section will be submitted as a revision to the currently approved PRA package CMS-10379 (OMB Control Number 0938-1141) for OMB review under the Paperwork Reduction Act.
94.
We note that a plan-level adjustment to account for unreimbursed CSRs is not considered actuarially justified under § 156.80 solely because the adjustment or methodology on which it is based was prescribed by a State.
96.
This should not be construed to prevent broad loading, as issuers are permitted to spread these costs evenly across all plans in the single risk pool. See for example, 78 FR 39870, 39878 (July 2, 2013) (administrative costs generally may be spread across an issuer's entire risk pool).
98.
Under the CMS standard methodology, issuers re-adjudicate the actual complete set of claims incurred by an enrollee in the CSR plan variation as if they had been enrolled in the associated standard plan to determine the difference the enrollee would have paid in deductibles, copayments, coinsurance, and other out-of-pocket expenses for EHBs (other than premiums and balance billing). The difference equals the amount of CSRs provided by the issuer. See Manual for Reconciliation of the Cost-Sharing Reduction Component of Advance Payments for Benefit Year 2017 (March 29, 2018) at
https://www.cms.gov/cciio/resources/forms-reports-and-other-resources/downloads/final-csr-reconciliation-guidance-by2017.pdf.
101.
Section 1311(c)(5) of the Affordable Care Act instead requires the Secretary to make available to all Exchanges a model Exchange website template developed by the Secretary. Section 1311(d)(4)(C) of the Affordable Care Act requires the Exchanges to maintain an internet website through which enrollees and prospective enrollees of qualified health plans may obtain standardized comparative information on such plans.
102.
Policy and operational priorities and then-new Federal laws included implementation of E.O. 13985 and E.O.14009; Affordable Care Act-related programs under the American Rescue Plan Act of 2021 (ARP) (namely, the State Exchange Modernization Grant Program) and the No Surprises Act; and activities undertaken by HHS to implement the COVID-19 SEP. While activities undertaken pursuant to the No Surprises Act continue, E.O. 13985 and 14009 have been rescinded. Additionally, many resources needed to implement and oversee administration of the enhanced subsidies codified under the ARP, and later extended under the Inflation Reduction Act of 2022, are no longer needed since they expired at the end of 2025. The State Exchange Modernization Grant program also has concluded and States closed out their grants between January and August of 2023. Additionally, activities related to implementing the COVID-19 SEP, including coordination with and oversight of State Exchanges with respect to similar SEPs they implemented in response to the COVID-19 public health emergency (PHE), concluded before the PHE ended in 2023.
105.
See
section 1311(d)(4)(D) of Affordable Care Act and 45 CFR 155.205(b).
Also see
sections 1311(c)(3) and (c)(4) of Affordable Care Act and §§ 155.1400 and 155.1405.
106.
Covered entities such as States, recipients of Federal financial assistance from HHS, programs or activities administered by HHS under title I of Affordable Care Act (such as the FFE), and programs or activities administered by any entity established under Title I (such as State Exchanges), must comply with applicable Federal civil rights laws that prohibit discrimination on the basis of race, color, national origin, sex, age, and disability. These laws include section 1557 of Affordable Care Act (42 U.S.C. 18116) (Section 1557), Title VI of the Civil Rights Act of 1964 (42 U.S.C. 2000det seq.) (Title VI), section 504 of the Rehabilitation Act of 1973 (29 U.S.C. 794) (Section 504), and the Americans with Disabilities Act of 1990 (29 U.S.C. 12101et seq.) (ADA).
107.
Section 1401(a) of Affordable Care Act added new section 36B to the Code, which provides for PTCs for eligible individuals, while section 1402 of Affordable Care Act provides for CSRs for eligible individuals. For individuals to be eligible to receive PTCs, among other requirements, the Affordable Care Act requires that individuals be enrolled in a QHP through an Exchange. We have interpreted this statutory language to allow a QHP issuer to enroll an applicant who initiates enrollment directly with the QHP issuer. See § 156.1230, whereby individuals enrolling directly on the website of a QHP issuer are considered enrolled “through an Exchange” so long as the issuer meets applicable requirements. We adopted a similar approach to allow a web-broker to enroll an applicant who seeks to enroll through the web-broker's website. See § 155.220(a)(2) and (c), whereby individuals enrolling directly through the site of a web-broker are considered enrolled “through an Exchange” so long as the web-broker meets applicable requirements.
108.
This approach is consistent with the 15-month State Exchange approval timeline requirements under § 155.106(a)(2) for States seeking to newly establish and operate a State Exchange to submit its State Exchange Blueprint for review and approval. While the SBE-EDE model is distinct from the State Exchange model, in the proposed rule we stated that we would consider a transition to the SBE-EDE model to require a significant operational effort to implement such that a consistent timeframe would have many benefits to the State and HHS, particularly while the SBE-EDE model remains a new Exchange model.
109.
This approach is consistent with the requirement that a State notify HHS and receive written approval from HHS before significant changes are made to the Exchange Blueprint. See, for example, 77 FR 18316. In the proposed rule, we stated that significant changes could include altering a key function of Exchange operations or other changes to the Exchange Blueprint that would have an impact on the operation of the Exchange. This includes, but is not limited to, the process for enrollment in a QHP. See, for example, 76 FR 41871.
110.
As detailed in § 155.105(e), HHS generally has 60 days after receipt of a completed request to complete its review of a significant change to an Exchange Blueprint and, for good cause, may extend the review period by an additional 30 days up to a total of 90 days.
111.
In addition to ensuring there is at least one website available in the State that satisfies all accessibility requirements under § 155.205(c), we proposed that there must also be at least one website available in the State through which consumers can view and enroll in all available QHPs in the State.
113.
On November 12, 2025, the Government Accountability Office (GAO) released a report “
Health Insurance Marketplaces: CMS Has Limited Assurance That Premium Tax Credits Exclude Certain State Benefit Costs.
GAO-25-107220, available at
https://files.gao.gov/reports/GAO-25-107220/index.html.
We concurred with the GAO's recommendation to review CMS' current oversight approach for defrayal of State mandated benefits and determine whether additional oversight is needed, and that work is ongoing.
114.
These elements appear in the EHB Final Rule (78 FR 12838) and the 2017 Payment Notice (81 FR 12242). We acknowledge that the element that the State requirement must be “specific to required care, treatment, or services” has not previously been included in § 155.170. However, in the EHB Final Rule (78 FR 12838), we stated that “[W]e interpret `State-required benefits' to include the care, treatment and services that an issuer must provide to its enrollees. Other State laws that do not relate to specific benefits, including those relating to providers and benefit delivery method, are not addressed in § 155.170.”
See also
the 2025 Payment Notice (81 FR 26264).
115.
We stated that if this proposal is finalized as proposed, the policy finalized in the 2025 Payment Notice would remain applicable for PYs 2025-2026. We stated that States would not be required to defray the costs of any State-mandated benefits that are included in the State's EHB-benchmark plan as EHB during PYs 2025-2026 but would be required to defray such costs beginning in PY 2027.
119.
MHPAEA generally does not mandate coverage for mental health or substance use disorder benefits. Rather, if a plan provides medical/surgical benefits and mental health or substance use disorder benefits, it must comply with MHPAEA's parity provisions.
120.
See 81 FR 12204, 12243-4 (Mar. 8, 2016) (explaining that imposing benefit mandates depending on a plan's status as a QHP or whether it is sold through the Exchange may violate section 1252 of the Affordable Care Act).
122.
The exception to this would be when the benefit and the provider type are interchangeable such that only that provider type can provide the service. For example, a mandate requiring inclusion of massage therapists would be tantamount to a mandated benefit for massage therapy.
126.
See for example, the GAO report published on December 3, 2025, in which the GAO developed and submitted fictitious applications via brokers and subsequently gained fully-subsidized health insurance coverage through the Federal Exchanges. GAO (2025, Dec. 3).
Patient Protection and Affordable Care Act: Preliminary Results from Ongoing Review Suggest Fraud Risks in the Advance Premium Tax Credit Persist. https://www.gao.gov/products/gao-26-108742.
131.
Some States define “carriers” as an entity authorized to provide health insurance, benefits, or services, including health maintenance organizations (HMOs), nonprofit health service plans, and authorized insurers. These are essentially insurance companies that offer health benefit plans regulated by the States.
134.
See 45 CFR 155.220(g)(3)(i). The one exception is for situations where the agent, broker, or web-broker fails to maintain the appropriate license under applicable State law(s). See 45 CFR 155.220(g)(3)(ii). In these limited situations, HHS may immediately terminate the agent, broker, or web-broker's Exchange agreement(s) for cause without any further opportunity to resolve the matter upon providing notice to the agent, broker, or web-broker. Ibid.
136.
The agent, broker, or web-broker must continue to protect any PII accessed during the term of their Exchange agreements.
See,
for example, 45 CFR 155.220(g)(4) and 45 CFR 155.260.
138.
In the May 6, 2024
Federal Register
, we finalized the Nondiscrimination in Health Programs and Activities final rule (89 FR 37522) (hereinafter referred to as the “2024 Final Rule”), which interpreted prohibited discrimination on the basis of sex to include, inter alia, discrimination on the basis of sex characteristics, including intersex traits, gender identity, and sex stereotypes. Several district courts vacated or stayed certain provisions of the 2024 Final Rule and preliminarily enjoined HHS from enforcing certain provisions of the 2024 Final Rule—primarily those prohibiting discrimination on the basis of gender identity.
See Florida.
v.
Dep't of Health & Hum. Servs.,
739 F. Supp. 3d 1091 (M.D. Fla. 2024);
Tennessee
v.
Kennedy,
807 F. Supp. 3d 613, 630 (S.D. Miss. 2025);
Texas
v.
Becerra,
No. 6:24-CV-211-JDK, 2024 WL 4490621 (E.D. Tex. Aug. 30, 2024). Although the Secretary filed appeals in these cases, the United States Court of Appeals for the Fifth and Eleventh Circuits subsequently dismissed all appeals pursuant to motions filed after the change in administration, and certain sections of the 2024 Final Rule relating to an expanded interpretation of sex discrimination remain vacated or stayed.
142.
The personal exemption amount was reduced to zero for tax years 2018 through 2025 by Section 11041 of the Tax Cuts and Jobs Act (Pub. L. 115-97). This reduction was made permanent by Section 70103 of the WFTC legislation.
161.
GAO. (2016 Nov.). Patient Protection and Affordable Care Act: Results of Enrollment Testing for the 2016 Special Enrollment Period, GAO-17-78.
https://www.gao.gov/products/gao-17-78.
172.
Source: Internal CMS enrollment data. CMS reviewed net premium changes for consumers who had a $0 premium for PY2024 and a subsequent >$0 premium for PY2025. The analysis shows how many consumers had net premiums of >$0-$5, >$5-$10, >$10-$15, >$15-$20, >$20-$25, >$25-$50, >$50-$100, >$100-$300, >$300-$500, and >$500.
176.
HHS has interpreted section 1411(a)(2)(A) of the Affordable Care Act to require an Exchange to align its APTC eligibility rules with the Code's PTC eligibility rules.
179.
GAO. (2016 Nov.).
Patient Protection and Affordable Care Act: Results of Enrollment Testing for the 2016 Special Enrollment Period,
GAO-17-78.
https://www.gao.gov/products/gao-17-78.
184.
CMS. (2025, September 4). Guidance on Hardship Exemptions for Individuals Ineligible for Advance Payment of the Premium Tax Credit or Cost-sharing Reductions Due to Income and Streamlining Exemption Pathways to Coverage. Available at
https://www.cms.gov/files/document/guidance-hardship-exemptions.pdf.
187.
Average enrollment-weighted monthly premium from MLR data for 2013 ($244) and from Unified Rate Review Template (URRT) filings for 2026 ($779), reflecting a 219 percent cumulative increase and a 26 percent increase in 2026 alone. See CMS, 2027 Payment Notice Proposed Rule, 91 FR 6292, 6353 n.123 (Feb. 11, 2026). By comparison, inflation increased 39 percent over the same period. See Bureau of Labor Statistics, U.S. Dep't of Labor, Consumer Price Index for All Urban Consumers (CPI-U): U.S. City Average, All Items, available at
https://www.bls.gov/cpi/.
Average hourly earnings for private sector employees increased 53 percent over the same period. See Bureau of Labor Statistics, U.S. Dep't of Labor, Current Employment Statistics Survey: Average
Hourly Earnings of All Employees, Total Private, available at
https://www.bls.gov/ces/.
197.
Average enrollment-weighted monthly premium from MLR data for 2013 ($244) and from Unified Rate Review Template (URRT) filings for 2026 ($779), reflecting a 219 percent cumulative increase and a 26 percent increase in 2026 alone.
See 91 FR 6292, 6353 n.123 (Feb. 11, 2026). By comparison, inflation increased 39 percent over the same period.
See
Bureau of Labor Statistics,
Consumer Price Index for All Urban Consumers (CPI-U),
available at
https://www.bls.gov/cpi/.
Average hourly earnings for private sector employees increased 53 percent over the same period.
See
Bureau of Labor Statistics,
Current Employment Statistics Survey: Average Hourly Earnings of All Employees, Total Private,
available at
https://www.bls.gov/ces/.
200.
See 42 U.S.C. 18071 (requiring issuers to reduce cost-sharing for eligible low-income enrollees in silver plans); 45 CFR 156.420 (establishing the cost-sharing reduction variants for silver plans at 73, 87, and 94 percent actuarial value).
201.
See 42 U.S.C. 18031(d)(4)(H) authorizing the Secretary to establish additional criteria for certifying health plans as qualified health plans, including such other criteria as the Secretary determines appropriate).
202.
See Pension Benefit Guaranty Corp.
v.
LTV Corp.,
496 U.S. 633, 650 (1990) (“It is a particularly dangerous ground on which to rest an interpretation of a prior statute when it concerns . . . a proposal that does not become law.”) (citing
United States
v.
Price, 361 U.S. 304, 313 (1960)).
236.
We considered the most recent projections from the Congressional Budget Office at the time, as we have in prior rulemakings, and our own internal data. See, for example, 89 FR 26218; see also, Congressional Budget Office (CBO). (2025, September 18).
The Estimated Effects of Enacting Selected Health Coverage Policies on the Federal Budget and on the Number of People With Health Insurance. https://www.cbo.gov/system/files/2025-09/61734-Health.pdf.
238.
Spanemberg, J.C., Cardoso, J.A., Slob, E.M.G.B, & Lopez-Lopez, J. (2019). Quality Of Life Related To Oral Health And Its Impact In Adults.
Journal of Stomatology, Oral and Maxillofacial Surgery, 120
(3), 234-239.
https://doi.org/10.1016/j.jormas.2019.02.004.
242.
According to 2025 U.S. Bureau of Labor Statistics data, smaller firms (defined by BLS as up to 249 workers) comprise 73 percent of all firms. See U.S. Bureau of Labor Statistics (BLS).
Employment By Size Of Establishment, Private Industry. https://www.bls.gov/charts/county-employment-and-wages/employment-by-size.htm.
247.
See
Elani HW, Rahman MS, Wallace J, Rosenthal MB, Sommers BD. (2024). Availability Of Adult Dental Plans In The Affordable Care Act Marketplaces, 2016-23. Health
Affairs
43(11):1587-1596. doi:10.1377/hlthaff.2024.00307.
251.
Due to an oversight, the proposed rule stated that “an individual who satisfies the requirements for a catastrophic plan at the time of enrollment in the plan under section 1302(e)(2) of the Affordable Care Act at the time of enrollment in the multi-year plan.”
252.
See CMS. (2026). Guidance on Hardship Exemptions for Individuals Ineligible for Advance Payment of the Premium Tax Credit or Cost-sharing Reductions Due to Income, and Streamlining Exemption Pathways to Coverage. guidance-on-hardship-exemptions.pdf.
253.
Musich, S., Wang, S., Hawkins, K., & Klemes, A. (2016). The Impact of Personalized Preventive Care on Health Care Quality, Utilization, and Expenditures. Population Health Management,
19(6),
389-397.
https://doi.org/10.1089/pop.2015.0171;
and Maciosek, M.V., LaFrance, A.B., Dehmer, S.P., McGree, D.A., Flottemesch, T.J., Xu, Z. Solberg, L.I. (2017). Updated Priorities Among Effective Clinical Preventive Services. Annals of Family Medicine.
https://pmc.ncbi.nlm.nih.gov/articles/PMC5217840/.
256.
For resources explaining the State payment transfer formula, see Pope, G.C.,
et al.
(2014). Risk Transfer Formula for Individual and Small Group Markets Under the Affordable Care Act.
Medicare and Medicaid Research Review, 4
(3).
https://www.cms.gov/mmrr/downloads/mmrr2014_004_03_a04.pdf.
257.
See 45 CFR 144.103 and 155.20 (defining “policy year” generally as the calendar year and “plan year” as “a consecutive 12 month period during which a health plan provides coverage for health benefits,” respectively).
See also80 FR 75488, 75494 (Dec. 2, 2015) and 81 FR 12204, 12210 (Mar. 8, 2016) (providing that a plan year may be shorter but not longer than 12 months).
258.
See section III.E.7 of this final rule, which explains how in this final rule, we are finalizing a proposal with modifications to increase the annual limitation on cost sharing that is required for catastrophic plans to be 130 percent of the annual maximum limitation on cost sharing and to delay implementation of this policy until PY 2028; and to newly allow QHP issuers in the individual market already offering a bronze plan that offers an annual limitation on cost sharing at or below the annual maximum limitation on cost sharing to also offer, within the same service area, bronze plans that use a higher annual limitation on cost sharing and to set a maximum limitation for bronze plans starting with PY 2027.
262.
CMS has consulted with the Treasury Department and the IRS and they have similarly advised that until further tax guidance is issued in connection with the Departments' VBID guidelines, catastrophic plans will only be treated as high deductible health plans that are HSA-compatible under Code section 223(c)(2)(H) if pre-deductible coverage is limited to preventive services described in section 2713(a) of the PHS Act and at least three primary care visits.
263.
Failure to pay premiums on a timely basis is not considered a loss of coverage that triggers a special enrollment period.
See 45 CFR 155.420(e). Therefore, individuals who voluntarily terminate coverage may not be able to enroll in other individual market coverage until the next annual open enrollment period.
267.
Cost sharing is defined at § 156.20 as any expenditure required by or on behalf of an enrollee with respect to EHB; the term includes deductibles, coinsurance, copayments, or similar charges, but excludes premiums, balance billing amounts for non-network providers that are not prohibited by the No Surprises Act, and spending for non-covered services.
269.
In the 2025 Patient Protection and Affordable Care Act; Marketplace Integrity and Affordability final rule (90 FR 27074, 27166 through 27168 (June 25, 2025)), HHS finalized a change to the methodology for calculating the premium adjustment percentage such that the average per capita premium will be based on the National Health Expenditure Accounts (NHEA) estimates of private health insurance (PHI) premiums (excluding Medigap and the medical portion of property and casualty insurance) for the 2026 benefit year and beyond. As discussed in the proposed rule, for the 2027 benefit year, HHS did not propose changes to the methodology to calculate the premium adjustment percentage or related parameters. As such, for the 2027 benefit year, we released these parameters in guidance entitled “Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage for the 2027 Benefit Year.” Available at
https://www.cms.gov/files/document/2027-papi-parameters-guidance-2026-01-29.pdf.
270.
For PYs 2014-2017, we applied a single trend factor for medical and prescription drug costs combined. We began applying different trend factors for medical and prescription drug costs in 2018.
271.
There is one year that is an exception. The maximum annual limitation on cost sharing decreased for PY 2025 due to updated NHEA data from the CMS Office of the Actuary. In the NHEA Projections 2021-2030 data set available at the time of calculation of the PY 2024 maximum annual limitation on cost sharing, the estimated 2023 per capita employer-sponsored insurance (ESI) premiums value used in the premium adjustment percentage index calculation was $7,292. In the NHEA Projections 2022-2031 data set available at the time of the calculation of the PY 2025 maximum annual limitation on cost sharing, the estimated 2024 per capita ESI premiums value used in the premium adjustment percentage index calculation was $7,110, which was lower than the previously projected 2023 per capita ESI premiums from the previous data set.
See
Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage for the 2025 Benefit Year (November 15, 2023) available at
https://www.cms.gov/files/document/2025-papi-parameters-guidance-2023-11-15.pdf. See also,
the Premium Adjustment Percentage, Maximum Annual Limitation on Cost Sharing, Reduced Maximum Annual Limitation on Cost Sharing, and Required Contribution Percentage for the 2024 Benefit Year (December 12, 2022) available at
https://www.cms.gov/files/document/2024-papi-parameters-guidance-2022-12-12.pdf.
The current NHEA projections are available at
https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/projected.
272.
Patient Protection and Affordable Care Act; HHS Notice of Benefit and Payment Parameters for 2018; Proposed Rule, 81 FR 61456, 61510 (September 6, 2016).
274.
After the 2023 Payment Notice raised the lower bound of the permitted AV
de minimis
range from −4% to −2%, no bronze plans could be certified as a QHP with an AV below 58 percent. In Table 11, where bronze plans' AVs are not permitted, they are marked “N/A”. The asterisks are used to indicate when that AV percentage is nearly impossible to reach for a bronze plan through its cost sharing design. The non-zero numbers marked with an asterisk represent actual bronze plans that had an even lower AV calculated for them than for a theoretical bronze plan that only provides non-preventative benefit coverage after an enrollee has reached their MOOP limit when it is set at the given plan year's annual limitation on cost sharing, with the MOOP set as equal to the given plan year's annual limitation on cost sharing. Bronze plans with AVs calculated as lower than this minimum-generosity design are no longer possible after an algorithm improvement in the 2021 AV Calculator, which ensured that plans using “copay with deductible” would no longer have an underestimated AV (due to previous AV Calculators overestimating enrollee spending during the plan's deductible phase).
275.
Expanded bronze plans are bronze plans currently referenced in § 156.140(c) that cover and pay for at least one major service, other than preventive services, before the deductible or meet the requirements to be a high deductible health plan within the meaning of section 223(c)(2) of the Code. (81 FR 94058).
276.
See
FDA
v.
Brown & Williamson Tobacco Corp.,
529 U.S. 120, 133 (2000) (explaining that statutes should be interpreted as a “symmetrical and coherent regulatory scheme”);
Gustafson
v.
Alloyd Co.,
513 U.S. 561, 570 (1995) (statutory provisions should not be interpreted in a manner that renders any part “superfluous”).
277.
See
King
v.
Burwell,
576 U.S. 473, 492 (2015) (recognizing that reviewing courts will exercise independent judgment in evaluating whether the agency has acted within its statutory authority and noting that the Affordable Care Act's statutory language must be read in context and in light of the statute's structure and purpose).
282.
Pursuant to § 150.203, in the event that a State notifies HHS that it does not have statutory authority to enforce or that it is not otherwise enforcing one or more of the provisions of title XXVII of the PHS Act, or if HHS determines that the State is not substantially enforcing the requirements, HHS has the responsibility to enforce these provisions in the State. As of the date of the proposed rule, the following States have notified HHS that they do not have the authority to enforce or are not otherwise enforcing the Affordable Care Act market reform provisions, including the EHB: Missouri, Oklahoma, Tennessee, Texas, and Wyoming.
286.
For example, section 1302(c)(1) of the Affordable Care Act requires HHS to index the maximum annual limitation on cost sharing forward in accordance with the premium adjustment percentage, while the IRS indexes the maximum allowable MOOP for HDHPs forward to account for inflation (see section 223(c)(2)(A)(ii)(I) of the Code). This creates a discrepancy between the Affordable Care Act's maximum annual limitation on cost sharing and the maximum allowable HDHP MOOP, which could also explain the recent shift in bronze plans at the upper end of the permissible +5 range.
287.
Under these requirements, when an internet website of a web-broker or issuer is used to complete the QHP selection, at a minimum the internet website must differentially display all standardized options prominently and in accordance with the requirements under § 155.205(b)(1) in a manner consistent with that adopted by HHS for display on the FFE website and with standards defined by HHS, unless HHS approves a deviation.
289.
Although the official nomenclature for these plans was “standardized options” in the 2017 through 2019 Payment Notices, when we resumed this policy in the 2023 Payment Notice and in all subsequent Payment Notices, the official nomenclature became “standardized plan options.”
297.
Taylor EA, Carman KG, Lopez A, Muchow AN, Roshan P, & Eibner C. (2016) Consumer Decision-making in the Health Care Marketplace. RAND Corporation.
298.
Chao Zhou and Yuting Zhang, “The Vast Majority of Medicare Part D Beneficiaries Still Don't Choose the Cheapest Plans That Meet Their Medication Needs.” Health Affairs, 31, no.10 (2012): 2259-2265.
299.
Taylor EA, Carman KG, Lopez A, Muchow AN, Roshan P, and Eibner C. Consumer Decision-making in the Health Care Marketplace. RAND Corporation. 2016.
300.
Chao Zhou and Yuting Zhang, “The Vast Majority of Medicare Part D Beneficiaries Still Don't Choose the Cheapest Plans That Meet Their Medication Needs.” Health Affairs, 31, no.10 (2012): 2259-2265.
304.
Plan-county combinations are the count of unique plan ID and FIPS code combinations. This measure was used because a single plan may be available in multiple counties, and specific limits on non-standardized plan options may have different impacts on one county where there are four plans of the same product network type and metal level versus another county where there are only two plans of the same product network type and metal level, for example.
305.
Taylor EA, Carman KG, Lopez A, Muchow AN, Roshan P, & Eibner C. (2016) Consumer Decision-making in the Health Care Marketplace. RAND Corporation; Chao Zhou and Yuting Zhang, “The Vast Majority of Medicare Part D Beneficiaries Still Don't Choose the Cheapest Plans That Meet Their Medication Needs.” Health Affairs, 31, no.10 (2012): 2259-2265.
308.
Geocoding is the process of converting provider street addresses, into geographic coordinates (latitude and longitude), enabling them to be used in the calculation of time and distance analysis.
311.
CMS currently uses a calculation for network adequacy that factors in both time and distance. Time and distance is especially critical in large metro areas where, for example 90 percent of Exchange eligible consumers must have access to certain types of providers within 15 miles and 30 minutes. There may be many providers available within 15 miles, but the time to travel would far exceed 30 minutes due to slower travel speeds in urban areas. The “and” condition makes it necessary for a provider location to be available within both the mileage and the time criteria. We are aware of State Exchanges and SBE-FP States that have implemented an “or” condition, particularly in rural areas where topographical limitations may make it feasible to meet a time requirement or a distance requirement without a need to meet both to ensure reasonable access to all services by enrollees without unreasonable delay.
313.
Revisions made to § 156.235(a)(2)(i) and (b)(2)(i) implemented separate minimum percentage requirements for the FQHC and family planning provider categories by specifying that a plan applying for QHP certification to be offered through an FFE must include as participating providers within their provider network at least a minimum percentage of available ECPs in each plan's service area
within certain ECP categories,
as specified by HHS. HHS applied this requirement to the FQHC and family planning provider categories.
314.
In calculating an issuer's satisfaction of the threshold requirements, we consider the number of in-network ECPs with which an issuer designates a contract is executed within their QHP certification application. The number of in-network contracted ECPs includes any qualified ECPs located within the plan's service area. The number of in-network contracted ECPs is the numerator in the threshold requirement calculation, and this number is divided by all available and qualified ECPs located within the plan's network service area in the denominator to create a threshold percentage. For the family planning provider and FQHC threshold requirements, we only count family planning providers and FQHCs in the calculation methodology within the numerator and denominator and not other ECP categories.
315.
For PY 2026, the average threshold percentage for all FFE QHP issuers, including issuers in States performing plan management, for the overall ECP threshold requirement was 71 percent, 85 percent for the family planning provider threshold requirement, and 79 percent for the FQHC threshold requirement.
316.
Ghost networks typically refer to circumstances where large numbers of providers or health care facilities are listed as “in-network” on an issuer's provider directory, but are not actually available to care for enrollees (that is, no longer in-network, not accepting new patients, inaccurate provider directory information, etc.).
320.
QHP certification and ECP Data Collection to Support QHP Certification are already assessed and
encompassed by the currently approved information collections (
Continuation of Data Collection to Support QHP Certification and other Financial Management and Exchange Operations
(OMB Control Number 0938-1187 (CMS-10433)/Expiration date: June 30, 2025) and
Essential Community Provider/Network Adequacy (ECP/NA) Data Collection to Support QHP Certification
(OMB Control Number. 0938-1415 (CMS-10803)/Expiration date: December 31, 2027)).
321.
The ECP UI is the web-based interface of the ECP section of the Marketplace Plan Management System (MPMS) Module, which is a sub-system of the Health Insurance and Oversight System, where QHP issuers demonstrate that they have a sufficient number and geographic distribution of ECPs. Medical QHP and SADP issuers submit provider data in each network associated with a QHP and/or SADP into the ECP UI.
322.
Options for contract negotiation statuses are as follows: Contract Executed; Contract Offer Made-Awaiting Response; Pre-Contract Negotiations in Progress (Contract Offer Not Made Yet); Offer Rejected; Contract Not Offered Due to No Response Following Issuer Outreach; Facility Closed; Facility Does Not Contract And Has No Interest To Contract With Commercial Insurance; Facility Does Not Provide Medical Services; Facility Does Not Provide Dental Services; Provider is in an Exclusivity Contract That Prohibits Us From Contracting With Them; Provider is Not Licensed, Accredited, or Certified by the State; Provider Has Relocated Outside Service Area Preventing Us From Contracting With Them.
325.
HHS has developed and regularly maintained an ECP List since 2015, which provides a large national snapshot of the universe of qualified ECPs across all States and by various category types.
332.
We stated in the proposed rule that such an exceptions process could, for example, ensure that the non-network plan covers any additional out-of-pocket costs incurred by an enrollee who could not locate an ECP willing to accept the plan's benefit amount as payment in full.
334.
Section 1311(e)(1)(B)(i) of the Affordable Care Act and § 155.1000(c)(2)(i) prohibit Exchanges from excluding a health plan from certification on the basis that such plan is a fee-for-service plan. We confirmed that under this proposal, an Exchange may properly conclude that a non-network plan that is a fee-for-service plan may be denied certification under the interest standard for other criteria besides the fact that it is a fee-for-service plan.
335.
Except that the Exchange may not exclude a health plan: (i) on the basis that such plan is a fee-for-service plan; (ii) through the imposition of premium price controls; or (iii) on the basis that the plan provides treatments necessary to prevent patients' deaths in circumstances the Exchange determines are inappropriate or too costly (77 FR 18405).
336.
As stated in the Exchange Establishment Rule (77 FR 18405), some examples of such additional selection criteria include: (1) reasonableness of the estimated costs supporting the calculation of the health plan's premium and cost-sharing levels; (2) past performance of the health insurance issuer; (3) quality improvement activities; (4) enhancements of provider networks, including the availability of network providers to new patients; (5) service area of the QHPs (that is, the size of a service area and the amount of choice afforded to the consumers within that service area); and (6) premium rate increases from previous years and proposed rate increases.
338.
For example, research indicates that among commercially insured adults with HIV, the mean all-cause and HIV-related per patient per month costs were $2,657 and $1,497, and all cause costs per patient per month for adults with PrEP were $1,761. Other research shows that the estimated direct costs of 4 to 6 months of tuberculosis treatment is an estimated $23,000 per person. Lastly, a meta-analysis found the average total annual costs for hemophilia treatment can start around $200,000 per patient and be as high as $869,940. Chen CY, Donga P, Campbell AK, Taiwo B. Economic Burden of HIV in a Commercially Insured Population in the United States.
JHEOR.
2023;10(1):10-19. doi:10.36469/001c.56928. PMID:36721765. Available at
https://jheor.org/article/56928-economic-burden-of-hiv-in-a-commercially-insured-population-in-the-united-states.
Winston CA, Marks SM, Carr W. Estimated Costs of 4-Month Pulmonary Tuberculosis Treatment Regimen, United States. Emerg Infect Dis. 2023 Oct;29(10):2102-2104. doi: 10.3201/eid2910.230314. PMID: 37735769; PMCID: PMC10521593. Available at
https://pmc.ncbi.nlm.nih.gov/articles/PMC10521593/.
Chen Y, Cheng SJ, Thornhill T, Solari P, Sullivan SD. Health care costs and resource use of managing hemophilia A: A targeted literature review. J Manag Care Spec Pharm. 2023 Jun;29(6):647-658. doi: 10.18553/jmcp.2023.29.6.647. PMID: 37276036; PMCID: PMC10387983. Available at
https://pmc.ncbi.nlm.nih.gov/articles/PMC10387983/.
342.
Enumah, S.J., & Chang, D.C. (2021). Predictors of Financial Distress Among Private U.S. Hospitals. The Journal of Surgical Research, 267, 251-259.
https://doi.org/10.1016/j.jss.2021.05.025.
343.
We have developed and regularly maintained an ECP List since 2015, which provides a large national snapshot of the universe of qualified ECPs across all States and by various category types. The ECP List helps us identify the exact geographic location and distribution of ECPs to highlight specific ECPs that may be available within an issuer's service area and available for contracting with the issuer to satisfy ECP requirements.
344.
Higgins, A., Brainard, N., & Veselovskiy, G. (2016). Characterizing Health Plan Price Estimator Tools: Findings From a National Survey. The American Journal of Managed Care, 22(2), 126-131.
https://pubmed.ncbi.nlm.nih.gov/26885672/;
Berlin, N.L., Chopra, Z., Bryant, A., Agius, J., Singh, S.R., Chhabra, K.R., Schulz, P., West, B.T., Ryan, A.M., & Kullgren, J.T. (2022). Individualized Out-of-Pocket Price Estimators for “Shoppable” Surgical Procedures: A Nationwide Cross-Sectional Study of US Hospitals. Annals Of Surgery Open: Perspectives Of Surgical History, Education, And Clinical Approaches, 3(2), e162.
https://doi.org/10.1097/AS9.0000000000000162.
347.
We have addressed the interest standard in past rulemaking, including in the 2012 Exchange Final Rule (77 FR 18405) and in the 2017 Payment Notice (81 FR 12289).
348.
Except that the Exchange may not exclude a health plan: (i) on the basis that such plan is a fee-for-service plan; (ii) through the imposition of premium price controls; or (iii) on the basis that the plan provides treatments necessary to prevent patients' deaths in circumstances the Exchange determines are inappropriate or too costly (77 FR 18405).
352.
Plan year data inaccuracies described to HHS or the State Exchange (as applicable) before the end of the 3-year period described in § 156.1210(c) beginning at the end of the plan year to which the inaccuracy relates are eligible for resolution and payment to the issuer of any confirmed APTC underpayments. Data inaccuracies identified after the 3-year period are not eligible for repayment to the issuer. However, should an issuer identify a payment error after the 3-year period, the issuer must notify HHS or the State Exchange (as applicable) and repay any overpayments.
353.
We stated in the proposed rule that the bases and processes for imposing CMPs in FFEs and the circumstances in which HHS may exercise enforcement in State Exchanges would not be impacted by a State's decision to implement the proposed DE option under § 155.221(j), if finalized.
354.
See PHS Act sections 2723(b)(2)(G), 2718(b)(3), and 2761(b) (indicating CMPs shall be paid to the Secretary and shall be available without appropriation and until expended for the purpose of enforcing the provisions for which the penalty was imposed); see also Affordable Care Act section 1321(c)(2) (authorizing the Secretary to impose CMPs on the same basis as detailed in section 2723(b) of the PHS Act).
355.
CMPs may be imposed on an issuer in an Exchange, if, based on credible evidence, HHS has reasonably determined that the issuer has engaged in one or more of the actions listed under § 156.805(a).
356.
See, for example,
§ 156.480(c)(4), which requires, in part, that a QHP issuer must comply with actions set forth in a final audit report and provide a written corrective action plan for HHS approval and QHP issuer implementation.
357.
Improper payments are often discovered long after an improper payment is made because these audits are conducted on benefit year data after the 3-year window for resolution of payment inaccuracies described in § 156.1210(c) closes, which is well after an issuer receives an APTC on behalf of an enrollee and claims were processed.
363.
In accordance with 45 CFR 156.480(c)(3)(i), HHS will share its preliminary audit findings with the issuer, who will then have 30 calendar days to respond to such findings in the format and manner specified by HHS.
See also,45 CFR 156.806 (requiring HHS to provide 30 days for the issuer to respond to and provide additional information to refute an alleged violation before imposing a CMP).
364.
In the 2022 Payment Notice (86 FR 24242), we set forth a framework for HHS enforcement of the applicable Federal APTC, CSR, and user fee standards in situations where State authorities fail to substantially enforce those standards with respect to the QHP issuers participating in State Exchanges and SBE-FPs.
368.
A CMP is assessed only after any applicable imposition and appeal processes set forth in 45 CFR subtitle A, subchapter B have been exhausted or expire.
371.
U.S. Bureau of Labor Statistics. Employed full time: Median usual weekly nominal earnings (second quartile): Wage and salary workers: 16 years and over [LEU0252881500A], retrieved from FRED, Federal Reserve Bank of St. Louis.
https://fred.stlouisfed.org/series/LES1252881500Q.
Annual Estimate, 2024.
374.
Certain values are rounded for readability and are indicated by the use of terms such as 'approximately' or 'average.' All cost and burden calculations are based on unrounded figures to ensure accuracy.
375.
Certain values are rounded for readability and are indicated by the use of terms such as `approximately' or `average.' All cost and burden calculations are based on unrounded figures to ensure accuracy.
376.
Certain values are rounded for readability and are indicated by the use of terms such as 'approximately' or 'average.' All cost and burden calculations are based on unrounded figures to ensure accuracy.
377.
See
the U.S. Bureau of Labor Statistics (n.d.). Occupational Employment and Wage Statistics, May 2024 Occupation Profiles. Dep't. of Labor.
https://www.bls.gov/oes/current/oes_stru.htm.
390.
Exemption forms and related information are approved under OMB control number 0938-1190 (CMS-10466). Information collected through the coverage application and used for the automated exemption process is approved under OMB control number 0938-1191.
See
Office of Management and Budget, Information Collection Review, OMB Control No. 0938-1190, available at
https://www.reginfo.gov/public/do/PRAOMBHistory?ombControlNumber=0938-1190.
396.
The reduction in APTC was calculated by multiplying the estimated new SVIs by the previous SVI expiration rate (293,073 × 0.137 = 40,151) and then multiplying that number by the estimated annual APTC amount per SEP consumer (40,151 × $2,625 = $105,396,375).
398.
Bhaumik, Deesha, et al., “What Happens if the Adult Medicaid Dental Benefit Goes Away?,” American Dental Association Health Policy Institute (March 2025).
399.
19 CareQuest Institute for Oral Health, “Dental Care in Crisis: Tracking the Cost and Prevalence of Emergency Department Visits for Non-Traumatic Dental Conditions,” (Oct. 2025).
402.
Plan year data inaccuracies described to HHS or the State Exchange (as applicable) before the end of the 3-year period beginning at the end of the plan year are eligible for resolution and payment to the issuer of any confirmed APTC underpayments. Data inaccuracies identified after the 3-year period are not eligible for repayment to the issuer. However, should an issuer identify a payment error after the 3-year period, the issuer must notify HHS or the State Exchange (as applicable) and repay any overpayments.
See 45 CFR 156.1210(c).
405.
Deshpande, Manasi, and Yue Li. 2019. “Who Is Screened Out? Application Costs and the Targeting of Disability Programs.”
American Economic Journal: Economic Policy
11 (4): 213-48.DOI: 10.1257/pol.20180076. Available at
https://pubs.aeaweb.org/doi/pdfplus/10.1257/pol.20180076.
406.
Homonoff, Tatiana, and Jason Somerville. 2021. “Program Recertification Costs: Evidence from SNAP.”
American Economic Journal: Economic Policy
13 (4): 271-98.DOI: 10.1257/pol.20190272. Available at
https://pubs.aeaweb.org/doi/pdfplus/10.1257/pol.20190272.
415.
See
the U.S. Bureau of Labor Statistics (n.d.). Occupational Employment and Wage Statistics, May 2024 Occupation Profiles. Dep't. of Labor.
https://www.bls.gov/oes/current/oes_stru.htm.
Use this for formal legal and research references to the published document.
91 FR 29526
Web Citation
Suggested Web Citation
Use this when citing the archival web version of the document.
“Patient Protection and Affordable Care Act, HHS Notice of Benefit and Payment Parameters for 2027; and Basic Health Program,” thefederalregister.org (May 20, 2026), https://thefederalregister.org/documents/2026-10050/patient-protection-and-affordable-care-act-hhs-notice-of-benefit-and-payment-parameters-for-2027-and-basic-health-progra.