Medicaid Program; Medicaid Managed Care State Directed Payments and Medicaid Fee-for-Service Targeted Medicaid Practitioner Payments
This proposed rule describes alternatives to modify the limit on the total payment rate and other requirements for State directed payments in Medicaid managed care. We propose t...
Centers for Medicare & Medicaid Services (CMS), Department of Health and Human Services (HHS).
ACTION:
Proposed rule.
SUMMARY:
This proposed rule describes alternatives to modify the limit on the total payment rate and other requirements for State directed payments in Medicaid managed care. We propose these changes based on our authority to interpret and implement section 1902(a)(4) of the Social Security Act (the Act) with respect to prepaid inpatient health plans and prepaid ambulatory health plans, and section 1903(m)(2)(A)(iii) of the Act, which require that contracts between States and managed care organizations to provide payments under a risk-based contract for services and associated administrative costs that are actuarially sound. This rule also proposes to set a limit for certain targeted Medicaid payments in Medicaid fee-for-service. We propose this change based on our authority to interpret and implement section 1902(a)(30)(A) of the Act with respect to certain targeted Medicaid payments which require that payments be consistent with efficiency, economy, and quality of care and are sufficient to enlist enough providers so that care and services are available under the plan at least to the extent that such care and services are available to the general population in the geographic area.
DATES:
To be assured consideration, comments must be received at one of the addresses provided below, by July 21, 2026.
ADDRESSES:
In commenting, please refer to file code CMS-2449-P.
Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
2.
By regular mail.
You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-2449-P, P.O. Box 8016, Baltimore, MD 21244-8016.
Please allow sufficient time for mailed comments to be received before the close of the comment period.
3.
By express or overnight mail.
You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-2449-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore, MD 21244-1850. For information on viewing public comments, see the beginning of the
SUPPLEMENTARY INFORMATION
section.
Inspection of Public Comments:
All comments received before the close of the comment period are available for viewing by the public, including any personally identifiable or confidential business information that is included in a comment. We post all comments received before the close of the comment period on the following website as soon as possible after they have been received:
https://www.regulations.gov.
Follow the search instructions on that website to view public comments. CMS will not post on
Regulations.gov
public comments that make threats to individuals or institutions or suggest that the commenter will take actions to harm an individual. CMS continues to encourage individuals not to submit duplicative comments. We will post acceptable comments from multiple unique commenters even if the content is identical or nearly identical to other comments.
Title XIX of the Social Security Act (the Act) established the Medicaid program as a Federal-State partnership for the purpose of providing and financing medical assistance to specified groups of eligible individuals. States [1]
have considerable flexibility in designing their programs but must abide by requirements specified in the Federal Medicaid statute and regulations. Each State is responsible for administering its Medicaid program in accordance with an approved State plan, which specifies the scope of covered services, groups of eligible individuals, payment methodologies, and all other information necessary to assure the State plan describes a comprehensive and sound structure for operating the Medicaid program, and ultimately, provides a clear basis for claiming Federal matching funds.
As of November 2025, the Medicaid program provided essential health care coverage to more than 76 million [2]
individuals. In 2024, Medicaid had annual outlays of more than $931.7 billion (total computable).[3]
The program covers a broad array of health benefits and services critical to many populations. For example, Medicaid pays for approximately 41 percent of all births in the United States,[4]
is the largest payer of long-term services and supports,[5]
and provides health coverage for more than half of all children in the United States.[6]
Depending on the State and its Medicaid program structure, beneficiaries access their health care services using fee-for-service (FFS) and/or managed care delivery systems. States also provide services through demonstrations and waiver programs under both delivery systems. In 2024, approximately 85 percent of Medicaid beneficiaries were enrolled in managed care; [7]
the remaining individuals
( printed page 30401)
received all or some services through FFS.
On June 6, 2025, President Trump signed a Presidential Memorandum titled “Eliminating Waste, Fraud, and Abuse in Medicaid” [8]
(hereinafter referred to as “the Presidential Memorandum”). This memorandum directed the Secretary of Health and Human Services (the Secretary) to eliminate fraud, waste, and abuse in Medicaid, including by ensuring Medicaid payment rates are not higher than Medicare, to the extent permitted by applicable law. The memorandum noted the Administration's concerns that certain State financing arrangements have, at times, been used to further waste, fraud, and abuse in Medicaid. It also noted that State directed payment (SDPs) have grown substantially in recent years, and that this trajectory threatens the Federal Treasury and Medicaid's long-term stability. It also pointed to distortions created by the incentives in arrangements in which provider taxes or intergovernmental transfers (IGTs) are returned to the same providers through Medicaid payments, thereby absolving States of their obligation to share in the burden of financing the joint Federal and State Medicaid program. When States are relieved of these financial obligations through such arrangements, the memorandum stated that States' incentives for prudent administration are reduced. The memorandum noted that both seniors on Medicare and Medicaid recipients deserve access to quality care in a system free from fraud, waste, and abuse. We are concerned that increased Medicaid payments that are not aligned with statutory objectives such as supporting access to care may instead reward providers primarily on the basis of their ability to supply the non-Federal share of their own payments, rather than on advancing access to or quality of care for Medicaid beneficiaries.
On July 4, 2025, Public Law (Pub. L.) 119-21 was enacted (which CMS refers to as the “Working Families Tax Cut” (WFTC) legislation). Section 71116(a) of the WFTC legislation directed the Secretary to revise § 438.6(c)(2)(iii) to limit the total payment rate for certain SDPs for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at an academic medical center (AMC) (hereinafter referred to as the “four services”) effective with the first rating period beginning on or after the date of enactment, July 4, 2025. Section 71116(b) of the WFTC legislation provides for the temporary grandfathering period for certain SDPs and requires a phase down beginning with the first rating period that starts on or after January 1, 2028.
To implement section 71116 of the WFTC legislation, the Secretary instructed us to develop and release this proposed rule. To aid State planning efforts until a final rule is issued, we issued a Dear Colleague Letter on February 2, 2026 with preliminary guidance on how we were interpreting certain provision in section 71116 of the WFTC legislation.[9 10]
We noted that the information was preliminary in nature and final policies would depend on the contents of the final rule. This letter also signaled that we were considering proposing changes to the limit for the total payment rate for SDPs for other services beyond the four services specified by section 71116 of the WFTC legislation as part of our broader effort to align this rulemaking with the Presidential Memorandum referenced in the letter.
SDPs have become a significant part of the Medicaid program. When designed and implemented with fiscal integrity, they can help States implement provider payment initiatives and delivery system reform efforts that further advance access to care and enhance quality of care in Medicaid managed care. However, as we have seen over time, they can also become vehicles for waste and abuse in the Medicaid program. For example, when these SDPs are not designed to improve care for beneficiaries and are instead designed to financially advantage a small number of providers and disincentivize States from investing in their own Medicaid programs by primarily relying on provider taxes or IGTs to fund the non-Federal share, these arrangements may contribute to inefficient or wasteful Medicaid spending. Through the issuance of the February 2, 2026 Dear Colleague Letter providing preliminary guidance on section 71116 of the WFTC legislation, and publication of the Preserving Medicaid Funding for Vulnerable Populations-Closing a Health Care-Related Tax Loophole Final Rule (91 FR 4794), we have taken steps to address fiscal integrity concerns in Medicaid. Reforming SDP requirements would allow CMS and States to refocus on the original purpose of these arrangements, which is to permit States to direct certain managed care plan expenditures [11]
within specified parameters to improve access and ultimately, quality of beneficiary care. We strongly believe that Medicaid beneficiaries deserve access to quality care in a system free from fraud, waste, and abuse and that promotes strong fiscal and program integrity.
A. Medicaid Managed Care Delivery Systems
The volume of Medicaid beneficiaries enrolled in Medicaid managed care has grown from 81 percent in 2016 to 85 percent in 2022.[12]
States may implement a Medicaid managed care delivery system using four Federal authorities—sections 1915(a), 1915(b), 1932(a), and 1115(a) of the Act; each is briefly described later in this section.
Under section 1915(a) of the Act, States can implement a voluntary managed care program by executing a contract with organizations that the State has procured using a competitive procurement process; we review and approve these contracts in accordance with § 438.3(a). To require beneficiaries to enroll in a managed care program to receive services, a State must obtain approval from us under two primary authorities:
Through a State plan amendment (SPA) that meets standards set forth in section 1932(a) of the Act, States can implement a mandatory managed care delivery system. This authority does not allow States to require beneficiaries who are dually eligible for Medicare and Medicaid (dually eligible beneficiaries), American Indians/Alaska Natives (except as permitted in section 1932 (a)(2)(C) of the Act), or children with special health care needs to enroll in an applicable managed care program. State plans, once approved by us, remain in effect until modified by the State, with our approval.
Through a waiver under section 1915(b) of the Act, States are permitted to require all Medicaid beneficiaries to enroll in a managed care delivery system, including dually eligible beneficiaries, American Indians/Alaska Natives, or children with special health care needs. After our approval, a State
( printed page 30402)
may operate a section 1915(b) waiver for a 2-year period before requesting renewal for an additional 2-year period. Section 1915(b) of the Act waivers may be approved for a 5-year initial period and renewed for additional 5-year periods if they include individuals who are dually eligible for Medicare and Medicaid.
We may also authorize managed care programs as part of demonstration projects under section 1115(a) of the Act that include waivers permitting a State to require all Medicaid beneficiaries to enroll in a managed care delivery system, including dually eligible beneficiaries, American Indians/Alaska Natives, and children with special health care needs. Under this authority, States may seek additional flexibility to demonstrate and evaluate innovative policy approaches for delivering Medicaid benefits, as well as the option to provide services not typically covered by Medicaid. Such demonstrations are approvable only if it is determined that the demonstration would promote the objectives of the Medicaid statute and the demonstration is subject to an independent evaluation.
With the exception of section 1915(a) of the Act, the authorities discussed previously all permit States to operate their Medicaid managed care programs without complying with the following standards of the Medicaid statute outlined in section 1902 of the Act:
Statewideness
(section 1902(a)(1) of the Act): States may implement a managed care delivery system in specific areas of the State (generally counties/parishes) rather than the whole State.
Comparability of Services
(section 1902(a)(10)(B) of the Act): States may provide different benefits to people enrolled in a managed care delivery system.
Freedom of Choice
(section 1902(a)(23)(A) of the Act): States may generally require individuals to receive their Medicaid services only from a managed care plan's network of providers or primary care provider, including through PCCMs and PCCM entities.
B. Relevant Medicaid Managed Care Rules
In the May 6, 2016
Federal Register
(81 FR 27498), we published the “Medicaid and Children's Health Insurance Program (CHIP) Programs; Medicaid Managed Care, CHIP Delivered in Managed Care, and Revisions Related to Third Party Liability” final rule (hereinafter referred to as “the 2016 final rule”) that modernized the Medicaid and CHIP managed care regulations to reflect changes in the use of managed care delivery systems. The 2016 final rule aligned many of the rules governing Medicaid and CHIP managed care with those of other major sources of coverage; implemented applicable statutory provisions; strengthened actuarial soundness payment provisions to promote the accountability of managed care program rates; strengthened efforts to reform delivery systems that serve Medicaid and CHIP beneficiaries; and enhanced policies related to program integrity. The 2016 final rule applied many of the Medicaid managed care rules to separate CHIP programs, particularly in the areas of access, finance, and quality through cross-references at subpart L of 42 CFR part 457 to 42 CFR part 438. States may administer CHIP programs that are separate CHIP programs or as programs that are operated as an expansion of the State's Medicaid program.
In the November 13, 2020
Federal Register
(85 FR 72754), we published the “Medicaid Program; Medicaid and Children's Health Insurance Program (CHIP) Managed Care” final rule (hereinafter referred to as the “2020 final rule”) which streamlined the Medicaid and CHIP managed care regulatory framework to relieve regulatory burdens; support State flexibility and local leadership; and promote transparency, flexibility, and innovation in the delivery of care. The rule was intended to ensure that the regulatory framework was efficient and feasible for States to implement in a cost-effective manner and ensure that States can implement and operate Medicaid and CHIP managed care programs without undue administrative burdens.
In the May 10, 2024
Federal Register
(89 FR 41002), we published the “Medicaid Program; Medicaid and Children's Health Insurance Program (CHIP) Managed Care Access, Finance, and Quality” final rule (hereafter referred to as the “2024 final rule”) which established new standards to help States improve their monitoring of access to care and codified requirements for State use of in lieu of services and settings. The final rule also enhanced quality, fiscal and program integrity requirements for SDPs, addressed impermissible redistribution arrangements related to SDPs, and added clarity to the requirements related to medical loss ratio calculations. The 2024 final rule also codified a limit to the total payment rate (often referred to as the “total payment rate limit”) for certain types of SDPs at the average commercial rate (ACR).
We note that SDPs authorized under § 438.6(c) do not apply to separate CHIP programs. SDPs can, however, be used in Medicaid programs that include Title XXI-funded Medicaid expansion CHIP beneficiaries; that is, programs in which a State receives Federal funding to expand Medicaid eligibility to optional targeted low-income children that meets the requirements of section 2103 of the Act. For purposes of this document, references to “Medicaid” mean = States' programs operated under Title XIX, including those that cover Medicaid expansion CHIP populations, and do not include separate CHIP programs.
C. History of State Directed Payments
Section 1903(m)(2)(A)(iii) of the Act requires that contracts between States and managed care organizations (MCOs) provide for payments under a risk-based contract for services and associated administrative costs to be actuarially sound. Under section 1902(a)(4) of the Act, we also have authority to establish methods of administration for Medicaid that are necessary for the proper and efficient operation of the State plan. Under this authority in section 1902(a)(4) of the Act, we extended the requirement for actuarially sound capitation rates to prepaid inpatient health plans (PIHPs) and prepaid ambulatory health plans (PAHPs). The regulations addressing actuarially sound capitation rates are set forth in § 438.4 through 438.7, and require that such rates be projected to provide for all reasonable, appropriate, and attainable costs required under the terms of the contract and for the operation of the managed care plan during the specified time period and for the population covered under the terms of the contract.
In risk-based managed care programs, managed care plans have the responsibility to manage the financial risk of the contract, and one of the primary tools plans use is negotiating payment rates with providers. Unless there are specific Federal statutory or regulatory requirements or State contractual restrictions, the provider payment rates and conditions for payment between risk-bearing managed care plans and their network providers are subject to negotiation between the parties and may reflect overall private market conditions, as documented in a
( printed page 30403)
network agreement. As long as managed care plans are meeting the requirements for ensuring access to care and network adequacy, States typically provide managed care plans latitude to develop a network of providers to ensure appropriate access to covered services under the contract for their enrollees and fulfill all of their contractual obligations while managing financial risk.
Subject to certain exceptions, States are generally not permitted to direct the expenditures of a Medicaid managed care plan under the contract between the State and the plan, or to make payments to providers for services covered under the contract between the State and the plan (§§ 438.6 and 438.60, respectively). However, there are circumstances in which a State may believe that requiring managed care plans to make specified payments to health care providers is an important tool in furthering the State's overall Medicaid program goals and objectives. For example, a State may direct managed care plan expenditures to ensure that certain minimum payments are made to safety net providers to ensure access to care, to enhance provider payment as mandated by State legislative directives, or to make quality payments to ensure providers are appropriately rewarded for meeting certain program goals. Because this type of State direction reduces the plan's ability to effectively manage costs, in the 2016 final rule, we established specific exceptions to the general rule prohibiting States from directing the expenditures of managed care plans under § 438.6(c)(1)(i) through (iii). These exceptions came to be known as SDPs.
The current regulations under § 438.6(c) specify the parameters for how and when States may direct the expenditures of their Medicaid managed care plans and the associated requirements and prohibitions on such arrangements. Permissible SDPs include directives that plans pay certain providers who participate in value-based purchasing (VBP) models, in multi-payer or Medicaid-specific delivery system reform or performance improvement initiatives, or that managed care plans adhere to certain fee schedule requirements for provider payment (for example, minimum fee schedules, maximum fee schedules, and uniform dollar or percentage increases). Among other requirements, § 438.6(c) requires SDPs to be based on the utilization and delivery of services under the managed care contract and expected to advance at least one of the goals and objectives in the State's managed care quality strategy.
All SDPs must be included in all applicable managed care contract(s) and described in all applicable rate certification(s) as noted under §§ 438.6(c) and 438.7(b)(6), respectively. Further, § 438.6(c)(2)(i) requires that most SDPs be approved in writing by us prior to implementation.[13]
To obtain our written prior approval, States must submit a “preprint” [14]
to us to document how the SDP complies with the Federal requirements outlined under § 438.6(c). States must obtain written approval of certain SDPs for us to approve the corresponding Medicaid managed care contract(s) and rate certifications(s).
Each SDP preprint submitted to us is reviewed by a Federal review team to ensure the payments comply with the regulatory requirements under § 438.6(c) and other applicable laws. The Federal review team may consist of subject matter experts from various components and groups within CMS, which may include those representing managed care policy and operations, quality, and/or actuarial science. Over time, these reviews have expanded to include subject matter experts on financing of the non-Federal share and demonstration authorities, when needed. The CMS Federal review team works diligently to ensure a timely review and that standard operating procedures are followed for a consistent and thorough review of each preprint. Most preprints are submitted for renewal on an annual basis; SDPs that are for VBP arrangements, delivery system reform, or performance improvement initiatives and that meet additional criteria in § 438.6(c)(3)(i) are eligible for multi-year approval. States also have the option to submit preprint amendments when it is necessary to modify the payment arrangement. We endeavor to complete the review of each SDP preprint submission within 90 days; however, there is no regulatory requirement that we approve or disapprove SDPs within a certain time period.
We issued guidance to States regarding SDPs on multiple occasions. In November 2017, we published the initial preprint along with guidance for States on the use of SDPs.[15]
In May 2020, we published guidance on managed care flexibilities to respond to the COVID-19 public health emergency (PHE), including how States could use SDPs in support of their COVID-19 response efforts.[16]
In January 2021, we published additional guidance for States to clarify existing policy, and also issued a revised preprint that States must use for rating periods beginning on or after July 1, 2021.[17]
The revised preprint [18]
is more comprehensive compared to the initial preprint, and it is designed to systematically collect the information that we identified as necessary as part of our review of SDPs to ensure compliance with the Federal regulatory requirements.[19]
This includes identification of the estimated total dollar amount for the SDP, an analysis of total provider payment rates for the class(es) of providers that the SDP is targeting, and information about the sources of the non-Federal share used to finance the SDP. In September 2025, we issued initial guidance regarding section 71116 of the WFTC legislation [20]
and in the letter, acknowledged that the guidance therein was preliminary in nature and final policies would be implemented through a process of notice-and-comment rulemaking. We also published additional guidance on SDP quality evaluations [21]
in September, which detailed regulatory
requirements and recommended best practices for state design and submission of SDP quality evaluation plans and findings.
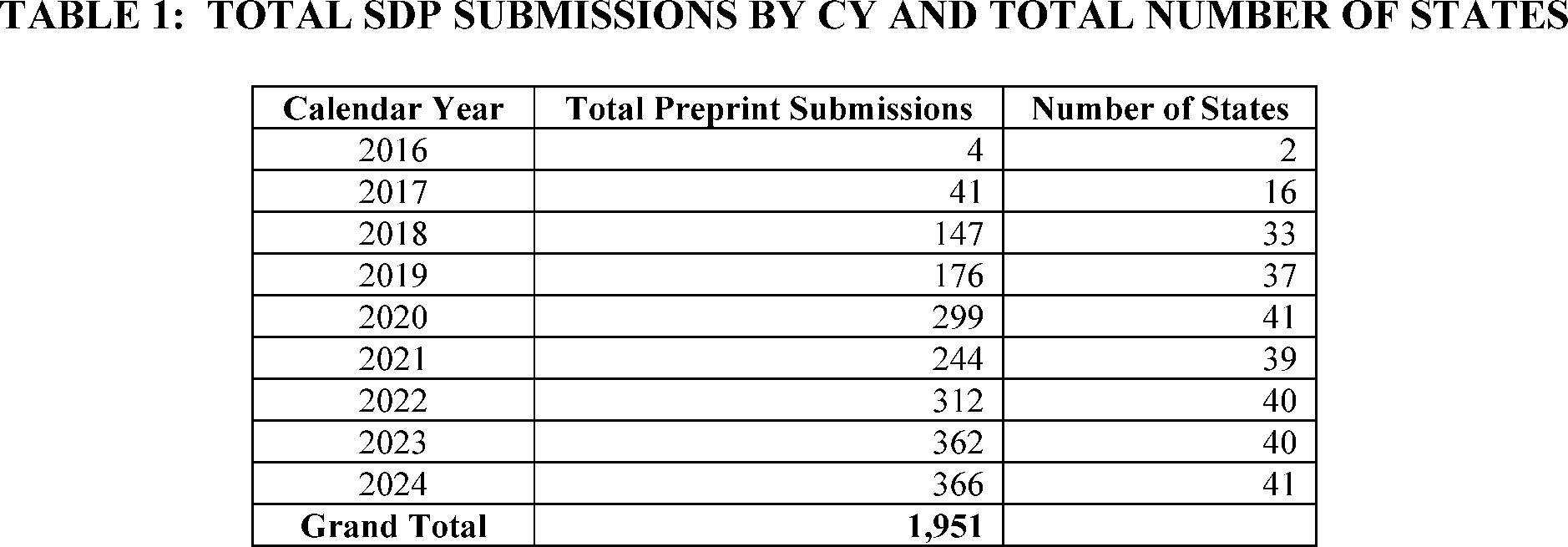
Since § 438.6(c) was finalized in the 2016 final rule, States have requested approval for an increasing number of SDPs. The scope, size, and complexity of the SDP arrangements submitted by States for approval has also grown steadily and quickly as illustrated by Table 1.22
( printed page 30404)
SDPs also represent a notable amount of State and Federal spending. Based on an analysis of all SDP preprints by our Office of the Actuary (OACT), we estimate that absent any changes to existing regulations and before accounting for the impact of the WFTC legislation, SDP spending is projected to be $97.8 billion in fiscal year (FY) 2024 (total computable) and projected to increase to approximately $124.3 billion (total computable) for FY 2025 and $144.6 billion for FY 2026. As total dollars flowing through SDPs have increased significantly even since publication of the 2024 final rule, we have grown increasingly concerned that additional fiscal guardrails are warranted. The proposed changes in this proposed rule are intended to ensure responsible fiscal stewardship of the Medicaid program, as required by section 71116 of the WFTC legislation and consistent with the Presidential Memo.
D. Historical SDP Payment Rate Limits
In the 2016 final rule, § 438.6(c)(2) specified that SDPs must be developed in accordance with § 438.4, and related actuarial standards specified in §§ 438.5, 438.7, and 438.8. Under the definition in § 438.4, actuarially sound capitation rates are “projected to provide for all reasonable, appropriate, and attainable costs that are required under the terms of the contract and for the operation of the MCO, PIHP, or PAHP for the time period and the population covered under the terms of the contract . . .” Consistent with this definition in § 438.4, we noted in the State Medicaid Director Letter (SMDL) #21-001 published on January 8, 2021 that we require States to demonstrate that SDPs result in provider payment rates that are reasonable, appropriate, and attainable as part of the preprint review process.[23]
In applying these standards during early SDP reviews, we encountered situations where the absence of a clear quantitative limit on the total payment rate, such as a requirement that rates be no greater than Medicare rates or no greater than the ACR created uncertainty during the CMS review process. In late 2017, we received an SDP preprint to raise inpatient hospital payment rates such that the total payment rate exceeded 100 percent of the comparable Medicare rates, but the payments would remain below the ACR for that service and provider class in that State. We had concerns about whether the payment rates were still reasonable, appropriate, and attainable for purposes of our approval of the SDP as being consistent with the regulatory requirement at the time that all SDPs must be developed in accordance with § 438.4 and the standards specified in § 438.5. At the time, we realized that approving an SDP that exceeded 100 percent of Medicare payment rates would be precedent setting for CMS.
As we noted in the 2024 final rule, Medicare is a significant payer in the health insurance market, and Medicare reimbursement is a standardized benchmark used in the industry. Medicare reimbursement is also a benchmark used in Medicaid FFS, including the Upper Payment Limits (UPLs) that apply to classes of institutional providers, such as inpatient and outpatient hospitals, nursing facilities, and intermediate care facilities for individuals with intellectual disabilities (ICFs/IID), that are based on a reasonable estimate of the amount that Medicare would pay for Medicaid services. The UPLs apply an aggregate payment ceiling based on an estimate of how much Medicare would have paid in total for the Medicaid services as a mechanism for determining economy and efficiency of payment for State plan services while allowing for facility-specific payments.
Generally, for inpatient and outpatient services, these FFS UPL requirements apply to three classes of facilities based on ownership status: (1) State government-owned or operated; (2) non-State government-owned or operated; and (3) private owned and operated. Hospitals within a class can be paid different amounts and facility-specific total payment rates can vary, sometimes widely, so long as in the aggregate, the total amount that Medicaid FFS paid across the class is no more than what Medicare would have paid to those providers for those services.
When originally considering the Medicaid FFS UPL methodologies, we had concerns that applying the same standards for the total payment rate under SDPs to three classes based on ownership status, would not be appropriate for implementing the SDP requirements. We stated in the 2024 final rule, that § 438.6(c)(2)(ii)(B) provides States with broader flexibility than what is required for FFS UPLs in defining the provider class for which States can implement SDPs. This flexibility has proven important for States to target their efforts to achieve their stated policy goals tied to their managed care quality strategy. For example, we have approved SDPs where States proposed and implemented SDPs that applied to provider classes defined as all providers that are certified to serve as a Patient-Centered Medical Home (PCMH) and therefore, provide increased care coordination compared to providers that are not certified as PCMHs. Not all providers providing a particular service in Medicaid managed care programs must be included in an SDP. Under § 438.6(c)(2)(ii)(B), States are required to direct expenditures
( printed page 30405)
equally, using the same terms of performance, for a class of providers furnishing services under the contract; however, they are not required to direct expenditures equally using the same terms of performance for all providers providing services under the contract. As we noted in the 2024 final rule, we could face challenges applying a similar UPL standard across provider classes under an SDP without some alignment between State defined classes and the FFS UPL framework.
In 2018, we ultimately interpreted § 438.6(c)(2)(i) to allow total payment rates in an SDP up to the ACR and required that States demonstrate, through a total payment rate comparison to the ACR, that total payment rates under the SDP would not exceed the ACR. We formalized this process in the revised preprint published in January 2021 and described it in the accompanying SMDL. Although we have collected this information for each SDP submitted for written prior approval, we historically requested the impact not only of the SDP under review, but any other payments made by the managed care plan (for example, other SDPs or pass-through payments) to any providers included in the provider class specified by the State for the same rating period.
When a State has not demonstrated that the total payment rate for each service and provider class included in each SDP arrangement is at or below either the Medicare or Medicaid FFS rate (when Medicare does not cover the service), we have generally requested documentation from the State to demonstrate that the total payment rate(s) that exceeds the Medicare or the Medicaid FFS rate do not exceed the ACR for the service and provider class. We have worked with States to collect documentation on the total payment rate, which has evolved over time.
With the growth of SDPs, oversight entities released reports focused on SDPs. In a December 2020 report,[24]
the Government Accountability Office (GAO) raised concerns that States' reliance on provider taxes and local government funds used for IGTs effectively shifted responsibility for a larger portion of Medicaid payments to the Federal government and away from States. The Medicaid and CHIP Payment and Access Commission's (MACPAC) June 2022 Report to Congress on Medicaid and CHIP [25]
recommended that CMS improve monitoring, oversight and transparency of SDPs. In December 2023,[26]
GAO echoed similar concerns regarding SDP transparency and weak fiscal guardrails in the absence of codified SDP payment limits. We published the 2024 final rule to address these concerns, among other goals.
The 2024 final rule codified the standard in § 438.6(c)(2)(ii)(I) that each SDP must ensure that the total payment rate for each service, and each provider class included in the SDP must be reasonable, appropriate, and attainable and, upon request from us, the State must provide documentation demonstrating the total payment rate for each service and provider class. We also finalized § 438.6(a) to define “total payment rate” as the aggregate for each managed care program of: (1) the average payment rate paid by all MCOs, PIHPs, or PAHPs to all providers included in the specified provider class for each service identified in the SDP; (2) the effect of the SDP on the average rate paid to providers included in the specified provider class for the same service for which the State is seeking written prior approval; (3) the effect of any and all other SDPs on the average rate paid to providers included in the specified provider class for the same service for which the State is seeking written prior approval; and (4) the effect of any and all allowable pass-through payments, as defined in § 438.6(a), to be paid to any and all providers in the provider class specified in the SDP for which the State is seeking written prior approval on the average rate paid to providers in the specified provider class. Under this definition, although the total payment rate is collected for each SDP, the information provided for each SDP must account for the effects of all payments from the managed care plan (for example, other SDPs or pass-through payments) to any providers included in the provider class specified by the State for the same rating period.
Although this proposed rule does not propose any provisions that pertain to Medicaid Disproportionate Share Hospital (DSH) payments, we nevertheless want to use this opportunity to remind States about the interaction between SDPs and DSH. Under the statutory hospital-specific limits found in section 1923(g) of the Act, a hospital's DSH payments may not exceed the costs incurred by that hospital in furnishing inpatient and outpatient hospital services during the year to certain Medicaid beneficiaries and the uninsured, less payments received under Title XIX of the Act (other than section 1923 of the Act) and payments by uninsured patients. The 2008 Disproportionate Share Hospital Payments final rule (73 FR 77904) stated that Medicaid managed care payments are part of the calculation and reporting requirements for DSH. For purposes of Medicaid DSH, the 2008 final rule, defined “Medicaid MCO payments” as “payments from MCOs to hospitals for inpatient and outpatient services provided to Medicaid managed care enrollees” (73 FR 77920). In the 2016 final rule (81 FR 27498), we established SDPs, which we later characterized as payments made by the State directly to providers or at the direction of the State managed care plan for plan-covered services.[27]
As such, SDPs paid to a hospital for inpatient or outpatient hospital services, when made in accordance with § 438.6(c), are regarded as payments for Medicaid services, and must be offset from costs when a State calculates the hospital-specific DSH limit.
The 2024 final rule also finalized § 438.6(c)(2)(i), which excludes SDPs that set a minimum fee schedule using Medicaid State plan approved rates for a particular service (specified in § 438.6(c)(1)(iii)(A)) from the written prior approval requirement. An SDP that sets a minimum fee schedule at exactly 100 percent of the total published Medicare payment rate that was in effect no more than 3 years prior to the start of the applicable rating period for a particular service (specified in § 438.6(c)(1)(iii)(B)) also does not require written prior approval by us, as specified in § 438.6(c)(2)(i). We believe that both specific payment rates meet the requirement for reasonable, appropriate, and attainable total payment rates because we have reviewed and determined these payment rates to be appropriate under the applicable statute and implementing regulations for Medicare and Medicaid, respectively. However, for other SDP arrangements, we believed at the time of rulemaking that additional analysis and consideration was necessary to ensure that the payment rates directed by the
( printed page 30406)
State meet the standard of reasonable, appropriate, and attainable.
To codify a payment limit for the service types that represented the largest proportion of SDP spending, the 2024 final rule also finalized § 438.6(c)(2)(iii) to establish a limit of 100 percent of the ACR for the total payment rate for each SDP for which written prior approval is required for inpatient hospital services, outpatient hospital service, nursing facility services, and qualified practitioner services at an AMC. In addition to this limit, we established specific standards for the data and documentation requirements necessary to demonstrate compliance with this limit. The 2024 final rule also finalized a definition of the ACR in § 438.6(a) to mean the average rate paid for services by the highest claiming third-party payers for specific services as measured by claims volume. Furthermore, we stated throughout the 2024 final rule that we were establishing a regulatory limit at 100 percent of the ACR for the total payment rate for each SDP for which written prior approval is required for these four service types, and would continue to use the ACR as the fiscal benchmark by which we would evaluate whether all SDP total payment rates are reasonable, appropriate, and attainable as specified in § 438.6(c)(2)(ii)(I) (89 FR 41065).
Beginning with the first rating period beginning on or after July 9, 2024, States were required to demonstrate compliance with these regulatory requirements, for SDPs for one or more of the four services by submitting both a total payment rate comparison using the ACR (that is, Table 2 in the currently published preprint) and an ACR demonstration that meets all of the requirements outlined under § 438.6(c)(2)(iii)(A). We require that the total payment rate comparison specified in § 438.6(c)(2)(iii)(B) be updated with each preprint renewal submission or amendment while the ACR demonstration must be updated at least once every 3 years thereafter, as specified in § 438.6(c)(2)(iii)(C). Operationally, this aligns with our historical practices but the data standards and regulatory definition of the ACR further refine the requirements for the commercial data to be used to demonstrate compliance with the ACR-based payment limit.
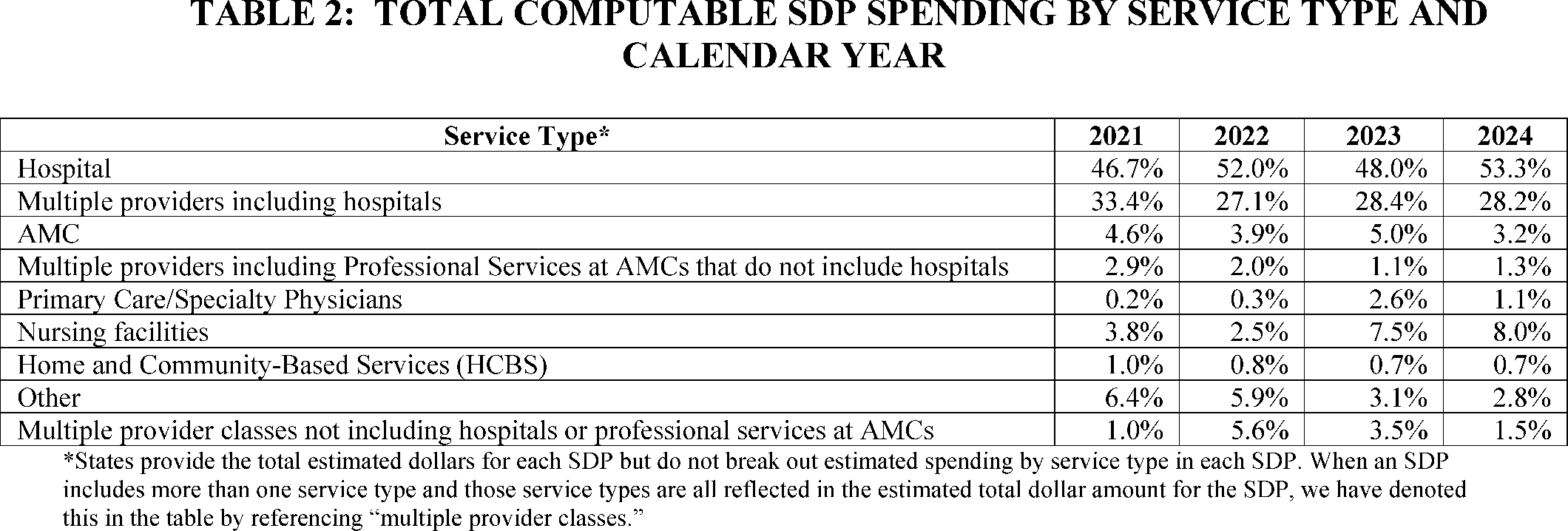
Both the volume of SDP preprints being submitted by States for approval and the total dollars flowing through SDPs have grown quickly since § 438.6(c) was established in the 2016 final rule. The number of States utilizing SDPs has increased from two States in 2016 to 41 States, in 2024. Currently, 83 percent of States with risk-based managed care delivery systems utilize SDPs. In 2024, over 80 percent of SDP preprint submissions were for hospitals, including inpatient and outpatient hospital services. Table 2 illustrates SDP total computable spending (Federal and non-Federal share) by service type from 2021 through 2024.
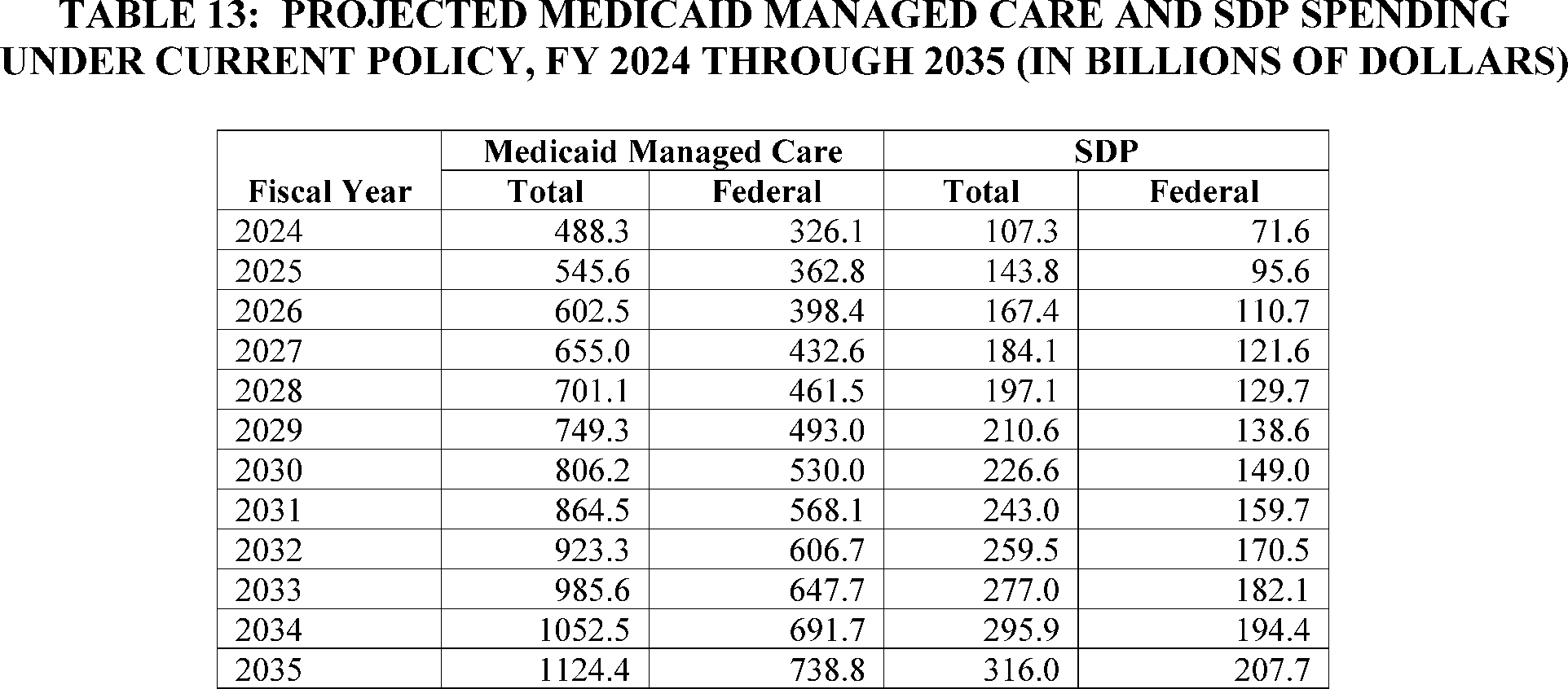
SDPs account for a significant portion of managed care spending; they are estimated to be 26.4 percent of the total Medicaid managed care spending in FY 2025 and 28.1 percent by FY 2034, without any changes to the existing regulations.[28]
The recent estimates for SDP spending developed by OACT project total computable spending to increase from $107.3 billion in FY 2024 to $295.9 billion in FY 2034 under current SDP regulatory requirements.
Through our review process of SDP preprints since publication of the 2024 final rule in May 2024, we have become increasingly concerned with the growth in the percentage of total Medicaid managed care expenditures made through SDPs. The source of the non-Federal share also plays an important role in our concerns regarding SDPs that utilize an ACR payment rate. The significant increase in SDP spending since the 2024 final rule has demonstrated that States are increasingly relying on SDPs as a mechanism for increasing Federal funding for their Medicaid programs, including those where the non-Federal share is funded via IGTs and provider taxes, in other words, by the providers themselves rather than the State. See section II.A. of this proposed rule for discussion on SDPs and the source of the non-Federal share. As SDP spending continues to increase and given the total payment rate limit for certain SDPs mandated in section 71116 of the WFTC legislation, we believe it is appropriate to propose additional regulatory requirements with respect to the totality of provider payment rates under SDPs to ensure proper fiscal and programmatic oversight in Medicaid managed care programs. These proposed changes would also be consistent with the Presidential Memorandum issued on June 6, 2025.
We are issuing this proposed rule, including the requirements that implement section 71116(a) of the WFTC legislation, based on our authority to interpret and implement section 1903(m)(2)(A)(iii) of the Act, which requires contracts between States and MCOs to provide payment under a risk-based contract for services and associated administrative costs that are
( printed page 30407)
actuarially sound, and our authority under section 1902(a)(4) of the Act to establish methods of administration for Medicaid that are necessary for the proper and efficient operation of the State plan. As explained in the 2016 final rule, regulation of SDPs is necessary to ensure that Medicaid managed care plans have sufficient discretion to manage the risk of covering the benefits specified in their contracts, which is integral to ensuring that capitation rates are actuarially sound as defined at § 438.4 (81 FR 27582). We have historically relied on section 1902(a)(4) of the Act to extend PIHPs and PAHPs the same requirements adopted in section 1903(m)(2)(A)(iii) of the Act for MCOs related to actuarially sound capitation rates.
E. Fee-for-Service Supplemental Payments
Section 1902(a)(30)(A) of the Act requires States to “assure that payments are consistent with efficiency, economy, and quality of care and are sufficient to enlist enough providers so that care and services are available under the plan at least to the extent that such care and services are available to the general population in the geographic area.” States are responsible for developing FFS rates to pay providers for furnishing health care services to beneficiaries who receive covered services through the FFS delivery system. In recognition of the States' front-line responsibility, the statute affords States considerable flexibility by not prescribing any particular rate-setting approach or method for most Medicaid services, but instead allows States to develop their own approaches unique to their local circumstances so long as they are consistent with applicable statutory requirements and provide the public and interested parties an opportunity to comment and offer input (84 FR 63723).
Generally, a State that operates its Medicaid program using a FFS delivery system establishes a Medicaid State plan that comprehensively describes the nature and scope of a State's Medicaid program and assures conformity with Title XIX of the Act, to serve as a basis for Federal financial participation (FFP). The Medicaid State plan includes a description of the payments the State will make to enrolled Medicaid providers, which are generally comprised of base and supplemental payments. We have previously discussed base and supplemental payments in SMDL #21-006 [29]
and a proposed rule (84 FR 62722). In that SMDL, we described base payments as State payment methodologies that typically provide for a standard payment to all Medicaid providers on a per claim basis for services rendered to a Medicaid beneficiary in a FFS environment, including any payment adjustments, add-ons, or other additional payments made to a provider that can be attributed to services identifiable as having been provided to an individual beneficiary. Operationally, in a FFS delivery system, base payments are generally predetermined rates that States pay providers for specific services according to their Medicaid fee schedule. We note that per the Ensuring Access to Medicaid Services final rule, these fee schedules must be publicly available by July 1, 2026 (89 FR 40550).
Supplemental payments are defined in section 1903(bb)(2) of the Act generally as payments made to providers that are in addition to the base payment the provider receives. Supplemental payments are generally understood to mean amounts other than the previously described base payment amount, and as such, may include payment for additional costs associated with Medicaid services. Because the term supplemental payments may refer to different types of payments in different contexts, within this proposed rule, we use the term supplemental payments when discussing payments that are in addition to base payments. However, we have not included this term in the specific provisions proposed later in this rule to ensure clarity of our intended scope and impact. We further note that while supplemental payments may seem like the FFS equivalent of managed care SDPs, and can serve similar functions, they should be viewed as separate concepts and discussions in this rulemaking and its proposed policies. We have endeavored to keep these discussions distinct to aid in ensuring a reader can fully understand the proposals for a particular delivery system.
For a number of years, States have been making FFS supplemental payments under the Medicaid State plan that are targeted to certain practitioners, such as physicians, dentists, emergency and non-emergency medical transportation providers (for example, ground emergency medical transportation (GEMT) providers, air emergency transportation providers, and non-emergency medical transportation (NEMT) providers) and other licensed professionals. We generally utilize the term provider when referring to an entity, such as a transportation provider or Certified Community Behavioral Health Clinic (CCBHC) provider, and the term practitioner when referring to an individual, such as a physician. Because our current guidance [30]
for ACR payments uses the term practitioner broadly to include physicians and transportation providers, we have generally maintained that terminology in this rule. However, as discussed later in this proposed rule, some providers, such as transportation providers, are also included in the scope of this rule.
Most commonly for physicians and dentists, States have targeted supplemental payments to practitioners affiliated with and furnishing services in AMCs and safety net hospitals. For transportation providers and other licensed professionals, States often have targeted supplemental payments to State or non-State government owned or operated entities, such as a county fire station, that fund the non-Federal share of the supplemental payment with an IGT. For these payments, States have used what is commonly described as an ACR calculation to establish an upper limit for these practitioner supplemental payments. The ACR is the average rate paid by commercial third-party payers for specific medical service codes (usually current procedural terminology (CPT) codes) to practitioners or providers, which is multiplied in the ACR calculation by the Medicaid claims for each code to establish an upper limit for these supplemental payments. For FFS supplemental payments, States can also calculate the Medicare equivalent of the ACR, discussed in more detail later.
We first approved ACR-based supplemental payments for physician services in the early 2000s. Since then, States have proposed and received our approval for supplemental payments calculated using the ACR for physicians, dentists, providers of medical transportation, and other practitioners under State plan authority. Like all FFS payments made under State plan authority, ACR-based supplemental payments are subject to section 1902(a)(30)(A) of the Act, which requires payments to be consistent with efficiency, economy, and quality of care, and sufficient to enlist enough providers. We interpret section 1902(a)(30)(A) of the Act as requiring a balanced approach to Medicaid rate-setting and we encourage States to use appropriate information and program experience to develop rates to meet all of the statute's requirements. Further, we expect States to document that
( printed page 30408)
Medicaid rates are economic and efficient when the State submits changes to payment methodologies through a SPA. To support States proposing supplemental payments calculated using the ACR, we previously issued sub-regulatory guidance regarding three payment methodologies generally utilized for payments made to physicians and practitioners—(1) payment up to the Medicare Physician Fee Schedule (MPFS) rate; (2) calculation of the ACR; and (3) calculation of the Medicare equivalent of the ACR (calculating the average payment amount allowed by commercial payers as a percentage of Medicare to determine an upper limit).[31]
For States that propose a supplemental payment up to the MPFS rate, the State Plan must comprehensively describe the payment methodology the State uses to calculate the supplemental payment in accordance with § 430.10. This includes, but is not limited to, the percentage (for example, 100 percent) of the MPFS the State will pay, the version (for example, the January 2025 fee schedule) of the MPFS the State will implement, whether the State will apply geographic practice cost indexes (GPCIs) that reflect geographic cost differences as defined by Medicare, and which site of service rate (facility or non-facility) the State will utilize. CMS verifies this information is included in SPAs proposing supplemental payments up to the MPFS rate.
For States that propose a supplemental payment and opt to calculate an ACR or Medicare equivalent of the ACR, States must calculate and submit a UPL demonstration of the proposed supplemental payment for compliance with section 1902(a)(30)(A) of the Act, in addition to comprehensively describing in the State Plan the payment methodology the State uses to calculate the supplemental payment in accordance with § 430.10. For States that calculate an ACR, CMS expects States to recalculate the UPL annually and submit this demonstration to CMS for review. For States that calculate the Medicare equivalent of the ACR, States are expected to recalculate at least every 3 years and submit this demonstration to CMS for review.
When States propose to utilize an ACR methodology (payment up to the ACR or Medicare equivalent of the ACR) to target payments to physicians or other practitioners, States submit data to CMS from each practitioner's top (generally five) commercial payers and provide an explanation of the data that was extracted from the practitioners' accounts receivable systems. The State compares the Medicaid payment for each billing code directly to either: (1) the average payment amount allowed by commercial payers for the same services, or (2) the Medicare equivalent of the commercial payers' average payment amount for the same services. The submitted ACR calculation includes data from each of the practitioners, group practices, or hospital-based practitioner groups eligible to receive the supplemental payment.
We issued SMDL #13-003 on March 18, 2013 to reaffirm mutual obligations and accountability on the part of the State and Federal governments for the integrity of the Medicaid program and the development, application, and improvement of program safeguards necessary to ensure proper and appropriate use of both Federal and State dollars.[32]
In SMDL #13-003, we stated our expectation that States submit annual UPL demonstrations for targeted physician [33]
supplemental payments beginning in 2014. Beginning in 2019, and modified in 2022, States began submitting UPL demonstrations using the OMB-approved templates for Qualified Practitioner Services. In 2021, we issued guidance for Medicaid Qualified Practitioner Services to support States in developing their UPL demonstrations for demonstrating compliance with section 1902(a)(30)(A) of the Act.[34]
We revised this guidance to align with the most current UPL template for Qualified Practitioner Services in 2022.[35]
Apart from this information provided in guidance, our regulations have been silent regarding payment limits for these types of providers.
In 2019, we issued a proposed rule with many financial provisions, one of which proposed to limit these types of supplemental payments (84 FR 63722),[36]
which would have implemented a UPL regulation like those that already existed for other payments. We proposed this change based on concerns that States were making practitioner payments that were not economic and efficient, consistent with section 1902(a)(30)(A) of the Act, and that they presented an oversight risk because they were based on proprietary commercial payment data and thus not readily verifiable or auditable. The 2019 proposed rule was much broader in scope in terms of the number of financial and payment topics than this proposed rule. While the entirety of the 2019 proposed rule was subsequently withdrawn in January 2021, we indicated at the time that the withdrawal action did not limit our prerogative to make new regulatory proposals in the areas addressed by the withdrawn proposed rule, including new proposals that may be substantially identical or similar to those described therein (86 FR 5105).
The Consolidated Appropriations Act, 2021 (CAA) was enacted on December 27, 2020.[37]
It established a number of new requirements for State Medicaid programs, including the addition of section 1903(bb) of the Act to specify new reporting requirements for supplemental payments. We issued guidance in SMDL #21-006, “New Supplemental Payment Reporting and Medicaid Disproportionate Share Hospital Requirements under the Consolidated Appropriations Act, 2021,” [38]
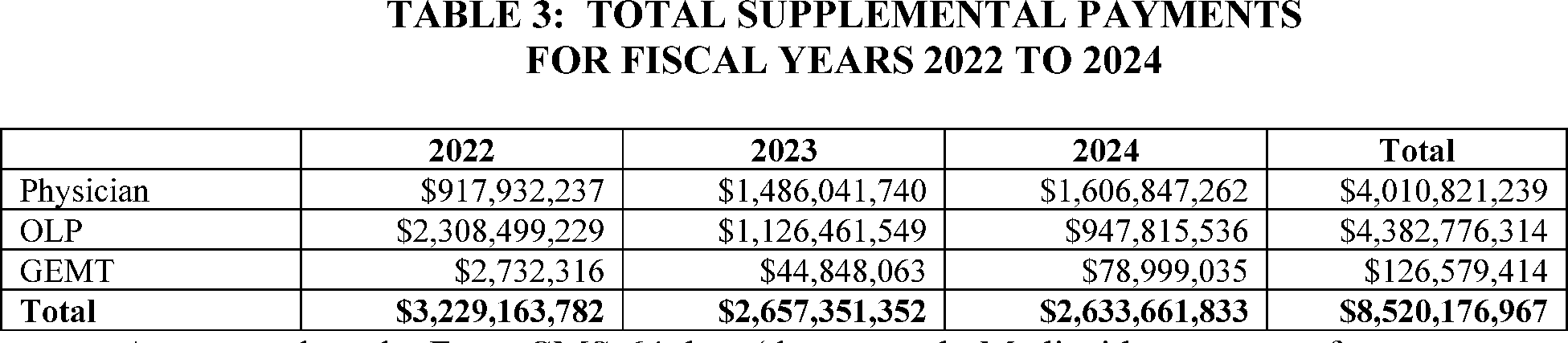
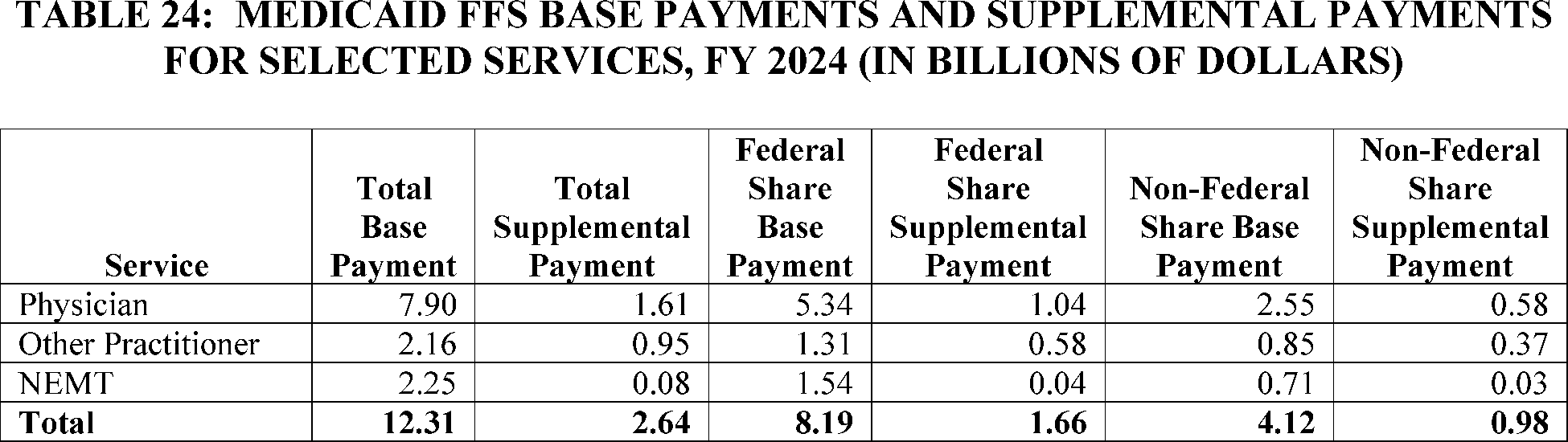
to address the new requirements, and since 2022, we have received more detailed supplemental payment data from States reported in the CMS-64. Table 3 shows the total reported supplemental payments since this requirement was implemented for physicians, other licensed practitioners (OLP), and GEMT.
( printed page 30409)
As reported on the Form CMS-64 data (the quarterly Medicaid statement of expenditures), States claimed approximately $2.63 billion (total computable) in expenditures for supplemental payments (including ACR-based payments but excluding DSH and any Medicare UPL payments) made to physicians, other licensed practitioners, and ground emergency medical transportation providers for FFY 2024. Over 60 percent of total supplemental payments ($1.6 billion total computable) were made to just 1,975 physicians or physician practices across 24 States that make supplemental payments to physicians. Currently approved ACR-based supplemental payments in States using the Medicare equivalent of the ACR average 207 percent of the Medicare rate for physicians and 153 percent for other licensed practitioners (for example, dentists and GEMT providers). While an outlier, one State currently pays ACR-based supplemental payments at 530 percent of Medicare equivalent of the ACR for physicians. Based on our analysis of State expenditure data, as further discussed in section II.B of this proposed rule, these targeted payments present clear oversight risks to Federal taxpayer dollars for which CMS is a financial steward. We recognize this is an opportune time to consider changes to our policies to address a similar problem across both delivery systems, FFS and managed care, in light of the changes made to SDPs by section 71116 of the WFTC legislation.
II. Provisions of the Proposed Regulations
We intend that if any provision in this proposed rule, if finalized, is held to be invalid or unenforceable by its terms, or as applied to any person or circumstance, or stayed pending further agency action, it shall be severable from the final rule (if and once finalized) and not affect the remainder thereof or the application of the provision to other persons not similarly situated or to other, dissimilar circumstances. This notice proposes provisions that are meant to and would operate independently of each other, even if each serves the same general purpose or policy goal. Where a provision is necessarily dependent on another, the context generally makes that clear (such as by a cross-reference to apply the same standards or requirements).
A. State Directed Payments in Medicaid Managed Care (§ 438.6)
Since publication of the 2024 final rule, we have received over 400 SDP preprint submissions from 41 States. Some of these submissions represent brand new SDPs or renewals of existing SDPs for which the total dollar amount attributable to the SDP has increased significantly. Many of these proposed SDPs bring provider payment rates up to 100 percent of the ACR or, in some cases, in excess of 100 percent.[39]
Recent State SDP submissions include:
A new $3.2 billion SDP for all inpatient and outpatient hospital services within the State that directs managed care plans to make an 186 percent uniform increase payment to bring average provider payments up to 100 percent of the ACR.
A $13 billion renewal SDP for inpatient and outpatient hospital services provided at all private hospitals in the State that would require managed care plans to make uniform dollar increase payments up to $5,146 per hospital service. This is the highest dollar amount SDP CMS has received to date and represents an 80 percent increase in the total SDP dollar amount requested compared to the prior rating period.
A new $1.3 billion SDP for physician services that would require managed care plans to make uniform percentage increases of up to 634 percent per physician service to bring average payments up to 142 percent of the ACR.
One State submitted 16 new SDPs for hospital services and qualified practitioner services at AMCs, each limited to a single hospital, totaling nearly $1.5 billion across the 16 SDPs. Each SDP would require different uniform increases that would bring each hospital up to between 27 percent and 100 percent of the ACR. Based on information submitted in the preprints, the SDPs appear to be designed to reward providers that finance the non-Federal share, rather than to meet the goals and objectives of the State's Medicaid program, including improving access to care, and enhancing quality of care in Medicaid managed care.
The 2024 final rule included projections that under the new regulatory requirements, including the ACR limit for certain services, SDP spending would increase to $74.9 billion in FY 2024 and up to $115.1 billion in FY 2028. However, more recent estimates developed by OACT based on SDP submissions approved through December 2024, project SDP spending to increase to $97.8 billion in FY 2024 and $246 billion in FY 2034 under current SDP regulatory requirements. These updated estimates indicate a substantial increase from the projections in the 2024 final rule and underscore the need to consider additional fiscal integrity protections to promote the long-term sustainability of the Medicaid program. The source of the non-Federal share also plays an important role in our concerns regarding SDPs that utilize an ACR payment rate. The significant increase in SDP spending since the 2024 final rule suggests that States are increasingly relying on SDPs as a mechanism for increasing Federal funding for their Medicaid programs, including those funded via IGTs and provider taxes without commensurate State general fund contributions toward the non-Federal share.
SDPs that result in total provider payment rates up to the ACR are most frequently funded by provider taxes and IGTs from local government sources or State university teaching hospitals and generally include only providers that have the ability to fund the non-Federal share of the ACR payments. It appears that, in some instances, these types of SDPs are often primarily developed
( printed page 30410)
based on the amount of available funding from providers rather than to drive improvements in access to or quality of care for beneficiaries or to achieve other, similar programmatic goals. For SDPs that were projected to exceed 100 percent of Medicare up to 100 percent of the ACR, States financed the underlying non-Federal share as follows: 39.8 percent were funded in part or wholly by IGTs (but not provider taxes), 26.9 percent were funded in part or wholly with provider taxes (but not IGTs), and 14.2 percent were funded in part or wholly by both IGTs and provider taxes. In total, 80.8 percent of SDPs that exceeded Medicare payment rates, including those up to the ACR, were funded in part or wholly via IGTs and/or provider taxes.[40]
When these IGTs or provider taxes are used, the State Medicaid agency does not contribute general funds for the non-Federal share of the associated payments because the funding comes from separate governmental entities (in the case of IGTs) or providers.
States have multiple methods to generate the non-Federal share (also known as the State share) to finance their Medicaid programs, including IGTs and health care-related taxes. These sources, while generally permissible, present the need for greater scrutiny, because the State is oftentimes collecting money to fund the non-Federal share for SDPs from the same entities that then receive those payments, resulting in higher provider payment rates than they would have received if they had not contributed funding via IGTs or provider taxes. We have taken recent steps to address impermissible arrangements related to financing sources but recognize the importance of examining the nature of the payments the State makes under these structures. SDPs and supplemental payments that reflect these financing patterns can result in payment levels that are not clearly aligned with Medicaid utilization, quality, health outcomes, or other program goals. These payments in turn drive significant Medicaid spending increases without a clear connection to quality or outcomes for Medicaid beneficiaries. Further, when the funds to support the non-Federal share of increased payments originate from the same providers that receive enhanced payments, the resulting spending increases raise fiscal integrity concerns for the Medicaid program and increase the burden on the Federal treasury and taxpayers.
In the 2023 proposed rule, we considered a total payment rate limit at 100 percent of the total published Medicare payment rate instead of the ACR, noting that Medicare payment rates are a standardized benchmark used in the healthcare industry (88 FR 28124). Compared to proprietary commercial data, Medicare payment rate data may be more easily verified and audited because Medicare payment rates are published yearly and available to the public. We also acknowledged that setting the limit at Medicare would serve to limit the growth in Medicaid managed care spending relative to an ACR limit. Many of the public comments received on the 2023 proposed rule supported an SDP payment limit at the total published Medicare payment rate, citing payment transparency, payment comparability among the largest public payers in the nation, and concerns that a limit at the ACR could accelerate Federal Medicaid spending. We also received comments supportive of an SDP total payment limit at the ACR for four services. These commenters noted concerns with finalizing a limit lower than the ACR, asserting that would reduce the ability of managed care plans to compete with commercial plans for providers to participate in their networks and could result in a reduction of access, particularly for States that already have SDPs at ACR (89 FR 41066). In the 2024 final rule, we finalized the limit on the total payment rate at no greater than 100 percent of the ACR and reminded States that they are not required to utilize SDPs and that there are separate regulatory requirements that require States that contract with a managed care plan to deliver Medicaid services to address network adequacy and access to care, regardless of the use of SDPs (89 FR 41066).
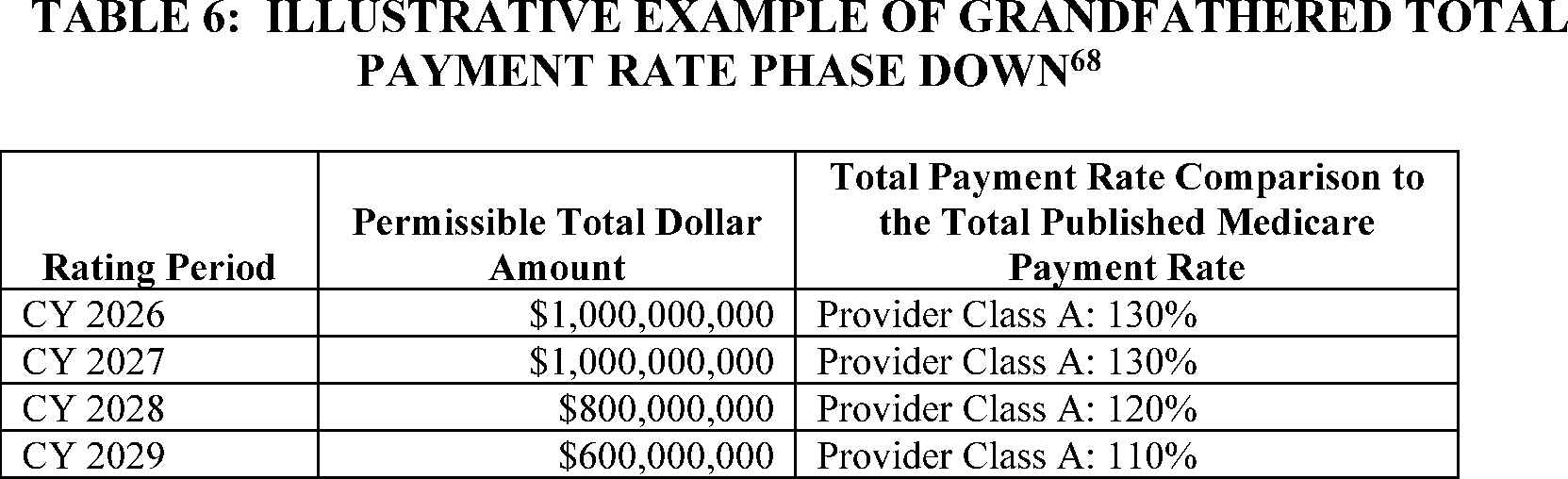
On July 4, 2025, President Trump signed the WFTC legislation into law. Section 71116 of the WFTC legislation directed the Secretary to reduce the total payment rate limit for certain SDPs for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at an AMC. Section 71116 of the WFTC legislation also included a provision allowing a temporary grandfathering period for certain SDPs until the rating period beginning on or after January 1, 2028, at which point such SDPs would be required to gradually transition down to the new payment limit. Our proposals in this rule seek to implement these provisions and, if finalized, could slow the growth of SDP spending in the future.
1. Payment Limit for SDPs (§ 438.6 (a), 438.6(c)(2)(ii)(I) and 438.6(c)(8))
The WFTC legislation and the Presidential Memorandum reflect what our experience reviewing SDPs since the 2024 final rule has demonstrated: the total published Medicare payment rate or the Medicaid State Plan rate are reasonable payment limits for SDPs compared to the ACR. The WFTC legislation and the Presidential Memorandum are consistent with concerns we have identified through our experience reviewing SDPs since the 2024 final rule, including that an SDP total payment rate limit of 100 percent of the ACR can contribute to substantial growth in SDP expenditures. The current payment limit framework may also contribute to financing arrangements that raise fiscal integrity concerns and reduce incentives for shared State funding responsibility. Using Medicare or Medicaid State plan rates as the payment limit for SDPs would bring consistency and predictability and could help moderate the growth of SDP expenditures while providing States flexibility to pursue provider payment initiatives and delivery system reform efforts that further advance access to care and enhance quality of care in Medicaid managed care.
Medicare payment rates are developed under Title XVIII of the Act and there are annual rulemakings associated with Medicare payment for benefits available under Medicare Parts A and B in the Medicare FFS program. Medicare payment rates are consistently and rigorously developed and vetted by us and are subject to public notice and comment periods. In our experience, many managed care plans use Medicare FFS rates as a benchmark as part of their provider payment negotiations. They are the only complete and reliable set of provider payment rates published annually and are freely and easily accessible to CMS, providers, States, managed care plans, interested oversight bodies, and the general public. Additionally, published Medicare payment rates are often utilized in the Medicare managed care delivery system. For example, section 1852(a)(2) of the Act provides that Medicare
( printed page 30411)
Advantage [41]
plans pay out-of-network providers at least the amount payable under Medicare FFS for benefits available under Medicare Parts A and B, taking into account cost sharing and permitted balance billing.
There is precedent for Medicaid alignment with Medicare payment rates. Medicaid FFS delivery systems currently use Medicare payment rates for the majority of regulatory UPLs (for further discussion of the existing UPLs that use Medicare in FFS programs, see section II.B.1 of this proposed rule). In the 2024 final rule under § 438.6(c)(2)(i), we removed the requirement for our written prior approval for SDPs that use a minimum fee schedule at 100 percent of the total published Medicare payment rate in effect no more than 3 years prior to the start of the rating period. We did this to acknowledge that total published Medicare payment rates met our regulatory standard requiring all SDPs to result in provider payments that are reasonable, appropriate, and attainable. We believe that the total published Medicare payment rate or State plan approved rate represent a reasonable payment limit for Medicaid services when a State is directing payment via a SDP.
The proposed limits to Medicaid managed care expenditures in this proposed rule would only apply when providers receive payments through SDPs (that is, when States opt to direct Medicaid managed care expenditures as permitted under § 438.6(c)). Absent SDPs, Medicaid managed care plans may continue to negotiate provider payment rates that exceed this payment limit when necessary to ensure a sufficient provider network. We remind States that under § 438.6(c)(1), States are not permitted to direct managed care plan expenditures in any way, outside of the permissible regulatory options outlined in § 438.6(b) through (d) or as specified in statute; we are not proposing any revisions to this provision. To curtail the growth in Medicaid managed care spending as a result of SDPs, implement the mandate in the WFTC legislation, protect the fiscal integrity and future of the Medicaid program, and promote transparency, we propose revisions to § 438.6(a) and (c) as outlined in the next paragraph.
a.
Regulatory Revisions Required by WFTC Legislation
Section 71116(a) of the WFTC legislation requires the Secretary to revise § 438.6(c)(2)(iii) to enact a new total payment rate limit with respect to a payment described in that section for all 50 States and DC, although it does not apply to the U.S. territories. Sections 71116(b) and (c) of the WFTC legislation establish transition and applicability rules for certain payments and States. This would establish a new regulatory limit for SDPs that require written prior approval and include any of the four services specified in § 438.6(c)(2)(iii).[42]
Section 71116(a) of the WFTC legislation also specifies that this new payment limit is to be applicable to services furnished during a rating period [43]
beginning on or after the date of enactment of the WFTC legislation (July 4, 2025), unless the SDP is eligible for a temporary grandfathering period (see section II.A.2. of this proposed rule). The total payment rate limit specified in section 71116(a) of the WFTC legislation for SDPs that include any of the four services is 100 percent of the total published Medicare payment rate for an expansion State, or 110 percent of the total published Medicare payment rate for a non-expansion State with respect to a payment made for a service furnished during an applicable rating period. In the absence of a total published Medicare payment rate for the Medicaid covered service, section 71116(a) of the WFTC legislation specifies that the total payment rate is limited to the payment rate under the Medicaid State plan (or under a waiver of such plan). We propose to codify these provisions in § 438.6(a) and (c).
b. Regulatory Revisions for Other SDPs, Services and Territories
Section 1903(m)(2)(A) of the Act requires contracts between States and MCOs to provide payment under a risk-based contract for services and associated administrative costs that are actuarially sound. Under risk-based managed care arrangements with States, Medicaid managed care plans have the responsibility to negotiate payment rates with providers. Subject to certain exceptions, States are not permitted to direct the expenditures of a Medicaid managed care plan under the contract between the State and the plan or to make direct payments to providers for services covered under the contract between the State and the plan (§§ 438.6 and 438.60, respectively). However, there are circumstances under which requiring managed care plans to make specified payments to health care providers is an important tool in furthering the State's overall Medicaid program goals and objectives. While this type of State direction reduces the plan's ability to effectively manage costs, it can be an important tool for States. In the 2016 final rule, we established specific exceptions to the general rule prohibiting States from directing the expenditures of MCOs, PIHPs and PAHPs in § 438.6(c)(1)(i) through (iii). These exceptions came to be known as State directed payments (SDPs). When SDPs are utilized, States are required to ensure that the capitation rates, inclusive of SDPs, under the risk-based contract for services covered under that contract and the associated administrative costs are actuarially sound. We use our authority under section 1902(a)(4) of the Act to apply the same requirements to contracts between States and PIHPs or PAHPs. Under our authority to interpret and implement sections 1902(a)(4) and 1903(m)(2)(A)(iii) of the Act we propose to extend these provisions and the payment limit to all SDPs and in all States, DC and the U.S. Territories. Our proposals are explained in greater detail further in this section.
a. Definitions
First, we address the existing definition of “total published Medicare payment rate” in § 438.6(a) which section 71116(d)(4) of the WFTC legislation adopts by reference. While the phrase “specified total published Medicare payment rate” is used in section 71116(a) of the WFTC legislation, we believe this phrase aligns with the existing definition of the total published Medicare payment rate to mean amounts calculated as payment for specific services that have been developed under title XVIII Part A and Part B of the Act. Since the regulatory definition already includes the word “specific” and we have always interpreted it to mean the exact total published Medicare payment rate for a specific service furnished to a Medicaid managed care enrollee, we do not believe it is necessary to revise our existing definition of “total published Medicare payment rate.” We therefore interpret the existing definition to apply wherever section 71116 of the WFTC legislation uses the phrase “specified total published Medicare payment rate.”
( printed page 30412)
In the absence of a total published Medicare payment rate for a Medicaid covered service, section 71116(a)(1) and (2) of the WFTC legislation specifies that the payment rate for each of the four service types is limited to the “payment rate under the Medicaid State plan (or under a waiver of such plan).” We believe that our existing definition of “State plan approved rates” under § 438.6(a) is aligned definitionally with “payment rate under the Medicaid State plan.” We have always interpreted the definition of State plan rates to include rates that are approved via a waiver of the State plan, such as through a waiver under section 1915(c) of the Act (see, for example, 81 FR 27537). As specified in § 438.6(a), State plan approved rates do not include supplemental payments, which are defined under § 438.6(a) as amounts paid in addition to State plan approved rates. We are proposing to revise the definition of “State plan approved rates” at § 438.6(a) to strike the phrase “CMS approved” and amend the latter part of the sentence to read “described under rate methodologies in the Medicaid State plan approved by CMS before the start of the rating period.” We believe this revision is necessary to address timing misalignment between the SPA approval process and the prospective nature of risk-based managed care. States are permitted to submit SPAs at any time during a State fiscal quarter which can then be approved by us for an effective date retroactive to the start of the quarter. The SPA review process is also lengthy and sometimes takes years to reach a conclusion. In an FFS delivery system, the State may choose to make payments under a submitted SPA prior to approval,[44]
or, once the SPA is approved retroactive to the start of the State fiscal quarter in which it was submitted the State may make retroactive payments to FFS providers to account for the payment differential for services rendered when the SPA was retroactively in effect.
In a managed care environment if a State directs their plans to pay providers a minimum fee schedule SDP using State plan approved rates, the State's actuaries will develop the capitation rates based on the State plan approved rates in effect for the applicable rating period, consistent with the actuarial soundness and prospective rate development requirements in §§ 438.4 and 438.7. If a SPA is not approved until the managed care rating period is underway or completed and the State wishes to direct plans to implement those updated payment rates via an SDP retroactive to the effective date of the approved SPA, they must submit both contract amendments and rate certifications to effectuate those changes. We have observed that these types of retroactive revisions to SDPs can create inconsistencies between certified capitation rates and actual plan payment obligations, lead to inaccurate implementation, cause uncertainty for providers, and hamper post payment validation efforts. We believe that requiring States to use the State plan rates approved before the start of the rating period would be consistent with prospective rate-setting processes and would add stability and predictability to SDPs. This change does not alter SPA approval authority under title XIX of the Act, but instead specifies how approved State plan rates may be implemented as a minimum fee schedule SDP and used for prospective capitation rate development in managed care.
For SDPs that require written prior approval and include any of the four service types specified in section 71116(a) of the WFTC legislation in the 50 States and DC, the WFTC legislation requires different SDP payment limits depending on whether the State has implemented Medicaid expansion, specified in section 71116(a)(1) of the WFTC legislation as a State that provides coverage to all individuals described in section 1902(a)(10)(A)(i)(VIII) of the Act (42 U.S.C. 1396a(a)(10)(A)(i)(VIII)) that is equivalent to minimum essential coverage (as described in section 5000A(f)(1)(A) of the Internal Revenue Code of 1986 and determined in accordance with standards prescribed by the Secretary in regulations) under the State plan (or waiver of such plan) of such State under title XIX of such Act. In section 71116(a)(1) of the WFTC legislation, the total payment rate limit is 100 percent of the total published Medicare payment rate for States that meet this definition of “Expansion State.” Section 71116(a)(2) of the WFTC legislation cross-references section 71116(a)(1) to specify that in the case of a State other than a State described in section 71116(a)(1) of the WFTC legislation, the total payment rate limit is 110 percent of the total published Medicare payment rate. We propose to add the term “Expansion State” to § 438.6(a) and propose a streamlined version of the definition in section 71116(a)(1) of the WFTC legislation to mean a State that provides medical assistance to all individuals described in section 1902(a)(10)(A)(i)(VIII) of the Act under a State plan under title XIX of such Act or under a waiver of such plan that provides minimum essential coverage as defined in section 5000A(f)(1)(A) of the Internal Revenue Code of 1986. We propose to also add the term “Non-Expansion State” that would mean a State that does not meet the definition of “Expansion State.”
Section 71116(d)(3) of the WFTC legislation defines “State” to mean 1 of the 50 States or DC We have historically not differentiated between the 50 States, DC, or U.S. territories with regards to the regulatory requirements for SDPs. The Presidential Memorandum also did not differentiate or distinguish between States, DC, or U.S. territories. We believe it is prudent and necessary for the fiscal integrity of the Medicaid program that we apply the payment limit to all States, DC, and the territories, as we have historically done. Therefore, we propose to add the term “State” to § 438.6(a) to mean, as used in § 438.6(c)(8)(ii) only and only until the first rating period beginning on or after January 1, 2029, the Single State agency of one of the 50 States or DC We also propose that the definition of “State” would, at other times and for other purposes in this section, unless otherwise specified, have the meaning given the term in § 438.2 of this part. This would have the effect of imposing the payment limit on SDPs for the U.S. territories with the first rating period on or after January 1, 2029, while retaining the applicability of all other SDP requirements to a
State
as defined in § 438.2, including the U.S. territories, before that date. See section II.A.1.B. of this proposed rule for discussion of proposed payment limits and applicability dates.
To streamline the regulatory text under § 438.6 and reduce redundancies, we propose to add the term “Payment limit” to § 438.6(a) as 100 percent of the total published Medicare payment rate for an Expansion State, 110 percent of the total published Medicare payment rate for a Non-Expansion State, and 100 percent of the State plan approved rate when there is no total published Medicare payment rate for the covered service. This definition would align with the SDP payment limits delineated in section 71116(a) of the WFTC legislation. We propose that the Medicare payment limit would differ for Expansion and Non-Expansion States as is required under section 71116(a) of the WFTC legislation for the 50 States and DC for SDPs that include any of the four services and require written prior approval. Section 71116(a)(1) and (2) of the WFTC legislation also provides that, in the absence of specified total published Medicare payment rate, the
( printed page 30413)
applicable payment rate is the payment rate under a Medicaid State plan (or under a waiver of such plan). Because the statute refers to “the payment rate under a Medicaid State plan” and does not modify that phrase to specify an applicable percentage for either an Expansion State or a Non-Expansion State, we interpret section 71116(a)(1) and (2) of the WFTC legislation to require that the exact rate(s) approved under the Medicaid State plan serve as the payment limit in the absence of a total published Medicare payment rate for a covered service, regardless of whether the State is an Expansion State or a Non-Expansion State.[45]
We believe this approach is appropriate and reasonable because State plan approved rates are reviewed and approved through the State plan amendment process, which includes State-specific review of each submission, as discussed further in this section of the rule.
Proposed FFS Medicare payment rates under Medicare Parts A and B are typically published via an annual notice of proposed rulemaking in late spring and summer, are subject to an open comment period, and then published in a final rule in fall or winter of each year. The effective date of the total published Medicare payment rates varies by fee schedule but is typically tied to either the calendar year (CY) or Federal fiscal year (FFY). Table 4 outlines selected Medicare FFS payment systems through which these payment rates are established, and the periodicity of rule publication. The table is not inclusive of all total published Medicare payment rates.
While
States may choose to implement SDPs, including those that do not require prior approval, in alignment with the most recently released total published Medicare payment rate(s), during the period those rates are in effect, States are reminded that they are required to comply with existing requirements for SDP submission and contract documentation. Beginning with rating periods starting on or after July 9, 2026, States are required to comply with § 438.6(c)(2)(viii) and submit all SDP preprints prospectively; that is, before the start date of the applicable SDP arrangement. This provision is intended to facilitate more timely and accurate implementation of SDPs by managed care plans by ensuring that they have ample notice of each SDP they are being directed to implement. We noted in the 2024 final rule that requiring States to submit preprints in advance of the start date of the arrangement (89 FR 41054) and document them in plan contracts within 120 days of the SDP start date [47]
would ensure efficient administration of contract and rate certification reviews (89 FR 41101 through 41102). This approach is also better aligned with the prospective nature of risk-based managed care. In addition, under § 438.7(c)(6), States are required to submit the rate certification or retroactive adjustment to capitation rates resulting from an SDP no later than 120 days after the start date of the SDP.[48]
States are required to meet all of these requirements when implementing any SDP, including when they seek to align an SDP, the associated contracts and certified capitation rates with updates to the total published Medicare payment rates that also serve as the basis of the applicable payment limit. This is especially important for periodic updates to Medicare fee schedules that are misaligned with States' rating periods for Medicaid managed care programs.
We specifically propose to apply the payment limit to each service included under an SDP as section 71116(a) of the WFTC legislation references “the payment rate for such service” when addressing the applicability of the payment limit. We also believe that this interpretation is aligned with the Presidential Memorandum which directs the Secretary to ensure “Medicaid payments rates are not higher than Medicare . . .” We interpret the term “payment rate(s)” in both the WFTC legislation and the Presidential Memorandum to mean the specific payment rate for a service furnished by a provider. Under our proposed definition of “Payment limit” in § 438.6(a), the total published Medicare payment rate would therefore serve as the basis of the payment limit for each service rendered to a Medicaid managed care enrollee when that service is included in an SDP. The SDP payment limit would not be calculated at an aggregate level, using a UPL-like approach that mirrors what is done to implement many existing payment limits in Medicaid FFS. Rather, the payment limit would be calculated at a service or discharge specific level, whether it be at the HCPCS code level or for Medicare Severity Diagnosis-Related Groups (MS-DRGs) as is used for Medicare IPPS. Neither section 71116 of the WFTC legislation nor the Presidential Memorandum references aggregate Medicare-equivalent payments or a UPL methodology. Therefore, we propose to implement the limit on a per service or per discharge basis.
We acknowledge that the “total published Medicare payment rate” as defined in § 438.6(a), may include applicable Medicare payment adjustments, including but not limited to geographic and quality adjustments. As discussed in the 2024 final rule (89 FR 41049), the total published Medicare payment rate is inclusive of all components included in the rate
( printed page 30414)
developed by CMS for Medicare payment. In addition to the Medicare payment final rules, we also publish web pricers or fee schedules [49]
for all total published Medicare payment rates and offer free, executable code for those web pricers.[50]
We would expect States to use these Medicare tools, which are validated and inclusive of all the necessary Medicare components and adjustments that comprise the total published Medicare payment rate, when determining the applicable payment limit for payments to providers under an SDP.
While the vast majority of Medicare services are paid based on prospectively published payment rates, several hospital types are exempt from prospective payment systems, some providers are instead paid using a cost-based payment methodology.[51]
Medicare providers that are reimbursed by Medicare on a cost-basis include critical access hospitals (CAHs), certain cancer hospitals, and freestanding children's hospitals. Hospital payment rates determined using a cost-based methodology are not published nor are they subject to review and public comment. Hospitals reimbursed by Medicare on a cost basis are required to submit cost reports to CMS using Medicare approved cost reporting principles during the cost reporting period.[52]
Medicare contractors validate these cost reports and the providers are generally paid for the proportion of allowable costs attributed to Medicare FFS beneficiaries.[53]
Typically, these providers receive interim payments based on estimated costs that are then reconciled to actual costs after the end of the cost reporting period.[54]
This retrospective approach for annual cost reports poses operational and policy concerns for determining compliance with the applicable payment limit for SDPs under section 71116 of the WFTC legislation. In a Medicaid managed care delivery system, actuarially sound capitation rates are determined prospectively, and beginning with rating periods starting on or after July 9, 2026, States must submit SDP preprints to CMS prospectively under § 438.6(c)(2)(viii). The prospective nature of risk-based managed care makes it difficult to impose and monitor a per service SDP payment limit when the SDP payment limit for a provider is tied to a retrospective cost report.
For providers paid under a cost-based methodology in Medicare, we believe it would be appropriate to consider the cost-based payment approach for applicable providers as the total published Medicare payment rate for the purpose of the SDP payment limit. However, we would need to publish specific instructions on allowable cost-reporting and cost allocation methodologies specific to Medicaid managed care. We could modify existing cost reporting instructions in Medicaid FFS that are based on Medicare cost reporting principles, for example disproportionate share hospital (DSH) cost reporting,[55]
for this purpose and as part of our proposal under § 438.6(c)(9) to publish guidance as needed. Due to the prospective nature of risk based managed care, we propose to use the most recent and complete Medicare cost report, which would be submitted to us to validate, for the purpose of establishing the prospective SDP payment limit on a per service or discharge basis, including through appropriate cost allocation methodologies to derive service-level payment amounts. We believe this approach would ease administrative burden while still allowing States and these providers the flexibility to mirror the applicable Medicare payment approach.
In a scenario where a provider submitted a cost report for a cost reporting period ending in 2027, we would expect that report be submitted to us in alignment with the submission timing requirements at § 413.24(f)(2)(i) and, when applicable, as part of proposed § 438.6(c)(8)(ii)(C) and (iii)(C), which would require States to submit any additional documentation requested by CMS to demonstrate compliance with the payment limit. This cost report would serve as the basis for the total published Medicare payment rate and therefore, the applicable payment limit for a State with an SDP for a rating period starting on July 1, 2028. We propose that the provider specific cost report would be submitted to CMS, when applicable, to fulfill the proposed regulatory requirements under § 438.6(c)(8)(ii)(A) and (iii)(A) that the State submit “the total published Medicare payment rate or State plan approved rate (when no total published Medicare payment rate exists for the covered service) that serves as the basis of the payment limit for each service covered under the State directed payment.” We believe this proposal is only appropriate in limited cases in which a provider covered under an SDP is not paid by Medicare and therefore does not utilize the Medicare PPS, fee schedule or cost report, and there is no total published Medicare payment rate. In this limited case only, we propose that the payment limit for the applicable SDP would be the applicable State plan approved rate.
As an alternative, we considered whether to revise the definition of total published Medicare payment rate to specifically exclude cost-based Medicare reimbursement methodologies. We considered this alternative because, while the cost-based Medicare reimbursement methodologies are publicly available, the provider specific reimbursement rates resulting from the application of these methodologies to the providers' cost reports are generally not publicly available, and may not meet the definition of a total published Medicare payment rate. If we finalized this option, the payment limit for providers paid by Medicare on a cost basis would default to the State plan approved rate. Another alternative we considered was requiring the State to use only total published Medicare payment rates that undergo the rule making process (for example, the Medicare IPPS rate or Medicare PFS rate) as the basis for the total published Medicare payment rate and therefore, the payment limit for all providers. This alternative would apply to providers reimbursed by Medicare on a cost basis, and the State would be required to use the equivalent total published Medicare payment rate for those providers as the basis for the SDP payment limit. This approach would ensure that all total published Medicare payment rates that serve as the basis for an SDP payment limit are transparent and prospectively established. We ultimately did not propose either of these alternatives because based on discussions and information provided by States and providers we understand that in many instances, the Medicare payment rate or State plan approved rate may be significantly lower than what these providers would be paid under a cost-based methodology.
We request public comment on the proposed approaches and the alternatives considered, and any additional considerations or mechanisms for determining compliance with the applicable payment limit for providers paid outside of the published Medicare fee schedules or Medicare PPS.
( printed page 30415)
In the absence of a total published Medicare payment rate for a Medicaid covered service included in an SDP, we propose a definition of payment limit under § 438.6(a) to specify that 100 percent of the State plan approved rate would be the payment limit for each service under an SDP. This is required under section 71116(a) of the WFTC legislation for the four service types, for the 50 States and DC, and we propose to apply this limit to all services covered under SDPs, for all States including DC and the Territories, when there is no total published Medicare payment rate under § 438.6(c)(8)(iii).
Although an increasing number of benefits are now covered under Medicare Parts A and B, such as opioid use disorder treatment and marriage and family counseling, many Medicaid benefits continue to lack a corresponding total published Medicare payment rate. Generally, Medicaid covers a broader array of services than Medicare and commercial payers, such as some treatments for mental health and substance use disorder, and long-term services and supports, including HCBS. As such, for some of these Medicaid services, there is no comparable payment rate under Medicare.
In those situations, consistent with section 71116 of the WFTC legislation, we believe that using State plan approved rates that have undergone the SPA review process provides the most appropriate benchmark for the payment limit in the absence of a Medicare payment rate. Compared to proprietary, non-standard, or non-existent commercial payment data (as could be relevant to SDPs in the Territories where there may be very low commercial health insurance penetration or for services other than the four services addressed in section 71116 of the WFTC legislation), using State plan approved rates would provide greater transparency, consistency, and validity to support the basis of a payment limit when States opt to direct managed care expenditures via an SDP. The SPA review process is a statutorily defined process that we believe would reduce ambiguity and provide operational ease for States and CMS in terms of implementing a payment limit for SDPs when there is no total published Medicare payment rate for the covered service. The State plan review and approval process ensures that Medicaid State plan approved FFS rates are consistent with efficiency, economy, and quality of care and are sufficient to enlist enough providers so that care and services are available under the plan, at least to the extent that such care and services are available to the general population in the geographic area, as required under section 1902(a)(30) of the Act.
We also consider provider payment rates reviewed and approved by us as part of a section 1115 demonstration waiver or a waiver of the State plan (for example, a section 1915(c) waiver) to meet the definition of State plan approved rates for purposes of establishing the payment limit. Such rates would serve as the basis for the Payment limit when there is no total published Medicare payment rate for the covered service. Although these provider payment rates are not reviewed through the SPA process, they undergo a similarly rigorous review by our staff before they are approved as part of the broader demonstration or waiver authority. This circumstance most commonly arises with health related social needs (HRSN) services and HCBS, which are generally not benefits covered by the Medicare program and in some instances, only available in the Medicaid program via a section 1115 demonstration or other waiver authority. We believe this review process is robust and similar to the SPA review because both the underlying benefits and provider payment rates are subject to CMS review and approval, including to ensure consistency with section 1902(a)(30)(A) of the Act.
b. Payments Limits
To effectuate the proposed payment limit in § 438.6(a), we propose to revise § 438.6(c)(2)(ii)(I) and revise § 438.6(c)(8). First, we propose to replace the existing SDP standard at § 438.6(c)(2)(ii)(I) with new text that would require that all SDPs not exceed the payment limit set forth in revised § 438.6(c)(8). We also propose to revise existing paragraph (c)(8) as (c)(9) and add an introductory phrase “For rating periods beginning” to revised paragraph (c)(8); revise paragraph (c)(8)(i) to specify the applicability date for the requirements proposed in paragraphs (c)(8)(i)(A) and (B); and to incorporate the existing text from paragraph (c)(2)(ii)(I) into paragraphs (8)(i)(A) and (B). We believe these revisions would improve readability and make the applicability date clear. These proposed changes would maintain the existing regulatory requirements for SDPs that do not require written prior approval and ensure that such SDPs would not be subject to the proposed payment limit until the additional limits proposed in § 438.6(c)(8)(iii) are finalized.
Next, we propose to revise paragraph (c)(8)(ii) to require that States not exceed the payment limit for each inpatient hospital service, outpatient hospital service, qualified practitioner service at an academic medical center, or a nursing facility service covered under an SDP described in § 438.6(c)(2)(i), for services furnished during a rating period beginning on or after July 4, 2025. As described in this section, we propose to define “State” at § 438.6(a), solely for the purposes of § 438.6(c)(8)(ii) and only until the first rating period beginning on or after January 1, 2029, to mean one of the 50 States or DC For other purposes and time periods, “State” would also include the Territories. This proposal would apply the payment limits set forth under section 71116 the WFTC legislation to SDPs for the four services that require written prior approval. Under proposed § 438.6(c)(8)(ii), any SDP that requires written prior approval for one or more of the four services and that does not meet the definition of a grandfathered SDP would be subject to the payment limit beginning with the first rating period beginning on or after July 4, 2025. For example, a State that submitted a
new
SDP for hospital inpatient and outpatient services for a CY 2027 rating period would be subject to the payment limits beginning with that rating period because the SDP would not meet the definition of a grandfathered SDP. (See section II.A.2. of this proposed rule for discussion on grandfathered SDPs.)
We also propose to apply the payment limit, which differs for Expansion and Non-Expansion States to all services covered under SDPs via proposed § 438.6(c)(8)(iii). We believe that imposing the same payment limit on all SDPs would be a reasonable and appropriate approach to improve the fiscal integrity of the Medicaid program and would align with the directive in the Presidential Memorandum that Medicaid payment rates not exceed Medicare payment rates. Using consistent benchmarks for evaluating the proposed payment limits for all services within SDPs would help ensure that States do not engage in cost shifting, such as attempting to increase payments to providers for services other than the four services specified in section 71116 of the WFTC legislation to offset the loss of revenue reductions resulting from the payment limit on the four services. For example, hospitals could seek to mitigate the impact of the payment limit by consolidating with other healthcare provider entities, such as independent provider practices and clinics, and by shifting certain services from an outpatient hospital setting to a clinic setting, where SDP payments
( printed page 30416)
would not be subject to the payment limit established in section 71116 of the WFTC legislation. Cost shifting practices of this nature are counter to our goal of greater fiscal integrity within the Medicaid program and could be used to obscure fraud, waste and abuse. We are also proposing § 438.6(c)(8)(iii) to extend the proposed payment limit to all services covered under SDPs in the U.S. territories as our fiscal integrity concerns noted above apply to all 50 States, DC, and U.S. territories.
To provide States sufficient time to redesign SDPs, work with interested parties and legislative bodies, and engage in technical consultation with CMS, we propose to apply the payment limit to all SDPs in the 50 States, DC, and the Territories effective with the first rating period beginning on or after January 1, 2029. We considered earlier effective dates, such as the first rating period beginning after the effective date of the final rule or, on or after January 1, 2027 or January 1, 2028, which could reduce incentives for cost shifting, and reduced SDP expenditures more expeditiously. However, we do not believe that those earlier effective dates would provide States sufficient time to complete the operational, technical, and administrative steps necessary to implement the proposed payment limit. We also considered whether a phase down period was necessary, as is required for grandfathered SDPs under section 71116 of the WFTC legislation. However, we do not believe that requiring a phase down period is necessary for these SDPs given the less complicated design most States have used in SDPs for services other than the four services specified in section 71116 of the WFTC legislation. SDPs for services other than the four specified in WFTC legislation also represent a significantly lower amount of Medicaid expenditures and we believe that a prospective compliance date with the payment limit already allows States sufficient time to transition and initiate their own phase down of implicated SDPs, if desired. We remind States that, regardless of the use of SDPs, Medicaid managed care capitation rates are subject to actuarial soundness requirements and States must comply with all regulatory requirements including network adequacy standards, and CMS contract oversight. These requirements ensure beneficiary access to providers and services, separate and apart from SDPs which are always optional for States.
We propose to prospectively apply, through new paragraph (c)(8)(iii), the same payment limits specified in section 71116 of the WFTC legislation to all services, all States, and all SDPs, applicable with the first rating period beginning on or after January 1, 2029. This proposal would apply the Payment limit defined at § 438.6(a) to the U.S. territories, to SDPs that do not require written prior approval under paragraph (c)(1)(i), and to all other services covered under SDPs.
These proposals to impose payment limits aligned with but in excess of the requirements of section 71116 of the WFTC legislation are based on our authority to interpret and implement section 1903(m)(2)(A)(iii) of the Act, which requires contracts between States and MCOs to provide prospective payment under a risk-based contract for services and associated administrative costs that are actuarially sound and our authority under section 1902(a)(4) of the Act to establish methods of administration for Medicaid that are necessary for the proper and efficient operation of the State plan. These proposals would be extended to PIHPs and PAHPs through regulations based on our authority under section 1902(a)(4) of the Act. As noted in the 2016 final rule, regulation of SDPs is necessary to ensure that Medicaid managed care plans retain sufficient discretion to manage the financial risk associated with providing the benefits covered under their contracts, which is integral to ensuring that capitation rates are actuarially sound as defined in § 438.4 (81 FR 27582).
c. Payment Limit Monitoring and Compliance
To assess and monitor State compliance with the new payment limit, we propose in new § 438.6(c)(8)(ii)(A)(1) to require States to submit, for our review: a list of all providers eligible for the SDP and their National Provider Identifiers (NPIs), the total published Medicare payment rate or State plan approved rate (only when no total published Medicare payment rate exists for the covered service) that serves as the basis of the payment limit for each service covered under the SDP. We also propose in § 438.6(c)(8)(ii)(A)(2) that States would be required to provide a detailed description of how the State would ensure that payment to each provider for each furnished service would not exceed the payment limit. With these proposals, States would be aware of the payment limits and have a plan in place to ensure compliance. We would expect States to provide detailed information about the processes, systems, technology or other controls they would utilize to ensure that each payment under the SDP does not exceed the payment limit.
In addition, under proposed § 438.6(c)(8)(ii)(C), we would have authority to request additional documentation from States to assess compliance with the payment limit. We believe that this documentation would allow us to fully understand how a State would verify regulatory compliance and allow us or other oversight bodies to engage in robust post-implementation monitoring and oversight. For example, we or another oversight body could utilize the submitted NPI list to extract relevant Transformed Medicaid Statistical Information System (T-MSIS) data for each provider eligible for an SDP during a specific rating period, and then compare the actual paid amount in T-MSIS to the total published Medicare payment rate or State plan approved rate (only when no total published Medicare payment rate exists for the covered service) that serves as the basis of the payment limit for each service covered under the SDP to determine if payment for each service covered under an SDP has complied with the applicable payment limit.
For States implementing VBP SDPs as permitted under paragraphs (c)(1)(i) and (ii), we propose § 438.6(c)(8)(ii)(B) to require States to provide a detailed validation methodology to ensure that payments from VBP SDPs do not exceed the payment limit on a per service basis. For example, a State that opts to implement a population-based payment SDP under § 438.6(c)(2)(vi)(C) would be expected to reconcile prospective population-based payments to actual utilization occurring during the rating period to verify that the payment limit was not exceeded on a per service basis. States implementing performance-based payments under § 438.6(c)(2)(vi)(B) would need to account for the base payments paid to providers [56]
and ensure through a detailed validation methodology that the per service payment limit was not exceeded. Providers that already receive base payments (that is, negotiated rates) from managed care plans that exceed the payment limit would not be eligible to receive additional SDP payments that would result in the per service payment limit being exceeded. We believe a validation methodology would be necessary for VBP SDPs specifically because there is greater risk of unintentionally exceeding the payment limit given how VBP SDP models are developed under § 438.6(c)(2)(vi)(C).
( printed page 30417)
We considered several alternative proposals because we recognize that a per service payment limit may pose operational and logistical complexities, particularly in the context of population and condition-based SDP arrangements. VBP SDPs have been important tools for States to improve the value of and quality of care furnished to Medicaid managed care enrollees, and we are always available to provide technical assistance to States interested in implementing VBP SDPs. Because such arrangements are typically structured as prospective payments to providers (that is, per member per month (PMPM) payment) for an attributed population and defined set of services, we considered alternative proposals in recognition of the unique challenges that may arise for States when implementing VBP SDPs.
One alternative approach we have considered for VBP SDPs is requiring the State to work with its actuaries to develop the population or condition-based SDP using actuarial principles and have the State's actuary certify that the provider payment under the SDP (inclusive of any performance based payments and/or shared savings) was developed in such a way that payment to providers would not exceed the permissible applicable payment limit based on the services covered under the SDP. We seek public comment on this alternative and other operational or oversight approaches to ensure fiscal integrity with regards to the payment limit and VBP SDPs. We also seek potential ideas to operationalize alternative value-based arrangements in Medicaid, given that value-based care is a is a tool to support CMS priorities including holding providers accountable for health outcomes and reducing wasteful spending.
We remind States of certain existing regulatory requirements that are applicable to their monitoring and oversight of SDP implementation and compliance with the payment limit. The term “overpayment” is defined at § 438.2 to mean any payment made to a network provider by a managed care plan to which the network provider is not entitled to under Title XIX of the Act or any payment to a managed care plan by a State to which the plan is not entitled to under Title XIX of the Act. Payments under SDPs to providers in excess of the applicable payment limit would meet the definition of an overpayment. Part 438 subpart H outlines requirements with respect to overpayments, including both State and managed care plan obligations. Contracts with managed care plans must specify policies and procedures related to reporting, documentation, and recovery of overpayments made by the managed care plan to the provider, as required at § 438.608(d). Given these requirements, States and plans should already have in place policies and procedures to address overpayments and should consider whether any refinements are necessary to address SDP-related overpayments. This level of oversight and monitoring should occur with regularity throughout the applicable rating period and at least on a quarterly basis.
While States may work with their managed care plans to implement upfront processes and system guardrails to avoid per service payments in excess of the SDP payment limit, such as automating a limit in the claims processing system, § 438.242(d) requires States to review and validate encounter data collected, maintained, and submitted by their managed care plans. Under § 438.242(c)(3), the encounter data must include allowed amounts and paid amounts. By regularly validating encounter data inclusive of the amount paid by the managed care plan, the State can ensure that any SDP overpayments are identified and addressed in a timely manner. In accordance with § 438.608(d)(4), the State must use that encounter data and information collected on overpayments identified or recovered for purposes of setting actuarially sound capitation rates for each managed care plan consistent with the requirements at § 438.4. States must work with their actuaries to ensure that assumptions related to overpayments are accounted for in capitation rate development.[57]
We remind States that they must reimburse us for an amount equal to the Federal share of overpayments consistent with section 1903(d)(2) of the Act and § 433.312.
If States do not provide sufficient documentation of their monitoring approaches as required in proposed § 438.6(c)(8)(ii)(A) and (B), and to ensure that we would be able to require any additional documentation necessary to ensure compliance with the proposed payment limit, we propose § 438.6(c)(8)(ii)(C) that would require States to provide any additional documentation that we request to document compliance. In our experience reviewing and approving SDPs since 2017, we often must request additional materials or data as part of our SDP review to ensure State compliance with Federal requirements and to mitigate fiscal and program integrity concerns. This proposal would formalize our authority to continue to request additional documentation when needed to ensure that States are complying with the applicable payment limit.
We propose to repeat the requirements proposed at § 438.6(c)(8)(ii)(A) through (C) in paragraphs (8)(iii)(A) through (C) but add “upon request” to the last phrase of the introductory text in paragraph (8)(iii). We believe it would be necessary to repeat these requirements to ensure that when the payment limit applies to all SDPs as proposed in § 438.6(c)(8)(iii), we are able to continue to request this information from States to assess compliance with the payment limit. This proposed revision would enable us to request this documentation from States with SDPs that do not require submission of a preprint for written prior approval by us. We propose that paragraph (c)(8)(iii) would be applicable beginning with the first rating period on or after January 1, 2029, to all 50 States, DC, and the U.S. territories.
Based on our experience reviewing and approving SDPs since 2016, States often request extensive technical assistance on SDP policies and regulatory requirements including guidance on key SDP policy, SDP design, the SDP quality evaluation, compliance with the applicable payment limit, associated documentation that must be submitted to CMS, and strategies for State monitoring and oversight of SDP implementation. We also acknowledge that as the Original Medicare program revises their payment rules and policies, States will have questions about the applicability of those changes to the SDP payment limit in Medicaid managed care. Under § 438.7(e), we issue additional guidance to States on a number of topics and elements relevant to requirements for rate certification submission; this guidance came to be known as the Medicaid Managed Care Rate Development Guide [58]
and is published on an annual basis. We believe that similar published guidance is necessary for SDPs given the complexity of SDP policy and the new payment limit under the law. We propose new § 438.6(c)(9) which would require us to issue guidance, as needed, on topics including: Federal requirements and standards for the SDP, documentation required to determine that the SDP has been developed in
( printed page 30418)
accordance with the requirements of § 438.6(c), any considerations for applicability of the payment limit, the documentation required to demonstrate compliance with the payment limit, any updates or developments in the State directed payment review process to facilitate prompt CMS review, and any considerations for state monitoring, oversight, and evaluation of the SDP. We believe that this guidance will be necessary to provide more granular guidance to States than is possible under a regulation.
d. State Expansion Status
For States that begin providing expansion coverage on or after July 4, 2025 (the date of enactment of the WFTC legislation), section 71116(c) of the WFTC legislation specifies that the payment limit for SDPs described under current § 438.6(c)(2)(iii) would be the applicable payment limit for Expansion States as outlined in section 71116(a)(1) of the WFTC legislation. Section 71116(c) of the WFTC legislation states that this newly applicable SDP payment limit would apply to services furnished during the first rating period on or after the date of enactment. Because section 71116(c) of the WFTC legislation ties the applicability of the payment limit (see proposed definition of “payment limit” in section II.A.1.A. of this proposed rule) to the rating period in which the service is furnished, we interpret this to mean that the payment limit for an Expansion State (see proposed definitions of “Expansion State” and “Non-Expansion State” in section II.A.1.A. of this proposed rule) would apply beginning with the first rating period that begins on or after the date the State begins providing expansion coverage.
We also believe that the reverse would be true; that is, if a State were to transition from an Expansion State to a Non-Expansion State, that State's SDPs would then be subject to the applicable payment limit for Non-Expansion States. Although this scenario is not delineated in section 71116(c) of the WFTC legislation, we believe that the payment limit for a State's SDPs should be tied to its expansion status as explicitly defined in sections 71116(a)(1) and (2) of the WFTC legislation. We believe this would be necessary to implement the proposed payment limit equitably among States and with clarity for enforcement. We are not proposing any specific regulation text to address this policy; we believe our proposals to define and implement the payment limit (see sections II.A.1.A. and B. of this proposed rule) would permit us to enforce this interpretation, if finalized as proposed. We seek public comments on all of our proposals.
2. Grandfathered SDPs (§ 438.6(a) and (c)(2)(iii))
Section 71116(b) of the WFTC legislation provides for delayed compliance with the payment limit (described in section II.A.1. of this proposed rule and in section 71116(a) of the WFTC legislation) for certain, eligible SDPs. In this proposed rule, we refer to section 71116(b) of the WFTC legislation as the “grandfathering provision” and SDPs that are described in and subject to the provision are referred to as “grandfathered SDPs.” We also refer to the period of delayed full compliance with the payment limit in section 71116(a) of the WFTC legislation for grandfathered SDPs as the “temporary grandfathering period.” The criteria for an SDP to qualify as a grandfathered SDP are specified in section 71116(b) of the WFTC legislation, including applicable types of services, the applicable rating periods, and status of the SDP preprint.
a. Definition of a Grandfathered SDP
The first criterion for an SDP to qualify to be grandfathered is that it be described under § 438.6(c)(2)(iii), which is limited to SDPs that require written prior approval and are for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at an AMC. The current regulatory requirements in § 438.6(c)(2)(iii) specify that the total payment rate for each SDP for which written prior approval is required for the four services must not exceed the ACR. Because the grandfathering provision in section 71116(b) of the WFTC legislation allows delayed compliance with the payment limit in section 71116(a) of the WFTC, we propose to adopt these criteria pertaining to the four services and an SDP that requires written prior approval as part of the definition for “Grandfathered State directed payment” under § 438.6(a).
The second criterion is that the SDP must be for a “rating period occurring within 180 days of the date of enactment” of the WFTC legislation. We interpret “180 days” to refer to 180 business days. We believe this interpretation is appropriate because activity on SDP preprints, including our review and approval, occurs on business days and not on weekends or Federal holidays. To align with Federal practice, we propose to define “Business day” under § 438.2 to mean Monday through Friday, excluding Federal holidays as set forth under 5 U.S.C. 6103.[59]
Other government agencies, such as the Office of Personnel Management (OPM) rely on 5 U.S.C. 6103 to determine Federal holidays, and we believe aligning our definition with that framework provides clarity and administrative consistency.
Section 71116(b) of the WFTC legislation further specifies that the rating period must be “occurring within” the 180-day timeframe. A rating period is defined in § 438.2 as a period of 12 months selected by the State for which actuarially sound capitation rates are developed and documented in the rate certification submitted under § 438.7(a). States utilize different rating periods. For example, some States utilize a CY rating period while others use 12-month rating periods that begin in April, July, August or October. In some cases, these non-CY rating periods align with a State fiscal year (SFY). Given these variations, we interpret the phrase “occurring within 180 days of enactment” to encompass rating periods that begin within 180 business days before or within 180 business days after July 4, 2025, the date of enactment of the WFTC legislation. Under this proposed interpretation of this criterion, the grandfathering provision would apply to eligible SDPs in rating periods that include any business days between October 11, 2024 through July 3, 2025 or between July 5, 2025, and March 27, 2026. This would include rating periods for CY 2024, SFY 2025, CY 2025, SFY 2026, and CY 2026 which we refer to as “eligible rating periods” in this proposed rule. Rating periods that do not include any business days within those timeframes, including SFY 2027, would not qualify. We propose to incorporate this interpretation into the definition of a grandfathered SDP proposed at § 438.6(a).
The third criterion to determine whether an SDP is eligible for the grandfathering provision in section 71116(b) of the WFTC legislation pertains to the status of an eligible SDP preprint. Specifically, SDPs for an eligible rating period with one of the below statuses could qualify for the grandfathering provision, consistent with section 71116(b) of the WFTC legislation. We acknowledge that the terms “good faith effort” and
( printed page 30419)
“completed preprint” are further described in this section.
SDPs (other than for rural hospitals) for which written prior approval was made by us before May 1, 2025;
SDPs (other than for rural hospitals) for which a good faith effort to receive our approval was made before May 1, 2025;
SDPs for rural hospitals for which written prior approval was made by us before July 4, 2025;
SDPs for rural hospitals for which a good faith effort to receive our approval was made before July 4, 2025; and
SDPs for which a completed preprint was submitted to us prior to July 4, 2025.
The terms “rural hospital” and “written prior approval” utilized in section 71116(b) of the WFTC legislation are defined in section 71116(d) of the WFTC legislation. Rural hospital is defined in section 71116(d)(2) of the WFTC legislation to mean: (1) a section (d) hospital (as defined in paragraph (1)(B) of section 1886(d) of the Act (42 U.S.C. 1395ww(d))) that— (i) is located in a rural area (as defined in paragraph (2)(D) of such section); (ii) is treated as being located in a rural area under paragraph (8)(E) of such section; or (iii) is located in a rural census tract of a metropolitan statistical area (as determined under the most recent modification of the Goldsmith Modification, originally published in the
Federal Register
on February 27, 1992 (57 FR 6725)); (2) a critical access hospital (as defined in section 1861(mm)(1) of such Act (42 U.S.C. 1395x(mm)(1))); (3) a sole community hospital (as defined in section 1886(d)(5)(D)(iii) of such Act (42 U.S.C. 1395ww(d)(5)(D)(iii))); (4) a Medicare-dependent, small rural hospital (as defined in section 1886(d)(5)(G)(iv) of such Act (42 U.S.C. 1395ww(d)(5)(G)(iv))); (5) a low-volume hospital (as defined in section 1886(d)(12)(C) of such Act (42 U.S.C. 1395ww(d)(12)(C))); or (6) a rural emergency hospital (as defined in section 1861(kkk)(2) of such Act (42 U.S.C. 1395x(kkk)(2))). Section 71116(d) of the WFTC legislation specifies that the term “written prior approval” has the meaning reflected in its use in § 438.6(c)(2)(i) (or a successor regulation).
The term “completed preprint” as used in section 71116(b) of the WFTC legislation is not defined in section 71116(d) of the WFTC legislation or existing regulation. In the
CMCS Informational Bulletin (CIB)
published on November 7, 2023,[60]
we outlined guidance on the components of a complete submission for Medicaid managed care contracts, rate certifications, and SDP preprints. On page 6 of this CIB, we noted that “[a] complete State directed payment preprint submission requires a State directed payments preprint form as well as the preprint addendum tables in an Excel workbook, as necessary. . . . The preprint must be completed in full, and all information must be provided only in the fillable sections of the preprint and the addendum tables.” We believe it would be appropriate to define a “completed preprint” consistent with the definition in this guidance, as it is an accurate representation of the information necessary from States to begin review of an SDP preprint, and would ensure that States had adequate notice of this definition prior to enactment of the WFTC legislation. We propose the definition of “completed preprint” at § 438.6(a) to mean an SDP preprint with all relevant sections of the preprint filled out, and all information provided only in the fillable sections of the preprint and the published addendum tables, as applicable. Given the significance of a completed preprint for implementation of section 71116(b) of the WFTC legislation, we believe § 438.6(c) would be more comprehensive and clear if it included a definition of “preprint” and explicitly stated the requirement for submission to obtain written prior approval. Although preprint submission has been the only method by which a State could obtain written prior approval of an SDP since their inception, we believe § 438.6(c)(2)(i) would benefit from the addition of a definition of “preprint” in § 438.6(a) to reference the template published by us and an explicit requirement in § 438.6(c)(2)(i) that preprints would have to be submitted for all SDPs that require written prior approval.
The term “good faith effort” is also not defined in section 71116(d) of the WFTC legislation or in existing regulation. As noted in the CIB published on November 7, 2023, “[f]or those State directed payments that require written prior approval, we must receive a complete preprint before we will begin review.” Consistent with this guidance, we interpret a State's submission of a completed SDP preprint prior to the applicable statutory date to constitute a good faith effort to receive our approval. Therefore, we believe the term “good faith effort” in status “2” and status “4” to mean submission of a completed preprint. We believe this interpretation gives effect to the phrase “good faith effort” by recognizing States that took affirmative steps within the established SDP approval framework to seek written prior approval. Under the existing regulatory structure, submission of a completed preprint is the only objective action that initiates our review, and other actions short of submission of a completed preprint do not initiate review and therefore do not demonstrate a good faith effort to obtain our approval. We do not believe that adopting a broader interpretation of “good faith effort” would result in the inclusion of additional SDPs beyond those already encompassed within statuses “1” and “5”. We considered another interpretation of “good faith” to mean that the SDP had been documented in Medicaid managed care contracts and rate certifications by July 4, 2025. However, the SDPs under the purview of the statute are those that specifically require prior approval [61]
by us, meaning that the State must submit a preprint for our review and approval prior to implementation. In the absence of a completed SDP preprint submission, documentation in contracts and rate certifications does not sufficiently represent a good faith effort to receive our approval. The preprint submission is needed for us to complete our review and approval of an SDP that requires prior approval. We considered whether technical assistance calls or informal consultation might rise to level of a “good faith effort;” however, these activities do not provide sufficiently cogent or detailed information for us to reasonably initiate a SDP review.
Additionally, as a practical matter, SDPs for which a completed preprint has been submitted to us prior to July 4, 2025 (status “5”), would encompass all SDPs that would otherwise be eligible under statuses “1” through “4.” Under our existing review process, a State cannot obtain written prior approval without submitting a completed preprint. As a result, any State that received written prior approval from us before May 1, 2025 or July 4, 2025, would necessarily have submitted a completed preprint before July 4, 2025. Therefore, rather than repeatedly list all five statuses in this proposed rule, we propose that an SDP would be eligible under the third criterion if a completed preprint was submitted to us prior to July 4, 2025. We propose to adopt this criterion as part of the definition for a grandfathered SDP at § 438.6(a).
( printed page 30420)
In addition, we propose that the grandfathering provisions apply only where an SDP exceeds the payment limit set forth in § 438.6(c)(8). In general, the statutory phase down framework applies to bring higher payment levels into compliance with the applicable limit. Where an SDP is already at or below the payment limit, application of the grandfathering framework would not have practical effect and could limit a State's ability to modify the SDP to increase payments up to the permissible payment limit. In summary, to more easily reference SDPs that meet these criteria for grandfathering in this proposed rule and in § 438.6, we propose to add the term “Grandfathered State directed payment” to the definitions under § 438.6(a). We propose to define “Grandfathered State directed payment” to mean an SDP for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at academic medical centers that received written prior approval under paragraph (c)(2)(i); is for a rating period that includes at least 1 business day between October 11, 2024 and July 3, 2025 or July 5, 2025 and March 27, 2026; and for which a completed preprint with an eligible rating period and documented total dollar amount (as specified in item 4 of the current SDP preprint) was submitted to us prior to July 4, 2025. It is essential to require that the completed preprint submitted to us prior to July 4, 2025 contains an eligible rating period and documented total dollar amount as these elements are essential to establish eligibility for grandfathering. Under our proposed definition, States would not be permitted to revise a preprint submission after July 4, 2025 to change the rating period to qualify as a grandfathered SDP, or to increase the total dollar amount of a grandfathered SDP. The SDP would also need to exceed the payment limit set forth in paragraph (c)(8).
b. Temporary Grandfathering Period
Grandfathered SDPs are eligible for a temporary grandfathering period and subject to a phase down of the total amount of the SDP to the payment limit beginning with the first rating period on or after January 1, 2028, as specified in section 71116(b) of the WFTC legislation. Section 71116(b) of the WFTC legislation specifies that beginning with the rating period on or after January 1, 2028, a State must begin an annual phase down of the “total amount” of the Grandfathered SDP. We believe the specified “total amount” of the SDP refers to the total amount of the SDP approved for the rating period for which the SDP qualified for grandfathered SDP status (for example, SFY 2025, CY 2025, CY 2026 or SFY 2026). For SDPs that require written prior approval, States are required to submit an SDP for written prior approval using the current CMS issued preprint.[62]
Item 4 of the current SDP preprint captures the State's estimated total dollar amount associated with the SDP to provide transparency regarding the fiscal impact (Federal and non-Federal share) of the State's proposal and to aid our review for written prior approval required under § 438.6(c)(2)(i), including our assessment of whether the SDP complies with standards outlined in § 438.6(c)(2). Therefore, we believe the estimated total dollar amount listed in item 4 of the preprint would be the most reasonable, practical, and consistent way to interpret and implement “total amount” in section 71116(b) of the WFTC legislation. In the interest of controlling the rapid growth in SDP spending and consistent with section 71116 of the WFTC legislation and the Presidential Memorandum, we propose to utilize the total dollar amount documented in item 4 of the preprint approved by us for each grandfathered SDP as the maximum amount of expenditures that would be allowed for that SDP during the temporary grandfathering period prior to the start of the phase down that begins with rating periods on or after January 1, 2028. We propose to define “Grandfathered total dollar amount” under § 438.6(a) to mean the total dollar amount approved by us for a grandfathered SDP. When preprint submissions of the same SDP for different rating periods meet the definition of a grandfathered SDP, the highest total dollar amount approved by us is the maximum grandfathered total dollar amount. For example, if a State has a SFY 2025 preprint and a SFY 2026 preprint for the same SDP that both qualify as grandfathered SDPs, and the SFY 2025 preprint totals $100 million (as specified in item 4 of the approved preprint) while the SFY 2026 preprint totals $105 million (as specified in item 4 of the approved preprint), then $105 million would be the grandfathered total dollar amount.
As described, the grandfathered total dollar amount identified in item 4 of the preprint represents the maximum total amount of expenditures for the SDP and is subject to the required phase down. This makes it more challenging to incorporate a grandfathered SDP into capitation rates as an adjustment to the capitation rates because fixed aggregate funding amounts are generally not compatible with prospective capitation rate development and actuarial soundness in risk-based managed care. Capitation rates are generally paid on a PMPM basis and total spending in a managed care program can fluctuate with enrollment and utilization changes. When grandfathered SDPs are included in the PMPM as an adjustment to the capitation rates it presents the possibility that the grandfathered total dollar amount could be exceeded if enrollee utilization is higher than projected. It could also increase the administrative burden on States, which would need to monitor actual utilization and SDP spending, and submit SDP preprint amendments and/or rate amendments, as applicable to ensure that the grandfathered total dollar amount is not exceeded.
We have considered how best to ensure fiscal integrity of the grandfathered total dollar amount during the temporary grandfathering period and through the phase down period. One option we considered is to permit grandfathered SDPs to use separate payment terms on a time-limited basis. However, as we have stated in prior guidance, “[a]s CMS has reviewed State directed payments and the related rate certifications, CMS has identified a number of concerns around the use of separate payment terms. Frequently, while there is risk for the providers, there is often little or no risk for the plans related to the directed payment, which is contrary to the nature of risk-based managed care. This can also result in perverse incentives for plans that can result in shifting utilization to providers in ways that are not consistent with Medicaid program goals.” [63]
We further stated in the 2024 final rule that “some States are increasingly relying on this payment mechanism to circumvent risk-based payment to managed care plans. More specifically, it is a way to circumvent compliance with the requirement that SDPs be developed in accordance with § 438.4, and the standards specified in §§ 438.5, 438.7, 438.8, and generally accepted actuarial principles and practices.” [64]
While we continue to have concerns with separate payment terms, we also acknowledge that, in this limited context resulting from the WFTC legislation, they may provide a more
( printed page 30421)
transparent and administratively feasible mechanism for Federal and State monitoring and oversight of compliance with the grandfathered total dollar amount and associated phase down requirements as a separate payment term can be directly targeted to the total dollar amount. For this reason, we are proposing and seek comment on a time-limited exemption to the prohibition on separate payment terms only in this limited circumstance. More specifically, we propose in § 438.6(c)(2)(iii)(F) to permit a State to delay compliance with the separate payment term prohibition in § 438.6(c)(6) and the preprint timing submission requirements in § 438.6(c)(2)(viii) for a grandfathered SDP until the first rating period in which the payment limit is met in accordance with § 438.6(c)(8). Beginning with the first rating period that the payment limit is met under § 438.6(c)(8), the State would be required to comply with the prohibition on separate payment terms and the prospective preprint submission requirements because, under the proposed definition of “Grandfathered State directed payment” in § 438.6(a), an SDP that no longer exceeds the payment limit would no longer qualify as a grandfathered SDP. This means that with the first rating period that the payment limit is met (as demonstrated by the total payment rate comparison in Table 2 of the preprint submission), the State would be required to incorporate the SDP as an adjustment to the capitation rates, submit the preprint prospectively (if applicable) and, if the SDP is for a rating period that starts on or after January 1, 2028, the State would be required to comply with the permissible types of SDPs (that is, minimum fee schedule, maximum fee schedule or value-based payment arrangement). We request public comment on this specific approach and if there are any other operational considerations we should take into account. States with grandfathered SDPs are required to ensure that the grandfathered total dollar amount is not exceeded in any rating period during the phase down period. We are not proposing to revisit these regulatory provisions for any other SDPs or scenarios and intend this as a time-limited exemption for eligible grandfathered SDPs only.
We reiterate that we continue to have concerns with separate payment terms and have considered several alternative proposals. An alternative we considered, and invite comment on, was to maintain the prohibition on the use of separate payment terms, without exceptions, in § 438.6(c)(6) and the preprint timing submission requirements in § 438.6(c)(2)(viii). Under this alternative, all SDPs would be required to comply with the requirements finalized in the 2024 final rule. Another alternative we considered was to maintain the prohibition on the use of separate payment terms, require that all SDPs be incorporated into rates as adjustments to the base capitation rates and create narrow flexibilities to ease the administrative burden for States to monitor compliance with the grandfathered total dollar amount, including monitoring of actual utilization and SDP spending. We also considered waiving only the prospective preprint submission timing requirements in § 438.6(c)(2)(viii), without waiving the prohibition on separate payment terms in § 438.6(c)(6). This alternative would allow States to retroactively modify their SDP preprints once utilization is known to ensure that the grandfathered total dollar amount is not exceeded for a specific rating period. We recognize that this alternative would be less consistent with the prospective submission framework established in § 438.6(c)(2)(viii), but considered it as a potential means of reducing the risk that actual expenditures would exceed the grandfathered total dollar amount.
We also considered whether we should require States to use separate payment terms and uniform increase SDPs for all grandfathered SDPs. Separate payment terms are typically structured as predetermined, finite pools of funding, which aligns with our proposals for a grandfathered total dollar amount. In our experience, it is difficult to incorporate a minimum fee schedule or maximum fee schedule type SDP into the capitation rates as a separate payment term because a fee schedule by nature means that total provider payments that are based on the fee schedule will ultimately vary due to utilization. For this reason, if we were to require separate payment terms, we would likely also need to require that States utilize either a uniform increase type SDP or value-based payment SDP which can be more easily incorporated into the capitation rates as a separate payment term. However, we did not propose this alternative because of our longstanding concerns with the use of separate payment terms, including that they are utilized by States to circumvent risk-based payment to managed care plans (89 FR 41109). We are also concerned that such an alternative would remove the State's ability to determine the type of SDP that furthers the State's overall Medicaid program goals and objectives and could be overly prescriptive.
In the 2023 proposed rule, we proposed a number of regulatory provisions related to separate payment terms and we consider their relevancy again given the new statutory requirements under the WFTC legislation. We also considered whether to amend § 438.6(a) to define “Separate payment term” as a pre-determined and finite funding pool that the State establishes and documents in the Medicaid managed care contract for a specific SDP. Payments made from this funding pool are made by the State to the managed care plan exclusively for SDPs and are made separately and in addition to the capitation rates identified in the contract as required under § 438.3(c)(1)(i).[65]
Defining the term “separate payment term” could offer additional clarity to States regarding the nature and permissibility of a separate payment term. We seek public comment on this potential definition. We also consider whether it would be beneficial to again propose a regulatory revision that the separate payment term could not exceed the total dollar amount documented in the written prior approval for each SDP, for additional clarity regarding the hard limit on the grandfathered total dollar amount.[66]
We seek public comments on all alternatives considered.
We propose to revise § 438.6(c)(2)(iii)(A) through (C) as § 438.6(c)(2)(iii)(C)(1) through (3) and to replace the existing text in § 438.6(c)(2)(iii) with proposed text stating that SDPs that meet the definition of a grandfathered SDP would be eligible for delayed compliance with the payment limit. We also propose new introductory text in § 438.6(c)(2)(iii) to make the requirements at § 438.6(c)(2)(iii)(A) through (F) applicable to all grandfathered SDPs.
To establish clear guardrails to ensure that the maximum total amount for a grandfathered SDP would not be exceeded during each rating period of the temporary grandfathering period, we propose in § 438.6(c)(2)(iii)(A) that subsequent renewals of or amendments to a grandfathered SDP must not exceed the grandfathered total dollar amount for each rating period beginning on or after July 4, 2025 but before January 1, 2028.
Under § 438.6(c)(2)(iii)(C), we propose that the total payment rate that would be effective under proposed paragraphs
( printed page 30422)
(c)(2)(iii)(A) and (B) (that is, the limits on total amount and phase down applicable to a grandfathered SDP) must not exceed the ACR. We believe this would prevent States from redesigning grandfathered SDPs to result in total payment rate(s) that could exceed ACR without exceeding the maximum total amount permitted for a grandfathered SDP. For example, a State could choose to redesign a renewal of a uniform increase grandfathered SDP during the temporary grandfathering period. As part of that redesign, the State could redefine the eligible provider classes and modify the uniform increase for each provider class and service type such that the renewal SDP would not exceed the maximum total amount permitted in paragraph (c)(2)(iii)(A) for the SDP overall, but the total payment rate(s) by provider classes would exceed the ACR.
We believe it would be necessary to monitor for a time-limited period how the total payment rate under a grandfathered SDP would compare to the ACR so as not to create a loophole that would allow States to direct managed care plans to make payments to providers under a grandfathered SDP that exceed ACR. This loophole would run counter to Congressional intent to decrease SDP payment rates for the four services from rates up to the ACR as currently allowed under regulation to the new statutory payment rate limits based on the total published Medicare or Medicaid State plan payment rates, as well as our goals of fiscal integrity and more reasonable payment rates for Medicaid providers via SDPs. Monitoring how the total payment rate compares to ACR may only be necessary through the end of the first rating period of the phase down period for a grandfathered SDP, after which we anticipate that the general design of each SDP would remain relatively stable as States focus on the required phase down and a comparison to new payment limits, that is, the new limits based on the total published Medicare payment rate or Medicaid State plan approved rate.
We contemplated whether States should be required to continue demonstrating compliance with ACR demonstration and total payment rate comparison [67]
to ACR for a longer period of time, given that States retain flexibility to redesign grandfathered SDPs during the phase down period so long as they comply with the required phase down schedule. With this in mind, we considered extending the ACR requirements beyond the first rating period of the phase down, including a period of more than 1 year and up to 10 years. We believe that a 10-year requirement is likely unnecessary given the required phase down schedule (see section II.A.2.c. of this proposed rule for additional information about the phase down) which will significantly reduce the risk of exceeding the ACR as the total dollar amount associated with the SDP phases down over time. In addition, maintaining the ACR demonstration and total payment rate comparison to ACR for a longer period of time would increase the administrative burden for both us and the State as States with grandfathered SDPs would be required to calculate and submit additional annual total payment rate comparisons under our proposals. We request public comment on whether the ACR monitoring requirement should apply for 1 year, or for another whole numbers of years, up to 10 years to ensure that we have adequate oversight into how total payment rates compare to the ACR.
By redesignating the existing ACR demonstration and total payment rate comparison currently in § 438.6(c)(2)(iii)(A) through (C) as § 438.6(c)(2)(iii)(C)(1) through (3) and maintaining applicability of these provisions to the original applicability dates in the 2024 final rule, we propose that the State would continue to provide an ACR demonstration and total payment rate comparison using ACR for a grandfathered SDP until the first rating period beginning on or after January 1, 2029. We are not proposing to change any of the existing requirements for an ACR demonstration or total payment rate comparison.
We seek public comments on all of our proposals.
c. Phase Down of Grandfathered SDPs
Section 71116(b) of the WFTC legislation provides that grandfathered SDPs are subject to a temporary grandfathering period followed by a required phase down of the total amount of the grandfathered SDP to the allowable payment limit. Section 71116(b) of the WFTC legislation requires that beginning with the first rating period on or after January 1, 2028 for grandfathered SDPs, “the total amount of such payment shall be reduced by 10 percentage points each year until the total payment rate for such service is equal to the rate for such service specified in section (a).” In section II.A.2.b. of this proposed rule, we explained our interpretation of the phrase “total amount” of such payment to mean the total amount of the SDP approved for the rating period for which the SDP qualified for grandfathered SDP status as identified in item 4 of the preprint approved by us for each grandfathered SDP. We also proposed a definition of “grandfathered total dollar amount” under § 438.6(a) to mean the total dollar amount approved by us for a grandfathered State directed payment. When preprint submissions of the same SDP for different rating periods meet the definition of a grandfathered State directed payment, the highest total dollar amount approved by us is the grandfathered total dollar amount.
Next, we consider the phrase “the total amount of such payment shall be reduced by 10 percentage points each year.” We interpret this provision to require an annual reduction equal to 10 percentage points of the grandfathered total dollar amount, calculated using the original grandfathered total dollar amount as the baseline, each year of the phase down period until the applicable payment limit is reached. We base this interpretation on the statutory language “10 percentage points each year,” which supports a fixed annual reduction from a constant baseline (that is, the grandfathered total dollar amount). Section 71116(b) of the WFTC legislation requires that the grandfathered SDP be phased down until “the total payment rate for such service is equal to the rate for such service specified in section (a).” In sections II.A.2.a. and 2.b. of this proposed rule, we explain our interpretation of section 71116(a) of the WFTC legislation and propose a definition of “Payment limit” under § 438.6(a) to mean, as applicable, one of the following: 100 percent of the total published Medicare payment rate for an Expansion State; 110 percent of the total published Medicare payment rate for a Non-Expansion State; and only in instances when there is no total published Medicare payment rate for the covered service, 100 percent of the State plan approved rate. See sections II.A.1.a. and 1.b. of this proposed rule for further discussion of the proposed definition of “Payment limit” in § 438.6(a) and applicability of the payment limit in § 438.6(c)(8).
We believe it is reasonable to interpret sections 71116(a) and (b) of the WFTC legislation to require that beginning with the first rating period on or after January 1, 2028, the grandfathered total dollar amount must be phased down by the amount that represents 10
( printed page 30423)
percentage points of that amount annually, unless a greater reduction is requested by the State, until the applicable payment limit is reached. As discussed in sections II.A.2.a and II.A.2.b. of this proposed rule, the payment limit is defined in proposed § 438.6(a) and reflects the limits specified in section 71116(a) of the WFTC legislation. To implement this phase down consistent with the statute, we propose to add § 438.6(c)(2)(iii)(B) which would require that beginning with the first rating period on or after January 1, 2028, the State would be required to decrease the total dollar amount of a grandfathered SDP by at least 10 percentage points annually, until the payment limit proposed in § 438.6(c)(8) is met. Under our proposal, the 10-percentage point phase down is based on the original grandfathered total dollar amount rather than an annually compounding reduction.
To illustrate our proposal, we outline a phase down example for a State with an SDP for a CY 2025 rating period that meets the definition of a grandfathered SDP. In this example, the grandfathered total dollar amount for CY 2025 is $1 billion, as identified in item 4 of the approved preprint. Under our proposal, the State would be permitted to submit SDP renewals to maintain or reduce the Grandfathered total dollar amount ($1 billion) for each of the two subsequent rating periods (CY 2026 and CY 2027). Beginning with the CY 2028 rating period (that is, the first rating period beginning on or after January 1, 2028), the State would be required to phase down the grandfathered total dollar amount by at least 10 percentage points annually (that is, $100 million) until the applicable payment limit is reached. Under our proposal, that annual reduction amount would be at least $100 million, which is 10 percent of the Grandfathered total dollar amount of $1 billion. In the event that a State opted to phase down by greater than the annual reduction amount for a year, we expect the following annual phase down reduction amount would still follow the prescribed schedule but the reduction could be pro-rated to reflect the cumulative reduction required under § 438.6(c)(2)(iii)(B), taking into account any excess reduction in the prior rating period. Using the $1 billion grandfathered total dollar amount example, if the State chooses to phase down by $150 million in the first rating period of the phase down, they would only need to phase down by an additional $50 million in the subsequent rating period. The State would not be permitted to direct their managed care plans to expend amounts exceeding the applicable total dollar amount of the grandfathered SDP for each year of the grandfathering period or during the required phase down period. States would need to work closely with their managed care plans each year to monitor and ensure that the total dollar amount of projected and actual expenditures for the grandfathered SDP paid by managed care plans to providers for the rating period does not exceed the applicable total dollar amount under § 438.6(c)(2)(iii)(B) for each rating period during the grandfathering period and the phase down period.
We believe monitoring by both CMS and the State is necessary to ensure compliance and assess the State's progress toward the payment limit. We propose § 438.6(c)(2)(iii)(D) to require certain documentation annually in the form and manner prescribed by us for each grandfathered SDP beginning with the first rating period on or after January 1, 2027. We selected the first rating period beginning on or after January 1, 2027 as the start for our proposed documentation requirement because we believe baseline information is necessary before States would commence the required phase down beginning with the first rating period on or after January 1, 2028.
For the purposes of this required documentation, the State would need to annually monitor the total payment rate(s) for each grandfathered SDP and submit a total payment rate comparison demonstrating whether the payment limit proposed under paragraph (c)(8) has been met. For purposes of this comparison, States should calculate the total payment rate using the components defined in § 438.6(a) and compare that rate to the applicable payment limit under paragraph (c)(8). States currently perform a total payment rate comparison as part of SDP preprint submissions for approval, amendment, and renewal, using ACR as the benchmark. Under this proposal, States would instead be required to submit this comparison annually beginning with the first rating period on or after January 1, 2027, using Medicare or State plan approved rates as the point of comparison. In Table 5 of this section, we provide an illustrative example of how the total dollar amount phase down of the grandfathered total dollar amount for a Non-Expansion State might translate to the total payment rates for a Medicaid managed care program and a provider class (Provider Class A) covered under the illustrative grandfathered SDP. In this scenario, the State would reach the applicable payment limit (110 percent of the total published Medicare payment rate) by CY 2031.
( printed page 30424)
To monitor the phase down process and compliance with the payment limit, we propose § 438.6(c)(2)(iii)(D) to require that, beginning with the first rating period on or after January 1, 2027, the State submit a total payment rate comparison, certified by an actuary, for services included in the grandfathered SDP, expressed as a percentage of the most recent total published Medicare payment rate, or State plan approved rate only when no total published Medicare payment rate exists for the covered service. Under the proposed introductory text in § 438.6(c)(2)(iii)(D), this total payment rate comparison would be submitted annually in the form and manner prescribed by us. The term “Total payment rate” is defined under § 438.6(a) and lists the components for the total payment rate analysis; § 438.6(c)(2)(iii)(D) would require that the total payment rate comparison be conducted using Medicare or State plan approved rates as the point of comparison for grandfathered SDPs. This total payment rate comparison may be captured in the preprint, as currently reflected in Table 2 of the preprint.
We considered whether to mandate specific methodologies or permissible methodologies and specify data sources for the proposed total payment rate comparison under § 438.6(c)(2)(iii)(D). Based on our experience, States currently use a myriad of different methodologies when completing the total payment rate comparison currently required in § 438.6(c)(2)(iii)(B), often reflecting differences in commercial data availability. We request public comment as to whether it would be more beneficial to require that States use specific methodologies or sources of data for the total payment rate comparison. The total payment rate comparison should be developed using the same assumptions utilized for the development of the related capitation rates. For this reason, we believe it is appropriate to require that the total payment rate comparison proposed under § 438.6(c)(2)(iii)(D) be certified by an actuary.
Once the payment limit has been reached, the State would be required to comply with the proposed requirements under § 438.6(c)(1)(iii). See section II.A.3.c. of this proposed rule for discussion of our proposals regarding changes to uniform increase SDPs.
We also considered an alternative approach under which the phase down would apply to the total payment rate, rather than to the total dollar amount of the SDP. Under this alternative, the total payment rate (as a percentage of the total published Medicare payment rate) in the grandfathered SDP would be reduced by 10 percentage points each year until it reaches the applicable Medicare rate, as illustrated in the following table for a Non-Expansion State.
Because many
States include multiple services, provider classes and/or managed care programs within a single SDP, this approach would require calculating and applying the phase down separately for each provider class, service and program. We believe this would impose a significant administrative burden on States. This alternative would also significantly increase our administrative burden to review and assess compliance with the phase down process. We invite public comment on this alternative proposal and on all proposals in this section.
These proposals implement section 71116(a) and (b) of the WFTC legislation, which establishes statutory payment limits for certain SDPs and provides a temporary grandfathering period followed by a phase down of the total amount of grandfathered payments. They are also based on our authority to interpret and implement section 1903(m)(2)(A)(iii) of the Act, which requires contracts between States and MCOs to provide payment under a risk-based contract for services and associated administrative costs that are actuarially sound and our authority under section 1902(a)(4) of the Act to establish methods of administration for Medicaid that are necessary for the proper and efficient operation of the State plan. These requirements would be extended to PIHPs and PAHPs through regulations based on our authority under section 1902(a)(4) of the Act.
3. Types of Permissible SDPs and Provider Classes (§ 438.6(c)(1)(iii), (c)(2)(i), and (c)(2)(iii)(E))
a. Minimum Fee Schedule SDPs
We believe several other regulatory revisions would be needed to create guardrails to ensure that the regulations do not include weaknesses or gaps that could result in SDPs that exceed the payment limit. In the 2024 final rule, we finalized § 438.6(c)(1)(iii)(B), which allowed States to adopt a minimum fee schedule for providers that provide a particular service under the contract using a total published Medicare payment rate that was in effect no more than 3 years prior to the start of the rating period, and under which the minimum fee schedule to be used by the managed care plan is 100 percent of the total published Medicare payment rate. Through cross reference in § 438.6(c)(2)(i), States are not required to submit these SDPs to us for written prior approval via the current CMS issued preprint, but as is the case with all SDPs, these SDPs must be documented in the applicable managed care contracts and rate certifications and must comply with the requirements currently at § 438.6(c)(2)(ii).[69]
When we finalized those provisions, we relied on the rationale that allowing States to utilize a total published Medicare
( printed page 30425)
payment rate in effect no more than 3 years prior to the start of the rating period would be consistent with how § 438.5(c)(2) requires use of base data that is at least that recent for Medicaid managed care rate development. However, considering the proposed changes in this proposed rule in § 438.6(c)(2)(iii)(B)(1), we believe aligning the minimum fee schedules that States would be able to use for SDPs more closely with our proposed payment limit would be prudent to facilitate accurate implementation and validation.
We also have similar concerns with SDPs that use minimum fee schedules tied to State plan approved rates for services that have a published Medicare rate. SDPs that use minimum fee schedules tied to State plan approved rates are permitted in existing § 438.6(c)(1)(iii)(A) and do not require written prior approval, as specified in § 438.6(c)(2)(i). As discussed in section II.A.1. of this proposed rule, the new proposed payment limit for all SDPs for rating periods beginning on or after January 1, 2029 would be 100 percent of the total published Medicare payment rate for Expansion States, 110 percent of the total published Medicare payment rate for Non-Expansion States, and only when there is no total published Medicare payment rate for the Medicaid covered service, would the limit be 100 percent of State plan approved rates. We are concerned that if we continue to permit SDPs that use minimum fee schedules tied to State plan approved rates for services that have a published Medicare rate, there would be greater risk of States implementing SDPs using minimum fee schedules that could exceed the total published Medicare payment rate since States set their own State plan rates within broad Federal parameters including the requirements under section 1902(a)(30)(A) of the Act. Because such SDPs currently do not require written prior approval, we might only be able to identify if a State had exceeded, or was at risk of exceeding, the total published Medicare payment rate as part of a targeted SDP and Medicaid managed care contract audit.
To address our concerns related to minimum fee schedule SDPs and organize § 438.6(c)(1)(iii) for improved readability, we first propose to move current § 438.6(c)(1)(iii)(A) through (E) to § 438.6(c)(1)(iii)(A)(1) through (5), and to revise the introductory text in § 438.6(c)(1)(iii)(A) which would establish that the types of SDPs proposed in paragraphs (1) through (5) would be limited to rating periods beginning from July 9, 2024, but before January 1, 2028. This would limit the use of the existing minimum and maximum fee schedule arrangements in current § 438.6(c)(1)(iii)(A) through (E), as redesignated as § 438.6(c)(1)(iii)(A)(1) through (5) in this proposed rule, to rating periods beginning from July 9, 2024, but before January 1, 2028. This proposed time period would precede our proposed effective date for the applicability of the payment limit to all SDPs and States.
Next, we propose to revise § 438.6(c)(1)(iii)(B) to add introductory text that would specify the applicability date as beginning with the first rating period on or after January 1, 2028 for the proposed payment arrangements at § 438.6(c)(1)(iii)(B)(1) through (2). Since we are proposing these changes to ensure that States would not exceed the payment limit, we believe it would be reasonable that our proposed revisions to the types of allowable fee schedules would precede the proposed applicability date for the payment limit to all SDPs outlined in section II.A.1. of this proposed rule.
In lieu of listing the three types of minimum fee schedules currently permitted at § 438.6(c)(1)(iii)(A) through (C) separately, we propose to combine them into one type and revise the wording in § 438.6(c)(1)(iii)(B)(1) for improved readability and clarity. Specifically, we propose in § 438.6(c)(1)(iii)(B)(1) that States would be permitted to direct managed care plans to adopt a minimum fee schedule for providers that provide a particular service under the contract and that minimum fee schedule is no greater than the payment limit. This would provide States the flexibility to direct managed care plans to implement an SDP using a minimum fee schedule up to the proposed payment limit. Under our proposal, States would also have flexibility to design their own fee schedules for services that have a published Medicare rate as is permitted under current § 438.6(c)(1)(iii)(C), as long as that fee schedule on a per service basis would not exceed the applicable payment limit. Since our proposed revisions in § 438.6(c)(1)(iii)(B)(1) would explicitly prohibit fee schedules selected for SDPs that use a minimum fee schedule from exceeding the proposed payment limit, we believe this would substantially reduce the risk that States would breach the payment limit. Therefore, we believe it would be appropriate not to require written prior approval by CMS for such SDPs using minimum fee schedules, consistent with the current treatment of SDPs specified under § 438.6(c)(1)(iii)(A) through (B). We again remind States that SDPs that do not require written prior approval must still be documented in the relevant Medicaid managed care contracts and rate certifications, comply with the requirements at § 438.6(c)(2)(ii), and comply with all applicable Federal requirements.
b. Maximum Fee Schedule SDPs
Section 438.6(c)(1)(iii)(E) permits States to direct managed care plans to implement maximum fee schedules for providers so long as the plan retains the ability to reasonably manage risk and has discretion in accomplishing the goals of the contract. We believe that maximum fee schedule SDPs still represent an important tool that States may use to control Medicaid managed care expenditures for providers. We propose to revise the existing language in § 438.6(c)(1)(iii)(E) and move to newly proposed § 438.6(c)(1)(iii)(B)(2). Proposed § 438.6(c)(1)(iii)(B)(2) would allow States to require managed care plans to adopt a maximum fee schedule for providers that provide a particular service under the contract and the maximum fee schedule would be no greater than the payment limit, so long as the MCO, PIHP, or PAHP retains the ability to reasonably manage risk and has discretion in accomplishing the goals of the contract. Retaining the phrase beginning with “so long” is important to ensure that a State would not direct a managed care plan to adopt a maximum fee schedule that is so low it could jeopardize the basic tenets of a risk-based managed care delivery system by preventing the development of adequate provider networks. As noted earlier, we propose to revise § 438.6(c)(1)(iii)(B) to add introductory text that would permit the payment arrangements proposed at § 438.6(c)(1)(iii)(B)(1) through (2) applicable beginning with the first rating period on or after January 1, 2029. To ensure that States do not exceed the proposed payment limit for SDPs that use a maximum fee schedule, we propose that § 438.6(c)(1)(iii)(B) would be applicable for rating periods beginning on or after January 1, 2029, to align with the applicability of the payment limit to all SDPs (see section II.A.1. of this proposed rule).
c. Uniform Increase SDPs
We are increasingly concerned that States are inappropriately using SDPs that require managed care plans to pay “uniform increases,” as permitted in existing § 438.6(c)(1)(iii)(D), and that make a tenuous or overly broad connection between the SDP and what is actually needed to advance the goals and objectives in the State's Medicaid
( printed page 30426)
managed care quality strategy as required under § 438.6(c)(2)(ii)(C). Uniform increases are the most common type of SDP, and in our experience reviewing SDPs, are increasingly designed to ensure that managed care plans expend a specific amount on payments to a provider class and that providers receive that specific aggregate amount. States almost exclusively fund uniform dollar or percentage increase SDPs with IGTs or provider taxes and then design the SDP in such a way that the uniform increase will change depending on utilization during the rating period to ensure that the entire funding amount collected from the IGT or tax, plus at least a portion of the Federal matching funds are expended via the SDP. In our years reviewing and approving SDPs, we have seen States amend an SDP to direct a higher dollar increase when utilization is lower than projected, effectively, retrospectively rewarding providers with higher payments on a per-service basis for furnishing fewer services to Medicaid beneficiaries.
To illustrate how States may structure these arrangements, consider an example drawn from our experience reviewing uniform increase SDPs. In this scenario, a State receives a total of $10 million in IGTs from two AMCs ($5 million each) to fund the State's share of the SDP. Applying the minimum 50 percent Federal match rate, the State uses the $10 million IGT as the non-Federal share for the SDP and obtains $10 million in Federal matching funds, bringing the combined total available for the SDP to $20 million. With the $20 million in hand, the State designs an SDP totaling $20 million benefiting a provider class comprised of the two IGT-contributing AMCs so that they are the only entities receiving SDP dollars. The State then determines a uniform dollar amount to be added to each claim payment by dividing the total available dollar amount ($20 million total computable) by the projected number of visits that Medicaid enrollees in managed care plans are expected to make to the two AMCs during the rating period. Throughout the rating period, the State actively monitors actual utilization against those projections. Should the total number of Medicaid enrollee visits to the two AMCs fall below the original estimate, the State adjusts the uniform dollar amount upward. This ensures that both AMCs ultimately receive their full expected share—$10 million each—through claims payments for services rendered during the rating period, regardless of fluctuations in patient volume. In this example, the State contributes no non-IGT funds to the SDP other than those provided by the AMCs. As a result, the AMCs net $10 million in SDP payments that are effectively financed through Federal matching funds.
It is difficult to see how structuring a SDP in this manner furthers the specific goals and objectives in the State's Medicaid managed care quality strategy, and it appears, based on our review of these arrangements, that they operate primarily as a financing mechanism that spares State budgets and rewards providers that are positioned to participate in IGTs or that bear higher tax burdens. (See section II.B. of this proposed rule for discussion on SDPs and the source of non-Federal financing.) While these sources of the non-Federal share generally can be permissible, we do not believe that SDPs should be designed solely with the intent of ensuring that an entire pool of Medicaid payments is returned to certain providers that have been able to supply the non-Federal share of those payments. These types of scenarios also raise concerns about potential compliance issues with section 1903(w) of the Act and are not aligned with the prospective, risk-based nature of Medicaid managed care. Ideally, the State would instead direct plans to pay a prospectively established uniform increase that the State has carefully analyzed and determined is necessary to increase provider payments above the negotiated provider payment rates to effectuate improvement in quality and/or access to care. Total aggregate provider payments would then vary depending on actual utilization during the applicable rating period.
SDPs were created to give States flexibility to pursue provider payment initiatives and delivery system reform efforts that further advance access to care, enhance quality of care in Medicaid managed care, and to help reach the goals they defined in their quality strategy. In explaining why we created SDPs as a payment mechanism in the 2016 final rule, we noted the Federal and State interest in strengthening delivery systems to improve access, quality, and efficiency throughout the health care system and in the Medicaid program (81 FR 27582). For uniform increase SDPs, we believed they would be used to help ensure that additional funding was directed toward a class of providers to enhance services and ensure access, rather than benefiting only particular providers (81 FR 27583). However, in recent years, we have observed a trend in which States revise the amount of the uniform increase to adjust for lower-than-expected utilization simply to expend the full amount collected to a few specific providers. This trend leaves us concerned that these payments are not, in practice, being used to enhance services and ensure access for Medicaid beneficiaries, but rather to reward providers based on their ability to provide non-Federal share.
As we have seen the trend of repayment to specific providers increasing among States, we believe we need to address this issue in this proposed rule. This is consistent with the Presidential Memorandum, which highlighted that when States use financing arrangements in which funds collected from providers are returned to those same providers through Medicaid payments, the State lacks an incentive to be prudent in the amount of payment provided.
States' use of uniform increase SDPs has increased over time. Prior to the 2024 final rule, States were designing SDPs that sought to require managed care plans to pay providers in ways that resulted in specific, predetermined total aggregate payments. At times, these were characterized as either minimum fee schedules or, more frequently, as uniform increase SDPs. These uniform increase SDPs utilized uniform methodologies in which States were not directing a specific dollar amount or a specific percentage increase, but rather directing the use of a consistent methodology that would result in a specific aggregate pool amount paid per provider, again usually commensurate with the provider's contributions to the non-Federal share financing the SDPs. In our reviews of these submissions, these uniform increase SDPs appeared, at first, to look similar to UPL methodologies approved in Medicaid State plans—intended to bring total aggregate payments up to what Medicare was projected to have paid across a class of providers. But over time, States started to take this further and design uniform increase SDPs using uniform methodologies in more complex arrangements.
We sought to clarify the original intent of permitting States to implement uniform increase SDPs in the 2024 final rule by defining “uniform increase” at § 438.6(a) as any SDP that directs the managed care plan to pay the same amount (the same dollar amount or the same percentage increase) per Medicaid covered service(s) in addition to the rates the managed care plan negotiated with the providers included in the specified provider class for the service(s) identified in the SDP. We also adopted definitions for other types of SDPs, including minimum fee schedules
( printed page 30427)
and maximum fee schedule. Since adopting the definition for “uniform increase,” we have grown increasingly concerned with States' inability to prospectively establish a specific uniform dollar or percentage increase. We now routinely require States to document the specific uniform increase per provider class in the preprint. Our operational experience indicates that many SDPs prior to the 2024 final rule used uniform increase methodologies that were intended to provide the difference between the base payment rate received by providers from managed care plans and a specific amount, such as the Medicare rate or the ACR. In such instances, there is no uniform dollar or percentage increase paid uniformly across the State's originally defined provider class. Instead, the amount of the SDP can vary among providers due to the base rates negotiated by the managed care plans varying among providers. While such States could choose to revise their SDPs to adopt a minimum fee schedule tied to the Medicare rate, some States have instead elected to maintain a uniform increase methodology, determine all the different increase amounts by provider, and then revise their SDP to further subdivide the original provider class(es) to ensure the desired results of ensuring specific providers or provider classes receive a pre-determined pool of funding, regardless of actual utilization and services delivered during the applicable rating period. To effectuate changes to the uniform methodology to ensure the full pool is paid out, States will often submit SDP amendments after the end of the rating period when utilization is known. Such complex SDPs make monitoring exceptionally challenging and increase the possibility of fraud, waste and abuse.
Finally, uniform increases also raise concerns with ensuring compliance with the new proposed payment limit, which we have proposed would apply to each service rendered by a provider receiving payment that includes an SDP. Uniform increases, by definition, are uniform dollar or percentages paid
in addition to the rates the plan negotiated
with the providers included in the specified provider class. While States may be able to estimate current provider payment rates by analyzing historical encounter data submitted by managed care plans, States are often not privy to the rates that managed care plans negotiate with providers prospectively. If managed care plans and providers negotiate a rate that varies significantly from historical rates, States could unintentionally require managed care plans to pay uniform increases that would result in total payment rates that exceed the payment limit on a per service basis. We believe that States could reasonably achieve their program goals using SDPs requiring minimum and/or maximum fee schedules that do not exceed the proposed payment limit. As an example, a State that wished to improve access to care and prohibit potentially wasteful spending for durable medical equipment could establish minimum and maximum fee schedules at exactly the payment limit which would require managed care plans to pay the exact payment limit. This approach would avoid the risk that a uniform increase applied to an unknown negotiated rate could exceed the payment limit. It would also remove the incentive for States to structure uniform increase SDPs so that a predetermined aggregate amount of Medicaid payments is provided to certain providers over the course of the rating period. Therefore, we propose that beginning with the first rating period on or after January 1, 2028, new uniform increase type SDPs and renewals of non-grandfathered uniform increase type SDPs would no longer be permitted. We reflect this in proposed § 438.6(c)(1)(iii)(B) for rating periods beginning on or after January 1, 2028 by only specifying minimum and maximum fee schedule SDPs as options. Additionally, we propose to update cross-references to § 438.6(c)(1) that are included in § 438.6(c)(3)(ii) and (c)(5)(iii) for accuracy to address the proposed changes to § 438.6(c)(1) noted throughout section II.A.3. of this proposed rule. We believe this would be sufficient time for States to redesign SDPs and to account for the SDPs in their managed care contracts and rate certifications; the vast majority of SDPs are submitted on an annual basis and States regularly revise their SDPs from year to year.
Together, the temporary grandfathering framework and the proposed applicability date are intended to provide States sufficient time to transition away from uniform increase SDPs, including redesigning SDPs, amending managed care contracts, and adjusting associated financing arrangements. We recognize that some States may have structured SDPs and associated financing arrangements in reliance on prior policy permitting uniform increase SDPs; however, we believe the proposed applicability date provides sufficient time for States to redesign SDPs, amend contracts, and adjust associated financing mechanisms as needed. We are always available for technical assistance, should States need additional guidance on permissible SDP designs, managed care contracts or rate certifications.
We believe a limited exception to this prohibition is warranted for grandfathered SDPs, only during the temporary grandfathering period, as many of the grandfathered SDPs are uniform increase SDPs approved as permitted in § 438.6(c)(1)(iii)(D). In section II.A.2. of this proposed rule, we describe our proposals for grandfathered SDPs and our proposed interpretation of the grandfathered total dollar amount. For SDPs designated as grandfathered, which would be limited to the approved total dollar amount of the grandfathered SDP until the first rating period beginning on or after January 1, 2028, we believe that States would need to retain some flexibility to redesign their grandfathered SDPs and to adjust their uniform increases to different provider classes to ensure that the total dollar amount of a subsequent renewal of a grandfathered SDP is not exceeded. To permit uniform increase SDPs only for grandfathered SDPs and only until the first rating period in which the payment limit is reached for the grandfathered SDP, we propose to add § 438.6(c)(2)(iii)(E). We also propose in § 438.6(c)(2)(iii)(E) to clearly require that once the payment limit is met, the State must comply with paragraph (c)(1)(iii) of this section. In practice this would mean that a State with a grandfathered SDP at the payment limit would be required to modify their SDP design to comply with the requirements for types of SDPs under paragraph (c)(1)(iii); the State would no longer be permitted to operationalize the SDP as a uniform increase.
We seek public comments on all of our proposals.
d. Grey Area Payments and Other Prohibited Practices
Under § 438.6(c)(1), States are not permitted to direct in any way the expenditures of a Medicaid managed care plan under the contract between the State and the plan except when the direction is: (1) an SDP that complies with § 438.6(c); (2) permissible under a specific Federal legal authority under Title XIX of the Act and its implementing regulation related to payments to providers and applicable to managed care; or (3) a permissible pass-through payment that meets requirements in § 438.6(d). States are also not permitted to make payments directly to providers for services covered under the contract between the State and a managed care plan as specified in § 438.60.
( printed page 30428)
As States consider the SDP proposals outlined in this rule, we are concerned that some States may attempt to circumvent the proposed or existing requirements by including general or vague contract requirements for provider payment, known as “grey area payments”, which are not subject to approval as an SDP under § 438.6(c) nor as a pass-through payment under § 438.6(d). As we explained in the 2023 proposed rule (88 FR 28112 through 28113) and 2024 final rule (89 FR 41044), building on prior guidance including the November 2017 CMCS Informational Bulletin and SMDL #21-001, these types of arrangements took advantage of an unintended loophole in regulatory oversight and are not permissible since any direction of payment must comply with § 438.6(c) or (d), or be permissible under a specific Federal legal authority under Title XIX of the Act and its implementing regulation. We have worked diligently since the 2024 final rule (89 FR 41045) to ensure that any of these types of payment arrangements were eliminated, and we want to be clear in this proposed rule that grey area payments remain impermissible.
As States consider the proposals under this rule and how best to ensure compliance with applicable regulations, we remind States that absent the exceptions in § 438.6(c)(1), States may not in any way direct managed care plan expenditures under the contract (see 89 FR 41083 through 41085 for further details). States should not implement any payment arrangements that could be considered grey area payments nor submit SDP preprints that do not comply with SDP requirements. To aid States in their planning and development of future SDPs, we describe several new scenarios that are generally impermissible or would either be considered grey area payments or unallowable practices, and therefore not eligible for approval under § 438.6(c).
To explain our concerns, we offer a few examples. First, we want to address limitations related to incentive arrangements and withhold arrangements, as we have received questions from States indicating confusion about how SDPs may interact with these arrangements. Some States seem to conflate incentive and withhold arrangements with SDPs while other States appear to be calling certain practices incentive and withhold arrangements to direct provider payments outside the requirements of § 438.6(c). States are permitted under § 438.6(b)(2) and (3) to implement a managed care plan level incentive arrangement or withhold arrangement provided the State complies with all Federal regulatory requirements, including establishing the specified activities, targets, performance measures or quality-based outcomes that are necessary for the plan to receive payment under the arrangement. However, incentive arrangements and withhold arrangements specified at § 438.6(b) are payments only to managed care plans and cannot be used as substitutes for SDPs, which are payments to providers. States are not permitted to direct a managed care plan's expenditures under the terms of an incentive arrangement or withhold arrangement by requiring some or all of the funding in the incentive or withhold arrangement to be paid to providers. Such direction constitutes impermissible State direction of plan expenditures unless it complies with § 438.6(c) or (d). Second, we have encountered documentation in managed care contracts between States and plans that requires actuaries to develop the associated capitation rates using certain assumptions about provider payment rates. In one instance, a State included a contractual requirement that the actuaries develop the capitation rates using a maximum payment rate for a certain type of provider. In another instance, the State legislature appropriated a certain amount of funding for enhanced provider payment rates and the State required the actuaries to include that appropriation as an assumption for increased provider payment rates for rate development. Both of these scenarios constitute SDPs because the State is directing assumptions about provider payment levels through rate development assumptions. Further, both of these scenarios involve rate setting practices that are not based on historical experience or actual plan-level obligations under the managed care contract. In these instances, the State must comply with the regulatory requirements under § 438.6(c). The State must also submit a preprint for written prior approval by us, as applicable under § 438.6(c)(2)(i). When such contractual requirements are not subject to prior written approval under § 438.6(c)(2)(i), they must still comply with other applicable requirements under § 438.6(c) because they constitute SDPs.
Finally, we have become aware of instances in which States are attempting to direct managed care plans, including by imposing requirements on providers through plan contract provisions or SDP conditions, to pay a portion of SDP expenditures to specific entities for activities not based on the utilization and delivery of services, as required under § 438.6(c)(2)(ii)(A). These entities have included private consultants and provider associations. Such arrangements are typically implemented through the State's managed care plan contracts or through the SDP preprint where the State requires the third-party arrangement as part of the eligibility criteria for an SDP provider class. In one example, a State requires that providers under an SDP pay a portion of received SDP reimbursement to a specific entity chosen by the State to collect provider taxes as well as process, redistribute, and track the SDP payments made to providers. As another example, a State requires that a portion of the SDP be allocated to pay the managed care plan for its administrative activities related to the SDP.
These practices are either impermissible or, when an SDP is involved, not consistent with the intent of SDPs to improve access to or quality of care for Medicaid beneficiaries. SDPs must comply with the requirements in § 438.6(c)(2)(ii), including that payments must be based on the utilization and delivery of services, advance the goals and objectives of the State's quality strategy, and result in achievement of the stated goals and objectives in alignment with the State's SDP evaluation plan. SDP arrangements under § 438.6(c)(1)(i) through (iii) permit States to direct managed care plan expenditures to providers that furnish a particular service under the contract and are not intended to be utilized to direct expenditures to entities other than the furnishing provider. Section 438.6(c)(1) does not permit States to direct distribution of SDP funds to a third-party entity and any such State direction to a managed care plan or provider is impermissible. Further, we are concerned that these arrangements could be designed to circumvent requirements on financing of the non-Federal share, rather than advancing access to or quality of care for Medicaid beneficiaries. Such arrangements are typically implemented through State direction to managed care plans, including requirements incorporated into plan contracts or SDP conditions that are imposed on participating providers.
It is impermissible for a State to require that a portion of the SDP payments be allocated to the managed care plan for administrative activities associated with the SDP, as capitation rates already include a non-benefit component to cover reasonable administrative costs, consistent with § 438.5(e).
( printed page 30429)
We reiterate States are not permitted to direct managed care plans and/or providers to pay a portion of SDP expenditures to entities for activities not based on the utilization and delivery of services to Medicaid managed care beneficiaries. Such arrangements are not consistent with § 438.6(c) and will not be approved. We also reiterate grey area payments are not permissible and we will not approve managed care contracts or SDPs that contain this type of provision. To clarify this requirement, we propose to clarify and affirm these longstanding requirements by revising § 438.6(c)(2)(ii)(A) to specify that SDPs must be based only on the utilization and delivery of services furnished by a provider. States cannot condition provider participation in an SDP on paying any portion of an SDP to an entity other than the furnishing provider. We consider this proposal a clarification of longstanding SDP requirements.
e. Provider Classes
One of the standards for all SDPs in § 438.6(c)(2)(ii)(B) is that a State must direct expenditures equally and using the same terms of performance for a class of providers (hereafter referred to as a “provider class”) providing the service under the contract. This means that when a State defines an eligible provider class under an SDP, all providers within that provider class must be treated equally with regard to payment and performance under the SDP. For example, if a State established two eligible provider classes under a minimum fee schedule type SDP, it would need to ensure that the specific minimum fee schedule that the managed care plan is directed to pay is the same for each provider included in a specified provider class. As an illustrative example, if a State directs their managed care plans to pay two classes of dental providers, such as urban and rural, a minimum fee schedule for certain dental services, the State might direct that each provider in Provider Class A (urban dental provider) would receive a minimum payment of $100 for a pediatric dental cleaning, while each provider in Provider Class B (rural dental provider) would receive a minimum payment of $200 for a pediatric dental cleaning.
Another current SDP standard in § 438.6(c)(2)(ii)(I) is that the State must provide documentation demonstrating the total payment rate for each service and provider class. This ties the State's defined provider classes to the total payment rate comparison that we request for all SDPs that require written prior approval. The documentation demonstrating the total payment rate, as defined in § 438.6(a), is completed for each specified provider class for each service type covered in the SDP. In current § 438.6(c)(2)(iii), we further require that the total payment rate for each SDP for the four services (inpatient hospital services, outpatient hospital services, qualified practitioner services at AMCs and nursing facility services) not exceed the ACR, meaning that payment under an SDP for each provider class and service type for a managed care program could not exceed ACR. In practice, we have observed that some States define provider classes in ways that result in maximizing the total payment rate received by each provider in a provider class under an SDP while remaining below or at the ACR. In some instances, States have submitted individual preprints [70]
with the provider class so narrowly defined that the SDP applies to a single provider. We have observed that these arrangements are often associated with the source of the non-Federal share of payments, and in nearly all such cases, the SDP is financed through an IGT.
We have historically granted States significant latitude in how they define a class of providers and noted this in both the May 2020 CIB:
Medicaid Managed Care Options in Responding to COVID-19[71]
and January 2021 SMDL #21-001:
Additional Guidance on State Directed Payments in Medicaid Managed Care.[72]
In the 2024 final rule, we affirmed this flexibility and finalized several regulatory revisions that permitted States to include non-network providers as provider classes too (89 FR 41050). We thought that this flexibility with the provider class definition was necessary for States to be able to achieve their stated policy goals tied to their managed care quality strategy. For example, we have approved SDPs where States proposed and implemented SDPs that applied to provider classes defined by criteria such as participation in State health information systems. In other SDPs, the eligible provider class was established by participation in learning collaboratives that focused on best practices for quality improvement or data collection and reporting.
At § 438.6(c)(2)(ii)(B), States are required to direct expenditures equally, using the same terms of performance, for a
class
of providers furnishing services under the contract; however, they are not required to direct expenditures equally using the same terms of performance for
all providers
providing services under the contract (89 FR 41057). However, in our experience since the 2024 final rule, we have witnessed States increasingly designing SDPs with provider classes defined so narrowly that they appear to be correlated with the source of non-Federal share financing or to achieve other policy goals and objectives that may be less germane to the goals and objectives of their Medicaid managed care quality strategy. In one instance, a State designed an SDP that established multiple hospital provider classes with differing uniform increase amounts for those provider classes depending on whether the hospitals had committed to a certain medical debt policy. Another State submitted 16 single hospital provider class SDP preprints. In these instances, defining a provider class to include a single provider may effectively operate as a provider-specific payment arrangement, ensuring that a particular provider receives a specified aggregate payment amount, often tied to the source of the non-Federal share of financing, rather than advancing common performance objectives or the goals and objectives of the State's managed care quality strategy under § 438.6(c)(2)(ii)(C). These provider classes may only be tenuously connected, if at all, to specific elements in the State's managed care strategy. We recognize why States design such policies and are concerned that SDPs designed with goals and objectives outside of the managed care quality strategy may not meet the existing standard in § 438.6(c)(2)(ii)(C).
We have concerns that SDPs with these types of provider classes may increase Medicaid expenditures without commensurate improvements in access to or quality of care furnished to the Medicaid managed care population. To better understand whether additional guardrails may be warranted to safeguard the fiscal integrity of the Medicaid program and ensure that SDPs are used consistent with applicable program requirements, we are soliciting comment on whether and how to define “provider class” at § 438.6(a). We are not proposing to define “provider class” in this rule. However, one option that we have considered is defining provider class to mean a group of providers as defined in the approved Medicaid State plan. Aligning each provider class defined in an SDP with a group of providers defined in the Medicaid State
( printed page 30430)
plan may, in some instances, better ensure that States are designing SDPs and specifying provider classes that are aligned with the needs of their Medicaid programs and advance the goals and objectives of the managed care quality strategy. For example, a State could define a provider class by reference to an existing State plan provider grouping or service category, such as institutional providers or nursing facilities, as specified in the approved State plan. Because State plan amendments undergo rigorous review processes by us, we believe this proposal could also limit the use of provider class definitions that functionally restrict a class to a single provider or a very small number of providers for purposes unrelated to advancing access to care, enhancing quality of care in Medicaid managed care, and the specific goals and objectives of the managed care quality strategy.
We have also considered alternative approaches under which the criteria for defining the provider class for an SDP would be required to be directly tied to the goals and objectives of the State's Medicaid managed care quality strategy and to be specific to the services and enrollees to which the SDP applies. This alternative could further reinforce the requirement that SDPs advance the goals and objectives in the State's managed care quality strategy as required under § 438.6(c)(2)(ii)(C). We are exploring whether this approach could help ensure that SDP investments are more directly targeted to the needs and priorities of the Medicaid managed care population, rather than reflecting factors not directly tied to Medicaid managed care delivery, such as correlation with the source of non-Federal share financing, or other State policy considerations, including but not limited to rewarding particular provider policies concerning medical debt or uncompensated care. We are also evaluating whether this approach could be overly broad or insufficient to address our concerns described previously in this section.
We solicit comments on these possible approaches to defining “provider class”, including the advantages and disadvantages of each approach, as well as alternative definitions or factors we should consider. We emphasize that we are not proposing a definition of the term “provider class” in this rule; rather, we are seeking input to inform future notice-and-comment rulemaking. Nothing in this discussion limits CMS's authority to request additional information from States regarding provider classes identified in SDP preprints as part of our review of SDPs under § 438.6(c)(2)(i).
f. Written Prior Approval
To specify which SDPs would and would not require written prior approval by us under our proposals, we propose to revise § 438.6(c)(2)(i) to specify that States would need to submit preprints to us for SDPs described in paragraphs (c)(1)(i) and (ii) and (c)(1)(iii)(A)(3) through (5) of this section. As discussed in sections II.A.3.a and b of this proposed rule, beginning with the first rating period on or after January 1, 2028, States would no longer be required to submit permissible minimum fee schedule or maximum fee schedule preprints to us for written prior approval. We could continue to obtain documentation from States as required under proposed § 438.6(c)(8)(i)(B) and, beginning with the first rating period on or after January 1, 2029, under proposed § 438.6(c)(8)(iii)(C). We remind States that SDPs that do not require prior approval must comply with the requirements at § 438.6(c)(2)(ii) and be appropriately documented in the managed care contract(s) and rate certification(s).
These proposals are based on our authority to interpret and implement section 1903(m)(2)(A)(iii) of the Act, which requires contracts between States and MCOs to provide payment under a risk-based contract for services and associated administrative costs that are actuarially sound and our authority under section 1902(a)(4) of the Act to establish methods of administration for Medicaid that are necessary for the proper and efficient operation of the State plan, and is extended to PIHPs and PAHPs through regulations based on our authority under section 1902(a)(4) of the Act. Our proposed changes to the types of permissible SDPs are necessary for proper and efficient operation of the State plan and to reduce the inefficient and improper operation of SDPs that increase the risk of fraud, waste, and abuse.
We seek public comments on all our proposals.
4. Applicability Dates (§ 438.6(c)(10))
Throughout the other sections of this proposed rule we have stated when our proposal would include a specific applicability date. As noted in section II.A.1. of this proposed rule, we revised § 438.6(c)(8), the existing applicability section, as § 438.6(c)(10). We also propose to redesignate § 438.6(c)(8)(i) through (vii) as § 438.6(c)(10)(i) through (vii). We propose to amend § 438.6(c)(8)(i) as § 438.6(c)(10)(i) and to clarify that the listed provisions apply as adopted in the July 9, 2024 final rule, beginning July 9, 2024, and to distinguish those provisions from amendments proposed in this rule. To effectuate the proposed revised definition of “State plan approved rates” in paragraph § 438.6(a), we propose to move § 438.6(c)(8)(vii) to § 438.6(c)(10)(vii) and revise to specify that the definition of: “State plan approved rates” in paragraph (a), as proposed in this rule applies no later than the first rating period for contracts with MCOs, PIHPs, and PAHPs beginning on or after January 1, 2028.
We solicit public comments on these proposals.
B. Targeted Medicaid Payment Limit in an FFS Delivery System (§ 447.381)
In the absence of existing regulatory standards that establish UPLs for practitioner services, we have generally allowed States to make Medicaid supplemental payments for practitioner services up to Medicare payment amounts or the ACR, provided the proposed payment methodology meets applicable Federal requirements. Unlike other supplemental payments subject to UPLs, some practitioner supplemental payments have resulted in payment amounts that far exceed a reasonable estimate of what Medicare would have paid for the services furnished, as the relevant ACRs generally are higher than Medicare rates. This result is possible because, other than economy and efficiency requirements at section 1902(a)(30)(A) of the Act, there currently is no Federal UPL requirement applicable to payments for practitioner services (as well as certain provider services).
When ACR-based FFS supplemental payments were first approved by us in the early 2000s, States initially proposed using the Medicare equivalent of the ACR. We found that State ACR calculations were between 135 percent and 165 percent of the Medicare rates for the same services. For example, one early SPA payment methodology from a State in 2012 within that range reflected a Medicare equivalent of the ACR payment at 143 percent of Medicare rates and estimated a Federal fiscal impact of $11 million in FFY 2012 for certain physician payments. The State subsequently expanded ACR-based payments to physicians affiliated with children's hospitals, physicians at general acute care non-State government-owned hospitals, and physicians affiliated with certain medical centers. By 2023, the State had increased the payment to 238 percent of Medicare rates, which continued to be
( printed page 30431)
below the ACR according to the State's ACR demonstration submitted to us to support the payment.
The source of the non-Federal share plays an important role in our concerns regarding ACR-based FFS payments. In our experience, ACR-based payments can be funded by IGTs derived from State or local government funds, including revenues provided by State university teaching hospitals, and are generally made exclusively to providers that have the ability to fund the non-Federal share of the ACR payments. Based on our review of State submissions, some of these ACR-based payments often appear to be made without clear consideration of any benefit to the Medicaid program, such as improvements in access to, or quality of, care for beneficiaries. For example, under the ACR methodology, a State could calculate supplemental payments totaling $20 million to physicians at the only State university teaching hospital. Assuming a Federal medical assistance percentage of 50 percent, this hospital, as a unit of government, could make an IGT of $10 million to the State Medicaid Agency and receive a $20 million payment, with the State obtaining Federal matching funds of $10 million. Because the State Medicaid Agency targeted the total payment amount to physicians affiliated with State university teaching hospitals and there is only one such hospital in the State, the State contributes no funds to the payment other than those provided by the hospital itself. As a result, the provider nets a $10 million payment that is entirely funded by the Federal government and taxpayers. In instances where providers fund the non-Federal share of their own payment, the Federal government contributes its share while State Medicaid Agencies may have no budgetary stake in ensuring an appropriate Medicaid payment level. While this structure may be permissible under current rules, it can reduce State incentives to ensure that rates are economic and efficient, while remaining sufficient to ensure quality and access. As States and practitioners realized that Medicaid payments could be increased using ACR-based payment methodologies with funding through IGTs provided by the same providers receiving the payments, we began to receive an increasing number of proposals expanding these ACR-based payments to other Medicaid-participating practitioners, increasing the risk to the Federal treasury and the fiscal integrity of the Medicaid program.
States have increasingly proposed paying up to the ACR to certain practitioners and providers that are willing and able to provide the non-Federal share, resulting in some States seeking approval from us to make Medicaid practitioner payments up to 530 percent of the Medicare rate for physicians. Currently approved payments average 207 percent of the Medicare rate for States using the Medicare equivalent of the ACR for physicians and 153 percent for other licensed practitioners (for example, dentists and GEMT providers). While these percentages account for outliers among States making ACR payments, the resulting payments are considerably larger than we have seen historically and with no discernable improvements in Medicaid access, quality of care, or other relevant programmatic metrics. In FFY 2024, the most recent full FY for which data were reported in the Form CMS-64 (the quarterly Medicaid statement of expenditures), States claimed approximately $2.64 billion (total computable) in expenditures for supplemental payments (including ACR-based payments, but excluding DSH and any UPL payments) made to physicians, other licensed practitioners, and ground emergency medical transportation providers.[73]
The growth in ACR as a percentage of Medicare has raised concerns over whether these payment levels remain economical and efficient. One recent State proposal, for example, reflected a Medicare equivalent of 530 percent of Medicare rates. The substantial increase in both the percentage above Medicare and the number of proposals submitted by States has caused us to reevaluate the ACR as a benchmark for meeting the statutory requirement that Medicaid payments be economical and efficient, and to question whether the demonstrations submitted by States to CMS are truly representative of the amounts commercial payers pay for Medicaid-covered services. These concerns are exacerbated by our limited ability to verify the commercial payer data underlying ACR demonstrations, which are based on proprietary data that we cannot independently audit. Nevertheless, absent additional information indicating that the payment methods were not economical or efficient, we have continued to approve ACR methodologies submitted by States based on our historical practice and because we had not established a Medicare-based upper limit for practitioner supplemental payments in regulation, as we have for certain other categories of FFS supplemental payments.
In FFY 2024, 24 States paid $1.6 billion (total computable) in ACR supplemental payments to 1,975 physicians or physician practices. The largest FFS ACR supplemental payment amount was $277.5 million, targeted to 21 physicians/practices (where a practice may include multiple physicians), resulting in a per-physician/practice payment that exceeds $13 million, the highest per physician/practice ACR supplemental payment amount among all States. The smallest amount was $969,190, targeted to 12 physicians/practices ($80,765 per physician/practice). The number of physicians/practices targeted by States ranged from two physicians/practices to 448 physicians/practices. Totals for ACR supplemental payments for which we have provider-level data also include other licensed practitioners and NEMT. For other licensed practitioners, 16 States paid almost $950 million (total computable) in ACR supplemental payments to 5,384 providers with one State making almost $500 million in supplemental payments targeted to 416 other licensed practitioners such as dentists and GEMT providers (for example, a county fire department), or about $1.2 million per other licensed practitioner. For NEMT, two States paid almost $80 million (total computable) in supplemental payments to 256 providers, with the largest supplemental payment amount of $58.2 million targeted to 144 NEMT providers (about $404,166 per provider).
In this proposed rule, we are proposing new limits on targeted payments that currently are limited to the ACR. Based on our review of State SPAs over the last two decades, as well as and State supplemental payment expenditure data reported on the CMS-64, we have become increasingly concerned that these targeted payments, made to a small number of practitioners or providers (relative to all practitioners or providers enrolled in all State Medicaid programs), may not be economical and efficient, as required by section 1902(a)(30)(A) of the Act. Moreover, we have not identified information indicating that these payments broadly improve access to care, quality, or other relevant programmatic outcomes, as they are typically targeted only to providers, or practitioners employed by or affiliated
( printed page 30432)
with such providers, that have the means and ability to fund the non-Federal share of the payments. Finally, as discussed in more detail later in this section, this is an opportune time to make such a change to address similar issues across managed care and FFS delivery systems, in light of the changes made to managed care payment approaches by the WFTC legislation, which limits SDPs to 100 percent or 110 percent of the specified total published Medicare payment rate, or in the absence of a specified total published Medicare payment rate, the payment rate under a Medicaid State plan (or under a waiver of such plan).
Targeted payments present clear oversight risks to Federal taxpayer dollars. First, ACR-based supplemental payments are based on proprietary commercial payment data and thus not readily verifiable or auditable. We generally are unable to validate the commercial payer data received from States or to determine whether those data have been inflated, and we have historically relied on the data submitted by States. Second, given the limits of the data we receive through State reporting on the CMS-64, which reflects aggregated payment and provider totals and does not routinely include provider-level detail, there is limited transparency regarding how many providers receive FFS ACR supplemental payments and the total amount paid to each provider. This lack of transparency further impedes our ability to assess whether such payments are economical and efficient, as required by section 1902(a)(30)(A) of the Act.
Within the FFS provisions in this proposed rule, we are proposing to establish limits on payments targeted to a subset of participating practitioners or providers, which would encompass supplemental payments that currently use an ACR methodology. Specifically, we are proposing to limit the total payment a State may make when payments are targeted to a subset of practitioners or providers, rather than to all practitioners or providers participating in the State Medicaid program. As reflected in the Background section, our current guidance regarding payments [74]
uses the term “qualified practitioner.” In this proposed rule, we are not proposing to retain that terminology for the practitioner payments discussed in the FFS provisions, nor are we proposing to adopt the definition for qualified practitioner services at an academic medical center at § 438.6(a), as we have not identified a need for additional clarity on this term. However, we want to make clear that payments previously subject to the ACR limit and discussed in the guidance on qualified practitioner payments would remain within the scope of the payments addressed in this section of the proposed rule.
Effectively, the proposed limits would apply to both the base and supplemental payments made to practitioners or providers when either or both are targeted to a subset of practitioners or providers. Targeting of base payments generally occurs when a State sets a new base rate under an alternate fee schedule for a subset of participating practitioners or providers furnishing the applicable services. This approach informs why we are proposing to place a limit on targeted payments, which, for purposes of this proposed rule, can include targeted base payments. This contrasts with an alternative approach of limiting only supplemental payments and is intended to ensure consistent application of the limit, if finalized, across differing State payment methodologies. It also avoids creating an inadvertent loophole by confining the proposed new limit to only base payments or to only supplemental payments. We want to be clear that a State cannot set targeted fee schedules, characterize them as base rates, and then assert that the proposed provisions would not apply because the proposed policies are limited to supplemental payments. In such circumstances, the State would be subject to the applicable proposed limit on the total payment made to the practitioner.
Despite an earlier reference to how SDPs should be accounted for in DSH payments, we want to clarify that DSH payments are not targeted payments within the scope of the FFS provisions of this proposed rule. DSH payments to a particular hospital are limited to that hospital's uncompensated care costs, as specified in section 1923(g) of the Act. In addition, DSH payments are not an open-ended entitlement; they are limited by annual allotments described in section 1923(f) of the Act, which serve as an additional limiting factor not present in State plan rates. In summary, we do not consider DSH payments to be targeted payments for the purposes of this rulemaking.
We also want to clarify that the limits we propose in this section would not establish another UPL akin to those that already exist in regulation or statute. These proposed limits differ in both structure and purpose. Current UPLs are applied on an aggregate basis, meaning the limit applies to the total payments made to all entities within a UPL class, such as hospitals, and are generally calculated as a reasonable estimate of the amount Medicare would pay for the specified services based on Medicare cost principles or using cost report data as the basis for the estimate that is no more than 2 years old and trended to the current payment period. By contrast, the limits we are proposing (see section II.B.3. of this proposed rule), would be specific to a practitioner or provider, for that practitioner's or provider's total payments. In addition, the practitioner or provider-specific limit would be based on actual Medicare payment rates applicable to the practitioner or provider for the same time period as the Medicaid State plan payment rate year.
The nature of the practitioner-level payment (in most instances) and services to which they apply also supports this practitioner- or provider-specific limit, rather than a class-aggregate approach used for existing UPLs. If, for example, States were required to submit physician-specific data for all physicians, as they must with respect to hospitals for inpatient hospital UPL calculations and demonstrations, this would require a tremendous amount of data and analysis for a State to produce and validate for all Medicaid-participating physicians. The service types associated with this proposed limit generally are not facility-based services and thus by their nature are more individualized, such that UPL-style aggregate payment reporting could be excessively burdensome for the State to produce and validate, and for us to review and potentially audit.
As mentioned in section II.A. of this proposed rule, inflated SDPs and supplemental payments can reward providers based on their ability to fund the non-Federal share. As such, by proposing to address these payments and set more appropriate limits, we would remove an incentivizing factor associated with certain State financing schemes. However, the effect would go beyond changing (and formalizing) the limit from ACR to Medicare. Specifically, these FFS proposals, if finalized, would establish a limit applied at the individual practitioner or provider level. If we applied this limit instead as an aggregate UPL, a State could still target a particular practitioner or provider with additional payments made available through remaining room under the aggregate UPL, which could be made possible through lower payments to other practitioners or providers. This practitioner- or provider-specific approach further dismantles a key element of the structure necessary for
( printed page 30433)
certain financing schemes to succeed in lessening a State's obligation to fund the non-Federal share.
As previously stated, the FFS provisions in this proposed rule differ from the managed care SDP provisions in how payments subject to the proposed limits are characterized. Although there are differences between the delivery systems, we aim to ensure consistency across the Medicaid program to the extent practicable. Accordingly, we are proposing to limit total FFS payments to the corresponding total Medicare payment rate for targeted Medicaid payments, which we propose to align with the Medicare-based limits in the SDP proposals to the extent practicable. Although the standard in section 1902(a)(30)(A) of the Act applies specifically to FFS payments, we believe that the Medicare payment rates provide an appropriate measure of economy and efficiency for both delivery systems, as discussed in more detail in section II.B.3. of this proposed rule. Furthermore, this alignment serves to prevent States from shifting SDPs previously approved up to the ACR into the FFS delivery system in a manner that could negate or diminish the intent of the proposed SDP limit or the changes made by Congress in section 71116 of the WFTC legislation. Notably, this proposal does not interfere with States' abilities to rely on allowable sources of non-Federal share derived from State or local units of government, such as IGTs, to make Medicaid payments. Rather, the proposal would limit the total targeted payment that a State may make. We believe these limits are necessary to ensure that the payments are economic and efficient as required by statute, and that the data used to calculate Medicaid payments is verifiable by States and CMS.
In this proposed rule, we describe the policies related to the targeted Medicaid payment limit. First, we discuss the general proposal and define the scope of the Medicaid practitioner payments subject to this policy. Next, we describe our proposal to limit the total Medicaid payment (when some or all of the payments are targeted) to the equivalent Medicare service payment rates, with the limit determined by whether the State is an Expansion State, and the requirement for this to be reflected in a State plan. Then, we describe certain exceptions to this proposed limit and the alternate procedures States must follow in those limited cases. Next, we propose a transition period for States currently making targeted payments that would not comply with the proposals in this rule, if finalized, to bring payments into conformity with the new requirements. Finally, we describe compliance actions CMS may undertake for States that continue to make payments that exceed the applicable limit.
1. General (§ 447.381(a))
We propose at § 447.381 to establish limits on payment for services when those payments are targeted to certain Medicaid practitioners or providers. Specifically, in paragraph (a), we propose that this section would establish “a Medicaid practitioner or provider-specific limit for the total Medicaid FFS payment authorized under the State plan in instances where all or a portion of such payment is targeted to a subset of participating practitioners or providers furnishing the applicable Medicaid-covered services.” In other words, a payment is considered targeted when it is not available to all practitioners or providers furnishing the same Medicaid-covered service. We discuss this in more detail later in this section.
As discussed earlier in this section of the proposed rule, the limit would be applied as a practitioner or provider-specific limit and not as an aggregate UPL. “Practitioner,” as specified in proposed paragraph (a) would include physicians, dentists and other dental practitioners, and other licensed practitioners (such as nurse practitioners). “Provider” would include providers such as GEMT providers, air ambulance providers, and NEMT providers (referred to collectively as transportation providers in this proposed rule), as well as other providers such as clinics or CCBHCs. As such, the proposed limit applies to providers that are entities, which would also include an academic medical center that is part of a hospital, as discussed in this section. As discussed in section I.E. of this proposed rule, we use practitioner in many instances to reflect the current terminology in guidance for FFS payments made up to ACR, but have endeavored to reference providers as needed to ensure the scope of this proposed rule is clear.
States target these practitioners or providers most commonly for ACR-based payments. However, States could potentially target an ACR-based payment to any practitioner or provider type delivering Medicaid services under the State plan; and therefore, we are not specifying an exhaustive list of the existing practitioners or providers to whom payments subject to the limit in regulation could be targeted. If our proposal was overly restrictive on practitioner or provider type, it could result in a situation where unrestricted use of targeted payments continued for other practitioner or provider types, particularly if and when new types begin to participate in the Medicaid program, which could then require further rulemaking to update the regulation if this proposal and an eventual final rule prescribed an exclusive list.
Payments that would be subject to these provisions are primarily practitioner payments, although some provider payments would also fall within the scope of this proposed limit. In instances where a State targets a payment to certain practitioners (for example, peer support specialists, physicians, and dentists) the proposed limit in this rule would apply. We also use the term provider to ensure clarity that this proposed payment limit would be applied to payments to providers of Medicaid services that may not clearly fall within the description of a practitioner, such as transportation, clinic, or CCBHC providers, and to ensure payments targeted to entities would be subject to the proposed payment limit as well. We emphasize that payments targeted to an entity not otherwise subject to a UPL or other similar limit, such as a clinic, would be subject to the proposed limit. However, a payment targeted to a provider service subject to a UPL, such as inpatient services in a hospital associated with an academic medical center, rather than practitioner-level data such as physician services, would be subject to the inpatient hospital UPL regulatory requirements at § 447.272 and would not be subject to the proposed new limit. We invite public comments on the proposed use of the terminology “practitioner or provider” to reflect the different individuals or entities to which payments can be targeted and therefore subject to the proposed payment limits at § 447.381(c), and if CMS should characterize these individuals and entities differently for improved clarity or to more effectively capture the intended scope of individuals and entities to which we intend the proposed payment limit to apply.
In proposed paragraph § 447.381(a), we are proposing to establish a limit “for the total Medicaid FFS payment authorized under the State plan or waiver in instances where all or a portion of the payment is targeted to a subset of participating practitioners or providers furnishing the applicable Medicaid-covered services.” For purposes of this provision, State plan or waiver authority includes services authorized under sections 1915(i), 1915(j), 1915(k) of the Act; section
( printed page 30434)
1915(c) waiver authority; and section 1115(a) demonstration authority. By total payment, we mean the entirety of the Medicaid FFS payment on a per service basis, regardless of whether the payment is characterized as a base or supplemental payment. We are not limiting this terminology to FFS supplemental payments because the proposal applies to the total Medicaid FFS payment, including both base and supplemental components, where some or all of that payment is targeted and varies from payments available to all participating providers furnishing the service.
As previously discussed, operationally in an FFS delivery system, base payments are generally predetermined rates that States pay providers for specific services according to their Medicaid fee schedule. Payments that may be part of or added onto these payments include, but are not limited to, add-on payments, payment adjustments, and supplemental payments (including but not limited to quality incentive payments that are made to providers for increased quality of care). If a State is proposing a payment to certain practitioners that would be supplemental to the base payment, the limit would apply to the combined total of the supplemental payment and the applicable base payment, along with any associated add-on or payment adjustments. If the State is proposing an alternate fee schedule for certain practitioners that represents the base payment for a subset of participating practitioners furnishing those services, the limit would likewise apply. In paragraph (a), we include the language “in instances where all or a portion of such payment is targeted to a subset of participating practitioners or providers furnishing the applicable Medicaid-covered services.” Thus, even where a base payment applies to all practitioners, if a State proposes a supplemental payment available only to a subset, the limit proposed in paragraph (c) applies to the total payment, even if only a portion of that payment is targeted, subject to the scope and exceptions proposed in paragraphs (b) and (d), respectively, discussed later. However, in instances where different practitioners within a benefit category (for example, a nurse practitioner and a pharmacist under the other licensed practitioner benefit) are paid differently for the same service, when the payment differential is tied to provider qualifications, the payment is not considered targeted and the limit would not apply.
Within the FFS provisions of this proposed rule, Medicaid payments that are “targeted” refer to any payment that a State directs to a specific practitioner or provider type, or group of practitioners or providers furnishing Medicaid-covered services. By targeting a payment to certain practitioners or providers that provide a particular service, the payment is not available to all practitioners or providers furnishing the same Medicaid-covered services under the State plan. A State may target payments in various ways, including: (1) developing a fee schedule specifically for certain practitioners or providers that exceeds the fee schedules available to others (excluding certain providers like FQHCs and RHCs for which there is a statutory requirement for a particular payment rate or methodology, such as that specified in section 1902(bb) of the Act for FQHCs and RHCs, as discussed later in section II.B. of this proposed rule); (2) creating qualifications or eligibility requirements that target certain practitioners or providers that can receive the supplemental payment; and (3) creating a quality incentive payment or value-based payment that targets certain practitioners or providers and excludes other similar practitioners or providers from participation or from receiving the incentive or value-based payment.
As such, this proposed “targeted” regulatory language, as opposed to characterizing as a supplemental payment limit, would ensure States cannot simply reclassify payments as something other than a supplemental payment to avoid the proposed regulatory requirements. For example, a State with an approved ACR supplemental payment may currently pay a total of $10 million in supplemental payments to only four out of 500 providers in the State when those four providers contribute the non-Federal share of the payment through an IGT. We intend to prevent a situation in which the State reclassifies that $10 million from a prior ACR supplemental payment as a $10 million rate “add-on” or some other type of additional payment to maintain the same payment level for the same four providers that finance the non-Federal share of the payment through an IGT. In that case, although the payment may be characterized as an add-on to the base rate and not as a supplemental payment, it remains targeted because it is only available for certain providers of the relevant Medicaid-covered services. Conversely, we do not intend to prevent a situation where the State incorporates a $10 million supplemental payment into the base rates for all 500 providers in the State, as this would then be Statewide and therefore not targeted, under proposed paragraph (b)(1). When a payment is not targeted, it would not be subject to the proposed practitioner or provider-specific payment limit in the FFS provisions of this proposed rule.
As a result, quality incentive or value-based payments that all Medicaid-participating practitioners or providers of a given Medicaid-covered service have the opportunity to earn would generally be excluded from the scope of proposed § 447.381(a). As discussed in SMDL #20-0004, VBPs under FFS State plan authority have historically included concepts such as bundled payment rates, payment based on episodes of care, shared savings, accountable care organizations, integrated care models, primary care medical homes, health homes, and advanced payments.[75]
If participation in the VBP methodology is open to all participating Medicaid practitioners or providers under the applicable service payment methodology, payments resulting from these VBP methodologies would not be targeted payments under § 447.381. However, if the State designs a VBP methodology where participation is limited to such an extent that only a select group of practitioners or providers (such as those with the means and ability to fund the non-Federal share) can reasonably participate, such payments would be considered targeted under § 447.381 and subject to the limit described in the next section. In that regard, under this proposal, States would retain flexibility to promote quality improvement, which may result in better care and reduced program cost over time across the entire Medicaid program, but may not use value-based or quality payments in a manner that effectively targets certain practitioners or providers in a way that circumvents the proposed limit. We acknowledge this proposed FFS VBP policy, where a VBP is not inherently subject to the limit, differs from the managed care VBP provisions of this proposed rule, which applies the limit to all VBP SDPs. This difference is due to inherent differences between both delivery systems. In the FFS delivery system, the State is the payer of Medicaid services; and therefore, has flexibility and sole control in proposing and implementing VBP methodologies, unlike in managed care, where managed care plans can establish these payments outside of direct State control.
Under FFS State plan authority, States target a payment to certain practitioners
( printed page 30435)
or providers through a SPA submission in various ways. A SPA might list certain provider groups by name or affiliation or apply provider eligibility or provider qualification requirements to receive the payment. For example, a State may require practitioners or providers to be in a certain State-determined geographical location of the State, effectively targeting the practitioner in a specific State-determined location rather than relying on existing county, parish, borough, or municipality lines. States can target providers of a particular size or level of Medicaid utilization by specifying that a provider is only eligible for a payment if the provider has a specific dollar amount of Medicaid revenue. A State may also establish a practitioner or provider qualification for a payment where the requirements are so administratively burdensome that the payment effectively targets only those practitioners or providers that are capable of and willing to satisfy those requirements, even though such requirements would not otherwise be required to receive payment for services. We would examine the proposed payment methodology, including all criteria that must be satisfied for a participating practitioner or provider to receive the payment, as part of our standard rate proposal review practices to confirm that all participating practitioners or providers of the relevant Medicaid services will receive or have a reasonable opportunity to earn the payment in determining whether a payment is targeted for purposes of these proposed provisions.
2. Scope (§ 447.381(b))
We propose at § 447.381(b) to specify the scope of when the limit on Medicaid payments described in proposed § 447.381(c) would not apply. Specifically, we first propose that the limit would not apply when a State's FFS payment methods are uniform for all participating practitioners or providers within the State, or within a geographic region of the State (that is, a county, parish, borough, or other municipality) that is referenced under a payment methodology specified in the State plan. As mentioned previously, when a State targets payment to certain practitioners or providers, the payment is not available to all practitioners or providers furnishing the same Medicaid-covered services under the State plan. If the payment is uniform across the State, or within one or more counties, parishes, boroughs, or other municipalities in the State, we would not consider such payments to be targeted and therefore the limit would not apply. A State must still be prepared to demonstrate that the uniform (that is, non-targeted) rate is economic and efficient, as is the case for all rate proposals under section 1902(a)(30)(A) of the Act.
The proposed scope provision would require, for a payment to be considered uniform, that an applicable geographic region be a county, parish, borough, or other municipality. This means that a State could not define a special purpose district solely for rate-setting purposes (or utilize a pre-existing district such as one associated with tax rates) to the extent it does not align (as in, share the same boundaries) with a county, parish, borough, or municipality, to characterize a payment rate as uniform for that geographic region. This applies where the rate is not uniform for all practitioners or providers furnishing the applicable Medicaid covered services in a geographic area defined by the previously referenced political boundaries and instead effectively targets a limited number of practitioners or providers and therefore would be presumed to not be economic and efficient. We note that although a total payment may be uniform for a State or geographic region(s), the fact that these payments fall outside the scope of this limit is not intended to suggest a rubber stamp of approval for a payment methodology solely because it is uniform within a State or permissible geographic region. We still intend to scrutinize the features of the geographic areas associated with rates, to ensure economy and efficiency under section 1902(a)(30)(A) of the Act, which applies independently of the uniformity criteria. As an example, one way a State could demonstrate economy and efficiency for payment rates that differ across geographic regions is by showing that the region aligns with a distinct geographic Medicare Administrative Contractor (MAC) rate for Medicare. We acknowledge that MAC geographical boundaries may not align with a State's county, parish, borough, or other municipality lines. To the extent that a MAC rate is available in a similar geographic region, we would expect and generally defer to the State to develop a reasonable methodology for aligning the rates associated with geographical regions in their State with Medicare payment areas and those rates for purposes of then using that MAC rate as the rate applicable to the limit proposed in this rule. States also have the flexibility to develop and propose alternative reasonable methodologies for demonstrating economy and efficiency under section 1902(a)(30)(A) of the Act for a payment methodology that varies by geographic region, and we expect States to include an explanation of the State's reasoning and methodology with its SPA submission for CMS to evaluate.
We also believe that excluding payment rates that are uniform for a geographic region from the scope of the limits in paragraph (c) would provide the necessary flexibility for States to establish rates that account for rural providers. We expect geographic boundaries such as counties to allow a State to sufficiently identify a rural region consisting of one or more counties, for example, to establish separate but uniform rates for those regions. As such, we are not proposing a distinct policy or separate limit for rural areas. Rather, States could explain any rural considerations relevant to a proposed geographic rate when demonstrating that the payment rate is economic and efficient for the applicable county, parish, borough, or municipality. We invite comment on whether additional guidance would be helpful for States seeking to preserve or increase the supply of providers in rural areas, including whether there are other appropriate means of identifying State-defined rural districts, provided such approaches do not allow States to define rural districts in a manner that targets a particular practitioner or provider. We also considered, but did not propose, excluding payment rates that are uniform for a geographic region from paragraph (b), in which case they would fall within the scope of paragraph (c). In this instance the proposed limits in paragraph (c) would apply. We invite comments on this alternative policy or other potential approaches for these payments.
Next, we propose that the limit would not apply when the total payment is subject to another limit. Specifically, the limit would not apply when the total payment for a Medicaid-covered service is already subject to a limit under §§ 447.271, 447.272, 447.321, or 447.325, or sections 1903(i)(7) or 1903(i)(27) of the Act, but only to the extent that the total payments are subject to such other limit. The regulatory limits listed in this section are the existing UPLs; specifically: § 447.271 (upper limit based on customary charges for inpatient hospital services); § 447.272 (inpatient services furnished by hospitals, NFs, ICFs/IID, and IMDs); § 447.321 (outpatient services furnished by hospitals and clinics); and § 447.325 (other inpatient and outpatient facility services, which includes psychiatric residential treatment facilities (PRTFs)). Most of these existing limits in regulation are
( printed page 30436)
tied to amounts that Medicare would pay for the relevant services. The primary exception is PRTFs, for two reasons: (1) § 447.325 limits Medicaid payment for each facility to the provider's customary charge and requires that payments not exceed prevailing charges in the locality for comparable services under comparable circumstances (also referred to as usual and customary charges); and (2) Medicaid typically is the only payer of PRTF services and therefore PRTFs typically lack applicable Medicare payment rates to serve as comparators for a Medicare-based UPL demonstration. In addition, sections 1903(i)(7) and 1903(i)(27) of the Act limit Medicaid payments for certain durable medical equipment (DME) expenditures [76]
and clinical diagnostic laboratory (CDL) services, respectively. We are proposing to exclude payments subject to these existing payment limits from the proposed limit at § 447.381(c) to avoid unnecessary duplication of requirements and to focus on addressing payments that lack clear and objective payment limits in Federal requirements today. We request comment on whether any other existing limits or required payment methodologies, in addition to §§ 447.271, 447.272, 447.321, and 447.325 and sections 1903(i)(7) and (27) of the Act, should be accounted for in proposed § 447.381(b), and whether they should be accounted for by excluding them from the proposed scope or otherwise.
We recognize that statutorily required payment floors, such as those applicable to FQHCs and RHCs (section 1902(bb) of the Act), CCBHC demonstrations (section 223 of the Protecting Access to Medicare Act of 2014 (Pub. L. 113-93), and hospice providers (section 1902(a)(13)(B) and (30)(A) of the Act), may interact with the limit proposed in this rule where those statutory payment methodologies result in rates that exceed applicable Medicare rates. To the extent that a targeted payment, within the meaning of this rule is subject to a specific statutory payment methodology, we propose regulatory language in § 447.381(c) to ensure that the proposed limit would not conflict with those statutory rate requirements. As discussed later in section II.B. of this proposed rule, we propose language to ensure that this proposed limit, if finalized, would operate consistent with applicable statutory payment requirements.
However, we want to highlight the proposed language “only to the extent that the practitioner's or provider's total payments are subject to such other limit.” Under this provision, a State would not be able to target a payment to a particular practitioner or provider that exceeds the limit proposed in paragraph (c) on the basis that the practitioner or provider receives a portion of their total Medicaid payments for services subject to a UPL or receives payment from another entity for furnishing those services. For example, physician group-A is contracted by inpatient hospital-B to furnish inpatient hospital services to Medicaid beneficiaries. Inpatient hospital-B furnishes Medicaid-covered inpatient hospital services and receives Medicaid payment subject to the inpatient hospital UPL under § 447.272 and subsequently compensates physician group-A for inpatient hospital services rendered. Separately, the State proposes a targeted supplemental payment for physician services under section 1905(a)(5) of the Act to physician group-A. In this example, the Medicaid payments made to inpatient hospital-B that are subject to the UPL under § 447.272 remain outside the scope of the proposed limit because they are for inpatient hospital services and thus subject to another UPL. However, the targeted supplemental payment made directly to physician group-A would be subject to the limit proposed in paragraph (c) because it is a targeted payment for an entirely different service (
e.g.
physician services). In other words, the limit proposed in paragraph (c) applies to the targeted payments for physician services even if physician group-A receives payment for other Medicaid services (
e.g.
inpatient hospital services) that are also subject to a different UPL. The existence of other Medicaid payments subject to a UPL does not remove the targeted supplemental payment from the scope of paragraph (b).
3. Targeted Medicaid Payment Limit (§ 447.381(c))
Within the scope of FFS targeted Medicaid payments discussed previously, we propose to limit these payments to a percentage of Medicare rates, depending on the circumstances of the State. Specifically, in paragraph (c), we propose that “a State's Medicaid State plan fee-for-service payment methodology must specify that, except as provided in paragraph (b) of this section, total Medicaid payments made to a practitioner or provider for a Medicaid-covered service may not exceed the percentages, listed in paragraphs (c)(1) and (2), of the Medicare fee-for-service payment rate that would be paid to the practitioner or provider for the service if it were paid under the applicable Medicare payment rates established under Parts A or B of Title XVIII of the Act effective for the FY or CY, as applicable, that corresponds to the State plan rate year. For this purpose, the State plan rate year is the first State plan rate year that begins during the FFY or CY in which the Medicare payment rate is in effect.” Then, we specify the applicable percentages: for Expansion States, as defined in proposed § 438.6(a), the limit would be 100 percent of Medicare rates, and for Non-Expansion States, the limit would be 110 percent of Medicare rates. These thresholds align this proposal with the treatment of Expansion and Non-Expansion States in the managed care proposals, which would implement the statutory framework established in section 71116 of the WFTC legislation.
This requirement would apply to all targeted payments within the scope of § 447.381 that are not subject to an exception under proposed paragraph (d). However, we propose to specify that for “Medicaid payment rates subject to a statutory requirement for a particular payment rate or methodology, the limit under this paragraph may not be less than the required Medicaid payment rate or the rate calculated under the required methodology.” This language is intended to ensure that the proposed limits would not conflict with rate requirements such as those for FQHCs or RHCs (section 1902(bb) of the Act), and recognizes that certain Medicaid payment amounts, such as hospice rates (sections 1902(a)(13)(B) and 1902(a)(30)(A) of the Act), may exceed applicable Medicare rates because of statutory coverage requirements.
Historically, in practice, we have treated the ACR as an effective UPL for targeted practitioner payments, instead of applying aggregate UPLs based on reasonable estimates of Medicare payment amounts, as is done for most other Medicaid services subject to a UPL and have permitted States to pay up to the ACR for these services. We are not characterizing the proposed targeted practitioner payment limit as a UPL, for several reasons. We addressed previously in this section the distinction between this practitioner or provider-specific limit and other UPLs, which are calculated in the aggregate. In addition, we are not proposing to require a separate demonstration associated with this limit beyond the documentation submitted with the initial proposal (for example, with a SPA), and therefore this proposed limit is distinguished from other UPLs that include demonstration requirements. In other words, if
( printed page 30437)
finalized, this proposed rule would not require States to submit demonstrations to us on an annual basis (for ACR methodologies) or triennial basis (for Medicare equivalent of the ACR), as we have expected States to do in connection with ACR supplemental payments in FFS Medicaid. In this case, the proposed language makes clear that the requirement to limit targeted payments would be reflected in the State's Medicaid State plan payment methodology. When a State proposes a payment rate in a SPA, whether to update a payment to comply with this limit, if finalized, or to implement subsequent payment adjustments, the SPA would be required to make clear how the total payments for practitioners or providers being targeted would not exceed the applicable percentage of the corresponding Medicare payment rates.
Any Medicare payment rate corresponding to a Medicaid service subject to this payment limit would function as the basis for the limit for Medicaid; however, we believe Medicare's Physician Fee Schedule (PFS) and Ambulance Fee Schedule (AFS) would serve as the primary sources of Medicare payment rates for the basis of the payment limit proposed under § 447.381(c). We are proposing to apply a limit on targeted Medicaid payments using a percentage of the Medicare payment rate as a measure of economy and efficiency in accordance with section 1902(a)(30)(A) of the Act. Although we have explained how we view this limit as distinct from UPLs, we note that this proposed rule aligns with the existing UPL regulations to the extent that both limit payments (albeit in the aggregate, in the case of a UPL) to a reasonable estimate of what Medicare would have paid or a provider's usual and customary charge. Although we are not proposing to require States to submit a UPL demonstration for this limit, the proposed limit would function as a ceiling for Medicaid payment rates authorized through the State plan, rather than UPL demonstrations. Similarly, by proposing to use Original Medicare as the basis of the FFS payment limit on targeted Medicaid payments for services that are not already subject to a UPL, we are seeking to ensure more consistent application of section 1902(a)(30)(A) of the Act across Medicaid services. Furthermore, this approach would align with the directive in the Presidential Memorandum discussed earlier that instructs the Secretary to, where possible, ensure Medicaid payment rates are not higher than Medicare, to the extent permitted by applicable law.
We propose to utilize Original Medicare payment rates as the basis for the general payment limit for targeted Medicaid payments for three principal reasons. First, both Medicaid and Medicare are government health coverage programs available to citizens in every State and with a similar number of enrollees (averaging 70 million per program). Second, since 2001, FFS Medicaid has relied on a reasonable estimate of what Medicare would pay for most services subject to UPL requirements (distinguished earlier) to ensure economy and efficiency as required under section 1902(a)(30)(A) of the Act. Third, Medicare maintains publicly available and transparent methodologies for calculating its FFS payment rates, unlike commercial payer rates that are generally proprietary and not verifiable. Finally, as discussed, we believe it is important and appropriate to align Medicaid delivery systems as much as possible; thus, we are proposing to utilize Medicare to align with the managed care provisions of this proposed rule.
For the reasons previously described, we are proposing to use Medicare FFS payment rates as the basis of the general limit for targeted Medicaid payments, because we believe that the Medicare FFS payment rates are likely to serve as a reliable balance between the requirement that rates be economic and efficient—the specific concern this proposed limit is intended to address—as well as the ability for States to maintain a level of payment sufficient to enlist providers to furnish the relevant services to beneficiaries at high quality as required under section 1902(a)(30)(A) of the Act. Furthermore, we believe lowering the limit from, in practice, ACR to a Medicare-based benchmark would be a more prudent approach, discussed in more detail in section V. of this proposed rule, as Medicare rates are generally lower than commercial rates for physician and hospital services.[77]
As described earlier, this Medicare-based benchmark would be operationalized through percentage limits that vary by State circumstances, with different percentage caps applying for Expansion and Non-Expansion States. We are seeking public comment on the proposed use of Medicare FFS payment rates established in the applicable fee schedule as the basis of the general limit for targeted Medicaid payments.
While the proposed regulatory requirements at § 447.381(c) refer to “applicable Medicare payment rates established under Parts A or B of Title XVIII of the Act,” we generally expect that States would operationalize this regulatory language by identifying Medicare payment rates from Medicare's PFS and AFS under Part B, because most services relevant to this proposed rule are covered under Part B of Title XVIII of the Act. For targeted Medicaid payments for physician and other licensed practitioner services that would be subject to proposed § 447.381 and where there is an existing Medicare equivalent, the Medicaid payment would be limited to the applicable percentage of the published Medicare PFS payment rate in effect for the FFY or CY, as applicable, that would be paid to the provider or practitioner. If finalized, this proposed rule would require States that target a payment to specific Medicaid practitioners or providers to limit such payment to the applicable percentage of the Medicare payment rate as established under Part A or under Part B of Title XVIII of the Act, including Medicare applicable PFS or AFS payment rate.
The Medicare PFS sets different payment rates by provider type (that is, physician versus non-physician practitioner), site of service (that is, facility versus non-facility), and geographical location. We are proposing States account for these different payment rates when ensuring compliance with the payment limit proposed at § 447.381, if this proposed rule is finalized. Medicare pays physicians 100 percent of the Medicare PFS rates; however, Medicare pays certain NPPs (nurse practitioners, physician assistants, and clinical nurse specialists) at 85 percent of the full MPFS amount.[78]
Accordingly, we expect States to limit targeted Medicaid payments for other licensed practitioners, including nurse practitioners, physician assistants, and clinical nurse specialists, to the applicable percentage of the Medicare amount that reflects how Medicare pays the practitioner type, which would effectively permit payment up to 85 percent of the full Medicare PFS amount for Expansion States and up to 93.5 [79]
percent of the full Medicare PFS amount for Non-Expansion States, to account for
( printed page 30438)
the application of the proposed percentage limits to the Medicare payment rate for non-physician practitioners.
Medicare also adjusts the PFS payment amounts based on the site of service (non-facility versus facility setting). The applicable rate (facility or non-facility) is determined by the place of service (POS) code, which identifies the setting where the beneficiary received the face-to-face encounter with the billing practitioner. In this rule, we propose to characterize the applicable Medicare payment rates established under Part B of title XVIII of the Act as described in paragraph (c) as the non-facility payment rate, rather than facility payment rate, as listed on the Medicare PFS. As previously discussed, the proposed payment limits would only apply to services for which no portion of the total practitioner or provider payment is already subject to a limit under §§ 447.271, 447.272, 447.321, or 447.325, and sections 1903(i)(7) and 1903(i)(27) of the Act, which apply primarily to facility-based services (with limited exceptions such as DME or CDL services). Therefore, we believe that the Medicare PFS facility rates generally are not relevant to the proposed payment limit at § 447.381. However, we invite comments on this proposed policy. Given the remaining Medicaid practitioners and services that could receive a targeted payment, we believe that the Medicare PFS non-facility rates are the most appropriate source for States to utilize in complying with proposed payment limit at § 447.381, if finalized.
Medicare sets a national level payment rate on the PFS but also varies their PFS payment rates by geographical location through calculated adjustments that reflect variation in practice costs across geographic areas. Geographical location is accounted for through the geographic practice cost index (GPCI). As described in Chapter 12—Physicians/Nonphysician Practitioners of the Medicare Claims Processing Manual, most physician services are paid according to the Medicare PFS and the fee schedule amounts for a particular procedure code (including CPT and HCPCS (Healthcare Common Procedure Coding System)) are computed using a resource-based formula made up of three components of a procedure's relative value unit (RVU): physician work, practice expense, and malpractice, with geographic adjustments applied to each component.[80]
Medicare establishes a GPCI for every Medicare payment locality for each RVU component and applies the GPCI in calculating the fee schedule payment amount by multiplying the RVU for each component by the corresponding GPCI.[81]
As previously stated, in most instances, we expect States will find the equivalent Medicare payment rates on the Medicare PFS or AFS as established under Part B of title XVIII of the Act. However, we are including a reference to Medicare payment rates as established under Part A of title XVIII of the Act in proposed § 447.381(c). We believe there may be limited instances where Medicare payment rates established under part A of title XVIII of the Act would be the equivalent for a targeted Medicaid payment rate that a State is seeking to implement, such as hospice services and certain home health care services. Additionally, we are including a reference in proposed § 447.381(c) to the FFY because some payment rates established under Part A of title XVIII of the Act are provided on a FFY basis, such as hospice payment rates. In these cases, a State would be able to utilize the Medicare FFY rate for its full State plan rate year, consistent with how States can align their rates with the CY rates under Part B of title XVIII of the Act. However, in most instances, the Medicare payment rates under Part A of title XVIII of the Act are associated with services that are subject to existing regulatory Medicaid UPLs or statutory Medicaid payment limits, such as inpatient hospital services, and are outside the scope of this proposed rule.
As discussed in § 447.381(c), we propose generally limiting targeted Medicaid payments for Medicaid-covered services to a percentage of the applicable Medicare FFS payment rates. For States that propose a targeted Medicaid payment rate for a service that does not have an exact Medicare equivalent, we would expect the State to develop a methodology for identifying a reasonably comparable Medicare payment rate for a comparable Medicare-covered service or set of Medicare-covered services, if applicable. We would expect States to include with their SPA submissions, an explanation of the State's reasoning and methodology for constructing the Medicare rate used for comparison to the Medicaid payment rate. As discussed, we would review the State's approach based on the documentation submitted with the SPA, including the services selected for comparison and the assumptions used, to assess compliance with the proposed requirements. We discuss later in this proposed rule the process for exceptions when there is no reasonable method to identify an equivalent Medicare service.
In developing a methodology for identifying a reasonably comparable Medicare payment rate for a comparable Medicare-covered service, States could consider factors such as: clinically similar code service descriptions (for example, CPT code descriptors, which are clinically focused and utilize common standard [82]
), time-based services where the unit of time for one code could mathematically be extrapolated (for example, multiplying a Medicare payment rate for a 15-minute unit of service by two to derive a Medicare payment rate for a 30-minute unit), or similar service descriptions in which there is a minor difference in one aspect of the service (for example, the same service furnished using different medical equipment).
We acknowledge that many States create Medicaid bundled payment rates that are unique to that State and billed using State-specific codes. In such cases, we would expect the State to identify the constituent services included within the bundled payment rate and to cross-walk those constituent services to the corresponding Medicare payment rate, to the extent feasible. Where a State-specific bundled payment rate includes one or more codes that do not have an exact Medicare equivalent, we expect the State to identify those constituent services included within the bundled payment rate, cross-walk such constituent services to a reasonably comparable Medicare service (using the State's methodology for identifying a reasonably comparable Medicare payment rate for a comparable Medicare-covered service), and, as necessary, adjust the units of service where Medicare uses a different unit than the State.
To illustrate how a State may handle a bundled rate, we provide an illustrative, non-exhaustive example of how a State could crosswalk a State-created bundled rate for Medicaid services to a Medicare equivalent, if this proposed rule is finalized. Assume State-A pays a bundled weekly payment rate of $301.56 for opioid treatment under its rehabilitation services benefit in the State plan. This bundled rate
( printed page 30439)
includes the following discrete services as part of the weekly bundled payment rate: evaluation and management; screening, brief intervention, and referral to treatment; individual psychotherapy; psychotherapy for crisis situations; toxicology testing; chronic care management; and peer support services. Drugs are excluded from the weekly bundled payment rate under the rehabilitation services benefit and are instead paid under the pharmacy benefit. Under State A's payment methodology, the practitioner or provider bills HCPCS code H0020 to represent the weekly bundled rate and also reports the most specific billing code (CPT or HCPCS) that accurately and completely describes each service furnished. For a particular individual's weekly opioid treatment, a practitioner or provider reports: HCPCS code H0020 together with CPT or HCPCS code 99212, H0050, 90832, 90839, 80305, 99490, and H0038.
Medicare covers and pays for the same or comparable discrete services that State-A includes in its bundled rate billed under HCPCS code H0020. The State would be expected to crosswalk the individual codes the provider billed under Medicaid to corresponding Medicare payment rates, including for the individual services included within the bundled payment. State-A determines that Medicare pays for the following codes from the MPFS: 99212, 90832, 90839, 80305, and 99490. However, Medicare does not pay for H0050 or H0038 from the MPFS. For H0050 or H0038, the State would be expected to identify reasonably comparable Medicare services, meaning services that are similar but do not have an exact code match. For example, a State may identify G0396 and G0536 as Medicare equivalents for H0050 or H0038, respectively (see Table 7. In applying this crosswalk, the State would be expected to account for the differences in units of service by adjusting the Medicare payment rate to reflect the unit definition, used by Medicaid, such as by dividing the Medicare payment rate of $41.29 for a 30-minute service by two to derive a 15-minute payment rate of $20.65. See Table 7 for an example of this crosswalk.
We acknowledge there are instances where States may have bundled payment rates that have been in place for many years, even decades, and for which the State currently does not have available information regarding how the payment rates were originally developed, including the specific constituent services or payment rates for those constituent services. As a result, a State may lack historical data sufficient to crosswalk each constituent service to a corresponding Medicare payment rate. The absence of a historical rate regarding the development of a State
( printed page 30440)
created bundled payment rate, standing alone, would not qualify for an exception under proposed § 447.381(d). In such circumstances, we would generally expect a State to develop a reasonable methodology to identify the constituent services currently included in the bundled payment rate and to reasonably estimate or deduce the Medicaid payment rate attributable to each constituent service included in the bundled payment rate. Consistent with proposed § 447.381(c), States would be expected to ensure the total Medicaid payments attributable to the constituent services included in the Medicaid bundle payment rate do not exceed the percentage of the corresponding Medicare payment rates. If, after reasonable efforts, a State cannot identify a comparable Medicare payment rate for one or more constituent services, the State would be able to seek an exception under proposed § 447.381(d)(1), consistent with the process described later in this section.
We also emphasize that mere differences in coding, by themselves, would not be sufficient to conclude that no equivalent service exists. Differences in coding practices for otherwise identical or very similar services do not necessarily mean that there is no reasonably comparable Medicare service, and States setting rates should, where appropriate, map between such codes. For example, if Medicare uses a code “99202,” but a State Medicaid Agency codes that same service as “99202MCAID” in its Medicaid billing system, then we would expect the State to align these codes and apply the applicable Medicare-based limit, provided the codes describe substantially similar or identical services. Similarly, the absence of a single Medicare equivalent code within a targeted payment methodology that otherwise utilizes multiple codes would not, by itself, render the entire targeted payment eligible for an exception to this limit. In these situations, we would expect the State to make reasonable efforts to identify a reasonably comparable Medicare code for the service without a direct equivalent, to ensure that the overall targeted payment remains comparable to what Medicare would pay for those same or similar services. If this proposed rule is finalized, we would expect States that make targeted Medicaid payments to physicians and other licensed practitioners to source the Original Medicare payment rates from the published Medicare fee schedule amounts on the Medicare PFS through one or both of the following sources: the Physician Fee Schedule Look-Up Tool [83]
on the CMS website or Excel file downloads of the Medicare PFS Relative Value Files [84]
for the relevant CY from the CMS website. When rates are not available in the Look-Up Tool, the Excel file downloads of the Medicare PFS Relative Value Files contains the necessary information for calculating Original Medicare payment rates.
Medicare has established a Quality Payment Program (QPP), which includes the Merit-based incentive payment system (MIPS) and Alternative Payment Models (APMs). The QPP is designed to reward high-value, high-quality Medicare clinicians with payment adjustments based on performance.[85]
For purposes of this proposal, the Medicare payment rates that serve as a basis for the payment limit under proposed § 447.381(c) would be “the applicable Medicare payment rates established under Parts A and B of Title XVIII of the Act effective for the FY or CY, as applicable, that corresponds to the State plan rate year. For this purpose, the State plan rate year is the first State plan rate year that begins while the applicable Medicare payment rate is in effect.” Our proposal would exclude Medicare QPP payment adjustments because not all providers are eligible for QPP payments, and because we anticipate that States would face significant administrative burden in obtaining and applying Medicare QPP payment data when calculating compliance with the proposed limit. Therefore, the Medicare limit for purposes of proposed § 447.381(c) would not include Medicare QPP payments.
For targeted Medicaid payments for transportation providers (for example, GEMT providers, air emergency medical transportation providers, and NEMT providers) that would be subject to proposed § 447.381 and for which there is a Medicare equivalent service rate, the applicable Medicaid payment would be limited to the published Medicare AFS payment rates in effect for the relevant CY that would be paid to transportation providers. Under the AFS, Medicare Part B pays for a medically necessary non-emergency and emergency ground ambulance, and emergency air ambulance transportation of the beneficiary to the nearest appropriate facility that can treat the patient's condition, when transport by other means would endanger the health of the beneficiary. Therefore, the AFS generally serves as the appropriate comparator for services in these categories. The Medicare AFS payment rates are listed on the Medicare AFS website [86]
effective January 1 of each year and are updated annually by the ambulance inflation factor and geographic adjustment factor (non-facility practice expense component of the geographic practice cost index (GPCI) of the Medicare PFS).
Medicare established AFS payment amounts that include both a base payment, a separate payment for mileage to the nearest appropriate facility and a geographic adjustment factor (GAF) based on the geographic location of the point of the ambulance pick-up. Section 414.610 includes the basis of payment for the AFS. Ground and air ambulance services are paid according to the AFS fee schedule amounts for a particular HCPCS procedure code) which are computed using a resource-based formula that includes an RVU, conversion factor, GAF, including the GPCI and beneficiary point of pick up, and a national uniform loaded mileage rate as well as two applicable permanent and three temporary add-on payments for urban, rural, or super rural areas of the point of ambulance pick up.[87]
The geographical areas applicable to the Medicare AFS are the same as those used for the Medicare PFS.
We recognize that Medicare often sets payment rates for services that are not covered or paid for by Medicare and lists these rates on the PFS fee schedules, which can result in outdated or unreviewed rates remaining listed. In these instances, we do not intend to unintentionally limit State Medicaid payment rates by reference to a Medicare FFS payment that is no longer reflective of current Medicare payment policy. For purposes of the Medicare PFS, we are proposing that States rely on Medicare FFS payment rates for codes with a status indicator of A (Active), R (Restricted), or T (Injections), as such codes generally include RVUs and are subject to Medicare's standard rate-setting and update process. Although some codes with these status indicators may have limited or no Medicare coverage, we may nevertheless establish RVUs and payment amounts for these codes, and where such amounts are established, States would
( printed page 30441)
be expected to rely on them when applying the proposed payment limit under § 447.381, if this proposed rule is finalized. For purposes of the Medicare AFS, which does not utilize code status indicators analogous to those under the Medicare PFS, we would expect States to rely on the published Medicare AFS payment rates as the most appropriate comparator when applying the proposed limit under § 447.381, if finalized.
In instances where a State believes a payment rate listed on the Medicare PFS or AFS has not been updated in a manner that reflects current Medicare payment policy, the State could propose to CMS a methodology, such as a formula, to approximate a more current Medicare payment rate. Such proposed methodologies could include, for example, applying an appropriate inflation factor such as the Medical Care Services component of the Consumer Price Index for All Urban Consumers [88]
or the Medicare Economic Index, to extrapolate the Medicare payment rate to a more current period. States doing so would be expected to provide, with its proposed methodology for calculating a more current Medicare payment rate, supporting documentation describing how the State identified the Medicare rate as outdated, the basis for selecting the time period and inflation factor used, and the steps taken to derive the State's extrapolated Medicare rate. In addition, where a Medicare code is no longer maintained for billing purposes, a State may propose to use a successor Medicare code, provided the successor code is reasonably comparable to the discontinued code and consistent with the overall expectation that States identify reasonably comparable codes whenever feasible. We invite public comments on how to operationalize this flexibility in a manner that ensures Original Medicare payment rates used for purposes of proposed § 447.381 remain reflective of current Medicare payment policy while minimizing administrative burden for States and CMS.
Medicare fee schedule rates under both PFS and AFS reflect the total Medicare payment amount for a service, including any applicable beneficiary co-insurance and deductible amounts. Under proposed § 447.381, targeted Medicaid payments should similarly reflect the total computable payment amount that a provider would reasonably expect to receive as payment-in-full for the provision of Medicaid services. Section 447.15 describes payment-in-full as “the amounts paid by the agency plus any deductible, coinsurance or copayment required by the plan to be paid by the individual.” Therefore, when States make targeted Medicaid practitioner payments, the total payment used for purposes of compliance with proposed § 447.381 must include both the Medicaid agency payment and any applicable cost sharing to the extent that a beneficiary is expected to be liable for those payments. For example, where a State's Medicaid physician fee schedule rate otherwise accounts for beneficiary cost-sharing payment amounts, the State would need to account for such amounts when determining compliance with the proposed payment limit.
We propose to include language specifying that the relevant State plan rate year as “the first State plan rate year that begins during the FFY or CY in which the Medicare payment rate is in effect” to provide States clarity on how proposed targeted payments would need to be aligned with Medicare rates, given the differences in rate years between States and Medicare, if this rule is finalized. As previously discussed, in Medicaid, States commonly target payments to certain physicians and other licensed practitioners (including non-physician practitioners (NPPs) such as nurse practitioners, physician assistants, and clinical nurse specialists for whom the Medicare PFS specifies payment rates, making the Medicare PFS an ideal source for a significant number of the payment rates that would limit the targeted payments to these practitioners. The Medicare PFS is based on the annual PFS final rule that is published in November of each year with the Medicare payment rates listed on the Medicare PFS as effective the following January 1 (for example, the PFS final rule published in November 2024 contains rates effective January 1, 2025).
We acknowledge that many States set their fee schedules in alignment with their SFY, which can begin on various dates, most commonly July 1. A State may wish to align its relevant fee schedule with the CY, under an approved SPA methodology, to ensure the fee schedule consistently reflects the most up to date Medicare rates. As an example, a State with their SFY 2029 starting on July 1, 2028 would need to set its relevant State fee schedule effective July 1, 2028, at no more than 100 or 110 percent of the CY 2028 Medicare PFS rate (effective January 1, 2028) for applicable payments, if this rule is finalized. However, we would not regard States that set their SFY based fee schedules as out of compliance with the CY Medicare rates when the next January rates are released solely on the basis of the timing of the State's fiscal year. As proposed, rates should align for “the first State plan rate year that begins during the FFY or CY in which the Medicare payment rate is in effect.” This means that a State would still be able to set annual rates for its July 1 SFY and have those rates regarded as aligned with the January 1 calendar year of Medicare rates. The same would be true in instances where a State relies on a Medicare Part A rate associated with the FFY; in such cases, the State plan should specify the applicable FFY rates for use during the corresponding State plan rate year.
We are aware that we may issue a correction to the Medicare PFS after the final rule is in effect, and such a correction may change the previously published payment rate for one or more codes. In instances where a State has set their Medicaid payment rates to 100 or 110 percent of the Medicare PFS for a given CY and Medicare later issues a correction that changes previously published payment rates, we would not expect States to update their Medicaid payment rates mid-year. However, States have the flexibility to submit a SPA to update their payment rates to implement the corrected Medicare PFS if they choose. We would permit States that set State plan rate year rates to align with Medicare rates on a calendar year to rely on those rates as set for the duration of the State plan rate year. However, we further wish to highlight that States could include evergreen language when designing payments by submitting a SPA that ties the payment to the “current” Medicare PFS rates, which would have the effect of automatically updating the State's Medicaid payment in alignment with the correction to the Medicare PFS according to the timing specified by Medicare. In instances where States choose not to update their Medicaid payments in alignment with corrections to the Medicare PFS, we encourage States to submit SPAs annually that update their rates tied to Medicare PFS rates to a specific year (that is, the State's Medicaid payment rates for State plan rate year starting on July 1, 2026 are tied specifically to the January 1, 2026 Medicare PFS and subsequent updates will not be implemented by the State). We invite comment on the proposed meaning of “State plan rate year” within this rule and how States would expect to operationalize their programs under this proposal.
4. Exceptions (§ 447.381(d))
As mentioned, there are limited instances where we propose that the
( printed page 30442)
limits proposed in § 447.381(c) would not apply, and as a result targeted payments would be subject to a different review standard. For payments falling within an exception under proposed paragraph (d), we propose that the “State must explain and provide supporting information in the form and manner specified by CMS sufficient to demonstrate that the payments are consistent with section 1902(a)(30)(A) of the Act.” Under section 1902(a)(30)(A) of the Act, payments must be, among other things, consistent with efficiency and economy, and these are aspects we would seek to assess. We describe below the proposed exceptions, followed by a discussion of how States may demonstrate compliance with section 1902(a)(30)(A) of the Act in these circumstances.
The first exception would apply when there is no reasonable Medicare equivalent rate. As discussed in the previous section, we expect States to make reasonable efforts to identify reasonably comparable Medicare rates for the Medicaid services that form the basis of a targeted payment. This exception would apply where, despite such efforts, there is no reasonably comparable Medicare service for some or all of the services included in the targeted payment. In such circumstances, a State would be unable to demonstrate compliance with a Medicare-based limit, and an alternative approach would be necessary. We would expect this circumstance to arise mostly in the context of broad service categories that generally are not covered by Medicare, such as personal care services.[89]
We intend to closely scrutinize the services in question in instances where a State has indicated there is no comparable Medicare rate, for accuracy.
We considered whether to define an alternative limit for use in situations where there is no reasonable Medicare equivalent. In this proposed rule, we have emphasized that we no longer believe the ACR is an economic and efficient threshold, but we have not proposed another benchmark for when a Medicare rate is unavailable. Therefore, we invite comments on potential approaches that could assist States in demonstrating compliance with section 1902(a)(30)(A) of the Act where no Medicare rate exists, including benchmarks that would generally fall below the ACR, while preserving appropriate State flexibility for rate setting to ensure access to quality care, particularly with respect to rural providers.
The second exception would apply to payments that are reconciled to a practitioner's or provider's actual, incurred costs. In these circumstances, we have historically viewed payment methodologies that reconcile to allowable costs, consistent with applicable cost principles, as generally consistent with economy and efficiency. For payment rates reconciled to cost, we follow the cost principles set forth in the Office of Management and Budget (OMB) cost principles at 2 CFR part 200, which are also used by the Medicare program. In that respect this exception is aligned with Medicare. If this proposed rule is finalized, CMS would consider the context of the State's proposal and approved payment methodologies when assessing whether exceptions to the proposed targeted Medicaid payment limit at § 447.381 apply. For example, where a State proposes to pay governmental providers or practitioners based on reconciled costs while continuing to pay private providers under an existing, uniformly applicable fee schedule, payments to governmental providers would fall within the exception in § 447.381(d)(2). In such circumstances, we would not consider payments to the private providers to be targeted within the meaning of this proposed rule based only on the different treatment of governmental providers, because the underlying fee schedule methodology continues to apply uniformly to all providers within that category. In summary, in this example the distinct methodology applied to governmental providers falls within the cost reconciliation exception in proposed § 447.381(d)(2), and the remaining private providers continue to be paid under a uniform fee schedule consistent with § 447.381(b); therefore, the application of different methodologies only to apply a reconciled cost-based payment methodology to the subset of governmental providers does not render the uniform fee schedule-based payments to the remaining private providers targeted.
There are many ways a State may be able to demonstrate that the standard of economy and efficiency has been met when an exception applies. As stated earlier, our intent is not to create another UPL-like demonstration requirement. Consistent with proposed § 447.381(d), a State would be required to provide supporting information only upon request by us, typically in connection with SPA review or program oversight activities, not on a regular or recurring basis. When such a request occurs, we believe our standard practices for reviewing payment rates during an SPA review provide an appropriate framework for the information needed to assess whether the payment rate is economic and efficient, as this is a standard to which all State plan payment rates must already adhere. For example, we may ask a State to describe any cost components used to construct the rate, the calculations used, and the supporting data. We may also request documentation showing how the targeted payment rate was calculated, including the data sources used, the methodology for calculating or trending those data, and the time periods associated with the data. Depending on the context, we may specify a particular form and manner, such as data extracted from a particular source and formatted in a specific way, to ensure that information is reliable and usable for purposes of assessing whether the payment is economic and efficient. In all cases, we would take into account administrative burden and would request data in a form and manner intended to minimize unnecessary burden.
We considered, but did not propose, that when a practitioner's or provider's payments (1) have no reasonable Medicare equivalent rate or (2) are reconciled to cost, total payments made to a practitioner or provider may not exceed 200 percent of the total fee-for service base payments authorized under the State plan. We invite comments on this alternative benchmark or other potential approaches.
5. Transition Period (§ 447.381(e))
We recognize that States already making ACR-based targeted payments may need time to prepare and submit State plan amendments to come into compliance with the proposed new limit, if finalized. For States whose State plans currently provide for targeted Medicaid payments that would exceed the limit in § 447.381(c), if finalized, we are proposing in § 447.381(e) that States would have until the start of the first State fiscal year that begins on or after January 1, 2029, to comply with the limit at § 447.381(c). Specifically, we propose that States with State plan payments that exceed the limit under paragraph (c) of this section, and to which an exception under paragraph (d) does not apply, would be required to submit a State plan amendment to remove these payments or update them to comply with the limit in paragraph (c), with an effective date no later than the start of the first State fiscal year that
( printed page 30443)
begins on or after January 1, 2029. We selected this timeframe to align with the managed care provisions, which would prohibit States from exceeding the applicable payment limit for each service covered under a State directed payment submitted for an effective date on or after January 1, 2029. As an alternative, we invite comments on shorter or longer transition periods from the effective date of the final rule, including 6 months, 1 year, and 2 years, or another date before or after January 1, 2029. We also invite comment on two alternative phase-down transition approaches for targeted payments. Under the first approach, we could establish an interim limit, such as 200 percent of Medicare rates, midway through the transition period leading to January 1, 2029. Under the second approach, we could require an annual percentage reduction, such as 10 percent, of the total payment amount that exceeds Medicare over the course of a 10-year transition period from the effective date of the final rule until the targeted Medicaid practitioner or provider payment comports with the proposed new payment limit, to incorporate a phase-down concept as utilized, albeit differently, in the managed care transition proposal. Under our proposal, States would have the option voluntarily to phase down their targeted practitioner payments that do not comply with the limit in § 447.381(c); however, use of these alternatives would require States to lower such payments one or more times during the transition period, which could effectively create a mandatory glidepath to full compliance. We are not proposing to consider any exemptions or exceptions to the transition period timeline.
For example, a Non-Expansion State with an existing targeted payment, such as an enhanced fee schedule for physicians employed by an academic medical center that results in payment exceeding 110 percent of the corresponding Medicare payment rate would be required by this proposed rule, if finalized, to submit a SPA to lower its State fee schedule rate to no more than 110 percent of the Medicare PFS payment rate for the relevant year within the transition period described in section II.B.4. of this proposed rule. As another example, assume a State has a targeted payment in its FFS delivery system for nurse practitioner services furnished at AMCs, and that targeted payment is based on ACR. Assume further that the State's fiscal year begins on July 1. Under the proposed transition period, if finalized, the State would then have until September 30, 2029 to submit a SPA to obtain a July 1, 2029 effective date to adjust the targeted payment. We note that the effective date of this SPA could not be earlier than the first day of the calendar quarter in which an approvable amendment is submitted, in accordance with § 430.20. However, nothing would prevent a State from submitting a SPA earlier in the transition period if an earlier effective date better aligns with the State's programmatic objectives. In these instances, the SPA could be in full compliance, or reflect an aforementioned voluntary phase-down. However, in this latter instance, a SPA that provides for payment higher than the applicable percentage of the Medicare payment rate would be required to include a sunset date for that methodology, such that it would comply with the limits set forth in § 447.381(c) by the end of the applicable transition period. If a State failed to submit a SPA to establish payments that comply with § 447.381(c), if finalized, the State would not be authorized to continue making the targeted payments and could be subject to deferral or disallowance of noncompliant payments, or to a State plan compliance action under section 1904 of the Act, discussed in the next section.
The following example illustrates how the proposed limit and transition period would be applied in practice, if finalized. Assume State-A, an Expansion State, has a targeted payment for physicians furnishing services at an AMC. State-A uses the ACR to set the targeted payment amount and for submitting an annual demonstration to CMS. In this example, State-A makes this targeted payment as a supplemental payment, as opposed to an alternative fee schedule. Currently, to calculate the supplemental payment and ACR demonstration, State-A and the physicians receiving the payment obtain payment data from their top five commercial payers in the State for specified services. They obtain the data from the billing systems of the physicians eligible for the targeted payment and include data for each CPT code furnished by the physicians eligible for the payment. Assume CMS finalizes this rule as proposed to limit targeted Medicaid payments to 100 percent of Medicare for Expansion States. Then assume State-A's fiscal year begins on July 1. State-A would have until September 30, 2029, to submit a SPA to CMS with an effective date no later than July 1, 2029, that adjusts the targeted payment to comply with the new limit, reducing total targeted payments to no more than 100 percent of the Medicare rate from the previous ACR limit. State-A would not need to continue with its supplemental payment approach, and could instead implement an alternative fee schedule to set the targeted Medicaid payment rates at 100 percent of Medicare. State-A could look at the same CPT codes, find a Medicare equivalent, and either set an alternative fee schedule up to 100 percent of Medicare, or calculate the difference between the base rate and the amount that is 100 percent of the Medicare rate, to be paid as a supplemental payment. Alternatively, State-A may decide that it does not want to maintain these targeted payments subject to this new limit, and instead could submit a SPA that expands a supplemental payment (or a base payment fee schedule) to the entire county where the AMC is located. In this alternative case, State-A would need to be prepared to demonstrate the proposed rates are economic and efficient, in accordance with section 1902(a)(30)(A) of the Act, as part of the SPA submission. We again note that we are not proposing to consider any exemptions or exceptions to the transition timeline other than the alternative transition approaches we have specifically discussed. We invite comments on the transition period proposed and the alternatives considered, including the alternatives of requiring one or more phased reductions in the targeted Medicaid practitioner or provider payment during the transition period, on the way to full compliance with the proposed new payment limit.
6. Compliance With the Targeted Medicaid Payment Limit (§ 447.381(f))
In proposed new paragraph § 447.381(f), we propose to specify the compliance actions to which a State may be subject to if it fails to address payments that exceeds the proposed limit, if finalized. If this proposed rule is finalized as proposed, should a State submit a SPA that proposes a targeted Medicaid practitioner or provider payment that exceed the proposed limits after the effective date of the final rule, we would advise the State via formal written communication during the SPA review process to amend their payment methodology to adhere to the applicable payment limit. Should the State submit a SPA that does not amend its payment methodology, we would document that in a Request for Additional Information (RAI) and if the State continued to not adhere to the payment limit, then CMS would proceed to disapprove this SPA for non-compliance with the payment limit. For
( printed page 30444)
States whose State plans currently provide for targeted Medicaid payments that would exceed the applicable limit in § 447.381(c), and that do not address it in the timeframe described in paragraph (e) of this section, CMS may reduce future grant awards. We may defer and/or disallow the portion of the claim for FFP attributable to targeted Medicaid practitioner or provider payments that exceed the applicable limit, and where appropriate, may initiate a State plan compliance action if the State fails to conform its plan or operation of its plan to the payment limit, consistent with 42 CFR 430.35, 430.40, 430.42, and 430.45. In estimating the amount subject to deferral or disallowance, we would review the State-submitted information about the payment in question, such as the most recent SPA establishing or amending the payment, and would assess the extent to which Medicare payment rates are available for the associated services and the degree to which the applicable limit has been exceeded.
In paragraph (f), we also propose that States submitting a SPA that proposes to exceed the limit under paragraph (c) of this section, and to which an exception in paragraph (d) of this section does not apply, would be subject to SPA disapproval under § 430.15(c) of this chapter. Disapproval of a SPA means that the State would not have authority to implement the proposed payment methodology and would be required to continue to pay providers according to the rate methodology set forth in the already approved State plan. However, that SPA disapproval does not authorize a State to continue making payments that exceed the limit described in paragraph (c) of this section if that is the currently approved rate methodology and the transition has expired. Furthermore, when an exception under paragraph (d) applies but a State fails to furnish information requested by us to determine whether the payment is consistent with section 1902(a)(30)(A) of the Act, the SPA would likewise be disapproved.
III. Collection of Information Requirements
Under the Paperwork Reduction Act of 1995 (PRA) (44 U.S.C. 3501 et. seq.), we are required to provide notice in the
Federal Register
and solicit public comment before a “collection of information” requirement, as defined under 5 CFR 1320.3(c) of the PRA's implementing regulations, is submitted to the Office of Management and Budget (OMB) for review and approval. To fairly evaluate whether an information collection should be approved by OMB, section 3506(c)(2)(A) of the PRA requires that we solicit comment on the following issues:
The need for the information collection and its usefulness in carrying out the proper functions of our agency.
The accuracy of our estimate of the information collection burden.
The quality, utility, and clarity of the information to be collected.
Recommendations to minimize the information collection burden on the affected public, including automated collection techniques.
We are soliciting public comment on each of these issues for the following sections of this document that contain confirmed or potential information collection requirements. Comments, if received, will be addressed in the subsequent final rule (CMS-2449-F).
A. Wage Estimates
To derive average costs, we used data from the U.S. Bureau of Labor Statistics' (BLS') May 2024 National Occupational Employment and Wage Estimates for all salary estimates (
https://www.bls.gov/oes/tables.htm). Table 8 presents BLS' mean hourly wage, our estimated cost of fringe benefits and other indirect costs (calculated at 100 percent of salary), and our adjusted hourly wage.
As indicated, we are adjusting our employee hourly wage estimates by a factor of 100 percent. This is necessarily a rough adjustment, both because fringe benefits and other indirect costs vary significantly from employer to employer, and because methods of estimating these costs vary widely from study to study. Nonetheless, we believe that doubling the mean hourly wage to estimate total cost is a reasonably accurate estimation method.
B. Proposed Information Collection Requirements (ICRs)
1. ICRs Regarding Special Contract Provisions Related to Payment (§ 438.6)
The following proposed changes will be submitted to OMB for review under control number 0938-1453 (CMS-10856). We anticipate revising the SDP preprint at a later date to address needed revisions under a final rule.
This rule's proposed amendments to § 438.6(c)(1)(iii) would significantly reduce the number of preprint submissions because prior approval would no longer be required for minimum fee schedule and maximum fee schedule SDPs and uniform increase SDPs would be phased out. We believe 42 States would no longer submit 272 SDP preprints to us on an annual basis. Based on the preprint, we estimate an active burden of 2 hours at $129.80/hr for an actuary, 2 hours at $128.00/hr for a general and operations manager, and 6 hours at $87.52/hr for a business operations specialist. In aggregate, we estimate an annual State burden reduction of minus 2,720 hours (272 SDPs × 10 hr) and minus $283,076 [272 preprints × [(2 hours × $129.80/hr) + (2 hours × $128.00/hr) + (6 hours × $87.52/hr)]). When taking into account the Federal administrative match of 50
( printed page 30445)
percent, we estimate an annual State savings of minus $141,538 ($283,076 × .5).
Section § 438.6(c)(2)(iii) in the 2024 final rule required States to submit documentation demonstrating that the total payment rate would not exceed the ACR for SDPs [90]
for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at an academic medical center. Our active burden estimates are for 6 hours at $129.80/hr for an actuary, 3 hours at $128.00/hr for a general and operations manager, and 6 hours at $130.68/hr for a software and web developers. Since this proposal would remove this regulatory requirement, we estimate a reduction of minus 900 hours (60 demonstrations × 15 hr) and minus $116,813 (60 demonstrations × [(6 hr × $129.80/hr) + (3 hr × $128.00/hr) + (6 hr × $130.68/hr]). As this was a requirement to update once every 3 years, we annualize our burden estimates to minus 300 hours (900 hr/3 years) and minus $38,938 ($116,813/3 years). When taking into account the Federal administrative match of 50 percent, we estimate an annual State savings of minus $19,469 ($38,938 × .5).
We estimate this rule's proposed amendments to § 447.381 would require, based on data in our MBES system regarding existing supplemental payments with ACR demonstrations, 25 States to submit a payment SPA to amend targeted payments, either to adhere to the new Medicare limit, or to expand the payment so that it is no longer targeted. States also may fold this work into another planned SPA submission, but for purposes of this estimate we will view them as standalone submissions (25 total SPAs). Finally, we do not believe these proposals would require any changes to the Form CMS-179 included with a SPA submission but we invite comment as to whether we would need to revise the Form CMS-179.We estimate it would take 10 hours at $61.12/hr for a social science research assistant to prepare and submit the SPA, 6 hours at $129.80/hr for an actuary to prepare the payment data, and 3 hours at $128.00/hr for a general and operations manager to review the data and SPA. In aggregate, we estimate one-time burden of 475 hours (25 SPAs × 19 hr/SPA) at a cost of $44,350 (25 States [(10 hr × $61.12/hr) + (6 hr × $129.80/hr) + (3 hr × $128.00/hr)]). When factoring in OMB's typical 3-year approval period, we estimate an annual burden of 158 hours (475 hr/3 years) and $14,783 ($44,350/3 years). When taking into account the Federal administrative match of 50 percent, we estimate an annual State cost of $7,392 ($14,783 × 0.5).
The following proposed changes will be submitted to OMB for review under control number 0938-0618 (CMS-R-148).
Under this rule's proposed changes and based on data reviewed in MBES as of the second quarter of FY 2025, we estimate that 17 States (13 States submitting annual demonstrations + 12 States submitting every 3 years or an annualized amount of 4 States) would no longer need to submit a demonstration at a prescribed cadence, but must be prepared to provide similar information, upon request. As such, the recordkeeping burden will remain unchanged from what is currently approved by OMB under the aforementioned control number while the reporting time and frequency would decrease since the demonstration documentation would be submitted less frequently to us. We also project that the reporting template “Qualified Practitioner Services Average Commercial Rate Template” would no longer be necessary by the proposed changes. We invite comment on this assumption.
We estimate that the time for a social science research assistant to prepare and submit demonstration documentation would decrease by 5 hours at $61.12/hr and the time for a general and operations manager to review the submission would decrease by 3 hours at $128.00/hr.
As previously mentioned earlier in this section, the 17 States submitting demonstrations are accounted for in our
( printed page 30446)
burden calculations as 17 demonstrations per year to account for the States submitting demonstrations annually and every 3 years. In aggregate, we estimate an annual burden reduction of minus 136 hours (17 demonstrations/year × 8 hr/demonstration) and minus $11,723 (17 demonstrations × [(5 hr × $61.12/hr) + (3 hr × $128.00/hr)]). When taking into account the Federal administrative match of 50 percent, we estimate an annual reduced State cost of $5,862 ($11,723 × 0.5).
C. Summary of Proposed Collection of Information Requirements and Associated Burden Estimates
D. Submission of PRA-Related Comments
We have submitted a copy of this proposed rule to OMB for its review of the rule's information collection requirements. The requirements are not effective until they have been approved by OMB.
We invite public comments on these potential information collection requirements. If you wish to comment, please submit your comments electronically as specified in the
DATES
and
ADDRESSES
sections of this proposed rule and identify the rule (CMS-2449-P), the ICR's CFR citation, and OMB control number.
IV. Regulatory Impact Analysis
A. Statement of Need
This proposed rule would advance CMS's efforts to improve fiscal integrity and stewardship of the federal funds used in the Medicaid program. In addition, the proposed rule would better align payment requirements across FFS and managed care programs and across different provider types.
B. Overall Impact
We have examined the impacts of this rule as required by Executive Order 12866, “Regulatory Planning and Review”; Executive Order 13132, “Federalism”; Executive Order 13563, “Improving Regulation and Regulatory Review”; Executive Order 14192, “Unleashing Prosperity Through Deregulation”; the Regulatory Flexibility Act (RFA) (Pub. L. 96-354); section 1102(b) of the Social Security Act; and section 202 of the Unfunded Mandates Reform Act of 1995 (Pub. L. 104-4).
Executive Orders 12866 and 13563 direct agencies to assess all costs and benefits of available regulatory alternatives and, if regulation is necessary, to select those regulatory approaches that maximize net benefits (including potential economic, environmental, public health and safety, and other advantages; distributive impacts). Section 3(f) of Executive Order 12866 defines a “significant regulatory action” as any regulatory action that is likely to result in a rule that may: (1) have an annual effect on the economy of $100 million or more or adversely affect in a material way the economy, a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or State, local, or tribal governments or communities; (2) create a serious inconsistency or otherwise interfere with an action taken or planned by another agency; (3) materially alter the budgetary impact of entitlements, grants, user fees, or loan programs or the rights and obligations of recipients thereof; or (4) raise novel legal or policy issues arising out of legal mandates, or the President's priorities.
A regulatory impact analysis (RIA) must be prepared for a regulatory action that is significant under section 3(f)(1) of Executive Order 12866. Based on our
( printed page 30447)
estimates, the Office of Management and Budget's (OMB) Office of Information and Regulatory Affairs (OIRA) has determined that this rulemaking is significant under section 3(f)(1) of Executive Order 12866. Accordingly, we have prepared an RIA that to the best of our ability presents the costs, benefits, and transfers of the rulemaking. Therefore, OMB has reviewed these proposed regulations, and the Departments have provided the following assessment of their impact.
C. Detailed Economic Analysis
We have examined the proposed provisions in this rule and determined that most of the proposed revisions to parts 438 and 447 outlined in this proposed rule are expected to minimally or moderately increase administrative burden and associated costs, as we note in the COI (see section III of this proposed rule). Aside from our analysis of burden in the COI, we believed that certain provisions in this proposed rule should specifically be analyzed in this regulatory impact analysis as potentially having a significant economic impact. These include provisions on the proposed new limits on total payment rates for SDPs and for targeted Medicaid payments for certain services through FFS.
1. Benefits
There are several benefits to this proposed rule. We expect that this proposed rule would increase transparency of Medicaid provider payment rates and financing. We also believe that this proposed rule would create consistency between Medicaid and Medicare by requiring the Medicaid total payment rates through SDPs and targeted FFS practitioner payments to be no greater than—
100 percent of the specified total published Medicare payment rate (or, in the absence of a specified total published Medicare payment rate, the payment rate under the Medicaid State plan (or under a waiver of such plan)) for an Expansion State; or
110 percent of the specified total published Medicare payment rate (or, in the absence of a specified total published Medicare payment rate, the payment rate under the Medicaid State plan (or under a waiver of such plan)) for a Non-Expansion State.
There is a limited exception to the payment limit for SDPs that qualify for a temporary grandfathering period. The proposed rule would further align Medicaid managed care programs and FFS programs.
The proposed rule is anticipated to reduce administrative costs and burdens on CMS. Currently, we are expending more resources on reviewing and approving SDP preprints as required in § 438.6(c)(1)(i), and those costs would likely increase as the number of and total dollar amounts of SDPs grow. The proposed rule would result in simpler administration of SDPs and reduce the time, effort, and cost it takes to provide oversight of SDPs in managed care programs.
Finally, we believe that the proposed rule would provide greater fiscal integrity to the Medicaid program. CMS, as well as other government entities, have been concerned with the rapid growth of SDPs and whether the additional spending improves access, quality, or program outcomes. These proposed changes would strengthen Federal Medicaid oversight and reduce potentially inefficient spending.
We are not able to quantify these benefits.
2. Costs
The proposed rule may result in several potential costs. These changes may require additional time and effort for State Medicaid programs, managed care plans, and providers to revise managed care contracts. In some cases, there may be adverse impacts on providers and consequently on beneficiaries. We are not able to quantify these costs (beyond those reflected in the Transfers analysis below). We request comments on these potential impacts.
3. Transfers
a. State Directed Payments (SDPs) (§ 438.6)
The 2024 final rule set new requirements for the total payment rates for SDPs, with a limit of 100 percent of the ACR for inpatient hospital services, outpatient hospital services, qualified practitioner services provided by AMCs, and nursing facility services. For all other services, the requirement remained the same as in the 2016 final rule—that is, that provider payment rates are “reasonable, appropriate, and attainable.”
SDPs are a substantial component of Medicaid managed care programs. States may direct payment from Medicaid managed care plans to providers. These payments must relate to one or more of the goals and objectives of the Medicaid managed care quality strategy required under § 438.340, which can include improving access to care and healthcare quality. States are estimated to have paid $143.8 billion of SDPs in FFY 2025 (excluding SDPs for which States are not required to receive written prior approval by us under § 438.6(c)(2)(i) via submission of a preprint). This represents 14 percent of all Medicaid benefit spending and 26 percent of Medicaid managed care payments. The largest recipients of these payments were hospitals (87.5 percent), AMCs (4.9 percent), physicians (3.6 percent), and nursing facilities (2.5 percent). States also made SDPs to HCBS providers, transportation providers, and other healthcare professionals. Under current regulations, States are allowed to use SDPs to increase payments to providers up to 100 percent of ACR for inpatient hospital services, outpatient hospital services, qualified practitioner services at AMCs, and nursing facility services. In the 2024 final rule, we noted our intent to continue using ACR as the fiscal guardrail by which we would evaluate all other SDPs as reasonable, appropriate, and attainable.
These projections are based on the projections of Medicaid spending in the President's FY 2027 Budget, updated with SDP data through the end of December 2025, and excluding any changes in spending attributable to the WFTC legislation. Total managed care spending is projected to grow at an average annual rate of 7.5 percent, reflecting growth in use of healthcare services, prices of services, and enrollment in Medicaid. Total SDP spending is projected to grow at an average annual rate of 8.2 percent, outpacing overall managed care spending growth through 2027 and then assumed to grow at the same rate as managed care spending beginning in 2028. The average federal share nationally is approximately 66 percent in 2025 and is expected to remain the same through 2035. Table 13 shows our projections of Medicaid managed care and SDP spending for 2024 through 2035.
( printed page 30448)
Estimating the impact of the proposed SDP provisions is challenging for several reasons. First, the projected and actual spending data that we collect from States is not standardized, and in some cases aggregated across provider types. States submit information in the SDP preprints, for SDPs that require written prior approval under § 438.6(c)(2)(i), but information is sometimes incomplete and there are other limitations to this data. Moreover, SDPs have grown rapidly over the last several years, and future SDP spending under current policy could be higher or lower than projected here.
Second, it is often difficult to determine how total payment rates in SDPs compare, especially when States use different benchmarks for payment (for example, comparing SDPs using Medicare payment rates to those using ACR payment rates). In addition, there is frequently limited information on ACR payment rates. It is difficult to determine how the ACR is calculated and how the calculation may vary across different States and providers. For this proposed rule, this is a key consideration in estimating the impact and is discussed further in this section. To account for limited data on provider payment rates, we have developed a range of estimates using different relative price assumptions between Medicaid, Medicare, and the ACR. Those estimates are presented later in this section.
We have developed a model to estimate the impacts of the SDP provisions of this proposed rule. This model is based on SDP data collected by us through the SDP preprints, including in Table 2 of the current preprint. We collected data by State and SDP and included: the service category; the provider class; the comparative rate basis for assessing the SDP payments (for example, Medicare, the ACR, Medicaid State plan); the average base payment level from plans to providers before the application of the SDP; SDP change (that is, the effect of the SDP on the total payment levels); and final payment levels by provider class; and the estimated total SDP amount. The model primarily relies on data for SDPs with effective dates starting in 2025; there is some additional data for SDPs with effective dates starting in 2024 or 2026. Data from 2025 reflects information on most SDPs and captures all known current SDP spending.
There are some exclusions to the data set. SDPs without payment rate information and for which it is not possible to determine reasonable assumptions of those rates (for example, from more information submitted with the preprint or from a prior year's preprint) are excluded. These excluded SDPs amounted to $1.4 billion of SDPs with rating periods starting in 2025. In addition, there are 6 preprints that do not include total SDP amounts because the State estimated a zero-dollar impact. Thus, spending from these payments is not included. We also have made some adjustments for preprints where information submitted in the preprints is believed to be incorrect. Some examples of these adjustments include: (1) cases where the sum of the base payment level and SDP, plus the effect on the total payment level of other SDPs or pass-through payments, did not match the reported total payment rate; and (2) preprints where the reported total dollar amount appears to be incorrect (often including the base payment level and SDP together). These adjustments to the data have been minor.
In total, there is data for $136.0 billion in SDPs for payments with effective dates starting in calendar year 2025, which we believe is mostly complete (based on the limitations described previously). This does not include SDPs that are not required to have a preprint submitted or receive written prior approval by us under § 438.6(c)(2)(i).
The preprints are also limited in detail. Notably, most States do not report projected, total SDP spending by provider or by provider class in preprints with more than one provider class. To develop estimates, we assumed that the spending was equally distributed across provider class in preprints with multiple classes.
There is a limited amount of information available on the relative prices across different payers. SDP preprints typically only include the payment rates relative to the selected basis utilized for the provider payment analysis in Table 2 of the preprint (for example, the ACR, Medicare, Medicaid State plan) and do not provide comparisons to other payers. There is not enough detail in the preprints to evaluate these payment rates.
There is some analysis comparing prices across the three key payers (Medicaid, Medicare, and commercial payers) and different services. We relied on research from several studies to complete our
analysis.91 92 93 94 95 96
( printed page 30449)
These studies compared prices between Medicare and commercial payers, or between Medicaid and Medicare. We used the conclusions of these analyses (or, where multiple analyses exist, the median of those results) to develop assumptions for these estimates. Using this research, we developed the following price relativities by payer and by service for the estimates in this analysis (expressed as percentages of Medicare payment rates).
For several services, there is less information available on prices across payers. Notably, there is little information on nursing facility prices and the services that Medicare covers may be significantly different than those covered by private payers and Medicaid; and for HCBS, there may not be comparable services provided by Medicare and commercial insurers in many cases. In those cases, we developed assumptions shown in Table 14. The range of commercial-to-Medicare price ratios is large and that the actual differences may vary from these estimates. In addition, the ratios may differ by States and for specific providers. Therefore, we also include low and high scenarios for different relative prices as part of this analysis:
( printed page 30450)
We welcome comments on the assumptions about relative prices between Medicaid, Medicare, and commercial payers.
For each provider class in each SDP, we used the preprint data to calculate the base payment amount, SDP amounts, other SDPs and adjustments that apply to the provider class, and the final payment rate and the ratio of the payment rates to the benchmark rate. We used the projected trends from the President's Budget
excluding the impact of the legislation
to develop estimates of annual spending for each provider class in each SDP prior to the impact of the legislation. We refer to these as the “pre-legislation SDP amounts.”
Then we calculated the new annual limits and compared those amounts and rates to the new limits defined in this proposed rule. Beginning with the first rating period starting on or after July 4, 2025, the total payment rate for SDPs for inpatient and outpatient hospital services, nursing facility services, and qualified practitioner services at an academic medical center must not exceed the applicable payment limit. Specifically, the total payments (that is, the sum of the base payment, SDP, and any other SDPs applicable to the same provider and the impact of any pass-through payments) may not exceed 100 percent of the Medicare payment rate for Expansion States and 110 percent of the Medicare payment rate for Non-Expansion States, unless no total published Medicare payment rate exists for the service, in which case the payment limit is the State plan approved rate. For rating periods that start on or after July 4, 2025 but before January 1, 2028, a grandfathered SDP may not exceed the grandfathered total dollar amount. States would be permitted to implement new SDPs for the four services at the applicable payment limit for rating periods starting on or after July 4, 2025. Beginning with the first rating period starting on or after January 1, 2028, States must reduce 100 percent of the grandfathered total dollar amount by 10 percentage points annually until the payment limit is reached (that is, 90 percent in 2028, 80 percent in 2029, etc.). States are able to phase down faster or transition the grandfathered SDP to an SDP that complies with the applicable payment limits sooner, at their discretion. We refer to these as the “post-legislation SDP limits.”
If the pre-legislation SDP amounts exceeded the post-legislation SDP limits for applicable rating periods, then the SDP was reduced by an amount such that the final payment (base payment plus SDP plus other SDPs and adjustments) was equal to the post-legislation SDP limit. If the pre-legislation SDP amounts were less than or equal to the post-legislation SDP limits, then we assumed that there was no change to the SDP. The difference between the pre-legislation SDP amounts and post-legislation SDP limits is reflected as a reduction in Medicaid spending under this proposed rule, and a transfer from affected providers and other relevant individuals and entities (such as State or local jurisdictions that reimburse providers for otherwise-uncompensated care) to the States and the Federal government.
In addition, we project that additional savings from reduced growth in new SDPs for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at AMCs because SDPs that do not meet the definition of a grandfathered SDP must comply with the new payment limits with the first rating period beginning on or after July 4, 2025. By placing stricter limits on SDPs for these services, we expect to avoid further spending on new SDPs created by States. To estimate the impact of this effect, we assumed that half of SDP growth in excess of growth in the non-SDP portion of managed care spending was for new SDPs (3.4 percent growth in 2026 and 0.9 percent growth in 2027), and that 80 percent of new spending would be above the SDP limits described in this rule. Those estimated amounts are also counted as a reduction in Medicaid spending, and transfers from providers and other affected entities and individuals to States and the Federal government.
As an example, we refer back to the example presented in the preamble (Table 5) of an SDP in an Expansion State of $1 billion in 2025. Expanding on this example, we assume (1) that the base payments for these services are equal to $500 million, (2) that the SDP currently reflects payments equivalent to 150 percent of the Medicare payment rate, and (3) that the SDP payments would grow 5 percent per year. (For the purposes of this example, we assume no growth in base payments and that Medicare payment rates increase annually.) In this example, the SDP would be $1 billion in 2026 and 2027 under the proposed policy, as those amounts would be kept at 2025 levels because the applicable payment limit constrains further growth above that level. Starting in 2028, payments would decrease by 10 percent annually ($100 million) until the total payment rate (base payments plus SDP) equals 100 percent of the Medicare payment rate. (For a non-Expansion State, the decreases would end when total payments were equal to 110 percent of the Medicare rate.) The annual impacts are shown in Table 17.
( printed page 30451)
In this example, expenditures decrease by $50 million as compared to what would have been paid in 2026, and by 2035 expenditures would have decreased by $1.129 billion. As shown in Table 17, the total payment rate under the SDP is equal to 100 percent of Medicare rates by 2032, and thus the SDP is not reduced any further after that.
We project that the proposed rule would reduce total computable (Federal plus non-Federal shares) Medicaid spending by $774.8 billion from 2026 through 2035 (in real 2026 dollars). The annual impacts are shown in Table 18.
We project that the proposed rule would reduce Federal Medicaid spending by $510.1 billion from 2026 through 2035 (in real 2026 dollars). The annual impacts are shown in Table 19.
( printed page 30452)
There are also impacts expected on State Medicaid expenditures. State expenditures would also decrease under the proposed rule, as States make fewer SDPs to providers. However, States often finance the non-Federal share of SDPs with provider taxes and IGTs. SDP preprint data indicates that by the end of 2025, 80 to 90 percent of SDPs relied entirely or in part on provider taxes or IGTs. It is likely that if SDPs were substantially reduced, there may also be decreases in provider tax revenues and IGTs that support the non-Federal share. Thus, the reduction in net State expenditures (State Medicaid payments minus revenue from provider taxes and IGTs) would likely be lower than the gross reduction in State Medicaid expenditures.
An analysis by the Medicaid and CHIP Payment and Access Commission (MACPAC) illustrates how provider taxes and IGTs are related to SDPs.[97]
MACPAC reviewed payments to private and public hospitals in one State. For a private hospital, MACPAC found that the base payments made by Medicaid were 65 percent of what Medicare would have paid, and SDPs added 87 percent of what Medicare would have paid, for a total payment equal to 152 percent of Medicare rates. However, after excluding the amount that the hospital paid to the State in provider taxes, the SDP amount was reduced from 87 percent of Medicare to 24 percent of Medicare, and the total payment was equal to 89 percent of what Medicare would have paid. Similarly, for a public hospital, MACPAC found the base Medicaid payment was equal to 42 percent of Medicare, the pass-through payment was equal to 46 percent of Medicare, and the SDP was equal to 40 percent of Medicare, for a total of 128 percent of what Medicare would have paid. After accounting for IGTs, the pass-through payment was reduced to 22 percent of Medicare and the SDP to 17 percent of Medicare, for a total payment of 82 percent of what Medicare would have paid. The impacts across different States and providers may vary substantially, but this analysis illustrates the complexity of the impacts to States and providers. We request feedback, including suggestions for data from a broader set of providers and States than what is reflected in this MACPAC report, that would facilitate more thorough quantification of how effects flow through the health care system to various entities, individuals, and jurisdictions.
We project that the proposed rule would reduce State Medicaid spending by $264.4 billion from 2026 through 2035 (in real 2026 dollars). The annual impacts are shown in Table 20 below.
( printed page 30453)
In addition to these impacts, we propose to extend these policies to other services not listed in section 71116 of the WFTC legislation. There are fewer SDPs for these services, and these service categories account for only 1 to 2 percent of total SDPs. Moreover, as shown in Table 14, we assume that the ratios of ACR payment rates to Medicare payment rates are not as high for these services as those subject to section 71116 of the WFTC legislation. Therefore, the projected impacts of this policy on spending for these other services are less. These proposed limits would not go into effect until January 1, 2029, and thus the impacts would not begin until 2029. Those projected impacts are shown in Table 21.
We estimate that applying this policy to other services would reduce Medicaid spending by $5.34 billion over the period from 2029 through 2035. Federal spending would be reduced by $3.51 billion, and State spending would be reduced by $1.83 billion.
We welcome comments on the projected impacts to the Federal government and the States.
Providers would lose revenue as a result of reduced SDPs under this proposal. However, as described previously, the net effect on providers may be less than the total quantified impact. To the extent providers pay provider taxes or IGTs that are used to support the non-Federal share for SDPs, the net change in provider revenue (SDPs minus provider taxes and IGTs paid and transferred by providers) could be significantly less. Due to the lack of provider-level data and the wide variation in SDPs across States and provider categories, we are unable to estimate the impacts on providers in more detail.
We expect that there may be significant interactions with other provisions of the WFTC legislation. Notably, sections 71115 (provider taxes) and 71117 (requirements regarding waiver of uniform tax requirement for Medicaid provider tax) of the WFTC legislation are anticipated to reduce the amount of provider taxes collected by States. Provider taxes are a common source of financing of the State share for SDPs. We anticipate that reducing the amount of provider tax collections under these provisions may also lead to reductions in SDPs even absent section 71116 of the WFTC legislation. Thus, there is potential overlap in measuring the effects of these sections. We expect to provide an analysis of the interaction between these proposals in future rulemaking.
Managed care plans may also lose some revenue due to the proposed rule. Plans may receive higher premiums when SDPs are incorporated into capitation rates, or they may be able to retain a small portion of SDP funding for administrative activities. Those amounts would likely be reduced under the proposed rule. We are not able to quantify those impacts.
We welcome comments on the impacts to providers and managed care plans.
As we noted previously, a major source of uncertainty is the relative prices paid between Medicaid, Medicare, and commercial payers. There is wide variation across services and States and it is not clear how these prices compare for each SDP. Research on prices shows a wide range of outcomes as well. Thus, we have developed low and high scenarios to account for the potential differences in relative prices.
In the low scenario, we assumed Medicaid, Medicare, and the ACR rates are relatively closer together, as shown in Table 15. In the low scenario, we project that Medicaid spending would be reduced by $408.4 billion over 2026 through 2035 (in real 2026 dollars) under the proposed rule. Federal Medicaid spending would be $272.1 billion lower, and State Medicaid spending would be $136.3 billion lower. The annual impacts are shown in Table 22.
( printed page 30454)
In the high scenario, we assumed Medicaid, Medicare, and the ACR rates are relatively further apart, as shown in Table 12. In the high scenario, we project that Medicaid spending would be reduced by $989.7 billion over 2026 through 2035 (in real 2026 dollars) under the proposed rule. This includes the impacts to services subject to the payment limits under section 71116 of the WFTC legislation and additional services with limits proposed under this rule. Federal Medicaid spending would be $649.7 billion lower, and State Medicaid spending would be $339.6 billion lower. The annual impacts are shown in Table 23.
We welcome comments on these scenarios.
There is significant uncertainty regarding these estimates. First, these estimates rely on the SDP data reported to us by the States. There are limitations to these data and in some cases data may be incomplete or incorrect. As noted previously, we have taken steps to refine the data for this analysis. It is possible that actual SDP spending could be higher or lower than shown here, and the distribution of spending across services may vary. There is also limited information on prices paid by different payers. Most notably, there is very little public information on what the average commercial reimbursement rates are and how they compare to other payers. To the extent commercial rates are higher or lower relative to Medicare and Medicaid than we have assumed, these estimates may differ from the actual impacts if this proposal is implemented. This specific source of uncertainty is addressed in the range of estimates provided in this section. In addition, SDP spending may grow faster or slower under current law than we have projected. We welcome any additional comments on these estimates.
b. Fee-for-Service Targeted Medicaid Payments
FFS supplemental payments [98]
for physicians, other practitioners, and NEMT were $2.64 billion in FY 2024, with the Federal government paying $1.66 billion and States paying the remaining $0.98 billion. Table 24 shows these payments by service in FY 2024.
( printed page 30455)
Table 25 shows our projections of FFS supplemental payments for these services for 2024 through 2035. These projections are based on forecasted growth of Medicaid FFS spending.
Estimating the impact of the proposed rule on these FFS supplemental payments is difficult. As with SDPs, it is hard to compare payment rates across payers generally, and even more so for specific services and across States. Similar to the SDP analysis, we have developed a range of estimates with different relative prices between Medicaid, Medicare, and the ACR. Those estimates are presented later in this section. In addition, there is less information about supplemental payments than SDPs. States do not provide the same level of detail for supplemental payments as they do for SDPs. However, it is worth noting that these supplemental payments are substantially smaller than SDPs.
To estimate the impact of the proposed rule on these supplemental payments, we relied on the analysis we developed for SDPs. We used the percentage change in SDP spending for these services (physicians; other practitioners, which includes emergency medical transportation and dental services; and NEMT) to develop assumptions for the impact on supplemental payments. We note that we have not assumed that States would offset these reductions by increasing base payments across provider types (but we welcome feedback that would allow for refinement of the quantitative analysis to account for this possibility). Table 26 shows the estimated percentage impacts by service and by scenario (low, medium, and high).
( printed page 30456)
We believe that these are reasonable assumptions for the impacts on supplemental payments. Actual impacts may vary, as supplemental payments and SDPs may have different base payment rates and final payment rates. In addition, impacts likely would differ across States. We welcome comments on these assumptions and projected impacts.
We multiplied these percentages by supplemental payment spending by service to calculate the annual impact of the proposed rule. We also adjusted the estimates for the expected effective date of the proposed rule. We assumed that the FFS supplemental payment requirements of the proposed rule would go into effect in January 2029 and that these changes would first affect States in July 2029, at the beginning of most States' fiscal years. This adjustment reduced the effective impact by 75 percent for fiscal year 2029.
We project that the proposed rule would reduce total computable (Federal plus non-Federal shares) Medicaid spending by $2.44 billion from 2029 through 2035 (in real 2026 dollars).[99]
The annual impacts are shown in Table 27.
We project that the proposed rule would reduce Federal Medicaid spending by $1.54 billion from 2029 through 2035 (in real 2026 dollars). The annual impacts are shown in Table 28.
There are also impacts expected on State Medicaid expenditures. State expenditures would also decrease under the proposed rule, as States make fewer supplemental payments to providers. However, States may finance the non-Federal share of supplemental payments with provider taxes and IGTs. It is likely that the reduction in net State expenditures (State Medicaid payments minus revenue from provider taxes and IGTs) would be lower than the gross reduction in State Medicaid expenditures.
We project that the proposed rule would reduce State Medicaid spending by $0.90 billion from 2029 through 2035 (in real 2026 dollars). The annual impacts are shown in Table 29.
( printed page 30457)
We welcome comments on the projected impacts to the Federal government and States.
Providers would lose revenue as a result of reduced targeted practitioner payments under this proposal. However, as described previously, the net effect on providers may be less than the total quantified impact. To the extent providers may be paying provider taxes or IGTs that are used to support the non-Federal share for supplemental payments, the net change in provider revenue (supplemental payments minus provider taxes and IGTs) could be significantly less. We are unable to estimate the impacts on providers in more detail. We welcome comments on the impacts to providers.
As we noted previously, a major source of uncertainty is the relative prices paid between Medicaid, Medicare, and commercial payers. There is wide variation across services and States, and it is not clear how these prices compare for each targeted practitioner payment. Research on prices shows a wide range of outcomes as well. Thus, we have developed low and high scenarios to account for the potential differences in relative prices.
In the low scenario, we project that Medicaid spending would be reduced by $1.40 billion over 2029 through 2035 (in real 2026 dollars) under the proposed rule. Federal Medicaid spending would be $0.89 billion lower, and State Medicaid spending would be $0.51 billion lower. The annual impacts are shown in Table 30.
In the high scenario, we project that Medicaid spending would be reduced by $4.91 billion over 2029 through 2035 (in real 2026 dollars) under the proposed rule. Federal Medicaid spending would be $3.11 billion lower, and State Medicaid spending would be $1.80 billion lower. The annual impacts are shown in Table 31.
( printed page 30458)
We welcome comments on these scenarios.
There is substantial uncertainty regarding these estimates. First, these estimates rely on the supplemental payment data reported to us by the States, and there is limited information in these reports. It is possible that supplemental payments for these services could be higher or lower than shown here, and the distribution of spending across services may vary. There is also limited information on prices across payers. Most notably, there is very little information on average commercial reimbursement rates and how they compare to other payers. To the extent commercial rates are higher or lower relative to Medicare and Medicaid than we have assumed, these estimates may differ from the actual impacts if this proposal is implemented. This source of uncertainty is addressed in the range of estimates provided in this section. In addition, supplemental payments may grow faster or slower under current law than we have projected. We welcome any additional comments on these estimates.
4. Regulatory Review Cost Estimation
If regulations impose administrative costs on private entities, such as the time needed to read and interpret this proposed rule, we should estimate the cost associated with regulatory review. Due to uncertainty in quantifying the number of entities that will review the rule, we assume the following entities will review: State Medicaid Agencies, State governments, managed care plans, and some health care providers. We assume at least 3 people at every State Medicaid Agency (56) will review and two people in every State and territory government (56), for a total of 280 reviewers. It is more difficult to predict how many individuals in how many managed care plans and providers will review, so we are therefore utilizing our estimate from the 2024 Managed Care final rule of 415 reviewers, for a total of 695. We welcome any comments on the approach in estimating the number of entities which will review this proposed rule. We also recognize that different types of entities are affected differently by the SDP and FFS sections of this proposed rule, we nevertheless assume all reviewers will read the entire rule to confirm applicability and understanding. We seek comments on this assumption.
Using the wage information from the Bureau of Labor Statistics (BLS) for medical and health service managers (Code 11-9111), we estimate that the cost of reviewing this rule is $132.44 per hour, including overhead and fringe benefits (
https://www.bls.gov/oes/current/oes_nat.htm). Assuming an average reading speed, we estimate that it would take approximately 2 hours for staff to review this proposed rule. For each reviewer that reviews the rule, the estimated cost is $264.88 (2 hours × $132.44). Therefore, we estimate that the total cost of reviewing this regulation is $184,091.60 ($264.88 × 695).
D. Alternatives Considered
1. State Directed Payments (SDPs)
In developing the SDP provisions of this proposed rule, we considered several alternatives. This subsection provides a description of those alternatives and their estimated impacts, as available.
a. Methodology To Grandfather SDPs
One consideration was how to interpret the text of section 71116(b) of the WFTC legislation (Grandfathering Certain Payments): “. . . beginning with the rating period on or after January 1, 2028, the total amount of such payment shall be reduced by 10 percentage points each year until the total payment rate for such service is equal to the rate for such service specified in subsection (a).” We considered whether to interpret this to mean that the total payment rate, measured as a percentage of the total published Medicare payment rate, would be reduced by 10 percentage points annually (as opposed to the approach proposed in this rule, which reduces 100 percent of the grandfathered total dollar amount by 10 percentage points each year until reaching the limit).
We have estimated the impacts on Medicaid spending under this alternative. In this alternative scenario, we project that Medicaid spending would be reduced by $757.1 billion over 2026 through 2035 (in real 2026 dollars) under the proposed rule. Federal Medicaid spending would be $498.1 billion lower, and State Medicaid spending would be $258.7 billion lower. These impacts include only those on services subject to payment limits under section 71116 of the WFTC legislation. The annual impacts are shown in Table 32.
( printed page 30459)
Over 10 years, the impact on Medicaid spending is not projected to be substantially different under this alternative than the proposed approach ($757 billion and $774 billion, respectively). However, there are some other more significant differences under this alternative approach. First, while the overall impacts are similar, there may be larger differences between the two approaches for individual States. States with larger SDPs that are currently paid at a higher ratio of Medicare spending would likely see a smaller financial impact under this alternative option. In these cases, the 10-percentage point reduction in the ratio to Medicare would result in a smaller annual reduction in SDPs than the 10-percentage point reduction in the amount. Conversely, States with SDPs that are currently paid at a relatively lower rate compared to Medicare would likely see larger financial impacts over the first few years. Second, if SDPs are currently being paid at higher rates relative to Medicare than we have assumed in our estimates, the difference between the impact of the proposed approach and the alternative approach would be larger than shown here. In general, as the SDP payment rate relative to Medicare increases, the annual change in SDP spending would be lower under this alternative approach.
Third, under the proposed approach, we expect all SDPs will be reduced to the new limits within 10 years. However, under the alternative approach, we believe that it may not be until as late as 2075 that all SDP would be reduced to the new limits. For SDPs with higher payment rates, it is possible that the grandfathering period could take 40 to 50 years, or potentially longer if the difference between ACR and Medicare is larger than we have assumed.
b. Determination of SDPs Eligible to be Grandfathered
Another option we considered was determining which SDPs were eligible to be grandfathered. Section 71116(b) of the WFTC legislation provides criteria for grandfathering SDPs, “In the case of a payment described in section 438.6(c)(2)(iii) of title 42, Code of Federal Regulations (or a successor regulation) for which written prior approval (or a good faith effort to receive such approval, as determined by the Secretary) was made before May 1, 2025, or a payment described in such section for a rural hospital (as defined in subsection (d)(2)) for which written prior approval (or a good faith effort to receive such approval, as determined by the Secretary) was made by the date of enactment of this Act,
for the rating period occurring within 180 days of the date of the enactment of this Act. . .” (emphasis added). We have proposed interpreting this condition as 180 business days. However, we also considered whether to interpret this as 180 calendar days. If we were to use this alternative approach, we believe that at least eight additional SDPs would not qualify for the temporary grandfathering period (four new SDPs, and four renewals or amendments).
We have estimated the impacts on Medicaid spending under this alternative. In this alternative scenario, we project that Medicaid spending would be reduced by $778.7 billion over 2026 through 2035 (in real 2026 dollars) under the proposed rule. Federal Medicaid spending would be $514.2 billion lower, and State Medicaid spending would be $264.4 billion lower. These impacts include only those on services subject to payment limits under section 71116 of the WFTC legislation. Overall, we estimate that this alternative would reduce Medicaid spending over the next 10 years by $3.9 billion as compared to the proposed policy. The annual impacts are shown in Table 33.
( printed page 30460)
Under this alternative, the Medicaid spending reductions would be somewhat larger than under the proposed approach, given that several SDPs would not be eligible to be grandfathered.
2. FFS Provisions
In developing the FFS provisions of this proposed rule, we considered multiple alternatives. We considered, but did not propose, applying the targeted Medicaid practitioner payments limit to only physicians. Based on our experience reviewing SPAs and analyzing State expenditures, limiting only targeted Medicaid physician payments would address a large portion of targeted Medicaid payments. However, as previously described, our goal is to avoid a situation where unrestricted use of targeted practitioner payments continues under other practitioner types and when new practitioner types are authorized in statute under the Medicaid program, counter to the intent of this proposed rule.
We considered, but did not propose, limiting the targeted Medicaid payments to the Medicare equivalent of the ACR. Again, based on our experience reviewing SPAs, we have seen significant increases in the percentage of Medicare applied to practitioner payments since first approving ACR-based payments in the 2000s. We did not propose this because this policy would not address perpetual issues with the proprietary nature of commercial data as well as a continued burden on States to keep submitting demonstrations to CMS on a triennial basis.
We considered, but did not propose, establishing an aggregate limit (still tied to Medicare) on providers' Medicaid payments or a provider-level limit for Medicaid payments. This policy would create significant burden on States to develop UPL-like demonstrations for all Medicaid service payments, beyond the services currently subject to UPLs. Additionally, Medicaid has a number of unique services that Medicare does not cover or pay for; therefore, establishing a reasonable Medicare equivalent would not be possible for all services. However, we could have included a similar procedure to the one proposed under § 447.381(d), if we had proposed this alternative policy.
We considered, but did not propose, adding a demonstration requirement to the current proposal. However, due to the nature of the limit itself, we felt that the existing demonstration requirement for payments up to the ACR, or the Medicare equivalent of ACR, was no longer necessary.
We considered, but did not propose, that when a practitioner's or provider's payments (1) have no reasonable Medicare equivalent rate or (2) are reconciled to cost, total payments made to a practitioner or provider may not exceed 200 percent of the total fee-for service base payments authorized under the State plan. We invite comments on this alternative benchmark or other potential approaches.
Finally, we also considered, but did not propose, excluding payment rates that are uniform for a geographic region from paragraph (b), in which case they would fall within the scope of paragraph (c). In this instance the proposed limits in paragraph (c) would apply. We invite comments on this alternative policy or other potential approaches for these payments.
E. Accounting Statement and Table
Consistent with OMB Circular A-4 (available at
https://www.whitehouse.gov/wp-content/uploads/2025/08/CircularA-4.pdf), we have prepared an accounting statement in Table 34 showing the classification of the impact associated with the provisions of this rule. In the case of SDPs, we categorize these as transfers from the Federal government and States to health care providers and other relevant individuals (such as beneficiaries) and entities (such as State or local jurisdictions that reimburse providers for uncompensated care).
This provides our best estimates of the transfer payments outlined in the “Section C. Detailed Economic Analysis.” We present our best (or primary) estimate, as well as estimates for the low and high end of the ranges in this section. This range accounts for potential differences in relative prices paid by Medicaid, Medicare, and commercial payers and the variations across different services and States.
These impacts are discounted at 7 percent and 3 percent, respectively, as reflected in Table 34.
( printed page 30461)
( printed page 30462)
These transfers represent reductions in payments to providers and other individuals and entities (such as State or local jurisdictions that reimburse providers for uncompensated care) from the Federal government and the States. The majority of these projected reductions would be for hospitals, with some reductions for AMCs and nursing facilities, and smaller reductions for other provider types, including physicians.
F. Regulatory Flexibility Act (RFA)
The RFA requires agencies to analyze options for regulatory relief of small entities, if a rule has a significant impact on a substantial number of small entities. Individuals and States are not included in the definition of a small entity. The entities this proposed rule would regulate, if finalized, are State governments, and therefore this proposed rule, if finalized, will not have a significant economic impact on a substantial number of small businesses or other small entities.
Furthermore, because the policy operates at the State level and SDPs are ultimately optional for States to implement, we do not have data that would allow us to reliably attribute or disaggregate these impacts to specific provider types or to small entities as defined by SBA size standards (for example, by NAICS codes or employer status). In addition, any effects on providers would be indirect and mediated through State-level policy. For these reasons, we cannot estimate impacts across disaggregated small entity sizes and apply thresholds for “significant impact” and “substantial number” at the small entity level. We also cannot estimate how managed care plan market negotiations with providers may ameliorate the impact of this rule. Nevertheless, we have considered the potential for indirect effects on providers, including small entities, to the extent feasible using available data, and these effects are reflected in the RIA, section IV of this proposed rule. We welcome any information from the public that could help us better assess potential downstream effects on small entities.
G. Unfunded Mandates Reform Act (UMRA)
Section 202 of the Unfunded Mandates Reform Act of 1995 (UMRA) also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2026, that threshold is approximately $193 million.
H. Federalism
Executive Order 13132 establishes certain requirements that an agency must meet when it issues a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on State and local governments, preempts State law, or otherwise has Federalism implications. This proposed rule would not impose substantial direct requirement costs on State and local governments, preempt State law, or otherwise have Federalism implications.
Executive Order 14192, entitled “Unleashing Prosperity Through Deregulation” was issued on January 31, 2025, and requires that “any new incremental costs associated with new regulations shall, to the extent permitted by law, be offset by the elimination of existing costs associated with at least 10 prior regulations.” This proposed rule, if finalized as proposed, is expected to be exempt from otherwise-applicable requirements of Executive Order 14192, per footnote 1 of OMB's Accounting Methods.[100]
We estimate that this proposed rule would generate $0.13 million in annualized cost savings at a 7 percent discount rate relative to year 2024, over a perpetual time horizon.
V. Response to Comments
Because of the large number of public comments we normally receive on
Federal Register
documents, we are not able to acknowledge or respond to them individually. We will consider all comments we receive by the date and time specified in the
DATES
section of this preamble, and, when we proceed with a subsequent document, we will respond to the comments in the preamble to that document.
In accordance with the provisions of Executive Order 12866, this regulation was reviewed by the Office of Management and Budget.
Mehmet Oz, Administrator of the Centers for Medicare & Medicaid Services, approved this document on May 15, 2026.
Business day
means Monday through Friday, excluding the Federal holidays as determined under 5 U.S.C. 6103.
* * * * *
3. Section 438.6 is amended—
a. In paragraph (a) by adding the definitions for “Completed preprint”, ”Expansion State”, “Grandfathered State directed payment”, “Grandfathered total dollar amount,” “Non-Expansion State”, “Payment limit”, “Preprint”, “State”, and “State plan approved rates” in alphabetical order; and
b. By revising paragraphs (c)(1)(iii)(A), (B), (c)(2)(i), (ii)(A) and (I), (iii) (c)(3)(ii), introductory text in paragraphs (c)(5)(iii)(A) through E and (8); and
Completed preprint
means a State directed payment preprint with all relevant sections of the preprint filled out, and all information provided only in the fillable sections of the preprint and the published addendum tables, as applicable.
* * * * *
Expansion State
means a State that has elected to provide medical assistance to all individuals described in section 1902(a)(10)(A)(i)(VIII) of the Act under a State plan under title XIX of the Act or under a waiver of the plan that provides minimum essential coverage as defined in section
( printed page 30463)
5000A(f)(1)(A) of the Internal Revenue Code of 1986.
* * * * *
Grandfathered State directed payment
means a State directed payment for inpatient hospital services, outpatient hospital services, nursing facility services, or qualified practitioner services at academic medical centers that meets all of the following:
(1) Receives written prior approval under paragraph (c)(2)(i) of this section.
(2) Is for a rating period that includes at least 1 business day between—
(i) October 11, 2024 and July 3, 2025; or
(ii) July 5, 2025 and March 27, 2026.
(3) Was described in a completed preprint with an eligible rating period and documented total dollar amount that was submitted to CMS on or before July 4, 2025.
(4) Exceeds the payment limit set forth in paragraph (c)(8) of this section.
Grandfathered total dollar amount
means the total dollar amount approved by CMS for a Grandfathered State directed payment. When preprint submissions of the same State directed payment for different rating periods meet the definition of a Grandfathered State directed payment, the highest total dollar amount approved by CMS is the Grandfathered total dollar amount for that State directed payment.
* * * * *
Non-Expansion State
means a State that does not meet the definition of Expansion State as specified in paragraph (a) of this section.
* * * * *
Payment limit
means—
(1) As applicable, one of the following:
(i) 100 percent of the total published Medicare payment rate for an Expansion State.
(ii) 110 percent of the total published Medicare payment rate for a Non-Expansion State.
(iii) Only in instances when there is no total published Medicare payment rate for the covered service, 100 percent of the State plan approved rate.
* * * * *
Preprint
means the template published by CMS for use by States to request written prior approval of a State directed payment.
* * * * *
State
as used in paragraph (c)(8)(ii) of this section only, and only until the first rating period beginning on or after January 1, 2029, means the Single State Agency of 1 of the 50 States or the District of Columbia. At other times and for other purposes in this section, unless otherwise specified,
State
has the meaning given the term in § 438.2 of this part.
State plan approved rates
means amounts calculated for specific services identifiable as having been provided to an individual beneficiary described under rate methodologies in the Medicaid State plan approved by CMS before the start of the rating period. Supplemental payments contained in a State plan are not, and do not constitute, State plan approved rates.
* * * * *
(c) * * *
(1) * * *
(iii) * * *
(A) For rating periods beginning on or after July 9, 2024 and before January 1, 2028:
(
1) Adopt a minimum fee schedule for providers that provide a particular service under the contract using State plan approved rates.
(
2) Adopt a minimum fee schedule for providers that provide a particular service under the contract using a total published Medicare payment rate that was in effect no more than 3 years prior to the start of the rating period and the minimum fee schedule is equivalent to 100 percent of the total published Medicare payment rate.
(
3) Adopt a minimum fee schedule for providers that provide a particular service under the contract using rates other than the State plan approved rates or one or more total published Medicare payment rate described in paragraph (c)(1)(iii)(A)(
2) of this section.
(
4) Provide a uniform dollar or percentage increase for providers that provide a particular service under the contract.
(5) Adopt a maximum fee schedule for providers that provide a particular service under the contract, so long as the MCO, PIHP, or PAHP retains the ability to reasonably manage risk and has discretion in accomplishing the goals of the contract.
(B) For rating periods beginning on or after January 1, 2028, adopt one or both of the following:
(1) A minimum fee schedule for providers that provide a particular service under the contract and the minimum fee schedule is no greater than the payment limit.
(2) A maximum fee schedule for providers that provide a particular service under the contract and the maximum fee schedule is no greater than the payment limit, so long as the MCO, PIHP, or PAHP retains the ability to reasonably manage risk and has discretion in accomplishing the goals of the contract without exceeding the payment limit.
* * * * *
(2) * * *
(i) State directed payments specified in paragraphs (c)(1)(i) and (ii), (c)(1)(iii)(A)(
3) through (
5)of this section must be submitted to CMS using a preprint and have written prior approval that the standards and requirements in this section are met.
(ii) * * *
(A) Be based only on the utilization and delivery of services furnished by a provider that provides a particular service under the contract;
* * * * *
(I) Not exceed the payment limit set forth in paragraph (c)(8) of this section; and
* * * * *
(iii) Grandfathered State directed payments are eligible to delay compliance with the payment limit set forth in paragraph (c)(8) of this section. The following is applicable to all Grandfathered State directed payments:
(A) For each rating period beginning on or after July 4, 2025 and before January 1, 2028, renewals of or amendments to a Grandfathered State directed payment may not exceed the Grandfathered total dollar amount.
(B) For each rating period beginning on or after January 1, 2028, the State must decrease 100 percent of the Grandfathered total dollar amount by at least 10 percentage points annually, until the payment limit in paragraph (c)(8) of this section is met.
(C) The total payment rate for State directed payments in paragraphs (c)(2)(iii)(A) and (B) of this section must not exceed the average commercial rate. States must submit all of the following for each Grandfathered State directed payment until the first rating period beginning on or after January 1, 2029:
(
1) The average commercial rate demonstration, for which States must use payment data that meets all of the following:
(
i) Is specific to the State.
(
ii) Is no older than from the 3 most recent and complete years prior to first rating period beginning on or after July 9, 2024.
(
iii) Is specific to each service(s) addressed by the State directed payment.
(
iv) Includes the total reimbursement by the third-party payer and any patient liability, such as cost sharing and deductibles.
(
v) Excludes payments to FQHCs, RHCs, and from any non-commercial payers, such as Medicare.
(
vi) Excludes any payment data for services or codes that the applicable Medicaid MCOs, PIHPs, or PAHPs do not cover.
( printed page 30464)
(
2) A total payment rate comparison, for which States must provide a comparison of the total payment rate for these services included in the State directed payment to the average commercial rate that meets all of the following:
(
i) Is specific to each managed care program that the State directed payment applies.
(
ii) Is specific to each provider class to which the State directed payment applies.
(
iii) Is projected for the rating period for which the State is seeking approval of the State directed payment under paragraph (c)(2)(i) of this section.
(
iv) Uses payment data that are specific to each service included in the State directed payment.
(
v) Describes each of the components of the total payment rate as a percentage of the average commercial rate (demonstrated by the State as provided in paragraph (c)(2)(iii)(C)(1) of this section) for each of the services included in the State directed payment.
(
3)(
i) The ACR demonstration described in paragraph (c)(2)(iii)(C)(
1) of this section must be included with the initial documentation submitted for written prior approval of the State directed payment under paragraph (c)(2)(i) of this section, and then subsequently updated at least once every 3 years thereafter until the payment limit set forth in paragraph (c)(8) of this section is met.
(
ii) The total payment rate comparison described in paragraph (c)(2)(iii)(C)(2) of this section must be included with the documentation submitted for written prior approval under paragraph (c)(2)(i) of this section and updated with each amendment and subsequent renewal.
(D) Beginning with the first rating period on or after January 1, 2027, the State must annually submit in the form and manner prescribed by CMS for each Grandfathered State directed payment a total payment rate comparison, certified by an actuary, for services included in the State directed payment as a percentage of the most recent total published Medicare payment rate, or State plan approved rate only when no total published Medicare payment rate exists for the covered service. This total payment rate comparison must be submitted until the first rating period the payment limit in paragraph (c)(8) of this section is met.
(E) The State may require the MCO, PIHP or PAHP to provide a uniform dollar or percentage increase for providers that provide a particular service under the contract until the first rating period the payment limit in paragraph (c)(8) of this section is met. Once the payment limit is met, the State must comply with paragraph (c)(1)(iii) of this section.
(F) The State may delay compliance with paragraphs (c)(2)(viii) and (c)(6) of this section until the first rating period the payment limit is met.
* * * * *
(3) * * *
(ii) Written prior approval of a State directed payment adopting a minimum fee schedule, uniform increase, or maximum fee schedule described in paragraph (c)(1)(iii) of this section is for one rating period.
* * * * *
(5) * * *
(iii) * * *
(A) For State directed payments adopting a minimum fee schedule described in paragraph (c)(1)(iii)(A)(1), (2), and (3) or (c)(1)(iii)(B)(1) of this section:
* * * * *
(B) For State directed payments providing a uniform increase described in paragraph (c)(1)(iii)(A)(4) of this section:
* * * * *
(C) For State directed payments adopting a maximum fee schedule described in paragraph (c)(1)(iii)(A)(5) or (B)(2) of this section:
* * * * *
(D) For State directed payments implementing value-based purchasing models or participating in a multipayer or Medicaid-specific delivery system reform or performance improvement initiative described in paragraph (c)(1)(i) and (ii) of this section that condition payment based upon performance:
* * * * *
(E) For State directed payments implementing value-based purchasing models or participating in a multipayer or Medicaid-specific delivery system reform or performance improvement initiative described in paragraph (c)(1)(i) and (ii) of this section using a population-based or condition-based payment as defined in paragraph (a) of this section:
* * * * *
(8)
Payment limits.
For rating periods beginning as follows—
(i) On or after July 9, 2024 until the first rating period beginning on or after January 1, 2029, a State as defined in § 438.2 of this part must:
(A) Ensure that the total payment rate for each service and provider class included in the State directed payment must be reasonable, appropriate, and attainable; and
(B) Upon request from CMS, the State must provide documentation demonstrating the total payment rate for each service and provider class.
(ii) On or after July 4, 2025, a State as defined in § 438.6(a) of this part may not exceed the payment limit for each inpatient hospital service, outpatient hospital service, qualified practitioner service at an academic medical center, or nursing facility service covered under a State directed payment described in paragraph (c)(2)(i) of this section. To demonstrate compliance with the payment limit, the State must submit all of the following:
(A)(
1) A list of all providers eligible for the State directed payment and their National Provider Identifiers, the total published Medicare payment rate or State plan approved rate (when no total published Medicare payment rate exists for the covered service) that serves as the basis of the payment limit for each service covered under the State directed payment; and
(
2) A detailed description of how the State will ensure that payment to each provider for each furnished service does not exceed the payment limit.
(B) For State directed payments described in paragraphs (c)(1)(i) and (ii) of this section, a detailed validation methodology that the State will implement to ensure that payment under such SDPs does not exceed the payment limit on a per service basis.
(C) Any additional documentation requested by CMS to demonstrate compliance with the limit.
(iii) On or after January 1, 2029, a State as defined in § 438.2 of this part must not exceed the payment limit for each service covered under a State directed payment. To demonstrate compliance with the payment limit, upon request from CMS, the State must submit all of the following:
(A)(
1) A list of all providers eligible for the State directed payment and their National Provider Identifiers, the total published Medicare payment rate or State plan approved rate (when no total published Medicare payment rate exists for the covered service) that serves as the basis of the payment limit for each service covered under the State directed payment; and
(
2) A detailed description of how the State will ensure that payment to each provider for each furnished service does not exceed the payment limit.
(B) For State directed payments described in paragraphs (c)(1)(i) and (ii) of this section, a detailed validation methodology to ensure that payment under the SDPs does not exceed the payment limit on a per service basis.
(C) Any additional documentation requested by CMS to demonstrate compliance with the limit.
( printed page 30465)
(9)
Provision of additional guidance.
CMS issues guidance, as needed, including all of the following:
(i) Federal requirements and standards for the State directed payment.
(ii) The documentation required to determine that the State directed payment has been developed in accordance with the requirements of this part.
(iii) Any considerations for applicability of the payment limit.
(iv) The documentation required to demonstrate compliance with the payment limit.
(v) Any updates or developments in the State directed payment review process to facilitate prompt CMS review.
(vi) Any considerations for state monitoring, oversight, and evaluation of the State directed payment.
(10)
Applicability dates.
States must comply with the specified requirements in accordance with the applicability dates as follows:
(i) Paragraph (a), except for the definition of “State plan approved rates,” and paragraphs (c)(1), (c)(1)(iii), (c)(2)(i), (c)(2)(ii)(A) through (C), (c)(2)(ii)(E), (c)(2)(ii)(G), (c)(2)(ii)(I) and (J), (c)(2)(vi)(A), and (c)(3) of this section as contained in 42 CFR part 438, applicable beginning on July 9, 2024.
(ii) Paragraphs (c)(2)(iii), (c)(2)(vi)(B), and (c)(2)(vi)(C)(
1) and (
2) of this section no later than the first rating period for contracts with MCOs, PIHPs and PAHPs beginning on or after July 9, 2024.
(iii) Paragraphs (c)(2)(vi)(C)(
3) and (
4),
(c)(2)(viii), and (c)(5)(i) through (iv) of this section no later than the first rating period for contracts with MCOs, PIHPs, and PAHPs beginning on or after 2 years after July 9, 2024.
(iv) Paragraphs (c)(2)(ii)(D) and (F), (c)(2)(iv), (c)(2)(v), (c)(2)(vii), (c)(6), and (c)(7) of this section no later than the first rating period for contracts with MCOs, PIHPs, and PAHPs beginning on or after 3 years after July 9, 2024.
(v) Paragraph (c)(5)(v) of this section no later than the first rating period for contracts with MCOs, PIHPs, and PAHPs beginning on or after 4 years after July 9, 2024.
(vi) Paragraph (c)(4) of this section no later than the date specified in the T-MSIS reporting instructions released by CMS.
(vii) Notwithstanding paragraph (c)(10)(i) of this section, State plan approved rates as defined in paragraphs (a) and (c)(2)(ii)(H) of this section no later than the first rating period for contracts with MCOs, PIHPs, and PAHPs beginning on or after January 1, 2028.
* * * * *
PART 447—PAYMENTS FOR SERVICES
3. The authority citation for part 447 is revised to read as follows:
(a)
General.
This section establishes a Medicaid practitioner or provider-specific limit for the total Medicaid fee-for-service payment authorized under the State plan or waiver in instances where all or a portion of the payment is targeted to a subset of participating practitioners or providers furnishing the applicable Medicaid-covered services.
(b)
Scope.
The limit in paragraph (c) of this section does not apply if either of the following applies:
(1) A State's Medicaid fee-for-service payment methodologies for Medicaid-covered services not described in paragraph (b)(2) of this section are uniform for all Medicaid practitioners or providers furnishing the applicable Medicaid-covered services within the State, or within a geographic region of the State (that is, county, parish, borough, or municipality) that is referenced under a payment methodology specified in the State plan.
(2) The Medicaid practitioner's or provider's total Medicaid fee-for-service payment for a Medicaid-covered service is already subject to a payment limit under §§ 447.271, 447.272, 447.321, or 447.325, and sections 1903(i)(7) or 1903(i)(27) of the Act, but only to the extent that the practitioner's or provider's total payments are subject to such other limit.
(c)
Targeted Medicaid payment limit.
A State's Medicaid State plan fee-for-service payment methodology must specify that, except as provided in paragraph (b) of this section, total Medicaid payments made to a Medicaid practitioner or provider for a Medicaid-covered service may not exceed the percentages, listed in paragraphs (c)(1) and (2) of this section, of the Medicare fee-for-service payment rate that would be paid to the practitioner or provider for the service if it were paid under the applicable Medicare payment rates established under Parts A and B of Title XVIII of the Act effective for the FFY or CY, as applicable, that corresponds to the State plan rate year. For this purpose, the State plan rate year is the first State plan rate year that begins during the FFY or CY in which the Medicare payment rate is in effect. For Medicaid payment rates subject to a statutory requirement for a particular payment rate or methodology, the limit under this paragraph may not be less than the required Medicaid payment rate or the rate calculated under the required methodology.
(1) For an Expansion State as defined in § 438.6(a), 100 percent.
(2) For a Non-expansion State as defined in § 438.6(a), 110 percent.
(d)
Exceptions.
In either of the following instances, the limit described in paragraph (c) of this section does not apply. Upon request, the State must explain and provide supporting information in the form and manner specified by CMS sufficient to demonstrate that the payments are consistent with section 1902(a)(30)(A) of the Act:
(1) If there is no reasonable Medicare equivalent payment rate.
(2) If payments are reconciled to a practitioner's or provider's actual, incurred cost.
(e)
Transition period.
States with approved State plan payments that exceed the limit under paragraph (c) of this section to which an exception in paragraph (d) of this section does not apply must submit a State plan amendment to remove these payments or update them to comply with the limit in paragraph (c) of this section, with an effective date no later than the start of the first State fiscal year that begins on or after January 1, 2029.
(f)
Compliance with the targeted Medicaid payment limit.
(1) For States that fail to comply with the requirements of this section, future grant awards may be reduced under the procedures set forth at 42 CFR part 430, subparts C and D by the amount of FFP that CMS estimates is attributable to the portion of payments that exceed the limit established in paragraph (c) of this section.
( printed page 30466)
(2) State plan amendments that propose to exceed the limit under paragraph (c) of this section, to which an exception in paragraph (d) of this section does not apply, are subject to State plan amendment disapproval under § 430.15(c) of this chapter, as would State plan amendments for payments to which an exception in paragraph (d) of this section does apply, and for which a State does not furnish the information requested by CMS to determine the payment is economic and efficient.
Robert F. Kennedy, Jr.,
Secretary, Department of Health and Human Services.
Footnotes
1.
The use of the term “State” refers to all 50 states, the District of Columbia and the territories unless otherwise noted.
11.
Throughout this document, the use of the term “managed care plan” includes MCOs, PIHPs, and PAHPs, and is only used when a reference applies to all three arrangements. An explicit reference is used if the provision applies to primary care case management (PCCM) or PCCM entities.
13.
SDPs that use minimum fee schedules for providers that provide a particular service under the contract using State plan approved rates as defined in § 438.6(a), or using a total published Medicare payment rate that was in effect no more than 3 years prior to the start of the rating period are not subject to the written prior approval requirement in § 438.6(c)(2)(i); however, they must comply with the requirements currently in § 438.6(c)(2)(ii)(A) through (J) (other than the requirement for written prior approval) and be appropriately documented in the managed care contract(s) and rate certification(s).
24.
U.S. Government Accountability Office, “CMS Needs More Information on States' Financing and Payment Arrangements to Improve Oversight,” December 7, 2020, available at
https://www.gao.gov/assets/gao-21-98.pdf.
26.
U.S. Government Accountability Office, “Medicaid Managed Care: Rapid Spending Growth in State Directed Payments Needs Enhanced Oversight and Transparency,” December 14, 2023, available at
https://www.gao.gov/assets/gao-24-106202.pdf.
33.
We initially referred to physicians specifically but later expanded to “practitioners” to account for the practitioners other than physicians that provide professional services.
39.
These examples include preprints submitted by States to CMS but do not necessarily represent approved SDPs; CMS does not approve SDPs that exceed 100 percent of the ACR.
40.
This is based on an analysis conducted in June 2025 of 402 SDPs approved by CMS between January 1, 2022 and December 31, 2024 where the total payment rate was projected to exceed Medicare payment rates or up to the ACR. The analysis excludes (1) COVID-19 expedited reviews and (2) SDP arrangements related to HCBS covered by section 9817 of the American Rescue Plan Act of 2021 and (3) SDPs where the State projected the total payment rate to be less than or equal to Medicare and (4) that total payment rate was not compared to the Medicare or ACR.
41.
Medicare+Choice is the former name for Medicare Advantage, as it was renamed by the Medicare Prescription Drug, Improvement, and Modernization Act of 2003.
43.
“Rating period” is defined at § 438.2 as a period of 12 months selected by the State for which the actuarially sound capitation rates are developed and documented in the rate certification submitted to CMS as required by § 438.7(a).
45.
If Congress had intended instead to specify an alternative rate of 110 percent of the payment rate under the Medicaid State plan in the case of a Non-Expansion State, this could have been done, for example, by specifying “(or, in the absence of a total published Medicare payment rate, of the payment rate under a Medicaid State plan (or under a waiver of such plan))” in section 71116(a)(2) of the WFTC legislation.
48.
States are required to comply with all of relevant regulatory requirements in § 438.7(c), including the requirements at §§ 438.7(c)(2) and 438.7(c)(5). These provisions outline the requirements for retroactive adjustments to the capitation rates.
56.
We use the term “base payments” to mean the rates the MCO, PIHP, or PAHP negotiated with the providers. This is consistent with language used in the definition of “uniform increase” at § 438.6(a).
57.
The Medicaid Managed Care Rate Development Guide outlines documentation requirements for rate certifications related to overpayments (see section I, Item 3.B.ii.).
59.
Holidays include the 12 Federal holidays, including Inauguration Day, as recognized by OPM (
https://www.opm.gov/policy-data-oversight/pay-leave/federal-holidays). Federal government closures by Executive Order are also applicable to this timeframe. Those known at the time of proposed rule publication include December 24, 2024, January 9, 2025, December 24, 2025 and December 26, 2025.
67.
In accordance with § 438.6(c)(2)(iii)(C) the ACR demonstration must be included with the initial documentation submitted for a SDP, and then subsequently updated at least once every 3 years thereafter as long as the State continues to renew the SDP. The total payment rate comparison must be included and updated with each preprint amendment and subsequent renewal.
68.
In this example, the total dollar amount of managed care plan base payments (before the SDP) is $1,600,000,000 per year, and the total dollar amount of Medicare payments according to published rates is $2,000,000,000 per year.
70.
At least two States have submitted over a dozen individual SDP preprints, each with a single provider class and only one eligible provider in that class.
89.
For HCBS more broadly, although in many instances these are not covered by Medicare, Medicaid rates for these services are reviewed under State plan and waiver authorities.
96.
Laura Skopec, Avani Pugazhendhi, Stephen Zuckerman, “Updated Medicaid-to-Medicare Fee Index: Medicaid Physician Fees Still Lag Behind Medicare Physician Fees,” Health Affairs, vol. 44, no. 5, May 2025,
https://www.healthaffairs.org/doi/10.1377/hlthaff.2024.01530.
98.
In this section, we will repeatedly refer to supplemental payments as we did in the “Background” section of this proposed rule, as this terminology is used internally related to the data used to populate these estimates.
99.
In this section, we use real 2026 dollars to align with estimates in other sections and consistency in the calculations in the Regulatory Impact Analysis.