Medicare Program; Strengthening Oversight of Accrediting Organizations (AOs) and Preventing AO Conflicts of Interest, and Related Provisions
This final rule with comment period sets forth provisions to strengthen the oversight of Medicare national accrediting organizations by addressing conflicts of interest, establi...
Centers for Medicare & Medicaid Services (CMS), Department of Health and Human Services (HHS).
ACTION:
Final rule with comment period.
SUMMARY:
This final rule with comment period sets forth provisions to strengthen the oversight of Medicare national accrediting organizations by addressing conflicts of interest, establishing consistent standards, processes, and definitions, and updating the validation and performance standards systems. Additionally, this final rule with comment period revises the psychiatric hospital survey process, adds a limitation on terminated deemed providers and suppliers when reentering the program, and provides technical corrections for End-Stage Renal Disease facilities and Transplant Programs.
DATES:
Effective date:
These regulations are effective on June 16, 2027.
Comment date:
To be assured consideration, comments on sections VI., “Collection of Information” and VII., “Regulatory Impact Analysis” must be received at one of the addresses provided below, by August 17, 2026.
ADDRESSES:
In commenting, please refer to file code CMS-3367-FC.
Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
2.
By regular mail.
You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-3367-FC, P.O. Box 8010, Baltimore, MD 21244-8010.
Please allow sufficient time for mailed comments to be received before the close of the comment period.
3.
By express or overnight mail.
You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-3367-FC, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore, MD 21244-1850.
For information on viewing public comments, see the beginning of the
SUPPLEMENTARY INFORMATION
section.
Inspection of Public Comments:
All comments received before the close of the comment period are available for viewing by the public, including any personally identifiable or confidential business information that is included in a comment. We post all comments received before the close of the comment period on the following website as soon as possible after they have been received:
https://www.regulations.gov.
Follow the search instructions on that website to view public comments. CMS will not post on
Regulations.gov
public comments that make threats to individuals or institutions or suggest that the commenter will take actions to harm an individual. CMS continues to encourage individuals not to submit duplicative comments. We will post acceptable comments from multiple unique commenters even if the content is identical or nearly identical to other comments.
Table of Contents
I. Executive Summary
A. Purpose
B. Summary of the Major Provisions
II. Background
A. Legislative History
B. Regulatory Overview of CMS' Rules Regarding AO Programs
C. Congressional Report on the Oversight of National AOs and CMS-Approved Accreditation Programs
D. CMS Validation Survey Pilot
E. Overview of Transparency and Oversight of Accrediting Organizations
F. Prior Rulemaking—Accrediting Organizations Conflicts-of-Interest Request for Information (RFI)
G. Conflicts of Interest—The AO Owner's, Surveyor's and Other Employee's Interest in or Relationship With a Healthcare Facility That the AO Accredits
H. Public Comment on Whether it Is a Conflict of Interest for AO Board Members or Advisors To Have an Interest in, or Relationship With, a Healthcare Facility That the AO Accredits
III. Summary of the Proposed Provisions, Public Comments, and Responses to Comments on the Proposed Rule
A. General Comments in Support of the Proposed Rule
B. Comments Expressing General Opposition to the Proposed Rule
C. Add Definition of “Unannounced Survey” to § 488.1
D. Conflicts of Interest
E. Comments on the Proposed Requirement That AOs Obtain and Submit Surveyor Declarations of Any Interest in and Relationships With Healthcare Providers the AO Accredits to CMS on an Annual Basis (Proposed § 488.5(a)(22))
F. Proposed Restrictions on Fee-Based Consulting Services Provided by AOs to the Medicare-Certified Providers and Suppliers They Accredit (Proposed § 488.8(i))
G. Require AOs To Provide CMS With Information About the Fee-Based Consulting They Provide (Proposed § 488.8(i)(5))
H. Actions Against AOs Found To Be Providing AO Fee-Based Consulting Services to the Healthcare Providers or Suppliers They Accredit in Violation of the Restrictions in § 488.5(i)(1) Through § 488.5(i)(3) (Proposed § 488.8(i)(6))
I. Require Accrediting Organizations To Have Written Fee-Based Consulting Firewall Policies and Procedures (§ 488.8(j))
J. Prohibit AO Owners, Surveyors, and Other Employees From Involvement With the Survey and Accreditation Process for Healthcare Facilities With Which They Have an Interest or Relationship (§ 488.8(k))
K. Require the AOs That Accredit Medicare-Certified Providers and Suppliers To Use Medicare Conditions; and Strengthened Survey Process Comparability (Proposed § 488.4(a)(1) and (2))
L. Revise the Crosswalk Requirements at § 488.5(a)(3)
M. Strengthen the Comparability of the Survey Process Between the AOs and the States
N. Revise the AO Application Documentation Requirements Related to the Survey Processes (§ 488.5(a)(4); § 488.5(a)(4)(iii); § 488.5(a)(4)(v); § 488.5(a)(4)(vii); § 488.5(a)(4)(xi); § 488.5(a)(5); § 488.5(a)(6); § 488.5(a)(12); § 488.5(a)(13))
O. Revisions to § 488.5(a)(4)(v) (Survey Review Process)
P. Revision to § 488.5(a)(4)(vii) (Correction of Identified Non-Compliance)
Q. Revisions to § 488.5(a)(4)(xi) (AO Training and Education Programs)
R. Revisions to § 488.5(a)(5) (Composition of Survey Team)
S. Revisions to § 488.5(a)(6) (Adequate Number of Surveyors for Size of Facility)
T. Revisions to § 488.5(a)(12) (Complaint Survey Documentation Requirements)
U. Revisions to Accreditation Decision-Making Policies and Reporting § 488.5(a)(13)
V. Require AOs To Provide CMS With Survey Findings (§ 488.5(a)(4)(viii)(A))
( printed page 36371)
W. Require That AO Surveyors Must Take the CMS Online Surveyor Basic Training (§ 488.5(a)(8))
X. Establish Criteria for “National in Scope” (§ 488.1)
Y. Revise the Definition of “Rate of Disparity” and To Use the Process and Outcome Disparity Rates and Performance Measures (§ 488.1)
Z. Require AOs To Submit a Publicly Reportable Plan of Correction for Unacceptable Performance Measure Scores (§§ 488.8(a)(2) and (4))
AA. Revisions to the AO Survey Validation Program (§ 488.9)
BB. Revise the Psychiatric Hospital Survey Process
CC. Limitation on Terminated Deemed Providers/Suppliers Seeking Re-Entry Into Medicare/Medicaid (§ 489.57, § 488.4(b) and § 488.5(a)(21))
DD. Finalizing Technical Correction for End-Stage Renal Disease (ESRD) Facilities and Kidney Transplant Programs (§ 488.4(a)(4))
IV. Information Regarding Timeframes and Expectation for the Submission of AO Applications
V. Severability of Provisions
VI. Collection of Information Requirements
A. Information Collection Requirements (ICRs) Related to Conflict-of-Interest Requirements
B. ICR Associated With the Requirement That AOs Provide Detailed Crosswalks Identifying Incorporation of the CMS Standards
C. ICRs Associated With the Requirement That AOs Use Survey Processes That Are Comparable to Those Used by CMS and the SAs
D. ICRs Associated With the Establishment of a Definition for “National in Scope”
E. ICR Associated With the Revision of the AO Performance Measures and To Require a Publicly Reportable Plan of Correction
F. Summary of Estimated Burden
VII. Regulatory Impact Analysis
A. Statement of Need
B. Overall Impact
C. Detailed Economic Analysis
D. Alternatives Considered
E. Regulatory Flexibility Act (RFA)
F. Unfunded Mandates Reform Act (UMRA)
G. Federalism
H. E.O. 14192 “Unleashing Prosperity Through Deregulation”
VIII. Waiver of Notice of Proposed Rulemaking
IX. Response to Comments
I. Executive Summary
A. Purpose
The Centers for Medicare & Medicaid Services (CMS) seeks to protect the health and safety of all patients who receive services from Medicare- and Medicaid-participating providers and suppliers, including those facilities that are accredited by CMS-approved accrediting organizations (AOs). We continue to review and revise our patient health and safety requirements and our survey process requirements to ensure that these regulations effectively drive the quality and safety of the care our beneficiaries and all patients receive from these accredited providers and suppliers.
In 2015, we published a final rule in the
Federal Register
entitled, “Medicare and Medicaid Programs: Revisions to Deeming Authority Survey, Certification, and Enforcement Procedures” (80 FR 29796), hereinafter referred to as the “2015 AO final rule” to clarify and strengthen the oversight of AOs, specifically to provide additional criteria for AOs that apply for, and are granted, recognition and approval of an accreditation program (see section “II. Background” of this final rule with comment period for additional background information). Since 2015, CMS has continued to evaluate the effectiveness of these regulatory changes and the performance of AOs. In our proposed rule, published February 15, 2024 (89 FR 11996), we proposed multiple provisions to further strengthen our oversight and enforcement capabilities of the AOs. The need for these provisions is based on multiple factors, which include: (1) direct observation and review of the AOs' accreditation programs for those AOs with CMS-approved deeming programs; (2) media reports and complaints against facilities that are deemed; (3) the CMS validation program and analysis of disparity rates between State survey agencies (SAs) and the AOs; and (4) our performance evaluations of AOs. Section IV. of the proposed rule discussed each of the proposed provisions. More specifically, the preamble provided background and analysis of why CMS proposed additional provisions and revisions to existing requirements. CMS is responsible for the oversight of the national AOs' Medicare accreditation programs, and for ensuring that providers or suppliers under CMS-approved deeming programs by the AOs meet the baseline quality and patient safety standards required by the Medicare conditions (please refer to section “II. Background” of this final rule with comment period for additional information). Based on several years of experience and data analysis, we proposed the revisions and the new requirements in the February 15, 2024, proposed rule to strengthen our oversight of AOs.
B. Summary of the Major Provisions
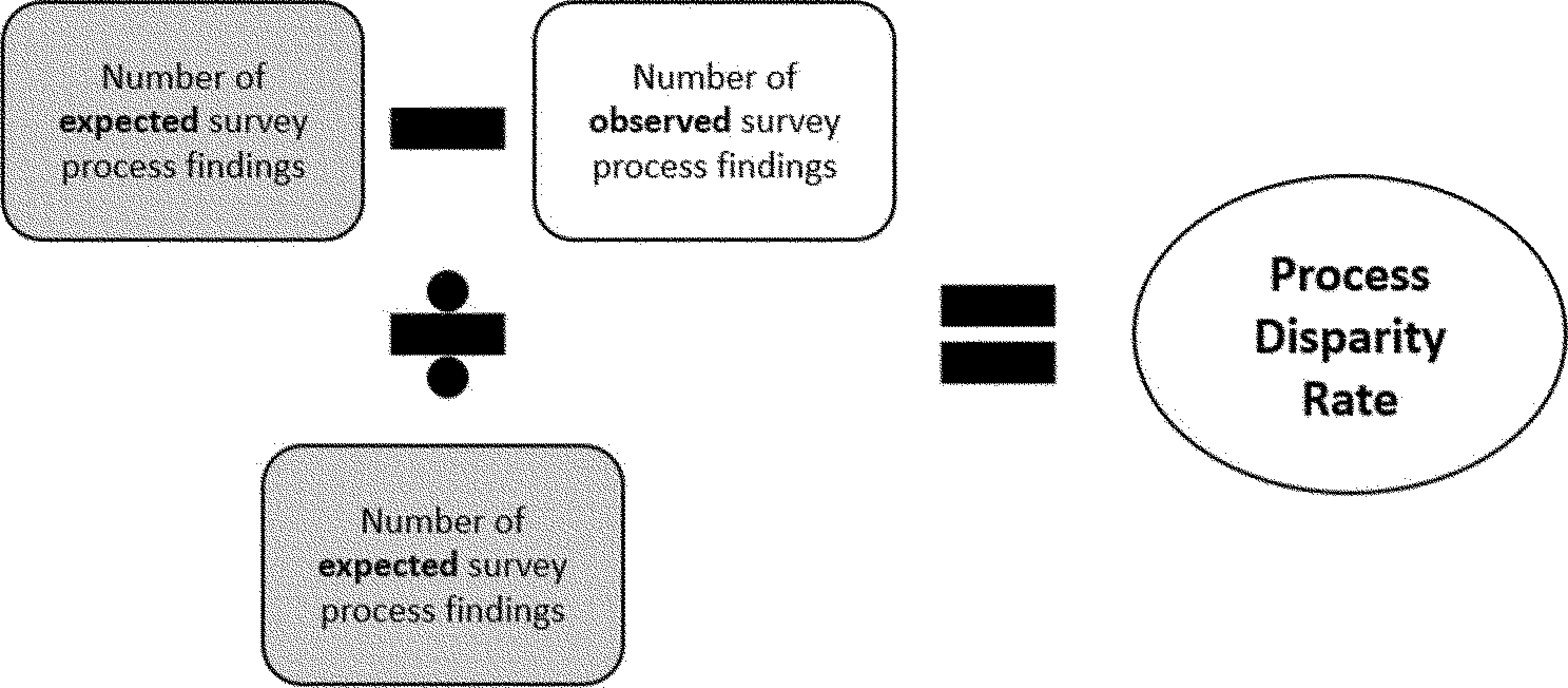
We proposed at § 488.1 to add the definitions of “geographic regions”, “national in scope”, “outcome disparity rate”, “process disparity rate”, and “unannounced survey”. In addition, we proposed to revise the definition of “national accrediting organization,” and remove the definition of “rate of disparity”.
We proposed to establish a new requirement at § 488.4(a)(1) that would require the AOs that accredit Medicare-certified providers and suppliers to include the language of the applicable Medicare Conditions of Participation (CoPs), Conditions for Coverage or Conditions for Certification (CfCs), or requirements (collectively referred to as “Medicare conditions”) set forth in the applicable CMS regulations for each provider and supplier type as their minimum accreditation requirements. However, the AOs would be free to establish additional accreditation requirements that exceed Medicare conditions, as permitted by section 1865(a)(1) of the Social Security Act (the Act).
We proposed to add language at § 488.4(a)(2) regarding use of a comparable survey process approved by CMS, as outlined and contemplated in § 488.5.
We proposed to add a new regulation at § 488.4(b) that would state that if Medicare terminated the participation agreement of a Medicare-certified provider or supplier, then CMS would no longer recognize the facility's AO accreditation for deemed compliance. At proposed § 488.4(b)(2), we would require a terminated provider or supplier to meet all requirements set forth at § 489.57 before their new agreement for participation in the Medicare/Medicaid program can be approved.
We proposed to require AOs to develop a crosswalk between their accreditation standards and the Medicare conditions, at proposed § 488.5(a)(3).
We proposed to strengthen the requirements at § 488.5(a)(4), § 488.5(a)(4)(iii), § 488.5(a)(4)(v), § 488.5(a)(4)(vii), § 488.5(a)(4)(xi), § 488.5(a)(5) and § 488.5(a)(6) related to the comparability of survey processes as mentioned above. We also proposed changes under § 488.5(a)(5)(viii)(A) related to survey reports. These strengthened requirements would be applicable to initial and renewal applications, effective 1 year after the effective date of the rule.
We proposed at § 488.5(a)(8)(i) through § 488.5(a)(8)(iv) to require that AO surveyors complete the applicable CMS online surveyor trainings.
We proposed to add a requirement at § 488.5(a)(10) that the AOs must provide, as part of their initial and
( printed page 36372)
renewal applications, specific policies and procedures that would address how the AOs would prevent and address conflicts of interest. We proposed that AOs provide information on a number of specific policies and procedures regarding conflicts of interest.
We proposed to revise requirements under § 488.5(a)(12) related to the AO procedures for investigating and responding to complaints against accredited facilities.
We proposed revisions to § 488.5(a)(13) related to the AO's accreditation status decision-making process, to strengthen the comparability of the survey processes.
We proposed to add a new requirement at § 488.5(a)(21) that would require an AO to submit a statement with its initial or renewal application certifying that, in response to a written notice from CMS notifying the AO that one of its accredited providers or suppliers has been involuntarily terminated from the Medicare/Medicaid program, the AO agrees to terminate or revoke its accreditation of the terminated provider or supplier within 5 business days from receipt of said written notice.
We proposed at § 488.5(a)(22) to require an AO submit a declaration from each surveyor disclosing any interests or relationships the surveyor may have in or with another survey agency or in or with a healthcare facility the AO accredits (as defined in § 488.5(a)(10)).
We proposed at § 488.8(a)(2) to expand the types of accreditation survey validation activities included in CMS' performance review.
We proposed at § 488.8(a)(4) to require an AOs submit a plan of correction that would be subject to a public reporting requirement, when the AO's performance on survey activities identify disparity concerns, either through the outcome disparity rates or process disparity rates.
We proposed at new § 488.8(i) to place restrictions on the fee-based consulting services provided by AOs to the healthcare providers and suppliers they accredit. At § 488.8(i)(1), we proposed that an accrediting organization or its associated fee-based consulting division or company may not provide fee-based consulting services to any healthcare provider or supplier prior to an initial accreditation survey. At § 488.5(i)(2), we proposed to prohibit AOs from providing fee-based consulting services to healthcare providers and suppliers they accredit within 12 months prior to the next scheduled re-accreditation survey of that provider or supplier. At § 488.5(i)(3), we proposed that AOs may not provide fee-based consulting services to a healthcare provider or supplier in response to a complaint received by the AO regarding that provider or supplier.
At § 488.8(i)(4), we proposed circumstances in which the restrictions to the provision of AO fee-based consulting services would not apply.
We proposed at § 488.8(i)(5) to require AOs to provide specific information to CMS on a bi-annual basis about the fee-based consulting services they provide.
We proposed at § 488.8(i)(6) to take actions against AOs for the provision of prohibited fee-based consulting services.
We proposed at § 488.8(k) that when an AO owner, surveyor, or other employee, currently or within the previous 2 years, has an interest in or relationship with a healthcare facility that the AO accredits, the AO would be required to take steps to prevent the surveyor from having any involvement with the survey of that facility; having input into the results of the survey and accreditation for that facility; having involvement with the pre- and post-survey activities for that facility; and having contact with or access to the records for the survey of that healthcare facility.
We proposed at § 488.9(b) to revise the types of validation programs by adding a new type of validation survey to be conducted by SA or CMS surveyors.
We proposed a new paragraph § 489.20(z) which would require a terminated provider attempting to re-enroll to follow the terms of proposed new § 489.57(b) noted below.
We proposed to redesignate the current § 489.57(a) and (b) and add a new paragraph (b) at § 489.57, to require that Medicare-certified providers or suppliers that have been involuntarily terminated from the Medicare and/or Medicaid program must meet several requirements before CMS will approve their new Medicare agreements. Proposed § 489.57(b)(1) would place the terminated provider or supplier under the oversight of the SA for a reasonable assurance period (with the length of time to be determined by CMS) for the purpose of demonstrating compliance with the Medicare conditions. Proposed § 489.57(b)(2) would require the provider or supplier to remain under the exclusive oversight of the SA until the SA has certified and/or CMS has determined its full compliance with all Medicare conditions, and CMS has approved the new agreement for participation in the Medicare/Medicaid program. Proposed § 489.57(b)(3) would require that while a provider or supplier was terminated from the Medicare program, under the oversight of the SA, and when a new agreement for Medicare participation was pending, CMS would not accept or recognize deeming accreditation of that provider or supplier from a CMS-approved accrediting organization.
We also proposed to remove the reference at § 488.4(a)(2) (inadvertently proposed as a revision to the proposed recodification at § 488.4(a)(4)) that currently excludes end-stage renal disease (ESRD) facilities from the opportunity for accreditation, to reflect a change included in the Bipartisan Budget Act of 2018 (Pub. L. 115-123). Consistent with this same provision, we also proposed to remove the reference restricting transplant programs from utilizing an accreditation option.
We proposed to integrate the acute care hospital and psychiatric hospital survey processes for SAs to ensure that there was a systematic and integrated survey of psychiatric hospital quality and safety. We also proposed to expand the acute care hospital accreditation program for AOs to include current psychiatric hospital accreditation standards that would require AOs with existing CMS-approved hospital programs to expand their existing hospital programs to include survey activities of psychiatric services in psychiatric hospitals.
We solicited comments on whether CMS should limit the number of times an AO could submit an incomplete initial application for a new accreditation program. We sought comment on this question because we recently received several incomplete applications which required multiple pass backs due to the applicant's failure to provide information about issues, such as their financial viability, survey processes which appeared not to be operationalized, or similar concerns.
We note that the regulations have some minor phrasing changes related to updated style guidelines.
II. Background
A. Legislative History
To participate in the Medicare program, providers and suppliers of healthcare services must, among other things, be in substantial compliance with the applicable statutory requirements of the Social Security Act (the Act), as well as CMS' regulatory requirements related to the health and safety of patients. These health and safety requirements are generally called CoPs for most providers; Requirements for Participation for skilled nursing
( printed page 36373)
facilities (SNFs) and Medicaid Nursing Facilities (NFs) (collectively, long-term care facilities); and CfCs for Ambulatory Surgical Centers (ASCs), Rural Health Clinics (RHCs), Federally Qualified Health Centers (FQHCs), ESRD facilities, and some types of suppliers (collectively referred herein as Medicare conditions). A Medicare-certified provider or supplier that does not comply with the Medicare conditions risks having its Medicare provider or supplier agreement terminated. Medicaid service providers or suppliers that are required by CMS or the State to have Medicare approval would also be affected.
In accordance with section 1864 of the Act, the SAs or other appropriate local agencies, under an agreement with the Secretary of the Department of Health and Human Services (the Secretary), perform surveys of healthcare providers and suppliers to assess their compliance with the applicable Medicare conditions for the purpose of certification for participation in the Medicare/Medicaid program. There are several types of surveys conducted, including initial certification, recertification, and complaint surveys. The SAs and CMS also perform surveys in certain circumstances for the providers and suppliers that are accredited by an AO and deemed to meet Medicare requirements. For example, the SA performs complaint surveys for healthcare providers that are accredited by an AO, if the complaint was received by the SA directly. The SA also performs surveys of AO-accredited healthcare providers that have had their participation in the Medicare program terminated, that wish to be surveyed by the SA instead of an AO, and for the purpose of validation of the results of an AO's surveys. Rules, regulations, and guidance for the certification process performed by the SAs are discussed in the CMS State Operations Manual (SOM) [1]
or communicated via Quality, Safety & Oversight (QSO) policy memorandums.[2]
Some provider types may only be surveyed by the SA and cannot use AOs while others cannot be surveyed by SAs pursuant to statute but can only participate in Medicare if accredited by a CMS-approved AO. We refer readers to section “III. Summary of the Proposed Provisions, Public Comments, and Responses to Comments on the Proposed Rule” of this final rule with comment period for additional information. For those providers participating via State survey, based on the SA's certification of a provider's compliance or noncompliance and recommendation, CMS determines whether the provider or supplier qualifies, or continues to qualify, for participation in the Medicare program. Additionally, section 1865(a) of the Act allows most healthcare facilities to demonstrate their compliance with the Medicare conditions through accreditation by a CMS-approved program of an AO, in lieu of being surveyed by SAs for certification. This is referred to as “deeming” accreditation. This is because CMS-approved AOs are recognized by the Secretary as having accreditation programs with accreditation standards that meet or exceed those of Medicare. Therefore, any provider or supplier that is accredited by an AO under a CMS-approved accreditation program is deemed by CMS to have also complied with the applicable Medicare conditions or requirements. The AOs perform initial, re-accreditation, follow-up, and certain complaint surveys.
In December 2020, Division CC, section 407 of the Consolidated Appropriations Act of 2021 (CAA, 2021) (Pub. L. 116-260), amended Part A of Title XVIII of the Act to add a new section 1822 to the Act, and amended sections 1864(a) and 1865(b) of the Act, establishing new hospice program survey and enforcement requirements. CMS issued implementing regulations for SAs and AOs in the CY 2022 Home Health Prospective Payment System Rate Update (HH PPS) final rule (86 FR 62240). The HH PPS rule finalized changes to increase and improve transparency, oversight, and enforcement for hospice programs under SA and AO oversight. Additionally, the HH PPS final rule in part requires hospice program AOs to measure and reduce inconsistency in the application of survey results among all surveyors. The HH PPS final rule: (1) requires AOs with CMS-approved hospice programs to use the same survey deficiency reports as the SAs (Form CMS-2567, “Statement of Deficiencies” or a successor form) to report survey findings; (2) requires comprehensive training and testing of SA and AO hospice program surveyors; and (3) prohibits SA and AO surveyors from surveying hospice programs for which they have worked in the last 2 years (and by which there might be a perceived or actual conflict of interest for these surveyors).
CMS is responsible for: (1) providing ongoing oversight of AO accreditation programs to ensure that a provider or supplier accredited by an AO meets the required Medicare conditions; (2) ensuring that an AO has formalized procedures to determine whether the healthcare facilities deemed under its accreditation programs meet the AO's accreditation standards (which must meet or exceed the applicable Medicare program requirements); and (3) ensuring that the AO's accreditation standards and practices for surveying providers and suppliers meet or exceed the Medicare conditions and practices for granting approval.
For some provider and supplier types, accreditation is voluntary and seeking deemed status through an accreditation organization is an option, not a requirement, for these Medicare-certified providers and suppliers. A provider or supplier has the choice to seek deeming status and accreditation from an AO with a CMS-approved program or certification through the SA survey process. A nationally recognized AO may have accreditation services which are not specifically related to Medicare-participation or Medicare conditions and an AO may offer accreditation services to a provider or supplier which Medicare does not recognize for deeming status, such as long-term care facilities. The AO may also provide accreditation with a deeming option, which is that their deemed program is recognized and approved by CMS to meet or exceed the Medicare program requirements. We refer readers to section “III.K. Require the AOs that Accredit Medicare-Certified Providers and Suppliers to Use Medicare Conditions; and Strengthened Survey Process Comparability” of this final rule with comment period for additional context.
AOs typically charge healthcare facilities a fee for the accreditation services they provide. AOs generally offer at least two accreditation options, which include non-CMS approved accreditation, and accreditation for the purpose of participating in the Medicare program. By “non-CMS approved accreditation” we mean accreditation that is offered by the AOs with an accreditation program but is not approved by Medicare, and which is not used for Medicare purposes. Such accreditation could be used for individual State accreditation purposes or additional professional accreditations that a provider or supplier seeks for business purposes, such as The Joint Commission's (TJC's) Nursing Care
( printed page 36374)
Center accreditation for skilled nursing facilities, which is not recognized by CMS as an option for deemed status.
This final rule with comment period will apply only to the AOs with CMS-approved programs that accredit Medicare-certified providers and suppliers and those entities they accredit. The provisions of this final rule will not apply to the following parties: (1) healthcare providers and suppliers that are not currently accredited by AOs, such as, but not limited to, nursing homes and comprehensive outpatient rehabilitation facilities (CORFs); (2) healthcare providers and suppliers that are certified by the SAs, such as those who elect not to be deemed through an AO; (3) AOs that accredit non-certified suppliers; (4) non-certified suppliers; and (5) AOs that accredit laboratories (under the Clinical Laboratory Improvement Amendments of 1988 (CLIA)).
B. Regulatory Overview of CMS' Rules Regarding AO Programs
The current regulations at 42 CFR 488.4 set forth the general provisions for CMS-approved accreditation programs for Medicare-certified providers and suppliers. 42 CFR 488.5 sets out application and re-application procedures for national AOs that seek to obtain CMS approval of their accreditation programs, often called “deeming authority.”
The AO application and re-application procedures set forth at § 488.5 for Medicare-certified providers and suppliers task CMS with the responsibilities of approval and oversight of the AOs' accreditation programs while ensuring that the accredited providers and suppliers meet or exceed the Medicare conditions.
CMS conducts a thorough review of each accreditation program application submitted by an AO for CMS approval. This review establishes the “comparability” of the AOs accreditation standards with Medicare, to determine whether the AO's standards meet or exceed the Medicare conditions. The application review process also includes a review of the AO's survey processes and procedures, the AO's surveyor training, and their policies and procedures for the oversight and enforcement of provider or supplier entities they accredit. The application review team also reviews the qualifications of the AO surveyor staff. In addition, CMS reviews the AO's financial status, to determine their solvency and potential for longevity of operations.
Section 488.5(e)(1) requires that we publish a notice in the
Federal Register
when we receive a complete initial or renewal application from a national AO seeking CMS approval of its accreditation program. The
Federal Register
notice identifies the organization and the type of providers or suppliers to be covered by the accreditation program and provides a 30-day public comment period. CMS has 210 days from the receipt of a complete application to publish notice of approval or denial of the application. Upon approval, any provider or supplier subsequently accredited by the AO's approved program would be deemed by CMS to have met the applicable Medicare conditions and would be referred to as having “deemed status.”
C. Congressional Report on the Oversight of National AOs and CMS-Approved Accreditation Programs
We are required by section 1875(b) of the Act to submit an annual Report to Congress [3]
on CMS' oversight of national AOs and their CMS-approved accreditation programs. This report contains information related to the AOs' activities in a fiscal year (FY) and provides a comparison of these activities to the activities of previous years. Within this report, we also measure the “disparity rate,” which is a comparison rate based on AO findings of non-compliance during an accreditation survey and the SA findings of non-compliance for the same facilities found during a look-back validation survey.
For certain types of healthcare facilities, there are three levels of adverse findings on an SA survey: immediate jeopardy (IJ); condition-level deficiencies; and standard-level deficiencies. Sections 488.1 and 489.3 define immediate jeopardy as a situation in which the provider's or supplier's non-compliance with one or more of Medicare requirements, conditions of participation, conditions for coverage or certification “has caused or is likely to cause, serious injury, harm, impairment, or death to a resident or patient.” When investigating a potential immediate jeopardy situation, surveyors must find that there is non-compliance by the provider or supplier, that serious harm has occurred or is likely to occur, and that immediate action needs to be taken by the provider/supplier (see Appendix Q of the SOM for additional guidance). A condition-level deficiency means that for that particular requirement under a Medicare condition of participation or condition for coverage, also known as a CoP or a CfC respectively, the facility's noncompliance is such that it substantially limits the provider's or supplier's capacity to furnish adequate care or adversely affects the health and safety of patients (§ 488.24(b)). Surveyors may determine that a deficiency under a single standard alone may have substantially limited a facility's capacity to furnish adequate care and/or adversely affected the health and safety of the facility's patients such that it rises to the level of a condition-level deficiency. The manner and degree of the deficient practice is considered to determine whether there is substantial noncompliance (that is, a condition-level deficiency) or not. A standard-level deficiency means that the provider is out of compliance with one or more aspects of a regulatory condition or requirement that is not severe enough to rise to the level of a condition-level deficiency. A condition-level deficiency, however, is considered more serious in nature and could lead to a facility being terminated from the Medicare and Medicaid programs for non-compliance. Immediate jeopardy citations are condition-level deficiencies that pose immediate jeopardy to patient health and safety. On a validation survey, when the SA cites a condition-level deficiency for which the AO has not cited a comparable deficiency, the deficiency is considered by CMS to have been missed by the AO and is a factor in determining the AO's “disparity rate” for each facility type. The identification of one missed condition-level deficiency by the AO results in the entire survey being counted toward the disparity rate. The number of disparate surveys is divided by the total number of validation surveys performed with respect to that AO by various SAs, to determine the AO's disparity rate.
According to the most recent report, the FY 2020 Report to Congress,[4]
average disparity rates for all CMS-approved AO programs for the following facility types for the most recent year in the report (FY 2019) are: Hospitals (42 percent); Psychiatric hospitals (45 percent); Critical Access Hospitals (46 percent); Home Health Agencies (HHAs, 8 percent); Hospices (19 percent) and Ambulatory Surgical Centers (34 percent). From FY 2018 to FY 2019, hospitals, HHAs and ASCs had the only decreases in disparity rates, with a decrease of 5 percentage points, 11
( printed page 36375)
percentage points, and 7 percentage points, respectively. The disparity rates for psychiatric hospitals increased by seven percentage points from FY 2018 to FY 2019. The disparity rates for Critical Access Hospitals (CAHs) and hospices increased by 5 percentage points and 3 percentage points respectively from FY 2018 to FY 2019. The findings and other information are consistent with previous reports, and no other notable changes were observed in the FY 2020 Report to Congress covering the FY 2019 period of activities. We note the impact of the COVID-19 public health emergency (PHE) in relation to the decreased representative validation survey sample size and disparity rates during FY 2020, and the continued suspension of look-back validation surveys since that point.
D. CMS Validation Survey Pilot
As part of our ongoing efforts to enhance transparency and our oversight of the AOs, in 2018, CMS began a pilot for integrated validation surveys for accredited hospitals, known as the Validation Redesign Program (VRP) pilot. In a VRP pilot survey, the SA teams accompany the AO survey teams on a reaccreditation survey for an accredited facility for the purpose of evaluating the AO surveyors' competency at performing surveys and overall effectiveness during the survey process. The initial findings of the VRP pilot were discussed in the proposed rule at sections IV.J. and IV.L.3. CMS plans to continue to refine the validation process over the next several years to enhance AO oversight and verify that providers/suppliers under deemed status are in compliance with the Medicare conditions and focus surveys on key quality concerns while reducing provider/supplier burden.
A national AO seeking approval of its accreditation programs in accordance with section 1865(a) of the Act must apply for and be approved by CMS for a period not to exceed 6 years. (See §§ 488.5(a), (e)(2)(i)). An AO must submit a renewal application if it wishes to seek re-approval of its accreditation program(s) before the expiration date of its current CMS approval. Review of the AO's renewal application in a timely manner allows CMS to ensure that there would not be a lapse in accreditation for the providers and suppliers accredited by the AO. Requiring the AO to submit a renewal application periodically allows CMS to ensure that the providers or suppliers accredited by that AO meet or exceed the Medicare conditions.
E. Overview of Transparency and Oversight of Accrediting Organizations
In September 2017, an article in the Wall Street Journal [5]
raised concerns regarding the performance and transparency of AO surveys and noted potential conflicts of interest between an AO's accreditation services and its consulting services. As a result of this article, CMS initiated an investigation into these allegations.
F. Prior Rulemaking—Accrediting Organizations Conflicts-of-Interest Request for Information (RFI)
CMS is aware, from the information submitted with their applications, that some AOs with CMS-approved accreditation programs are also providing fee-based consultative services to Medicare-participating healthcare facilities. Our understanding is that typical AO fee-based consultative services include, but are not limited to, the following:
Assistance for clinical and non-clinical leaders (including administrators) in understanding the AO standards and Medicare conditions for compliance;
Review of facility standards and promised early intervention and action through simulation of a real survey, such as a mock survey with comprehensive written reports of findings;
Review of a facility's processes, policies, and functions;
Identification of, and technical assistance for, changing and sustaining areas in need of improvement; and
Educational consultative services.
CMS acknowledges that independent fee-based consulting is a valuable resource that can help providers and suppliers improve the quality and safety of the care they provide. This does not mean that the providers or suppliers who elect not to receive fee-based consulting from an AO that offers it, or that providers or suppliers that are accredited by an AO that does not offer this service would not provide safe, quality care.
There are many third-party consultants that offer fee-based consulting across all provider and supplier types. The availability of third-party fee-based consultants give providers and suppliers access to this educational service, if their AO does not provide fee-based consulting. If a provider's/supplier's AO already offers fee-based consulting, third-party consultants can offer such providers and suppliers with an alternative, allowing providers and suppliers to compare the effectiveness and quality of consultants to address their needs within their cost limitations. The provider or supplier may also be able to negotiate a price for educational services provided by a third-party consultant, while this may not be an option with the AOs that offer fee-based consulting. It is important to note there would be no conflict of interest associated with the use of third-party fee-based consultants because these consultants do not also make compliance determinations about the provider or supplier.
Fee-based consulting services offered by AOs are not prohibited by law or regulation. However, CMS is concerned that an AO's provision of such fee-based consulting results in perceived or actual conflicts of interests because of the contractual and financial relationship that exists between the healthcare provider and the AO, which is a private entity that profits from the performance of the inherently governmental function of regulating healthcare providers through accreditation.
Because of this, on December 20, 2018, we published a Request for Information (RFI) in the
Federal Register
entitled, “Medicare Program: Accrediting Organizations Conflict of Interest and Consulting Services; Request for Information” (83 FR 65331), hereinafter referred to as “2018 AO Conflict-of-Interest RFI”, in response to increasing concern about potential conflicts of interest created by the accreditation and consultative activities of the AOs. Specifically, we solicited public comments to determine whether offering consultative services to the same entities an AO accredits may create actual or perceived conflicts of interest between an AO's accreditation program and its consultative program. We stated that this dual function may undermine, or appear to undermine, the integrity of the accreditation programs and could erode public trust in the safety of providers and suppliers that have been accredited by CMS-approved AOs. We further acknowledged that certain consulting services offered by some of the AOs, such as quality improvement work and training of facility staff, may be beneficial to some facilities and result in improvements in operations or the quality of care furnished and may be provided with the best of intentions. We stated that circumstances could arise where an AO has recommended a facility for deemed status through their accreditation
( printed page 36376)
service, while the consultancy service of the AO was generating revenue assisting the same facility in passing the AO's own accreditation surveys. Some AOs have indicated that they establish firewalls between the arms of their businesses, but we stated that these firewalls may not be sufficient to ensure that no conflicts of interest result from these activities.
We further stated that, similar to quality improvement organization (QIO) and external quality review organization programs, any AO with a Medicare-approved accreditation program has assumed a position of public trust and is responsible for acting on behalf of the public, because the AO is performing a function that assists in the Federal government's enforcement programs. We also expressed our view that AOs voluntarily take on this position and responsibility when they seek accreditation approval from CMS to accredit providers and suppliers for participation in Medicare. Because of the responsibility to maintain public trust and public health, we continually ensure that all entities and programs, including AOs and their accreditation programs that require CMS approval, be held to high standards of ethical conduct so that everyone can have complete confidence in the integrity of Federal government certification. We stated that the AOs' decisions to accredit facilities must be made without regard to any additional services that a Medicare provider or supplier might obtain through the AO or its subsidiaries. We stated that this policy would ensure and maintain public trust in the Medicare certification program.
In the 2018 AO Conflict-of-Interest RFI, we solicited public comments to gather information for potential future rulemaking and to obtain insight on mechanisms to address this potential conflict of interest. We were specifically interested in ways to potentially modify § 488.5(a), which sets out the required information to be submitted with an AO's application. For example, § 488.5(a)(10) states that the application information from the AO include the organization's policies and procedures to avoid conflicts of interest, including the appearance of conflicts of interest, involving individuals who conduct surveys or participate in accreditation decisions.
We stated that potentially expanding § 488.5(a)(10) by adding provisions that would require the AOs to disclose information about any consultative services they offer to facilities could further enhance our oversight of AOs.
In addition, we solicited comments on the following issues:
With respect to fee-based consultative services provided by AOs to the facilities they accredit—
++ How are these services provided and communicated to the facilities?
++ Are potential conflicts of interest disclosed?
Are there other entities that could provide this training besides the AOs?
Whether commenters perceive a conflict of interest in AOs providing fee-based consultative services to the facilities they accredit.
Whether the ability of an AO to collect fees for consultation services from entities they accredit could degrade the public trust inherent in an AO's CMS-approved accreditation programs.
What the appropriate consequences or impacts should be, if a conflict does exist.
What firewalls may exist within an AO between accreditation and consultation services, or what firewalls would be prudent, to avoid potential and actual conflicts of interest.
Examples of positive and negative effects which may arise as a result of a conflict of interest.
What the potential impact, financially and overall would be if CMS were to finalize rulemaking which would restrict certain activities that might give rise to a real or perceived conflict of interest.
When and/or under what circumstances it would be appropriate for AOs to provide fee-based consultative services to the facilities which they accredit.
Whether, and if so under what specific circumstances, CMS should review a potential conflict of interest, and what factors CMS should look at to determine if a conflict of interest exists.
A list describing under what circumstances the AOs or interested parties would believe there to be a conflict; and under which circumstances a conflict does not exist.
The type of information which would be considered necessary, useful and/or appropriate in proving or refuting our hypothesis of a connection between the use of consultative services and preferential treatment of accredited providers and suppliers. (See83 FR 65335.)
We received 128 public comments in response to the 2018 AO Conflict-of-Interest RFI. Approximately half of the commenters (consisting primarily of AOs and healthcare facilities that use consulting services) supported the use of AO consulting services and stated that there is no conflict of interest associated with fee-based consulting. The other half of the commenters (consisting of individuals, provider associations, medical advocacy groups and one AO) stated that the provision of fee-based consulting by the AOs creates a conflict of interest.
Several commenters stated that the benefits derived from AO fee-based consulting far outweigh any potential or actual conflict of interest that may result. Many commenters believe that AO consulting services allow the facility to seek information and guidance that helps them understand, interpret and comply with the Medicare conditions and regulatory requirements. These commenters stated that use of the AO's fee-based consulting services helped to improve the safety and quality of the care provided by the healthcare facility.
Many commenters stated that there are already implemented checks and balances between CMS and the AOs that are sufficient to ensure that no conflicts of interest occur between the AOs and their accredited facilities. These commenters stated that the AOs have robust firewall policies and procedures in place to prevent conflicts of interest related to fee-based consulting. Many commenters also stated that CMS has a specific AO fee-based consulting firewall policy in place and that this policy is adequate to prevent any conflicts of interest. However, CMS does not currently have such a policy.[6]
Several commenters stated that AOs are commissioned to ensure compliance with the Medicare conditions. These commenters stated that a big part of compliance is not only being punitive but informational/educational. One commenter suggested that AOs are in a unique position to provide this education and technical assistance because they understand the complexity of the Medicare conditions. One commenter stated that if AO fee-based consulting services were not provided, facilities could see additional deficiencies cited due to misinterpretation of requirements and multiple rounds of surveys, generating still more cost to the facility.
Several commenters stated that the financial benefit derived by the AOs from providing fee-based education is not significant. Some of these commenters also stated that the AOs gained no benefit from the success or results of accreditation whether they had assisted the provider to deliver better services or not.
( printed page 36377)
One commenter stated that they are not aware of other organizations that would be capable of educating and advising healthcare providers in a similar fashion as the AOs' consulting services. Several other commenters expressed concern about having fee-based consulting services provided by an independent third-party. These commenters stated that, while there are other entities besides the AOs, such as QIOs, that could provide training, the focus would solely be on quality rather than the outcome of an accreditation.
Many commenters stated that the integrity of the accreditation process is of utmost concern for regulators, providers, and patients alike and that AOs should position themselves to be above reproach regarding overseeing patient care and quality of services that healthcare facilities provide, so as to retain the trust of patients and the public. Several commenters suggested that anything that may undermine the integrity of accreditation programs or the public trust in CMS accredited providers and suppliers be considered and addressed. One commenter stated that the ability of AOs to provide both survey services and consulting services is a conflict of interest, which results in a decreased level of trust among providers, Medicare, and the public.
Many commenters expressed concern about the financial and contractual relationship that exists between AOs and the healthcare facilities they accredit. These commenters expressed concern that the existence of a financial relationship between AOs and healthcare providers casts a veil of doubt over the entire CMS hospital accreditation process, eroding the public trust in CMS to maintain the standard of care at our nation's hospitals and to ensure that Medicare patients are receiving safe, therapeutic care. One commenter opined that the business connection between the provider and the AO creates a relationship that the AO could have an incentive to manipulate.
In addition, several commenters expressed concern about the significant financial interest the AOs have in the provision of fee-based consulting. One commenter stated that since AOs are being paid by the healthcare facilities for both accreditation services as well as consulting services, it is obviously in their financial interest to keep the healthcare facilities accredited and not to create too much dissatisfaction to incite the organization to seek another AO. Several commenters expressed concern that this financial relationship might provide the incentive for the AOs to ignore or downplay deficiencies during the survey of a consultative client to increase the apparent efficacy of its consulting services. Or, perhaps, an AO could exaggerate the deficiencies on surveys to increase the apparent value of the consulting services to providers. Because of the previously stated concerns, several commenters suggested that CMS prohibit the AOs from providing fee-based consulting to the healthcare providers and suppliers they accredit.
G. Conflicts of Interest—The AO Owner's, Surveyor's, and Other Employee's Interest in or Relationship With a Healthcare Facility That the AO Accredits
It is typical for an individual healthcare professional, such as a physician or nurse, to have concurrent employment relationships with more than one healthcare provider. Many healthcare professionals, such as physicians, physician assistants, and nurse practitioners have multi-setting practices or are employed at more than one healthcare facility. For example, a registered nurse (RN) may work on staff at a hospital but also work at other hospitals through a medical staffing agency. In addition, as employees of a healthcare facility, these healthcare professionals could possibly gain a financial interest in the healthcare facility through means such as being a contributor to the construction costs of a new wing of the facility or buying stock in the facility or its parent corporation. Management employees could be awarded stock or stock options for the facility or its parent corporation as part of their compensation and benefits package.
AOs frequently hire surveyors that are also employed at one or more outside healthcare settings because the professional associations, expertise, knowledge and skills held by these healthcare practitioners make them an asset as a surveyor. This might include, for example, an RN who is employed by a hospital and also works as a surveyor for an AO. This employment scenario does not generally violate CMS policy or regulations. Furthermore, an AO surveyor having other employment does not, in and of itself, necessarily create a conflict of interest. However, if the AO provides accreditation services to the healthcare facility that employs the AO surveyor, this could cause a conflict of interest if that surveyor is permitted to have any involvement in the survey process for that healthcare facility.
CMS has recently encountered two situations in which an AO's surveyor was also employed by the healthcare facility that was being accredited by the AO. In one of these situations, an AO surveyor was also employed in an administrative position at a rehabilitation facility that was being surveyed by the AO. This situation was not disclosed to CMS by the AO. Currently, CMS has no specific regulations that would prohibit a conflict of interest related to an AO surveyor's relationship with a healthcare facility that the AO accredits, except for home health agencies and hospice programs.
Section 488.5(a)(10) of our regulations requires that an AO provide, with its application seeking CMS approval of its accreditation program, “the organization's policies and procedures to avoid conflicts of interest, including the appearance of conflicts of interest, involving individuals who conduct surveys or participate in accreditation decisions.” However, § 488.5(a)(10) does not provide requirements for specific types of information or requirements that should be contained in the AO's conflict-of-interest policies and procedures. This regulation does not specifically prohibit or define conflicts of interest and based on the comments to the 2018 AO Conflict-of-Interest RFI, CMS proposed to revise this regulation to more specifically address situations that should be included in the AO's conflict-of-interest policy.
As noted previously, the SAs and AOs perform similar work. Section 4008 of the SOM describes examples of scenarios that would be conflicts of interest for SA surveyors who have an outside relationship with a facility that is surveyed by the SA.[7]
Currently, section 4008 of the SOM applies only to SA surveyors and not AO surveyors.
Scenarios in which an AO surveyor has a relationship with a healthcare facility that their AO accredits could represent a conflict of interest. As CMS has no specific regulations that would proactively address such conflicts of interest for AOs that accredit healthcare providers other than home health agencies and hospice programs, we proposed establishing several requirements to help mitigate such conflicts of interest in section IV.B.7. of the proposed rule.
( printed page 36378)
H. Public Comment on Whether it Is a Conflict of Interest for AO Board Members or Advisors To Have an Interest in, or Relationship With, a Healthcare Facility that the AO Accredits
As previously stated, it could be a conflict of interest when an AO surveyor is involved with the survey of a facility with which that surveyor has an employment, financial, business or other interest or relationship. We note that in most cases, the AO board members do have interests in or relationships with the healthcare facilities the AO accredits. In many cases, the board members of the AOs frequently hold upper management positions of a healthcare facility the AO accredits, such as chief executive officer (CEO), director, or President. In the proposed rule, we sought public comment as to whether it would be a conflict of interest for an AO board member, AO advisor, or CEO or other executive team members to also have a relationship with a healthcare organization accredited by such AO. An AO advisor would be an advisory committee member, advisor to the CEO, or an advisor to the board of directors. We refer readers to the revisions related to an AO owner's, surveyor's or other employee's interest in, or relationship with, a healthcare facility the AO accredits in section III.J. of this final rule with comment period.
We received comments in response to our request for public comments on whether it is a conflict of interest for AO board members or advisors to have an interest in or relationship with a healthcare facility that the AO accredits. The comments and responses can be found in section III.D. of this final rule with comment period.
III. Summary of the Proposed Provisions, Public Comments, and Responses to Comments on the Proposed Rule
As stated in section “I. Executive Summary” and section “II. Background” of this final rule with comment period, there are several provisions related to oversight of AOs that we believe require strengthening since we issued the 2015 AO final rule. Over the last several years, we have worked closely with the AOs to establish and implement an AO Liaison program in which we meet with each AO regularly (at least on a quarterly basis). These meetings and discussions have provided an avenue for CMS to also receive feedback on existing Medicare conditions and our interpretive guidelines and allowed us an opportunity to clarify our expectations for the AOs. Most importantly, this experience has helped us to identify areas of our AO oversight regulations in need of revision so that we might more clearly articulate the requirements for all AOs with CMS-approved accreditation programs. Therefore, we have become aware of the need to clarify, reorganize, and amend our regulations to support a more efficient and effective oversight process.
The proposed rule, titled “Medicare Program; Strengthening Oversight of Accrediting Organizations (AOs) and Preventing AO Conflict of Interest, and Related Provisions” (89 FR 11996 through 12064), was published in the
Federal Register
on February 15, 2024, with a comment period that ended on April 15, 2024. We received approximately 250 individual public comments from 58 separate commenters on our proposals, including comments from AOs; ESRD facilities; national renal groups, nephrologists, and patient organizations; patients and care partners; manufacturers; healthcare systems; and nurses.
In this final rule with comment period, we provide a summary of each proposed provision, a summary of the public comments received and our responses, the policies and requirements we are finalizing for AOs (including those for preventing AO conflicts of interest), and other related provisions we are finalizing in this rule.
A. General Comments in Support of the Proposed Rule
Comment:
Many commenters supported the provisions of the proposed rule. They stated that the rule aims to protect patients, strengthen oversight of AOs to ensure that the highest quality of care is being delivered to all patients. Commenters also stated that this rule will help to ensure that all AOs conduct their work in a consistent, rigorous, and unbiased manner. The proposals made in the rule, if finalized, will prevent conflicts of interest, streamline survey processes and ensure more consistency between AOs and CMS or SA surveyors. One commenter supported the proposed rule because they believe it is imperative that as CMS seeks to improve oversight and transparency of AOs, it avoids introducing unnecessary obstacles to the ability of providers to seek accreditation through these AOs. One commenter the proposal made in the proposed rule and further suggested that CMS be more aggressive in their effort to strengthen the requirements and process for deeming hospices eligible for Medicare certification given the ongoing challenges related to hospice fraud, waste, and abuse. Another commenter supported the proposed rule because it will help the public know which healthcare facilities to choose from and to be confident that any accredited facilities they do choose will provide high-quality care.
Response:
We thank these commenters for their support of the provisions of the proposed rule.
B. Comments Expressing General Opposition to the Proposed Rule
Comment:
Two commenters believe the proposed oversight will require additional administrative work from CMS, which one commenter believes is already concerned with existing staffing levels and which the other commenter believes is only now returning to normal workloads after the COVID
-
19 PHE.
Response:
We appreciate these commenters' concerns for the administrative burden on CMS staff to implement the provisions of this rule. We will consider the potential for additional burden to CMS staff when implementing these provisions. We anticipate a fully developed workflow for the increased AO oversight provisions prior to implementation of the rule.
Comment:
One commenter opposed the provisions in the proposed rule because they believe the extent of changes proposed are vast and far reaching; they stated that many provisions contain ambiguities and needed additional clarification.
Response:
We thank this commenter for their comment. We appreciate this commenter's concern for clarity. However, we are not able to respond to this comment because the commenter did not provide enough detail about the provisions they think were excessively far-reaching and/or unclear.
Comment:
Several commenters oppose the proposed rule because they believe that CMS does not have the statutory authority to make such proposals. One commenter stated that the Congress delegated only limited authority to CMS to grant private AOs the ability to “deem” that a provider or supplier meets or exceeds the Medicare conditions and that CMS' limited authority to regulate AOs must be tied to the statutory purpose.
Another commenter believes that the Congress has not granted CMS the authority to determine the AO's service offerings or to regulate any aspects of the AO's operations, governance structure, or business practices. In proposing that AOs only be allowed to provide certain services at certain times, the commenter believes CMS has exceeded its authority under the statute,
( printed page 36379)
venturing into operational grounds with which the Congress never intended the agency to interfere.
Response:
We respectfully disagree. CMS is using the authority established by the Congress under section 1865 of the Act to establish certain requirements for AOs in this rule. The Congress gave CMS broad authority for oversight over the AOs.
Comment:
One commenter recommended that instead of implementing all of the provisions in the proposed rule, we instead select provisions for implementation that receive the least amount of negative public comments, then at a later date, update the proposed changes that may be viewed by some as more burdensome and imprecisely drafted, followed by the issuance of a RFI with an extended comment period that allows time for detailed and evidence-based responses. The commenter believes this segmented approach will allow both CMS and the AOs to focus on perfecting the selected changes without being overwhelmed and overly burdened by the number of changes implemented at one time.
Response:
We thank the commenter for their recommendations but respectfully disagree with this approach to finalizing the rule we proposed in February 2024. We note that we did publish an RFI on December 20, 2018 (83 FR 65331), seeking public input on our oversight of AOs, particularly with regard to AO conflict-of-interest issues. We carefully considered the information received on the 2018 RFI as well as the public comments received on the February 2024 proposed rule as we developed this final rule with comment period.
C. Add Definition of “Unannounced Survey” to § 488.1
We proposed to add a new definition of “unannounced survey” to § 488.1. The definition of “unannounced survey” would be consistent with the definition of “unannounced” contained in the Merriam-Webster dictionary, which is “without previous notice or arrangement and therefore unexpected”. Adding this definition of “unannounced survey” would support the existing requirements set out at § 488.5(a)(4)(i) and in our sub-regulatory guidance. This proposal clarifies and codifies existing requirements under § 488.5(a)(4)(i), which requires that surveys must be unannounced, which means that the facility must be unaware of the survey until the time that the survey team arrives, and that the provider or supplier would not receive notice of the survey until the survey team arrives at the facility. Our long standing policy behind the term “unannounced survey” is within Chapter 2, Section 2700A of the SOM, outlining the expectation that all surveys of providers and suppliers (other than clinical laboratories) must be unannounced to the provider or supplier being surveyed. This means that the provider or supplier to be surveyed would not receive notice of the survey until the survey team arrived at the facility for the survey, as is also currently the AO's process for complaint surveys. The proposed definition for “unannounced survey” would also state that unannounced surveys must be scheduled by the AO in a manner so that their timing and occurrence will not be predictable to the healthcare facility being surveyed.
One of the primary reasons surveys conducted by either the SA or the AO are required to be unannounced is to prevent the provider or supplier from making unusual preparations for the survey that would not represent the ongoing typical condition of the provider, and the true nature and quality of care provided. Examples of these activities would include unusual cleaning activities, painting, clearing obstructions from halls and entrances, denying leave to staff during that time or calling staff back to inflate staffing availability, and re-reviewing medical records outside of what is normally done. If a provider or supplier knows the exact time a surveyor will be onsite, it may temporarily adjust its typical practices such as staffing, which would provide an unrepresentative picture to surveyors of the quality of care typically provided to patients or residents. Any notice to facility leadership via organizational websites, emails, or phone calls prior to surveyors arriving onsite is considered a violation of CMS regulations.
In 2009, CMS clarified this expectation in the Survey & Certification Policy Memorandum 09-41,[8]
to advise that announcing of surveys was in conflict with CMS regulations. In the effort to align AO survey processes with CMS survey processes (which are followed by the SA surveyors), as outlined in section IV.C. of the proposed rule, we determined that additional clarity regarding this prohibition was needed. Defining the term “unannounced survey” within the regulation as opposed to our SOM (sub-regulatory guidance) would provide clarity regarding our expectations, and would mirror the processes used by the SAs, who do not announce their surveys (except for clinical laboratories); as noted, any AO practice of announcing surveys could undermine the integrity of the survey process. While we recognize that some AOs may have provided up to a 60-minute advance notice of the survey team arriving onsite for initial and reaccreditation survey activities, this practice is inconsistent with the processes followed by our SAs and inconsistent with the AOs' own survey processes for complaint surveys (which are always unannounced). Therefore, in accordance with § 488.5(a)(4)(i), which requires unannounced surveys, as well as our long-standing policy in Chapter 2, Section 2700A of the SOM, we proposed to define “unannounced survey” to clarify through this definition that all surveys of providers and suppliers (other than clinical laboratories) must be unannounced and any advance notice to facilities would be prohibited. This definition would ensure clarity in the requirement that applies to AOs as well as SAs and further support our initiative to bring consistency to survey practices as outlined in section IV.C. of the proposed rule.
Furthermore, the definition of “unannounced survey” ensures that the timing of recertification surveys is also unpredictable. AOs generally complete comprehensive re-accreditation surveys of their client providers and suppliers every 32 to 36 months. However, some providers or suppliers have informed us that they know when an AO is scheduled to survey the facility—the AO may schedule the facility for survey within the same week or month every survey cycle, or has narrowed its schedule via the use of blackout days, or informed the facility close to the time of the survey via administrative contact from the AO, such as payment collection, confirmation or change of address notification or other facility-AO specific information. All of these practices undermine the integrity of the unannounced survey process.
We received several comments, with a majority of the comments in general support of our proposed definition. The comments and our responses to the comments are set forth below.
Comment:
We received several comments supporting our proposal for unannounced surveys, restricting blackout dates and ensuring the unpredictability of surveys. One commenter stated that an unannounced survey will enable the surveying organization to more effectively assess the organization in its normal state, identify areas of risk and subsequently
( printed page 36380)
improve patient care. One commenter supported our proposed definition of “unannounced survey”, highlighting that unannounced surveys would not only provide more consistency among AOs and SAs, but also may impact the proliferation of fraudulent hospices. Another commenter stated that announcing any survey allows companies time to prepare and that unannounced surveys will ensure that surveyors receive honest results. One commenter also stated that all surveys should be unannounced without the facility being aware of the survey until the arrival of the survey team. One commenter also stated that among CMS' proposals for increased comparability, the most important aspect was use of the unannounced survey to avoid rigging of the system.
Response:
We appreciate the commenters support of the proposed definition of “unannounced surveys”. We agree that adding the definition will help ensure more consistency among AOs and SAs and the integrity of survey results.
Comment:
We received one comment noting that the proposed definition of “unannounced surveys” and the preamble discussion within the proposed rule are consistent with CMS' 2023 notice letter to AOs (discussing unannounced surveys and blackout dates). The commenter stated that CMS overestimated the actions facilities could take to improve the results of an impending survey on short notice. The commenter urged CMS to consider allowing hospitals a 24-hour notice of the survey to ensure appropriate staff would be available during the survey and to maximize access to hospital leadership and other staff who could answer surveyor questions. The commenter suggested that this would allow for a more efficient survey process and that survey results would be more useful and reflective of the care provided by the facility. The commenter stated that a 24-hour window would not allow sufficient time to make outcome-changing preparations. Finally, the commenter also suggested that when AOs combine complaint investigations with the required 36-month reaccreditation survey the type of survey is frequently not identified by the surveyor. The commenter implied that this process is confusing for hospital staff and risks conflating the results and urges CMS to ensure surveyors clearly identify the purpose of the survey with outreach to hospital staff to address issues which may arise.
Response:
While we appreciate the commenter's concern, we note that we proposed to add a definition, which does not change the requirement at § 488.5(a)(4)(i) that was discussed in the 2023 letter the commenter mentioned, which is a letter from our Quality, Safety & Oversight Group Director that was sent to the AOs through our AO liaisons. Surveys are intended to assess the daily operations of the facility at any time. Facilities should always have processes in place to ensure continuity of care and operations in the event that leadership is not available or onsite. Therefore, we believe that advance notice could give leadership an opportunity to appear involved in the facility, when in normal operations, leadership could be absent or not as involved as made out to appear. Additionally, a 24-hour notice could allow for a facility to increase staffing for the day of the survey or clean areas of the facility which otherwise would have not been changed. As for the commenter's concern that when complaint investigations are incorporated into a recertification/reaccreditation survey, we note that Chapter 5 of the SOM allows both SAs and AOs to combine complaint investigations into the next survey activity if the complaint was triaged as low-priority. However, we understand the commenter's concerns for the need of a transparent process and believe that adding a regulatory definition for “unannounced survey” will further that goal.
Comment:
We received several comments raising concerns about unannounced surveys and the potential for this to disrupt operations. One commenter specifically stated that unannounced surveys disrupt the daily operations of healthcare facilities, potentially affecting patient care and staff workflows. The commenter also stated that this is a resource burden where facilities may need to allocate more resources to maintain constant readiness for survey. Another commenter stated that some individuals who support regulatory surveys may not work onsite at the facility and that certain departments such as infection prevention, quality or others may be covered by individuals working in multiple locations, especially in rural locations. Alternatively, one commenter stated that surveys should not be delayed more than 30 minutes of the reported opening time. Finally, two commenters also advised that notification on the initial day of survey is critical to ensure key members are present, negate interruptions in the facility's operations, and ensure coordination, especially for multi-site institutions. One of the two commenters specifically stated that same-day notification would protect patient and workforce safety.
Response:
While we appreciate the commenters' concerns, we note that CMS has expected that all survey activities from the SAs and AOs are to be unannounced and has reiterated this expectation in § 488.5(a)(4)(i), the SOM, and other subregulatory guidance.[9]
This long-standing requirement ensures that surveyors can observe a facility's daily operation and that facilities do not make adjustments to pass the survey, as implied by the commenter. Surveyors are flexible and are required to work around the facility's schedules and its daily requirements to provide patient care. For instance, if a Registered Nurse is assisting a survey team with record reviews but needs to see patients, the expectation is that patient care takes priority over survey activities. Similarly, should a facility have staff which support the daily operations but may be off-site, surveyors will wait for their arrival and conduct other survey activities during that time, or even conduct telephone interviews should the individual not be able to travel to the facility on the survey date(s). We agree with the one commenter related to delay of survey activities upon arrival beyond 30 minutes should not be the norm; however, we believe that the facility's verification of the survey team and beginning the survey processes (including the facility gathering required documentation) should not be significantly slowed. Surveyors may delay the formal entrance conference to await leadership or staff the facility may want present, especially in situations with multiple locations.
Comment:
One commenter advised that unannounced surveys and the inability to provide blackout dates would pose challenges for hospitals and accreditation specialists. Specifically, the commenter suggested that blackout dates and announced surveys offer crucial preparation time, the ability to allocate resources efficiently, conduct self-assessments and identify deficiencies proactively. The commenter also stated that lack of prior knowledge of the survey amplifies stress among the facility's staff and hampers productivity and morale in a hospital setting. The commenter also suggested that announcing survey activities in advance would allow for continuous improvement and ensure high standards of care.
( printed page 36381)
Response:
We thank the commenter for expressing concerns related to unannounced surveys and blackout dates. While we understand unannounced survey activities can pose a challenge, this has been a long-standing requirement. Unannounced survey activities are intended to assess a facility's quality of care provided on any given day and to prevent the provider or supplier from making special preparations for the survey that would not represent the ongoing typical condition of the provider and true nature and quality of care provided, such as increasing staffing that would not usually be scheduled; adjusting records and practices; and unusual cleaning or changes to its physical environment. We do not want to provide an opportunity for facilities to demonstrate a different picture to surveyors from how the facility normally operates. Additionally, we expect that facilities are survey-ready, meaning always in compliance with the Medicare conditions, at all times. Therefore, allowing facilities to choose dates that they wish not to be surveyed further compromises a true depiction of how the facility operates on any normal business day. Related to the commenter's suggestion that announced surveys allow for continuous improvement and ensure high standards of care, we believe by adding the definition of “unannounced survey” and continuing the requirement for unannounced surveys should have no bearing on facilities providing high-quality care to patients.
Comment:
We received two comments raising concerns specific to our discussion and restriction of blackout dates. One commenter stated that prohibiting blackout dates would make it very difficult for organizations to successfully support survey activities while maintaining day-to-day operations. The commenter stated that organizations may not always have the bandwidth to support multi-day regulatory surveys, as staff or leaders must escort surveyors, answer questions, and attend meetings all while supporting and providing patient care. Another commenter voiced significant concerns with the prohibition of blackout dates, highlighting the drastic workforce shortages as the result of the COVID-19 pandemic and a strained health system. This commenter implied the burden associated with staff having to provide care to patients while providing support to surveyors and that the ability for a facility to request blackout dates, as well as pre-survey contact with the AO, ensures that the facility has the necessary resources, to include staff, files, manuals, and policies, when the survey team arrives. Additionally, the commenter raised concerns related to unannounced surveys, as some facilities may be supported by individuals who cover multiple locations.
Response:
We appreciate the commenters' concern related to blackout dates and the challenges which could arise regarding adequate staff to support the survey teams. The existing regulations 42 CFR 488.5(a)(4)(i) require unannounced surveys, as well as our long-standing instructions in Chapter 2, Section 2700A of the SOM. If a provider or supplier knows the exact time a surveyor will be onsite, even shortly before their arrival, it may temporarily adjust its potentially noncompliant and typical practices (for example, regarding staffing). This can lead to findings that are not representative of the quality and the safety typically provided to the facility's patients. Allowing facilities to request dates when they wish not to be surveyed is not consistent with our survey expectations. Furthermore, some AO blackout date policies provide the caveat that the wishes of the facility may not be guaranteed, we believe this practice is inconsistent with the requirements and policies for unannounced surveys and the expectation that a provider/supplier must be always “survey ready”. If an AO learns that a facility has a situation that would decrease the efficacy of an onsite survey (such as a sole practitioner who will not be at an ASC and no surgeries will be performed that day), the AO may pick an alternate date. This decision, however, rests with the AO and should not be driven by the facility. We appreciate the commenter's concerns surrounding staffing shortages in a post COVID-19 environment and the challenges for supporting survey activities. Surveys are intended to assess the normal day-to-day operations of a facility and are not intended to be disruptive. We recognize staff participating in survey activity may need to pause assisting surveyors to provide patient care or manage the facility's operation. Surveyors and processes are intended to be flexible when onsite and patient care and safety is our number one priority. However, it is imperative to use unannounced surveys to assess the daily operations at the facility, and to also ensure that patients receive quality care and sufficient staff are available to the patients to provide a safe environment.
Comment:
We received several comments raising concerns related to the physical security and safety of staff. One of the commenters noted that AOs had adopted pre-arrival notifications because health systems experienced incidents of individuals impersonating surveyors accessing a facility with fake credentials; the commenter also cited Bureau of Labor Statistics data showing an increase in the number of healthcare workers physically attacked. Another commenter noted that violence against healthcare workers is on the rise, and pre-arrival notification would allow proper identification of surveyors. A few commenters also stated that a 30-minute to 60-minute pre-arrival notice would not allow sufficient time for usual preparations to be made. Another commenter echoed the comment regarding safety risks and stated that The Joint Commission's process for pre-notification includes a survey agenda, letter of instruction, biography, and picture of the surveyors for facilities to verify and validate the surveyors are legitimate. Another commenter stated that pre-survey notifications allow facilities to maintain the physical security of the facility. This commenter stated that notification ensures that health systems can inform their security personnel and receptionists to expect the survey team.
Response:
We appreciate the concerns related to unauthorized individuals who may attempt to gain entry using fake credentials, however, we note that this occurrence has not been reported by any non-deemed facilities under various SAs' jurisdictions. SAs present credentials at the time of arrival for authentication and entry into the facility. We would expect AOs present their credentials as is currently customary upon arrival. Furthermore, allowing a one-hour notification to the facility could provide sufficient time for the facility to adjust schedules or make certain environmental changes which would not represent the true picture of the facility. Additionally, with respect to the one AO's process for notification (including photographs, biographies, and a survey agenda), AOs may implement these types of processes upon arrival and entry to the facility. Facilities are not restricted from verifying the survey team, whether the survey team is from the SA or an AO; facilities may request that surveyors wait until identification and verification is complete. Furthermore, we note that complaint surveys are unannounced, therefore arrival procedures and processes should not be different for initial or reaccreditation surveys. We encourage AOs to develop processes to ensure the integrity of unannounced surveys is maintained, while accounting
( printed page 36382)
for processes which allow facilities additional time to verify surveyor identities.
Comment:
One commenter, while in general support of the proposed provision, also urged CMS to include instructions or guidance to surveyors to be prepared with all the necessary identify verification documentation immediately upon arrival and to allow some period of time for hospitals to verify those identities before commencing the survey. This commenter emphasized the importance of safety of patients and staff.
Response:
We appreciate the commenter's general support of unannounced surveys, and we appreciate the commenter's concerns on verification of identities. As outlined in the SOM program appendices, surveyors are already expected to present their identification upon entry at the facility. For example, Hospital Appendix A, Task 2 states “The entire survey team should enter the hospital together. Upon arrival, surveyors should present their identification.” AOs must have comparable processes. Furthermore, we note that some AOs have already put identify verification processes in place, such as upon entry of the surveyor, the surveyor lead uploads identification information and survey notifications into portals accessible by their deemed facilities. We encourage AOs to develop processes that ensure identity verification and arrival procedures that align with CMS' expectations of unannounced surveys.
Comment:
We received several comments related to the predictability of surveys and the requirement that AOs conduct surveys at least every 36 months. One commenter suggested that facilities roughly are aware of the timeframe of their reaccreditation window. Multiple commenters observed that the requirement for surveys every 36 months makes surveys somewhat predictable.
Response:
We thank the commenters for their concerns, and we agree that while an accreditation/deeming cycle provides some level of predictability, surveys must be unannounced with no prior notice of arrival to the facility to maintain the integrity of the survey process. The intent of the proposed provision and definition of “unannounced survey” is to ensure an AO's administrative contact with facilities is variable and does not specifically address or imply the survey dates or month.
Comment:
We received several comments related to pre-survey contact for administrative purposes. One commenter also stated that administrative contact an AO has with its deemed facility is critical to ensuring that the size and complement of survey teams, and the length of surveys, are appropriate. This commenter stated that contact prior to survey ensures that the AO has the facility's application information, list of documents that will be required during the survey, contact information, hours of operation, and surgical schedules. The commenter stated that this maximizes the efficiency of the survey process. Another commenter stated that small, solo practitioner, and low-volume ambulatory surgical centers (ASCs) may operate with significantly smaller staff or may be closed during regularly scheduled hours due to illnesses of staff or due to vacations or personal matters of the practitioner. The commenter suggested CMS did not account for these operational challenges for pre-survey contact and pre-arrival notifications. One commenter stated that the proposed definition of “unannounced survey” is counterproductive and penalizes responsible providers from engaging with the AO for a productive survey. This commenter stated that communication between the AO and the provider is crucial to seamless execution of an unannounced survey and that surveys are resource-intensive, therefore by prohibiting preparatory dialogue would waste valuable time during the survey. The commenter also stated that pre-communication does not compromise the integrity of the survey process; operational preparations, including the logistical and operational scope of the survey should occur in advance for an efficient survey process.
Response:
We appreciate the commenters' concerns related to pre-survey contact, specifically administrative contact with a facility. Our proposal aims to ensure administrative contact with facilities prior to surveys is variable. We are not restricting AOs from contacting facilities to verify application details or request additional information, such as their current operating hours, upcoming surgical schedules, any extension locations, or providing the facilities with an agenda. However, contact prior to survey to gather additional information must not suggest when the survey will occur. For example, facilities due for a survey in December (near the end of their accreditation cycle), should not be contacted each September and surveys should not always be scheduled exactly in the same weeks of November or December. We note that the proposed provisions do not intend to limit an AO from communicating with their respective organizations prior to the survey to gather certain administrative information, such as operating hours and surgery schedules. The intent is for AOs to vary their preparatory contacts in a manner which is unpredictable and to ensure onsite surveys are unannounced. AOs must survey facilities at least every 36 months; therefore, we would expect any contact to be made 6 months, 3 months, 1 month or 2 weeks prior to onsite surveys randomly. We also appreciate the commenter's concerns and those challenges which may present due to small volume provider types with limited hours of operation, such as ASCs that operate once a week or a few times a month. We believe these requirements would not inhibit an AO from gathering needed information to facilitate planning for an unannounced survey.
Comment:
We received one comment that the proposed definition for “unannounced survey” does not reflect the flexibility of Section 2700A of the SOM. The commenter stated that flexibilities allowed by the SOM include a provision stating that non-long-term care facilities (other than home health) may be given advance notice in certain situations; and that our proposed definition does not reference the SOM, furthering the concern that the advance notice provision could be removed from future SOMs (for example, in effort to align with regulatory text). Another commenter recommended that CMS retains a window for notice of the survey the morning of and retain blackout dates to protect time for emergency preparedness and key activities requiring staff and resources.
Response:
We appreciate the commenter's concern related to the proposed definition of “unannounced survey” and our subregulatory guidance in Chapter 2, Section 2007A of the SOM. The subregulatory guidance provides for exceptions in limited circumstances. We recognize that in emergency events, a survey could disrupt the facility's ability to appropriately respond. However, CMS believes that emergency events would be unforeseen and not predicted and SAs and AOs will generally assess whether any survey activity would be feasible; the facility would not need to provide blackout dates in such cases.
Comment:
We received one comment suggesting inconsistent implementation of unannounced surveys with one AO, which has led to confusion. The commenter urged CMS to clarify its requirement for unannounced surveys, including recognition that some
( printed page 36383)
inpatient facilities could experience crisis scenarios that would not allow leadership to concurrently respond to an on-site survey in a timely manner.
Response:
We appreciate the commenter's concerns, and we note that the proposed provisions aim to clarify expectations for unannounced survey activities across all AOs. We recognize that in managing emergency events or crises that leadership may not be available during the survey. However, we expect facilities to designate an individual for daily operations should leadership be unavailable.
Comment:
While generally supportive of the definition and proposals, we received three comments which provided further recommendations for improving the unannounced survey process and encouraged CMS to consider these additional areas in subregulatory guidance. For example, two commenters stated to ensure the unannounced process works effectively, that CMS consider requiring providers to ensure a “duly authorized W-2 employee member of management” or a designated alternate be onsite at all times the office/facility is open. These commenters suggested that this would ensure an individual knowledgeable of company operations that has access to materials needed by surveyors is present, in turn limiting the potential for independent consultants to appear and act as the representative of the owner. Finally, the commenters also suggested that CMS consider “adding authorized W-2 employee” on the CMS-855 enrollment application as another category for management which could allow SAs and CMS to identify and monitor those individuals who appear as managing employees for multiple facilities and identify potentially fraudulent operations. Another commenter recommended CMS set clear expectations that an authorized employee be onsite when the facility opens to ensure survey activities are not delayed, as delays could limit the surveyor's ability to conduct a robust survey which could benefit lower performing agencies. This commenter suggested promoting prompt start times.
Response:
We appreciate the commenter's support for our definition of “unannounced survey.” We agree that leadership and a representative knowledgeable of the facility is important during the survey process and during the daily operations of the facility. We believe that when facility leadership is not onsite or on personal time off, the facility's governing body or leadership should appoint a knowledgeable individual able to provide continuity of care and operations for the facility; this individual should be able to provide SA and AO surveyors with the information needed and guide the survey processes. As noted in many CMS program appendices of the SOM, such as Appendix A Task 2 for hospitals, CMS guidance to survey teams states “If the Administrator (or person in charge) is not onsite or available (for example, if the survey begins outside normal daytime Monday through Friday working hours), ask that they be notified that a survey is being conducted. Do not delay the survey because the Administrator or other hospital staff is/are not on site or available.” We expect surveyors to begin survey activities upon arrival, and to notify staff and management that a survey is currently taking place. Surveyors may delay the entrance conference of the survey for leadership to arrive and begin requesting documentation from the facility while waiting. As for requiring prompt survey start times, we agree with the commenter, yet we also recognize the need for flexibilities to allow staff who may not be present at the time of the survey team arrival to travel to the facility. Surveyors aim to be flexible to ensure robust surveys are conducted with the appropriate staff. We encourage healthcare facilities to have the appropriate leadership and staff present during a survey.
Comment:
We received one comment, while in general support of unpredictability and unannounced surveys, that recommended unannounced surveys only apply to follow-up surveys when a provider or supplier has been previously cited for deficiencies. This commenter suggested that this approach would work for a common purpose to achieving excellence and that unannounced surveys as part of a follow up survey of a corrective action would be more appropriate. This commenter suggested this would build a level of trust and support, encourage facilities to excel in quality and allow a safe space for exploration to ensure health and safety standards are met, as opposed to penalizing poor performance or actively seeking mistakes.
Response:
We agree with the commenter that the intent of an unannounced survey is not to give the impression that surveyors are there to observe mistakes. The intent of an unannounced survey is to ensure the facility is always providing quality and safe patient care and to assess the daily operations of a facility against the Medicare requirements. Surveys by both SAs and AOs are not punitive but rather are an opportunity to identify deficiencies and mitigate potential harm to patients as well as staff. Unannounced surveys will provide a better assessment of the day-to-day operations at the facility. Furthermore, without an accurate assessment during an initial or recertification/reaccreditation survey and only requiring unannounced surveys as part of the plan of correction process for condition-level deficiencies (45-day revisit to the facility) would not accurately capture the normal daily operations of the facility and allow for unusual preparations hindering the integrity of the survey process.
Final Decision:
The requirement for unannounced surveys has been a long-standing requirement that ensures the integrity of the survey process and provides surveyors a clear depiction of the day-to-day operations of the facility without preparatory adjustments which may not reflect the true quality of care being provided to patients. While we appreciate some of the commenter's concerns surrounding physical security as well as the need for preparation for the survey, both at the facility level as well as from AOs gathering necessary information pre-survey, we are hereby finalizing the definition of “unannounced survey” without changes.
D. Conflicts of Interest
In the proposed rule, we cautioned that AOs that provide fee-based consulting would not be allowed to raise their accreditation fees or otherwise raise costs for the provider or supplier because of the provision of survey-related education (90 FR 12009).
We proposed changes to § 488.5(a)(10) to require AOs to have policies and procedures for the prevention and handling of conflicts of interest, and to notify CMS when those conflicts of interest arise, because on several occasions, AOs have failed to notify CMS of such conflicts of interest. These changes would broaden our oversight of the AOs' handling and reporting of conflicts of interests. Additionally, by requiring the AOs to provide CMS with more specific information about their conflict-of-interest policies and procedures, CMS would be afforded a more comprehensive look at how the AOs plan to handle specific scenarios that CMS would deem to be conflicts of interest. These proposed requirements would require those AOs that did not have policies and procedures to prevent, address, and handle conflicts of interests to develop and use them.
The proposed requirements at § 488.5(a)(10)(iii) for the submission of the AO's policies and procedures to
( printed page 36384)
avoid conflicts of interest (as defined in paragraph (a)(10)(v) of this section) included more detailed examples of possible scenarios that could be conflicts of interest for accrediting organization owners, surveyors, or other employees than those examples currently set forth in section 4008 of the SOM, which provide examples of potential conflicts of interest for SA surveyors.
A more detailed conflict-of-interest requirement is not necessary for the SA surveyors because SA surveyors, who are State employees, are generally required to report incidences of conflicts of interest to the SA management, who is tasked with taking the appropriate action. Additionally, State employees are generally prohibited from taking certain types of conflicting outside employment as a matter of course, so it is much less likely for such conflicts of interest to be an issue for them and their management. By contrast, AOs are more likely to encounter conflicts of interest. For example, AO owners, board members, surveyors and other employees might also be employed by healthcare facilities that are surveyed and accredited by that AO. Therefore, the proposed requirements for AOs were more detailed and prescriptive than those for SAs.
We also note here that we proposed two, slightly different, definitions of “immediate family member” at § 488.5(a)(10)(iii)(I) and at § 488.8(k)(2) (89 FR 12060 and 12062 through 12063). While we believe that the two definitions are legally and functionally equivalent, to avoid confusion over the minor language differences we have decided to standardize the definition in both provisions so that the language is the same. Therefore, we are making minor changes to the definition of “immediate family member” at § 488.8(k)(2) to now conform with the language we are finalizing at § 488.5(a)(10)(iii)(I). We do not believe that these minor changes to § 488.8(k)(2) in this final rule with comment period are substantively different than what we proposed, and therefore do not require a new round of public comment or a waiver of proposed rulemaking.
We received the following general comments about the conflict-of-interest proposals made in the proposed rule that are not associated with a specific conflict-of-interest proposed provision. We have grouped these comments by general topic.
Comments Stating General Support for the Conflict-of-Interest Proposals
Comment:
Many commenters supported the proposals that would prevent conflicts of interest, streamline survey processes, and ensure more consistency between AOs and CMS or SA surveyors. Commenters also voiced strong support for ensuring that organizations responsible for issuing standards, guidelines, education, training, and evaluations of performance are not adversely affected by competing interests in real or perceived conflicts of interest.
Response:
We thank the commenters for their support of our AO conflict-of-interest proposals.
Comments Expressing General Opposition to the Conflict-of-Interest Proposals
Comment:
One commenter stated that CMS has made multiple proposals intended to prevent conflicts of interest and recommended that CMS limit its conflict-of-interest (COI) proposals to sharing COI policies and the COI log during a corporate onsite review or at the agency's request. One commenter opined that the AOs should have the opportunity to investigate and verify the existence of a conflict of interest before providing notification to CMS.
Response:
Limiting our proposals to only requiring that AOs share their conflict-of-interest policies during application reviews would be insufficient to fully identify and address AO conflicts of interest. We agree that the AOs should be allowed to investigate and verify conflicts of interest before reporting them to CMS. No proposals included in the proposed rule prohibit an AO from verifying conflicts on the part of its owners, surveyors, and other employees before notifying CMS of these conflicts.
Comment:
One commenter stated that they were perplexed as to why CMS is not proposing the same conflict-of-interest requirements for SAs. This commenter also pointed out that, in the proposed rule, CMS stated that it believes a more detailed conflict-of-interest requirement is not necessary for the SA surveyors because SA surveyors, as State employees, are generally required to report incidences of conflicts of interest to the SA management, who are tasked with taking the appropriate action. CMS also opined that AOs are more likely to encounter conflicts of interest.
This commenter further stated that, while they agree that the nature of the business relationship between AOs and providers inherently creates greater opportunity for conflicts of interest, they believe nearly all the same situations CMS proposes as conflict-of-interest definitions are potentially present with SA surveyors.
This commenter also pointed out that in the proposed rule, CMS defined “conflict of interest” as a situation in which an AO, its owner(s), surveyors, or other employees, or the AO's successors, transferees, or assigns, or the immediate family members of the AO owners(s), surveyors, and other employees, have an employment, business, financial or other type of interest in or relationship with a healthcare facility the AO accredits. CMS would deem a conflict of interest to have occurred if one of the stated parties either knowingly or unknowingly exploited their interest in or relationship with that provider or supplier.
Response:
We agree that there are potential conflicts of interest for surveyors or other employees of the SA division conducting surveys, and for the immediate family members of these individuals, if there is an employment, business, financial or other type of interest in or relationship between a health facility the SA surveys and its surveyors and other SA employees and/or their applicable immediate family members. However, in response to the comment questioning why CMS did not propose the same conflict-of-interest requirements for SAs, CMS does not believe that additional Federal conflict-of-interest requirements are necessary for SAs as they are for AOs because individual State laws, rules, and regulations regarding conflicts of interest apply to each SA and its employees.
Comment:
One commenter appreciated CMS' diligence in preventing conflicts of interest during the accreditation process and agrees that the proposed language will mitigate inappropriate biases from affecting the survey processes. However, this commenter also recommended that CMS establish language that prohibits SA surveyors from surveying any facility where they were employed the previous 2 years, including facilities that are part of a larger health system. This commenter further opined that this is imperative in eliminating all conflicts of interest from surveyors, regardless of the agency that employs them.
Response:
SAs make their own policies and procedures regarding staff matters such as the handling of staff conflicts of interest and the Federal government typically does not interfere in internal State decisions.
( printed page 36385)
Nevertheless, consistent with Agreements between states and CMS under section 1864 of the Act, CMS holds the SAs responsible for assuring that any surveys for Medicare/Medicaid certification meet all Federal requirements, including conflict of interest requirements. Also, Chapter 4, Sections 4008 and 4008A of the SOM address the issue of conflicts of interest on the part of SA employees. Section 4008 of the SOM contains suggestions as to how the SA could handle such conflicts of interest. Section 4008A provides examples of conflict-of-interest scenarios on the part of SA employees that are similar to those we set forth in the proposed rule (89 FR 12005).
Comment:
One commenter stated that they have been proactive in taking steps to prevent real or perceived conflicts of interest to maintain the integrity and rigor of the accreditation process. This commenter also stated that they implemented strong firewall and COI policies to prevent any perceived or actual conflict of interest between its fee-based consulting company and accreditation divisions. This commenter stated that they strongly disagree with CMS' proposals to place limitations on fee-based consulting services provided by AOs to Medicare-certified providers and suppliers they accredit because of concerns related to conflicts of interest.
Response:
We note that in this final rule with comment period we have not prohibited AO fee-based consulting in its entirety; we have placed some limited restrictions on this service to help mitigate the conflicts of interest associated with specific AO consulting services and the timing of those services.
Comment:
One commenter observed that the restricted periods, prior to the initial survey and 12 months prior to each reaccreditation survey, are exactly when education is needed. This commenter further stated a belief that: (1) healthcare providers new to healthcare should attend workshops that provide the interpretation of regulations; (2) these workshops serve as a guide for businesses looking to navigate the complex world of healthcare regulations; (3) by attending these workshops, organizations could gain valuable insights and knowledge on compliance requirements; and (4) this knowledge would enable them to operate efficiently and effectively within the healthcare industry. This commenter further stated that, in addition to attending the workshops, the healthcare providers could also purchase workbooks and tools that could further assist them in understanding and implementing regulatory requirements.
Another commenter stated their view that the proposed rule would prohibit AOs from providing support and guidance to the facilities that they accredit in the months directly preceding a reaccreditation survey, when it is most needed. The commenter argued that AOs provide the most effective guidance to the facilities that they accredit because they are intimately familiar with the specific requirements of their standards. The commenter believed that the proposed rule would seek to disadvantage a facility by preventing the accrediting AO from providing valuable education during a critical period. In the commenter's view, the proposed rule places unnecessary obstacles in a facility's path to the provision of high-quality care.
Response:
The restrictions on consulting do not prohibit the AOs from providing consulting services or workshops to the providers and suppliers they accredit prior to a re-accreditation survey. Consulting services, as defined in § 488.1, must not be provided within 12 months prior to the next scheduled re-accreditation survey pursuant to § 488.8(i)(2). This means, for example, that the AOs would still be able to provide consulting, including workshops, to the providers and suppliers it accredits during the 24 months after each accreditation survey was completed in a 36-month accreditation cycle.
We believe that, after an accreditation survey, an AO's consulting services would be geared towards helping the facility correct deficiencies and non-compliance with the AO's accreditation standards that were detected during the survey. We further believe that the best time for an AO to provide such consulting services would be within the 24-month period after an accreditation survey has been completed. During this period, the survey findings are fresh in the minds of the facility management and compliance team and there would be an impetus to address and correct the deficiencies cited. We further believe if the AO provides consulting services to address deficiencies and compliance concerns early in the 3-year accreditation period, the AO could work with the affected provider or supplier, at their own pace, to implement long-lasting and sustainable changes that would address the deficiencies identified. On the other hand, if the AO waited until 12 months prior to the next accreditation survey due date to provide consulting, it might only result in the implementation of quick temporary solutions or corrective action just prior to the next accreditation survey.
Comment:
One commenter stated that CMS' proposal to prohibit receiving fee-based consulting services from an AO at any time before an initial accreditation survey or in the 12 months before a re-accreditation survey would restrict the ability of many health systems to receive necessary education and could delay their ability to be accredited in a timely manner.
Response:
We respectfully disagree with this commenter's contention that our restrictions on AO consulting, as finalized, will prohibit providers and suppliers that are seeking accreditation by an AO that provides consulting from seeking consulting prior to the initial survey. This is because these providers and suppliers would be permitted to seek fee-based consulting from a third party at any time, without restrictions. Also, any provider or supplier already accredited by any AO can seek consulting services from another AO provided that AO does not accredit the provider or supplier at the time the consulting services are furnished.
Comment:
One commenter noted that, under the proposal, providers would not have the benefit of receiving education from the creator of the standards who could best teach the requirements of compliance. The AO standards include not only regulatory language but also AO-specific requirements. Many organizations seek Medicare certification through an AO versus the State Agency because of the valuable education that the AO provides. The type of education provided often distinguishes one AO from another. Restricting the provision of fee-based education diminishes competition, and forces each AO to provide the exact same product.
Response:
General education provided by an AO would not necessarily constitute a conflict of interest and is not entirely prohibited under this rule, regardless of whether it is fee-based education. Section 488.8(i)(4) finalized here allows AOs to provide general education as well as fee-based consulting services at specific times and under certain conditions. However, any AO fee-based education that meets the definition of fee-based consulting services finalized here and does
not
meet the timing and condition requirements at § 488.8(i)(4) would be prohibited by this rule.
Comment:
One commenter opposed the proposals that would limit the ability of health systems to receive fee-based consulting services from their AO for the following reasons:
( printed page 36386)
AOs are uniquely situated to provide consulting services with firewalls in place that prevent conflicts of interest.
Fee-based consulting services can include educating health system staff on the CoPs and guiding them on how best to comply with them.
Fee-based consulting services play an important role in assisting providers with their compliance with CoPs and their quality and patient safety improvement efforts.
Fee-based consulting can assist health systems in improving the safety and quality of the care they provide to their patients.
Response:
In our view, the restriction on fee-based consulting will not completely prohibit providers and suppliers accredited by the AOs from obtaining fee-based consulting. These providers and suppliers will only be restricted from receiving AO fee-based consulting from their AO prior to their initial survey and during the 12 months immediately preceding their reaccreditation survey. The accreditation period for most providers and suppliers is 36 months; therefore, the providers and suppliers would be able to receive AO fee-based consulting during the first 24 months of the 36-month accreditation period. In addition, providers and suppliers may seek fee-based consulting at any time from third party consultants because there is no conflict of interest associated with the fee-based consulting provided by third parties.
Comment:
One commenter stated that if CMS' proposals are finalized, overall survey costs will increase, due to factors such as limited consulting resources or increased interruptions in hospital operations.
Response:
We disagree that these requirements as finalized in this rule will inevitably lead to increased overall survey costs due to the factors the commenter noted. While the rule puts specific limitations on an AO that provides consulting services to a facility that the AO accredits, the rule does not prohibit an accredited facility from using the consulting services provided by other AOs that do not accredit the facility or by third-party consultants, and thus does not limit the overall consulting services that might be available to facilities. Without further clarification by the commenter, we are not clear why they believe that this rule would cause interruptions in a hospital's or other facility's operations.
Comment:
One commenter supports the proposed definition of conflict of interest.
Response:
We thank this commenter for their support of our proposed definition.
Comment:
One commenter noted that proposed § 488.5(a)(10)(iii)(I) would provide that an immediate family member of an AO surveyor who was employed in a healthcare facility that was accredited by the AO would be deemed a conflict of interest. This commenter further observed that, by contrast, the United States (U.S.) Federal government does not restrict immediate family members from working in different facets of the government or as a contractor to the government.
Response:
This commenter is correct that the proposed regulations would prohibit an AO owner, AO surveyor or other AO employee from having any involvement in the survey process for the healthcare facilities in which they, or their immediate family members, have a relationship or interest that existed within 2 years prior to the AO owner's, surveyor's or other employee's employment by the AO. If such a situation were to exist, it would be a conflict of interest. We have proposed to add the provisions at §§ 488.5(a)(10)(iii)(I) and 488.8(k) to prevent such conflicts of interest, including those involving immediate family members as defined at § 488.8(k)(2), from occurring. The commenters' reference to multiple family members working for governmental entities is not comparable to the scenario in which an AO surveyor might be expected to change his assessment to benefit the facility family member because family members working for different government agencies generally are not able to provide benefits for each other.
Comment:
One commenter disagreed with the proposed definition of “immediate family member”. This commenter noted that this proposed definition closely resembles that used in reference to the professional courtesy exception for physician and healthcare entity referral prohibitions, Securities and Exchange Commission restrictions on transactions with related persons, and laws related to campaign contributions.
This commenter stated that such an expansive definition of “immediate family member” as used for the purposes of securities transactions and campaign contributions would be inappropriate for application to healthcare conflict-of-interest considerations.
Response:
We used the same definition of “immediate family member” that we finalized for hospices in the CY 2022 Home Health Prospective Payment System Rate Update (86 FR 62368 and 62426), which is codified at § 411.351. While this definition may be the same or similar to other rules for other subject matter, this does not make it inappropriate for use in a healthcare setting.
A definition of “immediate family member” is necessary because, at § 488.5(a)(10)(iii), we proposed to require the AOs to provide policies and procedures for the prevention and handling potential or actual conflicts of interest that could arise from situations in which an AO owner, surveyor, or other employee has a business, employment or financial interest in or relationship with another survey agency or healthcare facility to which the AO provides accreditation services.
At proposed § 488.5(a)(10)(iii), we stated that such interests or relationships would include but not be limited to, “(I)
Having members of their immediate family engaged in any of the above stated activities.”
Moreover, at § 488.8(k), we proposed that it would be a conflict of interest if AO employees, surveyors, and other employees have a member of their immediate family employed at a healthcare facility that is accredited by the AO. We made this proposal because it is possible that one of the subject individuals could either consciously or unconsciously exploit their interest in or relationship with that provider or supplier. Also, allowing an AO owner, surveyor or other employee that has an interest in or relationship with or that has an immediate family member that is employed by or has an interest in or relationship with (as defined by proposed § 488.5(a)(10)(iii)) a healthcare facility that is accredited by the AO would not only be inappropriate but could result in inaccurate survey results and/or preferential treatment of the facility. We say this because if an AO owner, surveyor or other employee has a family member employed at a healthcare facility that is accredited by the AO, that AO owner, surveyor or other employee may have a bias towards or against that facility which could have an effect on the survey results.
An AO surveyor, owner, or other employee that has an interest in or relationship with a healthcare facility the AO accredits might have additional motivation to improperly give that healthcare facility notice about the survey ahead of the scheduled survey date. Surveys are required to be unannounced to prevent the facility from preparing for the survey by activities such as unusual cleaning activities, painting, clearing obstructions from halls and entrances,
( printed page 36387)
covering up and hiding deficiencies, coaching staff, and otherwise preparing in advance for the survey. If the survey is unannounced, the healthcare facility is not able to make advance preparations so that the survey team is able to assess the facility in its usual condition and observe the typical standard of care provided.
If an AO owner, surveyor or other employee has an immediate family member that is employed by a healthcare facility that is accredited by the AO, that immediate family member might provide confidential or proprietary information about the healthcare facility to the AO owner, surveyor or other employee that the AO would not otherwise be entitled to receive. The immediate family member employed at a healthcare facility accredited by the AO could also provide information about incidents that have occurred at the facility, safety and quality concerns or other issues. This would be a problem because this unfiltered information may be damaging to the facility for several reasons. First, this person may have incomplete or inaccurate information. Second, the information provided by the family member could affect the course of the survey, the survey findings and objectivity of the survey results.
Comment:
One commenter stated a concern that the conflict of interest on the part of some extended family members included in the definition of “immediate family member” are unlikely to be known in many instances.
This commenter was concerned that, while a potential conflict could exist if conflicts with immediate family members are known to the AO, there is no requirement within this proposed rule that the information
actually
be known for a conflict to exist because the proposed rule (89 FR 12005) says “unknowingly exploited interest”.
To illustrate their concern, the commenter provided the following scenario:
An AO surveyor resides in Washington and has a brother-in-law that resides in Georgia.
The surveyor only speaks to her brother-in-law every other year at Thanksgiving.
The AO at which the surveyor is employed accredits a small ASC in Tennessee (fictional “Anytown ASC”).
The AO surveyor performs a survey of Anytown ASC in Tennessee in May 2024.
The surveyor's brother-in-law has an ownership interest in Anytown ASC in Tennessee that his sister-in-law is surveying. This interest was obtained in January 2023.
The AO surveyor was not aware that her brother-in-law obtained an ownership interest in Anytown ASC in January 2023.
This commenter requested that CMS reconsider the definition of “immediate family member” to address its appropriateness, reasonableness, and applicability.
Response:
We have proposed to require AOs provide annual surveyor declarations of conflicts of interest and also that AO owners, surveyors, and other employees be prohibited from having involvement in the survey process for any healthcare facility accredited by the AO with which they or their immediate family members have an interest or relationship. While these proposals are silent on this issue, it is implied that the AOs will only be required to report and act on known conflicts of interest. We certainly cannot hold AOs, their owners, surveyors, and other employees accountable for any conflicts of interest of which they are unaware. Therefore, we do not believe that it is necessary to revise the proposed definition of “immediate family member.”
This does not mean that the AOs, their owners, surveyors, and other employees can ignore such potential conflicts of interest. AOs, owners, surveyors, and other employees have a duty to investigate whether they or their immediate family members, as defined in the proposed rule at § 488.5(a)(10)(iii), might have applicable conflicts of interest. AOs will be required to obtain surveyor conflict-of-interest information on an annual basis. AO surveyors and other employees will be required to take reasonable steps to determine whether they have interests in or relationships with healthcare facilities accredited by the AO, both on their part and on the part of their immediate family members.
If an AO, AO owner, surveyor, and other employee should reasonably have known about a conflict of interest on their part or the part of an immediate family member and it is not reported to CMS on a surveyor declaration, or an AO owner, surveyor, or other employee was permitted to have involvement with the survey process for a healthcare facility for which they reasonably should have known they had an interest in or relationship with, CMS has the option to place the AO on a CMS-approved accreditation program review pursuant to § 488.8(c).
Comment:
One commenter requested that CMS clarify the applicability of the proposed requirement for information to be submitted with the AOs' conflict-of-interest policies and procedures to different types of AO employees.
Response:
Our proposal for information to be submitted with the AOs' conflict-of-interest policies and procedures applies to the AO and not any specific individual or group of AO employees. This proposal requires that the AO provide more specific information with the conflict-of-interest policies and procedure it provides to CMS with the initial and all subsequent renewal applications for CMS approval of the AOs accreditation programs.
However, § 488.5(a)(10)(iii) does require an AO to submit information to CMS regarding its policies and procedures for the prevention and handling of potential or actual conflicts of interest and it does specify that these conflicts of interest are those that could arise from situations in which an accrediting organization owner, surveyor, or other employee has an interest in or relationship with a SA or with a healthcare facility to which the accrediting organization provides accreditation services. In response to the commenter's request for clarity as to whom the requirements for such information would apply, § 488.5(a)(10)(iii) provides examples of the interest and relationships with a healthcare facility that would be a conflict of interest on the part of an AO owner, surveyor or other employees, including:
being employed as a SA surveyor;
being employed in a healthcare facility that is accredited by the AO;
having an ownership, financial or investment interest in a healthcare facility that is accredited by the AO;
serving as a director of or trustee for a healthcare facility that is accredited by the AO;
serving on a utilization review committee of a healthcare facility that is accredited by the AO;
accepting fees or payments from a health facility or group of health facilities that is/are accredited by the AO;
accepting fees for personal services, contract services, referral services, or for furnishing supplies to a healthcare facility that is accredited by the AO;
providing consulting services to a healthcare facility that the AO accredits;
having members of their immediate family engaged in any of the stated activities; and
engaging in any activities during the course of the survey of the facility that would be or cause a conflict of interest.
Section 488.8(k) provides that it would also be a conflict of interest if an AO owner, surveyor or other employee
( printed page 36388)
has an immediate family member that has an interest in or relationship with a healthcare facility accredited by the AO. In such a scenario, the AO owner, surveyor, or other employee should not be permitted to have any involvement with the survey process for the healthcare facility at which their family member is employed or has an interest or relationship.
2. Comments Generally Supporting the Proposal for Information To Be Submitted With an AO's Conflict-of-Interest Policies and Procedures
Comment:
Five commenters supported the proposed requirement that the AOs provide, as a part of their initial and renewal application, specific policies and procedures that would address how the AO addresses and prevents conflicts of interest. One commenter stated that proposed revision to § 488.5(a)(10) for information to be submitted with the AOs' conflict-of-interest policies and procedures are common sense updates on unintended gaps in the accreditation ecosystem. This commenter further stated that if these unintended gaps are not fixed, opportunities for conflicts of interest will persist in the system. One commenter stated that the requirement that the AOs provide, as part of their initial and renewal applications, specific policies and procedures that would address how the AOs prevent and address conflicts of interest would put pressure on AOs to create firewalls to address these concerns. One commenter expressed support for the proposed requirements for AOs that do not have policies and procedures to prevent, address and handle conflicts of interest to develop and use them. One commenter expressed support for the proposal for expansion and revision of conflict-of-interest policies and procedures. This commenter stated that these AO conflict-of-interest improvements would secure the overall fairness and transparency of the survey process. One commenter supported CMS' efforts to increase oversight of AO conflicts of interest while providing a requirement that does not impose additional burden on providers. One commenter stated that § 488.5(a)(10) is already a requirement for approval of an AO. This commenter further opined that the proposed requirement could strengthen our policies to reflect the high standards of their AO. One commenter fully supported our proposal to require the AOs to provide more specific information in the conflict-of-interest policies and procedures they submit to CMS. This commenter stated that the requirement will protect the integrity of the survey process and provide guidance to surveyors.
Response:
We thank these commenters for their support of our proposal at § 488.5(a)(10) to require the AOs to submit more specific information with their conflict-of-interest policies. Robust and strictly enforced firewall policies and procedures can help mitigate the effects of conflicts of interests. We believe that it is important for the AOs that provide fee-based consulting to have fee-based consulting firewall policies and procedures. We thank these commenters for their support of our proposed requirement at § 488.5(a)(10) that the AOs submit policy and procedure to address conflicts of interest.
3. Comments Generally Opposing the Proposal for Information To Be Submitted With an AO's Conflict-of-Interest Policies and Procedures
Comment:
One commenter stated that requiring AOs to turn over their conflict-of-interest policies and logs over to CMS would require the AOs to share proprietary information and internal business operations.
Response:
We respectfully disagree with this commenter. We are not sure what this commenter considers to be proprietary information and internal business operations. However, we do not consider the AOs conflict-of-interest policies and procedures or information about AO conflicts of interest to be proprietary information. AOs are already required by our regulations to provide their accreditation standards and all policies and procedures related to the accreditation and survey processes (including those related to detecting and handling conflicts of interest) to CMS as part of their initial and renewal applications they submit seeking approval for their accreditation program. For example, § 488.5(a)(10) already requires AOs to provide their
“
policies and procedures to avoid conflicts of interest, including the appearance of conflicts of interest, involving individuals who conduct surveys or participate in accreditation decisions.”
Although we do not believe that the surveyor declarations and reports containing information about the fee-based consulting services provided would fall under the category of proprietary information or internal business operations, we have no plans to publish this information. It is our intent, to the extent permissible by law, that the information collected be for internal CMS use only.
Comment:
One commenter requested clarification on how the revised requirements at § 488.5(a)(10), if finalized, will be different from the existing requirement of this regulation.
Response:
In the proposed rule (89 FR 12005), we discussed the difference between the existing regulation and the revised requirements at § 488.5(a)(10). Section 488.5(a)(10) currently requires that the AO submit
“the organization's policies and procedures to avoid conflicts of interest, including the appearance of conflicts of interest, involving individuals who conduct surveys or participate in decisions.”
This requirement does not require the AO to address any specific areas or issues in their conflict-of-interest policies and procedures. In addition, the AOs only need to submit this information to CMS with their initial and renewal applications, which is currently every 6 years or less, as established by CMS.
Comment:
One commenter recommended that CMS ensure that the new policies the AOs will need to develop do not unintentionally result in disruptions to providers seeking to become accredited or maintain accreditation.
Response:
We do not anticipate that the accreditation process will be disrupted by the revised requirements at § 488.5(a)(10)(i) to § 488.5(a)(10)(v). All AOs that accredit Medicare-certified providers and suppliers will be required to submit conflict-of-interest policies and procedures that comply with the requirements of proposed § 488.5(a)(10)(i) to (v). To be approved by CMS, all AOs are required to have some type of conflict-of-interest policies and procedures; however, prior to this proposed rule CMS did not have any minimum requirements for the contents of these COI policies. This means that the AOs will simply need to update their existing COI policies and procedures to comply with the new requirements.
Final Decision:
After consideration of all comments received regarding the proposed requirement for AOs to submit specific information with the conflict-of-interest policies and procedures they submit to CMS with their initial and each subsequent renewal application, we have decided to finalize the requirements with a minor clarifying revision to § 488.5(a)(10)(iii) to change the proposed language of “... potential or actual conflicts of interest that could arise from situations in which an accrediting organization owner, surveyor, or other employee has an interest in or relationship with
another State survey agency or a healthcare facility
to which the accrediting organization provides accreditation
( printed page 36389)
services” [emphasis added] by changing the word “another” to “a” and adding the words “with a” so that the finalized provision reads “... situations in which an accrediting organization owner, surveyor, or other employee has an interest in or relationship
with a State survey agency or with a healthcare facility
to which the accrediting organization provides accreditation services” [emphasis added]. We are making this revision in this final rule with comment period to clarify the requirement.
Additionally, commenters requested that we establish a clear definition of the AO consulting services on which we will be placing the proposed restrictions and provided us with an example of such a definition for purposes of this rule. We have used this definition from the public comments as the basis for the definition of “fee-based consulting services” that we are including in this final rule with comment period. We discuss this definition in more detail in section III.D.3. of this final rule with comment period.
E. Comments on the Proposed Requirement That AOs Obtain and Submit Surveyor Declarations of Any Interest in and Relationships With Healthcare Providers the AO Accredits to CMS on an Annual Basis (Proposed § 488.5(a)(22))
A conflict of interest may exist when an AO surveyor has interest(s) in or relationship(s) with a healthcare facility the AO accredits. We believe that requiring AOs to obtain and submit declarations detailing such interests and relationships would ensure that CMS would be notified of potential or actual conflicts of interest AO surveyors might have with the providers and suppliers the AO accredits. Such notice would allow CMS to be aware of the existence of these potential or actual conflicts of interest, some of which would preclude a surveyor from participating in survey activities (see § 488.8(j) discussion at section IV.B.6. of the proposed rule) and some of which would not.
We proposed to add a new provision at § 488.5(a)(22) that would require the AO to obtain declarations from all surveyors employed or contracted to the AO regarding any employment, business, financial or other interests in or relationships they have with the healthcare facilities the AO accredits. We proposed that AOs would initially be required to submit the surveyor declarations with their initial application for CMS approval of their accreditation programs. We further proposed to require that the AOs update the surveyor declarations on an annual basis, and that the information from the annual updated surveyor declarations be submitted to CMS no later than December 31st each year. Annual updates would be necessary because a surveyor's interests in and relationships with healthcare facilities the AO accredits could change over time. This requirement would ensure that the information contained in the surveyor declarations remains up-to-date and accurate. We proposed that this provision at paragraph (a)(22) would be become applicable beginning 1 year after the effective date of the final rule with comment period. We further proposed to require the AOs to begin submitting their surveyor declaration information on or before the December 31st date that occurs after the proposed applicable date of this requirement.
We received the following comments regarding this proposal. We group the comments and our responses by topics for clarity.
a. General Comments About the Proposal To Require AOs To Submit Surveyor Conflict-of-Interest Declarations
Comment:
One commenter supported our proposal to require AOs to obtain and submit surveyor declarations of any interest in and relationships with healthcare providers the AO accredits to CMS on an annual basis for the following reasons:
Organizations entrusted with the public's well-being must disclose their affiliations to ensure impartiality and maintain public trust.
Any suggestion of impropriety or conflict of interest could compromise the integrity of the accreditation process, emphasizing the paramount importance of full transparency.
Prioritizing excellence, quality, and integrity over financial interests is crucial.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter stated that they have always required the completion of conflict-of-interest statements from all their staff as a standard compliance practice. The commenter further stated that they are diligent in managing and enforcing their conflict-of-interest processes as a first-line measure in controlling any threat to their accreditation program's integrity. Another commenter stated that they require the completion of a conflict-of-interest statement in the following instances:
All staff complete a COI statement at the time of hire; senior leadership staff additionally sign a COI statement annually.
Board of Director members sign a COI statement at the time of board appointment and annually throughout their term.
Surveyors sign a COI statement at the time of hire, annually, and if new conflicts of interest arise.
Response:
We thank this commenter for their comment. We further commend this commenter on their commitment to preventing, detecting, and managing conflicts of interest.
b. Comments in Support of the Proposal for AOs To Submit Surveyor Conflict-of-Interest Declarations
Comment:
Two commenters supported our proposal to establish processes for ensuring that AO surveyors do not have conflicts of interest in the review process, including surveyor relationships with a healthcare facility or another survey agency.
Response:
We thank these commenters for their support of this proposal.
Comment:
One commenter stated that they already have a strict surveyor conflict-of-interest process. The commenter further stated that requiring a declaration from each surveyor is unnecessarily burdensome to their established process.
Response:
We thank this commenter for their comment and note their concern about the burden related to this proposal. Please see section VI. Collection of Information of this final rule with comment period for more information about the burden associated with this rule.
Comment:
One commenter supported our proposal to require the AOs to provide conflict-of-interest information on past employees and other areas.
Response:
We believe this commenter is referring to our proposal to require the AOs to collect surveyor conflict-of-interest declarations and submit them to CMS on an annual basis. If so, we thank this commenter for their support of this proposal. We would like to point out that this requirement, as finalized, doesn't require the AOs to collect conflict-of-interest information about past employees or areas other than current interests in or relationships the AO's surveyors may have in any healthcare providers or suppliers accredited by the AO.
Comment:
One commenter had several questions about this proposal including:
How are new hires and terminated surveyor declarations to be handled throughout the year? Are the submissions to be electronic? What does CMS intend to do with this information? For instance, would CMS review each
( printed page 36390)
one of the declarations annually and would declarations of “no conflict of interest” be confirmed? If so, how would this be accomplished?
Response:
We will provide subregulatory guidance on submission and compliance when this requirement becomes effective.
Comment:
One commenter stated that they require all employees to complete annual COI declarations regarding any employment, business, financial, or other interests in or relations they have with healthcare facilities that this AO accredits. The AO expressed concerns with the proposal to require AOs to submit surveyor COI declarations to CMS because these declarations have personal information that may violate employee confidentiality or other privacy laws if shared publicly. This commenter recommended that CMS modify this proposal to require only a review of AO surveyors' COI declarations at the time of the CMS corporate onsite review for each AO. This commenter stated that their suggested alternative would still allow CMS to achieve its stated goal and that there was no reason for CMS to require AOs to unnecessarily disclose sensitive information. This commenter also stated that the AO should not be required to submit the surveyor conflict-of-interest disclosures to CMS because they would contain sensitive information.
Response:
Our rule, as finalized, will require the AO to submit declarations from all surveyors the AO employs, describing any employment, business, financial or other interests in or relationships they have with the healthcare facilities the AO accredits. Even if this is sensitive or confidential information, it is necessary for enforcement of our policy and, to the extent permitted by law, we would keep this information internally and not publish it or provide it to any outside source. Proprietary commercial information and trade secrets are protected from public disclosure under FOIA Exception 4 (5 U.S.C. 552(b)(4)).
e. Recommended Changes to Proposal That AOs Submit Surveyor Declarations
Comment:
One commenter recommended that CMS modify this proposal to allow the AOs to submit 100 percent of surveyor COI declarations for year one after the final rule with comment period implementation date. Thereafter, for each calendar year, AOs would only submit COI declarations for new surveyors and updated COI declarations for surveyors where a baseline COI declaration was submitted in year one.
Another commenter suggested that implementing and managing a COI declaration process might complicate the survey process and increase the administrative burden on AOs and complicate the survey process by requiring additional resources. This commenter recommended that CMS make the implementation of the surveyor declaration process as minimally burdensome as possible on all entities.
Several commenters expressed support for the proposed requirement for collection of surveyor declarations on an annual basis but requested that AOs be allowed to keep the declarations and not be required to submit them to CMS. One of these commenters suggested that CMS review them during the corporate office visit as part of each AO's initial/renewal application rather than requiring the AO to submit them to CMS on an annual basis.
Response:
After consideration of the comments received regarding our proposal to require the AOs to submit surveyor conflict-of-interest declarations to CMS on an annual basis, we have decided not to finalize this proposal as proposed. We are not finalizing our proposal to require the AOs to obtain and submit the surveyor declarations to CMS annually. We will instead require the AOs to submit the surveyor conflict-of-interest declarations for CMS to review upon request and during each application review process.
Comment:
One commenter stated that receiving and maintaining the declarations could be unnecessarily burdensome to CMS. This commenter requested that the surveyor declarations be handled on an exceptions basis whereby the declaration would only need to be reported to CMS if it indicated a conflict of interest. In the alternative, CMS could conduct audits of the AOs annually to ensure the declarations are obtained and maintained as required.
Response:
We have also considered the burden to CMS associated with the receipt and review of these declarations and have decided to modify our proposal related to surveyor declarations as stated in the “Final Decision” section.
Final Decision:
After consideration of the comments received regarding our proposal at § 488.5(a)(22) to require the AOs to submit surveyor conflict-of-interest declarations to CMS on an annual basis, we have decided not to finalize this as proposed. We will instead require the AOs to maintain the surveyor conflict-of-interest declarations, to be provided to CMS to review upon request and during each application review process. We are also modifying the provision as proposed by removing the sentence from applicable regulations text, “This provision will become applicable beginning [DATE 1 YEAR AFTER THE EFFECTIVE DATE OF THE FINAL RULE].” We are making this modification for the final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date and individual provisions will no longer need to be specified in the regulatory text.
F. Proposed Restrictions on Fee-Based Consulting Services Provided by AOs to the Medicare-Certified Providers and Suppliers They Accredit (Proposed § 488.8(i))
CMS recognizes the value of consulting services provided by independent, third-party consultants who provide insight and expertise to assist facilities in achieving and maintaining compliance with the AO and Medicare health and safety standards. These interventions are beneficial and often tailored to meet a facility's specific compliance needs. Consulting services also may assist a provider or supplier in identifying quality concerns, whether based on the Medicare requirements or standards of practice, and therefore these services may improve the safety of patient care. AO consulting activities are not prohibited by Federal law and there are no current CMS regulations prohibiting AOs from providing consulting services.
However, AOs assume a public trust role when voluntarily applying to CMS for deeming authority. This authority, once granted, conveys Medicare certification for those entities accredited by the AO and it is essential that the integrity of the AO oversight process be above question. A number of AOs with CMS-approved accreditation programs currently provide AO consulting services to the Medicare-participating healthcare facilities they accredit as well as to facilities that they do not accredit. When an AO provides consulting services to a provider or supplier it accredits, it may create a conflict of interest for several reasons.
First, AOs provide deeming surveys to providers or suppliers on behalf of CMS. AOs are required to use accreditation standards that are comparable to or exceed the Medicare standards and survey processes in the performance of deeming surveys. A potential or actual conflict of interest arises from allowing a CMS-approved AO with deeming authority the ability to charge a provider or supplier to conduct a deeming survey to identify non-compliance (for
( printed page 36391)
Medicare participation) and also charge for providing AO consulting services to help the provider meet Medicare requirements.
Second, providers and suppliers often choose AO consulting specifically for the additional resources and assistance provided. Some AOs publicly advertise the ability of their consulting services to simulate what to expect from the actual AO survey. It is possible that providers and suppliers found to be non-compliant by their AO may assume that the most direct path to compliance is to hire the AO's consulting services. Such an assumption would provide AOs with consulting services an unfair advantage over other, third-party consulting services.
Finally, by charging for accreditation services (for example, deeming surveys) and also for the subsequent consulting services, for the purpose of remediating deficiencies identified by the same AO, there may be an expectation from providers and suppliers that the AO would demonstrate the effectiveness of their consulting services for such deficiencies on subsequent compliance surveys. In other words, the provider or supplier may expect to receive a favorable survey report because they have paid the AO not only for accreditation but also for consulting services which are promoted by the AOs to help the provider or supplier do well on their survey. In addition, this expectation may push AOs to ignore significant deficiencies found during survey of its consulting clients to demonstrate the efficacy of its consulting and to promote these services.
In short, an AO's business model is geared toward retention of its accredited providers and suppliers. AOs that provide both regulatory oversight through Medicare deeming surveys and also consulting services, which are geared towards assisting clients comply with the requirements required to pass the surveys, invite concerns about the integrity of their final compliance determinations.
CMS issued an AO Conflict-of-Interest RFI (83 FR 65331) in 2018 to gather feedback related to AO conflict-of-interest practices. We received 128 public comments in response to the RFI. Many commenters stated that consulting provided by an AO or its associated consulting division or company to the healthcare facilities it accredits is a conflict of interest. These commenters stated that this conflict of interest arises from granting the inherently governmental function of monitoring patient safety, by regulating healthcare providers through accreditation, to a private entity, especially when that private entity profits from those who are regulated.
Several commenters alleged that AOs that provide fee-based consulting may have the incentive to ignore deficiencies detected during the accreditation survey, to provide a “good” survey report to demonstrate the apparent efficacy of their AO consulting services and also to keep the paying customer(s) happy. Many commenters also suggested that if an AO provides poor survey results to a healthcare facility that has paid a significant fee for accreditation, it is unlikely that the facility would continue to retain that AO as a service provider.
After careful review and analysis of the public comments received in response to the RFI, we agree that a conflict of interest arises from the contractual and financial relationship between the healthcare provider and the AO, which is a private entity that profits from the performance of regulating healthcare providers through accreditation. AOs that provide consulting services generate additional revenue beyond the fees realized for accreditation services by providing consulting services to the same facilities they accredit.
We proposed at § 488.8(i) several restrictions on fee-based consulting provided by these AOs, their consulting divisions, or separate business entities. By “fee-based consulting division,” we mean a separate division within the AO that provides consulting services. This division of the AO would have a separate manager and staff. By “separate business entity,” we mean a business entity, such as a company or corporation, that is separate and apart from the AO and that has been established by the AO, either under a similar or different name, for the purpose of the providing consulting services.
The proposed regulation at § 488.5(i) would still allow AOs to provide fee-based consulting services to the providers and suppliers they accredit with restrictions that address the conflict-of-interest issues associated with this service.
We proposed at § 488.8(i)(1) that, unless excepted under proposed § 488.8(i)(4), AOs and their associated consulting divisions or companies would be prohibited from providing fee-based consulting services to any healthcare provider or supplier to which the AO provides accreditation services prior to an initial accreditation survey. However, the healthcare provider or supplier may seek fee-based consulting services from an entity entirely uninvolved in that provider's or supplier's accreditation process. This option allows these providers and suppliers support they may believe necessary to meet Medicare standards and requirements prior to serving patients while eliminating any conflict of interest for their AO.
For purposes of proposed § 488.8(i)(1), the term “initial survey” would mean the first accreditation survey of a healthcare provider or supplier performed by an AO. The term “prior to the initial accreditation survey” would mean the time period beginning on the day the provider or supplier enters into a contract with the AO to provide accreditation services and continuing until the date that the initial accreditation survey is completed. The survey completion date would include the completion of any required plans of correction by the provider or supplier. In addition, if a healthcare provider or supplier was terminated or withdrew from the AO's accreditation and later retained the services of that AO, the first survey of the returning healthcare provider or supplier performed by the AO would be considered an initial accreditation survey.
The requirement of proposed § 488.8(i)(1), which would prohibit an AO from providing fee-based consulting or coaching to a healthcare provider or supplier prior to the initial accreditation survey, would provide a more accurate assessment of the provider's or supplier's baseline operating conditions and deficiencies on the initial survey. Such a raw assessment would not be possible if the provider or supplier receives AO consulting prior to the initial accreditation survey.
In addition, such a baseline assessment of deficiencies would be useful to the AO in assessing areas needing improvement and developing a plan of correction and areas of focus for its consulting services. This restriction would also remove the financial incentive on the part of the AO to ignore deficiencies during the initial survey of providers and suppliers that paid for consulting services prior to an initial survey.
We note that this proposal only restricts an AO with deeming authority and a consulting practice from providing consulting services to its accredited providers and suppliers prior to the initial accreditation survey. It does not prohibit providers and suppliers from hiring third-party consulting services prior to their initial AO survey— in other words, this proposal does not prohibit other
( printed page 36392)
consulting services from being used during this period.
We do not anticipate that this proposal would cause a negative impact on the patient care provided by the provider or supplier for several reasons. First, providers or suppliers would be able to obtain AO consulting during the first 24 months of the 36-month reaccreditation cycle which occurs after the initial survey. This education could be tailored to address the deficiencies found during the initial survey. Second, the provider and supplier could always seek consulting services and education prior to the initial survey from a third-party consultant or an AO other than the one that is doing their survey. The purpose of our proposal to prohibit AO fee-based consulting prior to the initial survey and during the 12-month period prior to each reaccreditation survey was to reduce or remove any potential or actual conflict of interest. However, if a provider or supplier were to seek consulting from a third-party consultant that has no relationship to the AO that accredits that provider or supplier, no conflict of interest would exist.
We also proposed at § 488.8(i)(2) to prohibit AOs from providing fee-based consulting services to a healthcare provider or supplier it accredits within 12 months prior to the next scheduled re-accreditation survey of that provider or supplier. For purposes of proposed § 488.8(i)(2), the term “re-accreditation survey” would mean any subsequent accreditation surveys performed by the AO after the initial survey.
The accreditation cycle for most Medicare-certified providers and suppliers is 36 months (3 years), which means that the AOs perform an accreditation survey of these providers and suppliers no less than every 36 months. The proposed language at § 488.8(i)(2) would allow AOs to provide fee-based consulting during the first 24 months (2 years) of the accreditation cycle, but not during the 12-month (1-year) period preceding the re-accreditation survey. For example, with this proposal, if the initial survey was completed on June 1, 2025, the provider's or supplier's reaccreditation survey would be due by June 2, 2028. The AO could provide consulting to the provider or supplier from June 2, 2025, to June 2, 2027. The AO would be prohibited from providing AO consulting to the provider or supplier from June 2, 2027, to June 2, 2028. An accredited provider or supplier would retain the ability to use consultants, including other AOs, not affiliated with their AO at any time, including any timeframe prior to or after an accreditation survey for Medicare compliance.
The proposed requirement would provide the accredited provider or supplier ample time, prior to their next accreditation survey, to obtain the education they need to understand the CMS requirements and the AO's accreditation standards and survey process, to implement the AO's accreditation standards and CMS standards in their facility, and to rectify any deficiencies found during the initial survey.
The proposed requirement at § 488.8(i)(2) would address the actual or potential conflicts of interest associated with AO fee-based consulting because it creates a 1-year time period prior to the re-accreditation survey in which the AO is prohibited from providing any type of additional teaching or “coaching” that would help the provider or supplier “pass” or obtain better scores on the upcoming accreditation survey.
We further proposed at § 488.8(i)(3) that the AOs or their associated consulting divisions or companies be prohibited from providing fee-based consulting services to a healthcare provider or supplier in response to a complaint received by the AO regarding that provider or supplier. Our rationale for this requirement is that AOs are required by CMS regulation to investigate and resolve complaints received regarding their accredited providers and suppliers (that is, 42 CFR 488.5(a)(4)(ix); 42 CFR 488.5(a)(12)). This regulatory requirement includes investigating the complaint and working with the accredited provider or supplier to help them resolve any deficient practices identified in the complaint. AOs charge significant fees for their consulting services. AOs should not profit by providing consulting to a provider and supplier in response to a complaint that they are regulatorily required to investigate and resolve. This proposed regulation would prevent this from occurring.
We proposed at § 488.8(i)(4)(i) to (iv) that the restrictions upon AO fee-based consulting would not apply to the following situations: (1) AO fee-based consulting services provided during the 24-month period after the date the initial or re-accreditation survey is performed (proposed § 488.8(i)(4)(i)); (2) AO fee-based consulting services provided to address complaints received and investigated by the SA regarding an AO's accredited provider or supplier in which one or more condition-level or immediate jeopardy deficiencies are identified, provided that the fee-based consulting must occur after the SA complaint investigation and survey has been completed and must only address those issues identified by the complaint survey (proposed § 488.8(i)(4)(ii)); (3) AO fee-based consulting services provided to healthcare providers or suppliers the AO does not accredit at the time the consulting services are furnished (proposed § 488.8(i)(4)(iii)); and (4) consulting or general education provided by the AO about their accreditation program (proposed § 488.8(i)(4)(iv)).
Proposed § 488.8(i)(4)(ii) would allow AOs to provide AO fee-based consulting services in response to complaints received by the SA regarding an AO's accredited provider or supplier. However, this consulting must be provided by the AO after completion of the SA investigation and complaint survey. We would permit AO consulting services after a complaint is received by the SA, because the SA, not the AO, would perform an investigational survey. Therefore, the affected provider or supplier should be permitted to seek consulting from its AO, in accordance with the restrictions stated, to address the issues identified in the SA complaint and complaint survey, if appropriate.
It is important to note that AO consulting should only be provided when serious deficiencies have been identified in the SA's complaint investigation report. By serious deficiencies, we mean deficiencies that would be considered condition-level by the SA and the AO. However, the AO should first work directly with the provider or supplier, as part of their accreditation services package, to resolve the issues identified in the SA's complaint investigation report and only provide separate AO consulting services if these issues cannot be resolved successfully through other methods. It has always been the duty of the AOs to address and resolve complaints received regarding its accredited providers and suppliers, whether said complaint is received by the AO or the SA. An AO receives a significant fee for the accreditation services provided. We believe that the investigation and resolution of complaints falls squarely under these paid accreditation services. We do not believe it appropriate for AOs to offer fee-based consulting/educational services in response to each and every complaint received regarding one of its accredited providers or suppliers. In other words, an AO should not realize additional profit from its paying customers, when it has already been paid to perform the task at hand.
Proposed § 488.8(i)(4)(ii) would prohibit AO fee-based consulting until after completion of the SA's
( printed page 36393)
investigation and complaint survey. By “completion of the SA's investigation,” we mean the date upon which the SA has completed all work required to investigate the complaint and has issued its findings. This restriction is necessary because if the affected provider or supplier were to receive consulting from the AO prior to the completion of the SA's investigation and complaint survey, the affected provider or supplier potentially could alter processes, operations, or documentation, all of which could compromise the SA's investigation of the complaint. In such a scenario, the investigation and complaint survey report would not be an accurate reflection of the issues identified in the complaint. While it may seem counter-productive for the affected provider or supplier to obtain AO consulting after completion of the SA's investigation and complaint survey, we believe that it would be helpful to the affected provider or supplier. After completion of the SA's complaint survey and investigation, the affected provider or supplier would receive a complaint investigation report, which would allow the AO to tailor the consulting services or other educational activities to address any deficiencies identified in said report. Also, through AO consulting services, the AO could work with the affected provider or supplier at their own pace to implement long-lasting and sustainable changes that address the deficiencies identified, as opposed to the implementation of quick temporary solutions or corrective action prior to completion of the complaint investigation. A quick temporary solution would be one that the provider or supplier implements on a short-term basis, typically only during the time that the surveyors are present. By contrast, a long-lasting and sustainable solution would be one in which the provider or supplier implemented the solution, oriented the staff to its requirements, regularly monitored for compliance with the requirements, and corrected non-compliance on a continual basis.
Proposed § 488.8(i)(4)(iii) would further allow AOs to provide fee-based consulting services to healthcare providers or suppliers the AO did not accredit at the time the consulting services were furnished. If the AO had not provided accreditation services to a provider or supplier at the time consulting services were provided, the AO would not have a preexisting financial relationship with that provider or supplier. Thus, no conflict of interest would exist.
Proposed § 488.8(i)(5) would require AOs to report information about the fee-based consulting provided to the providers and suppliers they accredit to CMS. Proposed § 488.8(i)(6) would provide for actions against AOs that provide fee-based consulting in violation of the restrictions set forth in proposed § 488.8(i)(1) to § 488.8(i)(3). We proposed at § 488.8(i)(6)(i) that if an AO was found to be in violation of the restrictions set forth in paragraphs §§ 488.8(i)(1), (2) and (3), CMS could initiate actions against the AO. These remedies would be set forth in proposed § 488.8(i)(6)(i) and (ii) and would include placing the AO on a program review, and involuntary termination of the CMS-approved AO's accreditation program(s).
Whether or not we would impose the remedies proposed in §§ 488.8(i)(6)(i) and (ii) would depend on the severity of the violation and the facts and circumstances surrounding the violation. Such facts might include the number of providers and suppliers that contracted for prohibited AO consulting services, and the number of times the AO violated the restrictions of § 488.8(i). We proposed at § 488.8(i)(7) that the requirements at § 488.8(i) would become applicable 1 year from the effective date of the final rule with comment period to allow for an appropriate time of transition. We believe that this would provide ample time for the AOs to prepare for and implement the proposed requirements at § 488.8(i).
We note that other CMS programs have established similar conflict-of-interest and independence provisions for organizations that have a public trust role in assessing the quality of services provided. For example, in the Medicaid program, CMS has established regulatory standards with respect to the independent judgment of any External Quality Review Organization that reviews the quality of the Medicaid managed care organization for the State (42 CFR 438.354). These regulations establish, among other requirements, that an External Quality Review Organization may not review any managed care entity for which that organization has also conducted a private accreditation review within the previous 3 years.
Our proposal to place restrictions on the provision of specific consulting services by AOs to their currently-accredited providers and suppliers is authorized by section 1865(a)(2) of the Act, which gives CMS the broad power of oversight of the activities of AOs. The provision of specific AO consulting services is one of the factors in section 1865(a)(2) of the Act that should be considered in determining whether a national accreditation body demonstrates that all of the applicable conditions or requirements of this title are met or exceeded and that its determination is free from any conflict of interest such as that discussed in this rule.
The comments and our responses are set forth below.
Comment:
We received several comments of general support for the proposal to place restrictions on consulting services provided by AOs to the Medicare-certified providers and suppliers they accredit. One commenter expressed appreciation for CMS' recognition that AOs provide helpful direction and support via fee-based consulting to facilities seeking accreditation. Another commenter voiced their appreciation for CMS' efforts to provide policies that aim to ensure actual or perceived conflicts of interest do not arise when AOs offer accreditation and consulting services. One commenter agreed that there is fee-based consulting abuse by specific AOs while another commenter stated that they agreed with the overall intent of the proposed provisions to curb such behavior.
Response:
We thank the commenters for their input and support of the proposals.
Comment:
One commenter stated that there was no proposal to add a definition of the term “consulting services” to the CMS regulations at § 488.1. This commenter further suggested that CMS define and qualify “consulting services” as it relates to deemed accreditation. Another commenter stated that they define “consulting” as providing professional or expert advice for the purpose of finding a solution to a problem. This commenter suggested that CMS use this definition for “fee-based consulting”. Several commenters requested that CMS add a definition of “consulting services” in § 488.1 or elsewhere in the final rule with comment period.
One commenter encouraged CMS to clearly define what was meant by “consulting services”, and they proffered the following definition for consideration:
“Consulting is defined as the provision of any of the following:
“• On-site or remote assessments of an accredited organization's compliance to AO' standards and/or the Medicare Conditions of Participation—commonly known as mock surveys.
“• Providing direct or indirect assistance in developing and/or implementing corrective actions plans for deficiencies identified as a result of any type of survey activity. This does not include a review of submitted
( printed page 36394)
corrective action plans to an AO as a result of deficiencies identified during survey activities.
“• Providing direct or indirect assistance to an accredited organization in specific preparation activities for an AO and/or Medicare survey. This does not include providing standards interpretation or general information and resources about the survey process.”
The commenter stated that they believe that the above definition addresses the salient concerns promulgated in the proposed rule but is not so overly expansive that it prohibits an AO from working effectively with its accredited providers and suppliers.
Another commenter stated that the Merriam-Webster dictionary defines
“consulting”
as
“providing professional or expert advice.”
This commenter further states that the Merriam-Webster dictionary defines
“education”
as
“the action or process of educating or of being educated; to provide with information.”
This commenter stated the opinion that, based on these definitions, they do not view the provision of general education as a conflict of interest.
Another commenter stated that no definitions were provided to distinguish between consulting, education, or training. The words are used interchangeably throughout the document. There could be a conflict of interest if the AO provides consulting services whereby the AO provides individualized analysis of a particular organization and participates in preparing, guiding, and assisting a specific organization in creating the processes and documentation necessary to pass accreditation. There is no conflict if the AO makes available tools and education to assist organizations to come into and remain in compliance with accreditation standards, and Federal and State regulations. AOs should be permitted to provide tools and education through workshops, webinars, gap analysis, policies, and forms that are designed for a general audience.
Response:
While we did not propose a definition, we did include a description of
“fee-based consulting services”
in the proposed rule (89 FR 12001). This is the same description of fee-based consulting defined in the “
Medicare Program: Accrediting Organizations Conflict-of-Interest and Consulting Services Request for Information,
that was published on December 20, 2018 (83 FR 65331); hereinafter referred to as “2018 AO Conflict-of-Interest RFI”.
After careful consideration of the many comments received on both the 2018 AO Conflict-of-Interest RFI and the proposed rule regarding fee-based consulting services versus consulting services, we are retaining the qualifying term, “fee-based,” and are adding a definition of consulting services at § 488.1 that would be incorporated into the requirements at §§ 488.8(i) and (j).
Comment:
One commenter was concerned that the definition of fee-based consulting at § 488.5 includes fee-based general education. Another commenter stated that they provide free education to the providers they accredit including a range of fee-based general education certification programs for providers accredited by the AO and those not accredited by the AO.
This commenter further stated that these courses contain high-level content, are taught by the AO staff, and include testing knowledge acquisition and retention at the end of the course. The commenter stated that their intent in offering these courses is to support the CMS mission of ensuring healthcare providers who are certified by Medicare understand the intent of the regulatory text to provide high-quality safe care to beneficiaries and their families. One commenter stated that they conduct fee-based 'training' workshops for individuals about regulatory and quality requirements, sales, and leadership, and faculty may include part-time surveyors. The commenter questioned whether that would be considered a form of fee-based consulting or a conflict of interest. One commenter questioned how CMS would view a part-time surveyor of the AO who provides consulting services during their time when they are not actively on the clock for the AO. One commenter agrees there should be restrictions on fee-based consulting activity of AOs (or associated division/business entities) when it directly conflicts with the business of accreditation. This commenter stated that particular AOs are engaging in fee-based services for the provider and suppliers they accredit through activities such as completing mock surveys to identify an organization's areas of non-compliance, assisting organizations with the plan of correction completion, offering for purchase products such as survey readiness and policy/procedure manuals, and advising services that help an organization pass a survey.
This commenter stated that while these services are couched as advisory or gap analysis services by the AO, they still represent a conflict of interest. One commenter was concerned that the definition of fee-based consulting at § 488.5 includes fee-based general education. One commenter stated that while they would like to offer all their education free of charge, as a nonprofit, this would significantly impact their ability to operate. One commenter stated that they are generally supportive of this proposal but have major concerns regarding the language in the proposed rule specifically, (89 FR 12009), stating that the restrictions on fee-based consulting would not prohibit an AO from providing free education about the Medicare conditions, the AO's accreditation standards and survey process as long as the AO does not raise its accreditation fees or do anything else that would cause the provider or supplier to incur any additional costs for the education provided by the AO's accreditation division or consulting division or consulting company. This commenter stated that they provide a variety of support services (educational webinars, staff training resources, template documents, standards interpretation, etc.) to its accredited organizations free of charge. The services are not targeted to a specific organization or in response to any organization's specific needs. They are simply available to all organizations to use as they wish. There is no requirement for an accredited organization to use these services, nor is the organization's survey affected by such use or non-use. They believe this approach should not be construed as being tied to accreditation fees and thus be considered fee-based consulting services.
This commenter further stated that they provide an annual education conference that is open to both accredited and non-accredited organizations. There is a separate per person fee charged to attendees. The commenter stated that the fee barely covers the cost of the conference and there is no profit made. Their accredited providers and suppliers are not required to attend, nor does attendance (or lack thereof) impact any survey activity or their accreditation status. They state that this is essentially a community-wide education conference. They point out that if this is considered fee-based consulting services, then their accredited facilities would not be able to attend. This commenter strongly urged that the noted language be stricken from the final rule.
One commenter stated that, relative to fee-based consulting and education provided by the AOs, CMS specifies that the proposals would not prohibit the AOs from providing no-cost education, such as general education about the AO's accreditation and survey process and mock surveys. The restrictions on
( printed page 36395)
AO fee-based consulting would also not prohibit AOs from providing education about the Medicare conditions, AO standards, or survey process, to its accredited healthcare providers and suppliers, as long as this education was provided completely free of charge. The commenter observed that the provision would confuse the industry as the distinction between education and consulting was unclear. This commenter stated that providers have shared with them that a primary driver of utilization of an AO is the ability of the facility to seek information and guidance that helps them understand, interpret, and comply with the Medicare conditions and regulatory requirements.
This commenter recommended that AOs be allowed to provide this type of education on a global basis, that is, through workshops sponsored by the AO, workshops where AO staff present, conference presentations, and webinars hosted by the AO or other entities such as national or State associations.
One commenter stated that while they do not presently offer fee-based consulting services, they do offer training services and other supportive services that complement accreditation and quality improvement activities in their accredited providers. This commenter requested that we clarify our definitions of all the types of services subject to this requirement, to ensure that discretionary interpretations do not unfairly impact AOs or restrict their ability to do business. One commenter stated that allowing AOs to provide no-cost education could enhance healthcare providers' understanding of accreditation standards and processes without compromising the impartiality of the AOs. One commenter generally agreed with our views on the necessity of avoiding potential conflicts of interest that may arise from the provision of fee-based consultations by AOs to accredited providers and suppliers. However, they noted that providers benefit from the educational resources provided by AOs.
The commenters stated that should CMS finalize this requirement as proposed, providers would face uncertainty about the timing of accessing otherwise beneficial education from an AO and that CMS itself recognizes that AOs have expert insight that is valuable to providers in meeting their specific compliance needs.
Response:
We are not going to opine on the legality of specific hypothetical examples of education, training, and consulting services provided by commenters at this time. However, general education provided by an AO would not constitute a conflict of interest. Section 488.8(i)(4)(iv) allows AOs to provide general education unless it meets the definition of consulting services we are finalizing in this rule. As we have noted previously, we have also added a definition of “Fee-based consulting services” at § 488.1 that more clearly outlines the type and general timing of the specific consulting services an AO might provide to facilities that it accredits and that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. We believe that this definition will help AOs and providers determine which types of AO consulting services are restricted by this rule and when these restrictions would apply.
Comment:
One commenter stated that two of the three AOs that accredit home health and hospice providers offer intensive educational courses about the AO's standards, conditions of participation and survey process. Individuals successfully completing these intensive workshops are granted a “certification”. The information in these workshops is extremely helpful to individuals in learning about the Medicare conditions of participation as well as the AO standards, interpreting and applying them correctly. The types of individuals completing these workshops are those employed by facilities that are accredited or going through the accreditation process as well as those consulting in these areas or employed by larger consulting firms. CMS should consider the potential for conflicts of interest with the consultants and consulting firms with these certifications.
Response:
We thank the commenter for this information.
Comment:
One commenter noted that some AOs also certify products for meeting the AO's standards and/or verify products for innovation. While the AOs state on their website what certification/verification means, providers and the public may view these products as being endorsed by the AO as meeting the conditions of participation. CMS should consider requiring the AOs to specify that the products are not endorsed as meeting the conditions of participation or in any other way endorsed by CMS.
Response:
This comment is outside the scope of this rule, but we thank this commenter for their suggestion.
Comment:
One commenter requested that CMS clearly define “interest in or relationship with” accredited organizations, to avoid any discretionary concerns among AOs or provider entities.
Response:
We proposed such definitions in the proposed rule (89 FR 12005). We believe that the definition provided in the proposed rule is adequate and are finalizing it in this rule without change.
Comment:
One commenter stated that some AOs in the healthcare sector that offer consulting services to the same entities they accredit perform the roles of both inspecting and accrediting. This commenter believes that this dual role compromises the objectivity and fairness of the accreditation process.
Response:
We are not clear as to what the commenter means here by the term, “inspecting”, especially in relation to the term “accrediting”, but we thank this commenter for their comment.
Comment:
One commenter requested clarification on whether the restrictions on AO fee-based consulting restrictions would apply to Medicare-certified providers and suppliers that seek only AO accreditation without deemed status. This commenter noted that some providers and suppliers obtain non-deeming AO accreditation and use the SA for Medicare certification.
Another commenter requested that additional language be added to specify that fee-based consulting that is related to accreditation services is restricted. This commenter stated that that they offer fee-based growth strategy consulting services. The commenter stated that this program is available to accredited (deemed/non-deemed) and non-accredited provider organizations to assist them in developing an ethical marketing plan to boost admissions and revenue through strategic solutions tailored to their market, referral sources, and needs. The commenter further stated that their fee-based growth strategy consulting services are in no way linked to their accreditation activity and was assessed by the AO and cleared before implementation for conflict-of-interest issues.
Response:
We believe that the provision of marketing and growth strategy and development services to facilities that the AO accredits for deeming purposes would still create a conflict of interest for the AO and would be subject to the requirements of this rule.
However, in our discussion of the proposed restrictions on fee-based consulting, we did not specifically address the scenario in which the AO provides fee-based consulting to a provider or supplier that receives accreditation from an AO for non-deeming purposes and uses the State survey agency for certification. We only considered the scenario in which the AOs provide fee-based consulting to the
( printed page 36396)
providers and suppliers that they accredit for deeming purposes, as discussed in the preamble (89 FR 12006). We believe that in cases where a facility uses the SA for certification and participation in the Medicare program and only uses the AO for non-Medicare accreditation and/or consulting purposes, no conflict of interest would exist and therefore no specific requirements would be needed to address these situations.
Comment:
One commenter recommended that CMS revise the proposed regulatory text at § 488.5, to qualify that only fee-based consulting that is directly linked to accreditation services and impacts survey activity be restricted.
Response:
In the proposed rule, we stated that the restrictions on fee-based consulting did not apply to (1) AO fee-based consulting services provided during the 24-month period after the date the initial or re-accreditation survey is performed (proposed § 488.8(i)(4)(i)); (2) AO fee-based consulting services provided to address complaints received and investigated by the SA regarding an AO's accredited provider or supplier in which one or more condition-level or immediate jeopardy deficiencies were identified, provided that the fee-based consulting occurred after the complaint investigation and survey has been completed and only addressed those issues identified by the complaint survey (proposed § 488.8(i)(4)(ii)); (3) AO fee-based consulting services provided to healthcare providers or suppliers to which the AO does not provide accreditation services (proposed § 488.8(i)(4)(iii)); and (4) no-cost consulting or general education provided by the AO about their accreditation program (proposed § 488.8(i)(4)(iv)).
We further stated that “[w]e believe that it is important that healthcare providers and suppliers receive education that would assist them in compliance, so long as it is not provided on a for fee basis, which would introduce another financial relationship between the AO and the provider or supplier that could cause a conflict of interest.” (89 FR 12009.)
We did not address the situation either in the RFI or proposed rule about fee-based consulting that was related to non-deeming accreditation. However, we believe that in cases where a facility uses the SA for certification and participation in the Medicare program and only uses the AO for accreditation and/or consulting purposes, no conflict of interest would exist (because the facility's Medicare participation would be based on the findings of a SA, with which the AO has no financial relationship) and therefore no specific requirements would be needed to address these situations. We have also added a definition of the specific consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period.
Comment:
One commenter urged CMS to clarify that limitations on the “fee-based consultation services” would apply specifically to individual hospitals with which the AO contracts to provide the consultation services—and not to all hospitals across an entire hospital system, many of which may not contract with the AO for these services.
Response:
We have added a definition of the specific consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. The definition of, and the restrictions on, fee-based consulting services in this final rule with comment period will only apply to those individual hospitals and other facilities that have contracted for AO consulting services and will not apply to all facilities within a hospital or healthcare system.
Furthermore, the restrictions on consulting will only impact those individual providers and suppliers (with individual CMS Certification Numbers (CCNs)) that might contract with the AO's consulting division or company to receive the specific consulting services defined in this final rule with comment period. The AO's consulting services are services that are separate and apart from the AO's accreditation services and a separate fee is usually charged. Use of an AO's consulting services is optional on the part of the provider or supplier accredited by that AO. The restrictions on consulting, as finalized here, will not affect any providers and suppliers that do not contract for an AO's consulting services, regardless of whether they are part of a larger overall system where other providers or suppliers in the system might be contracting with an AO for consulting services. For example, if an AO accredits Hospital A, which is part of a larger system that includes Hospitals B and C, the AO would be prohibited from also providing consulting services to Hospital A under the definition and the restrictions that we are finalizing in this rule. However, this same AO would only be prohibited from providing consulting services to Hospital B or Hospital C if the AO also accredited B or C and only in accordance with the definition and requirements that we are finalizing in this rule. Accreditation of one hospital or facility that is part of a larger system does not disqualify an AO from providing consulting services unless the parameters established by our definition and the requirements in this rule are met for these facilities and the AO involved in both accreditation and consulting.
b. Comments on Restrictions on Providing Fee-Based Consulting in Response to Complaints
Comment:
One commenter stated that AOs should be free to provide consulting expertise to accredited providers who are seeking to correct or remedy a complaint situation that is being investigated by a SA. This commenter further stated that there should be a restriction on consulting only when the AO is addressing a problem with the provider that is considered a “condition” level. The AO should be permitted to provide consulting services to address Standard or Immediate Jeopardy levels of SA complaint investigations.
Response:
While an AO would be prohibited from providing specific consulting services to a provider or supplier it accredits in response to a complaint the AO receives about that provider or supplier, the AO would be permitted to provide AO consulting services in response to complaints received by the SA regarding an AO's accredited provider or supplier. However, this consulting must be provided by the AO
after
completion of the SA investigation and complaint survey.
We proposed to permit AO consulting services after a complaint is received by the SA, because the SA, not the AO, would perform an investigational survey. Therefore, the affected provider or supplier should be permitted to seek consulting from its AO, in accordance with the restrictions stated, to address the issues identified in the SA complaint and complaint survey, if appropriate. However, we believe that an AO's consulting should only be provided in response to an SA complaint when serious deficiencies with the provider/supplier have been identified as part of the SA's complaint investigation report. In the proposed rule, we described “serious deficiencies” as deficiencies that would be considered condition-level by the SA and the AO.
We say this because it has always been the regulatory duty of AOs, as part of the accreditation services they provide, to respond to and investigate any complaints regarding its accredited providers and suppliers, whether said
( printed page 36397)
complaints are received by the AO or the SA.
Therefore, the AO should first work directly with the provider or supplier, as part of their accreditation services package, to resolve the issues identified in the SA's complaint investigation report and only provide the specific AO consulting services defined in this rule if these issues cannot be resolved successfully through other methods.
Comment:
The proposed rule states. . . “In other words, AOs should not realize additional profit from its paying customers, when it has already been paid to perform the task at hand.” All AOs do not price their services to include an unlimited supply of addressing their client complaints. Accreditation clients want a cost-effective solution and that can involve a base pricing structure for the accreditation service only and services to provide a complaint visits or related consulting to assist the provider to resolve a complaint would be billed on an as needed basis.
Response:
As we stated, it has always been the duty of the AOs to respond to and investigate any complaints regarding its accredited providers and suppliers, whether said complaints are received by the AO or the SA. The AOs should perform this task regardless of how much they charged the provider or supplier for accreditation services. In other words, the investigation and resolution of complaints by the AO is an administrative service on the part of the AO that they are required to perform as a condition of approval by CMS as an AO exercising “deeming authority”.
Comment:
One commenter opined that the use of third-party fee-based consultants would avoid perceived conflicts because they do not make compliance determinations about the provider or supplier. Another commenter stated that, as a matter of public policy, fee-based consulting services should largely be run by third parties, not the AOs themselves.
Response:
We thank the commenters for their comments.
Comment:
One commenter noted that in the proposed rule CMS acknowledged that independent fee-based consulting is a valuable resource that can help providers and suppliers improve the quality and safety of the care they provide. They stated that, however, CMS has proposed to put restrictions on the use of AO fee-based consulting by healthcare providers and suppliers without adequate justification, and that it appears the agency is contradicting itself as the agency expressly acknowledges the value of such services.
Response:
In the proposed rule, we recognized the value of fee-based consulting by independent, third-party consultants who provide insight or expertise to assist facilities in achieving or maintaining compliance with AO and/or Medicare's health and safety standards (89 FR 12006). The consulting services provided by AOs to the providers and suppliers it accredits can be beneficial in assisting the providers and suppliers in achieving or maintaining compliance with the AO's and Medicare's health and safety standards. However, because of the conflict of interest associated with specific consulting services, we proposed restrictions on specific AO consulting services and at certain points in the process. We believe these restrictions are minimal in comparison to a total ban on consulting. The restrictions finalized in this rule would also not prevent an AO from providing any consulting or general education to its providers and suppliers about their accreditation program.
Comment:
One commenter noted that CMS states the prohibition on an AO providing fee-based consulting prior to an initial survey is to provide a “more accurate assessment of the provider's or supplier's baseline operating conditions and deficiencies on the initial survey.” Yet, CMS would allow healthcare providers or suppliers to use a third-party consultant prior to the AO's initial survey. Another commenter stated that continuing to allow third-party consultants both acknowledges the role of education pertaining to compliance with Medicare requirements and contradicts the agency's belief that consulting prior to an initial survey by AOs also conducting the initial survey—even when paired with a robust firewall that fully mitigates any COI concerns—would not result in an accurate assessment of baseline operating conditions.
Response:
This commenter is correct that our restrictions on consulting will allow the providers and suppliers accredited by an AO to seek fee-based consulting from third-party consultants at any time, without restrictions. The proposals we have made for restrictions on consulting are to address and mitigate, to the extent possible, the conflicts of interest associated with AO consulting. We had no need to propose any restrictions on the consulting provided by third-party consultants because no conflict of interest is associated with the provision of consulting by these parties. Even if we were inclined to prohibit or restrict the provision of fee-based consulting by third-party consultants, we do not have the statutory or regulatory authority to do so.
Comment:
One commenter stated that in the proposed rule, CMS suggested that providers found to be non-compliant by their AO might assume that the most direct path to compliance would be to hire the AO for its consulting services; such assumption would provide AO consulting services with an unfair advantage over other, third-party consulting services. These fee-based consulting services provide the extra benefit of bringing actual survey experience. Therefore, there is no rational justification for artificially distorting the market to dissuade healthcare provider and suppliers from receiving such benefit, which would ultimately benefit patients.
Response:
We have added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. In this final rule with comment period, we have not prohibited AO fee-based consulting in its entirety but have merely placed some limited restrictions on this service to help mitigate the conflicts of interest associated with specific AO consulting services and the timing of those services. The purported benefit that the commenter notes is exactly related to the conflict of interest for AOs that we are addressing in this rule. Facilities may still use the services of third-party consultants as well as the consulting services provided by an AO that does not accredit the facility.
Comment:
One commenter stated that while it is understandable that there could be a public perception of conflicts of interest when a subsidiary of an AO consults with the hospitals it accredits, hospitals report that the “firewall” between their accrediting AO and its consultative subsidiary is sufficient to prevent any such conflict of interest.
Response:
We agree with this commenter that there is a potential conflict of interest associated with the provision of consulting to the providers and suppliers the AO accredits. However, we disagree with this commenter that a “firewall” would eliminate this conflict of interest entirely and are therefore finalizing additional restrictions and parameters for consulting services provided by AOs to the facilities they accredit for deeming purposes.
Comment:
One commenter stated that they have policies in place to address conflicts of interest during surveys and accreditation decisions. This commenter stated that as long as conflict-of-interest requirements and related processes are followed, actual conflicts of interest that
( printed page 36398)
could undermine the integrity of a CMS-approved accreditation program can be mitigated.
Response:
We thank this commenter for sharing this information.
Comment:
One commenter stated that it has robust, government-evaluated firewall policies which prohibit the sharing of information related to accreditation surveys and decisions between its accreditation and fee-based consulting divisions. This commenter further stated that its firewall policies help to ensure that accreditation surveys and decisions are free from real or perceived conflicts of interest. Another commenter stated that the U.S. Government Accountability Office (GAO) reviewed its firewall policies and found no concerns with the policies; GAO recommended that that AO continue with its current process to assess and monitor the firewall policies.
Response:
We appreciate the information shared by the commenter. However, as stated, we do not believe that firewall policies alone are sufficient to eliminate conflicts of interest that CMS is addressing in this rule.
Comment:
One commenter that provides fee-based consulting stated that they have shown that appropriate policies, such as strong COI policies and a robust firewall policy, have maintained the integrity of their accreditation survey process and decisions while also ensuring their accredited facilities have access to quality improvement tools.
Response:
We thank the commenter for this information.
Comment:
One commenter stated that it is important for CMS, the public, and patients to have faith in the accrediting decisions of AOs and in the health and safety of the health systems where they seek care. However, AOs should be able to continue providing these services if they are able to demonstrate that they maintain robust firewalls between the consulting and accrediting units of the organization and report on these consulting relationships.
Response:
We agree with this commenter that it is important that the public and patients have faith in the accrediting decisions of AOs and in the health and safety of the health systems where they seek care. Our proposal for restrictions on fee-based consulting did not prohibit providers and suppliers that are accredited by AOs that provide fee-based consulting from obtaining these services. We have also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. Therefore, the requirements of this final rule with comment period will only restrict the provision of specific types of AO consulting services to specific time periods during the accreditation period.
Comment:
One commenter opined that fee-based consulting services promote understanding of accreditation requirements by providers and suppliers and help them attain accreditation. However, they agree that a better separation between those fee-based consulting services and the accrediting/surveying services needs to exist to ensure conflicts of interest do not result in inappropriate accreditation.
Response:
We thank this commenter for submitting their comment. We agree that it is necessary for the AOs that provide consulting services to have and to strictly enforce robust firewall policies and procedures to ensure that the AO's accreditation and consulting divisions remain completely separated. This is necessary to maintain the integrity of the accreditation process.
Comment:
One commenter stated that CMS stated that a real or perceived conflict of interest arises when an AO provides fee-based consulting services to help a provider or supplier meet Medicare requirements while also charging the provider for conducting a deeming survey to assess compliance. This commenter also stated that CMS incorrectly assumes there are concerns with the integrity of AO compliance determinations when an AO that provides Medicare deeming surveys also has a separate and distinct arm that provides fee-based consulting services.
This commenter stated that CMS did not consider the fact that the AO has robust firewall policies between its fee-based consulting and accreditation divisions. The firewall policies ensure that there is no exchange of accreditation survey and decision information between these two entities.
Response:
We did consider AO firewalls between their consulting and accreditation divisions and have determined that firewalls alone are insufficient to prevent conflicts of interest. We continue to believe that the additional conflict-of interest requirements in this rule, including those specific to firewall policies and procedures between the survey and consulting arms of an AO, are still needed. Therefore, we have also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period so that we can further clarify and strengthen the firewall requirements that are an integral part of what AOs must do to prevent and mitigate conflicts of interest in this area. In this final rule with comment period, we are therefore limiting the restrictions on AO consulting services that were previously proposed and more clearly specifying what those restrictions are.
Comment:
One commenter stated that, although CMS notes that providers or suppliers could still access AO fee-based consulting during the first 24 months of the 36-month reaccreditation cycle after the initial survey, providers and suppliers should not be cut off from all available resources and tools prior to accreditation or reaccreditation. This commenter further stated that the opinion that CMS' intention to restrict consulting prior to an initial survey to assess a baseline operating condition—even where there is no basis for any conflict-of-interest concern on account of a robust firewall—runs counter to the intent of the quality improvement process, which aims not to assess a facility at its lowest performance but to assess performance and to provide tools and resources to implement and sustain improvement initiatives.
Response:
We have determined that firewalls alone are insufficient to prevent conflicts of interest and have therefore also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. In this final rule with comment period, we are therefore clarifying the restrictions on AO consulting services that were previously proposed.
Comment:
One commenter stated that, due to the firewall, surveyors have no idea what issues were addressed by consultants, so there is no way in which it can bias the survey. The commenter further state that, ironically, one could even state that it would be an improvement of process if the surveyors were aware of prior deficiencies to ensure that they were adequately and durably addressed.
Response:
As we have previously stated, we have determined and firmly believe that firewalls alone are not sufficient to prevent conflicts of interest. The conflict of interest may not affect the details of a survey but manifest in the accreditation decision itself. We have therefore also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. In this final rule with comment period, we are therefore clarifying the restrictions on AO consulting services that were previously proposed.
Comment:
Several commenters stated that they are in favor of fee-based consulting services provided by AOs to
( printed page 36399)
strengthen oversight and prevent conflict of interest. One commenter opined that, due to the complexity of the Medicare CoPs and CfCs, AOs are in a unique position to provide this education and technical assistance, and that hospitals rely on these services not only to prepare for surveys, but to identify and implement opportunities for quality improvement. Another commenter opined that hospitals must expend tremendous resources to ensure compliance with complex accreditation requirements. They benefit from the expertise of consultative services in providing education, training, publications, and technical assistance to assist in understanding standards and preparing for surveys.
Response:
We agree that the consulting services provided by AOs can help the providers and suppliers accredited by the AO to understand the Medicare CoPs and CfCs. We would like to point out that providers and suppliers can also obtain these consulting services from third parties. There is no conflict of interest associated with the consulting services provided by third parties because these parties do not also provide the accreditation surveys for these providers and suppliers as the AOs do. In this final rule with comment period, we have not prohibited AO fee-based consulting in its entirety but have merely placed some limited restrictions on this service when it is provided by the provider's AO, to help mitigate the conflicts of interest associated with specific AO consulting services and the timing of those services.
We have also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. In this final rule with comment period, we are therefore limiting the restrictions on AO consulting services that were previously proposed.
c. Comments Supporting Proposed CMS Restrictions on AO Fee-Based Consulting Services
Comment:
Several commenters expressed support for our proposal to place restrictions on the fee-based consulting services provided by AOs to the healthcare providers and suppliers they accredit.
One commenter stated that the proposal to prohibit AOs from providing fee-based consulting services to their accredited facilities addresses legitimate concerns about maintaining the objectivity and credibility of the accreditation process. However, it also acknowledges the value of education and guidance by permitting no-cost educational services and allowing third-party consulting. Another commenter stated that our proposed restrictions of fee-based consulting seek to balance the need for impartial accreditation with the ongoing need for healthcare provider organizations to prepare effectively for such assessments. One commenter stated that there may be appropriate times when fee-for-service consulting is warranted and or/needed and should be allowed and accounted for where there are firewalls to protect the integrity of the process within the guidelines of this rule. Reporting requirements and proposed penalties for non-compliance underscore the seriousness of these concerns while aiming to ensure transparency and accountability. One commenter stated that while the proposed restrictions by CMS aim to safeguard the integrity of the accreditation process and maintain public trust in AOs, they also recognize the importance of education and preparation for healthcare provider organizations.
Response:
We thank the commenters for their support of our proposals for restrictions on fee-based consulting. We have also added a definition of the specific AO consulting services that would be subject to the requirements of §§ 488.8(i) and (j) in this final rule with comment period. In this final rule with comment period, we are therefore limiting the restrictions on AO consulting services that were previously proposed.
Comment:
One commenter stated that they agreed with CMS that without certain restrictions (such as demonstrable management separation between the consulting and accrediting divisions and limitations on when the fee-based consulting affiliate could provide consulting services relative to the date of the survey) an AO providing both regulatory oversight (through Medicare deeming surveys) as well as consultation on passing those surveys could call into question the integrity of the accreditation process.
This commenter stated that the proposed measures will ensure accountability of AOs and their fee-based consulting services to comply with CMS rules related to conflicts of interest.
One commenter strongly encouraged CMS to ensure that AOs have zero conflicts of interest by identifying and halting any survey practices and outcomes that could generate downstream revenue to an AO from IPFs and other providers that received negative audit findings. This commenter further stated that establishing and maintaining this critical check and balance should be a top priority for CMS. This commenter further stated that this practice should include prohibiting fee-based consulting services that AOs provide to IPFs and other providers following an accreditation determination.
Response:
We thank the commenters for their support of our AO fee-based consulting proposals. In this final rule with comment period, we have not prohibited AO fee-based consulting in its entirety but have merely placed some limited restrictions on this service to help mitigate the conflicts of interest associated with specific AO consulting services and the timing of those services.
Comment:
One commenter who does not provide fee-based consulting services stated that “[h]undreds of our clients each year successfully achieve accreditation without any fee-based consulting services from our organization. While we appreciate that education is an important part of the accreditation process, fee-based consulting services are not”.
Response:
We thank this commenter for their comment. We believe that education is an important part of the accreditation process.
Comment:
One commenter expressed support for the proposals related to fee-based consulting services, including the proposed restrictions on the provision of fee-based consulting services provided by AOs to healthcare providers and suppliers they accredit prior to the initial survey, and within 12 months prior to the next scheduled reaccreditation survey of a provider or supplier.
Response:
We thank this commenter for their support of the proposals related to fee-based consulting.
Comment:
One commenter stated that the proposed restrictions on fee-based consulting should be “seen as a regulatory floor by CMS, not the end of all potential areas for regulatory development moving forward.”
Response:
We thank this commenter for their comment and will take their suggestion under advisement. We will be monitoring the consulting activities of the AOs after the provisions become effective to see what, if any, additional regulation on this activity is needed.
Comment:
One commenter stated that they believe that the proposed restrictions on fee-based consulting could ultimately raise healthcare costs because the fees associated with purchasing fee-based consulting would be passed on to the consumer. This commenter further stated that they have been told by their clients who have worked with other AOs that those AOs
( printed page 36400)
increase, and sometimes double, accreditation fees to fund the consulting hours necessary to successfully manage relationships with other AOs.
Response:
We thank this commenter for their comment, but we do not believe the restrictions in this rule on fee-based consulting would increase healthcare costs since the requirements do not completely prohibit AOs from providing fee-based consulting services. The requirements in this rule also do not mandate that accredited facilities must purchase consulting services from AOs or third-party consultants. The use of fee-based consulting services in preparation for either an SA or an AO survey is a choice made by each facility.
Comment:
One commenter stated that the need to purchase consulting services in the accreditation space essentially creates a “haves and have nots” scenario among accreditation clients, in which smaller entities would not be able to afford the fee-based consulting services offered by the AO. The commenter also stated that AOs that market and provide fee-based consulting services for the facilities they accredit prior to an accreditation survey for deeming purposes are potentially implying that the purchase of such services would guarantee the facility's accreditation and deemed status. The commenter states that this puts smaller facilities with potentially limited budgets when compared to larger facilities, and especially those in medically underserved communities, into a difficult situation, one which might ultimately exacerbate issues of patient access to care in these communities.
Response:
We thank this commenter for their comment. We agree that there may be smaller providers and suppliers that are not able to afford the consulting services offered by some AOs. However, we have seen no evidence that would suggest that larger providers that use fee-based consulting services consistently perform better on surveys than smaller facilities that do not use consulting services.
Comment:
One commenter supported our proposal to prohibit AOs from providing fee-based consulting services prior to an initial accreditation survey within 12 months prior to reaccreditation surveys, and in response to a complaint received by the AO regarding the provider or supplier. This commenter further stated that these proposed restrictions on fee-based consulting are reasonable.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter stated that the proposed provisions related to fee-based consulting would allow CMS to proactively ensure that conflicts of interest would not arise by increasing transparency.
Response:
We thank this commenter for this comment.
Comment:
One commenter agreed that there should be restrictions on the fee-based consulting activities of AOs (or associated division/business entities) when they directly conflict with the business of accreditation. This commenter stated that particular AOs provide fee-based services for provider organizations that they accredit. Examples include completing mock surveys to identify an organization's areas of non-compliance, assisting organizations with the plan of correction completion, offering for purchase products such as survey readiness and policy/procedure manuals, and advising services that help an organization pass a survey. These services are couched as advisory or gap analysis services, but they represent conflicts of interest.
Response:
We thank this commenter for their comments.
Comment:
One commenter supported our proposals to place restrictions on the fee-based consulting services provided by AOs to the healthcare providers and suppliers they accredit; prohibit an accrediting organization or its associated fee-based consulting division or company from providing fee-based consulting services to any healthcare provider or supplier prior to an initial accreditation survey; prohibit AOs from providing fee-based consulting services to healthcare providers and suppliers they accredit within 12 months prior to the next scheduled re-accreditation survey of that provider or supplier; and prohibit AOs from providing fee-based consulting services to a healthcare provider or supplier in response to a complaint received by the AO regarding that provider or supplier.
Response:
We thank this commenter for their support for this proposal. We note that in this final rule with comment period we have not prohibited AO fee-based consulting in its entirety but have merely placed some limited restrictions on this service to help mitigate the conflicts of interest associated with specific AO consulting services and the timing of those services.
Comment:
One commenter supported our proposed restrictions on fee-based consulting services provided by the AOs to the providers and suppliers they accredit for the following reasons:
Limiting fee-based consulting services encourages AOs to prioritize their primary role of objective accreditation.
By restricting fee-based consulting services, accrediting bodies can reinforce the principle that accreditation should be a fair and objective evaluation of quality standards, fostering a culture of excellence and continuous advancement in healthcare provision.
This approach promotes a clearer separation of duties and diminishes the likelihood of financial factors influencing accreditation decisions.
Paid consulting undermines the significance and integrity of accreditation, potentially leading to a focus on identifying errors to generate consultation work rather than supporting quality improvement in a collaborative, collegial environment.
When all interested parties are committed to serving the public, the outcomes will be more robust.
Response:
We thank this commenter for their support of this proposal.
d. Restrictions on Fee-Based Consulting and Accreditation Fees
Comment:
Creating educational materials involves costs at every stage, from research and development to production and distribution. These expenses are necessary to ensure quality and effectiveness in providing valuable learning resources. Without generating revenue to cover these costs, sustaining the production of educational materials would be challenging. A successful business model must factor in these overhead costs and set pricing strategies accordingly. Charging for educational products is essential to maintain sustainability and invest in continuous improvement.
Response:
We understand that the AOs would have some expense associated with the development of educational materials. However, once developed, we believe that the AOs would be able to use these materials over and over without further expense. Also, the AO generates revenue from the fees it collects for the accreditation services provided. Educational materials related to the AOs accreditation standards and survey process should properly be part of the accreditation program; any cost for the development for same would be paid from the accreditation fees collected.
In addition, there are currently nine AOs that accredit Medicare providers and suppliers. Only four of these AOs provide fee-based consulting. The other five AOs provide the required education and materials to the providers and suppliers they accredit free of charge. It is our understanding that the four AOs that charge for education and materials
( printed page 36401)
do so for profit. While we do not object to this arrangement, we note that it does not appear to be necessary to maintain an AO as a going concern.
Comment:
One commenter alleged that, in addition to dictating what services an AO can provide, the proposed rule seeks to establish for what services an AO could receive payment. AOs can provide education about the Medicare conditions, AO standards, or survey process, to its accredited healthcare providers and suppliers, as long as this education is provided completely free of charge.
Response:
While this commenter's allegation is rather general in nature, we believe it refers to fee-based consulting. We respectfully disagree with this commenter, for several reasons. First, we note that they have misconstrued our proposed exception to the restrictions on fee-based consulting as an attempt by CMS to dictate what services an AO can provide and establish services for which an AO can receive payment. In the proposed rule, we generally defined fee-based consulting as any type of education for which the AO charges a fee. We stated that the restrictions on fee-based consulting would not apply to any type of education for which the AO does not provide a fee or provides at no change to the providers and suppliers it accredits. We have not dictated what type of content the AO can or cannot provide with its fee-based education or education that is provided for free. We have only proposed to place restrictions on the provision of fee-based consulting in certain circumstances.
Further, while CMS has proposed to place restrictions on fee-based consulting, we have not restricted the AOs ability to charge for the fee-based consulting that is provided within those restrictions. In the proposed rule we stated that we would expect the AOs not to raise their accreditation fees to recoup any lost profits caused by our proposed restrictions on AO fee-based consulting. To do so would be to penalize the providers and suppliers that do not contract with the AO for fee-based consulting. Also, if an AO were to raise its accreditation fees to recoup lost profits from the restrictions on fee-based consulting, this action would demonstrate to us that profit is the main motivation for the provision of its fee-based consulting services to its accredited providers and suppliers. Please see the previous discussion of the conflict-of-interest requirements at section IV.D. of this final rule with comment period for our arguments as to why these requirements are needed to ensure that profit is not the main motivation for the services that an AO might provide to its accredited facilities.
Comment:
The proposed rule concludes that the AO would not be allowed to raise the price of their accreditation services because of the provision of this education or do anything else that would cause the provider or supplier to incur any additional costs for the education provided by the AO, its consulting division or separate consulting company to the providers or suppliers it has contracted with to provide accreditation services. The impact of this cannot be overstated. Not only is CMS attempting to shape the services offered and the way they are delivered, but it is also dictating the pricing structure. This level of control impinges on operational autonomy, hindering the capacity of the AO to thrive in a competitive market and manage a not-for-profit with a viable financial margin. Navigating these stringent guidelines places significant strain on resources, diverting the focus from the AO's core mission and impeding long-term sustainability.
Response:
We define fee-based consulting generally as any type of education for which the AO charges a fee. We stated that the restrictions on fee-based consulting would not apply to any type of education for which the AO does not provide a fee or provides at no charge to the providers and suppliers it accredits.
While CMS has proposed to place restrictions on fee-based consulting, our proposal would not restrict the AOs ability to charge for the fee-based consulting that is provided within those restrictions.
In the proposed rule we stated that we would expect the AOs not to raise their accreditation fees to recoup lost profits caused by our restrictions on AO fee-based consulting. To do so would be to penalize the providers and suppliers that do not contract with the AO for fee-based consulting. Also, if an AO were to raise its accreditation fees to recoup lot profits from the restrictions on fee-based consulting, this action would demonstrate to us that profit is the main motivation for the provision of its fee-based consulting services.
Comment:
Creating educational materials involves costs at every stage, from research and development to production and distribution. These expenses are necessary to ensure quality and effectiveness in providing valuable learning resources. Without generating revenue to cover these costs, sustaining the production of educational materials would be challenging. A successful business model must factor in these overhead costs and set pricing strategies accordingly. Charging for educational products is essential to maintain sustainability and invest in continuous improvement.
Response:
We understand that the AOs would have some expense associated with the development of educational materials. However, once developed, we believe the AOs would be able to use these materials over and over without further expense.
Also, the AO generates revenue from the fees it collects for the accreditation services provided. Educational materials related to the AOs accreditation standards and survey process should properly be part of the accreditation program and we believe any cost for the development for same should come from the accreditation fees collected.
In addition, there are currently nine AOs that accredit Medicare providers and suppliers. Only four of these AOs provide fee-based consulting. The other five AOs provide the required education and materials to the providers and suppliers they accredit free of charge. It is our understanding that the four AOs that charge for this education and materials do so for profit.
Comment:
One commenter stated that healthcare providers and suppliers should not be cut off from all available resources and tools prior to accreditation or reaccreditation. This commenter further was concerned that if there is a harmful situation, such as poor infection control practices, and deficiencies in fire safety, appropriate review of physician conduct, or other serious deficiencies, then letting those deficiencies persist until an inspection only perpetuates the risk for harm of one or more patients.
Response:
We respectfully disagree with the premise of this comment. The AO not being allowed to provide fee-based consulting to a provider or supplier prior to a survey should not affect how such deficiencies are handled by the facility prior to that survey. Medicare-certified providers and suppliers must comply with all Medicare patient health and safety requirements as a condition for participation in the Medicare program, regardless of whether they are surveyed for compliance by an SA or an AO and regardless of when the next survey may occur. All participating providers and suppliers must take immediate action to address deficiencies that could result in patient harm as soon as they become aware of such deficient practices and harmful situations and should not wait for the next survey. If a facility believes that it needs consulting or educational assistance to fully address such deficiencies, the requirements of this
( printed page 36402)
rule do not prohibit it from using another AO's consulting services or those of a third-party consultant.
Comment:
One commenter stated that our proposed restrictions on AO-fee-based consulting restrict providers from seeking all available tools and resources and has the potential to decrease the quality of care. The commenter states that the fee-based consulting provided by third-party consultants isn't “as good” as that provided by the AOs. This commenter also contends that the use of third-party fee-based consulting has the potential to decrease the quality of patient care.
Response:
We respectfully disagree with this commenter. The only way that we could restrict the access of providers and suppliers accredited by AOs that provide fee-based consulting to available tools offered by the AO would be if we prohibited fee-based consulting altogether. However, we only proposed to place limited restrictions on the fee-based consulting provided by the AOs. As finalized, the provider or supplier will have access to the AOs fee-based consulting services and other included resources, manuals and tools during the first 24-months of each 36-month accreditation period. In addition, the providers and suppliers can seek fee-based consulting from third-party consultants at any time, even prior to the initial accreditation survey.
We disagree with the claims made by the commenters about third-party fee-based consulting. There is little difference between the consulting services provided by the third-party consultant and the AOs. The fee-based consulting provided by the AOs focuses on the AO's accreditation standards, whereas third-party consulting is based on the Medicare standards, since the consultants may not have access to the AO's accreditation standards.
Comment:
One commenter stated that for its fee-based consulting division to comply with the prohibition on fee-based consulting during the 12 months prior to each reaccreditation survey, the AO's consulting division would need continually updated information from the AO's accreditation division on which provider and suppliers were being accredited by the AO and the next expected survey date.
Response:
The commenter is correct.
Comment:
One commenter stated that for AOs to comply with the proposed prohibition on fee-based consulting to a provider in response to a complaint received by the AO regarding that provider, the consulting affiliate would need communication from the AO regarding the complaint and to determine whether what the provider is seeking consulting is related to the complaint. The proposed CMS firewall requirements and The Joint Commission firewall policies strictly prohibit AOs from sharing complaint information with the consulting affiliate. As proposed, these requirements would lead to a less rigorous firewall than currently used by The Joint Commission.
Response:
We respectfully disagree with this commenter for several reasons. First, AOs will be completely prohibited from providing fee-based consulting to a provider or supplier in response to a complaint received by the AO about that provider or supplier. Second, we have proposed such a restriction because, pursuant to our existing regulations, it is the AO's responsibility to respond to and investigate complaints involving its accredited providers and suppliers. To resolve the issues identified in the complaint, it may be necessary for the AO's accreditation division to provide non-fee-based education. We do not believe it is appropriate for the AO to use a complaint filed against one of its accredited providers or suppliers as an opportunity to unjustly profit from providing fee-based consulting. It would also be a violation of the AO's firewall policy to communicate to the AOs fee-based consulting division that a complaint has been received regarding one of the AOs accreditation clients.
Comment:
One commenter stated that CMS failed to provide an explanation of why the AO's fee-based consulting services must only address those issues identified by the complaint survey when the complaint has been received and investigated by the SA regarding an AO's accredited provider or supplier in which one or more condition-level or immediate jeopardy deficiencies have been identified.
This commenter further stated that an AO's fee-based consulting should be permitted to work with healthcare organizations (HCOs) to address all quality and safety issues and not just those identified during an SA complaint survey otherwise quality and safety issues may remain unresolved.
Response:
We respectfully disagree with this commenter. We discussed the rationale for this proposal in the proposed rule (89 FR 12008), where we explained that that AOs are required by CMS regulation to investigate and resolve complaints received regarding their accredited providers and suppliers (that is, 42 CFR 488.5(a)(4)(ix); 42 CFR 488.5(a)(12)). This regulatory requirement includes investigating the complaint and working with the accredited provider or supplier to help them resolve any deficient practices identified in the complaint. AOs charge a significant fee for their fee-based consulting. AOs should not profit by providing fee-based consulting to a provider and supplier in response to a complaint that they are regulatorily required to investigate and resolve. This regulation would prevent this from occurring. We further explained in the proposed rule that AO fee-based consulting should only be provided when serious deficiencies have been identified in the SA's complaint investigation report. By serious deficiencies, we mean deficiencies that would be considered condition-level by the SA and the AO. However, the AO should first work directly with the provider or supplier, as part of their accreditation services package, to resolve the issues identified in the SA's complaint investigation report and only provide AO fee-based consulting if these issues cannot be resolved successfully, through other methods. We would expect to find that if an AO offers fee-based consulting/educational services to the provider or supplier, they do so only after trying all non-cost options available, and that the fee-based consulting/education was reasonably expected to resolve the deficiencies identified in the compliant.
Comment:
One commenter supported our proposed requirement that the AOs that provide fee-based consulting services must have or implement AO fee-based consulting firewall policies and procedures that ensure complete separation between their AOs fee-based consulting and accreditation divisions. However, this commenter stated that two of the AOs that provide fee-based consulting provide home health and hospice fee-based consulting programs that have a unique collaboration and teaching ethos. This commenter stated that these fee-based consulting programs should be enhanced and supported, not restricted. They encouraged CMS not to create barriers to these trainings or restrict AOs ability to provide these educational opportunities to providers. The commenter further stated that these home health and hospice fee-based consulting programs could provide immense value to providers and suppliers by ensuring compliance with CoPs.
Response:
We thank this commenter for their support for our proposed firewall policies and procedures. However, this commenter supported our proposal, so long as it was not related to or did not affect fee-based consulting programs for home health and hospice providers.
Our rule will not completely prohibit AOs from providing fee-based
( printed page 36403)
consulting to the providers and suppliers it accredits. It will only prevent the AOs from providing this service during specific times including prior to initial surveys and during the last 12 months of the 36-month accreditation cycle. The AO would be able to provide fee-based consulting to the providers and suppliers it accredits during the first 24 months of the 36-month accreditation cycle. Providers and suppliers would be able to seek fee-based consulting from a third-party consultant at any time with no restrictions.
Comment:
One commenter stated that the proposed restrictions on AO fee-based consulting, if finalized, would eliminate a key source of provider education and compliance and as a result, stifle consulting relationships. This would undermine the very health and safety goals CMS seeks to advance. Health systems leveraging these relationships would have to identify another AO to use or an external consulting service, which would hinder their ability to maintain continued compliance with health and safety regulations.
Response:
We respectfully disagree with this commenter because providers and suppliers would be permitted to seek fee-based consulting from a third party at any time, without restrictions, so long as that AO does not provide accreditation services to the provider or supplier at the time the consulting services are furnished.
Comment:
One commenter stated that the proposed restrictions on fee-based consulting, if finalized, would be disruptive to existing relationships and processes, particularly in cases where health system staff have had longstanding relationships with their AO's fee-based consulting divisions. The commenter provided an example scenario in which a health system currently receives fee-based consulting services from an AO and is due for a re-accreditation survey in the next 12 months. The health system would essentially have to terminate its consulting relationship with the AO or find another AO to use for accreditation, which could delay its ability to receive accreditation in a timely manner. In the case of termination of the consulting arrangement with the AO, the health system would have to find another suitable consultant that meets the needs of the health system.
Response:
We respectfully disagree with this commenter. We believe that the 12-month restriction requirement in this final rule with comment period addresses the actual or potential conflicts of interest associated with AO fee-based consulting because it creates a 1-year time period prior to the initial or re-accreditation survey in which the AO is prohibited from providing any type of additional teaching or “coaching” that would help the provider or supplier “pass” or obtain better scores on the upcoming accreditation survey.
We also believe that for a provider or supplier to correct deficiencies and make long-lasting cultural changes to the facility, they need to have plenty of time to do so. We further believe that when a provider or supplier waits until the last minute to correct deficiencies and come into compliance with the AO's accreditation standards, the changes made will be hastily made and will not last.
Comment:
One commenter stated that the proposed prohibitions on fee-based consulting are inconsistent with the aims of existing conflict-of-interest policies and proposed requirements. In their comment, this commenter stated that CMS has “prohibited” fee-based consulting, this commenter stated that these “prohibitions” on fee-based consulting are inconsistent with the existing conflict-of-interest policies and proposed requirements. This commenter does not state whether they are referring to their own policies and procedures or those of CMS.
Response:
In the proposed rule, we proposed some limited restrictions on the fee-based consulting provided by AOs. We do not believe that the restrictions as finalized will conflict with existing CMS regulations, guidance, policies and procedures. This is because CMS does not currently have any regulations, guidance, policies or procedures related to fee-based consulting provided by AOs.
To the extent our final rule with comment period conflicts with the AOs existing policies and procedures, our restrictions are being implemented pursuant to the broad oversight authority of AOs granted to CMS by section 1865 of the Act. After the provisions of the final rule with comment period and new regulations for restrictions on AO fee-based consulting become effective, the AO will be required to revise its existing policies and procedures to be consistent with the provisions of the final rule with comment period and new CMS regulations.
Comment:
One commenter stated they believed that there is significant variation in the types of fee-based consulting services provided by AOs, ranging from educational support and guidance on understanding the CoPs to specific, targeted recommendations on how to address potential or actual deficiencies. Therefore, not all types of consulting services would implicate concerns about a potential conflict of interest.
Response:
We respectfully disagree with this commenter. If the fee-based consulting provided by an AO to the providers and suppliers it accredits is in any way related to the AO's accreditation process, the accreditation survey, the AO's accreditation standards and/or the CMS standards, then a conflict of interest would exist. This conflict of interest arises from the contractual and financial relationship between the AO and the provider or supplier. The AO charges a fee for the fee-based consulting that is designed to assist the provider or supplier do better on the accreditation that is also administered by the same AO.
The business connection between the provider and the AO creates a relationship that the AO could have incentive to manipulate. For example, the AO could gain from ignoring the deficiencies of certain providers; these missed deficiencies would call the AOs' neutrality into question. The AO could also have the incentive to downplay deficiencies during the survey of a consulting client to increase the apparent efficacy of its consulting services, or perhaps play up the deficiencies of non-clients to increase the apparent value of the consulting services to these prospective clients.
Comment:
One commenter suggested that CMS can address many of its concerns through better oversight and reporting, as proposed in the rule, such as biannual AO reporting to CMS of fee-based consulting services. This proposal entails the AO providing information on the fee-based consulting services it offers, any providers and suppliers to which the AO provides consulting services, and detailed information on the nature and scope of these consulting services. Providing this data will equip CMS with the necessary tools to monitor conflicts of interest.
Response:
We thank this commenter for their suggestion. We will take it under advisement.
Comment:
One commenter stated the opinion that many of the AO oversight proposals in the proposed rule work at cross purposes with one another, lack context, violate the legislative intent of accreditation oversight, and are inconsistent. This commenter also stated that the proposed restrictions on fee-based consulting, which are aimed at reducing conflicts of interest, will limit the AOs' contact with facilities seeking or renewing deemed status and constrain the nature of communications and services AOs may offer to such
( printed page 36404)
facilities. This commenter also opined that this proposal, if finalized, will prohibit the AOs that provide fee-based consulting from communicating with facilities within a year of their survey.
This commenter further stated that many AO communications are meant to facilitate improvement in facilities, at the precise moment the facilities are most receptive to input and have their attention most focused on compliance. If the healthcare system's collective goal is to improve the care provided to beneficiaries, any information that can help the facility should be welcome. Instead, these limits remove valuable information from facilities, making it harder for facilities to comply and increasing the odds that AOs perform poorly on the proposed scores. The proposed rules would create tension by prohibiting communications that could improve AO scores.
Response:
In this final rule with comment period, we are restricting the AOs that provide fee-based consulting from providing fee-based consulting at the following times:
At any time prior to the initial survey
During the last 12 months of each 36-month accreditation period
In response to a complaint received by the AO about an accredited provider or supplier.
However, our restrictions on fee-based consulting
do not
prevent the AOs from communicating with its accredited provider or supplier during the restricted periods, so long as the communication does not consist of the provision fee-based consulting services. In addition, providers and suppliers are free to seek fee-based consulting from a third-party consultant or another AO that does not provide accreditation to that provider or supplier at the time the consulting services are furnished. The providers and suppliers are free to seek fee-based consulting from third party consultants and other AOs at any time without restrictions.
Comment:
One commenter that does not provide fee-based consulting objects to the specific time boundaries proposed in § 488.8(i) of the proposed rule. This commenter stated that these limitations would adversely and unfairly affect their ability to communicate with their customers in the ordinary course of business. The commenter further stated that their annual survey model would preclude such limitations.
This commenter requested that CMS clarify these terms and date triggers, as accreditation activities are intensely date-driven and discretionary reviews would adversely affect these timelines.
Response:
We are not sure what this commenter means by limitations on communications. We proposed at § 488.8(i) to place limitations on the fee-based consulting provided by the AOs. These limitations on fee-based consulting, as finalized, will prohibit the AOs that provide fee-based consulting from providing these services prior to the initial survey and during the 12 months prior to each reaccreditation survey. This means that the AOs can provide fee-based consulting to their clients that contract for this service during the first 24 months of the 36-month accreditation cycle.
Our restrictions on fee-based consulting, as finalized, will not prevent the AO's accreditation division from communicating with their accreditation clients at any time or interfere with the AOs accreditation activities. In fact, this proposal will not affect those AOs that do not provide fee-based consulting services, or educational events found to be consistent with fee-based consulting at all.
Final Decision:
After consideration of the comments received, we have decided to finalize our proposal to place restrictions on fee-based consulting with a minor change to § 488.8(i)(1) to reference the definition “fee-based consulting services” as finalized at § 488.1. We are also modifying the provision as proposed by removing the sentence, “The provisions at paragraph (i) of this section will become applicable beginning [DATE 1 YEAR FROM THE EFFECTIVE DATE OF THE FINAL].” We are making this modification for this final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date of this final rule with comment period and individual provisions will no longer need to be specified in the regulatory text.
G. Require AOs To Provide CMS With Information About the Fee-Based Consulting They Provide (Proposed § 488.8(i)(5))
We proposed at § 488.8(i)(1), § 488.8(i)(2), and § 488.8(i)(3) to place restrictions on the fee-based consulting services provided by AOs. To enforce our proposals, we proposed at § 488.8(i)(5) to require the AOs that provide fee-based consulting services to submit information to CMS, on a calendar year bi-annual basis, about the fee-based consulting services they provide.
We proposed to add a requirement at § 488.8(i)(5) that would require the AOs that accredit Medicare-certified providers and suppliers to provide CMS with information regarding the fee-based consulting services no later than 15 days after the end of each calendar year bi-annual (6-month) period.
More specifically, this proposal would require these AOs to submit a document which contains the following information to CMS:
Whether the AO or an associated consulting division or company established by the AO provides fee-based consulting services.
The names and CCN numbers of all healthcare providers and suppliers to which the AO or its associated consulting division or company has provided fee-based consulting services during the previous calendar year quarter.
The dates the AO fee-based consulting services were provided to each provider and supplier listed.
Whether the accrediting organization has, at any time in the past provided, or is currently providing accreditation services to each healthcare provider or supplier listed in said document, and if so, the date the accreditation services were provided.
The date of the most recent accreditation survey performed, and the date the next re-accreditation survey is due to be performed for each healthcare provider and supplier listed in said document.
A description of the AO fee-based consulting services provided to each healthcare provider or supplier listed in said document.
We further proposed that the two bi-annual reporting periods would consist of January 1st to June 30th and July 1st to December 31st each year. The submission deadline for the first period would be July 15th each year. The submission deadline for the second period would be January 15th each year. This would ensure that AOs are not providing fee-based consulting services to providers and suppliers prior to an initial survey, within 12 months prior to a re-accreditation survey, or in response to a complaint received regarding an accredited provider or supplier. In addition, this information would also allow CMS to see the number of providers and suppliers to which the AOs are providing fee-based consulting services.
We proposed that these provisions would become applicable 1 year from the effective date of the final rule with comment period to allow for an appropriate time of transition. We believe that this would provide the AOs with ample time to prepare for and implement this requirement.
The comments and our responses to the comments are set forth below.
( printed page 36405)
Comment:
One commenter requested that CMS provide the rationale for requesting biannual detailed information about which provider organizations have or are receiving fee-based consulting services from the AO and what this information would be used for by CMS.
Response:
In the proposed rule, we stated that the biannual submission of the information requirement would ensure that AOs are not providing fee-based consulting services to providers and suppliers prior to an initial survey, within 12 months prior to a re-accreditation survey, or in response to a complaint received regarding an accredited provider or supplier. (89 FR 12010). However, we appreciate the comments regarding the regulatory burden and usefulness to CMS of requiring AOs to submit this information twice a year and have decided not to finalize this part of the proposed requirements in this rule. Please see the further discussion of this in the final decision section.
Comment:
One commenter requested clarification on whether the information requested is for deemed status provider organizations only.
Response:
The final rule with comment period requires that an AO submit the names and CCN numbers of all healthcare providers and suppliers to which the AO or its associated consulting division or company has provided fee-based consulting services during the previous 6-month period to CMS, upon request and during each application review process.
Comment:
One commenter suggested that CMS consider publicly reporting the fee-based consulting information reported in a database similar to the Open Payments program.
Response:
We thank this commenter for their recommendation. We will take it under advisement.
Comment:
One commenter stated the opinion that the requirements at § 488.8(i)(5) pose an excessive administrative burden to the AOs who do not facilitate these types of consultative services. One commenter stated that the requirement to have AOs report bi-annually about fee-based consulting is too frequent and too cost-burdensome and recommends that this be an annual requirement.
Response:
We thank the commenter for their comments regarding the administrative burden of this proposed requirement, but we believe the burden associated with the requirements at § 488.8(i)(5) is justified.
Comment:
Several commenters expressed support for the proposed requirement that AOs provide CMS with information about the fee-based consulting services they provide on a bi-annual basis. One commenter stated that the information to be reported and submission timing for these reports is necessary to ensure that AOs are upholding the integrity of their oversight role in a manner worthy of public trust.
Response:
We thank these commenters for their support of the requirement that AOs provide information to CMS about the fee-based consulting services they provide.
Comment:
One commenter supported a healthcare provider's or supplier's choice to work with an AO to affirm compliance with Medicare CoPs. This commenter further stated that many of its members shared positive stories of how AOs helped them better understand their deficiencies and achieve robust compliance in follow up surveys through the provision of fee-based consulting. This commenter states the belief that the additional cost of fee-based consulting is well worth the extra support to improve quality and compliance to serve beneficiaries.
However, this commenter did acknowledge and agree with CMS' concerns that oversight of these entities has led to program integrity concerns. The commenter provided an example of one accrediting body that was allegedly responsible for accrediting nearly half of the fraudulent hospices accredited in California, Nevada, Arizona, and Texas in 2022. The growth of hospice across these four States raised alarms and initiated a nation-wide program integrity effort.
Response:
We recognize the value of fee-based consulting services. None of our proposed restrictions would prevent providers and suppliers from seeking fee-based consulting from the AO that accredited them during the non-prohibited times. These proposed restrictions on fee-based consulting, if finalized, would not prohibit said providers and suppliers from seeking fee-based consulting from third party consultants at any time.
Comment:
One commenter supported our proposal to require the AOs to report information about the fee-based consulting services provided for the following reasons:
Requiring additional documentation as it relates to fee-based consulting services provided by AOs to accredited facilities helps mitigate conflicts of interest, promotes a fairer and more objective accreditation system, and ultimately contributes to better quality care and patient safety.
Detailed documentation provides a clearer picture of the nature and extent of consulting services offered by AOs to the facilities they accredit. This allows CMS to assess potential conflicts of interest more effectively.
Paid consulting undermines the significance and integrity of accreditation, potentially leading to a focus on identifying errors to generate consultation work rather than supporting quality improvement in a collaborative, collegial environment.
When all interested parties are committed to serving the public, the outcomes will be more robust.
This proposal, if finalized, will ensure that the data collected through the process will be more consistent across all AOs serving CMS.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter expressed strong opposition to the amount of detailed information on an AO's fee-based consulting services which would be required by CMS.
Response:
We note this commenter's opposition to this requirement. As we stated in the proposed rule, we made this proposal to ensure that AOs are not providing fee-based consulting services to providers and suppliers prior to an initial survey, within 12 months prior to a re-accreditation survey, or in response to a complaint received regarding an accredited provider or supplier. In addition, this information would also allow CMS to see the number of providers and suppliers to which the AOs are providing fee-based consulting services.
Comment:
One commenter stated that CMS' proposal is contrary to the AO firewall policies and the agency's proposed minimum requirements for a firewall because the specific details to be reported to CMS would require the AO's accreditation and fee-based consulting divisions to routinely share information regarding when fee-based consulting occurred, the type of consulting that occurred, and when an accreditation survey occurred. This commenter opined that this is exactly the type of sharing that firewall policies are intended to prohibit.
Response:
We proposed to require the AOs to submit information about the fee-based consulting they provide to CMS on a bi-annual basis. More specifically, we proposed to require these AOs to submit a document (as previously described) to CMS.
We believe that the AO's fee-based consulting division should already have the required information about fee-based consulting to be reported to CMS. For example, the AO's fee-based consulting division should already know whether they have provided any
( printed page 36406)
fee-based consulting services during the previous 6-month period, the dates that the AO fee-based consulting services were provided, and a description of the AO fee-based consulting services provided. In addition, the AOs fee-based consulting division would be able to obtain the information about whether the AO has, in the past provided, or is currently providing accreditation services to each healthcare provider or supplier listed in said document, the CCN numbers for the providers and suppliers receiving AO fee-based consulting, the date of the most recent accreditation survey performed, and the date the next re-accreditation survey is due to be performed directly from each provider and supplier that receives AO fee-based consulting.
CMS defines the term “firewall” as the complete and total separation between the AO's accreditation activities and its fee-based consulting services. However, we believe that after a provider or supplier accredited by the AO voluntarily signs up for the AO's fee-based consulting services, it would not violate the AO's fee-based consulting firewall policy for the AO's accreditation division to share the limited information necessary for the AO's fee-based consulting division to complete the biannual report for CMS. We say this for several reasons.
First, we see little harm in the AO's accreditation division of the AO providing some of the limited information that would be necessary for the biannual report, but that cannot be provided by its clients, to the AO's fee-based consulting division. While this may reveal to the AO's accreditation division the identity of some of its accredited providers and suppliers that have signed up for the AO's fee-based consulting services, we believe this would be a rare occurrence. We say this because most of an AO's fee-based consulting clients would be able to provide the information that the AO's fee-based consulting division does not already have.
Second, if our proposal to require the AOs to submit information to CMS about the fee-based consulting they provide is finalized, the AOs will be mandated by the CMS regulations to send the required information to CMS. Therefore, it will be necessary for the AO's fee-based consulting division to obtain the required information from their clients if the AO's fee-based consulting division clients are not able to provide all of the required information for the report.
Comment:
One commenter stated that the proposed Federal reporting requirements for AOs that provide fee-based consulting, if finalized, would create an unfair market advantage for third-party consultants because they would be wary of any AO fee-based consulting because of Federal reporting requirements. This commenter also believes that providers and suppliers would opt for services from a third-party consultant that did not have a Federal reporting requirement, which could significantly limit the work of AO fee-based consulting divisions that have dedicated substantial resources to maximizing patient safety and care.
Response:
We respectfully disagree with this commenter. This commenter alleges that our proposal to require that the AO provide information to CMS about the fee-based consulting it provides to CMS on a biannual basis would somehow create an unfair market advantage for third-party consultants. We do not see why there would be any reason for a provider or supplier accredited by an AO to select a third-party consultant instead of the fee-based consulting services provided by their AO simply because of the reporting requirements. We believe it is likely that providers and suppliers that decide to take part in fee-based consulting would choose the fee-based consulting services provided by their AO as opposed to those provided by a third party. As we stated in the proposed rule, “. . . providers and suppliers often choose AO fee-based consulting specifically for the additional resources and assistance provided. Some AOs publicly advertise the ability of their fee-based consulting to simulate what to expect from the actual AO survey. It is possible that Providers and suppliers found to be non-compliant by their AO may assume that the most direct path to compliance is to hire the AO's fee-based consulting services. Such an assumption would provide AOs with fee-based consulting services with an unfair advantage over other, third-party consulting services”.
Comment:
One commenter stated that while CMS did not intend to do so, the AO fee-based consulting reporting requirements would result in the unintended consequence of completely restricting AOs providing AO fee-based consulting services.
Response:
This commenter is correct in their assumption that CMS did not intend to completely restrict an AO's ability to provide fee-based consulting services to the providers and suppliers it accredits. While this commenter contends that the AO fee-based consulting reporting requirements would result in the unintended consequence of completely restricting AOs providing AO fee-based consulting services, they did not provide any specific rationale for this contention. We respectfully disagree with this commenter's contention. We do not understand how requiring an AO's fee-based consulting division to provide information about the fee-based consulting it provides to CMS would affect the AO's ability to provide fee-based consulting or restrict it completely.
Comment:
One commenter recommends that CMS conduct a baseline assessment of each AO's consulting services and, based on the outcome, require submission of the requested information.
Response:
We thank this commenter for their recommendation. We will take it under advisement.
Comment:
One commenter recommended that CMS develop a streamlined system and processes for submission of the requested information.
Response:
When this reporting requirement begins, CMs will require the AOs to send the requested information via secure email. However, we will look into other, more streamlined ways to collect this information.
Comment:
One commenter suggested that if CMS finalizes the fee-based consulting proposal as proposed, that a grandfather clause be added that would: (1) make any existing contract the AOs already had for the provision of fee-based consulting services exempt from the requirements; and (2) make the requirements applicable only to all new contracts that the AOs enter into for the provision of fee-based consulting services the AOs enter into after the date the requirements become effective. This would allow the AOs to satisfy contractual obligations for fee-based consulting that they entered into prior to the effective date of the requirements.
Many fee-based consulting services contracts are for several years. Also, fee-based consulting contracts frequently include nondisclosure obligations, which must be maintained under the existing fee-based consulting contracts. The proposed effective date for the prohibitions on fee-based consulting 1 year after the rule is finalized would not be enough time to complete the AO consulting division's contractual obligations.
Response:
We thank this commenter for their suggestion. We acknowledge that some AOs may have existing contracts for fee-based services when the requirements of this final rule with comment period become effective 1 year after its publication. However, AOs must still meet all requirements in this rule, including the fee-based consulting
( printed page 36407)
requirements, once the rule becomes effective, even if this requires an AO to revise the terms of any existing contract to comply with these regulations.
Comment:
One commenter stated that the AO would be required to provide documentation regarding its consulting activities and customers to CMS on a biannual basis, which would force the two separate divisions (accreditation and education) to share provider information internally, which CMS has prohibited. In addition, the commenter stated that the biannual report would be seeking unobtainable information, that is, it requires the names and CMS Certification Numbers (CCNs) of all providers that receive fee-based consulting or general education from the accrediting organization. The commenter further stated that many attendees at workshops are individuals interested in understanding what accreditation is about, independent of any established provider or supplier, they may not have CCNs for a facility at the time they attend one of the AO's workshops.
Response:
We respectfully disagree with the premise of the commenter that the names and CCNs of the providers and suppliers to which the AO has provided fee-based consulting services are “unobtainable.” For Medicare certified facilities, this information is made publicly available by CMS and can be easily obtained by the AO using the name of the facility (see
https://data.cms.gov/search). The requirements in this final rule with comment period are clear that the AO must submit the names and CCNs of those facilities to which it has provided fee-based consulting services as defined in this rule at § 488.1. The requirement would not apply to individuals attending AO workshops or otherwise obtaining general education from the AO about its programs; such activities do not meet the definition of “fee-based consulting services” finalized in this rule.
In response to the commenter's reference to our proposed requirement for AOs to submit this information on a biannual basis, we also note that we have withdrawn our proposal to require biannual reporting of the documentation that was proposed at § 488.8(i)(5) so that such information, and firewall policies and procedures only need be submitted upon request by CMS and at the time of application or re-application for approval of their Medicare accreditation programs.
Final Decision:
After consideration of the comments received, we have decided to finalize our proposal at § 488.8(i)(5) to require the AOs collect information about the consulting information they provide with a modification to the proposed regulations text. Based on the comments, we are not finalizing our proposal to require AOs submit these reports to CMS on a biannual basis. We will instead require the AOs to submit the consulting information for CMS to review upon request and for review during each application review process.
We are also modifying the provision as proposed by removing the sentence, “The provisions at paragraph (i) of this section will become applicable beginning [DATE 1 YEAR FROM THE EFFECTIVE DATE OF THE FINAL].” We are making this modification for this final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date of this final rule with comment period and individual provisions will no longer need to be specified in the regulatory text.
H. Actions Against AOs Found To Be Providing AO Fee-Based Consulting Services to the Healthcare Providers or Suppliers They Accredit in Violation of the Restrictions in § 488.5(i)(1) Through § 488.5(i)(3) (Proposed § 488.8(i)(6))
We proposed to implement regulations that place restrictions on the fee-based consulting services AOs provide to the healthcare providers and suppliers that they accredit. To enforce these regulations, we proposed at § 488.8(i)(6) to implement actions for the violation of the restrictions on AO fee-based consulting.
We proposed at § 488.8(i)(6)(i) that if an AO is found to be in violation of the restrictions set forth in paragraphs § 488.8(i)(1), (2) and (3), CMS may penalize the AO. These remedies were set forth in proposed § 488.8(i)(6)(i) and § 488.8(i)(6)(ii) and include placing the AO on a program review, and involuntary termination of the CMS-approved AO's accreditation program(s).
Whether or not we impose the remedies provided in § 488.8(i)(6)(i) and (ii) would depend on the severity of the violation and the facts and circumstances surrounding the violation. Such facts might include the number of providers and suppliers that contracted for prohibited AO fee-based consulting services, the number of times the AO violated the restrictions of § 488.8(i), or other facts.
The purpose of these proposed provisions was to discourage AOs from violating the proposed restrictions on the provision of fee-based consulting to the providers and suppliers they accredit.
We proposed that these provisions would become applicable 1 year from the effective date of the final rule with comment period. We believe that this would provide ample time for the AOs to prepare for the implementation of the requirements of this rule.
The comments and our responses to the comments are set forth below.
Comment:
One commenter stated that they are supportive of the proposal for actions against AOs found to be in violation of the restrictions on fee-based consulting and urge its adoption.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter supported our proposal for actions against AOs that are found to be providing fee-based consulting services to the providers and suppliers it accredits in violation of the restrictions. This commenter supports this proposal for the following reasons:
This proposal is essential for upholding public trust and ensuring the integrity of the accreditation process.
Penalties for violations must be stringent, substantial, and enduring, given the critical nature of maintaining public confidence.
The fundamental concept of fee-based consultancy is incompatible with the mission of accrediting bodies, as it creates a conflict of interest and fosters the perception that accreditation can be bought rather than earned through adherence to quality standards.
Moreover, relying on fee-for-service arrangements diminishes the incentive for continuous improvement within healthcare facilities, as they may simply pay consultants to meet accreditation requirements rather than genuinely striving to enhance their practices.
Accreditation should serve as an ongoing process driving improvement, rather than a one-time hurdle to overcome.
Response:
We thank this commenter for their support of this proposal.
Final Decision:
We are finalizing the requirements here as proposed.
I. Require Accrediting Organizations To Have Written Fee-Based Consulting Firewall Policies and Procedures (§ 488.8(j))
We proposed at § 488.8(j) to require any AO that provides fee-based consulting services or its associated fee-based consulting division or company to have written fee-based consulting “firewall” policies and procedures. We defined the terms “consulting division” and “associated company” in section IX.B.3. of the proposed rule. We defined the term “firewall” as the complete and total separation between the AO's
( printed page 36408)
accreditation activities and its fee-based consulting services.
We proposed that these firewall policies and procedures must, at a minimum, include the following provisions: at paragraph (j)(1)(i) the AO's fee-based consulting services must be provided by a separate division of the AO or separate business entity (that is company or corporation) from the AO; at paragraph (j)(1)(ii) the AO's fee-based consulting division or separate company must maintain separate staff from that of the AO's accreditation division(s) to ensure that the fee-based consulting division staff do not perform AO's accreditation division functions and that the AO's accreditation division staff do not perform fee-based consulting division functions; and at paragraph (j)(1)(iii), the AO's accreditation staff and surveyors would be prohibited from marketing the AO's fee-based consulting services to the AO's accreditation clients.
The purpose of the provisions of proposed § 488.8(j) is to ensure that the AO maintains a complete division between their fee-based consulting program and their accreditation program. In other words, we sought to require an AO prevent any co-mingling of its fee-based consulting activities and staff with its accreditation activities and staff. We believe these requirements are necessary because several commenters to our 2018 AO Conflict-of-Interest RFI voiced concern that, even though some AOs have such firewall policies in place, the firewalls have still been breached. For example, one commenter stated that one AO's accreditation staff aggressively marketed that AO's fee-based consulting services to his healthcare facility. In addition, during a CMS validation pilot joint survey with an AO, a SA surveyor witnessed the AO's surveyors providing detailed education about the survey process to the healthcare facility staff prior to the start of the survey. This is inappropriate because surveys are to be unannounced to prevent the facility from preparing for the survey. At the beginning of a survey, a brief entrance conference is held for the purpose of introducing the survey team, providing the survey agenda to the facility staff, and telling the facility what records the surveyors will be reviewing during the survey. However, providing detailed information about the survey process and what areas the AO is going to focus on during the survey could give the facility an advantage and time to prepare for the survey. In addition, providing such education to a healthcare facility prior to a survey could assist that facility in getting a better survey report.
We do not currently have any regulations that provide oversight of the fee-based consulting services provided by AOs or their separate divisions or companies. Likewise, we do not currently have any regulations that specifically require AOs that provide fee-based consulting services to have written firewall policies or regulations that provide requirements for such policies. Regulations are needed so that CMS may ensure that an AO's fee-based consulting remains separate from an AO's accreditation activities. This division is necessary to reduce the conflict of interest associated with the provision of AO fee-based consulting services.
The comments and our responses to the comments are set forth below.
Comment:
One commenter supported this proposal and urged its adoption.
Response:
We thank this commenter for their support of our proposal to require AOs to have written fee-based consulting firewall policies and procedures.
Comment:
One commenter stated long time support for additional requirements that would formalize AO “firewall” policies between AOs and their fee-based consulting entities.
Response:
We thank this commenter for their support of our proposal to require the AOs to have written fee-based consulting firewall policies and procedures.
Comment:
One commenter supports the proposal to require AOs that have written “firewall” policies & procedures that provide for complete separation (“firewall”) between the AO's accreditation activities and fee-based consulting services.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter opined that “blockading the muddying of the AO accreditation role with the motivations of a fee-based consultancy is necessary to sustain the integrity of the AO regulatory oversight role.”
Response:
We agree with this commenter that allowing an AO to combine their accreditation and fee-based consulting activities “muddies” the integrity of the accreditation process. We further agree that the proposed requirement that AOs have and strictly enforce robust firewall policies and procedures to ensure that the AO's accreditation and fee-based consulting divisions remain completely separate is necessary to maintain the integrity of the accreditation process.
Comment:
One commenter supported the proposed minimum requirements for these written policies and procedures, including the requirement that fee-based consulting services be provided by a separate division or business entity from the AO, as being necessary to enforce compliance with the proposed restrictions on co-mingling of AO staff engaged in fee-based consulting activities with AO staff engaged in accreditation activities.
Response:
We thank this commenter for their support of the proposed minimum requirement for the AO's written fee-based consulting firewall policies and procedures.
Comment:
One commenter stated strong support for the proposal to require AOs that provide fee-based consulting to have written firewall policies and procedures for fee-based consulting. This commenter further opined that ensuring the integrity of the accreditation process is of the utmost importance.
Response:
We thank this commenter for support of our proposal to require the AOs that provide fee-based consulting to have written firewall policies and procedures for fee-based consulting.
Comment:
One commenter supported our proposal to require an AO submit a declaration from each surveyor disclosing any interests or relationships the surveyor may have in or with another survey agency or healthcare facility the AO accredits.
Response:
We thank this commenter for their support of the stated proposal.
Comment:
One commenter stated that AOs currently have robust firewall policies in place that contain provisions such as: (1) the entity providing consulting services is distinct from the entity providing accreditation services; and (2) the staff providing consulting services are separate from the survey and accreditation staff, ensuring that there is no conflict or interaction between the two teams.
This commenter further supported our proposed requirement for AOs to have AO fee-based consulting policies & procedures and minimum requirements for these policies and procedures. This commenter further stated that CMS' proposals on reporting would provide more transparency on these firewall policies.
Response:
We thank this commenter for their support of our proposed minimum requirements for the AO fee-based consulting requirements.
Comment:
One commenter supported our proposal to require the AOs that provide fee-based consulting to have written fee-based consulting firewall policies and procedures, for the following reasons:
( printed page 36409)
Firewall safety options are crucial for ensuring the integrity and impartiality of the accreditation process.
By establishing a clear firewall between fee-based consulting services and accreditation activities, accrediting bodies can mitigate the risk of conflicts of interest and perceptions of bias.
This separation helps maintain public trust by ensuring that accreditation decisions are based solely on the adherence to quality standards, rather than influenced by financial relationships.
Explicit firewall safety options provide a structured framework for AOs to uphold transparency and accountability, ultimately safeguarding the credibility of the accreditation system and the facilities it accredits.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter opined that it would only be possible for fee-based consulting firewalls to prevent conflicts of interest if they were clearly defined and well supported by the AO. Another commenter opined that it was possible for firewalls to address AO conflicts of interest but stressed they would need to be clearly defined and well supported by the AO.
Response:
We thank the commenters for their comments. We agree that using appropriate and robust firewalls can help reduce the conflicts of interest associated with fee-based consulting. That is why we proposed to establish a regulation at 42 CFR 488.8(j) that requires an AO to have written fee-based consulting firewall policies and procedures. We would add that the firewall policies must also provide for complete separation between the AO's accreditation and fee-based consulting divisions and activities, including separate governance, separate staff, and separate resources. Also, the fee-based consulting firewall policies and procedures must be strictly enforced by the AO.
Comment:
One commenter stated that the requirement for consulting services to be provided by separate staff is too onerous particularly for small AOs, but also for AOs that provide very specialized surveys. The commenter recommended that this restriction not be implemented, but rather an informational firewall of consulting services be established. They stated that, in other words, when a surveyor provides a survey, he/she must not be aware of any consulting services which may have been provided to the client by any other surveyor or corporate department of the AO. They also stated that AO staff should be allowed the operational flexibility to co-mingle staff to provide consulting services or AO survey services, provided that there is no knowledge by any accreditation surveyor that consulting services were provided or what the outcome or result of such services were. The AO surveyor could provide an attestation that he/she is not aware of consulting services.
Response:
The separation of an AO's accreditation services and fee-based consulting services is an absolute requirement of an AO fee-based consulting firewall policy. The separation of the two divisions necessarily requires that they each maintain separate staff, governance, policies and procedures, etc.
Even the AOs that provide fee-based consulting acknowledge the need for such separation. They already have AO fee-based consulting firewall policies and procedures that provide for complete separation of their accreditation and fee-based consulting divisions and staff.
Comment:
One commenter stated that the proposed rule would prohibit the AO from marketing the AO's fee-based consulting services to the AO's accreditation clients. Tools, resources, and services are provided to the public through general email distributions and publications available on the AO's website. It would not be practical to create an educational division and not alert providers to its existence.
Response:
We respectfully disagree with many of the premises of the commenters. In the proposed rule, we proposed that the AOs that provide fee-based consulting services or its associated fee-based consulting division or company must have written fee-based consulting “firewall” policies and procedures. We defined the term “firewall” as the complete and total separation between the AO's accreditation activities and its fee-based consulting services. The purpose of the provisions of proposed § 488.8(j) is to ensure that the AO maintains a complete division between their fee-based consulting program and their accreditation program. In other words, we seek to require AOs prevent any comingling of fee-based consulting activities and staff with their accreditation activities and staff. Development of a joint firewall policy would not be a breach of that policy.
We believe these requirements are necessary because several commenters on our 2018 AO Conflict-of-Interest RFI, as previously discussed, were concerned that firewalls in some instances could be breached. An AO's fee-based consulting division or company could find other ways to market their services to the AO's accreditation clients without approaching them during surveys and accreditation activities.
Final Decision:
After careful consideration of the comments received, we are finalizing this provision with a technical revision to § 488.8(j)(2) to include a cross-reference to the requirement at § 488.5(a)(10) to clarify that the date specified for an AO to submit its written consulting firewall policies and procedures to CMS will be the application deadline (as well as possible other dates as specified by CMS as part of the application process).
J. Prohibit AO Owners, Surveyors, and Other Employees From Involvement With the Survey and Accreditation Process for Healthcare Facilities With Which They Have an Interest or Relationship (Proposed § 488.8(k))
We proposed to add a new requirement at § 488.8(k)(1) to prohibit AOs from allowing AO owners, surveyors, or other employees from participating in the survey and accreditation process for healthcare facilities with which they have had an interest or relationship within the previous 2 years. At proposed § 488.8(k)(1) we would require that if an AO owner, surveyor or other employee has an interest in or relationship with a healthcare facility accredited by the AO, they would be prohibited from: (1) participating in the survey of that healthcare facility (proposed § 488.8(k)(1)(i)); (2) having input into the results of the survey and accreditation for that healthcare facility (proposed § 488.8(k)(1)(ii)); (3) having involvement with the pre- or post-survey activities for that healthcare facility (proposed § 488.8(k)(1)(iii)); or (4) having contact with or access to the records for the survey and accreditation of that healthcare facility (proposed § 488.8(k)(iv)). Proposed § 488.5(a)(10)(iii) lists proposed prohibited interests in or relationships with a healthcare facility accredited by the AO, which we discussed in section IV.D. of this final rule with comment period.
We proposed at § 488.8(k)(2) to define the term “immediate family member” as any person that has a lineal familial or marital relationship with the AO owner, surveyor or other employee. Immediate family members would include a husband or wife, birth or adoptive parent, child, or sibling; stepparent, stepchild, stepbrother, or stepsister; father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law, or sister-in-law; grandparent or grandchild; and spouse of a grandparent or grandchild. This definition is consistent
( printed page 36410)
with the definition used for the home health and hospice conflict-of-interest requirements. This definition is required for the purposes of § 488.8(k)(1), which states that a conflict of interest can also exist when an AO owner, surveyor or other employee has an interest in or relationship with a healthcare facility the AO accredits.
Allowing an AO owner, surveyor or other employee that has an interest in or relationship with a healthcare facility the AO accredits would not only be inappropriate but could result in inaccurate survey results and/or preferential treatment of the facility.
The comments and our responses to the comments are set forth below.
Comment:
Several commenters (2) supported the proposal to prohibit AO owners, surveyors, and other employees from involvement with the survey and accreditation process for healthcare facilities with which they have an interest or relationship requirements of proposed changes. This commenter stated that it would be reasonable to apply these policies to executives and other leaders in AOs.
Response:
We thank these commenters for their support of this proposal.
Comment:
One commenter supported our proposal to prohibit an AO owner, surveyor or other employees from having any involvement with the survey of any healthcare facilities with which the AO owner, surveyor, other employee or their immediate family members currently or within the past 2 years have had a relationship.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter supported prohibiting AO owners, surveyors, and other employees from engaging in the survey and accreditation process for organizations in which they have an interest or relationship.
Response:
We thank this commenter for their support of our proposal to prohibit AO owners, surveyors, and other employees from engaging in the survey and accreditation process for organizations in which they have an interest or relationship.
Comment:
One commenter supported defining the specific familial relationships listed in the proposed rule as creating a conflict of interest.
Response:
We thank this commenter for support of our proposed list of applicable “immediate family members” at § 488.5(a)(10)(iii)(I) whose relationships represent a conflict of interest on the part of a family member who is an AO owner, surveyor or other AO employee.
Comment:
One commenter supported our provision to prohibit an AO owner, surveyor, or other employee from engaging in the accreditation processes for an organization with which they have had past relationship or interest for 2 years.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter opined that numerous conflicts of interest could emerge without this proposed provision, and that such conflicts of interest are capable of seriously undermining the integrity of the AO accreditation process. This commenter stated the opinion that permitting a slackening of standards compromises the public trust.
Response:
We thank this commenter for their comments and agree.
Comment:
One commenter supported this proposal because they already have policies that prohibits their surveyors, or other employees from participating in the survey and accreditation process for healthcare facilities with which they have had an interest or relationship within the previous 3 years. This commenter noted that is an even longer period than proposed by CMS.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter supported our proposal to require AOs submit a declaration from each surveyor disclosing any interests or relationships the surveyor may have in or with another survey agency or healthcare facility that the AO accredits.
Response:
We thank this commenter for support of this proposal.
Comment:
One commenter supported our proposal to require AOs to take steps to prevent an owner or employee with an interest in or relationship with a healthcare facility that the AO accredits, within the previous 2 years, from having any involvement with the survey of that facility, having input into the results of the survey and accreditation for the facility, having involvement with the pre- and post-survey activities for the facility or having contact with or access to the records for the survey of the healthcare facility.
Response:
We thank this commenter for support of this proposal.
Comment:
One commenter supported our proposal to require AOs to collect and submit declarations from surveyors regarding any employment, business, financial, or other relationships they have with the healthcare facilities the AO accredits, aimed at enhancing transparency and trust in the accreditation process.
Response:
We thank this commenter for their support of our proposal at § 488.5(a)(22) to require AOs to obtain and submit surveyor declarations of any interest in and relationships with healthcare providers the AO accredits to CMS on an annual basis.
Comment:
This commenter opined that this requirement would lead to greater transparency in the accreditation process, building trust among interested parties by demonstrating vigilance in preventing conflicts of interest because the COI declarations process seeks to identify and mitigate any potential conflicts of interest that could bias the survey outcomes.
Response:
We thank this commenter for their support of our proposal at § 488.5(a)(22) to require AOs to obtain and submit surveyor declarations of any interest in and relationships with healthcare providers the AO accredits to CMS on an annual basis.
Comment:
One commenter agreed that it would be inappropriate for an AO owner, surveyor, or employee who has an affiliation or interest with a healthcare facility accredited by that AO to participate in the survey and accreditation process for that facility. This commenter urged CMS to hold SAs to the same standard.
Response:
We thank this commenter for their support of this proposal. As we have stated in this final rule with comment period, and in response to the comment urging CMS to apply the same conflict-of-interest requirements to SAs, we do not believe that additional Federal conflict-of-interest requirements are necessary for SAs as they are for AOs because individual State laws, rules, and regulations regarding conflicts of interest already apply to each SA and its employees. Section 4008 of the SOM describes examples of scenarios that would be conflicts of interest for SA surveyors who have an outside relationship with a facility that is surveyed by the SA.[10]
Currently, section 4008 of the SOM applies only to SA surveyors and not AO surveyors.
Comment:
One commenter urged CMS to prohibit AO owners, surveyors, and other employees—including their immediate family members who have an interest in or relationship with a surveyed healthcare facility from having direct or indirect input into survey results. This commenter further suggested that this prohibition apply to pre- or post-survey activities and a ban on access to all survey records.
Response:
We thank this commenter for their support of the proposals we
( printed page 36411)
have made to prevent these types of AO conflicts of interest.
Comment:
One commenter supported our proposal to prohibit AO owners, surveyors, and other employees from involvement with the survey and accreditation process for healthcare facilities with which they have an interest or relationship. This commenter stated that they support this proposal for the following reasons:
This proposal is essential for maintaining the integrity and impartiality of the accreditation process.
Allowing individuals with such connections to participate in accreditation activities not only creates a conflict of interest but also undermines the perception of fair and objective assessment of quality standards.
It opens the door to potential inaccuracies in survey results and the risk of preferential treatment toward affiliated facilities if AO owners, surveyor or other employees that have an interest in or relationship with a healthcare facility accredited by the AO are permitted to have any involvement with the survey process for that facility.
To uphold the credibility of accreditation and ensure the public's trust, it's imperative to enforce strict measures that prevent any undue influence or bias in the accreditation process.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter stated that the business model of using part-time reviewers (surveyors) could increase the likelihood of a conflict of interest and increase variation in the accreditation process.
Response:
We thank this commenter for their comments. We agree that part-time surveyors may be more likely to be employed by healthcare facilities that are accredited by the AO.
Comment:
One commenter stated that there are several steps an AO could take to help reduce the number of conflicts of interest for AO staff and surveyors. These steps include: (1) Hiring full-time surveyors who are sent to many geographic locations could result in fewer entanglements because they would not be hiring from the specific community where the reviews must be done; and (2) Not allowing AO employee surveyors to engage in outside consultant work.
Response:
We thank this commenter for sharing this information.
Comment:
One commenter stated that organizational investments in people and processes, such as providing ongoing training, interrater reliability assessments, and professional development from within their organization, drive out avoidable variation during an accreditation.
Response:
We thank this commenter for their comment. We agree that if an AO employee receives the professional development and training necessary to further their professional career, they may be less likely to seek secondary employment at a healthcare facility that can provide these benefits.
Comment:
One commenter acknowledged that certain types of relationships could result in perceived or actual conflicts of interest. However, this commenter stated that health systems are large organizations and there are bound to be scenarios where AO staff or a family member would have some type of relationship with the healthcare system.
This commenter stated that the proposed definition of “immediate family member” is broad and includes not only the AO owners, surveyors or employees, but also their family members (89 FR 12063). The commenter recommended that, if CMS decided to proceed with its proposal, the agency should narrow the scope of this provision by limiting the categories of individuals who would fall under this conflict-of-interest provision, as well as the types of financial or other relationships that would result in a conflict.
Response:
We used the definition of “immediate family member” set forth in the CY 2022 Home Health Prospective Payment System Rate Update (86 FR 62368). While this definition may be the same or similar to other rules for other subject matter, this does not make it inappropriate for use in the acute healthcare setting.
This issue of immediate family members arose because, at § 488.5(a)(10)(iii)(I), we proposed that AOs provide policies and procedures for the prevention and handling of potential or actual conflicts of interest that could arise from situations in which an AO owner, surveyor, or other employee has a business, employment or financial interest in or relationship with another survey agency or healthcare facility to which the AO provides accreditation services. This requirement made it necessary for us to provide examples of such situations. At proposed § 488.5(a)(10)(iii), we specifically noted that a conflict of interest would occur if the AO surveyor's immediate family (other than a non-managerial employee of a health facility accredited by the AO) engaged in any of the stated activities (89 FR 12005).
Allowing an AO owner, surveyor or other employee that has an interest in or relationship with or that has an immediate family member (as defined by proposed § 488.5(a)(10)(iii)) employed by or has an interest in or relationship with a healthcare facility that is accredited by the AO would not only be inappropriate but could result in inaccurate survey results and/or preferential treatment of the facility. We say this because if an AO owner, surveyor or other employee has a family member employed at a healthcare facility that is accredited by the AO, that AO owner, surveyor or other employee may have a bias towards or against that facility which could have an effect on the survey results.
As we stated in the proposed rule, an AO surveyor, owner, or other employees' or their immediate family member's interest in or relationship with a healthcare facility that the AO accredits could present a conflict of interest that could affect the results of a survey in several ways. For example, an AO owner, surveyor, or other AO employee involved in the survey of a healthcare facility with which the individual has an interest or relationship could have compromised judgment, consciously or unconsciously, regarding that facility.
For example, a surveyor with an interest in or relationship with the healthcare facility being surveyed could be inclined to minimize or ignore deficiencies, possibly because he or she believes these deficiencies are not representative of the facility. A surveyor who has an interest in or relationship with the facility being surveyed could possibly influence the findings made by other members of the survey team by asking them to give the facility credit for things not observed, since he or she can “vouch” for the facility.
Comment:
One commenter stated that the proposed restriction of not allowing AO owners, surveyors or other employees that have immediate family engaged in any of the stated activities, other than being a non-managerial employee of a health facility that is accredited by the AO be involved with the survey and accreditation decision making process for that facility is too restrictive.
Response:
We respectfully disagree with this commenter. The scenario in which an AO owner, surveyor or other employee has an immediate family employed at a facility accredited by the AO is a clear conflict of interest because the AO surveyor could have a reason to be biased for or against the facility. Also, the family member employed at the healthcare facility could provide the surveyor with information about the facility that may not be otherwise
( printed page 36412)
available to him or her during the survey process that could affect the outcome of the survey.
We believe that the benefits of prohibiting an AO owner, surveyor, or other employee from having any involvement with the survey process for a healthcare facility in which an immediate family member is employed, and thus removing a conflict-of-interest, far outweighs any inconvenience to the AO. In addition, we believe that the AOs are willing to prevent conflicts of interest.
We do not believe that having to prohibit an AO owner, surveyor, or other employee from having any involvement with the survey process for a facility at which an immediate family member is employed would be burdensome to the AOs. The AO could simply replace the conflicted surveyor with one that did not have any relationship or interest in the healthcare facility being surveyed. Moreover, we would not expect this kind of conflict-of-interest scenario to be a frequent occurrence.
Comment:
One commenter stated that this proposed restriction could prohibit family members from participating in any activities with each other such as program decision-making or outcome reviews that would involve both parties. Therefore, employment in either organization itself would not necessarily reflect a conflict-of-interest.
Response:
While we are not clear as to what the commenter means by “prohibit family members from participating in any activities with each other
such as program decision-making or outcome reviews”
[emphasis added], we disagree with this commenter if they mean that by participating with each other in program decision-making or outcome reviews, an AO owner, surveyor, or other employee has involvement with the survey and accreditation decision-making process for a healthcare facility in which an immediate family member is employed by the accredited facility and participates in the survey process for the facility, including the requisite interactions between the healthcare facility and the AO during this process. The purpose of this proposed restriction is to prevent both the facility and the AO from either consciously or unconsciously exploiting their interest in or relationship with such provider or supplier to bias the result of a survey. This restriction, as finalized, will only prohibit the AO owner, surveyor, or employee from involvement from the survey and accreditation decision-making process for that facility at which their immediate family member is employed, and which gives rise to an interest or relationship with that facility on the part of that AO owner, surveyor, or employee. The family member employed at the facility would not be restricted from performing the duties of their employment, unless they are required to participate in the survey process. The immediate family member facility employee would only be required to recuse themselves from any involvement with the survey process.
We do not anticipate a scenario in which an AO surveyor would be working with an immediate family member who is an employee of a healthcare facility that is being accredited by the AO, unless that AO surveyor was also employed at such healthcare facility. In such a case, this AO surveyor would have a direct interest in and relationship in the healthcare facility accredited by the AO that would disqualify them from involvement with the survey and accreditation decision making processes for that facility.
It is important to note that requirements of § 488.8(k) would not prohibit AO employees from working with the appropriate employees at a healthcare facility for the purposes of the pre-survey accreditation process and fee-based consulting (with the restrictions set forth as § 488.8(i).
Comment:
One commenter recommended that CMS qualify the definition of “immediate family member” at § 488.5(a)(10)(iii)(I) to limit it to an immediate family member employed by an AO who works in a position to make decisions or influence a survey outcome; only those individuals should be required to abstain from any accreditation activity. Another commenter proposed that the definition of “immediate family member” at § 488.5(a)(10)(iii) should pertain only to an immediate family member employed by an AO who works in a position to make decisions or influence a survey outcome should abstain from any accreditation activity for a provider organization that is accredited by the AO and has an immediate family member in its employment. Qualifying the circumstances for immediate family members is in line with standard Federal conflict-of-interest practice. This commenter stated that when an AO owner, surveyor, or other employee has an immediate family member that is employed at a healthcare facility that is accredited by the AO, only those AO employees that work in a position to make decisions or influence a survey outcome should abstain from any involvement in the survey and accreditation process for that particular facility.
Response:
This commenter requested that CMS limit the AO staff that would be prohibited from having involvement with the survey process to only those who work in a position to make decisions or influence a survey outcome. We do not believe that limiting this requirement to only those AO staff that work in a position to officially make decisions or influence a survey outcome would be restrictive enough to mitigate the conflict of interest associated with having a family member employed by a healthcare facility accredited by the AO. We say this because while only some of the AO staff officially make accreditation decisions, others have the potential to influence or alter these decisions.
The scenario in which an AO owner, surveyor or other employee has an immediate family employed at a facility accredited by the AO is a clear conflict of interest because the AO employee could have a reason to be biased for or against the facility, regardless of whether their job is to make accreditation decisions or not. For example, the family member of a surveyor who is employed at the healthcare facility could provide the surveyor with information about the facility that may not be otherwise available to the surveyor during the survey process that could affect the outcome of the survey. Also, an AO employee that does not make survey decisions and that has an immediate family member that works for the facility that is being surveyed could attempt to influence the survey outcome by: (1) discussing the facility with the survey team (that is, explaining the facility's policies and procedures to the survey team); (2) actively advocating on the facility's behalf. In addition, an AO secretary, who has a family member employed at a healthcare facility that was surveyed by the AO could potentially alter the survey report to make it better and hide deficiencies. Such activities could potentially influence the survey results and/or post-survey decision making process. Section 488.8(k) provides that any AO employee, including the AO owner, surveyors or other AO employee, who has a relationship with or interest in or has an immediate family member that is employed by a healthcare facility accredited by the AO would be prohibited from any involvement in the survey and accreditation process for that facility.
We believe that it is necessary to apply the requirements of § 488.8(k) for several reasons. As we stated in the
( printed page 36413)
proposed rule, surveyors must rely on their professional judgment, in addition to Federal rules and guidelines, to determine compliance. As previously discussed, an AO surveyor, owner, or other employees' interest in or relationship with a healthcare facility that the AO accredits could present a conflict of interest that could affect the results of a survey in several ways. Even if the AO employee with the interest in or relationship with the facility being surveyed is not part of the survey team for the facility, he or she could still potentially influence the members of the survey team prior to or after the survey. For example, attempting to influence the survey decision making process, or the AO's survey follow-up activities by attempting to discuss the facility with the survey team, such as explaining the facility's policies and procedures to the survey team, or even actively advocating on the facility's behalf, potentially influencing their analysis of observed survey results. An AO surveyor, owner, or other employee that has an interest in or relationship with a healthcare facility the AO accredits might have additional motivation to improperly give that healthcare facility notice about the survey ahead of the scheduled survey date. Surveys are required to be unannounced to prevent the facility from preparing for the survey by activities such as unusual cleaning activities, painting, clearing obstructions from halls and entrances, covering up and hiding deficiencies, coaching staff, and otherwise preparing in advance for the survey. If the survey is unannounced, the healthcare facility is not able to make advance preparations so that the survey team is able to assess the facility in its usual condition and observe the typical standard of care provided.
Comment:
One commenter recommended that time restrictions for individuals with interests in or relationships with healthcare facilities accredited by the AO to participate in the survey or accreditation process for those facilities be limited to the prior 1 year (not 2 years).
Response:
In the proposed rule, we proposed to prohibit an AO owner, surveyor, or other employee that has an interest in or relationship with a healthcare facility that AO accredits within the past 2 years from having any involvement in the survey process for that healthcare facility. We proposed a 2-year time-period for the interest in or relationship with a healthcare facility accredited by the AO to be consistent with other rules we have finalized. We believe it is best to have the same requirements across all healthcare settings. Therefore, we will not be following this commenter's recommendation.
Final Decision:
After careful consideration of the comments received in response to this proposal, we have decided to finalize these provisions as proposed, except for § 488.2(k)(2), which we are finalizing with a minor change to conform with the language proposed at § 488.5(a)(10)(iii)(I) for the reasons explained previously.
As finalized, § 488.8(k)(1) will require AOs that have an owners, surveyors or other employees who has an interest in or relationship with a healthcare facility accredited by the AO to prohibit said owners, surveyors, and other employees from engaging in the following activities related to the healthcare facilities with which they have a relationship or interest:
(1) Participating in the survey of that healthcare facility (§ 488.8(k)(1)(i));
(2) Having input into the results of the survey and accreditation for that healthcare facility (§ 488.8(k)(1)(ii));
(3) Having involvement with the pre- or postsurvey activities for that healthcare facility (§ 488.8(k)(1)(iii)); or
(4) Having contact with or access to the records for the survey and accreditation of that healthcare facility (§ 488.8(k)(iv)).
As finalized, § 488.5(a)(10)(iii) would define such relationships with or interests in healthcare facilities accredited by the AO as including but not be limited to:
(1) Being employed as a SA surveyor;
(2) Being employed in a healthcare facility that is accredited by the AO;
(3) Having an ownership interest in a healthcare facility that is accredited by the AO;
(4) Serving as a director of or trustee for the AO;
(5) Serving on a utilization review committee of a healthcare facility that is accredited by the AO;
(6) Accepting any fees or payments from a healthcare facility or group of healthcare facilities that is/are accredited by the AO;
(7) Accepting fees for personal services, contract services, referral services, or for furnishing supplies to a healthcare facility that is accredited by the AO;
(8) Providing consulting services to a healthcare facility that the AO accredits;
(9) Having an immediate family member engaged in any of the listed activities; or
(10) Engaging in any activities during the course of the survey of the facility that would be or cause a conflict of interest.
As finalized, § 488.8(k)(2) conforms with the definition at § 488.5(a)(10)(iii)(I) and defines the term “immediate family member” as any person with which the accrediting organization owner(s), surveyors or other employees have a lineal or immediate familial or marital relationship, including a husband or wife, birth or adoptive parent, child, or sibling; stepparent, stepchild, stepbrother, or stepsister; father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law, or sister-in-law; grandparent or grandchild; and spouse of a grandparent or grandchild. This definition is consistent with the definition used for the home health and hospice conflict-of-interest requirements.
K. Require the AOS that Accredit Medicare-Certified Providers and Suppliers To Use Medicare Conditions; and Strengthened Survey Process Comparability (Proposed § 488.4(a)(1) and (2))
Section 1865(a)(1) of the Act requires that if the Secretary finds that the requirements for accreditation from an accreditation organization demonstrate that a provider entity meets or exceeds all applicable conditions, the Secretary must deem such requirements to be met by the provider entity. The statutory language of “meets or exceeds” currently allows AOs to develop standards that are more stringent than those of Medicare. When an AO applies for “deeming authority,” we determine whether those standards meet or exceed ours. In accordance with § 488.5(e), CMS publishes a proposed notice when CMS receives a complete application from a national accrediting organization seeking CMS' approval of an accreditation program. The proposed notice identifies the organization and the type of providers or suppliers to be covered by the accreditation program and provides 30 calendar days for the public to submit comments to CMS. CMS subsequently publishes a final notice, rendering its decision to either approve or disapprove a national accrediting organization's application, within 210 calendar days from the date CMS determines the AO's application was complete. The final notice outlines a summary of the findings of CMS' review and any corrective action which was required to be taken by the AO to be considered to meet or exceed our standards, or comparable survey processes. When CMS approves or reapproves an accrediting organization for deemed status, the approval may not exceed 6 years.
We are concerned that the current application review processes under § 488.5 do not go far enough. Some of
( printed page 36414)
our concerns with the efficacy of the AO application review process are based on the results of the initial and renewal applications and the SA findings, as noted in this section:
AO Application Reviews:
Between 2017 to September 2021, we received a total of 22 AO applications for review. After review of these applications, we returned all 22 applications to the AOs because we found that the AOs' standards were not comparable to ours. The AOs' most common standards requiring revisions to meet or exceed Medicare conditions included: governing body, physical environment, emergency preparedness, patient rights, medical/clinical records, and care planning. Additionally, AO standards regarding coordination of services; skilled professional services; infection control; staff responsibilities, and quality improvement assessment programs (QAPI) all required revisions by the AOs.
SA Findings:
In FY 2019, CMS conducted 119 hospital surveys (including psychiatric hospitals) and 196 non-hospital surveys totaling 315 validation surveys. In FY 2019, the SAs found serious “condition-level” instances of non-compliance 60 times in accredited hospitals (including psychiatric hospitals), and 51 instances in which the AO missed the deficiencies. In these instances, even though the AOs did not find comparable levels of non-compliance, this non-compliance was sufficient to start enforcement proceedings against the subject hospitals. These results demonstrated that the AOs may have failed to ensure their facilities were meeting Medicare's minimum standards. In total, between FY 2017 and FY 2019, CMS conducted 363 hospital (including psychiatric hospitals) validation surveys, with SAs identifying condition-level non-compliance a total of 185 times, and 158 instances in which the AOs missed comparable deficiencies. Between FY 2017 and FY 2019, CMS also conducted a total of 369 validation surveys for HHAs and Hospices, with SAs identifying condition-level non-compliance a total of 57 times and 50 instances in which the AOs missed comparable deficiencies.[11]
This data has amplified CMS' concerns related to the comparability of survey processes as well as the need for increased AO oversight.
Therefore, under the statutory authority granted to us under section 1865(a)(1) of the Act, we proposed revisions at § 488.4(a)(1) to require that the AOs that accredit Medicare-certified providers and suppliers use the applicable Medicare conditions as set out in CMS regulations as their minimum accreditation standards. This meant that the AOs would be required to incorporate the Medicare conditions identical to our regulations within their accreditation standards for their deeming programs. However, AOs would be allowed to use additional accreditation standards that exceeded the Medicare conditions, as permitted under section 1865(a)(1) of the Act. We would, however, require the AOs to clearly delineate their additional accreditation standards that exceed the Medicare conditions when seeking CMS approval for deeming authority.
The requirement that the AOs identify the Medicare conditions as their accreditation standards would also allow providers and suppliers to know what the minimum Medicare deeming standards are and where the AO standards exceed these standards through its accreditation program, as permitted under section 1865(a)(1) of the Act. Facilities are expected to comply with regulatory requirements of CMS and the accreditation standards of the AO; however, we have found that in certain circumstances, the facilities were more familiar with AO standards and did not fully understand that the AO standards are sometimes more stringent than the Medicare conditions. There were several instances in which our comparability review of AO standards under § 488.5 resulted in the need for AOs to correct deficiencies in their survey standards and processes, because we determined that the minimum Medicare conditions would have not been adhered to. Despite these frequent reviews, the current regulations only require AO standards to be comparable, not duplicative of the Medicare conditions, therefore increasing the likelihood of inconsistencies in interpretation.
This proposed requirement would increase the likelihood that AO standards and processes would meet or exceed our regulatory requirements and transparency for providers to understand when the AO has more stringent standards, further explained in section IV.D. of the proposed rule.
We also proposed to strengthen our process for comparability review of the AOs survey processes at proposed § 488.4(a)(2), further explained in sections IV.E. and IV.F. of the proposed rule. More specifically, we proposed to re-designate existing paragraph (a)(1) as (a)(3) and re-designate existing paragraph (a)(2) as (a)(4) with revisions and add a new requirement at § 488.4(a)(1). This provision would require the AOs that accredit Medicare-certified providers and suppliers to use the exact text of the applicable Medicare conditions set forth in the applicable CMS regulations for each provider and supplier type as their minimum accreditation requirements. However, the AOs would be free to establish additional accreditation requirements that exceed Medicare conditions as permitted by section 1865(a)(1) of the Act. We proposed to add language at § 488.4(a)(2) that AOs use a survey process comparable to the processes set out for SAs in the SOM and approved by CMS, as outlined throughout § 488.5(a)(4). We also proposed that these requirements and changes at paragraphs (a)(1) and (2) would be applicable beginning 1 year from the effective date of the final rule with comment period.
These proposed changes to § 488.4(a)(1) and § 488.4 (a)(2) would align national health and safety standards across all AOs and strengthen the survey processes used by the AOs. We further believe that our proposal would ensure uniformity and transparency of the surveys performed by the AOs for deeming purposes and improve CMS' ability to accurately evaluate an AO's performance.
We proposed to re-designate the current § 488.4(a)(1) and (a)(2) to § 488.4(a)(3) and (a)(4). We also proposed to add requirements at paragraphs (a)(1) and (a)(2) that AOs incorporate the Medicare conditions and use survey processes comparable to those of the SA. We also refer readers to additional proposed changes made to § 488.4(a)(4) in section IV.O. of the proposed rule.
The proposal to require AOs to incorporate the Medicare conditions (as defined in § 488.1) as their minimum accreditation standards would become applicable 1 year after the effective date of the final rule with comment period.
We received several comments on the proposed provisions for use of same survey standards and the comparability of survey processes. The comments and our responses to the comments are set forth in sections III.K., III.L., and III.M. for the standards, crosswalk, and survey comparability provisions of this final rule with comment period.
We received two overarching comments related to the overall
( printed page 36415)
provisions for use of the same Medicare standards and survey comparability.
Comment:
One commenter stated that while the commenter appreciates CMS' desire to strengthen comparability, it is unclear how CMS intends to address variability within the deeming application documentation requirements. The commenter referenced that CMS currently provides a checklist for the application documentation and that the format is at the discretion of the AO. This commenter urged CMS to propose a more efficient and organized approach to reduce redundancy and duplication, while also easing burden on CMS during the application review. The commenter recommended adoption of a standard operating procedure (SOP) that includes a standardized application template enabling AOs to respond directly to the regulatory requirements and a standardized list of required attachments for the provision of supporting evidence. The commenter requested CMS to clarify what CMS is specifically looking for when determining “comparability.”
Response:
We appreciate the commenter's suggestion for CMS to provide an application template for those AOs seeking deeming authority. As noted by the commenter, CMS provides AOs with a checklist for the application documentation requirements, however we have not specifically identified a format as CMS has provided flexibilities to AOs. For instance, one AO may provide all documentation in a large zip-file, while other AOs may submit separate files. CMS will review the ability for more streamlined submissions in sub regulatory and policy guidance, yet our goal is to provide a level of flexibility and innovation by AOs. We believe that requiring a crosswalk with AOs using the same language as the CoPs for their minimum health and safety standards will further streamline CMS' application review processes and as outlined in the crosswalk example of the preamble in section III.L. of this final rule with comment period, CMS has suggested a template for use. Furthermore, our assessment of comparability is aimed at assessing an AO for comparable processes against those of the SA and as outlined in the SOM as outlined in the proposed provisions. The goal is to bring greater parity to the survey processes between SAs and AOs and reduce provider confusion. As outlined in the preamble, CMS has often required AOs to submit supplemental information such as information about surveyor training and requested the inclusion of questions posed by survey teams for evaluation of specific Medicare conditions, as the survey process policies may have not always included requirements which are expected by the SA when evaluating facilities as outlined in the SOM. For example, SA surveyors are expected to ask specific questions of the facility or during interviews with leadership depending on the specific Medicare condition. While AOs may generally have surveyor guidance suggesting a comparable review, CMS has observed firsthand during survey observations of the AOs (during their application processes), that AO surveyors omit asking facilities certain questions which CMS has deemed important to assess compliance. Therefore, the provisions pertaining to increased survey comparability aim to ensure survey processes between SAs and AOs are strengthened to ensure a consistent evaluation of both deemed and non-deemed providers and suppliers.
Comment:
One commenter, while in support of both provisions related to the use of same standards and the strengthened comparability of survey processes, also encouraged CMS to pursue granting deeming authority for Skilled Nursing Facilities (SNFs). In particular, the commenter observed that AOs may currently accredit a SNF, but that CMS does not recognize deeming authority for SNFs. The commenter believes the proposed provisions will provide greater consistency among SAs and AOs but also suggest that offering AOs deeming authority with respect to SNFs would provide value to survey and certification and alleviate pressure from deeply underfunded and overextended SAs.
Response:
We appreciate the commenter's support of our proposed provisions. With respect to allowing SNFs to participate in Medicare via accreditation, sections 1819(g) and 1919(g) of the Act specify that the State, rather than an AO, is responsible for certifying compliance with long-term care facility requirements. Consequently, the statute does not permit us to offer “deeming authority” for LTC facilities at this time.
Final Decision:
We are finalizing the revisions to § 488.4(a) as proposed with modifications to the numbering and ordering of the regulatory provisions. The proposed regulatory provisions at §§ 488.4(a)(3) and (4) will remain where they currently are at § 488.4(a)(1) and (2), respectively, and with the regulatory text finalized as proposed. Proposed § 488.4(a)(1) and (2) will be finalized at paragraphs (a)(3) and (4), respectively. We have also made technical changes with minor re-wording of the proposed requirements and the existing requirements to make the provisions more understandable. These changes were made in the interest of clarity and do not constitute any changes in policy, nor they do establish any new requirements in addition to those already proposed and finalized in this rule. We have included a Waiver of Notice of Proposed Rulemaking in section VIII. of this final rule with comment period.
We are also modifying the provisions as proposed at §§ 488.4(a)(1) and (a)(2) by removing the phrase, “which are applicable beginning [DATE 1 YEAR AFTER THE EFFECTIVE DATE OF THE FINAL RULE]”. We are making this modification for this final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date and individual provisions will no longer need to be specified in the regulations text.
For a more detailed discussion of the revisions to §§ 488.5(a)(3) and (a)(4), we refer readers to sections III.L., III.M., and III.N. of this final rule with comment period related to the finalization of our provisions for the crosswalk requirements and for the use of same survey standards and strengthened comparability of survey processes.
L. Revise the Crosswalk Requirements at § 488.5(a)(3)
As a result of our proposed requirement at § 488.4(a)(1) (revised as § 488.4(a)(3) in this final rule with comment period) to require the AOs to incorporate the Medicare conditions into their accreditation standards for their deeming programs, we also proposed to modify the regulations at § 488.5 that would be affected by this requirement. Section 488.5(a)(3) requires the AOs to submit with their initial and renewal application, “[a] detailed crosswalk (in table format, as specified by CMS) that identifies, for each of the applicable Medicare conditions (as defined in § 488.1) or requirements, the exact language of the organization's comparable accreditation requirements and standards.” Because section 1865(a) of the Act allows AOs to have accreditation standards for their deeming programs that meet or exceed the Medicare conditions, the content, format, and wording of AOs' accreditation standards have frequently differed significantly from that of the Medicare conditions. Therefore, we require the AOs to provide a crosswalk which identifies the applicable Medicare conditions that corresponds to each of the AO's accreditation standards. The purpose of this
( printed page 36416)
crosswalk is to help us determine to which Medicare condition each AO accreditation standard corresponds.
Since we proposed at § 488.4(a)(1) to require the AOs to incorporate the Medicare conditions into their accreditation standards, it would no longer be necessary to require the AOs to submit a crosswalk that provides “comparable” standards. Instead, we proposed that AOs would need to provide a crosswalk which demonstrates that the AO has incorporated the language of the Medicare conditions, as well as to provide the AO standards which exceed the Medicare conditions (for an example, see Table 2 in section VII.B.I of the proposed rule). Similar to the existing process for submission of the AO's crosswalk during an application, we proposed to revise § 488.5(a)(3) to require a crosswalk that demonstrates the AO's use of CMS' requirements and standards. AOs would provide their additional or exceeding standards under their use of the required exact language and annotate the exceeding standards. This would further allow providers and suppliers to easily identify the minimum Medicare deeming standards and where the AO standards exceed these standards through its accreditation program.
We proposed to revise § 488.5(a)(3) to first remove the requirement that the AO provide a “comparable” standard for each of the applicable Medicare conditions or requirements and replace it with the adoption of the CMS requirements in the AO accreditation standards for any deeming program. Second, in the application that is submitted to CMS for review, the AO would have to submit a detailed crosswalk. While we would not expect the AO to use the same CMS' CFR regulatory citations (for example, § 482.11(c) as in Tables 1 and 2) and survey tags (a letter/number identifier; for example, A-0023 as in the tables here) in place of the AO's specific standard numbers as they are used in the AO's internal processes and for surveys of its accredited facilities, we would expect the AO to use the applicable CMS identifiers in the appropriate column of the crosswalk table to meet the requirements being finalized in this rule. For example, CMS' regulatory requirement at § 482.11(c) requires hospitals to “assure that personnel are licensed or meet other applicable standards that are required by State or local laws.” In this example and aligned with our proposed provisions, the AO would be required to have an accreditation standard for its hospital deeming program which would state “The hospital must assure that personnel are licensed or meet other applicable standards that are required by State or local laws,” with the AO's applicable standard number. For this example, the crosswalk would appear as follows in Table 1, with the CMS CFR citations and survey tags in the first column and the AO standard numbers in the third column.
Table 1—AO Crosswalk-Meets CMS Requirements
CFR
citation and
survey tag
Medicare
conditions language
AO
standard number
AO
standards language
§ 482.11(c)
(A-0023)
The hospital must assure that personnel are licensed or meet other applicable standards that are required by State or local laws
XX.000
For hospitals under CMS deeming authority: The hospital must assure that personnel are licensed or meet other applicable standards that are required by State or local laws.
As seen in this example in Table 2, the AO standard number identification may vary from CMS' CFR regulatory citation. Additionally, as previously described, CMS is not restricting AOs from exceeding the Medicare conditions. Therefore, if an AO believes that additional accreditation standards would need to apply to their deemed facilities, an AO would submit the exceeding requirements under the particular standard. Using the same example, the AO would submit a crosswalk similar to the example below. As seen, AO Standard Number XX.001 would be exceeding the Medicare conditions.
Table 2—AO Crosswalk Exceeds CMS Requirements
CFR citation
and survey tag
Medicare conditions
language
AO standard number
AO standards language
§ 482.11(c)
(A-0023)
The hospital must assure that personnel are licensed or meet other applicable standards that are required by State or local laws
XX.000
For hospitals under CMS deeming authority: The hospital must assure that personnel are licensed or meet other applicable standards that are required by State or local laws.
XX.001
Hospitals must verify credentials of all providers including all contracted staff or individuals under arrangement. The verification must be completed prior to the official hiring of the staff.
Establishing a consistent standard across all AOs would bring transparency to the accreditation process. This would allow providers and suppliers to know what the minimum Medicare deeming conditions are and where the AO standards exceed these Medicare conditions through its accreditation program. It would also provide greater uniformity between an AO certification survey at a facility and a State survey that may be subsequently performed at that same facility, which could include a complaint survey or a validation survey.
Additionally, from CMS' oversight perspective of the AO applications for deeming authority and review of the crosswalks over the last several years, we have also identified that AOs have
( printed page 36417)
inadvertently omitted certain standards in their crosswalk submissions. Therefore, while the impression that requiring a crosswalk for AOs may seem unnecessary, as we would be requiring AOs to incorporate the Medicare conditions into their accreditation standards, it is imperative that CMS be able to ensure the AO has standards for each Medicare condition. The review of the exceeding standards is also critical for CMS to ensure that any additional requirements established under accreditation for deemed providers or suppliers do not conflict with the Medicare conditions.
We proposed that the provision would be applicable 1 year after the effective date of the final rule with comment period.
The comments and our responses to the comments are set forth below. We received several comments of general support for the proposal to require AOs to use the same minimum health and safety standard language as the Medicare conditions and to provide CMS with a crosswalk outlining use of the same standards and any exceeding standards.
Comment:
Several commenters provided overarching support for the proposed provisions. One commenter stated the proposal would promote clear communication of AOs' standards. Another commenter suggested this would contribute to consistently improved results. One commenter also stated that this provision would streamline an already-lengthy review process as well as provide further alignment across AOs and SAs. One commenter stated this proposal would provide transparency by ensuring AOs incorporate the language of the Medicare conditions even if the AO standards exceed the Medicare conditions. This commenter also stated the provision would provide transparency to providers and suppliers by better standardizing survey practices between SAs and AOs. Another commenter stated that alignment of the language is critical to decrease unnecessary hospital burden.
Response:
We appreciate the commenters' support of our proposal, and we agree this process would support overall transparency and standardization. We also appreciate and agree with the one commenter's statement that this would streamline review processes and further align AOs and SAs. We also agree that alignment of the language would decrease burden in relation to healthcare organizations understanding the minimum health and safety standards for Medicare participation.
Comment:
One commenter provided general support of the provisions for use of same language of the Medicare conditions and strengthened survey process comparability. The commenter suggested that these provisions will provide alignment and consistent application of standards, which is important for protecting patients and maintaining the integrity of the survey process. The commenter appreciated CMS' intent to ensure AOs are working in a consistent and unbiased manner. Another commenter echoed that alignment with the Medicare conditions would help improve alignment and ensure AOs conduct their work in a consistent, unbiased manner.
Response:
We agree with the commenters and thank them for their general support.
Comment:
One commenter stated that AOs that accredit Medicare-certified home health agencies and hospices do incorporate the Medicare conditions in their standards. This commenter agreed that adopting the same language as CMS regulations within the AOs accreditation standards is best and eliminates any ambiguity. The commenter was in support of this requirement and the crosswalk provisions. One commenter, in support of the proposed provisions, stated that the line between the Medicare conditions and additional accreditation standards can be blurry; therefore, providing clearer standards will prevent confusion among the medical staff and can potentially incentivize facilities to pursue higher standards of care. The commenter noted that this proposal would not prevent an AO or facility from being recognized for exceeding those standards. Another commenter, also in support, urged CMS to finalize the proposal and stated this would align health and safety standards across all AOs and strengthen consistency of the survey process while also improving the transparency of accreditation and reduce potential provider confusion and misinterpretation of accreditation standards. One commenter supported our proposed provision, stating that the requirement to provide a crosswalk linking the AO's accreditation standards to the corresponding Medicare conditions is a critical step in enhancing transparency, accountability, and consistency within the accreditation process. The commenter suggested that a crosswalk facilitates CMS in evaluating AOs accurately, ensuring that healthcare delivery meets quality standards effectively. Further, the commenter stated that this would provide a clear apples-to-apples comparison and facilitate thorough understanding of accreditation standards to drive improvements.
Response:
We appreciate the commenters' general overall support. We appreciate the commenters support on our proposed provision to require AOs to use the same minimum health and safety standards as the Medicare conditions. We agree that these proposals will not restrict an AO from requiring additional more stringent standards or for facilities to exceed the minimum standards. As the commenters stated, the proposal is to promote clarity and reduce confusion. We agree that the provisions of a crosswalk and use of one-to-one Medicare standards as the minimum health and safety standards provides transparency, consistency, and an understanding of the Medicare conditions for deemed facilities under an AO.
Comment:
One commenter stated that leveraging Medicare participation standards as a foundation offers numerous advantages, including a trusted benchmark, streamlining processes, and maintaining a primary focus on patient safety and quality. This commenter suggested the proposal would provide a solid framework for AOs to survey to the same CMS requirements and standards as the SAs, yet also advised that it is crucial to acknowledge the necessity of supplementing the standards with facility-specific criteria to ensure comprehensive and tailored assessments that truly reflect the diverse needs and standards across healthcare sectors.
Response:
We agree with the commenter, and we note that the proposed provisions do not restrict or limit AOs from continuing to impose additional health and safety requirements which exceed the Medicare minimum standards. However, the proposed provision is aimed to ensure greater clarity among Medicare-participating facilities on the Medicare requirements, and as suggested by the commenter, provides a solid framework.
Comment:
One commenter advised that members of its organization have established effective working relationships with the AOs to ensure Medicare's health and safety requirements are met or exceeded. This commenter specifically stated that members of its organization are Medicare participants that must comply with specified statutory requirements of the Act and other regulatory requirements designed to protect the health and safety of patients and that some of its members demonstrate compliance with the applicable CoPs by achieving accreditation through a CMS-
( printed page 36418)
approved national AO that CMS recognizes as applying standards and processes indicating regulatory compliance, rather than through a SA, in accordance with section 1865(a) of the Act. The commenter stated that the service provided by the AOs is of vital importance because the “deemed” status for accreditation earned by the hospitals satisfies the CMS requirement that a provider qualifies, or continues to qualify, for participation in the Medicare program.
Response:
We appreciate the comment and agree that establishing a rapport between a facility's staff and an AO is critical to ensure the Medicare requirements are understood for deemed programs. We further believe that by ensuring SAs and AOs use the same minimum health and safety standards will bring greater parity to the understanding of the regulatory requirements for Medicare participation.
Comment:
Two commenters supported CMS' efforts to require a crosswalk and urged CMS to make the crosswalks public to ensure providers have the complete and accurate information related to the standard requirements when choosing between using an SA or AO to meet their certification needs.
Response:
We appreciate the commenters' support and agree that transparency of the Medicare requirements and AO standards would be beneficial for the provider and supplier community. We would encourage AOs to consider transparency and public posting of their standards which would demonstrate the AOs minimum health and safety standards mirror those of the Medicare conditions and how participation with that respective AO also exceeds the minimum requirements, should the AO have exceeding standards. CMS believes exceeding standards further promote patient safety and quality of care. However, our provision is aimed at reducing potential inconsistencies while also ensuring healthcare entities are aware of the Medicare standards.
Comment:
One commenter supported the proposal and noted that this proposal, in connection with the proposals on strengthening survey process comparability, would further ensure that surveys identify lapses in patient safety and opportunities for improving strategies that strengthen the delivery of care. The commenter suggested that AOs such as The Joint Commission routinely meet or exceed the regulatory standards enforced by CMS yet was in support and referenced that this could align further with the prevention and reduction of hospital-acquired infection initiatives.
Response:
We appreciate the commenters support of our proposals to require AOs use the same minimum health and safety standards of the CoPs and our proposals to further align survey processes. We agree with the commenter that this proposal will support reducing inconsistencies in the implementation of standards which has implications for lapses in patient safety, including hospital acquired infections.
Comment:
One commenter stated that if accredited, an accreditation organization should be required to identify in its documentation the health and safety standards of CMS. While cost for implementation could be a concern, the proposal would guarantee that all AOs understand and support the mission and values of CMS.
Response:
We thank the commenter for feedback in support of requiring AOs to have the same language of CMS for their minimum health and safety standards, to ensure facilities which are deemed by a CMS-approved AO understand the CMS requirements. We also appreciate the cost concerns raised by the commenter, however we do note that we will continue to allow for AOs to exceed our standards, whereas we believe many AOs will continue to keep some of their existing standards, demonstrating that their standards are more stringent than CMS'.
Comment:
One commenter agreed with the intent of the proposal, stating that this would ensure that all accredited facilities meet a baseline level of quality and safety, align with the CMS regulations, and facilitate oversight. While the commenter agreed that the proposals are intended to enhance the quality and safety of healthcare delivery, they also present challenges for operational flexibility and innovation for AOs. Specifically, the commenter stated the requirement for use of same standards may limit the ability of AOs to innovate or tailor their standards to specific healthcare delivery contexts and the requirement to define additional standards separately when seeking CMS approval could potentially slow the process for updating or introducing new standards.
Response:
We appreciate the concerns raised by the commenter. The proposed provisions surrounding the crosswalk and AOs use of the Medicare standards as the minimum health and safety standard language does not prohibit an AO from further expanding or having higher/more stringent standards. As outlined, an AO may still have additional standards. However, this provision aims to reduce the inconsistency or challenges determining the comparability of an AO's health and safety standards. This provision would also increase greater understanding for healthcare organizations seeking deeming status through an AO with respect to the requirements of the Medicare conditions. Further, we note that AOs are currently required to submit any changes to their standards for any deemed program to CMS for review and approval, therefore this proposal would not add complexity or slow processes for AOs implementation of more stringent standards. As part of the application review process, when CMS imposes new health and safety standards; or when an AO proposes to add or revise additional standards, CMS reviews the standards crosswalks to ensure AOs more stringent additional requirements do not conflict with the intent of the Medicare conditions. These provisions do not prohibit AOs from continuing to exceed or tailor their standards to specific healthcare delivery contexts.
Comment:
One commenter, while generally supportive of the requirement, also encouraged CMS to consider how the proposed changes will affect hospitals and health systems that rely on the AO accreditation process to demonstrate their compliance with the Medicare conditions.
Response:
We appreciate the commenter's general support for our proposal and for raising concerns related to the impact to healthcare systems themselves, which rely on the AOs' accreditation process to demonstrate their compliance with Medicare CoPs. We believe the proposal to require AOs use of the same standard language as our CoPs as their minimum health and safety standards will benefit healthcare facilities in understanding the Medicare requirements and reduce the inconsistencies between SA and AO surveys. AOs will continue to be allowed to exceed the Medicare standards; however, AOs will need to provide education for facilities and surveyors to clearly understand the intent of the Medicare requirements.
Comment:
We received one comment challenging the assumption that a causal relationship exists between how an AO's standards are written and the issues an accredited facility may encounter in demonstrating that it is in compliance with the Medicare regulations. The commenter stated that the concept of “comparability” has been the mainstay of aligning AO standards and survey processes between AOs and that of CMS. The commenter stated that the proposal to change the language to be identical would impose a
( printed page 36419)
tremendous administrative burden by not only requiring the standards to be re-written, but in many cases the nomenclature used by an AO in organizing their standards would need to be revised. The commenter suggested this proposal creates a hardship for accredited providers and suppliers who are familiar with the terms of their accreditation manuals.
Response:
We appreciate the commenter's concern related to the proposal to require AOs to use the same Medicare language as their minimum health and safety standard and the potential administrative burden, to include revising the AO's individual classification system (AO standard numbers) to these standards. While we appreciate the concern, we believe AOs may simply add an additional area for its individual classification system to each corresponding standard and incorporate the CoP language or adjust current language within their current standards to include the minimum CoP language, as provided in the example within the impact section of this rule. For many years, CMS has continuously needed to request changes to the AOs standards based on our review for comparability during the application processes before it could grant or renew deeming authority. Often, language in an AO manual was missing key elements of the Medicare requirement or missing the intent of the regulatory requirement. While we recognize the potential administrative burden associated, we also believe that alignment of this language will ensure healthcare facilities deemed by AOs understand the CMS minimum health and safety requirements.
Comment:
One commenter questioned how CMS intends to administer this requirement when CMS does not have infection control standards for each program. The commenter stated the proposal was unclear about whether CMS would consider an AO's adaptation or implementation of the SOM and corresponding appendices as meeting this requirement. The commenter questioned if AO surveyors are provided access to these resources and educated their surveyors on the CMS guidance, will CMS consider this acceptable, or would CMS require AOs to recreate the documents for use in its programs. Finally, this commenter stated the requirements to use verbatim standards and processes appear to be viewing AOs as contractors without any differentiation or innovation, instead of independent organizations.
Response:
We appreciate the commenter's request for additional clarification. The intent of the requirement for AOs to use the language of Medicare requirements as their minimum health and safety standards is intended to reduce confusion among the provider/supplier community and ensure consistency. While CMS may not have infection control conditions for each provider type at this time, this does not restrict AOs from having additional standards where CMS has none. CMS is not requiring an AO to adopt the SOM and appendices. AOs may choose to fully adopt the Medicare standards and SOM/appendices for its deemed organizations, or the AO may use the minimum standards and exceed Medicare minimum requirements with additional standards. We refer the commenter to the survey process comparability section for additional context. Finally, the provision we are finalizing is not intended to reduce an AOs innovation, but rather to ensure consistency in the understanding of the Medicare conditions by both deemed and non-deemed organizations participating in the Medicare program.
Comment:
One commenter stated that it was unclear on the proposal to require the crosswalk as the existing regulatory language at § 488.5(a)(3) already requires a detailed crosswalk. The commenter stated that in addition to this crosswalk, CMS currently also receives a copy of the AO standards, which include the CMS regulatory references for each applicable standard.
Response:
We agree with the commenter that the requirement for AOs to provide a crosswalk and the copy of its standards is already required. However, we are finalizing provisions to require AOs also use the same language as our Medicare standards as their minimum health and safety standards for deemed programs. Therefore, as outlined and explained, AOs would need to submit a crosswalk which clearly identifies the one-to-one use of the Medicare standards, then further delineate any additional standards which may exceed the Medicare conditions.
Final Decision:
We appreciate all commenters who have provided input on this proposed revision requiring AOs to use the same language for their minimum health and safety standards. We agree with the commenters who have stated that this alignment would bring greater understanding to facilities and reduce confusion among the provider community. After consideration of the comments, we are finalizing this proposal with minor modifications to the proposed language for clarity. AOs would be required to revise their deeming standards to use the same language as the Medicare conditions; however, AOs will still be able to exceed the baseline language of the conditions with additional standards. AOs will be required to submit a revised crosswalk as part of the CMS-application review process using the template provided in this final rule with comment period.
However, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the regulations text stating “[DATE 1 YEAR AFTER THE EFFECTIVE DATE OF THE FINAL RULE]”. We are making this modification for the final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date and individual provisions will no longer need to be specified in the regulatory text.
M. Strengthen the Comparability of the Survey Process Between the AOs and the States
An AO must demonstrate to CMS that it has the ability to effectively evaluate a healthcare facility's compliance with the Medicare conditions using survey processes that are comparable to those survey methods, procedures, and forms required by CMS and as implemented by the SAs. A general description of SA survey processes is set out at § 488.26 and specified in the SOM.
As part of the application process as set out at § 488.5, CMS is required to complete a survey process review as part of the AO application review process. The purpose of the survey processes review is to determine whether the AO's survey processes are comparable to the CMS survey processes. The survey process comparability review is done by reviewing information in the application, such as, the AO's survey activity guides, organizational procedures for surveyors, surveyor training materials and AO survey requirements. CMS also conducts an in-person observation of an AO survey (carried out by a CMS survey observation team) as part of CMS' review of an AO's application. The purpose of the survey observation is to ensure that the AO surveyors follow the processes set out in the application and to ensure that the AO surveyors evaluate all Medicare requirements.
Sections 1865(a)(1) and 1865(a)(2) of the Act require us, when making this finding, to consider a national AO's “survey procedures” and “. . . its ability to provide adequate resources for conducting required surveys and
( printed page 36420)
supplying information for use in enforcement activities, its monitoring procedures for provider entities found out of compliance with the conditions or requirements. . . .” Our longstanding requirements at § 488.4(a)(3) implemented this statutory provision by requiring AOs to provide us with detailed information on their survey processes, and our regulations at § 488.5 and § 488.8 set out the procedures for comparability review. We further discussed AO survey procedures' comparability to our SA survey processes and the SOM in the May 22, 2015 final rule published in the
Federal Register
, entitled “Medicare and Medicaid Programs: Revisions to Deeming Authority Survey, Certification, and Enforcement Procedures” (80 FR 29796) (hereinafter referred to as the “2015 AO final rule”). We assess comparability by reviewing the information in the AO's application in light of the SOM survey process requirements for SAs, which implements the survey process requirements found in parts 488 and 489 of our regulations. The role of the SOM is to provide explicit guidance on the process to assess providers' and suppliers' compliance with our regulatory requirements. We do however note, that the AOs are already required to submit the documentation and that most AOs provide this within their applications, therefore we do not believe this imposes any additional burden, as this has been a long-standing expectation as described in the preamble of the proposed rule (89 FR 11996) and the 2015 AO final rule (80 FR 29796), which stated that while the explicit reference to the SOM was removed, “this will not change our practice of assessing comparability in light of the SOM survey process requirements for SAs, which implement survey process requirements found in parts 488 and 489 of our regulations governing certification and provider agreements”.
As previously noted, CMS received 22 AO applications between January 2017 and August 2021. Of those 22 applications, 14 were returned to the AO for revisions to the AO's survey processes and policies, as distinguished from the finding that all 22 AO's standards were not initially comparable with the Medicare conditions. These required survey process revisions included ensuring all surveys were unannounced in accordance with § 488.5(a)(1)(i), which we discussed in section IV.A. of the proposed rule. Other applications were returned for inconsistencies with our patient or representative complaint processing guidance set out in Chapter 5 of the SOM. Additionally, among these 22 applications, we identified concerns within the AO survey processes during the on-site survey observations, as authorized under § 488.8(h). The following concerns were noted during the survey observations for these 22 applications:
The survey citations and rationales for citing or not citing “Governing Body” Medicare condition violations (for example,42 CFR 482.12) were inconsistent with CMS' SA survey methodologies;
The AO failed to enforce the deadlines by which facilities must come into compliance after receiving adverse survey results;
The AO utilized timeframe(s) that were inconsistent with those of state SAs, such as deadlines for conducting follow-up activities, including follow-up surveys, for facilities that have previously demonstrated non-compliance at the condition-level; and
The AO didn't conduct a sufficient number of medical records reviews during a survey. (CMS expects that AO surveyors review a specific number of medical records, based on the facilities' patient volume, to ensure that the surveyor has an accurate picture of patient care services provided within the facility).
CMS also has longstanding concerns about the performance of AOs, including the failures of AOs to conduct in-depth investigations; the lack of consistency and comparability with CMS standards; and the repeated requests for AOs to resubmit applications with conforming corrections in survey standards and processes. We also have continued concerns about the excessive frequency of disparate findings between AOs and SAs (see section IV.I. of the proposed rule) and AOs' consistent failure to review medical records, as required by SA procedures. All of these endemic issues strengthen our resolve to ensure consistency in AO performance. Our initial and renewal application reviews are the foundation for our oversight of AOs to determine the AO's ability to ensure facilities adhere to minimum Medicare conditions.
Because of these disparities, we proposed to strengthen our requirements under § 488.5. The proposed requirements would require AOs that accredit Medicare-certified providers and suppliers to use a survey process that is comparable to the survey processes and procedures used by CMS and the SA. We note that this has been the expectation under the existing requirements, as a condition of obtaining and retaining deeming authority. We proposed to increase the specificity of our application and reapplication requirements for national AOs to improve documentation that would demonstrate this comparability.
We received a total of 25 comments on the proposal to strengthen survey process comparability. We note, the majority of comments responded generally to the proposed provisions under section IV.F instead of separate comments for each of § 488.5(a)(4); § 488.5(a)(4)(iii); § 488.5(a)(4)(v); § 488.5(a)(4)(vii); § 488.5(a)(4)(xi); § 488.5(a)(5); § 488.5(a)(6); § 488.5(a)(12); § 488.5(a)(13).
Comment:
We received several comments generally supportive of our proposal to increase comparability of survey processes among AOs and SAs. One commenter suggested that combined with our proposal for use of the same standards, this would enable comparability of the survey process across facilities that are all required to adhere to the same standards for Medicare reimbursement. Another commenter suggested that in conjunction with our proposal for AOs to use the same minimum health and safety standards, that this would thereby strengthen and improve consistency in the survey processes of AOs and SAs and improve the transparency of accreditation surveys and reduce confusion among providers. One commenter also stated our proposals around survey comparability will achieve efficiencies and benefit all interested parties as well as the surveying entities. The commenter implied that this proposal in conjunction with our proposal to apply consistent basic training for AOs and SAs would increase accuracy and cross-agency consistency of survey findings. One commenter also provided general support and stated that these proposed provisions would help improve alignment and ensure AOs conduct their work in a consistent manner.
Response:
We thank all the commenters in support of our proposed provisions to strengthen survey comparability between the AOs and SAs. We agree with the commenters and believe these provisions will work to provide greater clarity for Medicare-participating providers currently deemed by a CMS-approved AO. These proposals are intended to align survey processes for consistency, while not limiting an AO from exceeding our requirements.
Comment:
We received one comment stating that providers have long reported and continue to report inconsistency in
( printed page 36421)
understanding, interpretation and application of not only the Medicare conditions, but also the survey processes between SAs and AOs. The commenter supported our efforts for strengthening survey process comparability.
Response:
We appreciate the commenter's support of our proposals and agree that these provisions will work to strengthen comparability and understanding of the SA and AO survey processes.
Comment:
Two commenters, while generally supportive of all proposed provisions, urged CMS to consider how the proposed changes will affect hospitals and health systems that rely on the AO accreditation processes to demonstrate their compliance with the Medicare conditions. The commenters were in support of CMS proposals to ensure more consistency between AOs and the SA surveyors.
Response:
We appreciate the commenters' support for our proposals to strengthen survey comparability and provide greater consistency among the AOs and SAs. We appreciate the commenters' concerns related to the impact to healthcare systems themselves, which rely on the AOs accreditation process to demonstrate their compliance with Medicare. We note, the proposals surrounding AOs strengthened survey process comparability will be a benefit for healthcare facilities in understanding the Medicare requirements and reducing the inconsistencies between surveys of deemed and non-deemed facilities.
Comment:
One commenter suggested that our proposals for strengthened survey process comparability is a welcome step in promoting consistency and effectiveness. The commenter also encouraged sharing of data among SAs and AOs to improve outcomes, understand processes, and foster a culture of collaboration.
Response:
We appreciate the commenter's support and agree with the need to further collaborate and share information among SAs and AOs. We believe these proposals will first provide clarity and alignment of processes to bridge the gap of inconsistencies.
Comment:
One commenter provided support for the proposed provisions set forth in § 488.5(a)(4) to (13), as such provisions pertain to strengthened comparability for survey processes. The commenter specifically noted the importance of maximum documentation, transparency, and accountability within the accreditation process.
Response:
We appreciate the commenter's support.
Comment:
One commenter also requested that CMS consider proposals to strengthen comparability among the SAs. The commenter's experience with providers and health systems spanning across multiple States; the commenter implied that there were inconsistencies among SAs. The commenter also suggested that CMS consider proposing that all complaints related to a certified provider, including those deemed by a CMS-approved AO, should be followed up on by the SAs. The commenter suggested that AOs vary in response time and follow up, and that SAs could be relied on to respond quickly. The commenter stated that this approach would ensure a uniform complaint follow up process.
Response:
We appreciate the commenter's general support for our provisions for strengthening comparability among AOs and SAs. The proposed provisions are aimed to achieve consistency among SAs and AOs. CMS expects SAs to follow the guidance set forth in the SOM and applicable program appendices. In addition, AOs are expected to have comparable complaint processes to those of the SAs, and as outlined in Chapter 5 of the SOM. We appreciate the commenter's recommendation for complaints to be conducted by the SAs for all Medicare-participating facilities; however, these recommendations are outside of the scope of this proposed rule. CMS is continuing to review our survey processes and the complaint procedures across SAs and AOs.
Comment:
One commenter, in support of strengthening comparability, stated that the additional efforts CMS has proposed would further improve the survey process and ensure such surveys reliably identify lapses in patient safety and opportunities for improving strategies that strengthen the delivery of care. The commenter specifically referenced the prevention and reduction of healthcare-associated infections (HAIs) including the Centers for Disease Control and Prevention (CDC) 2022 National and State HAI Progress Report.[12]
The commenter noted that the resources of the commenter's organization are translated from research based on proven science-based methods. The commenter stated that its resources are often used by facilities and the policies help to meet or exceed the quality-of-care standards set forth by CMS and AOs.
Response:
We agree with the commenter that HAIs are a top priority, and we appreciate the commenter's organization providing valuable resources to healthcare facilities to combat HAIs. The proposed provisions do not aim to limit AOs from meeting or exceeding our standards and are designed to strengthen survey processes among SAs and AOs, including the identification of infection control deficiencies within facilities. The provisions also do not restrict healthcare facilities from using resources by any healthcare industry or organization to exceed CMS' minimum health and safety standards and strive for increased patient safety as it relates to infection prevention. Again, we appreciate the support of the strengthened survey comparability proposals between AOs and SAs.
Comment:
One commenter stated that its client facilities are generally supportive of the proposals, and the organization has already taken actions to align survey processes, such as survey process documentation, and creation of policies regarding the composition and number of survey teams. However, the commenter urged CMS to consider that cumulatively, these proposed provisions represent a change in requirements and will have significant cost burden, including staff burden, if implemented.
Response:
We appreciate the commenter's general support of the provisions and CMS recognizes the potential burden which may be associated with some of our proposals. Regarding strengthening survey comparability among SAs and AOs, as outlined in the impact section, we believe this is not a significant burden, as the provisions primarily aim to clarify existing requirements which AOs already provide as part of the application process for deeming authority. The survey process comparability aims to ensure CMS can see critical elements of the AOs survey processes, such as the surveyor probes and questions as part of the investigation. We thank the commenter for the support and the organization's current efforts to align with these provisions.
Comment:
One commenter agreed with the proposed provisions and clarifications that all AOs must use a survey process comparable to those processes set out in the SOM, yet implied that the reasoning provided in our proposed rule creates confusion as to what the actual requirement is for the definition of “comparable.” The commenter stated it was unable to determine if CMS is presenting comparability as sameness, meeting, or exceeding. The commenter also
( printed page 36422)
requested clarification from CMS on describing how the processes logically work together in a manner that does not provide confusion to the public and deemed facilities, and that a thorough understanding of the requirements is essential for AO compliance.
Response:
We appreciate the commenter's concerns related to the meaning of comparability, in particular the proposals surrounding survey process comparability. Of note, as explained in the preamble of the proposed rule, CMS' proposed provisions for survey processes are to clarify many already existing requirements with specific focus on areas of the application review processes where CMS has found deficient practices in the AOs' survey processes. The proposed provisions related to the survey process would not require the same language as the survey processes found in the SOM, nor would the proposals restrict AOs from exceeding certain survey processes. In this final rule with comment period we are clarifying existing requirements, such as requiring an AO to provide survey protocols (such as interview questions), which are transparent to the public as outlined in the SOM yet have not always been present within an AOs initial application or reapplication for deeming authority. SAs are guided to specific survey questions when performing reviews of the CoPs, however CMS has found that AO applications over the years and survey processes for evaluation of the CoPs do not always include interview probes for surveyors. Additionally, in our review of AO survey processes over the years, we also identified instances where AOs were conducting off-site complaint investigations, which are not permitted for acute and continuing care providers per the guidance in Chapter 5 of the SOM; therefore, these investigations were not comparable to the processes of the SA. CMS believes by strengthening the language, greater comparability between SAs and AOs will be achieved. Sameness would imply requiring the same exact language and process, which is not our intent under our comparability requirement. Our intent is to ensure that AOs will continue to have flexibilities in survey approaches, while providing clarity as to what information will be required in our review of AOs applying for deeming authority to ensure that AOs are meeting or exceeding the intent behind evaluating deemed facilities against the Medicare requirements. Survey process may still be exceeded by an AO, such as requiring more than CMS requires for review of medical records or evaluation of AO-specific standards which exceed our minimum health and safety requirements.
Comment:
One commenter, while appreciating our intent to strengthen comparability, also noted CMS provides a current checklist for application documentation for submission to CMS for initial and continued approval of the AOs deeming program. The commenter stated that it is left to the individual AO to determine how to package the information and suggests CMS consider a more efficient and organized approach to reduce redundancy, while also easing the burden on CMS. The commenter suggested CMS consider development and adoption of a standardized operating procedure, to include application templates, enabling AOs to respond directly to requirements.
Response:
We appreciate the commenter's suggestion for CMS to provide an application template for those AOs seeking deeming authority. As noted by the commenter, CMS provides AOs with a checklist for the application documentation requirements outlining the requirements at§ 488.5, however we have not specifically identified a format as CMS has provided flexibilities to AOs. For instance, one AO may provide all documentation in a large zip-file, while other AOs may submit documentation in separate files corresponding to each required element in § 488.5. We will review the application process to determine if there are opportunities for more streamlined submissions, and if appropriate, present any changes in subregulatory and policy guidance.
Comment:
CMS received one comment raising concern. The commenter stated that current inconsistencies among SAs from State to State suggest that CMS should focus on establishing consistency among SAs prior to moving to AOs. The commenter also raised concerns that CMS may not be sufficiently coordinating the investigative efforts among AOs and SAs and recommended removal of duplicative complaint survey activity among the two surveying entities.
Response:
We appreciate the commenter's recommendations and CMS remains committed to achieving consistency among the SAs.
Final Decision:
We appreciate the commenters who supported our proposal to strengthen the comparability of survey processes among SAs and AOs. We also recognize that some of the commenter's raised concerns on establishing consistency among the SAs as well. Based on our review of the comments received, we are finalizing this proposal without changes. We note, AOs will be provided with additional guidance by CMS when submitting their applications for initial or continued CMS-approval of their deeming programs.
N. Revise the AO Application Documentation Requirements Related to the Survey Processes
(§ 488.5(a)(4); § 488.5(a)(4)(iii); § 488.5(a)(4)(v); § 488.5(a)(4)(vii); § 488.5(a)(4)(xi); § 488.5(a)(5); § 488.5(a)(6); § 488.5(a)(12); § 488.5(a)(13))
To achieve our goal to require the AOs to use a survey process that is comparable to that used by CMS and the SAs (and in alignment with our proposal at § 488.4(a)(2) regarding comparable survey processes), we proposed the following revisions and additions to the existing AO application regulation requirements.
1. Revisions to § 488.5(a)(4) (Description of Survey Process)
At § 488.5(a)(4), we proposed to add language which includes what we believe to be the core fundamental activities of the survey process, such as pre survey preparation; offsite preparation; entrance interview and activities; information gathering and investigation, analysis of information; exit conference; post-survey activities; and statement of deficiencies-related activities. These are processes used by the SA which are needed to ensure that a Medicare-participating provider or supplier receives an unbiased, independent survey.
We have observed, both in our on-site observation of AOs during the existing process set out at § 488.8(h), as well as during the Validation Redesign Program (VRP) pilot conducted 2018 through 2019, that AOs often provided daily briefings to and had frequent discussions with the management of the surveyed facility whose purpose was not clearly described in the AO's applications. We noted that these meetings with facility management impeded or did not allow for sufficient time for the survey team to complete core survey activities, such as direct observations or interviews, in turn failing to complete a thorough review of the organization's compliance. Time spent to have casual briefings or meetings with facility management could have rather been spent to evaluate the facility's compliance with the Medicare requirements.
Therefore, the proposal to add the core activities, as well as the revisions outlined in this section, would further strengthen comparability between SAs and AOs, while continuing to allow for
( printed page 36423)
flexibilities in the survey processes used by AOs. However, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the regulations text stating “[DATE 1 YEAR AFTER THE EFFECTIVE DATE OF THE FINAL RULE]”. We are making this modification for this final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date and individual provisions will no longer need to be specified in the regulatory text.
The comments and our responses are set forth in section III.M. of this final rule with comment period.
2. Revisions to § 488.5(a)(4)(iii) (Documentation of Surveyor Forms and Guidance)
Section 488.5(a)(4)(iii) currently requires that AOs applying for deeming authority provide, among other documentation, copies of the organization's survey forms, guidelines and instructions to surveyors. We proposed to be more specific about the level of detail we require from the survey instructions and guidance the AO provides to us when seeking our approval. Specifically, we proposed to require detailed information regarding how the AO surveys for facility compliance with the following core activities or standards within the Medicare conditions, such as: Governing Body; Patient Rights; Emergency Preparedness; Quality Assessment and Performance Improvement; Medical Staff; Nursing Services; Medical Records Services; and Infection Control. These core activities and standards are part of every State survey and based on Medicare conditions. With respect to each of these survey subject areas, we would require the applying AO to provide documentation on the instructions it provides for surveying these Medicare conditions, including survey probes, interview questions, and methods for their own review of facility documentation pertaining to these Medicare conditions.
It has become evident through our validation and comparability reviews of AOs that the documentation we currently request from them no longer suffices to adequately determine whether the AO surveyors are investigating these Medicare conditions sufficiently to ensure the health and safety of Medicare beneficiaries and other patients. AOs have failed to survey adequately for facility compliance with their respective documentation requirements, including specific standards or survey processes. We also proposed that AOs submit their patient and staff interview questions. By having access to these questionnaires, we would be able to determine whether there are gaps in the survey processes which are leading to the disparity findings, as we have seen in our validation surveys.
Comment:
One commenter was unclear about the proposal and the identified “core activities” and inquired whether the detailed information will only be required for the aforementioned areas (for example, governing body, emergency preparedness, etc.).
Response:
We appreciate the commenter's concerns relating to clarity of this proposed provision. As noted previously, some AO applications have lacked information on surveyor interview questions, protocols, or probes, as outlined in the SOM. The intent of this proposed provision was for AOs to provide surveyor guidance and interview questions comparable to those of the SOM for all Medicare conditions. While AOs have flexibilities in the format, and we are not requiring the same exact questions or surveyor probes, information provided should ensure assessment of the facility's compliance with requirements is consistent with our expectations of the States, ranging from entrance activities, to opening conferences, to interview and documentation reviews and exit conferences with the facilities. We will provide AOs with additional guidance during their initial or continued applications for CMS-approval of their deemed programs.
Final Decision:
As outlined in section III.K. of this final rule with comment period, we are finalizing this provision without any changes.
O. Revisions to § 488.5(a)(4)(v) (Survey Review Process)
At § 488.5(a)(4)(v), we proposed to add additional areas clarifying and strengthening the requirement that AOs provide a description of their document review processes in their approval applications. We proposed to add that AOs must describe processes and surveyor procedures related to the review of medical records, medical staff credentialing procedures; personnel files (including staff competency); and the number of patient observations, patient interviews and staff and facility interviews.
We have noticed that many AOs fail to review adequate numbers of records for the provider/supplier type involved. In the review of the 22 AO applications received between 2017 and September 2021, a total of nine AOs were identified to have not reviewed the adequate number or records. Additionally, we have observed that some AO survey practices, such as interviewing patients in non-confidential settings, and deficient complaint investigations, undermine the integrity and accuracy of AO surveys. We are concerned that staff or patients may not be honest and candid if another facility staff member or supervisor is present during interviews. The expectations are that interviews are conducted privately with staff. For example, in Appendix A of the SOM, we explicitly require surveyors to “Explain that all interviews will be conducted privately with patients, staff, and visitors, unless requested otherwise by the interviewee.” Privacy in interviews with staff is important and encourages the likelihood of honest feedback about an organization. Additionally, we also identified a few instances (three of 22 applications) during our survey observations of AOs onsite, in which the AO did not observe actual performance of medication administration, wound care, or other services provided by the accredited facility, and most observations within the hospital setting were surgical time-outs (part of the Universal Protocol and performed in the operating room, immediately before the planned procedure is initiated). In one instance, the AO failed to ask the facility for any patient/representative complaint information, which indicates that the AO failed to conduct any investigation as to how the facility manages complaints and grievances. These specific examples raise concerns that the AO survey process does not sufficiently ensure safe practices for patients.
Furthermore, as noted in our discussion of proposed § 488.5(a)(4)(iii), we have also identified multiple instances in which the AOs have conducted limited review of facilities' staff credentialing and competency testing activities. For instance, in one survey observation, we observed that the AO reviewed the personnel files of only one licensed practical nurse (LPN) and one phlebotomist, and did not review any personnel files for RNs, pharmacists, or dietitians, as outlined in Appendix A of the SOM, which we consider to be critical staff for this provider setting. In another survey, the AO determined that nursing staff were not documenting chains of custody of narcotic medications but failed to review the facility's pharmaceutical policies and procedures and conducted
( printed page 36424)
no interviews of pharmacy staff. In such circumstances where a category of documentation was missing from the facility's record, we would mandate that the AO or SA conduct further investigations to determine the reason for the lapse.
The comments and our responses to the comments are set forth in IV.E. of this final rule with comment period.
P. Revision to § 488.5(a)(4)(vii) (Correction of Identified Non-Compliance)
At § 488.5(a)(4)(vii), we proposed to add additional language to the existing requirement that the AO must provide us with descriptions of their procedures and timelines for monitoring the provider's or supplier's correction of identified non-compliance with the accreditation program's standards. We believe this requirement is not specific enough for enforcement; we have regularly had to request revisions of documents submitted by AOs during our review of applications and re-applications over the years. We proposed to clarify this language by adding the requirement that AOs must also include documentation related to dates established by the AO and how those accreditation dates are determined by the AO when deficiencies may be found during initial and reaccreditation surveys, as well as the AOs process for accreditation decisions based on survey findings. We also proposed to require the AOs to provide as part of this standard, their investigative and organizational process which the AO uses to make determinations on accreditation or the removal of accreditation and recommendation to the Survey Operations Group (based out of the various CMS Survey and Enforcement Division Locations) to remove deemed status of the non-compliant facility. We also proposed additional changes at § 488.5(a)(4)(viii) and refer readers to section IV.G., “Proposal to Require AOs to Provide CMS with Survey Findings”, of the proposed rule.
The comments and our responses to the comments are set forth in section IV.E. of this final rule with comment period.
Q. Revisions to § 488.5(a)(4)(xi) (AO Training and Education Programs)
At § 488.5(a)(4)(xi), we proposed to add a new requirement to require AOs to provide CMS with documentation summarizing their staff training programs, whether web-based or via methods such as Power Point presentations or hard-copy materials, which would provide an overview of how they train surveyors to follow their survey processes, and, where applicable, highlight differences from CMS survey processes. Currently, CMS receives limited training materials that the AO provides to its surveyors; therefore, when conducting survey observations as under our authority at § 488.8(h), it is often challenging to understand differences in survey processes. We may receive an AO's printed materials for training and/or downloaded versions of electronic surveyor training platforms; however, these materials vary. These materials indicate that some AOs collect employees' oral evidence for a survey, as opposed to a more document-focused review done by the SAs. AOs' applications do not always provide us with the entire scope of surveyor education the AO provides to its surveyors, therefore limiting the scope of our review of comparability. The current regulation at § 488.5(a)(8) only requires the AO to give us “[a] description of the content and frequency of the organization's in-service training it provides to survey personnel.” CMS frequently asks AOs to submit additional training and education materials during the application review processes. Reviewing the AOs' staff training programs and documentation as outlined in the proposal will provide CMS with greater enforcement capabilities and allow CMS to better assess the AOs' consistency in training against those of required by the SAs. Additionally, because we review AO applications for comparability to CMS survey processes, this additional information would be invaluable to CMS' increased understanding of the AOs' survey processes prior to conducting a survey or during the validation or proposed direct observation process, as discussed in sections II.D. and IV.K.3. of the proposed rule.
The comments and our responses to the comments are set forth in section IV.E. of this final rule with comment period.
R. Revisions to § 488.5(a)(5) (Composition of Survey Team)
At § 488.5(a)(5), we proposed to add requirements which describe the AOs' minimum criteria for determining the size and composition of survey teams for the facilities they accredit. We proposed to require the AO to provide us with documentation describing the criteria or process by which the AOs determines the makeup of their survey teams, based on: (1) the size of the facility to be surveyed, based on average daily census; (2) the complexity of services offered, including outpatient services; (3) the type of survey to be conducted; (4) whether the facility has special care units or off-site clinics or locations; (5) whether the facility has a historical pattern of serious deficiencies or complaints; and, (6) whether new surveyors are to accompany a team as part of their training.
Our on-site survey observation of AO surveyors has found some concerning practices. For example, some AOs use time limits on the length of their investigations, which can limit the depth and accuracy of the investigation. One AO only permitted themselves a 2-day period in which to conduct a survey of a CAH, whereas the policy of the SA is based on the scope of services provided by the provider, type of survey to be conducted, complexity of services offered and whether the facility has off-site locations. The AO's policies did not allow for flexibility to have the survey exceed 2 days, which may not be enough to allow for all departments to be surveyed, or in the event of an immediate jeopardy or condition-level non-compliance finding, for a closer investigation to be conducted. While fortunately no condition-level non-compliance was identified in that instance, the strict AO policy on timeframe of survey conflicts with our intent for AOs to thoroughly complete the investigative process and did not allow for flexibility in survey length. It appears based on this example that at least one AO may not be giving consideration to the size and number of outpatient departments or provider-based locations per facility and the need to investigate immediate jeopardy or condition-level non-compliance when deciding on time limits for surveys. Additionally, some AOs have not always ensured surveys are conducted on all off-site locations that are still certified under the main campus or facility CCN as is required for SAs in accordance with Appendix A of the SOM—Survey Protocol, Regulations and Interpretive Guidelines for Hospitals, Survey Protocol, Task 3 (“Information Gathering/Investigation”).[13]
Clarifying these minimum expectations would help AOs meet Medicare conditions and create more consistency between the approaches used by AOs and the SAs.
Comment:
The commenter requested clarification. The commenter stated, specifically for CAHs, surveys are usually assigned to a single clinical surveyor for 2 to 3 days yet suggested our proposed provisions would limit
( printed page 36425)
survey composition to only registered nurses (RNs).
Response:
We appreciate the commenter's concern. We proposed to require AOs to be able to provide clear criteria by which the AOs determine the makeup of their survey teams. CMS made note that during observations, some surveyors assigned to a survey were rushed to complete survey activities due to the AOs current policies which may not have accounted for outpatient locations. Additionally, while no fault to an AO, we have observed new staff including leadership in many facilities which have not experienced a survey, where time onsite may be delayed. Our proposal was not to limit or restrict the composition, but rather to ensure that the survey team or surveyor is adequately prepared, can complete the investigative process of a survey, and has flexibility in survey length. CMS is not prohibiting AOs from using physicians as part of the survey teams when surveying CAHs or other providers for compliance. However, we do note that Appendix A and Appendix W of the SOM requires that when a survey calls for one clinical surveyor which must be a registered nurse (RN), that use of a physician in lieu of an RN would not be comparable, as the evaluation of nursing services is specific to an RN role. We would expect that AO surveyor team composition rules meet our minimum requirements and are comparable to those of the SA.
Final Decision:
As set forth in section IV.E. of this final rule with comment period, we are finalizing this proposal without revision, with the exception of the modification as outlined below. AOs will be expected to have comparable survey team composition as outlined within our SOM Appendices.
However, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the applicable regulations text stating that a particular provision(s) will become applicable 1 year after the effective date of the final rule with comment period, or any similar language to that effect. We are making this modification for the final rule with comment period since we have decided that all provisions of the rule will become effective 1 (one) year after the publication date and individual provisions will no longer need to be specified in the regulations text.
S. Revisions to § 488.5(a)(6) (Adequate Number of Surveyors for Size of Facility)
At § 488.5(a)(6), we proposed to add language to the existing requirement that requires the AO to provide documentation demonstrating the overall adequacy of the number of the organization's surveyors, including how the organization will increase the size of the overall survey staff to match growth in the number of accredited facilities while maintaining regular re-accreditation intervals for existing accredited facilities. We proposed to add language demonstrating that the AO has enough surveyors to ensure that it can complete all survey activities within the time allotted.
Through our direct observations as part of the application process, we identified several instances in which the scope of document reviews was limited and the content of medical records was not thoroughly reviewed, because it seems the AO surveyors did not have enough time to review records. This may be a systemic issue across AOs.
The comments and our responses to the comments are set forth in section IV.E. of this final rule with comment period.
T. Revisions to § 488.5(a)(12) (Complaint Survey Documentation Requirements)
At § 488.5(a)(12), we proposed to add additional elements critical to the AOs' effective investigation of complaints about their client facilities. Specifically, we proposed that the AO in its application documents for CMS approval of its deeming authority would also have to include: (1) a description of its process for triaging and categorizing complaints about the surveyed facility; (2) timeframes for responding to complaints and a method to track and trend complaints (for example, frequency of similar complaints, complaint type, etc.) received with respect to the AOs accredited facilities; (3) procedures and persons responsible for the review of plans of corrections; and procedures for follow up if the plans of corrections are not adequate; (4) AO requirements for plans of corrections for standard level deficiencies; (5) follow up survey procedures and monitoring of condition-level findings; (6) procedures for addressing immediate jeopardy deficiencies; and (7) sharing of previous deficiency findings or complaints with survey teams. The existing regulatory requirement for the AO to provide procedures for responding to, and investigating, complaints against accredited facilities, including policies and procedures regarding referrals is insufficient. Of our 19 AO initial and renewal applications received over the last several years, CMS has requested additional AO documentation for this particular standard to adequately assess the comparability of survey processes. Strengthening the language will bring greater clarity as to the expectations for documents to the AO submitting an initial or renewal application.
Comment:
One commenter stated that AOs currently already provide documentation related to complaints. The commenter suggested that the proposed rule for this section was unclear as it discussed complaints and also discussed overall survey process policies. The commenter questioned if the intent is to provide CMS with these policies only if they are related to complaint investigations.
Response:
We appreciate the commenter's request for additional clarification. Section E. of the proposed rule specifically aims to address overall survey comparability among the SAs and AOs. When discussing survey processes this includes complaint investigations and an assessment of AOs to ensure that AOs have a comparable process to Chapter 5 of the SOM. We agree with the commenter that AOs currently provide the information outlined in § 488.5(a)(12) for CMS-review during the application processes. However, we have added additional context and guidance to the rule to be more specific. We believe that by providing this level of specificity within the regulation ensures new organizations seeking to become a CMS-approved AO will be knowledgeable of what CMS is requiring from them to assess comparability. We further believe this will also ensure that CMS receives this documentation with all applications, potentially reducing the number of times CMS must request further information from an AO during the 210-day application review process.
Final Decision:
As outlined in section IV.E. of this final rule with comment period, we are finalizing this provision without any changes.
U. Revisions to Accreditation Decision-Making Policies and Reporting § 488.5(a)(13)
At § 488.5(a)(13), we proposed to re-designate existing paragraph (ii) to (iii) and add two new paragraphs at (ii) and (iv). The section currently requires an AO applying or re-applying for deeming authority to provide CMS with a description of its processes for accreditation status decision making. The proposed revision would require the AO to document its specific policies and procedures for reporting accreditation decisions to CMS, including timeframes for notification. Additionally, we proposed to require the AO to submit specific
( printed page 36426)
documentation describing how it will inform us when one of the facilities they accredit withdraws from accreditation. This communication is necessary since it alerts us that such facility will need to be surveyed by the SA next time. By requesting this additional information related to accreditation decisions made by the AOs, as well as reviewing documentation on how the AO notifies their facilities and CMS and our SAs of a facility withdrawing from the AO, CMS will strengthen the existing requirements and create a more consistent, uniform review of the AO survey process for comparability. We also believe we will be able to review the AOs' processes for reporting and identify under what circumstances an AO maintains accreditation of a facility versus the potential CMS decision to drop deeming authority by requiring this information. We have found in several instances that even after our determination of serious health and safety deficiencies in accredited facilities, and CMS' removal of the AO's deeming authority, a facility still remains nominally accredited, which may mislead the public into assuming that the facility has no health and safety concerns. When CMS provides deeming authority to an AO, the expectation is that its standards meet or exceed Medicare conditions and that surveys are comparable to those of the SAs, which may not be the case for an AO accreditation. Facilities may voluntarily end their deeming and accreditation from an AO or be involuntarily removed from deeming authority. When this occurs under the deeming process, the facility is placed under the SA's jurisdiction, meaning the SA will survey and monitor the facility for compliance with Federal requirements. Through the establishment of a more rigorous and comprehensive survey process review during the required application and renewal process, our concerns regarding insufficient compliance would be addressed. The proposed additional and revised requirements would ensure a more uniform assessment and improve our evaluation of AO performance to ensure that surveys conducted by AOs are comprehensive and fully examine all Medicare conditions. We also believe that adding these detailed documentation requirements in regulation would establish a consistent standard across all AOs and would bring uniformity and transparency to the accreditation process.
We proposed that the provisions clarifying the existing requirements to require AOs that accredit Medicare-certified providers and suppliers to provide us with more detailed descriptions of their survey processes and procedures would become applicable 1 year from the effective date of this final rule with comment period.
The comments and our responses to the comments are set forth in section IV.E. of this final rule with comment period.
V. Require AOs To Provide CMS With Survey Findings (§ 488.5(a)(4)(viii)(A))
General AO survey findings are entered into a CMS database known as the Accrediting Organization System for Storing User Recorded Experiences (ASSURE). This database collects general information about the accreditation survey, such as, date, survey findings and severity of problems indicated by the findings. It generally does not include actual survey reports. Currently AOs provide a limited set of data for surveys within the ASSURE database. We use this information in addressing administrative program elements, and in assessing AO performance. To date, we have not consistently required the AOs to submit copies of their survey reports and related information.
We proposed to modify § 488.5(a)(4)(viii) to require that AOs provide all survey reports to CMS, which would not be disclosed except under the limited circumstances permissible under subsection 1865(b) of the Act. AOs would be required to submit a statement that the organization agrees to provide CMS with a copy of all survey reports, including but not limited to, initial, re-survey, and complaint survey reports, and/or any other information related to survey activities as CMS may require (including corrective action plans) as part of its initial and renewal applications, or upon CMS request. The proposed revision to § 488.5(a)(4)(viii)(A) would expand the requirement from the current requirement that AOs provide survey reports from applicants seeking initial participation in Medicare (with other surveys only upon request). Under our proposal, we would have access to any survey reports, including initial, reaccreditation, complaint surveys, and corrective action plans that CMS may require. These reports, like those of survey agencies, would assist CMS in program analysis including tracking citations issued to accredited facilities to determine whether there is a concern with an AO's performance. Similarly, these reports would assist in reviewing disparate findings in which the SA may have cited a deficiency within an accredited facility that the AO failed to recognize.
Current §§ 488.5(a)(4)(viii) and 488.5(a)(11)(ii) allow CMS to receive copies of the AOs' survey reports. However, CMS is prohibited by section 1865(b) of the Act as well as § 488.7(b) from disclosing these surveys, with the exception that CMS may disclose such a survey and related information to the extent that they are from home health agencies, or hospice programs, or pertain to an enforcement action taken by CMS. Furthermore, the stem statement of § 488.7 requires that a Medicare participating provider or supplier, in accordance with § 488.4, must authorize its respective AO to release to CMS a copy of its most current accreditation survey including corrective action plans and any information related to the survey that CMS may require.” Section 488.7(b) further provides that CMS may publicly disclose an accreditation survey and information related to the survey, upon written request, to the extent that the accreditation survey and survey information are related to an enforcement action taken by CMS.
CMS has the authority under section 1875(b) of the Act as well as regulations at § 488.8(a)(1) to evaluate the performance of the AOs through review of the organizations' survey activity. Through consistent access to AO survey findings CMS would enhance our ability to analyze survey findings and processes, identify emerging quality of care issues and patterns in AO survey findings, and, ultimately, improve care for our beneficiaries.
As the proposal for revision to § 488.5(a)(4)(viii) is being made in connection with our proposal to require the AOs that accredit Medicare-certified providers and suppliers to use the proposed revised comparable survey processes and procedures, we propose that the revisions to § 488.5(a)(4)(viii) become applicable 1 year from the effective date of this final rule with comment period.
We received two comments which are set forth below.
Comment:
One commenter raised concerns that AOs already submit survey reports to CMS and any other report is available on request of CMS, as part of the application process. The commenter also raised concern related to ability for CMS to intake, review, house and access all survey reports from the AOs.
Response:
We appreciate the commenter's note that AOs already submit survey reports for their deeming surveys when requested by the CMS. Since CMS is actively working on
( printed page 36427)
technical implementation details, as notated in the final decision, we are not finalizing the proposal to require AOs to submit all survey reports to CMS. CMS will continue to expect, as outlined in our current regulations, that AOs submit survey reports to us upon request.
Comment:
One commenter requested clarification on the intended use of the detailed reports and whether the information was necessary to be provided for all surveys.
Response:
The intent of the proposed provision for AOs to submit all survey reports was to ensure CMS access to review AO survey findings at any time. Since CMS is actively working on technical implementation details, as described in the final decision, we are not finalizing the proposal to require AOs to submit all survey reports to CMS. CMS will continue to expect, as outlined in our current regulations, that AOs submit survey reports to us upon request.
Final Decision:
As set out in our responses to the commenter's concerns, we are not finalizing the proposal to require AOs to submit all survey reports to CMS. CMS will continue to expect, as outlined in our current regulations, that AOs submit survey reports to us upon request.
W. Require That AO Surveyors Must Take the CMS Online Surveyor Basic Training (§ 488.5(a)(8))
Prior to 2006, CMS offered basic surveyor training courses in a traditional in-person classroom setting. Over time, we began providing online basic surveyor training courses for each provider and supplier type (ambulatory surgical centers (ASCs), hospitals, home health agencies (HHAs), etc.), as well as training specific to writing skills for surveyor documentation.
Basic training online courses are designed to provide surveyors with the basic knowledge and skills needed to survey the respective provider or supplier type for compliance with the Medicare conditions. The online courses also help develop and refine surveying skills, foster an understanding of the survey process, and enhance surveyors' overall ability to conduct and document surveys. Courses are self-paced web-based training. Users may access the online courses at any time and have ongoing access to the course. This affords surveyors the opportunity to refresh knowledge regarding Medicare conditions and processes whenever necessary. The numbers of learners trained in online courses have been steadily increasing since their inception.
Currently, the trainings are publicly available through the CMS Quality, Safety & Education Portal (QSEP) website at
https://qsep.cms.gov.
These trainings are free of charge for AO surveyors and the public at large.
SA surveyors are required to take CMS program-specific trainings along with SA-led orientation, field survey observations, and mentoring as part of a comprehensive training and education program to assure an adequately trained, effective surveyor workforce.
SAs may perform validation surveys on a sample of providers and suppliers (such as hospitals, CAHs, ASCs, and HHAs) accredited by the AOs. Validation surveys compare the survey findings of the AO to those of the SA to see if there are any disparities. The disparities found between an AO's surveys and an SA's surveys is used in a performance measure called the “disparity rate” and is tracked by CMS as an indication of the quality of the surveys performed by the AO as described in the proposed rule. The disparity findings between AO surveyors and SA surveyors may, in part, be attributed to differences in surveyor training and education, which varies from AO to AO, and may be inconsistent with the CMS-provided SA surveyor training discussed earlier in the proposed rule.[14]
We further believe that uniform surveyor training would increase the consistency between the results of the surveys performed by SAs and AOs and have a positive impact on the historically high disparity rates. The Fiscal Year 2020 “Report to Congress: Review of Medicare's Program Oversight of Accrediting Organizations (AOs) and the Clinical Laboratory Improvement Amendments of 1988 (CLIA) Validation Program,” [15]
showed variation in overall disparity rates, by provider type, as well as by the AO. For example, for the disparity rate from FY 2018 to FY 2019, hospitals, HHAs and ASCs had the only decreases in disparity rates of all the program types, with a 5 percentage point, 11 percentage point and 7 percentage point decrease respectively. The disparity rates for psychiatric hospitals increased by 7 percentage points from FY 2018 to FY 2019. The disparity rates for CAHs and hospices increased by 5 percentage points and 3 percentage points respectively from FY 2018 to FY 2019. On November 9, 2021, we published a final rule in the
Federal Register
, entitled, “Medicare and Medicaid Programs; CY 2022 Home Health Prospective Payment System Rate Update” (86 FR 62240). In that final rule, we finalized implementing regulations, codified at § 488.1115(a), to require AO surveyors to have successfully completed the relevant CMS-sponsored basic hospice surveyor training prior to conducting any hospice program surveys in accordance with Division CC, section 407 of the Consolidated Appropriations Act of 2021 (CAA 2021) (89 FR 62367 to 62370).
In addition to these hospice program surveyor training requirements, we proposed to amend the provision at § 488.5(a)(8) by adding new paragraphs (a)(8)(i) to (a)(8)(iv), which would impose a new training requirement on those surveyors working for AOs that accredit Medicare-certified provider and suppliers (89 FR 12019). We noted that we had previously made a similar proposal in the calendar year (CY) 2019 Home Health Prospective Payment System Rate Update proposed rule (83 FR 32470, July 12, 2018). However, we did not finalize this proposal, due to commenters' concerns with course enrollment access and the amount of time we estimated it would require for an AO surveyor to complete the course.
CMS stated it believes the concerns raised by interested parties during the previous proposed rule comment period had been addressed by narrowing the scope of the required training and providing additional details regarding implementation. Therefore, we again made this proposal to address the consistency of surveyor knowledge and interpretation, since we proposed to require the AOs to use Medicare conditions and survey processes. We describe the courses required as well as the estimated time for each in section VII. of the proposed rule. We proposed at § 488.5(a)(8) a description of the content and frequency of the organization's in-service training it provides to survey personnel, and we would also require AOs to submit their training materials to CMS as part of the application process. We additionally proposed at § 488.5(a)(8)(i) to require that all AO surveyors complete two CMS mandatory courses which instruct surveyors, for all facility types, how to document their findings in the standardized survey materials. We stated we would also require AO surveyors to complete all relevant CMS online program-specific basic surveyor training, which we have already established for State and Federal surveyors. For example, AO hospital surveyors would be required to take the following CMS online courses: (1) Principles of Documentation for Non-
( printed page 36428)
Long-Term Care; (2) Basic Writing Skills for Surveyor Staff; and (3) Hospital Basic Training. A hospice surveyor would take the Principles of Documentation for Non-Long-Term Care; Basic Writing Skills for Surveyor Staff; and Hospice Basic Training courses. If an AO surveyor participates in both hospital and hospice surveys, they would take the two documentation courses and the two basic training courses. These courses would be the minimum mandatory requirements for AO surveyors. In addition, we stated we would also require that all AO surveyors would be required to take any updates to the CMS online surveyor courses when necessary. Any training above and beyond the minimum CMS online surveyor courses would be at the AO's discretion.
We proposed at § 488.5(a)(8)(ii), that AO surveyors hired after the date of implementation of this provision would be required to complete the required CMS online surveyor training courses prior to serving on a survey team (except as a trainee). We stated we believed a time requirement is necessary to ensure that the AO surveyors take the CMS online surveyor training in a timely manner and is consistent with the existing hospice program surveyor training requirements at 42 CFR 488.1115(a).
We proposed at § 488.5(a)(8)(iii) that AOs would also be required to document that the CMS online surveyor training courses were completed and the date of completion in the surveyor's staff personnel records. The purpose of this requirement would be to allow the AO and CMS to have records that document that the requirements had been met by each surveyor. We stated we would review these training records during our initial and renewal application review processes. We further proposed at § 488.5(a)(8)(iii) to require that the AOs maintain this documentation of course completion by each surveyor for no less than one accreditation cycle, so we could verify that AO surveyors had completed the online courses as part of the AO's next renewal application process. One accreditation cycle would be defined as the period of time during which the AOs' CMS approval is in effect, starting from the date of application approval and continuing until the date of approval of the next renewal application.
We explained this proposed requirement would align with and expand upon recent regulations that require hospice program AO surveyors to successfully complete the CMS online Basic Hospice Surveyor Training prior to performing any hospice program surveys.
In addition, we proposed at § 488.5(a)(8)(iv) that the provisions proposed at §§ 488.5(a)(8)(i) through (a)(8)(iv) would be applicable beginning 1 year after the effective date of this final rule with comment period.
The comments and our responses to the comments are set forth below.
Comment:
We received five comments specifically related to AO surveyors taking the CMS online basic training and documentation courses. Comments were generally accepting of the proposal but noted that AOs already provide comparable programmatic training to their surveyors. A few were strongly supportive of the requirement for AO surveyors to take the same online surveyor basic training as the SA surveyors to promote consistency in surveyor knowledge and interpretation in the survey process.
Response:
We appreciate the support and agree that for consistency purposes, AO surveyors and SA surveyors should be required to take the same online surveyor basic training courses.
Comment:
A commenter requested clarification on the proposed regulatory language that the AO will maintain this documentation for no less than one accreditation cycle. They questioned the use of “accreditation cycle” and requested clarity on whether CMS wanted AOs to maintain their completed training indefinitely or only for a 3-year period which is the timeframe for facility accreditation cycles.
Response:
We appreciate the opportunity to clarify this language and provide a clearer expectation for maintaining surveyor training records. As noted in Section H. of the proposed rule preamble, one accreditation cycle would be defined as the period of time during which the AOs' CMS approval is in effect, starting from the date of application approval and continuing until the date of approval of the next renewal application. As part of the deeming application review process, the CMS team reviews a sample of the AO surveyor files to ensure they meet the basic requirements for surveying, which includes but is not limited to any required licensure, education, and training. We would expect to see documented completion of the required CMS online training courses within the surveyor files. Therefore, we proposed the language of retaining that information for one accreditation cycle meaning one application cycle. However, the commenter raised a good point about needing clarity in the actual timeframes. In order for CMS to ensure oversight of these requirements and to be consistent with the proposed times for completing the training, we would need to see when the initial surveyor training was completed as well as any subsequent completions due to CMS required updates.
Final Decision:
After consideration of the public comments received, we are finalizing the requirement for AOs to complete two mandatory CMS online documentation courses and the relevant program-specific CMS online basic surveyor training course. However, we are modifying the language at 488.5(a)(8)(iii) for maintaining documentation “for no less than one accreditation cycle” to “of the initial completion and any subsequent completions.” We believe this revision is consistent with the original intent of the proposal.
However, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the applicable regulations text stating that a particular provision(s) will become applicable 1 year after the effective date of the final rule with comment period, or any similar language to that effect. For this final rule with comment period, we are making a modification that all provisions of the rule will become effective 1 (one) year after the publication of this rule.
X. Establish Criteria for “National in Scope” (§ 488.1)
On April 5, 2013, we published a proposed rule in the
Federal Register
entitled, “Medicare and Medicaid Programs; Survey, Certification, and Enforcement Procedures” (78 FR 20564), hereinafter referred to as the “2013 AO oversight proposed rule”, which proposed modifications to the CMS AO oversight regulations. In the 2013 AO oversight proposed rule, we stated that we proposed to revise § 488.5 and explained that the demonstration of “national in scope” by an AO must be specific to each accrediting program for which new or renewed CMS approval is sought (78 FR 20567). We also proposed to define “national accreditation organization” in § 488.1 and explained that CMS requires an AO program seeking initial approval to “already be fully implemented and operational nationally” (78 FR 20566). In the 2015 AO final rule (80 FR 29796), we explained that we would not require an AO to reach facility minimums or meet specific geographic distribution requirements to be deemed national in scope (80 FR 29802). We did this because we believed AOs should be able
( printed page 36429)
to demonstrate the ability to scale over time.
We have never specified objective criteria for “national in scope” in regulations. And, as the number of AOs (and the number of applications from AOs) grow, it is in the best interest of CMS and the AOs to establish specific criteria to define “national in scope.” Establishing a specific definition and criteria for what CMS would consider to constitute widely located geographically across the United States (U.S.) would ensure that CMS is objective and consistent during the AO application review process when deciding whether an AO's accreditation program is, in fact, national in scope. This would further ensure that new AOs, submitting applications for deeming authority, are represented across the nation and not clustered within one area of the country. Furthermore, this also provides an opportunity for facilities to choose any AO with a CMS-recognized accreditation program for its provider/supplier type, versus only having one AO to choose.
Therefore, we proposed to add a definition for “National in scope,” to the CMS regulations at § 488.1 to establish criteria for determining when an AO's accreditation program meets the requirement. We proposed that the definition, “National in scope” would mean that the providers and suppliers accredited by an AO under a specific accreditation program, must be widely located geographically across the U.S. The proposed requirement for “national in scope” would have two components. First, the AO would be required to have accredited at least five providers or suppliers under the accreditation program in question. Second, the five providers or suppliers accredited by the AO under that accreditation program would have to be geographically located in at least five out of the six geographic regions.
The addition of the proposed definition of “National in scope” requires that we also define the term “geographic regions of the U.S.”, because this is a component of the definition of “National in scope”. Therefore, we proposed to add a definition for “Geographic regions” at § 488.1.
The proposed six geographic regions consist of six groups of States that cover the northeast, southeast, mid-west, central, south, and western areas of the United States which provide six possible areas in which an AO could accredit a provider or supplier to meet the second part of the “national in scope” test. In contrast, the use of a simple north, south, east and west geographical division of the U.S. would only provide four possible regions in which an AO have accredited providers and suppliers.
We explained in the proposed rule that we believe that use of these six geographic regions as the geographical test for “national in scope” would provide a standard by which CMS could measure whether an AO has accredited the required number of healthcare providers or suppliers in varying geographical areas of the U.S. We further believe the requirement that an AO have one provider or supplier in at least five of the six geographic regions would demonstrate the AO's ability to scale up and develop a national presence over time and align with CMS' current consortiums or regions.[16]
AOs would need to be able to demonstrate this standard in their initial applications for deeming authority, as well as continue to meet this definition, which would be evaluated within their renewal applications.
We also explained that we believe that this proposed definition of “Geographic regions” would ensure that we are impartial and consistent during the application review process. We also believe that this proposed definition would provide the AOs with objective criteria for the definition of “national in scope” that they can strive to meet prior to submitting an application, especially for possible new accrediting programs.
We note that § 488.1 currently defines “national accrediting organization” as “an organization that accredits provider entities (as that term is defined in section 1865(a)(4) of the Act) under a specific program and whose accredited providers and suppliers are widely located geographically across the U.S.” Because we proposed to add a specific definition for “National in scope” to § 488.1, that requires a two-part test, we explained it would also be necessary to update the definition of “National accrediting organization” to add the requirement that the AO must be national in scope.
This would ensure that new AOs submitting applications for Medicare approval of their accreditation programs, would be required to show that they have the ability to provide accreditation services to providers and suppliers across the nation and not just those clustered within one area of the country. Making it a requirement that AOs be capable of providing accreditation services throughout the U.S. provides the opportunity to healthcare providers and suppliers in all regions of the U.S. to obtain deeming accreditation from the AO of their choice.
Therefore, we proposed to revise the existing definition of “National accrediting organization” at § 488.1. The proposed new definition of “National accrediting organization” would read as follows “
National accrediting organization
means an accrediting organization that is national in scope and accredits provider or suppliers, under a specific accreditation program.”
The comments and our responses to the comments are set forth below.
Comment:
We received three comments in strong support of the definition of “national in scope.” One commenter stated the clarification around national in scope determinations, along with defining the regions is helpful for new programs. One commenter stated their support and urged CMS to finalize its adoption, and the other commenter stated this change was a much-needed clarification of the application process.
Response:
We appreciate the commenters' support for defining “national in scope.” We agree that this clarification is helpful for new programs as well as new organizations wishing to apply for Medicare deeming authority.
Comment:
We received one comment disagreeing with the definition as the commenter suggested the defined regions are inconsistent with CMS' current regions. Additionally, the commenter noted that these provisions may create unintended competitive barriers to entry within the accreditation market. This commenter provided examples where an AO may have providers or suppliers in a Northeast State, a South and Western State, but no providers available in the Southeast or Central regions due to accreditation markets and demographic conditions. The commenter suggested that AOs would not be able to meet eligibility requirements since they would only have four regions rather than the required five. The commenter further implied that the language defined in section 1865(a)(4) of the Act, which states national accrediting organization to means an organization that accredits provider entities, under a specific program and whose accredited provider entities under each program are widely located geographically across the U.S. is sufficient.
Response:
While we appreciate these concerns, in 2020, CMS underwent a reorganization of the CMS Regional Offices, now known as the CMS Locations. The proposed regions
( printed page 36430)
outlined within the provisions align with the coverage of CMS' current six geographic locations of the Northeast, Atlanta, Chicago, Dallas, Denver and Seattle Locations. Furthermore, the requirement for five of the six geographic locations demonstrates that an organization is national as intended by the existing regulations and section 1865(a)(4) of the Act. For instance, an CMS-approved existing AO or a new organization wishing to apply for deeming authority would only be required to have one survey or provider seeking deemed status in five of the six locations, (1) Northeast: Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, West Virginia, New York, New Jersey, Puerto Rico, Virgin Islands, Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont; (2) Southeast: Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee; (3) Midwest: Illinois, Indiana, Michigan, Minnesota, Ohio, Wisconsin; (4) Central: Iowa, Kansas, Missouri, and Nebraska; Colorado, Montana, North Dakota, South Dakota, Utah, Wyoming; (5) South: Arkansas, Louisiana, New Mexico, Oklahoma, and Texas; (6) Western: American Samoa, Arizona, California, Hawaii, Commonwealth of the Northern Mariana Islands, Guam, Alaska, Idaho, Nevada, Oregon, Washington. This means the organization would only need to demonstrate national presence in five States out of 50 States. We do not believe this would cause undue burden.
Comment:
We received one comment raising concerns on the implications of transplant deeming programs. The commenter stated that in the case of transplant programs, there are approximately 260 programs nationwide and that the proposal would limit the number of programs available to demonstrate AO compliance. The commenter recommended that CMS consider limiting the proposal for transplant to three of the six regions to meet CMS' proposed definition of “national in scope”.
Response:
We appreciate the commenter's concerns related to transplant programs and the definition of “national in scope”. We note, to date CMS has not established or approved a transplant deeming program. We will take the commenter's concerns into consideration.
Comment:
We received one comment suggesting that CMS' proposed definition should not restrict the exploration of new methodologies and innovative approaches to accreditation. The commenter stated that instead of focusing solely on geographic coverage, accreditation standards should be rooted in scientifically developed criteria endorsed by nationally recognized bodies. The commenter believes this would ensure evolution with advancement in healthcare practices.
Response:
We appreciate the commenter's concerns. The intent for defining the geographic regions is to provide a method for assessing and ensuring organizations with deeming authority, or seeking deeming authority are of national presence as intended by the existing regulations. The proposed definition would not limit innovation or new methodologies but rather ensure consistency and one set process across all AOs.
Final Decision:
After consideration of the comments received, we are finalizing the definition and criteria as set out in the proposed rule without change.
Y. Revise the Definition of “Rate of Disparity” and To Use the Process and Outcome Disparity Rates and Performance Measures (§ 488.1)
In section IV.L. of the proposed rule, we proposed to revise the validation program by using two different types of validation surveys, which are: (1) the 60-day “look-back” validation survey and, (2) a direct observation survey approach, to evaluate the performance of the AOs. Validation surveys are full surveys performed for a representative sample of accredited facilities. Look-back validation surveys are completed by the SA within 60 days of an AO's full accreditation survey for the same facility. In some cases, representative sample “mid-cycle validation surveys” may be conducted whether or not there has been a preceding AO survey. The analysis of the validation survey findings is reported as a “disparity rate”. As previously discussed in section II.C. of the proposed rule, this rate of disparity is currently defined at § 488.1 as the percentage of all sample validation surveys for which a SA finds noncompliance with one or more Medicare conditions and where no comparable condition-level deficiency was cited by the AO and it is reasonable to conclude that the deficiencies were present at the time of the AO's most recent survey of that provider or supplier. The goal of the validation process is to determine whether the findings of the two surveys are comparable.
In calculating the current rate of disparity, the numerator is the number of surveys in which the AO missed at least one condition-level deficiency found by the SA and the denominator is the number of surveys in the validation sample. The result is the percentage of validation surveys where the AO missed finding a significant deficiency identified by the SA. If the AO missed at least one serious deficiency in a third of the validation surveys, the disparity rate would be 33 percent. A lower disparity rate indicates better AO performance.
The existing definition of “rate of disparity” is not applicable to the direct observation validation survey (DOVS) because it focuses on the survey process as opposed to the outcome of the survey. Therefore, we proposed to revise the current definition of “rate of disparity” located at § 488.1 and replace this definition with two new definitions, which are “outcome disparity rate” and “process disparity rate”.
The outcome disparity rate would be applicable to the look-back validation survey, which is the current method of validation. We proposed that the new definition of “outcome disparity rate” would generally remain as the existing definition of “rate of disparity” at § 488.1 but would be revised and retitled as “outcome disparity rate” to distinguish it from the “process disparity rate”.
When calculating the process disparity rate, the numerator for one provider or supplier for which the DOVS is done would be the number of observed survey process findings and the denominator would be the number of expected survey process findings for all DOVS. The observed survey process findings are the actual number of Medicare conditions that were observed being surveyed for by the AO. The expected survey process findings are the total number of Medicare conditions that the AO should have examined during the survey observation. The result would be reported as a percentage. A high percentage indicates greater disparity between the expected AO performance on DOVS and the actual AO performance on the DOVS. For example, a DOVS with 75 observed process findings out of 100 expected process findings would yield a process disparity rate of 25 percent [((100-75) ÷ 100) * 100], indicating a 25 percent difference between what is observed and what is expected (See Figure 1).
( printed page 36431)
The proposed process disparity rate would be applicable to the DOVS and would be defined as the difference between the observed survey process findings and the expected survey process findings.
The overall process disparity rate for a particular AO would be calculated by taking the average of the process disparity rate for each DOVS performed for an accreditation program of an AO. Preliminary results obtained from the VRP pilot during the period of June 2018 to July 2019 are shown in Figure 2. While we will analyze and explain the pilot data when more is available, we share preliminary data here as a sample of how the process disparity rate will be calculated.
Final Decision:
We received no comments specific to this provision. We are finalizing the removal of the definition of “Rate of disparity” and adding the definition of “Process disparity rate,” as we proposed. However, we are not finalizing the addition of the proposed definition of “Outcome disparity rate” because this term only applies to the look-back validation surveys, which we are also not finalizing in this rule.
Additionally, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the regulations text stating that a particular provision(s) will become applicable beginning on a specific date, or any similar language to that effect. We are making a modification that all provisions of the rule will become effective 1 (one) year after the publication of this final rule with comment period.
Z. Require AOs To Submit a Publicly Reportable Plan of Correction for Unacceptable Performance Measure Scores (§§ 488.8(a)(2) and (4))
In section IV.J. of the proposed rule, we proposed to revise the definition of “disparity rate” to include process and outcome disparity rates. We noted that the proposed definition of outcome disparity rate generally remains the same as the currently defined definition of disparity rate. We further noted that we have been measuring the outcome disparity rate as a performance measure for years. To monitor an AO's ongoing performance as provided by section 1875(b) of the Act and § 488.8, we proposed in paragraph (a)(2) of § 488.8 to expand the types of validation activities included in the performance review. We also proposed in paragraph (a)(4) to require AOs to submit a plan of correction that would be publicly reported, when the AO's performance on survey activities identify disparity concerns either through the outcome disparity rates or process disparity rates.
We proposed to revise § 488.8(a)(2) to broaden activities that CMS would evaluate in our ongoing review of AOs. Specifically, we would monitor the results of our outcome disparity rate, the look-back validation surveys, complaint surveys, and the process disparity rate as determined by DOVS. In addition, we proposed to revise § 488.8(a)(4) to require that when an AO's outcome disparity or process disparity performance measure scores, as
( printed page 36432)
determined from look-back and DOVS, reveal that the AO's accreditation survey activities do not meet an acceptable performance threshold established by CMS, the AO would be required to submit an acceptable plan of correction to CMS which identified corrective action the AO proposed to take to correct their performance.
We proposed at § 488.8(a)(4)(i), to require that the plan of correction be submitted to CMS for review within 10 business days of the AO being notified by CMS of not meeting the acceptable performance threshold. We also proposed that to be acceptable, the AO's plan of correction would have to: (1) document specific actions being taken by the AO to address improving performance (proposed § 488.8(a)(4)(i)(A)); (2) document the timeframe for implementation of the plan (proposed § 488.8(a)(4)(i)(B)); (3) plan for ongoing monitoring of the plan of correction toward achieving an acceptable level of performance (proposed § 488.8(a)(4)(i)(C)); and (4) identify the individual responsible for implementation and monitoring of the acceptable plan of correction (§ 488.8(a)(4)(i)(D)).
CMS would subsequently communicate with the AO on the acceptability of the plan of correction and would provide oversight of implementation. We proposed at § 488.8(a)(4)(ii) that upon review and approval of the submitted plan of correction, CMS would provide ongoing evaluation of the progress of plan implementation.
Finally, we proposed at § 488.8(a)(4)(iii) that the AO's plan of correction be made subject to public reporting by CMS. Once approved, the plan of correction would be publicly available for review. This means that the acceptable plan of correction would be displayed publicly by CMS once approved. This plan of correction would be utilized to increase an AO's accountability for maintaining performance standards.
The purpose of this oversight is to improve AO survey activity outcome and processes with the presumption that improvements toward acceptable performance would improve the health and safety of patients receiving services in Medicare-participating facilities. This is an effort to strengthen AO oversight by requiring AOs to address issues and take corrective action to improve to an acceptable level of performance. Previously, this was handled verbally or through written correspondence between the AO and CMS staff without a specific plan of correction.
The proposed publicly reportable plan of correction would be based on both an analysis of data to identify the outcome and process disparity performance measure(s) for which the AO did not meet acceptable performance as well as significant instances of disparity. An analysis matrix would outline both outcome performance and process performance areas of successful achievement and those areas for which achievement was less than acceptable as demonstrated by the outcome and process disparity rate data. An example of what a plan of correction matrix might look like is indicated in Figure 3.
Figure 3
The matrix in Figure 3 is representative of FY 2018 data collected during the DOVS, look-back validation surveys, and complaint surveys (which investigate specific allegations) conducted by the SA at AO facilities. If deficiencies were cited first by the AO and validated by the SA during a look-back or complaint survey this is considered an outcomes match. If the AO survey process under direct observation by the SA did not raise concerns, this indicates a positive outcome and positive process, which are represented in the top left box. The top right and bottom left boxes indicate where improvements need to be made in either the process or outcome of the respective Medicare requirement, while the bottom right box shows where improvements in both measures should be made.
The AO would be able to use this matrix to identify if the less than
( printed page 36433)
acceptable performance is either outcome-focused, process-focused, or both. The proposed plan of correction would be required to be submitted to CMS within 10 business days following CMS' notification to the AO of less than acceptable performance, and would have to address the areas of improvement and the specific actions to be taken by the AO to improve those areas on a sustainable basis.
The comments and our responses to the comments are set forth below. We received a total of four public comments on this provision.
Comment:
One commenter was supportive of this proposal and urged its adoption.
Response:
We appreciate the commenter's support of this provision.
Comment:
One commenter was pleased that CMS continues to demonstrate its commitment to improving the quality of care across the healthcare continuum.
Response:
We appreciate the commenter's support for this provision as we continue our commitment to improving the quality and safety of care for patients.
Comment:
One commenter supported the requirement for AOs to submit a publicly reported plan of correction for unacceptable performance measure scores. The commenter believes this will ensure quality control across AOs and ensure unacceptable performance is addressed.
Response:
We appreciate the commenter's support for this provision as we believe the transparency of AO oversight can improve the quality of AO performance.
Comment:
One commenter strongly opposed this provision to make plans of correction public believing it sets up the AO community to liability in the current litigious environment and may have a negative impact on providers/suppliers choosing AOs. The commenter noted that accreditation is voluntary and noted that providers/suppliers may use accreditation for initial surveys and then return to State jurisdiction after they receive their CCN. They believe this puts an additional burden on State agencies and will cause additional delays in State agency survey activity for these providers/suppliers.
Response:
We recognize the concerns of the commenter and the potential impact on business practices, but we have an obligation to be transparent in our oversight of AO performance. Public reporting provides transparency and allows providers the opportunity to make an informed decision about the performance of an AO when deciding the AO that best meets their needs.
Final Decision:
We are finalizing this section and modifying the proposed language of the requirements to remove the terms, “outcome disparity rate” and “look-back validation survey” from paragraphs (a)(2) and (a)(4) of this section.
AA. Revisions to the AO Survey Validation Program (§ 488.9)
Prior to discussing our finalized provisions, the following provides (1) background on validation surveys, (2) background on look-back validation surveys, and (3) background on additional approaches to conduct validation surveys, before (4) introducing CMS' proposed changes.
1. Background on Validation Surveys
Section 1864(c) of the Act permits the SAs to perform validation surveys of provider and supplier types participating in Medicare via accreditation under section 1865(a) of the Act; the SA surveys validate the AOs' accreditation processes. The accreditation validation program is one component of CMS' oversight of AOs with approved Medicare accreditation programs, and consists of two types of validation surveys:
Complaint surveys—focused surveys based on complaints from patients, family, facility staff, or other governmental entities, which, if substantiated, could indicate serious non-compliance with one or more Medicare conditions; and
Validation surveys—full surveys, which are routinely performed for a representative sample of deemed facilities as part of the annual CMS-AO representative sample validation survey program. These surveys are completed by the SA within 60 days of an AO full accreditation survey for the same facility.
Prior to 2007, section 1875 of the Act required CMS to report to Congress annually only on The Joint Commission's (TJC's) hospital accreditation program.[17]
In FY 2007, we expanded this oversight and began conducting representative sample validation surveys for selected non-hospital facility types (CAHs, HHAs and ASCs), in addition to those already being performed for accredited hospitals. In FY 2010, hospice look-back validation surveys were added, and in FY 2011, psychiatric hospital validation surveys were added. In FY 2019, we conducted a total of 315 representative sample look-back validation surveys for six facility types across the AOs.[18]
This total was comprised of 119 hospital surveys (including 20 psychiatric hospitals) and 196 non-hospital validation surveys. (See Figure 4.)
Figure 4
( printed page 36434)
Since 2007, CMS has worked to strengthen its oversight of AOs and increase the number of validation surveys. The recent history of completed validation surveys is as follows:
2015: 118 hospital and 240 non-hospital surveys totaling 358 surveys.
2016: 119 hospital and 254 non-hospital surveys totaling 373 surveys.
2017: 116 hospital and 244 non-hospital surveys totaling 360 surveys.
2018: 128 hospital and 188 non-hospital surveys totaling 316 surveys.
2019: 119 hospital and 196 non-hospital surveys totaling 315 surveys.
These numbers represent a 250 percent increase in the overall number of validation surveys conducted, from 90 in FY 2007 to 315 in FY 2019. During the same time period, the number of non-hospital validation surveys conducted increased by 460 percent, from 35 surveys in FY 2007 to 196 surveys in FY 2019. The number of hospital (including psychiatric hospital) validation surveys conducted increased by 116 percent, from 55 surveys in FY 2007 to 119 surveys (99 hospital validation suveys plus 20 psychiatric hospital validation surveys) in FY 2019.
2. Background on Look-Back Validation Surveys
The purpose of look-back validation surveys of deemed providers or suppliers is to assess the AO's ability to assess compliance with Medicare conditions. These surveys are on-site full surveys completed by SA surveyors no later than 60 days after the end date of an AO's Medicare accreditation program full survey. The SA performs these surveys without any knowledge of the findings of the AO's accreditation survey. CMS determines the number of look-back validation surveys to perform for each AO based on the total number of facilities the AO accredits for Medicare participation, as well as the overall budgeted validation survey targets, by State and facility type.
The proportion of look-back surveys completed for deemed facilities is calculated by dividing the number of look-back validation surveys conducted by the total number of deemed facilities. The proportion of deemed facilities that received a look-back validation survey in FY 2019 is as follows:
Hospitals:
Three percent of deemed hospitals received a validation survey in FY 2019 (99 validation surveys conducted out of 3,332 deemed facilities).
Psychiatric Hospitals:
Four percent of deemed psychiatric hospitals received a validation survey in FY 2019 (20 validation surveys conducted out of 466 deemed facilities).
CAHs:
Three percent of deemed CAHs received a validation survey in FY 2019 (13 validation surveys conducted out of 449 deemed facilities).
HHAs:
Two percent of deemed HHAs received a validation survey in FY 2019 (84 validation surveys conducted out of 4,034 deemed facilities).
Hospices:
One percent of deemed hospices received a validation survey in FY 2019 (32 validation surveys conducted out of 2,458 deemed facilities).
ASCs:
Four percent of deemed ASCs received a validation survey in FY 2019 (67 validation surveys conducted out of 1,803 deemed facilities).
3. Background on Additional Approaches To Conducting Validation Surveys
Over the years, we have looked for ways to improve the validation survey process and the disparity rate methodology. As discussed earlier in this final rule with comment period, the disparity rate for various provider types ranged between 8 percent for HHAs and 46 percent for CAHs.
To address concerns about high disparity rates, CMS has been testing a Validation Redesign Program (VRP) pilot since 2018. In the VRP pilot, instead of the separate look-back validation survey, a direct observation
( printed page 36435)
of the AO's survey is performed. During the DOVS, the SA surveyors are present when the AO surveyors perform an accreditation survey, so that they can directly observe and evaluate the ability of the AO surveyors to assess compliance with the Medicare conditions. The purpose of this direct observation is to evaluate, in real time, the AO's performance on the survey process. The real time observation of the survey allows the SA surveyors to make suggested improvements and address any concerns with AOs immediately.
From June 2018 through August 2019, CMS conducted a total of 30 VRP pilot surveys in 17 States in the acute care hospital program (11), ASC program (10), psychiatric hospital program (3), HHA program (5) and hospice program (1). This proposed direct observation validation process has yielded additional information about the extent to which the AO's process meets or exceeds the survey process used by the SA surveyors. Our findings from our VRP pilot surveys included the following:
Certain AOs have rigid survey schedules that proved to be burdensome to the SA observers while onsite due to difficulty of SAs in coordinating their own scheduled and mandated survey work of non-accredited facilities in their State with these AO survey schedules.
AOs may have strict timeframes for each section of the survey to which they adhere, regardless of the findings or need to further investigate an issue within a facility.
Not all AOs survey offsite locations consistently for all portions of the survey.
Certain AO survey methodology favored a “yes/no” or “have/don't have” format versus a more in-depth investigative approach followed by the SAs and detailed in the SOM; the survey approach used by some AOs in certain aspects of the survey could significantly affect the survey outcomes, for example missing subtle but systemic issues at facilities that could adversely impact patient care and safety if not identified during the survey.
Verbal assertion may have been considered adequate evidence of a facility's compliance, without verification via observations and/or document review.
4. Revisions to the Existing AO Survey Validation Program (Proposed Revisions to § 488.9)
We proposed to revise the validation program by using two different types of validation surveys, which are: (1) the look-back validation survey and (2) a DOVS approach, to evaluate the performance of the AOs. We proposed that direct observation surveys can be performed by the SA or CMS surveyors.
Specifically, we proposed at § 488.9(b) to revise the types of validation surveys. We proposed to continue using the look-back validation survey, through use of a sample of facilities in each program type, which would take place within 60 days following the AO surveys. These 60-day validation surveys are referred to as look-back validation surveys.
We proposed at § 488.9(b)(2) to also require validation using the DOVS, which focuses on real-time observation and evaluation of the AO's survey process. At § 488.9(c), we proposed rules for look-back validation surveys. At § 488.9(d), we proposed the rules for selection for look-back validation surveys. More specifically, proposed § 488.9(d)(1) would provide that “a provider or supplier selected for a look-back validation survey must cooperate with the SA that performs the look-back validation survey.” We proposed at § 488.9(d)(2) that “if a provider or supplier selected for a look-back validation survey fails to cooperate with the SA, it will no longer be deemed to meet the Medicare conditions or requirements, will be subject to a review in accordance with paragraph (a) of this section, and may be subject to termination of its provider agreement under § 489.53 of this chapter”.
At § 488.9(e), we proposed rules for the DOVS. These rules would include the following: (1) All DOVS would be unannounced to the AO and the facility being surveyed (proposed § 488.9(e)(1)); (2) The SA or CMS surveyors would generally be assigned to the AO surveyors on a 1:1 basis, matching the experience of the accreditation surveyor where possible, and using the CMS approved standards and processes to determine compliance with the Medicare conditions (proposed § 488.9(e)(2)); (3) the SA or CMS surveyors would observe the AO survey in accordance with CMS established policies and procedures and would report the findings directly to CMS (proposed § 488.9(e)(3)); and (4) where the SA or CMS surveyors disagree with the findings of the AO surveyors, and these differences could not be reconciled, CMS would render a final decision that would not be appealable under part 498 (proposed § 488.9(e)(4)).
At proposed § 488.9(f), we proposed circumstances in which an accredited provider or supplier would be deemed to have not met the applicable Medicare conditions or requirements, such as if: (1) the provider or supplier refused to authorize its AO to release a copy of their current accreditation survey to CMS (proposed § 488.9(f)(1)); (2) the provider or supplier refused to allow a validation survey (for either look-back or DOVS) (proposed § 488.9(f)(2)); or (3) CMS found that the provider or supplier did not meet the applicable Medicare conditions (also known as CoPs, CfCs, or requirements) (proposed § 488.9(f)(3)).
At § 488.9(g), we proposed the consequences for non-compliance. At § 488.9(g)(1), we proposed that if a CMS validation look-back or DOVS resulted in a finding that the provider or supplier was out of compliance with one or more Medicare conditions, deemed status would be removed by CMS and the provider or supplier would be subject to ongoing review by the SA or CMS (in accordance with § 488.10(d)) until the provider or supplier demonstrates compliance. At proposed § 488.9(g)(2), we proposed that CMS could take actions for the deficiencies identified in the in accordance with § 488.24, or could first direct the SA or CMS surveyors to conduct another survey of the provider's or supplier's compliance with specified Medicare conditions or requirements before taking the enforcement actions provided for at § 488.24. At proposed § 488.9(g)(3), we proposed that if CMS determined that a provider or supplier is not in compliance with applicable Medicare conditions or requirements, the provider may be subject to termination of the provider agreement and any other applicable intermediate sanctions and remedies.
At proposed § 488.9(h), we proposed considerations for the re-instatement of the deemed status of a provider or supplier. An accredited provider or supplier would be deemed to meet the applicable Medicare conditions or requirements in accordance with this section if any of the requirements are met, as applicable:
It withdraws any prior refusal to authorize its AO to release a copy of the provider's or supplier's current accreditation survey (proposed § 488.9(h)(1)).
It withdraws any prior refusal to allow a look-back or DOVS, if applicable (proposed § 488.9(h)(2)).
CMS finds that the provider or supplier meets all applicable Medicare CoPs, CfCs, or requirements (proposed § 488.9(h)(3)).
At proposed § 488.9(i), we proposed that the existence of any performance review, comparability review, deemed status review, probationary period, or any other action by CMS, would not affect or limit CMS in conducting any subsequent validation survey.
( printed page 36436)
Our proposal to revise the validation process by adding DOVS and our other proposed revisions to § 488.9 would be applicable 60 days after the effective date of the final rule with comment period.
We also proposed that the DOVS may be performed by not only the SAs but also by CMS surveyors. This would allow for flexibility and expediency in the performance of these validation surveys.
Our proposed revisions to the AO validation process at § 488.9 would not apply to laboratories, as they are subject to the provisions under part 493.
We received ten comments specifically on the proposed revisions to the validation program. The comments and our responses to the comments are set forth below.
Comment:
Comments were generally supportive of the proposed addition of the DOVS process. Specifically, commenters stated that direct observation surveys provide a more accurate, meaningful, and timely picture of AO performance and are less burdensome for facilities than the traditional look-back validation surveys.
Response:
We thank the commenters for their support.
In 2018-2019, CMS piloted a streamlined way to instead use direct observation during the AO reaccreditation surveys to evaluate an AO's ability to assess compliance with the Medicare conditions. With the end of the COVID-19 PHE on May 11, 2023, CMS resumed routine oversight activities that promote ongoing quality of care and patient safety. As announced via Admin-info Memo 23-14 (available at
https://www.cms.gov/files/document/admin-info-23-14-nltc.pdf), the DOVS pilot resumed in October 2023, utilizing a national contractor working on behalf of CMS to directly observe and evaluate an AO's ability to assess the Medicare conditions during surveys. Both DOVS pilots have provided CMS with an additional level of oversight and, overall, more consistent evaluation of AO performance. We acknowledge the look-back surveys do not provide a one-to-one comparison of the AO's survey process performance. We believe the DOVS process provides a more accurate and real-time picture of an AO's survey performance in ensuring compliance with the Medicare health and safety requirements.
Comment:
The majority of commenters encouraged CMS to phase out or completely abandon the existing 60-day look-back validation survey due to the burden on facilities, lack of CMS surveyors to complete survey workload, as well as the inaccuracy of assessing AO performance. Commenters stated they understand the validation process to be an assessment of AO process and performance rather than comparison of a provider's compliance with Medicare regulations at different points in time. They believe the look-back surveys capture information from different points in time and do not take into account any changes made by the facility immediately after the AO survey that could influence the overall disparity rate between the AO survey and subsequent SA survey. Commenters also expressed concern that continuing to utilize the look-back validation survey option fosters unreliable results of AO survey performance as it is impossible to evaluate their process when the SA validation survey occurs at separate times.
Response:
CMS is responsible for oversight of the national AOs' Medicare accreditation programs, and for ensuring that providers and suppliers under CMS-approved deeming programs meet the minimum quality and patient safety standards required by the Medicare conditions. Section 1864(c) of the Act permits validation surveys of provider and supplier types deemed for Medicare participation under Section 1865(a) of the Act as a means of validating the AOs' accreditation processes. Historically, we have measured the effectiveness of AOs by choosing a sample of facilities, performing State-conducted “look back” surveys within 60 days following AO surveys, and comparing results of the State surveys with the AO surveys. We acknowledge the commenters' concerns with the look-back validation survey process.
By withdrawing our proposed look-back validation survey method and proceeding only with the DOVS, we believe that this will reduce provider burden by not requiring an additional validation survey and thus reduce the number of times that healthcare providers have to undergo two full surveys within a 60-day period. We further believe this approach enhances the validation program and will be welcomed by both the AOs and the providers and suppliers.
Additionally, while the DOVS pilot program was successfully piloted over the last few years and AO feedback has been very positive, it has not been without its own set of challenges. The most challenging aspect of conducting a simultaneous survey for evaluating AO performance is scheduling. CMS receives AO pending survey schedules a month ahead and then chooses a representative sample of facilities from each AO for DOVS. During the DOVS pilot, surveys were always unannounced to the facilities but were announced to the AO being observed to facilitate the 1:1 matching for experience of the accreditation surveyor where possible and to determine timing of survey start and location so that the two teams could enter the facility together. Entering the facility together is important to minimize burden and confusion to the facility being surveyed. We must ensure facilities understand they are not undergoing a double survey, but that DOVS observers are there to evaluate the AO performance. On many occasions survey start dates were changed or canceled completely due to many factors including, but not limited to, surveyor illness or emergency, weather-related travel cancellations, or mistakes in provided survey schedules. Often, these changes occurred within 24-48 hours of the survey's scheduled start date causing the national contractor working on behalf of CMS to shuffle a survey team and revise travel arrangements. Sometimes these last-minute changes incurred travel costs to the government due to airline and hotel change fees. Throughout the 2023-2024 pilot, CMS attempted to mitigate these challenges but has not yet resolved this issue to clear a path for sending DOVS observer teams completely unannounced to meet the AO's staff onsite at the AO client's facility. Additionally, review of the pilot alleviated our original concern that AOs send their best and strongest surveyor teams when they know they are being observed. We did not find this to be the case during the pilot surveys and have observed a low incidence of repeat surveyor and survey teams during our observed DOV surveys. Therefore, we believe that validation surveys must remain unannounced to the facility and the applicable AO. However, due to the ongoing logistical concerns detailed here regarding coordination between AO surveyor teams and the CMS DOVS teams for individual surveys, we may have to exercise a degree of discretion in enforcing this requirement for AOs, after this rule is effective and implemented and once the DOVS program resumes.
Comment:
One commenter raised concern over the proposal at § 488.9(g) that a facility could lose its deemed status if a condition-level deficiency was discovered during a validation survey. They stated that this proposal suggests that a deemed status accreditation survey conducted by the AO does not hold the same value as a CMS survey and, therefore, seems to undermine the agency's intent to align standards and survey processes.
( printed page 36437)
Response:
We thank the commenter for raising this concern and appreciate the opportunity to clarify the proposal at § 488.9(g). We have always retained the right to remove deemed status (that is, to no longer recognize a facility's accreditation as a finding of compliance) from a Medicare-participating facility for noncompliance with one or more Medicare conditions or requirements, in accordance with section 1865(c) of the Act. This most often occurs during a substantial allegation complaint survey that is conducted by the SA in an accredited facility. Although we do intend to align standards and survey processes to the extent possible, an accreditation organization does not act as an agent of CMS, unlike State survey agencies who perform their duties according to CMS' terms under contract. We do not directly employ accrediting organizations but recognize the equivalence of their determinations by granting such organizations “deeming authority” upon review of their processes and standards. Therefore, our withdrawal of a facility's “deemed status” is the one of the few tools we have to ensure that an accreditation organization's standards and processes continue to “meet or exceed” our own.
Comment:
One commenter encouraged CMS to maintain a transparent process when making any future changes to the validation process policies and procedures. They requested that CMS involve AOs and other interested parties throughout the revision process and to utilize the feedback received during the pilot program to ensure the efficacy of validation surveys.
Response:
We appreciate the feedback from those AOs who have directly experienced the pilot DOVS process over the last few years as it has helped guide our decision-making process. We are committed to providing meaningful oversight in an efficient manner. We remain committed to providing transparency with any changes to the validation process as evidenced by our public release of the DOVS pilot program Standard Operating Procedure via Admin-info Memo 23-14 (available at
https://www.cms.gov/files/document/admin-info-23-14-nltc.pdf). We will continue to engage with AOs and other interested parties to ensure an efficient and effective validation program.
Comment:
One AO commented on their experience with the DOVS process and, while they agreed that the existing validation process needed revisions, they shared concerns with the DOVS process going forward. In particular, this AO was concerned that DOVS observers evaluated their performance based on personal/professional preference for particular survey methods without the supporting basis of a CMS requirement. The commenter does not believe that a CMS surveyor's personal/professional preference for a survey method should be the basis for a deficiency rating on AO performance. This commenter did acknowledge the DOVS reconsideration process as a way to address these situations if they arise but believes this is an additional burden on an AO to ask CMS for a reconsideration of the DOVS scoring.
Response:
Again, we appreciate the feedback from those AOs who have directly experienced the DOVS pilot process. We agree that personal opinion and preference should not influence observations or ratings of AO performance. The intent of DOVS is to evaluate an AO's survey process in assessing facilities for compliance with Medicare conditions. During our pilot, we have continuously engaged with AOs, clarified expectations, and ensured that evaluations conducted by DOVS observers are consistent with comparable survey processes of the SAs. As the commenter mentioned, CMS has a reconsideration process for AOs to request secondary review of the DOVS findings to determine correct interpretation of the Medicare conditions by both the AO and DOVS observers and we will continue to evaluate this process.
Comment:
Lastly, we received one comment stating that our proposal as drafted would subject Indian Health Service (IHS) facilities to State surveys and State surveyor oversight without their consent and that § 488.9 provides that “validation surveys” are conducted by State survey agencies without providing an exception for IHS providers.
Response:
CMS is clarifying that the CMS Survey & Operations Group, CMS Locations, remains responsible for the certification of all IHS and tribal facilities and this rule does not change the existing processes for how IHS and tribal facilities are surveyed.
Final Decision:
We have reviewed all the comments received on the proposed revisions to the validation program and we have also taken into account the experiences and AO feedback from our DOVS pilot over the last few years. We agree with commenters that the DOVS program has been successful and less burdensome for facilities. First, we have considered the concerns related to the look-back validation program and, based on the public comments received, are making revisions to the proposals at § 488.9 by withdrawing all of our proposed references to look-back surveys as a process for AO validation performance in this final rule with comment period. We are also withdrawing our proposed requirements specific to look-back validation surveys and methods and have reorganized § 488.9 accordingly in this final rule with comment period. We are withdrawing these proposed provisions since they only pertain to the findings of the look-back validation surveys, specifically outcomes of surveys and the disparities between SAs and AOs regarding the citing of non-compliance with the conditions and requirements.
We are also revising § 488.9(f) in this final rule with comment period (proposed as § 488.9(h)) by adding the clarifying clause, “in addition to substantive re-approval of the facility”, so that the provision will now read, “An accredited provider or supplier will be deemed to meet the applicable Medicare conditions or requirements in accordance with this section, if,
in addition to substantive re-approval of the facility,
the following requirements are met, as applicable” [emphasis added]. We have revised this provision to clarify that a facility, in addition to meeting the requirement, must also undergo a successful survey on substantive grounds in order to have its deemed status reinstated.
Additionally, we are renumbering proposed § 488.9(g)(2) in this final rule with comment period as § 488.9(e) to read: “
Consequences for a finding of non-compliance.
CMS may take actions for any deficiencies identified in the DOVS in accordance with § 488.24, or may first direct the State survey agency to, or CMS may, conduct another survey of the provider's or supplier's compliance with specified Medicare conditions or requirements before taking the enforcement actions provided for at § 488.24.”
We are finalizing the changes to § 488.9 with the modifications previously discussed. Based on our review and analysis of both the VRP and DOVS pilots, we recognize that direct onsite observation of AOs using the DOV survey method is the most effective process for measuring AO performance. AOs, SAs, facilities, and other interested parties have all expressed agreement that DOV surveys reduce burden compared to look-back surveys and are a more accurate depiction of AO survey performance. Therefore, we are removing all references to the 60-day “look-back” surveys in the regulations and retaining only DOV surveys for the validation program.
( printed page 36438)
Additionally, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the applicable regulations text stating that a particular provision(s) will become applicable 1 year after the effective date of this final rule with comment period, or any similar language to that effect. For this final rule with comment period, we are making a modification that all provisions of the rule will become effective 1 (one) year after the publication of this rule.
BB. Revise the Psychiatric Hospital Survey Process
Under section 1861(f) of the Act, psychiatric hospitals are a defined provider type. This statutory provision requires psychiatric hospitals to comply with most hospital Medicare conditions, known as CoPs, but includes a few provisions applicable exclusively to them. In 1986, special Medicare conditions for psychiatric hospitals were published and included, as part of the hospital Medicare conditions, as provisions of 42 CFR part 482. At that time, psychiatric hospital surveys were performed by either SA personnel or Healthcare Financing Administration [19]
(HCFA) mental health surveyors (board-certified psychiatrists, master's prepared psychiatric nurses, master's prepared psychiatric social workers, doctorally prepared clinical psychologists, and doctorally prepared clinical psychopharmacologists) who were under contract with HCFA. This extensive experience requirement was beyond what is required for other types of hospital services. This requirement limited the numbers of SAs with qualified surveyors. Therefore, a CMS contractor with specially trained and/or experienced psychiatric surveyors assisted the SAs in performing such surveys. This has resulted in a bifurcated survey process, as most psychiatric hospitals were subjected to two survey teams for each accreditation survey: the hospital survey team and the psychiatric component survey team.
However, in the FY 2014 Quality, Safety & Oversight Group Mission and Priority Document, the restrictive requirement for extensive education and/or experience for psychiatric surveyors was removed. CMS developed online psychiatric surveyor training, provided on-site psychiatric surveyor training through contractors and offered partnership training for surveyors who did not have extensive psychiatric education or experience. This training became the standard and expectation for qualification to survey to the psychiatric Medicare conditions.
The special Medicare conditions applying to psychiatric hospitals are set forth in § 482.60 through § 482.62. The special provisions at § 482.60 require the following: (a) that the hospital be primarily engaged in providing, by or under the supervision of a doctor of medicine or osteopathy, psychiatric services for the diagnosis and treatment of mentally ill persons; (b) meet the conditions of participation specified in §§ 482.1 through 482.23 and §§ 482.25 through 482.57; (c) maintain clinical records on all patients, including records sufficient to permit CMS to determine the degree and intensity of treatment furnished to Medicare beneficiaries, as specified in § 482.61; and (d) meet the staffing requirements specified in § 482.62. As noted earlier, participating psychiatric hospitals must also meet the applicable Medicare conditions for acute-care hospitals.
In March 2020, we eliminated the contract for separate psychiatric hospital surveyors and provided comprehensive online training for all SAs. This training focused on the specific psychiatric hospital Medicare conditions so that the SA surveyors would be fully trained to conduct all aspects of a complete psychiatric hospital inspection. At this time, we also combined the interpretive guidance at Appendix AA for psychiatric hospital surveys into the Appendix A for hospital surveys to provide a single location for all of the Medicare conditions during a full psychiatric survey.
At this time, TJC, DNV Healthcare, and the Center for Improvement in Healthcare Quality are the only AOs that have CMS-approved psychiatric hospital accreditation programs. They conduct one complete survey of the entire psychiatric hospital, to include inspection of the regular hospital Medicare conditions and the psychiatric hospital Medicare conditions. Any AO is eligible to submit an application for consideration for accreditation to survey psychiatric hospitals for deeming purposes.
In the proposed rule, we announced our intention to integrate the acute care hospital and psychiatric hospital survey processes for SAs to ensure that there is a systematic and integrated look at psychiatric hospital safety and quality (89 FR 12028-12029). Therefore, AOs that currently survey only hospitals would need to expand their hospital accreditation programs to include the Medicare special provisions applying to psychiatric hospitals (§ 482.60 through § 482.62) to survey for psychiatric hospitals as well.
We believe that consolidating psychiatric and acute care hospital Medicare condition oversight will improve the overall quality of the care by ensuring that systemic issues are more easily identified. With a single survey team conducting the survey for the entire facility, inconsistencies, trends, and subtle discrepancies can be connected more easily and provide a more comprehensive overview of underlying systemic issues. We believe that this comprehensive approach to survey both the psychiatric and acute care hospital will enhance patient health and safety by ensuring the system as a whole is evaluated to meet the applicable Medicare requirements. Moreover, a single survey team decreases the team's physical imprint on the facility which minimizes any facility disruption resulting from the survey. When revisits are required related to deficiencies in the psychiatric Medicare conditions, only one survey team will return for re-inspection, which will reduce coordination time and resources as well as impact on individual facilities. Finally, we have determined that combining the survey process for psychiatric hospital Medicare conditions into the hospital program would improve the cost efficiency of CMS' survey and certification activities and simplify the survey process for SAs and AOs alike.
For SAs, we would consolidate the deficiency report from psychiatric hospital survey activity into one Form CMS-2567, reporting on compliance with both the hospital Medicare conditions as well as the psychiatric services Medicare conditions. The survey process for inpatient psychiatric units located in acute care hospitals would not change, and this change would not require any revisions to our regulations.
To ensure that surveys of psychiatric hospitals and units located in hospitals are performed properly by the SA surveyors, they have been provided online training on the psychiatric hospital Medicare conditions. CMS developed this online training and released it in March 2020. It is now available to all SA and AO surveyors at
https://qsep.cms.gov/.
We proposed to expand the acute care hospital accreditation program for AOs to include current psychiatric hospital accreditation standards. As per § 488.8(b), CMS assesses the equivalency of the AOs programs to the
( printed page 36439)
CMS-approved program requirements, and, as such, this proposal to combine acute care and psychiatric hospital surveys necessarily required that we also proposed to revise the hospital accreditation program application process for AOs that have an approved hospital program, so as to include psychiatric hospital accreditation in their hospital programs. Those AOs that currently have an approved hospital program would be required to resubmit their standards, survey processes, and surveyor training (which may include the specific CMS surveyor training required by this rule for AO surveyors) to include review of the psychiatric Medicare conditions for psychiatric hospitals for CMS approval. This means that an AO that is seeking approval of a hospital accreditation program would be required to file one application that includes how they will assess for the two special Medicare conditions for psychiatric hospitals within their hospital accreditation program, whether or not they are currently accrediting psychiatric hospitals or have plans to do so in the future.
As part of this proposal, we also required that the AOs that already have an existing CMS-approved hospital program expand their existing hospital programs to include survey activities of psychiatric services in psychiatric hospitals. Those AOs who currently have an approved hospital program would be required to resubmit their standards, survey process and surveyor training for CMS approval in accordance with § 488.8(b) by no later than 30-calendar days from CMS notice to the hospital AOs using the existing process described in § 488.5(a)(19)(i). That process also permits CMS to give due consideration to a request for extension.
We hoped that this would encourage additional AOs to participate in deeming psychiatric hospitals. Overall, the intent of these proposals was to ensure that psychiatric services were evaluated in the context of the larger hospital program evaluation so that systemic quality issues were not missed. A single, comprehensive and focused survey team will be able to identify and connect individual issues and trends which may be occurring under two separate programs. Combining the two programs provides a more global view of the facility's potential deficiencies and is more likely to ensure the overall safety and quality of care delivered. For example, if there were significant issues with staff supervision of patients, one team of surveyors would be investigating areas which now cross the two sets of requirements and survey teams including patient-specific care planning, staff training, patient rights, and potentially governing body. Integrating the survey activities for hospital and psychiatric standards would also provide an avenue for additional AOs to participate in deeming psychiatric hospitals, which would produce more competition and provide facilities with more options for surveying authorities.
The comments and our responses to the comments are set forth below.
Comment:
Two commenters were in support of this proposal. There were no opposing comments.
Response:
We thank the commenters for their support.
Final Decision:
We are finalizing this section as proposed and will issue additional guidance to the AOs, once this rule becomes effective.
CC. Limitation on Terminated Deemed Providers/Suppliers Seeking Re-Entry Into Medicare/Medicaid (§ 489.57, § 488.4(b) and § 488.5(a)(21))
Involuntary termination of the Medicare provider agreement is the ultimate sanction for non-compliance with Medicare's basic health and safety requirements. On average, less than ten involuntary terminations occur each year for deemed providers and suppliers accredited by those AO programs that have a CMS-approved accreditation program. From January 2015 through September 2023, a total of fifty-eight accredited providers and suppliers, including ASCs, ESRD facilities, HHAs, Hospices, Hospitals, RHCs, and OPTs, were involuntarily terminated from the Medicare program for unresolved health and safety concerns. These providers currently have the option of seeking re-approval to participate in Medicare/Medicaid through accreditation by an AO with a CMS-approved program. We remain concerned that providers who have been involuntarily terminated from the Medicare program may continue to remain accredited by an AO and hold their continued accreditation out to the public as a marker of high-quality care. Most consumers, due to branding and advertising by the accredited community, associate quality of care with accreditation, rather than CMS certification of compliance with Medicare requirements. Therefore, involuntarily terminated providers who retain their AO accreditation status convey that they continue to meet high quality of care standards, despite their termination from Medicare. This situation could weaken public trust in accreditation as a marker of patient quality and safety. Since, for an AO that applies for CMS approval of its accreditation program, AO standards are required to meet or exceed those of Medicare, we proposed at § 488.5(a)(21) that termination by Medicare would represent prima facie evidence that the facility similarly failed to meet accreditation standards.
These concerns were highlighted in media reports that noted that psychiatric hospitals terminated from Medicare for harm to patients nonetheless retained their accreditation despite serious health and safety concerns.[20 21]
An article published in the Wall Street Journal (WSJ) on September 8, 2017 [22]
discussed patient-safety problems at three hospitals accredited by one of the AOs that also provides consulting services. These safety issues were so severe that CMS terminated two of the hospitals from the Medicare program. In each of these cases, the AO made no changes in the hospital's accreditation status and allowed it to continue promoting itself as fully accredited, despite being out of compliance with, and therefore no longer deemed to meet, the Medicare safety requirements.
The WSJ article reinforced concerns CMS had previously identified regarding the very small number of facilities that we terminated for failing to meet our basic health and safety regulations, but which nonetheless retained their AO accreditation. Continued accreditation of these outlier facilities, which have received the ultimate sanction CMS may impose based on their ongoing failure to meet basic health and safety requirements, raises serious concerns about the survey integrity and public trust attached to AO accreditation. Therefore, we proposed to explicitly prohibit AOs from allowing terminated facilities to retain their accreditation, to reduce confusion for patients and families about the continued health and safety of terminated entities.
To address the issue of terminated providers or suppliers remaining accredited by an AO, we proposed to add a new regulatory requirement at § 488.4(b) (currently reserved). More specifically, proposed § 488.4(b)(1) would provide that if CMS terminated the participation agreement of a Medicare-certified provider or supplier, under our authority at section 1865(c) of
( printed page 36440)
the Act, we would no longer recognize or accept the accreditation provided by an AO to that provider or supplier as demonstrating that the Medicare requirements have been met by the terminated provider or supplier.
In support of the proposed requirements at § 488.4(b), we also proposed to add a new requirement at § 488.5(a)(21) that would require AOs to provide, with their initial and subsequent renewal applications, a statement certifying that, in response to a written notice from CMS notifying the AO that one of its accredited providers or suppliers has been terminated from the Medicare/Medicaid program, the AO agreed to terminate or revoke its accreditation of the terminated provider or supplier within 5 business days from receipt of said written notice.
The accreditation provided to providers and suppliers by AOs through an applicable CMS-approved AO program permits Medicare participation (in lieu of certification by the SA) only if CMS also approves the AO's recommendation of deemed status for the accredited provider or supplier. Therefore, if a Medicare-certified provider or supplier chooses to obtain accreditation from an AO, and then their Medicare participation is involuntarily terminated after failing to meet the Medicare conditions, we would no longer recognize the validity of the AO's accreditation with respect to that provider/supplier under our oversight authority at section 1865 of the Act. We do not believe that it is appropriate for a terminated provider's or supplier's AO accreditation to remain effective for CMS deeming purposes after we have terminated this provider or supplier for significant deficiencies that the AO may not have cited, discovered, or fully recognized. A terminated provider or supplier may attempt to use the AO's accreditation as a quality marker, when in fact their practices are severely deficient, unsafe, and non-compliant with the CMS conditions.
Under section 1865 of the Act, we may involuntarily terminate CMS approval of an AO's overall deeming authority if they miss egregious deficiencies in one of their accredited provider's or supplier's practices. However, we would prefer to withdraw our recognition of the individual provider's or supplier's deemed status instead and separately work with the AO to determine why such deficiencies went undiscovered.
Proposed § 488.4(b)(2) would provide that, if CMS terminates the participation agreement of a Medicare-certified provider or supplier, the terminated provider or supplier would be required to meet the requirements set forth at § 489.57 before a new agreement for Medicare participation could be approved. We also proposed a new paragraph at § 489.20(z) that reinstatement of a terminated provider or certified supplier agreement would be subject to the proposed revisions to § 489.57.
The introductory text to proposed § 489.57 states that when a provider agreement has been terminated by CMS under § 489.53, or by the OIG under § 489.54, a new agreement with that provider cannot be accepted unless CMS or the OIG, as appropriate, finds that said provider or supplier meets the requirements set forth in § 489.57(a) and (b). We proposed to redesignate § 489.57(a) and (b) as § 489.57(a)(1) and § 489.57(a)(2) without any change to the text. Redesignated § 489.57(a)(1) requires a provider or supplier that has been terminated from the Medicare program to demonstrate that the reason for termination of the previous Medicare provider agreement has been removed and provide reasonable assurance that it will not recur. Redesignated § 489.57(a)(2) requires the terminated provider or supplier to fulfill, or make satisfactory arrangements to fulfill, all of the statutory and regulatory responsibilities of its previous agreement.
We also proposed to add a new paragraph (b) at § 489.57. Proposed § 489.57(b) would provide that before a new agreement for Medicare participation of the terminated provider or supplier is approved, such terminated provider or supplier would have to meet the requirements of proposed § 489.57(b)(1) through (b)(3).
Proposed § 489.57(b)(1) would require that the terminated provider or supplier be under the exclusive oversight of the SA for a reasonable assurance period of a length of time to be determined by CMS, for the purposes of the initial survey, certification and demonstration of compliance with the Medicare conditions. Proposed § 489.57(b)(2) would require that the terminated provider or supplier remain under the exclusive oversight of the SA until the SA or CMS has certified the provider's/supplier's full compliance with all applicable Medicare conditions and their application for participation in the Medicare/Medicaid program had been approved. Finally, proposed § 489.57(b)(3) would provide that, during the time period in which a terminated provider or supplier is not certified to participate in the Medicare program, while the prospective provider or supplier was under the oversight of the State survey agency, and while the new agreement for Medicare participation is pending, CMS would not accept or recognize accreditation from a CMS-approved accrediting organization for deeming purposes until the applicable Medicare requirements had been met or exceeded, as described in § 488.4 of this chapter. Our intent for proposing the new requirements at § 489.57(b) is to ensure that the SA would have the initial survey and certification oversight authority over terminated providers and suppliers seeking re-entry into the program and about which we had significant health and safety concerns. The terminated provider or supplier would remain under the oversight of the SA for a reasonable assurance (RA) period of a duration to be determined by CMS. During the RA period, the terminated provider or supplier would be required to provide reasonable assurance to the SA and CMS that the deficiencies that caused the termination have been rectified and that they are not likely to recur. This means that a terminated provider or supplier would have to use the SA, as opposed to an accrediting organization, to perform their initial participation survey and assessment of compliance before a new agreement for Medicare participation were approved. If, after completion of the reasonable assurance period, the SA found that the provider or supplier met all of the applicable Medicare conditions, it would certify said provider's or supplier's compliance and notify CMS of its findings. CMS would consider the SA's survey findings (certification) in deciding whether to approve or deny the provider's or supplier's new initial certification request for participation in the Medicare program. However, if the SA were to find deficiencies and determine that the provider or supplier did not meet the CMS conditions, the SA could take several courses of action, depending on the severity of the deficiencies. The SA could require the provider or supplier to submit a plan of correction and give the provider or supplier time to correct the deficiencies. The SA would then perform a subsequent survey to see if the deficiencies have been removed and compliance with all requirements has been achieved. If the deficiencies found during the initial SA survey were significant or egregious, the SA would reject the plan of correction and would notify CMS of its findings and recommendation, and then CMS could deny the provider's or supplier's request for new participation in the Medicare program.
( printed page 36441)
The SA cannot recommend certification of a previously terminated provider or supplier that has significant condition or immediate jeopardy level deficiencies, unless these deficiencies are properly and promptly addressed and removed by the provider or supplier. Therefore, the proposed new requirements at § 489.57(b) would provide reasonable assurance to CMS that the significant health and safety concerns that warranted termination of the provider's or supplier's Medicare agreement have been corrected and compliance with all applicable requirements and conditions has been achieved before a new agreement for participation in the Medicare program is approved. We believe that SA oversight during a reasonable assurance period (of a length to be determined by CMS), and SA survey and certification that the terminated provider or supplier now meets the Medicare conditions is a safer alternative to accepting AO survey and deeming of that terminated provider or supplier. This is because in the majority of cases of terminated providers and suppliers, the SA discovered the egregious deficiencies that caused terminations during a validation or complaint survey that took place within 60 days of an AO reaccreditation survey. The AOs that accredited the terminated providers and suppliers had not detected or cited these deficiencies during their surveys.
Section 1865(b) of the Act prohibits disclosure of surveys performed by AOs (with the exception of HHAs, hospice programs, and surveys that relate to an enforcement action taken by the Secretary). However, the proposed new requirements at § 489.57(b) would allow the findings from the compliance surveys performed by the SAs to be made publicly available under our regulations at 42 CFR 401.133(a) and our statutory authority at section 1864(a) of the Act, which states: “within 90 days following the completion of each survey of any healthcare facility, ambulatory surgical center, rural health clinic, comprehensive outpatient rehabilitation facility, laboratory, clinic, agency, or organization by the appropriate State or local agency described in the first sentence of this subsection, the Secretary must make public in readily available form and place, and require (in the case of skilled nursing facilities) the posting in a place readily accessible to patients (and patients' representatives), the pertinent findings of each such survey relating to the compliance of each such healthcare facility, ambulatory surgical center, rural health clinic, comprehensive outpatient rehabilitation facility, laboratory, clinic, agency, or organization with (1) the statutory conditions of participation imposed under this title and (2) the major additional conditions which the Secretary finds necessary in the interest of health and safety of individuals who are furnished care or services by any such healthcare facility, ambulatory surgical center, rural health clinic, comprehensive outpatient rehabilitation facility, laboratory, clinic, agency, or organization”.
Thus, the proposed new requirements at § 489.57(b) would allow for greater transparency regarding the current compliance of terminated healthcare providers and suppliers seeking re-entry into the program.
The requirements at § 488.4(a)(1) and (2) (redesignated as paragraphs § 488.4(a)(3) and (4) in this rule, with minor clarifying changes in the regulatory language) further delineate CMS' authority in accepting or recognizing accreditation from a CMS-approved accrediting organization for deeming purposes. In accordance with § 488.4(a)(1) and (2) (redesignated § 488.4(a)(3) and (4) in this final rule with comment period), when a provider or supplier demonstrates full compliance with all of the accreditation program requirements of the accrediting organization's CMS-approved accreditation program,
the accrediting organization may recommend
that
CMS grant deemed status
to the provider or supplier and
CMS may deem
the provider or supplier to be in compliance with the applicable Medicare conditions or requirements. [Emphasis added] Because CMS has concerns about a provider that was terminated under an AO's oversight to be deemed by that same AO upon re-entry to the Medicare program, CMS may have concerns about approving an AO's recommendation to deem that provider for a period of time after re-entry.
The comments and our responses to the comments are set forth below. We have presented these comments and responses in a topical fashion for clarity.
Comment:
One commenter stated that Indian health facilities are almost exclusively surveyed by CMS surveyors instead of State survey agencies, given their direct government-to-government relationship with the U.S. The commenter stated that Indian health facilities' right to a direct CMS survey and exemption from State health facility licensing was expressly recognized by the Medicare Claims Processing Manual, (CMS Pub, 100-04), Chapter 19, Section 40.2; and codified in the Indian Healthcare Improvement Act, Public Law 94-437, sections 221 and 408 (25 U.S.C. 1621(t) and 1647).
This commenter stated that § 489.57 would place all terminated providers under “exclusive oversight of the State survey agency”, again without stating an exception for Indian health facilities. This commenter also urged that both § 488.9 and § 489.57 be amended to expressly provide that the survey and oversight functions for terminated Indian health facilities be carried out directly by CMS surveyors unless the facility expressly requests otherwise.
Response:
While tribally owned and operated facilities may opt to seek deemed status and accreditation from an AO, State survey agencies performing surveys for CMS act as our agents. CMS is clarifying that surveys will continue to be performed
by or under the
direction of CMS.
Comment:
One commenter believes that a strict process and procedure for investigation should be followed before terminating a provider.
Response:
CMS does not terminate a provider or supplier from the Medicare/Medicaid program unless they have been found to have multiple, serious condition-level deficiencies they have failed to correct after being given opportunities to do so.
CMS does have a procedure for investigating and handling providers and suppliers that have been found to have such serious condition level deficiencies which is set forth in Chapter 2, Sections 2005A4 and 2005B of the SOM. This procedure includes investigation and attempts at correction prior to termination from the Medicare program for healthcare facilities that have been found to have serious deficiencies and non-compliance with the Medicare standards. There are additional termination processes for individual provider types such as hospitals.
Comment:
One commenter supports the proposed requirements, which they described as CMS withdrawing its approval of the accreditation programs of a provider or supplier that is involuntarily terminated by CMS from participation in the Medicare program.
Response:
We thank this commenter for their support of this proposal. However, this commenter seems to misunderstand the terms of this proposal. The commenter stated that CMS would withdraw approval for the
accreditation programs
of any provider or supplier that is involuntarily terminated from the Medicare/Medicaid program. We have actually proposed that CMS would not recognize the
AO accreditation
for any provider or
( printed page 36442)
supplier that is terminated from the Medicare program.
Comment:
One commenter supports the proposed requirement that a terminated provider or supplier must meet all of Medicare/Medicaid standards before a new agreement with that provider or supplier to re-enter participation in the Medicare/Medicaid program will be approved.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter stated for the proposed requirement that a terminated provider or supplier must be under the exclusive oversight of a State Agency or a CMS Regional Office throughout the time they are seeking to remedy past deficiencies and enter a new agreement for Medicare participation can be approved.
Response:
We thank this commenter for their support of this proposal.
Comment:
One commenter believes that it is imperative that all of the suggested changes, if implemented, are randomly and regularly audited to ensure AO compliance.
Response:
We thank this commenter for their comment.
Comment:
One commenter stated significant concerns about our proposal at § 488.5(a)(21) regarding this proposed prohibition and opposes the linkage of provider agreement termination and deemed status through an AO. This commenter stated they believe there is inconsistency and disconnection in this proposed requirement.
This commenter noted that CMS has proposed to require an AO agree to terminate or revoke its accreditation of any of its accredited providers or suppliers that have been terminated from the Medicare program within 5 business days from receipt of a written notice from Medicare notifying them of the termination. This commenter was concerned about providers and suppliers that may voluntarily terminate their Medicare provider agreement and believes that this proposal would imply that such providers or suppliers have failed to meet the CoPs, when that was not the reason for losing deemed status. The commenter voiced concern for the financial impact of losing deemed status as well as reputational impact to such providers and suppliers.
Response:
This proposal applies only to providers and suppliers that have been involuntarily terminated from the Medicare program for serious deficiencies.
Comment:
One commenter requested clarification on how the “reasonable assurance period” is defined.
Response:
Proposed § 489.57(b)(1) would require that the terminated provider or supplier be under the exclusive oversight of the SA for the purposes of the initial certification survey, initial certification and demonstration of compliance with the Medicare conditions. Proposed § 489.57(b)(2) would require that the terminated provider or supplier remain under the exclusive oversight of the SA until the SA had certified the provider's/supplier's full compliance with all applicable Medicare conditions and their application for participation in the Medicare/Medicaid program had been approved. Finally, proposed § 489.57(b)(3) would provide that CMS would not recognize accreditation from a CMS-approved accrediting organization for deeming purposes while the terminated provider or supplier was under the oversight of the SA and its new agreement for Medicare participation was pending. In addition, section 1865(c) of the Act provided that, after termination, the facility “
for such period as may be prescribed in regulations
[may] be deemed not to meet the conditions or requirements the entity has been treated as meeting pursuant to subsection (a)(1).” (Emphasis added). This means that the reasonable assurance period is set by CMS and would last until the SA had certified the provider's/supplier's full compliance with all applicable Medicare conditions and their application for participation in the Medicare/Medicaid program had been approved.
Comment:
One commenter requested clarification on whether the requirement to terminate or revoke accreditation within 5 business days after written notice from Medicare and not re-accredit until CMS has re-approved the provider or supplier applies to both voluntary and involuntary terminations. This commenter stated that they use the term “
voluntary terminations
” for what they consider withdrawals from Medicare and use the term “
involuntary terminations
” for what they consider terminations.
Response:
The proposed requirement at § 488.5(a)(21) would require AOs to terminate or revoke its accreditation of a provider or supplier terminated by CMS within 5 business days from receipt of said written notice of CMS' termination notice to the AO, and not re-accredit the provider until CMS has approved the provider or supplier for participation in Medicare. It would apply only to deemed providers and suppliers that are involuntarily terminated from participation in the Medicare program by CMS for condition-level noncompliance concerns.
Comment:
One commenter requested clarification on the meaning of the term “
receipt
” in the following “within 5 business days from receipt” proposed regulation text for § 488.5(a)(21). The commenter questioned whether “receipt” means the date the termination notification letter is sent by CMS, or if it refers to the date the AO opens/reads the email from CMS. The commenter stated that if the receipt date is 5 business days from when CMS sends the notice, it would be difficult for the AO to meet the deadline. The commenter further recommended that CMS increase this deadline to 10 business days.
Response:
In this final rule with comment period we are clarifying that we are referring to the AO's receipt of said written notice. We believe that the proposed timeframe of five (5) business days (versus five (5) calendar days) provides sufficient time for an AO to notify a terminated provider or supplier of its accreditation termination or revocation by the AO. We interpret the term “
receipt
” to be the date the AO receives the written termination notice from CMS and clarify that we consider the date of receipt for the AO to be 5 business days after the notice is mailed by CMS or immediately upon transmission to the AO via email by CMS.
Comment:
One commenter stated that it will not be possible for an AO to effectively implement and maintain compliance with these requirements unless effective communication is received from CMS, its locations, and Medicare Administrative Contractors (MACs). This is because levels of communication vary among CMS locations and MACs. The commenter stated that if the AOs are not advised by either the facility or CMS in advance of administrative work after provider/supplier submission of an application or post-survey, there could be significant associated burden for the AOs.
Response:
We thank this commenter for their comment and making their concerns known. We will take them under advisement. However, we believe that the only communication required by this proposal would be the communication from CMS to the AO providing notice that one of the AO's accredited providers or suppliers has been terminated from the Medicare program. The AO would be required to terminate its accreditation of this provider of supplier within 5 business days of receipt of this notification.
We further believe that the AO would not need to receive notifications from CMS or the MACs after it revokes or terminates its AO accreditation of the
( printed page 36443)
Medicare-terminated provider or supplier. We say this because after revoking or terminating the accreditation for the Medicare-terminated provider or supplier, proposed § 488.5(a)(21) would prohibit the AOs from providing accreditation to these terminated providers and suppliers while they remain terminated from the Medicare program. It would not be the duty of CMS to notify the AOs when a previously terminated provider or supplier is approved for participation in the Medicare program.
Comment:
One commenter requested additional clarity related to how these notifications would work, related to both notification of termination and notification of reinstated eligibility for deemed status through an AO.
Response:
At this time CMS is still considering how the notification to an AO that its accredited provider or supplier has been terminated from the Medicare program will work. However, we will develop the guidance and process for this notification requirement prior to its implementation.
Comment:
One commenter expressed concern that SAs may not have sufficient resources to meet the additional oversight requirements to ensure that significant health and safety deficiencies have been corrected.
Response:
There are only a few providers and suppliers accredited by AOs for deeming purposes that are terminated from the Medicare program each year (that is, on average, less than 10). As the number of terminations is low, we believe the SAs will have the ability to perform oversight for these terminated providers and suppliers.
Comment:
One commenter requested that we extend the effective date of the proposed requirement at § 488.5(a)(21). This commenter stated that if this proposal is finalized as proposed, they would need time to update their processes, obtain delegated authority from their Board for the prompt processing of such terminations, determine how terminations would be implemented within the AO's IT systems, and estimate cost implications and allocate the necessary funding.
Response:
We agree that the AOs will need time to implement the requirements into their systems and processes. Unless otherwise specified, final rules become effective 60 days after publication. However, we are specifying that the requirements of proposed § 488.5(a)(21) would not become effective until 1 year after the publication date of this final rule with comment period.
Comment:
Multiple commenters supported our proposal to place limitations on terminated providers/suppliers that are seeking re-entry into the Medicare/Medicaid programs.
One commenter stated that they would fully support the proposed processes for re-entry of a terminated deemed provider and supplier into the Medicare program, if the stated reasoning and process remains unchanged. One commenter stated that they “agree with the provision that a Medicare-accredited organization must terminate the contract with Medicare-certified providers and suppliers. This creates more accountability and compliance for Medicare-accredited healthcare facilities”. Another commenter supports the proposed requirement that AOs terminate or suspend the accreditation of providers and suppliers that are involuntarily terminated from the Medicare program within 5 days from being notified of the termination.
One commenter stated that they are generally supportive of the proposals CMS has put forth to strengthen comparability across AOs and between AOs and SAs, as well as the proposed documentation requirements as part of the application process. This commenter stated that they have already taken actions to align with CMS expectations proposed to be codified by the proposed rule.
One commenter supported the proposal that a provider or supplier terminated by Medicare for serious quality and safety deficiencies would also lose its AO accreditation status and remain under the oversight of a State agency, rather than the AO, for a “reasonable assurance period” until they correct the deficiencies which caused their termination by Medicare.
Response:
We thank the commenters for their support of our proposal to place limitations on terminated deemed providers/suppliers seeking re-entry into the Medicare/Medicaid programs.
Final Decision:
After careful consideration of the comments received, we have decided to finalize the revisions to § 489.57 with a minor technical correction to revise § 489.57(b)(3) in this final rule with comment period. Redesignated § 489.57(a)(1), as finalized, requires a provider or supplier that has been terminated from the Medicare program to demonstrate that the reason for termination of the previous Medicare provider agreement has been removed and provide reasonable assurance that it will not recur. Redesignated § 489.57(a)(2) requires the terminated provider or supplier to fulfill, or make satisfactory arrangements to fulfill, all of the statutory and regulatory responsibilities of its previous agreement.
Revised § 489.57(b)(1), as finalized, requires that the terminated provider or supplier be under the exclusive oversight of the SA for the purposes of the initial certification survey, initial certification and demonstration of compliance with the Medicare conditions. Revised § 489.57(b)(2), as finalized, requires that the terminated provider or supplier remain under the exclusive oversight of the SA until the SA had certified the provider's/supplier's full compliance with all applicable Medicare conditions and their application for participation in the Medicare/Medicaid program had been approved. Revised § 489.57(b)(3), as finalized, provides that CMS will not accept or recognize accreditation from a CMS-approved accrediting organization for deeming purposes while the terminated provider or supplier is under the oversight of the SA and its new agreement for Medicare participation is pending. As originally proposed, § 489.57(b)(3) would provide that, “[D]uring the time period in which a terminated provider or supplier is not certified to participate in the Medicare program, while the prospective provider or supplier is under the oversight of the State survey agency, and while the new agreement for Medicare participation is pending, CMS will not accept or recognize
deeming accreditation
from a CMS-approved accrediting organization until the applicable Medicare requirements have been met or exceeded, as described in § 488.4 of this chapter.”
[Emphasis added]
In reviewing the public comments received and preparing our responses to those comments, we recognized that the term used in the proposed rule, “deeming accreditation,” is not the correct term to use with regard to the accreditation provided by an AO to a provider or supplier under a CMS-approved AO program and CMS' subsequent decision to accept that accreditation as evidence to deem the provider or supplier as having met or exceeded the applicable Medicare requirements. “Deeming accreditation” incorrectly implies that a CMS-approved AO program and the AO automatically confer “deemed status” (and the subsequent certification to participate in the Medicare program) when the AO “accredits” the provider or supplier. This term, “deeming accreditation”, is therefore inaccurate because CMS is always the final authority in determining whether such accreditation can be used for “deeming purposes” (that is, having met or exceeded the applicable Medicare
( printed page 36444)
requirements and eligible to be certified for participation the Medicare program). In other words, accreditation of a provider or supplier by an AO for deeming purposes is a recommendation by the AO that CMS may recognize or accept the accreditation as evidence that the provider or supplier has met or exceeded the applicable Medicare requirements. Through this process, CMS either accepts or rejects the AO recommendation to deem the provider or supplier as having met or exceeded the applicable Medicare requirements.
Therefore, in this final rule with comment period we are making a clarifying revision to § 489.57(b)(3) so that it will now read as:
“During the time period in which a terminated provider or supplier is not certified to participate in the Medicare program, while the prospective provider or supplier is under the oversight of the State survey agency, and while the new agreement for Medicare participation is pending,
CMS will not accept or recognize accreditation from a CMS-approved accrediting organization for deeming purposes
until the applicable Medicare requirements have been met or exceeded, as described in § 488.4 of this chapter.”
[Emphasis added]
We are finalizing as proposed the new paragraph added at § 489.20(z), which states that reinstatement of a terminated provider or certified supplier agreement is subject to the proposed revision to § 489.57.
We are also finalizing as proposed § 488.4(b)(1) and (2), which provide that if CMS terminates the participation agreement of a Medicare-certified provider or supplier, under our authority at section 1865(c) of the Act, we will no longer recognize or accept the accreditation provided by an AO as evidence that the Medicare requirements have been met or exceeded for that terminated provider or supplier, and that the terminated provider or supplier must meet all requirements set forth at 42 CFR 489.57 before a new agreement with that provider or supplier for Medicare participation will be approved.
Finally, we are finalizing § 488.5(a)(21), as proposed, which would require AOs to provide, with their initial and subsequent renewal applications, a statement certifying that, in response to a written notice from CMS notifying the AO that one of its accredited providers or suppliers has been terminated from the Medicare/Medicaid program, the AO agrees to terminate or revoke its accreditation of the terminated provider or supplier within 5 business days from receipt of said written notice from CMS.
However, as we have stated elsewhere in this final rule with comment period, and for the reasons we have provided, we have modified the proposed provisions by removing any sentence or phrase from the applicable regulations text stating that a particular provision(s) will become applicable 1 year after the effective date of this final rule with comment period, or any similar language to that effect. For this final rule with comment period, we are making a modification that all provisions of the rule will become effective 1 (one) year after the publication of this rule.
DD. Finalizing Technical Correction for End-Stage Renal Disease (ESRD) Facilities and Kidney Transplant Programs (§ 488.4(a)(4))
Section 1865(a)(1) of the Act had historically excluded dialysis facilities from participating in Medicare via a CMS-approved accreditation program; however, section 50403 of the Bipartisan Budget Act of 2018 amended section 1865(a) of the Act to include renal dialysis facilities as provider entities allowed to participate in Medicare through a CMS-approved accreditation program. Section 50403 also removed a reference to section 1881(b) of the Act, which had prevented kidney transplant programs from being accredited via CMS-approved accreditation programs. However, CMS' existing regulations at § 488.4(a)(2) continue to exclude kidney transplant programs from participation in Medicare through accreditation, in direct conflict with the Bipartisan Budget Act of 2018 amendment. We therefore proposed to remove the exclusion specifically in our accreditation regulations, currently codified under § 488.4(a)(2) and redesignated in this final rule with comment period as § 488.4(a)(4), to align with the statutory changes implemented the Bipartisan Budget Act of 2018.
Final Decision:
We received no comments related to this technical correction and are hereby finalizing this correction within the regulatory provisions.
IV. Information Regarding Timeframes and Expectation for the Submission of AO Applications
We requested public comments on the timeframes and expectation for the submission of applications submitted by AOs, because our existing AO oversight regulations do not restrict how many times an AO may submit an initial application to CMS for review. Based on our initial review of an application for completeness, which verifies the AO has submitted all required elements under § 488.5, we often find the application to be incomplete and must return it to the AO for additional clarifications, missing items or revisions. CMS also receives applications that require multiple pass-backs due to the applicant's failure to provide complete information about issues, such as their financial viability, survey processes which appeared not to be operationalized, or similar concerns. Our existing regulations do not limit the number of times an AO may submit an application for review by CMS. It is possible that incomplete applications could be submitted an unlimited number of times.
Therefore, we solicited public comments on the following possible future limitations to the submission of applications by the AOs that accredit Medicare-certified providers and suppliers:
An AO may only re-submit an application for CMS re-review two additional times after CMS initially deems the application to be “incomplete”.
If the AO's application is found by CMS to be incomplete after the third submission, the AO must wait a minimum of 2 years before resubmitting the entire application for CMS consideration.
We received two comments related to our request for information.
Comment:
One commenter stated that while the commenter's organization recognizes the resource demand for reviews of an application by CMS, the commenter disagreed with placing limitations on the number of reviews. The commenter suggested this is particularly concerning with an organization applying for the first time. Alternatively, the commenter suggested that limitations be placed on the number of times an organization may change their point of contact for consistent communications. Further, the commenter stated that should CMS seek to impose a term of limitation, the commenter's organization recommends an additional four rounds (five total submissions) and the timeframe for reapplication to be decreased to 1 year.
Response:
We appreciate the commenter's suggestion and raised concerns. We do note that we believe this commenter may have not fully understood the proposal requesting information. The intent of the proposal is primarily geared toward new organizations wishing to apply for deeming authority, not those of our existing CMS-approved AOs. Over recent years, several organizations have applied for initial CMS-approval to become recognized for deeming
( printed page 36445)
authority but have failed to meet the requirements § 488.5. Some of the organizations failed to demonstrate their ability to have comparable survey processes to those of the SAs, including not reflecting the requirements outlined in our SOM program-specific appendices. Some other areas which led to CMS determine that initial reviews were incomplete were that the applicant organizations did not document accreditation decision making processes, sufficient staff, or financial support to be able to grow the organization to be a national organization; or did not provide evidence of having sufficient data systems. CMS expects organizations who wish to become an AO to be prepared to meet the requirements for submission of an application as outlined in the regulations. Further, we note one application may be in excess of 2,000 pages and in the event of four applications in 1 year a review of over 8,000 pages to determine an organization still does not meet the intent to be recognized for deeming authority greatly strains our limited resources.
Comment:
One commenter did not support our proposal to limit the number of AO applications. The commenter stated it is crucial to recognize that addressing issues comprehensively may require time, especially considering the complexity of healthcare. The commenter suggested we take a flexible approach where multiple opportunities for corrective action are provided. The commenter believes that there should be more room for individualization and that CMS should take into account unique circumstances, leading to more effective and equitable outcomes in the accreditation process.
Response:
We appreciate the concerns; however, we believe the commenter may have not understood the proposal. The intent to limit the number of applications is not directly correlated with healthcare facilities but with AOs themselves. AOs must initially apply for CMS-deeming authority and reapply at least every 6 years. Once received, CMS does the following: (1) conducts a thorough review of the application for evidence organization's ability to meet or exceed the Medicare standards; (2) assesses comparability of survey processes; (3) reviews survey files, complaint files, surveyor training and educational materials; and (4) performs an onsite evaluation of the AOs surveying a deemed facility. This process is required to be completed within 210-days of receipt of an organization's complete application. One application may range from 2,000 to 5,000 pages of policies and guidance alone. In general, this provision is unlikely to impact existing CMS-approved AOs, as the nine approved AOs are familiar with CMS evaluation and application process. The intent of this provision is to limit the number of times that a new accrediting organization can submit an application to CMS. Every application received by CMS starts a 210-day timeclock once deemed complete. What CMS has found is that new organizations may apply four or even up to eight times per year. Even after these ample opportunities to meet our requirements, these applicants have subsequently been denied deeming authority due to a lack of understanding of the requirements, documentation, failure to meet the requirements, financial viability, etc. By limiting the number of times an application can be reviewed by CMS, we can prioritize our workload more effectively.
We appreciate the two commenters input on this request for information. We will take these comments into consideration for future rulemaking.
V. Severability of Provisions
To the extent a court may enjoin any part of the rule as finalized, the Department intends that other provisions or parts of provisions should remain in effect. Any provision of the rule as finalized held to be invalid or unenforceable by its terms, or as applied to any person or circumstance, shall be construed so as to continue to give maximum effect to the provision permitted by law, unless such holding shall be one of utter invalidity or unenforceability, in which event the provision shall be severable from this section and shall not affect the remainder thereof or the application of the provision to persons not similarly situated or to dissimilar circumstances.
We note here that virtually all of the provisions in this final rule with comment period are inherently severable, with the exception of a few areas of the rule that are dependent upon each other, where such provisions describe procedures and deadlines for the completion of activities and the submission of materials required by this rule. For example, the overall structure of 42 CFR 488.5(a) through (e), describing the steps necessary to submit and receive approval of an accreditation program application, would not be severable to the extent that all steps in general of the process are needed in order to result in an approved entity. However, the individual items of information enumerated and being finalized in this rule at § 488.5(a), which describe the range of information that must be included in any application and re-application by a national accrediting organization for CMS approval of a specific accreditation program, are severable from each other because one impermissible requirement would not void the intent of an AO's application/re-application package submitted to CMS or make a decision impossible. This example is provided here to be illustrative of this final rule with comment periods' provisions that are not inherently severable, and it is not intended to be an exhaustive list of the provisions that are not severable in this rule.
VI. Collection of Information Requirements
Under the Paperwork Reduction Act of 1995 (PRA), 44 U.S.C. 3501-3520, we are required to provide notice in the
Federal Register
and solicit public comment before a collection of information requirement is submitted to the Office of Management and Budget (OMB) for review and approval. To fairly evaluate whether an information collection should be approved by OMB, 44 U.S.C. 3506(c)(2)(A) requires that we solicit comment on the following issues:
The need for the information collection and its usefulness in carrying out the proper functions of our agency.
The accuracy of our estimate of the information collection burden.
The quality, utility, and clarity of the information to be collected.
Recommendations to minimize the information collection burden on the affected public, including the use of automated collection techniques.
Wage Data
To derive average costs, we used data from the U.S. Bureau of Labor Statistics' May 2024 National Occupational Employment and Wage Estimates for all salary estimates (
https://data.bls.gov/oesprofile/). In this regard, Table 3 presents the mean hourly wage, the cost of fringe benefits and overhead (calculated at 100 percent of salary), and the adjusted hourly wage.
( printed page 36446)
Table 3—U.S. Bureau of Labor Statistics 2024 Wage Rates 23
A. Information Collection Requirements (ICRs) Related to Conflict-of-Interest Requirements
In this final rule with comment period, we are finalizing several requirements related to AO and AO surveyor conflicts of interest. We will address the cost and time burden associated with each of these requirements separately.
1. ICR Related to Conflict-of-Interest Policies & Procedures AOs Must Submit to CMS (§ 488.5(a)(10))
We are modifying § 488.5(a)(10) to add a requirement that the AOs must provide specific information with their conflict-of-interest policies and procedures with the application they submit to CMS. Specifically, the AO must submit the following policies and procedures: (1) the AO's policies and procedures for separation of its consulting services from its accreditation services; (2) policies and procedures for protecting the integrity of the AO's accreditation program, including the requirements of §§ 488.8(i) and (k); (3) policies and procedures for the prevention and handling of potential or actual conflicts of interest that could arise from situations in which an AO owner, surveyor, or other employee has a direct interest in or relationship with a State survey agency or with a healthcare facility to which the AO provides accreditation services, including being employed as an SA surveyor or having an ownership interest in a healthcare facility, etc.; and (4) policies and procedures for notification of CMS when a conflict of interest is discovered.
The AO would need to modify their current conflict-of-interest policies and procedures to include the previously stated information required under the revisions to § 488.5(a)(10). We estimate that this task would be performed by a team of at least two AO staff members. The AO staff that would most likely perform this task would be a person whose background is an RN or a health or medical services manager. According to the 2024 U.S Bureau of Labor statistics, the mean hourly wage for an RN is $47.32. This wage adjusted for the employer's fringe benefits and overhead would be $94.64. According to the U.S Bureau of Labor statistics, the mean hourly wages for a medical or health services manager is $66.22. This wage adjusted for the employer's fringe benefits and overhead would be $132.44.
We estimate that it would be at least two persons working in a full-time basis for 3 days for the AO staff to revise their conflict-of-interest policies and procedures to add the required information. Therefore, we estimate that the total time required for the two team members to perform this task would be 48 hours (8 hours × 3 days = 24 hours per each person × 2 persons = 48 hours).
As of June 23, 2025, there are 9 AOs that accredit Medicare-certified providers and suppliers. We estimate that the total time burden across these 9 AOs would be 432 hours (48 hours × 9 AOs).
We estimate that the cost burden related to the work performed by the RNs on the team would be $2,271.36 (24 hours × $94.64). We estimate that the cost burden related to the work performed by the medical or health services manager on the team would be $3,178.56 (24 hours × $132.44). Finally, we estimate that the total burden costs related to the requirements for § 488.5(a)(10) would be $5,449.92 per AO ($2,271.36 + $3,178.56). The total cost across the 9 AOs that accredit Medicare-certified providers and suppliers is $49,049.28 (9 AOs × $5,449.92).
We believe that the stated burden would be incurred by the AO once prior to the time that they submit their first application after this requirement becomes effective. However, we believe that after the AOs have made required modifications to their conflict-of-interest policies, they will not have to revise them again but will submit the same revised conflict-of-interest policies approximately every 6 years with their renewal applications, so this burden would not be incurred again. We do not count the burden related to the submission of the application because the AO would be required to submit the application approximately every 6 years to renew the CMS approval for their accreditation programs.
Comment:
One commenter stated that CMS' time and cost estimates also fail to account for the areas in the proposed rule where current information sharing requirements still allow CMS to achieve its oversight objectives. For example, in the proposed changes (for example, proposed changes at § 488.5(a)(10)(i through iv); § 488.5(a)(22); and § 488.8(i)(5)), CMS has not offered a reasoned explanation for concluding that oversight aims are not met with the current documentation requirements. As a result, the current requirements serve
( printed page 36447)
as a less burdensome means of achieving comparable goals.
Response:
We respectfully disagree with this commenter's contention that CMS' current information sharing requirements still allow CMS to achieve its oversight objectives. We further disagree with this commenter's contention that CMS has not offered a reasoned explanation for concluding that oversight aims are not met with the current documentation requirements and that the proposed changes at § 488.5(a)(10) (i through iv); § 488.5(a)(22); and 488.8(i)(5) are not necessary.
In the proposed rule. we provided ample rationale for our proposed changes at § 488.5(a)(10) (i through iv); § 488.5(a)(22); and 488.8(i)(5), such as making the existing requirements more specific (84 FR 12006 through 12010).
As we have ample justification for our proposed changes, there is no need for CMS to “account for the areas in the proposed rule where current information sharing requirements still allow CMS to achieve its oversight objectives,” as requested by the commenter.
2. ICR Related to Requirement That the AOs Submit Surveyor Declarations to CMS Upon Request and During Application Review Process (§ 488.5(a)(22))
We are adding a new paragraph (22) to § 488.5(a), which would require that the AO submit a declaration by each surveyor of any outside interests or relationships with the healthcare facilities that the AO accredits. This section would also require that the surveyor declarations must be updated and submitted to CMS upon request and during each application review process.
There would be a time and cost burden to the AO for having to collect declarations from each of their surveyors upon CMS request and during each application review process, which is currently every 6 years or less. There would also be a time and cost burden to the AO for the submission of the surveyor declarations to CMS.
We estimate that it would take at least two persons working on a full-time basis for 3 days (8 hours per day) to prepare the surveyor declarations, get each AO surveyor to complete a declaration and submit them to CMS. This would equate to 24 hours per person or 48 hours across both staff performing this task.
We believe that the AO staff that would be performing these tasks would be an RN and a management staff person, whose job duties meets the description of the U.S. Bureau of Labor Statistics job of category of health and medical services manager. As stated previously, the adjusted mean hourly wage for an RN is $94.64. The adjusted mean hourly wage for a medical and health services manager is $132.44.
We estimate that the time burden for this task per each AO would be 48 hours (24 hours × 2 staff persons). We further estimate that the total time burden across all 9 AOs that accredit Medicare-certified providers and supplier would be 432 hours (48 hours × 9 AOs).
We estimate that the cost burden related to the work performed by the RN would be $2,271.36 (24 hours × $94.64). We estimate that the cost burden related to the work performed by the medical or health services manager would be $3,178.56 (24 hours × $132.44). Finally, we estimate that the cost burden associated with the requirements for § 488.5(a)(22) per each AO would be $5,449.92 per AO ($2,271.36 + $3,178.56) if each had to submit these declarations annually. According to this requirement, CMS can request these submissions at any time from each AO, including annually. However, we expect that AOs will only have to submit surveyor declarations during each application review process, which generally occurs every 3 to 6 years, and as required under this provision. To estimate the total annual cost burden across the nine AOs that accredit Medicare-certified providers and suppliers for these submissions, we used the average of the every-3-to-6-years range for the AO application process. This resulted in an average of every 5 years (rounded up from 4.5 years) for each AO's period between application processes and its submission of the required surveyor declarations at a cost of $5,449.92 per AO (or $49,049.28 across 9 AOs) every 5 years, or $1,090 distributed annually per AO ($5,449.92/5 years = $1,090), or $9,810 across 9 AOs annually.
3. ICR Related to Requirement for Submission of Information About AO Fee-Based Consulting Services Provided (§ 488.8(i)(5))
We proposed a requirement at § 488.8(i)(5) that would require the AOs to provide CMS with the following information about the fee-based consulting services they provide to CMS on a bi-annual basis: (1) whether the AO or its fee-based consulting division or separate business entity (such as a company or corporation that provides fee-based consulting) provides fee-based consulting services; (2) the names and CCN numbers of all healthcare providers and suppliers to which the accrediting organization or its associated consulting division or company has provided fee-based consulting services during the previous 6-month period; (3) the dates the AO fee-based consulting services were provided to each provider and supplier; (4) whether the accrediting organization has, at any time in the past provided, or is currently providing, accreditation services to each healthcare provider or supplier listed in said document; (5) for each healthcare provider and supplier listed in said document, the date of the most recent accreditation survey performed, and the date the next re-accreditation survey is due to be performed; and (6) a description of the AO fee-based consulting services provided to each healthcare provider or supplier listed in said document.
The proposed regulation would further require that the document containing the information required by § 488.8(i)(5)(i) through (i)(5)(vi) must be submitted to CMS every 6 months.
Based on the public comments received on this proposed requirement, we are finalizing the requirements with a modification to require submission of the document to CMS upon request by CMS and during each application review process. We believe that this change in the requirements will be less burdensome for AOs while still providing CMS with the necessary information to maintain our AO oversight responsibilities.
We estimate that the burden associated with this requirement would include the time and costs associated with the gathering of the information necessary to prepare the required document, the time required to draft and update the document, and the time required to send the document to CMS. This burden would occur initially with the additional burden of updating the information when applicable. We would expect that AOs would most likely update the information on a yearly basis to keep the information as up to date as possible by documenting it on an ongoing basis.
We believe that the burden would be greater for the preparation of the first report. Thereafter, the AOs would have already prepared and formatted this report and would simply have to update the information prior to submitting to CMS upon request or prior to the beginning of each application review process.
We estimate that it would require at least two persons working on a full-time basis for 3 days to prepare and submit the first required statement to be submitted CMS. We further estimate that this team would consist of one RN and one Medical or Health Service Manager. Therefore, we estimate that
( printed page 36448)
the total hourly time burden for each team member would be 24 hours (3 days × 8 hours per AO staff member).
We estimate that the time burden per each AO for the work performed by the two AO staff members to prepare each report would be 48 hours (2 team members × 8 hours × 3 days). The total initial time burden per each AO would be 48 hours (1 report × 48 hours).
This provision would apply to all 9 AOs that accredit Medicare-certified providers and suppliers because it would require each AO to, at a minimum, respond to the requirement at § 488.8(i)(5)(i), which asks whether the AO or an associated consulting division or company established by the AO provides consulting services. Those AOs, or associated consulting divisions or companies, that do not provide any type of consulting or consulting services would simply respond in the negative to this question and would not have to provide any further information.
The time and cost burden to the AOs that do not provide consulting would be negligible because they would send this notice to CMS via email. This task would take an AO staff member less than a minute to complete and submit to CMS upon request or prior to when each application review process begins. Therefore, as this task is so minimal, we have not assessed burden for this task for the AOs that do not provide consulting services.
The cost burden related to the work performed by RNs on the team would be $2,271.36 (24 hours × $94.64 per hour). The cost burden for the work performed by the medical or health services manager would be $3,178.56 per each AO (24 hours × $132.44). The total estimated cost burden per each AO would be $5,449.92 ($2,271.36 + $3,178.56). The total estimated cost burden if all 9 AOs provided consulting services would be $49,049.28 ($5,449.92 × 9 AOs).
We believe that the previously mentioned time and cost burdens would be incurred by the AOs that provide consulting services only the first time that they prepare the required document and send it to CMS. We believe that after the AO has prepared their first report, they would have this report in an electronic format on their computers. Therefore, for the second and each subsequent report, we estimate that the preparation and submission of this report would only require the work of one RN and the time for that one RN would be reduced by at least two-thirds. This means that it would take only one RN a period of 8 hours to prepare the required statement and submit it to CMS. We estimate that the total time burden across all nine AOs (based on either those that currently provide consulting services or might provide such services in the future) would be 72 hours (8 hours × 9 AOs).
We estimate that the cost burden per each AO related to the work performed by an RN to prepare the second or subsequent report would be $757.12 (8 hours × $94.64). The total cost burden across all nine AOs would be $6,814.08 ($757.12 × 9 AOs).
4. ICR Related to Requirement That Accrediting Organization Establish Fee-Based Consulting Firewall Policies and Procedures (§ 488.8(j))
We proposed at § 488.8(j) to require that an AO, its consulting division, or separate business entity, such as a company or corporation that provides fee-based consulting services to the healthcare providers and suppliers the accrediting organization accredits, must have written fee-based consulting firewall policies and procedures, which, at a minimum, include the following provisions: (1) the AO's fee-based consulting services must be provided by a separate division or company from the AO's accreditation division; (2) the AO's fee-based consulting division or separate company must maintain separate staff from that of the AO's accreditation divisions to ensure that the fee-based consulting division staff do not perform AO's accreditation division functions and that the AO's accreditation division staff do not perform fee-based consulting division functions; and (3) the AO's accreditation staff and surveyors are prohibited from marketing the AO's fee-based consulting services to the AO's accreditation clients. As we have noted elsewhere in this final rule with comment period, we are removing the proposed term, “fee-based”, from the requirements of this section.
This requirement would only apply to the AOs that provide consulting services and would require these AOs establish new consulting firewall policies and procedures or revise their current policies and procedures to meet the requirements. It is our understanding, from review of the comments submitted by the AOs in response to the AO Conflict-of-Interest RFI, that these AOs already have such consulting firewall policies and procedures in place. If this is the case, then the time and cost burden associated with revising these policies and procedures would not be extensive.
In section VII.A.5. of the proposed rule, we estimated that it would take each AO that provides fee-based consulting services 80 hours to revise their consulting business documents, such as their business charter, business documents, employee training information, informational documents that are distributed to prospective clients, and their policies and procedures.
For this final rule with comment period, we estimate that the total time burden across all nine AOs (based on either those that currently provide consulting services or might provide such services in the future) would be 720 hours (80 hours for each AO). We estimate that it would require at least two people working on a full-time basis for 5 days (or 40 hours for each staff member) to prepare and submit the first required statement to be submitted CMS. We further estimate that this team would consist of one RN and one Medical or Health Service Manager. Therefore, we estimate that the total hourly time burden for each team member would be 24 hours (3 days × 8 hours per AO staff member).
We estimate that the time burden per each AO for the work performed by the two AO staff members to prepare each report would be 48 hours (2 team members × 8 hours × 3 days). The total initial time burden per each AO would be 48 hours (1 report × 48 hours). However, we believe the time and cost burden associated with this requirement is included with the burden calculation for 488.8(i).
Comment:
One commenter stated that they already maintain an effective conflict-of-interest requirement approved by CMS. This commenter stated that if the conflict-of-interest changes at § 488.8(k) are implemented as proposed, the structure of the AO's accreditation decision committee reviews would need to be reorganized in a manner that fully complies with the prohibition from having contact with or access to survey and accreditation records. Additionally, all current conflict-of-interest forms and disclosures will need to be updated and revised. Additionally, the size and structure of each AO with deeming authority varies greatly.
Many of the estimations based on assumed size, employment structure, and personnel count that have been presented by CMS throughout the ICR significantly understate the amount of investment that would be required.
Response:
We are not privy to much of the AOs' business information. Because of this, we have had to use estimates in preparing our burden costs for the ICRs here.
( printed page 36449)
B. ICR Associated With the Requirement That AOs Provide Detailed Crosswalks Identifying Incorporation of the CMS Standards
At § 488.5(a)(3), we will require AOs to incorporate the language of the CMS' Medicare conditions and provide CMS with a detailed crosswalk. While AOs are required to provide a similar crosswalk under the existing process, CMS previously only required a “comparable” standard, therefore through this new requirement, AOs will need to recreate their AO standards to incorporate the Medicare condition language into their accreditation standards for their accreditation programs. We also note that this will require a one-time overhaul of AO standards and the cost burden would be imposed for the first year following the effective date of this rule and not be a reoccurring annual burden. Burden costs subsequent to changes to the conditions made by CMS through future rulemaking would remain as current practice with updates required to be reviewed and approved as outlined in existing § 488.5.
We would expect that the AOs will use the existing CFR language they are required to crosswalk currently and assign an AO standard number or realign their existing AO standards in a manner which would allow for a one-to-one comparison to ensure their accreditation standards incorporate the CFR language. As previously noted, CMS is not restricting the AOs from exceeding the Medicare conditions. However, if the AO exceeded our standards, the AO would need to provide additional language or clearly delineate the exceeding language. For example, we would anticipate that the format used be similar to the one seen in Table 4.
Table 4—Example of Proposed Crosswalk
CFR citation and survey tag
Medicare conditions language
AO standard No.
AO standards language
§ 482.13(h) A-0215
Patient visitation rights. A hospital must have written policies and procedures regarding the visitation rights of patients, including those setting forth any clinically necessary or reasonable restriction or limitation that the hospital may need to place on such rights and the reasons for the clinical restriction or limitation
XX.000
Same as CMS.
Patient visitation rights. A hospital must have written policies and procedures regarding the visitation rights of patients, including those setting forth any clinically necessary or reasonable restriction or limitation that the hospital may need to place on such rights and the reasons for the clinical restriction or limitation.
XX.0001
Exceeds: The hospital must update these written policies on an annual basis with Governing body approval.
We anticipate that the AOs for each program type (that is, hospice, home health, outpatient physical therapy, hospitals, ESRD facilities, RHC, CAH, ASCs, psychiatric hospitals) for which the AO has deeming authority would be required to review and revise their existing crosswalk and standards into the required format. We further anticipate that the review and updating of AO standards crosswalk would be done by AO staff consisting of at least one RN and a medical secretary.
We estimate that the RN would spend 2 hours performing this task. We further estimate that a medical secretary would spend 198 hours performing this task. Therefore, the total time burden per each AO for this task would be 200 hours for each AO program. (2 hours per 1 RN + 198 hours per 1 medical secretary).
The adjusted mean hourly wage for an RN is $94.64. We estimate that the cost for the work performed by the RN to perform the work on this task would be $189.28 (2 hours × $94.64).
The adjusted mean hourly wage for a medical secretary is $43.82. We estimate that the cost burden for the work performed by the medical secretary on this task would be $8,676.36 (198 hours × $43.82). The total estimated cost burden for all work performed on this task would be $8,865.64 ($189.28 + $8,676.36).
CMS has 29 approved accreditation programs across nine AOs (as of 2026) for the eight distinct provider and supplier types:
Ambulatory Surgical Centers (ASCs) (five AOs with CMS-approved programs)
Critical Access Hospitals (CAHs) (four AOs with CMS-approved programs)
Hospitals (including Psychiatric Hospitals) (four AOs with CMS-approved programs)
Home Health Agencies (HHAs) (three AOs with CMS-approved programs)
Hospices (3 three AOs with CMS-approved programs)
End-Stage Renal Disease (ESRD) Facilities (two AOs with CMS-approved programs)
Rural Health Clinics (RHCs) (three AOs with CMS-approved programs)
Transplant Centers (four AOs with CMS-approved programs)
Outpatient Physical Therapy/Speech Pathology (OPT/SP) (one AO with a CMS-approved program)
This requirement applies only to those AOs that accredit Medicare-certified providers and suppliers for deeming purposes. There are 9 AOs that accredit Medicare-certified providers and suppliers through 29 CMS-approved accreditation programs. Therefore, the one-time, first-year cost burden for each of the 9 AOs for one program only would be $8,865.64. The number of approved programs for each AO ranges from one to six. There are currently 3 AOs that have 1 approved program each (one-time, first-year cost burden for each of these 3 AOs would be $8,865.64); 2 AOs that have 2 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $17,731.28); 2 AOs that have 3 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $26,596.92); and 2 AOs that have 6 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $53,193.84).
With 29 total programs across 9 AOs, we assumed an average of 3 programs per AO (29/9 = 3.2 or 3) and an average one-time, first-year cost burden of $26,598 per AO (3 programs per AO × $8,866 cost burden per program = $26,598).
C. ICRs Associated With the Requirement That AOs Use Survey Processes That Are Comparable to That Used by CMS and the SAs
The requirements from § 488.5(a)(4) through (13) will require the AOs to submit revised initial and renewal application information supporting comparability in the survey processes
( printed page 36450)
and guidance established by CMS and used by the SA. However, we note that while additional regulatory language changes are being made under § 488.5(a)(4) through (13), AOs are already required to submit this type of documentation. Our intent is to clarify in regulation the minimum standards and required documentation that AOs show comparability to CMS survey process, forms, guidelines, and instructions to surveyors.
1. ICR Related to Revised Documentation Submission Requirements Imposed by Requirements That AOs Use Comparable Survey Process at § 488.5(a)(13)
The requirements under § 488.5(a)(13) will require AOs to submit specific information on the AOs' notification procedures, including timeframes for notification, to CMS in regard to a facility which the AO accredits if the facility fails to meet accreditation standards or its accreditation status is affected, as part of the documentation currently required under § 488.5(a)(13). Furthermore, the existing requirements currently require the AOs to have: (1) procedures for responding and investigating complaints; and (2) a process for decision-making as it relates to accrediting status. In addition to the added requirement, we are also adding a requirement that AOs must submit documentation regarding the AO's process for facilities that withdraw from accreditation, including notification procedures.
We believe this review and revision would be conducted by one RN, one general healthcare support member, one medical secretary, and the CEO to develop these procedures, review and approve all changes. The adjusted mean hourly wage for an RN is $94.64. The adjusted mean hourly wage for a healthcare support staff person is $46.88. The adjusted mean hourly wage for a medical secretary is $43.82. The adjusted mean hourly wage for a CEO is $252.82.
We anticipate it would take approximately 5 hours for the AO staff to review the new requirements set forth in this final rule with comment period and to determine what changes need to be made to their standards, policies and procedures. We also estimate that it would take an additional 5 hours for the AO staff to make the revisions required to align their accreditation standards and policies and procedures with our revisions. Therefore, the total estimated time burden for each AO would be 10 hours.
This requirement applies to the 9 AOs (as of 2026) that accredit Medicare-certified providers and suppliers. Therefore, the total time burden across these 9 AOs would be 90 hours (10 hours × 9 AOs).
As stated, we believe that the AO staff that would perform this task would consist of an RN, a healthcare support staff person, a medical secretary, and the AO's CEO to review and approve all changes. We estimate that the cost burden for the work performed by the RN would be $236.60 (2.5 hours × $94.64 per hour). We estimate that the cost burden for the work performed by the healthcare support staff person would be $117.20 (2.5 hours × $46.88). We estimate that the cost burden for the work performed by the medical secretary would be $109.55 (2.5 hours × $43.82). We estimate that the cost burden for the work performed by the CEO would be $632.05 (2.5 hours × $252.82).
We estimate that the total cost burden for each AO for this task would be $1,095.40 ($236.60 + $117.20 + $109.55 + $632.05). The burden across the 9 AOs that accredit Medicare-certified providers and suppliers would be $9,858.60 ($1,095.40 × 9 AOs).
2. ICR Associated With the Requirement That the AOs Provide Documentation to CMS About Its Staff Training Programs for Its Revised Survey Process (§ 488.5(a)(4)(xi))
The requirement at § 488.5(a)(4)(xi) will require the AO to submit documentation summarizing its staff training programs, either web-based or hard copy training materials, to CMS, on how the AO provides training or education to surveyors on the AO's survey processes, and, where applicable, highlight differences from CMS survey processes.
As AOs currently have existing training for their surveyors on their survey processes, we believe that the preparation of these materials would only require the AOs to extrapolate what they believe are the core differences between the CMS survey process and those of their respective organizations.
We believe it would take approximately 5 hours for the review of the current AO processes and approximately 25 hours to develop an abbreviated course of their survey processes for their accredited programs. We believe that the persons at the AO who would perform these tasks would be two RNs and a medical secretary. We estimate that each RN would spend approximately 25 hours performing the required work. We further estimate that the medical secretary would spend 5 hours performing work on this task. The adjusted mean hourly wage for an RN is $94.64. The adjusted mean hourly wage for a medical secretary is $43.82.
We estimate that the total time burden for each AO would be 55 hours. This provision would apply to all 9 AOs that accredit Medicare-certified providers and suppliers. Therefore, the estimated total annual time burden for these tasks would be 495 hours (55 hours × 9 AOs) We estimate that the cost burden to each AO for the work performed by the RNs would be $4,732 ($94.64 × 50 hours). We further estimate that the cost burden to each AO for the work performed by the medical secretary would be $219.10 ($43.82 × 5 hours). The total estimated cost burden for each AO for this task would be $4,951.10 ($4,732 + $219.10).
This requirement will apply to all 9 AOs that accredit Medicare-certified providers and suppliers for deeming purposes. Therefore, we estimate that the total cost would be $44,559.90 ($4,951.10 × 9).
3. ICR Related to Requirement for AO To Submit Survey Findings/Reports
As mentioned in section IV.C. of the proposed rule, we also proposed to require the AOs as part of their application under § 488.5(a)(4)(viii) to acknowledge that it will submit any requested survey findings and reports, to include complaint survey reports to CMS for internal use.
This requirement would not cause the AOs to incur any new additional burden as the submission of this information is already required by this regulation and is therefore a usual and customary component of initial and renewal applications. AOs are also already required to submit the deficiencies and facility non-compliance in a roll-up format. Therefore, this proposed requirement for a full survey report could potentially be seen as a burden reduction as CMS would not require a specific new entry or format and reduce time spent by the AO summarizing the survey activity.
4. ICR Related to Documentation Requirements for Submission to CMS for Approval of the AOs' Revised Accreditation Standards and Survey Process (§ 488.8(b))
The AOs will be required to resubmit their new survey processes and standards for a comparability review as required by § 488.8(b)(1).
We believe that the AO staff that would work on this task would be a medical secretary. We believe that the medical secretary would gather all required documents, complete the compilation of documents and
( printed page 36451)
verification. The adjusted mean hourly wage for a medical secretary is $43.82.
We anticipate the total burden hours for each AOs to compile each accreditation program and the revisions as required within §§ 488.4(a)(1) and 488.4(a)(2) for a resubmission to CMS for review and approval would be 80 hours. The total estimated cost burden for each AO program would be $3,505.60 (80 hours × $43.82).
CMS currently has 29 approved accreditation programs across nine AOs (as of 2026) for the eight distinct provider and supplier types:
Ambulatory Surgical Centers (ASCs) (five AOs with CMS-approved programs)
Critical Access Hospitals (CAHs) (four AOs with CMS-approved programs)
Hospitals (including Psychiatric Hospitals) (four AOs with CMS-approved programs)
Home Health Agencies (HHAs) (three AOs with CMS-approved programs)
Hospices (three AOs with CMS-approved programs)
End-Stage Renal Disease (ESRD) Facilities (two AOs with CMS-approved programs)
Rural Health Clinics (RHCs) (three AOs with CMS-approved programs)
Transplant Centers (four AOs with CMS-approved programs)
Outpatient Physical Therapy/Speech Pathology (OPT/SP) (one AO with a CMS-approved program)
This requirement applies only to those AOs that accredit Medicare-certified providers and suppliers for deeming purposes. There are 9 AOs that accredit Medicare-certified providers and suppliers through 29 CMS-approved accreditation programs. Therefore, the one-time, first-year cost burden for each of the 9 AOs for one program only would be $3,505.60. The number of approved programs for each AO ranges from one to six. There are currently 3 AOs that have 1 approved program each (one-time, first-year cost burden for each of these 3 AOs would be $3,505.60); 2 AOs that have 2 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $7,011.20); 2 AOs that have 3 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $10,516.80); and 2 AOs that have 6 approved programs each (one-time, first-year cost burden for each of these 2 AOs would be $21,033.60).
With 29 total programs across 9 AOs, we assumed an average of 3 programs per AO (29/9 = 3.2 or 3) and an average one-time, first-year cost burden of $10,516.80 per AO (3 programs per AO × $3,505.60 cost burden per program = $10,516.80).
As mentioned in section IV.K. of this final rule with comment period, the changes would not implement a reoccuring annual burden, but rather have a one-time burden on the AOs until the survey processes and activities are aligned with our changes in this final rule with comment period. CMS would resume the current process for approval and re-approval of AOs and their accrediting programs as outlined within the revised § 488.5.
We note there is no direct burden associated with these changes to the deemed provider or supplier.
D. ICRs Associated With the Establishment of a Definition for “National in Scope” (§ 488.1)
As finalized at § 488.1, we will require the AO to provide documentation for meeting the definition of “national in scope” within their initial and reapplication process. As currently required by § 488.1, the AO must provide documentation that demonstrates the organization meets the definition of a “national accrediting organization” as it relates to the accreditation program. Therefore, we estimate the burden on AOs to be minimal as they are already required to provide documentation to this effect. Therefore, we estimate the following:
1. ICR Related to Documentation Requirements for “National in Scope”
We anticipate that a CEO of an AO would compile and verify that the AO meets the proposed definition of “national in scope”.
Since CMS is not requiring a specific format for this documentation, but suggests the AO provide a list which identifies the accredited facilities meeting the definition, we anticipate the compiling of this information would take approximately 40 minutes (0.66 hour) per each AO. For existing CMS approved AOs, the general re-application cycle is not to exceed 6 years. Therefore, we anticipate this burden to be applicable every 4 to 6 years. Therefore, we estimate that the total time burden across all 9 AOs would be 7.33 hours (or 7 hours & 20 minutes) every 4 to 6 years.
The average hourly wage of the AOs CEO is $252.82. Therefore, we estimate that the total cost burden for this task per each AO would be is $168.56 ($252.82 × .66). We further estimate that the total cost burden across the 9 AOs that accredit Medicare-certified providers and suppliers would be $1,517.04 ($168.56 × 9 AOs).
2. ICR Related to Incorporation of the “National in Scope” Requirements Into the AO's Application
We anticipate that a medical secretary would finalize and package/send the application for CMS approval. We believe this additional document of meeting “national in scope” would take approximately 5 minutes (0.083 hours) per each AO to be included in the package which is already required under § 488.5. This requirement would apply only to the 9 AOs that accredit Medicare-certified providers and suppliers. We estimate that the total time burden associated with this task across these 9 AOs would be 45 minutes (0.75 hour).
The adjusted mean hourly wage for a medical secretary is $43.82. Therefore, we estimate that the cost burden per each AO for this task would be $3.64 (5 minutes (0.083 hour) × $43.82). We further estimate that the total cost burden would be $40.16 ($43.82/60 min. per hour = $0.73 per min.) and ($0.73 per min. × 55 min. = $40.16 per 55 min) or ($4.462 × 9 AOs = $40.158).
This burden is imposed to ensure AOs submit verification of meeting the new definition. However, this burden would only be incurred by the AOs during the submission of their initial or renewal applications which would only take place every 4 to 6 years. The burden associated with these requirements will be submitted to OMB under OMB control number 0938-NEW.
We note that there is no direct burden associated with these changes to the deemed provider or supplier.
E. ICR Associated With the Revision of the AO Performance Measures and To Require a Publicly Reportable Plan of Correction
Traditionally, SAs performed validation surveys on a sample of providers and suppliers (such as hospitals, CAHs, ASCs, and HHAs) accredited by the AOs. These SA “look-back” validation surveys compared the survey findings of the AO to those of the SA to see if there were any disparities. The disparities found between an AO's surveys and an SA's surveys were used in a performance measure called the “disparity rate” and was tracked by CMS as an indication of the quality of the surveys performed by the AO as described earlier in this rule.
We are revising the validation process for Medicare-certified providers and suppliers by establishing a new type of validation survey known as a DOVS to replace the previous “look-back” validation survey performed by the SAs. As a result of the revisions made to the
( printed page 36452)
validation process, and for the reasons discussed in section III.Y. of this final rule with comment period, we have established a new definition for “disparity rate” to revise the definition of disparity rate as a “process disparity rate”, which is defined as, “for a DOVS, the difference between the observed survey process findings and the expected survey process findings expressed as a percentage”, in this final rule with comment period. As a result of removing the “look-back” validation surveys in this final rule with comment period, we are also withdrawing and not finalizing the proposed definition of “outcome disparity rate.”
At § 488.8(a)(4), we require that the AO submit a publicly reportable plan of correction for performance that is less than an acceptable threshold for established performance measures.
This is a new requirement and therefore will be a new burden for AOs to complete. The plan of correction will be completed and submitted to CMS within 10 business days following the notification of the AO of their less than acceptable performance. It will address the areas of improvement and the specific actions to be taken to improve those areas on a sustainable basis, the process for ongoing monitoring of progress toward acceptable performance, as well as the individuals responsible for overseeing the plan of correction and the anticipated implementation dates of the proposed actions.
In the proposed rule (89 FR 12040) we stated the following in estimating the costs of these proposed requirements, we believe that this task would be performed by the AO's CEO. We also anticipate that each AO would prepare approximately 123 plans of correction per year. We further estimate that it would take 80 hours of time by the AO's CEO to prepare each plan of correction. This is using the overall average disparity rate of 33 percent. There are approximately 374 annual validation surveys performed across all provider types (374 × 0.33 total plans of correction). We further estimate that the total annual time burden per each AO for the completion of POCs would be 9,840 hours (80 hours × 123). We further estimate that the total annual time burden for the completion of all POCs across all 11 AOs that accredit Medicare-certified providers and suppliers would be 108,240 hours (9,840 hours × 11 AOs). We estimate that the cost burden to each AO for the completion of each POC would be $16,385.60 (80 hours × $204.82). We further estimate that the annual cost burden per each AO for the completion of the estimated 123 POCs per year would be $2,015,428.80 (9,840 hours × $204.82). We further estimate that the total annual cost burden across all 11 AOs that accredit Medicare-certified providers and suppliers for the completion of all POCs annually would be $22,169,716.80 ($2,015,428.80 × 11 AOs).
In preparing and estimating the costs of this final rule with comment period for AOs, we recognized that our proposed estimates need to be revised in several areas. Based on our experience with AOs, we no longer believe that the plan of correction would be prepared by the AO's CEO. We believe the plan of correction would be more appropriately prepared by one of the AO's program managers and that it would not take 80 hours of the program manager's time for each plan of correction. We believe that we grossly overestimated the burden hours for this task. Therefore, based on our experience working with the AOs and their program managers on past survey process performance issues, that it would only take approximately 8 to 16 hours for an AO program manager to complete a plan of correction and submit it to CMS. We have averaged this estimate to 12 hours of burden for this new requirement.
We also no longer anticipate that each AO would need to prepare approximately 123 plans of correction per year. This estimate was based on the approximate number of 374 annual validation surveys performed across all AOs and provider and supplier types using the overall average disparity rate of 33 percent. Both the average annual number of validation surveys and the average disparity rate are based on the proposed look-back validation survey model, including the outcome disparity rate, that we are withdrawing in this rule, and not on the DOVS model and the process disparity rate being finalized in this rule. We believe this invalidates our use of those numbers for this final rule with comment period since they do not apply to DOVS and the process disparity rate and performance measures based on that rate. Therefore, we are revising our proposed estimates of these numbers based on what we anticipate will be the annual number of DOVS performed for all nine AOs using a representative sample of their CMS-approved accreditation programs after this rule is finalized.
Beginning on October 30, 2023, and ending on September 12, 2024, there were 151 DOVS performed by CMS surveyors across all nine AOs from a representative sample of nine different CMS-approved accreditation program types, including three new program types that had never been surveyed under the traditional look-back validation surveys. The DOVS pilot year was national in scope, taking place across 44 States.
Once CMS completed the DOVS scoring for the survey performance of each AO and its specific program type and surveyor team, CMS would send the scoring report to the applicable AO. The AO then had 10 days to review its scoring and request a reconsideration of its score if applicable. For the pilot year, CMS received 39 requests for reconsideration from AOs out of the 151 DOV surveys performed and scored, or 26 percent. CMS reviewed each request and made its decisions for reconsideration of AO DOVS scores based on evidence submitted by the AO in addition to the applicable CMS regulations in the CFR and the specific survey guidance contained in the SOM. Of the 39 requests for reconsideration of DOVS scores, CMS either partially or completely upheld the original scoring for 25 of the surveys, or 17 percent of the 151 DOV surveys and scores.
We believe that the number of DOV surveys performed by CMS in the pilot year of 2023-2024 per year (151) will remain relatively constant after this rule is finalized and after the DOVS program is resumed. We also believe that the 25 (17 percent)DOV survey scores in the pilot year that CMS upheld after reconsideration (and thus would most likely be those requiring an AO to correct deficiencies in its survey process through a plan of correction) are a reliable indicator of the number of DOVS findings and scores that will require plans of correction by AOs per year under the the requirements being finalized in this rule.
Based on these assumptions drawn from the DOVS pilot, we believe that it would take approximately 8 to 16 hours for an AO program manager (at a salary of $128 per hour) to complete a plan of correction and submit it to CMS. We have averaged this estimate to 12 hours of burden for this new requirement. We estimate that the burden hours for 25 plans of correction (divided equally among the 9 AOs for approximately three plans of correction for each AO) would be a total of 300 hours or 36 hours for each AO program manager. We estimate that the cost burden to each AO for the completion of each plan of correction would be $1,536 (12 hours × $128) We further estimate that the annual cost burden per each AO for the completion of the estimated three plans of correction per year would be $4,608 (36 hours × $128). We further estimate that the total annual cost burden across all 9 AOs that accredit Medicare-
( printed page 36453)
certified providers and suppliers for the completion of all plans of correction annually would be $41,472 ($4,608 × 9 AOs).
F. Summary of Estimated Burden
Table 5 provides a summary of the estimated burden related to the requirements of this final rule with comment period.
Table 5—Summary of Cost Burden
Time & Cost Burden Summary Table
Name of ICR
Time burden
Cost burden
A.
Information Collection Requirements (ICRs) Related to Conflict-of-Interest Requirements
• 48 hours per AO
• $5,449.92 per AO for 1st report.
1. ICR Related to Conflict-of-Interest Policies & Procedures AOs Must Submit to CMS (§ 488.5(a)(10))
• 432 hours across 9 AOs
• $49,049.28 across all 9 AOs.
2. Requirement that AO surveyors submit conflict-of-interest declarations to CMS upon request and during application review process (§ 488.5(a)(22))
• 48 hours per AO
• 432 hours across 9 AOs
• $1,090 per AO annually.
• $9,810 across all 9 AOs annually.
3. Requirement for Submission of Information About AO Fee-based Consulting Services Provided (§ 488.8(i)(5))
• 48 hours per AO for the 1st year report
• 432 hours across 9 AOs for 1st year reports
• $5,449.92 per AO for 1st report.
• $49,049.28 across all 9 AOs for 1st reports.
• 8 hours per AO for 2nd year report & all subsequent reports
• $757.12 per AO for the 2nd report & all subsequent reports
• 72 hours across all 9 AOs for 2nd year & all subsequent reports
• $6,814.08 across all 9 AOs for the 2nd year reports & all subsequent reports.
4. Requirement that Accrediting Organization Establish Fee-Based Consulting Firewall Policies and Procedures (§ 488.8(j))
• 0 hours (The time burden associated with this requirement is included with burden calculation for 488.8(i))
• $0 (The cost burden associated with this requirement is included with burden calculation for 488.8(i)).
B.
Requirement that the AO Incorporate the CMS standards to ensure improved evaluation of AO performance (§ 488.5(a)(3))
• 200 hours per AO program for first-year, one-time burden
• 5,400 hours across all 9 AOs for first-year, one-time burden
• $26,598 per AO for first-year, one-time cost.
• $239,382 across all 9 AOs for first-year, one-time cost.
C.
Burden Related to Requirement that AOs Must Use Comparable Survey Processes to That Used by CMS and the SAs
1. Burden Related to Documentation Requirements Imposed By Requirement that AOs Use Comparable Survey Process (§ 488.5(a)(13)
• 10 hours per AO
• 90 hours across the 9 AOs that accredit Medicare-certified providers & suppliers
• $1,095.40 per AO.
• $9,858.60 across 9 AOs.
2. Burden associated with the preparation of a presentation that AOs must prepare and provide to CMS to demonstrate how their survey processes are comparable to that of CMS
• 55 hours per AO
• 495 hours across the 9 AOs that accredit Medicare-certified providers & suppliers
• $4,951.10 per AO.
• $44,559.90 across 9 AOs.
3. ICR Related to Requirement for AO to Submit Survey Findings/Reports
• 0 hours
• $0—because the AOs are already required to do this.
4. Burden Related to Submission of Revised Accreditation Standards and Survey Processes for review and approval by CMS as required by § 488.8(b)
• 80 hours per AO program for first-year, one-time burden
• 2,160 hours across all 9 AOs for first-year, one-time burden
• $10,516.80 per AO for first-year, one-time cost.
• $94,651.20 across all 9 AOs for first-year, one-time cost.
D. Burden Related to Documentation Requirements for “National in Scope
• 0.66 hour every 4-6 years
• $168.56 per AO
1. Documentation requirement for “National in Scope”
• 6 hours across the 9 AOs that accredit Medicare-certified providers & suppliers
• $1,517.04 across the 9 AOs that accredit Medicare-certified providers & suppliers.
2. ICR related to incorporation of the “National in Scope” requirements into the AO's application
• 0.083 hour per AO
• 0.75 hours across the 9 AOs that accredit Medicare-certified providers & suppliers
• $4.46 per AO.
• $40.16 across the 9 AOs that accredit Medicare-certified providers & suppliers.
E. Revision of the AO Performance Measures and Requirements to Submit a Publicly Reportable Plan of Correction
• 12 hours per plan of correction
• 36 hours per AO annually for completion of 3 plans of correction per year
• $1,536 per plan of correction.
• $4,608 per AO for completion of 3 plans of correction per year.
• 324 hours annually across all 9 AOs that accredit Medicare-certified providers and suppliers
• $41,472 across all 9 AOs that accredit Medicare-certified providers and suppliers.
Total Estimated Time Burden
• 9,844 total burden hours across all AOs/accreditation programs
Year 1 Costs
$539,389.
Year 2 Costs
114,072.
Year 3 Costs
114,072.
Year 4 Costs
114,072.
Year 5 Costs
114,072.
( printed page 36454)
Average annual total costs over 5 years
199,135.
Total Average Annual ICR Cost Burden per AO
22,126.
Total ICR Cost Burden Across All AOs
199,135.
Total Net Cost Burden
199,135.
In the proposed rule, we solicited public comments to the collection of information section of this rule. We received the following comments regarding the time and burden calculations for the proposed rule.
Comment:
One commenter stated that the Office of Management and Budget (OMB) completed a Summary of Cost Burden that AOs would incur to implement the proposed rule. The total net cost burden is $
25,505,274.
When the total estimated loss of profit is added, the total net impact on AOs is $
39,114,116.
This impact will be felt proportionately according to the number of programs the AO has approved deemed status for. The two largest AOs are projected to bear approximately $
10 million
each of this burden. It raises serious concerns about the feasibility of expecting independent, not-for-profit AOs to absorb such a financial impact. This final rule with comment period poses a considerable threat to the financial stability and sustainability of these organizations.
Another commenter contended that even if the ICR calculations included within the proposed rule were accurate (and this commenter believes many of the burden calculations are significantly understated and burdensome), the cost impact would be more than $2.5 million per AO, with nearly all requirements becoming effective within a year or less, potentially further escalating costs.
Response:
We prepared this burden estimate based on what tasks we believed the AOs would be required to complete to implement the proposals made in the proposed rule if all proposals are finalized. The Collection of Information sections provide detailed descriptions of proposals, the tasks we believe would be required, and our estimated time and cost burdens for each.
It is important to note several facts about our burden estimates. First, these burden estimates are higher for the AOs that provide fee-based consulting and lower for those that do not. This is because the six proposals related to fee-based consulting services do not apply to the AOs that do not provide this service. Thus, the time and cost burdens for these AOs will be lower.
Also, these are just
estimated
costs for the
possible
tasks that might be required of the AOs to implement our proposals and the associated time and cost burdens. The AOs may not need to perform the stated tasks if they already follow some of the requirements or already have the required policies and procedures. Or it may not take the AO as much time as we estimated it would to perform a task, thus the estimated cost would be lowered. In addition, as we have detailed above in the preamble to the applicable sections of this final rule with comment period, we have not finalized some of our proposed requirements or we have revised them based on public comments in ways that still strengthen our oversight of AOs but also significantly lower the estimated costs of this final rule with comment period versus the estimated costs of the proposed rule. Additionally, we believe that a degree of burden is justified when the rulemaking better aligns our requirements with our statutory authority to oversee AOs and their survey programs for Medicare-certified providers and suppliers to ensure that those providers and suppliers improve the safety and quality of care for patients nationwide.
Comment:
One commenter stated that, in drafting the proposed rule, CMS may have made some errors in its calculations of cost and burden for AOs. This commenter cited to the cost and time burden estimate for the requirement that the AO surveyors take the CMS surveyor training as an example.
This commenter stated that in this burden estimate, CMS used an estimation of 75 surveyors per AO. This commenter stated that they employ several hundred surveyors. As a result, two-thirds of the total estimated cost and time burden used by CMS for all AOs (75 surveyors × 11 Medicare-deemed AOs) is in fact closer to a burden estimate for a single AO.
Response:
We respectfully disagree that our burden estimate is erroneous. At the time of the publication of the proposed rule, we did not have any information about how many surveyors are employed by each AO that accredited Medicare certified providers and suppliers. Therefore, we had to make an estimate of the number of surveyors employed by each AO.
Also, while this commenter is a larger AO that employs a larger number of surveyors, this is the exception rather than the rule. The remainder of the AOs are not as large and do not employ as many surveyors. Therefore, we chose to use, for the number of surveyors, a number that is more representative of the number of surveyors employed the majority of the AOs, and not just this commenter.
Further, to get the time and cost burden estimate that is representative of the number of surveyors they employ, this commenter could have just substituted their number of surveyors into the calculations to come up with a burden estimate for their AO. For example, in the proposed rule, we estimate that it would take each surveyor 35 hours to complete the required CMS surveyor training. If this commenter has 250 surveyors, then the total time burden across all its surveyors would be 8,750 hours (35 hours × 250 surveyors).
Also, in the proposed rule, we stated that the adjusted hourly wage for an RN is $94.64. The cost burden for each surveyor to take the CMS online surveyor training would be $3,312.40. (35 hours × $94.64). If an AO employs 250 surveyors, the cost burden across all 250 surveyors would be $828,100 (8,750 hours × $94.64 per hour).
This commenter stated that they employ “several hundred” surveyors but did not provide the exact number, therefore we have used an estimated number of 250 surveyors. The commenter can insert the exact number of surveyors they employ to get the exact burden calculations.
Comment:
One commenter expressed disagreement with the burden calculations estimated by CMS throughout this proposal. The impact calculated by the agency fails to take into account applicable administrative
( printed page 36455)
costs for each proposed change. The additional administrative costs to each AO include additional support services and personnel, IT and systems costs, marketing and education efforts, etc. Even proposed changes that are presented by CMS as having $0 estimated impact and noted as a usual and customary practice of the AO will require some level of investment for effective implementation to meet the proposals.
Response:
In the collection of information section of the proposed rule, we provided estimates of the time and cost burdens we believe the AOs will incur if our proposals are finalized. However, these are just estimates and not exact figures.
We can only include time and cost burdens for those tasks we anticipate the AOs would be required to implement as a result of our proposals. However, each AO is an individual and separate business entity that have different business operations, practice, policies, etc. CMS is not privy to how the AOs run their businesses or structure their organizations. Therefore, we may not have anticipated some tasks that the AOs may incur related to our proposals.
Comment:
One commenter was concerned that the burden calculations do not account for the additional time, cost, and resources that will be required from CMS and State agencies for review and enforcement. These additional costs will necessarily be passed on to taxpayers and the healthcare system; those burdens should be recognized by the agency and presented within the proposal.
Response:
While this information was not stated in the proposed rule, the costs to the Federal government are calculated.
Comment:
One commenter stated that the entire section of information collection and cost estimation required by the OMB grossly underestimates the time and cost of AOs to comply with this proposed rule. Not only are time estimates underestimated, but the wage data used is from 2021 before the explosion of labor cost inflation; and CMS is underestimating the cost burden and impact by at least 25 percent to 40 percent.
Response:
The information collection section of the proposed rule contains our estimates of the time and cost burdens caused by the proposals in the rule. In these burden estimates, we include the time and costs burden for the tasks we anticipate each proposed requirement will require the AOs to perform. However, CMS is not able to anticipate every single time and cost burden because each AO has different organizational structures, operating procedures, and varying numbers of staff and surveyors. Each AO may handle each proposed requirement differently. For example, while some AOs may use existing staff to perform the tasks associated with a proposed requirement, other AOs may decide to hire new staff to do so.
This commenter did not provide any information about which sections of our burden calculations are underestimated. We invite this commenter to provide CMS with the time and cost burden information we did not include in the Information Collection Request section of the rule. In the alternative, we suggest that this commenter calculate the additional time and cost burdens.
This commenter stated that CMS used outdated wage rates in the cost burden calculations. At the time of the writing of the proposed rule, we used the then-current wage rates from the U.S. Bureau of Labor Statistics. However, these wage rates have been updated in this final rule with comment period.
VII. Regulatory Impact Analysis
A. Statement of Need
We seek to strengthen the public trust in CMS-approved AOs' findings and to protect the health and safety of patients that seek services from Medicare and Medicaid-participating providers that are accredited by CMS-approved AOs. We believe that AOs that voluntarily seek approval for “deeming purposes” are taking on a critical quality assurance role for the American people. Patients need to be able to rely on the strength of that accreditation to be assured that their healthcare services will be safe and of high quality. Where there are gaps in that accreditation process, or where quality issues are not fully identified or investigated by the AO, it means that current and future patients may experience unnecessary harm or quality issues. Therefore, we are seeking to strengthen our oversight of AOs by revising existing regulations or implementing new regulations that would address the following issues: (1) place limitations on the fee-based consulting services AOs offer to the providers and suppliers they accredit; (2) implement remedies for violation of the prohibition against AO fee-based consulting; (3) require AOs to report information to CMS on a bi-annual basis about the fee-based consulting services they provide; (4) require AOs to report specific conflict-of interest information to CMS with their initial and renewal applications; (5) require AOs to submit surveyor conflict-of-interest declarations to CMS on an annual basis; (6) prohibit AO owners, surveyors and other employees, that currently or within the previous 2 years have had an interest in or relationship with a healthcare facility the AO accredits from doing the following: (a) participating in the survey of that healthcare facility; (b) having input into the results of the survey and accreditation for that healthcare facility; (c) having involvement with the pre-or post-survey activities for that healthcare facility, or (d) having contact with or access to the records for the survey and accreditation of that healthcare facility; (7) require AOs to incorporate the CMS conditions into their accreditation standards for its deeming programs; (8) use a comparable survey processes; (9) revise the validation process, implement new performance measures and the use of plans of correction for unacceptable performance measure scores; (10) revise the hospital application process for AOs that have an approved hospital accreditation program to incorporate surveys of psychiatric hospitals into their hospital programs; (11) add new definitions for the terms “unannounced survey”, “national in scope”, “geographic regions”, “process disparity rate”, and “outcome disparity rate”; and (12) place limitations on terminated providers or suppliers seeking re-entry into the Medicare program. We continue to review and revise our health and safety requirements and survey processes to ensure they are effective in driving quality of care for our accredited providers and suppliers.
B. Overall Impact
We have examined the impacts of this rule as required by Executive Order 12866, “Regulatory Planning and Review”; Executive Order 13132, “Federalism”; Executive Order 13563, “Improving Regulation and Regulatory Review”; Executive Order 14192, “Unleashing Prosperity Through Deregulation”; the Regulatory Flexibility Act (RFA) (Pub. L. 96-354); section 1102(b) of the Social Security Act; section 202 of the Unfunded Mandates Reform Act of 1995 (Pub. L. 104-4); and the Congressional Review Act (5 U.S.C. 804(2)).
Executive Orders 12866 and 13563 direct agencies to assess all costs and benefits of available regulatory alternatives and, if regulation is necessary, to select those regulatory approaches that maximize net benefits (including potential economic, environmental, public health and safety, and other advantages; distributive impacts.). Section 3(f) of Executive Order 12866 defines a “significant regulatory action” as any regulatory
( printed page 36456)
action that is likely to result in a rule that may: (1) have an annual effect on the economy of $100 million or more or adversely affect in a material way the economy, a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or State, local, or tribal governments or communities; (2) create a serious inconsistency or otherwise interfere with an action taken or planned by another agency; (3) materially alter the budgetary impact of entitlements, grants, user fees, or loan programs or the rights and obligations of recipients thereof; or (4) raise novel legal or policy issues arising out of legal mandates, or the President's priorities. Based on our estimates, the Office of Information and Regulatory Affairs (OIRA) has determined that this rulemaking is significant per section 3(f) of E.O. 12866. Accordingly, we have prepared a Regulatory Impact Analysis that to the best of our ability presents the costs and benefits of the rulemaking.
C. Detailed Economic Analysis
1. Benefits
In developing this final regulation, we carefully considered its potential effects including both costs and benefits. The overall benefit of this rule would be to improve CMS' oversight of the AOs and to improve the overall quality and safety of healthcare. More specifically, the benefits of this rule include the prevention and removal of potential and actual conflicts of interest, the improvement of the validation process and anticipated reductions in the validation disparity rate, the additional performance measure and the implementation of plans of correction that would help AOs that have low performance measure scores to prepare a plan for how to improve their performance. We note that the generation of benefits is contingent upon behavior change, which entails costs; provisions that are discussed later in this section as having negligible costs would therefore be anticipated to have minimal benefits.
However, we have identified a quantifiable benefit that this final rule with comment period will generate for AOs on an annual basis. Currently, 42 CFR 488.4(a)(2) does not allow any national AO to submit an application to CMS for approval of its transplant center accreditation program and thus excludes transplant centers from being deemed as having met the applicable CMS requirements through an AO accreditation survey. With the revisions to § 488.4(a)(2) in this final rule with comment period we have removed this transplant center exception from the regulatory language and will now allow AOs to develop accreditation programs for this provider type that they may submit to CMS for approval. CMS may then deem a transplant center to be in compliance with the applicable Medicare conditions or requirements if a CMS-approved AO accreditation program determines such compliance through its survey of the provider.
We believe that AOs will benefit from this potential new source of revenue since AOs charge providers and suppliers seeking participation in the Medicare program initial and annual fees for their accreditation services. A provider or supplier pays an AO to conduct the accreditation surveys so that it may be deemed by CMS as meeting the applicable conditions or requirements for participation in the Medicare and/or Medicaid programs. An AO may also charge its provider/supplier client for other services to assist them in maintaining their compliance with the CMS requirements, such as services it might provide through its fee-based consulting division or separate business entity. Accreditation by an AO is voluntary and is not required for Medicare participation.
There are currently 234 approved transplant centers participating in Medicare with 888 approved transplant programs nationwide. To be approved by Medicare, transplant programs must meet the requirements specified at § 482.72 through § 482.104. A transplant program is located in a Medicare-approved hospital and provides transplantation services for the following types of solid organs: heart, lung, liver, kidney, pancreas, or intestine. In addition to meeting the transplant CoPs, the transplant program must comply with the hospital CoPs (specified in 42 CFR 482.1 through § 482.57). Appendix X of the State Operations Manual contains the interpretive guidance and survey procedures for transplant programs.
To estimate the benefits of this change to the requirements for AOs, we made several assumptions based on our knowledge of and our experience with AOs and their accreditation programs as well as with the provider and supplier types that must meet the CoPs and other Federal requirements to participate in the Medicare and Medicaid programs. First, we believe that of the 234 currently approved transplant centers roughly 80 percent, or 187, of them would seek continued CMS certification through a CMS-approved accreditation program once this rule becomes effective. We base this assumption on the current percentage of hospitals that use accreditation for deeming purposes, an accreditation rate that has remained relatively steady for several decades now.
Second, we believe that each of the four AOs with currently approved hospital accreditation programs would submit an application to CMS for approval of a new transplant center program. Because transplant centers also have to meet the hospital CoPs, we believe that an AO with an established and approved hospital accreditation program is well positioned to develop a transplant center program that would be approved by CMS. That does not prohibit an AO currently without an approved hospital program from developing a transplant center program and submitting an application to CMS for its approval; however, such an AO would also need to develop a hospital program that would need CMS approval.
Estimates of how much each AO may charge a transplant center for accreditation range from $26,000 to $130,000. This cost range is based on what is generally known regarding what one of the AOs charges on average for a “small” hospital ($26,000) and for a “large” and more complex hospital/medical center ($130,000). TJC states on its website that its accreditation fees are based on the services provided and daily patient census and include annual fees that are invoiced each year during the triennial accreditation cycle as well as on-site fees that are invoiced during the year the survey is conducted.[24]
We believe that transplant centers fall under the category of a large hospital and have based our estimates on $130,000 averaged over the 3-year accreditation cycle for an annual stream of revenue of approximately $43,000 paid to the AO by a transplant center. We estimate that this represents a potential additional source of revenue of $8,041,000 for AOs annually ($43,000 − 187 transplant centers). We begin converting the revenue to a measure of producer surplus by multiplying this estimate by 20 percent for a total of $1,608,200 for accreditation services, consistent with an assumption that 80 percent of the incremental revenue attributable to the final rule would be offset by quantifiable marginal costs of delivering accreditation services. We derived the 20 percent estimate by reviewing financials that AOs submit as part of their application packages and found that their operating costs average 80 percent. The $1.6 million result
( printed page 36457)
reflects accounting profit, which provides an upper bound on economic profit (the amount that would appropriately be included as a welfare change in this regulatory impact analysis).
We have identified another benefit of this enabling provision that would generate additional annual revenue for these four AOs in the form of fee-based consulting services for those transplant centers that might contract for such services to achieve accreditation for deeming purposes. Recent industry surveys and analysis indicate that over 68 percent of hospitals have established budgets specifically for compliance consulting services such as those offered by AOs.[25]
Using this number, we believe that of the 234 currently approved transplant centers roughly 68 percent, or 159, of them would seek to maintain CMS certification through AO fee-based consulting services once this rule becomes effective.
Healthcare consultants typically charge hospitals between $100 to $400 per hour, or $10,000 to $100,000+ per project.[26]
For our estimates of AO fee-based consulting services cost, we believe that it is reasonable to use the same amount that we have used here to estimate how much AOs would charge annually on average for their accreditation services ($43,000). Therefore, we estimate that this represents a potential additional source of revenue of $6,837,000 for AOs annually ($43,000 − 159 transplant centers). We begin converting the revenue to a measure of accounting profit (an intermediate step toward estimating economic profit or producer surplus) by multiplying this estimate by 20 percent for a total of $1,367,400 for fee-based consulting services.
This serves as our estimate of an upper bound on the benefits accruing to AOs from this enabling provision of this final rule with comment period, valued at $3 million per year ($1.6 million + $1.4 million).
2. Provision-Specific Costs, Benefits and Transfers
We have identified the direct costs associated with this final rule with comment period as the costs associated with reporting, recordkeeping, and other costs. These costs are discussed below.
a. Impact Related to Conflict-of-Interest Requirements
In this final rule with comment period, there are several requirements related to AO and AO surveyor conflicts of interest. In the 2018 AO Conflict-of-Interest RFI, many commenters stated that AOs tend to ignore deficiencies during surveys to promote the efficacy of their consulting services. These commenters also stated that the AOs may ignore deficiencies to avoid giving poor survey results to their clients, who have paid substantial fees for both accreditation and AO fee-based consulting services. These commenters further stated that the financial relationship between the AO and the healthcare facilities they accredit causes a conflict of interest. We believe that the restrictions on AO fee-based consulting in this rule will reduce these conflicts of interest and hopefully remove the incentive for AOs to ignore deficiencies during surveys. We further believe that the conflict-of-interest requirements in this final rule with comment period will prevent potential and new conflicts of interest from occurring. We will address the financial impacts associated with each of these proposals separately.
(1) Impacts Related to Restrictions on Fee-Based Consulting Provided by AOs to the Healthcare Providers and Suppliers They Accredit (§ 488.8(i)(1) through (3))
In section IV.B.3. of this final rule with comment period, we are finalizing restrictions on AO fee-based consulting provided by accrediting organizations or their associated consulting divisions or companies. As finalized, § 488.8(i) will still allow AOs to provide consulting services to the providers and suppliers they accredit with restrictions that address the conflict-of-interest issues associated with these services.
The provision also requires the AOs that provide consulting to revise their consulting business documents, such as their business charter, business documents, employee training information, informational documents that are distributed to prospective clients, and their policies and procedures.
We believe that the AO staff that would be performing these tasks would be an RN and a management staff person that has a job that meets the U.S. Bureau of Labor Statistics job of category of health and medical services manager. The adjusted mean hourly wage for an RN is $94.64. The adjusted mean hourly wage for a medical and health services manager is $132.44.
We estimate that this rule will require the two AO staff members to work on a full-time basis for 1 week (that is, 40 hours per person) to complete the required revisions to the AO's consulting business documents initially when this rule becomes effective. Therefore, we estimate that the one-time burden per each AO for the two AO staff members to perform the required tasks would be 80 hours (2 team members × 40 hours).
At this time, there are only four AOs that provide fee-based consulting. However, because we are revising the term to include all consulting services, this requirement would apply to any AO that provides consulting services. Therefore, for purposes of this estimate, we must assume that all 9 AOs may provide consulting services as described in this rule and that the total one-time burden would be 720 hours (80 hours × 9 AOs).
The cost burden related to the work performed by the RN on this task would be $3,785.60 (40 hours × $94.64). The cost burden related to the work performed by the medical or health services manager on this task would be $5,297.60 (40 hours × $132.44).
Finally, we estimate that the first-year, one-time cost burden per each AO related to the requirements for § 488.8(i)(1) through (3) would be $9,083.20 ($3,785.60 + $5,297.60). We estimate that the total first-year, one-time cost burden to all nine AOs would be $81,748.80 ($9,083.20 × 9 AOs).
(2) Impact of Loss of Revenue to AOs Due to Requirement for Fee-based Consulting Services
We also believe that there will be a further financial impact to all AOs that provide fee-based consulting from the restrictions on fee-based consulting due to the requirements of this rule. Although the 2018 AO Conflict-of Interest RFI gathered information about the nature of these relationships, they did not provide enough information for us to accurately calculate the financial impact that the requirements of § 488.8(i)(1) would have on the AO. We do estimate that the AOs would have a decrease in approximately 25 percent of the fee-based consulting business due to the restriction on providing fee-based consulting prior to initial surveys. We say this because AOs perform accreditation on a 3-year cycle, following the initial survey. We estimate that 25 percent of the fee-based consulting performed by an AO on an annual basis would be for new clients prior to their initial survey. We further estimate that the remaining 75 percent of the AOs fee-based consulting
( printed page 36458)
business would be provided to providers and suppliers prior to a reaccreditation survey.
According to Internal Revenue Service financial disclosure statements filed by the AO that provides the most fee-based consulting through an associated fee-based and other consulting division or company, this AO realized gross revenue from fee-based consulting services in the amount of $44,960,143 in 2020 and $55,970,543 in 2021.[27]
This equates to an average annual revenue of $50,465,298 from fee-based consulting.
We estimate that new accreditation clients make up approximately 33 percent of an AO's client base and that the remaining 66 percent consist of existing clients that require reaccreditation surveys. We further estimate that, currently, only 25 percent (out of the 33 percent) of an AO's new clients elect to have fee-based consulting prior to the initial survey. Therefore, if the AOs are restricted from performing fee-based consulting prior to the initial survey of new clients, they would lose 25 percent of the revenue they receive from their fee-based consulting business. We estimate that the restrictions on fee-based consulting would cause the AO that provides the most fee-based consulting services to incur lost revenue in the amount of $12,616,324 per year ($50,465,298 divided by 4); due to data limitations, the portion of this revenue effect that consists of reduced profit (and thus would qualify as a cost in this regulatory impact analysis) has not been quantified.
While we do not have any independent information about the amount of profits the other AOs realize from their fee-based consulting services, we presume that these AOs do not realize as much revenue from the provision of fee-based consulting as this large AO. We say this for several reasons. First, the other AOs are smaller businesses and have a smaller client base than does this large AO. It is our understanding that these AOs provide fee-based consulting on a smaller scale because they have less clients and some that are smaller businesses that may not have the funds to pay for fee-based consulting services. Therefore, we are not able to provide an accurate estimate of how much loss in revenue will result from the restrictions in AO fee-based consulting.
We estimate that the AOs charge between $100,000 and $500,000 for the fee-based consulting they provide to each healthcare provider or supplier. We do not know how many providers or suppliers currently use the fee-based and other consulting services of their AO prior to their initial survey. Therefore, we are not able to provide an accurate estimate of the total amount of consulting services shifting to new consultants and away from AOs no longer permitted to provide such services to the providers and suppliers for whom they conduct initial surveys.
(3) Impact Related to Requirement That Accrediting Organizations Establish Fee-Based Consulting Firewall Policies and Procedures (§ 488.8(j))
At § 488.8(j) we will require any AO that provides fee-based consulting services, or its associated fee-based consulting division or company, to have robust, written fee-based consulting firewall policies and procedures. We would require that these firewall policies and procedures, at a minimum, include the following provisions: (1) the AO's fee-based consulting services must be provided by a separate division or company from the AO's accreditation division; (2) the AO's fee-based consulting division or separate company must maintain separate staff from that of the AO's accreditation divisions to ensure that the fee-based consulting division staff do not perform AO's accreditation division functions and that the AO's accreditation division staff do not perform fee-based consulting division functions; and (3) the AO's accreditation staff and surveyors are prohibited from marketing the AO's fee-based consulting services to the AO's accreditation clients.
This requirement only applies to those AOs that provide fee-based consulting and requires that these AOs establish new fee-based consulting firewall policies or revise their policies and procedures to meet the requirements.
We believe that the burden associated with the revision of the AO's fee-based consulting firewall policies and procedures would fall under the time and cost burden estimated in section VI.A.3. of this final rule with comment period. As such, we will not assess a separate burden here.
(4) Impact Related to Regulation to Prevent AO Owners, Surveyors or Other Employees That Have an Interest in or Relationship With a Healthcare Facility Accredited by the AO from Participating in Survey Activities for That Facility (§ 488.8(k))
We are finalizing requirements for AOs to avoid conflicts of interest related to employment relationships between AO surveyors and healthcare facilities that are accredited by the AO. At § 488.8(k) we will require the AOs to prohibit their owners, surveyors and other employees from doing the following: (1) participating in the survey of facilities with which they have a relationship; (2) having input into or influence the outcome of any survey performed for facilities with which they have a relationship; (3) having any involvement with the pre or post survey activities for the healthcare facilities with which they have a relationship; or (4) having any contact with the records from the surveys for any healthcare facilities with which they have a relationship. We believe that this should already be a usual and customary practice of the AOs and therefore there should be no additional burden to the AOs to comply with the requirements of this section.
b. Impacts Associated With the Requirement that AOs Incorporate the Medicare Conditions (§ 488.4(a)(1))
(1) Impacts Related to AO Providing Notice of the Revised Accreditation Standards to Their Accredited Providers and Suppliers via Their Website
In addition to changing the survey standards under § 488.4(a)(1), the AOs would be required to provide the newly revised AO standards to the facilities they accredit. There are approximately 15,143 accredited facilities across all program types. We believe that the majority of AOs have a website portal on which they make their standards available to their accredited providers and suppliers.
We believe that each AO would have an administrative assistant or secretary upload the revised standards to the AO's website for each AO program at an hourly rate of $43.82. We estimate that this would take no more than 2 hours. We estimate that the total impact across the 29 CMS-approved AO programs that accredit Medicare-certified providers and suppliers for providing notice of their revised accreditation standards on their website would be a one-time, first-year cost of $2,542 ($43.82 × 2 hours × 29 AO programs). Using our previous assumption of an average of three programs per AO, this would be a one-time, first-year cost of $282 per AO.
(2) Impact Related To Providing Notice of the Revised Accreditation Standards to the Accredited Providers and Suppliers via Email
We also believe an AO would need to provide notice of their revised accreditation standards to their
( printed page 36459)
accredited providers and suppliers directly via email. We believe this will be a group email that will be sent out to all of the AO's accredited providers and suppliers within each of the 29 different AO programs. We estimate that it will take only 1 hour for an AO administrative assistant or secretary (at an hourly rate of $43.82) to prepare and send this email to all 15,143 accredited providers and suppliers across 29 AO programs. Therefore, the total estimated financial impact for all 9 AOs for providing notice of the AO revised accreditation standards via email would be a one-time, first-year cost of $1,271 ($43.82 − 1 hour − 29 AO programs). Using our previous assumption of an average of 3 programs per AO, this would be a one-time, first-year cost of $141 per AO.
(3) Impacts Related to Education of Providers and Suppliers Regarding New Standards
In the proposed rule (89 FR 12050) we stated the following in estimating the costs of these proposed requirements, we believe that the AOs that accredit Medicare-certified providers and suppliers would be required to provide education to their accredited providers and suppliers about their new Medicare accreditation standards, which must be revised to be the same as the CMS standards, or more stringent. We believe that this training would most likely be provided by webinar. There are approximately 14,904 deemed facilities. We estimate that the cost impact to each facility would be $200.46 ($79.56 per RN + $120.90 per general or services manager). We further estimate that the total annual cost burden across all 14,904 accredited facilities would be $2,987,655.84.
In preparing and estimating the costs of this final rule with comment period for AOs, we recognized that our proposed estimates related to AOs providing education on their new standards through webinars needed to be revised in several areas. We now recognize that we were in error when we used the number of deemed facilities as a multiplier for the number of webinars that AOs would need to develop and present. AOs would only need to develop and present an educational webinar on their revised standards for each of their AO programs, which could then be made available for all of their accredited providers and suppliers. There is a total of 25 individual and specific programs across the 9 AOs. AOs would not need to develop and present a webinar for each individual facility as our estimates of the costs indicate in the proposed rule but instead for each individual and specific program. We believe that our assumptions for the cost impact of this requirement were grossly overestimated in the proposed rule and so we are revising our estimates in this final rule with comment period.
Additionally, we recognize that we significantly underestimated the burden hours that it would take an AO's RN and program manager to develop and present each program-specific webinar in the proposed rule, where we estimated that it would only take each AO staff member one hour to do this. We are correcting this underestimation in this final rule with comment period to what we believe will be 120 hours of burden for each pair of RNs and program managers working together to develop and present these educational webinars, and we have also updated their respective hourly rates using the most current BLS data in making these revisions here ($94.64 and $128).
We estimate that the total impact across the 29 CMS-approved AO programs that accredit Medicare-certified providers and suppliers for AOs to develop and present their revised accreditation standards through a program-specific webinar would be $774,787 ($222.64 × 120 hours × 29 programs = $774,787). Using our previous assumption of an average of 3 programs per AO, this would be a one-time, first-year cost of $86,087 per AO.
c. Impact Related to the Requirement That the AO Surveyors Take the CMS Online Surveyor Training
At § 488.5(a)(8), we added a new requirement that will require the AO to include a statement in their application for CMS approval of its program acknowledging that all AO surveyors have completed or will complete two CMS mandatory documentation courses and the relevant program-specific CMS online trainings established for SA surveyors, initially, and thereafter.
CMS provides a number of online surveyor training modules that are available to the SA surveyors. We will require the AO surveyors to take this training in an attempt to decrease the historically high disparity rate between the AOs' survey results and those of the validation surveys performed by the SA surveyors.
There are a total of 163 online training programs that are available the SA surveyors on the CMS Quality, Safety and Education Portal (QSEP) website. This website provides courses that are general in nature such as “Principles of Documentation for Non-Long Term Care” and “Basic Writing Skills for Surveyor Staff”, infection control, patient safety, Emergency Preparedness. The CMS QSEP website also offers courses related to specific healthcare settings such as hospitals, CAHs, ASCs, Laboratories, Community Mental Health Centers, Emergency Medical Treatment and Labor Act, Federally Qualified Health Centers (FQHCs), Home Health Agencies and Outcome and Assessment Information Set, Hospices, Nursing Homes and the Minimum Data Set, Outpatient Physical Therapy/Outpatient Speech Therapy. These courses are self-paced and the person taking the course can take the courses over a period of time. The amount of time required to complete each of these training course varies depending on the pace at which the trainee completes the training. The basic surveyor training courses for specific programs range in time from 16-82 hours for completion. We estimate the average time it takes to take one of the basic surveyor courses is 27 hours. This could be more or less depending upon the specific program that AO surveyors need to take.
We will require that each AO surveyor take the two mandatory documentation courses (that is “Principles of Documentation for Non-Long-Term Care” and “Basic Writing Skills for Surveyor Staff”) and the basic surveyor course for the care setting for which they perform surveys. We further estimate that it would take approximately 4 hours to complete each of these courses; however, these courses are self-paced and could take more or less time, depending on the individual surveyor. Therefore, an AO surveyor would incur a time burden of approximately 35 hours for the completion of all of the required CMS surveyor training courses.
Based upon this information, we estimate that the financial impact to the AOs will be $3,312.40 for each surveyor that completes the CMS online surveyor training (An AO RN surveyor at $94.64 per hour × 35 hours = $3,312.40).
We are not able to accurately estimate the total time and cost burden for each AO for the wages incurred for the time spent by all surveyors from each AO to take the CMS online surveyor training courses, because we do not know exactly how many surveyors each AO has. However, if we estimate that each AO has 75 surveyors, the estimated financial impact to each AO associated with this requirement would be $248,430 ($3,312.40 × 75 surveyors = $248,430). As of March 2026, there are currently 9 AOs that accredit Medicare-certified providers and suppliers. We estimate that the total estimated financial impact across these 9 AOs
( printed page 36460)
would be $2,235,870 ($248,430 × 9 AOs = $2,235,870).
Summary of Financial Impact Caused by the Requirements in This Final Rule With Comment Period
Table 6 summarizes the financial impact of the requirements that we are finalizing in this rule.
Table 6—Summary of Impact
Summary of Impact
A. Conflict-of-Interest Requirements:
Impacts Related to Restrictions on Fee-Based Consulting Provided by AOs to the Healthcare Providers and Suppliers They Accredit (§ 488.8(i)(1) through (3))
• One-time, first-year cost of $81,749 across all 9 AOs that currently provide fee-based consulting services.
• One-time, first-year cost of $9,083 per AO.
B. Requirement that the AO Incorporate the Medicare standards to ensure improved evaluation of AO performance:
1. Burden related to AO providing copies of their revised accreditation standards to their accredited providers and suppliers through the AO's website
• One-time, first-year cost of $2,542 across all 29 accreditation programs.
• One-time, first-year cost of $282 per AO.
2. Burden to AO related to providing copies of their revised accreditation standards to their accredited providers and suppliers via email
• One-time cost of $1,271 across all 29 accreditation programs.
• One-time, first-year cost of $141 per AO.
3. Burden to AO to provide education to its accredited providers and suppliers about the AO's revised accreditation standards
• One-time cost of $774,787 across all 29 accreditation programs.
• One-time, first-year cost of $86,087 per AO.
C. Impact of Requirement for AO Surveyors to Take CMS Surveyor Training
• $248,430 per each AO per 75 surveyors.
• $2,235,870 across 9 AOs.
D. Impact of AO Staff to Review This Final Rule With Comment Period
• One-time cost of $2,384 across 9 AOs.
Year 1 Costs
$3,098,603.
Year 2 Costs
$2,235,870.
Year 3 Costs
$2,235,870.
Year 4 Costs
$2,235,870.
Year 5 Costs
$2,235,870.
Average annual total costs over 5 years
$2,408,417.
Average annual cost per AO over 5 years
$267,602.
Total Regulatory Impact Costs Across All AOs
$2,408,417.
Total of ICR Costs (Table 5)
$199,135.
TOTAL ESTIMATED COSTS OF FINAL RULE WITH COMMENT PERIOD
$2,607,552.
TOTAL ESTIMATED COSTS OF FINAL RULE WITH COMMENT PERIOD PER AO
$289,728.
TOTAL NET IMPACT
$2,607,552.
TOTAL ESTIMATED PRODUCER SURPLUS (Section VII.C.1)
≤$2,975,600.
3. Regulatory Review Cost Estimation
Due to the uncertainty involved with accurately quantifying the number of entities that will review the rule, we assume that the total number of unique commenters to the 2018 AO Conflict-of-Interest Request for Information (December 20, 2018, 83 FR 65331) will be the number of reviewers of this final rule with comment period. We acknowledge that this assumption may understate or overstate the costs of reviewing this rule. It is possible that not all commenters reviewed the 2018 AO Conflict-of-Interest Request for Information in detail, and it is also possible that some reviewers chose not to comment on the proposed rule. For these reasons we thought that the number of past commenters would be a fair estimate of the number of reviewers of this rule. We welcomed any comments on the approach in estimating the number of entities which will review the proposed rule. We did not receive any public comments specific to our solicitation.
We believe that persons reviewing this rule would consist of AO management staff, healthcare association management staff, and healthcare facility management staff. We believe all of these persons would have positions that fall under the U.S. Bureau of Labor Statistics job category of medical and health services manager. Assuming an average reading speed, we estimate that it would take approximately 2 hours for the staff to review this final rule with comment period. Using the wage information from the BLS for Medical and Health Service Managers (Code 11-9111), we estimate that the cost of reviewing this rule is $264.88 ($132.44 per hour × 2 hours) × 9 AOs = $2,383.92 (
https://www.bls.gov/oes/current/oes_nat.htm).[28]
D. Alternatives Considered
1. Changes to AO Fee-based Consulting
We considered proposing a complete ban on AO fee-based consulting because of the conflicts of interest associated with the provision of these services by the AOs to the healthcare providers and suppliers they accredit. However, we presume the financial impact to the AOs associated with a complete ban on fee-based consulting would be larger. For example, the AO that provides the most fee-based consulting realized over $50 million dollars annually from providing these services. A complete or almost complete ban on the provision of AO fee-based consulting services would eliminate or severely limit this revenue source.
( printed page 36461)
Therefore, we decided to finalize more limited restrictions on AO fee-based consulting services that would still address the conflicts of interest while greatly reducing the cost burden and potential loss of revenue on AOs.
2. Changes to the Validation Program
We considered several alternatives for changes to the validation program. First, we considered making no changes to the validations program, which would mean that we would continue performing only look-back surveys. We also considered performing only direct observation surveys. After considering the alternative, we decided to finalize performing a combination of both look-back and direct observation surveys because this would result in a cost savings to providers and suppliers. If we were to continue the validation program as is, there would be no change in provider burden. If we modify the validation program by performing only DOVS, burden to providers and suppliers would be reduced significantly; however, the workload on the SAs would be increased significantly. The SAs have indicated during the pilot program that they would not be able to handle such an increased workload. Therefore, by only using the direct observation method for 100 percent of the validation surveys performed annually and continuing to use CMS surveyors (instead of SA surveyors), this would provide a significant decrease in provider and supplier burden while essentially removing this workload from the SAs.
By removing the look-back validation survey method and keeping only the direct observation validation survey process in this final rule with comment period, we believe that provider burden will be greatly reduced by not requiring an additional validation survey, thus essentially eliminating the number of healthcare providers that would have to undergo two full surveys within a 60-day period. We further believe this approach enhances the validation program, addresses the public comments we received, and will be welcomed by both the AOs, and the providers and suppliers.
3. Additional Alternatives to the Proposed Rule That Minimize Significant Economic Impacts on Small Entities
After consideration of the comments received regarding our proposal to require the AOs to submit surveyor conflict-of-interest declarations to CMS on an annual basis, we have decided not to finalize this proposal as proposed. We are not finalizing our proposal to require the AOs to obtain and submit the surveyor declarations to CMS annually. We will instead require the AOs to submit the surveyor conflict-of-interest declarations for CMS to review upon request and during each application review process. Finalizing this change will reduce the reporting burden on AOs while ensuring CMS can address conflicts of interest.
Based on public comments, we are also revising the proposed rule to clarify which AO consulting services will be restricted under this final rule with comment period, that is, an AO's (or its consulting division's) review of a [particular] facility's compliance with the Medicare standards through simulation of a real survey, such as a “mock” survey with comprehensive written reports of findings, for a facility accredited by the AO prior to an initial accreditation survey and within the 12 months prior to the next scheduled re-accreditation survey. This limitation does not apply to consulting or general education services for entities the AO does not accredit, or to education provided to their accredited entities.
We note here that the definition of fee-based consulting services that we are finalizing in this rule is not only based on the comments we received regarding the terms, but that, in its specificity and its parameters, the definition better aligns with our original intent in proposing these requirements
By finalizing this definition in this rule, we are pointing more clearly to what type of consulting services we believe may lead to potential conflicts of interest for an AO that provides such services for a provider or supplier it accredits. We then support this specific definition with the application of the requirements at §§ 488.8(i) and (j) that further specify at what times and under what circumstances in the accreditation and deeming process that these types of consulting services are restricted.
We believe that the changes in this final rule with comment period to more narrowly define the restricted consulting services (versus the more broadly defined restrictions in the proposed rule) will lessen the cost burden on AOs as well as potentially reduce the impact on the revenues that AOs derive from the provision of fee-based consulting services.
E. Regulatory Flexibility Act (RFA)
The RFA requires agencies to analyze options for regulatory relief of small entities if a rule has a significant impact on a substantial number of small entities. For purposes of the RFA, small entities include small businesses, nonprofit organizations, and small governmental jurisdictions. Six of the nine AOs impacted by this rule are small entities, either by being nonprofit organizations or by meeting the Small Business Administration (SBA) definition of a small business (having revenues of less than $24 million in any 1 year as of 2023).
According to the SBA's website at
https://www.sba.gov/content/small-business-size-standards,
AOs fall into the North American Industrial Classification System (NAICS) code 813920, Professional Organizations. The SBA defines small professional organizations as businesses having less than $24 million in total annual revenue.
Individuals and States are not included in the definition of a small entity. As its measure of significant economic impact on a substantial number of small entities, HHS uses a change in revenue of more than 3 to 5 percent.
According to the most recent tax data from ProPublica as well as the most recent audited financial statements that each AO must submit to CMS when applying for CMS approval or re-approval of its accreditation program(s) (at § 488.5(a)(16)), the 9 AOs impacted by this rule can be categorized as having current annual revenues as follows: one (1) AO with less than $1 million; two (2) AOs between $1 million and $5 million; one (1) AO between $5 million and $10 million; one (1) AO between $10 million and $15 million; and four (4) AOs greater than $15 million.[29]
As such, the requirements in this final rule with comment period will have a significant economic impact on a substantial number of small entities, which are defined as greater than 5 percent of impacted small entities. As shown in Table 6, three (3) of the nine (9) AOs, or 33 percent, would be significantly impacted by the requirements in this final rule with comment period, with a change in revenue of more than 3 to 5 percent for these AOs. We note here that, in the RFA section of the proposed rule (89 FR 12058), we included a statement that the Secretary certified that “this proposed rule would not have a significant economic impact on a substantial number of small entities”. We did not receive any public
( printed page 36462)
comments on this certification statement.
In our preparation of the COI, RIA, and RFA analysis sections of this final rule with comment period, we noted that we sometimes made assumptions about the applicability of the requirements to all of the AOs that may have overestimated the economic impact of this rule on the smallest AOs. For example, in our analysis of the impact of the requirement at § 488.5(a)(8), which will require AO surveyors to take the CMS surveyor training, we assumed an average of 75 surveyors for each AO. This number is most likely significantly higher than the number of surveyors, the 3 smallest AOs actually employ and for whom they would be paying 35 hours of each surveyor's salary to take the CMS training. Our use of this higher number on average led to our estimate of $248,430 per AO in annual costs for this requirement, a significant impact on the revenues of the three smallest AOs with a change in revenue ranging from 7 percent to 29 percent.
Additionally, we assumed the impact of this requirement as an annual cost for each AO when it is highly unlikely that each AO will have 75 or more of its surveyors taking the CMS training every year. We expect the annual numbers to be much lower for the nine AOs, especially for the three smallest AOs. After we published the proposed requirement in February 2024, we also realized that many of the AOs would most likely substitute or add the CMS training to their own individual surveyor training programs for which they are already paying their surveyors to take. Therefore, we believe that the requirement at § 488.5(a)(8) might not add any, or very little, additional cost burden to an AO's annual costs, with any required surveyor trainings constituting usual and customary business practices for all nine AOs.
We also considered whether the impact of the requirements related to AO fee-based consulting services and our estimated cost burden should be attributed equally to each AO (as we have done in this section), regardless of its size and/or whether the AO actually provides such consulting services. Our decision to attribute these costs equally across all nine AOs certainly accounts for more significant costs for the three smallest AOs than it does for the four largest AOs in terms of its impact on revenues. In addition, section 1102(b) of the Act requires us to prepare a regulatory impact analysis if a rule may have a significant impact on the operations of a substantial number of small rural hospitals. This analysis must conform to the provisions of section 604 of the RFA. For purposes of section 1102(b) of the Act, we define a small rural hospital as a hospital that is located outside of a metropolitan statistical area and has fewer than 100 beds. This rule pertains solely to AOs. Therefore, the Secretary has certified that this final rule with comment period will not have a significant impact on the operations of a substantial number of small rural hospitals.
Table 7—Regulatory Flexibility Act Analysis
Revenue group
Number of
AOs in group
Average
annual revenue
per group
Estimated
average annual
cost per firm
Average cost
divided by
average revenue
(%)
≤ $1 million
1
$1,000,000
$287,341
29
> $1 million
≤ $5 million
2
3,950,000
287,341
7
> $5 million
≤ $10 million
1
6,300,000
287,341
5
> $10 million
≤ $15 million
1
11,400,000
287,341
3
> $15 million
4
79,200,000
287,341
<1
All AOs
9
20,370,000
287,341
1
F. Unfunded Mandates Reform Act (UMRA)
Section 202 of the Unfunded Mandates Reform Act of 1995 (UMRA) also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2026, that threshold is approximately $193 million. This final rule with comment period will not impose a mandate that will result in the expenditure by State, local, and Tribal Governments, in the aggregate, or by the private sector, of more than $193 million in any 1 year.
G. Federalism
Executive Order 13132 establishes certain requirements that an agency must meet when it promulgates a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on State and local governments, preempts State law, or otherwise has Federalism implications. This rule will not have a substantial direct effect on State or local governments, preempt States, or otherwise have a Federalism implication.
H. E.O. 14192, “Unleashing Prosperity Through Deregulation”
Executive Order 14192, entitled “Unleashing Prosperity Through Deregulation” was issued on January 31, 2025, and requires that “any new incremental costs associated with new regulations shall, to the extent permitted by law, be offset by the elimination of existing costs associated with at least 10 prior regulations.” This final rule with comment period is neither a regulatory nor a deregulatory action, due to imposing no more than
de minimis
costs.
VIII. Waiver of Notice of Proposed Rulemaking
At § 488.4 in this final rule with comment period, we have made technical changes with minor re-wording of the proposed requirements and the existing requirements to make the provisions more understandable. These changes were made in the interest of clarity and do not constitute any changes in policy, nor they do establish any new requirements in addition to those already proposed and finalized in this rule.
We ordinarily publish a notice of proposed rulemaking in the
Federal Register
and invite public comment on the proposed rule. The notice of proposed rulemaking includes a reference to the legal authority under
( printed page 36463)
which the rule is proposed, and the terms and substances of the proposed rule or a description of the subjects and issues involved. This procedure can be waived, however, if an agency finds good cause that a notice-and-comment procedure is impracticable, unnecessary, or contrary to the public interest and incorporates a statement of the finding and its reasons in the rule issued. Because, as we have explained here, the changes to § 488.4 that we are making in this final rule with comment period are for the purposes of greater clarity in the wording of the provisions and are not intended as new policy or additional requirements beyond what already exists in the CFR or what has been previously proposed with public comments received and addressed in this final rule with comment period, we believe that a notice-and-comment procedure is both impracticable and unnecessary, and that it would be contrary to the public interest to delay this rule through such a procedure.
Therefore, we find good cause to waive the notice of proposed rulemaking and to issue this final rule with comment period.
This final regulation is subject to the Congressional Review Act provisions of the Small Business Regulatory Enforcement Fairness Act of 1996 (5 U.S.C. 801et seq.) and has been transmitted to the Congress and the Comptroller General for review.
IX. Response to Comments
Because of the large number of public comments we normally receive on
Federal Register
documents, we are not able to acknowledge or respond to them individually. We will consider all comments we receive by the date and time specified in the
DATES
section of this preamble, and, when we proceed with a subsequent document, we will respond to the comments in the preamble to that document.
Mehmet Oz, Administrator of the Centers for Medicare & Medicaid Services, approved this document on June 11, 2026.
Fee-based consulting services
mean those services provided by an accrediting organization (AO), or its consulting division or separate business entity (such as a company or corporation) that provides such services, for the review of a [particular] facility's standards, processes, policies, and functions for compliance with the AO's standards and the Medicare requirements through simulation of a real survey, such as a mock survey, with comprehensive written reports of findings and early intervention and action to correct deficiencies prior to an actual accreditation survey.
* * * * *
Geographic regions
—CMS uses specified geographic regions of the Unites States to measure whether an accrediting organization's accreditation program meets the definition of “national in scope.” For this purpose, the United States is divided into the following five geographic regions:
(1)
Northeast:
Delaware, District of Columbia, Maryland, Pennsylvania, Virginia, West Virginia, New York, New Jersey, Puerto Rico, Virgin Islands, Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, and Vermont;
(2)
Southeast:
Alabama, Florida, Georgia, Kentucky, Mississippi, North Carolina, South Carolina, and Tennessee;
(4)
Central:
Iowa, Kansas, Missouri, and Nebraska; Colorado, Montana, North Dakota, South Dakota, Utah, Wyoming;
(5)
South:
Arkansas, Louisiana, New Mexico, Oklahoma, and Texas;
(6)
Western:
American Samoa, Arizona, California, Hawaii, Commonwealth of the Northern Mariana Islands, Guam, Alaska, Idaho, Nevada, Oregon, Washington.
* * * * *
National accrediting organization
means an accrediting organization that is national in scope and accredits provider or suppliers, under a specific accreditation program.
National in scope
means that the providers and suppliers accredited by an accrediting organization under a specific accreditation program, are widely located geographically across the United States. The requirement for “national in scope” has two components. First, the accrediting organization must have accredited at least five providers or suppliers under the accreditation program in question. Second, the five providers or suppliers accredited by the accrediting organization under that accreditation program must be geographically located in at least five out of the six geographic regions.
Process disparity rate
means, for a direct observation validation survey, the difference between the observed survey process findings and the expected survey process findings expressed as a percentage.
* * * * *
Unannounced survey
means a survey that is conducted without any prior notice of any type, through any means of communication or forums, to the facility to be surveyed, and therefore, is unexpected to the facility until the arrival onsite by surveyors. This also means that the accrediting organizations must schedule their surveys so that the facility is unable to predict when they will be performed.
General rules for a CMS-approved accreditation program for providers and suppliers.
(a) CMS approves a national provider or supplier accreditation program and grants it “deeming authority” if, after the application procedures set out in § 488.5, CMS finds under § 488.5(e)(2)(i) that such accreditation program provides CMS with reasonable assurance as defined at § 488.1, and that all providers and suppliers accredited by such program are in compliance with all applicable Medicare conditions or requirements.
( printed page 36464)
(1) Accreditation by a CMS-approved accreditation acts as a recommendation that CMS deem such provider or supplier to be in compliance with such conditions or requirements, and to certify such provider or supplier to participate in Medicare.
(2) A provider or supplier granted deemed status is subject to validation surveys as set out at § 488.9.
(3) The accrediting organizations that accredit Medicare-certified providers and suppliers must include the applicable Medicare regulatory language as their minimum accreditation standards.
(4) The accrediting organizations that accredit Medicare-certified providers and suppliers must use a survey process comparable to the processes set out in the CMS State Operations Manual, or as issued via policy memorandums, and approved by CMS, as defined in § 488.5.
(b) The following requirements apply for termination of a provider's or supplier's Medicare participation agreement on CMS recognition of its accreditation provided by an Accrediting Organization:
(1) If CMS terminates the participation agreement of a provider or supplier, CMS will no longer recognize or accept the accreditation provided by an accreditation organization to that provider or supplier as demonstrating that the Medicare requirements have been met by such provider or supplier; and
(2) If CMS terminates the participation agreement of a provider or supplier, the terminated provider or supplier must meet all requirements set forth at § 489.57 before a new agreement with that provider or supplier for Medicare participation will be approved.
4. Section 488.5 is amended by—
a. Revising paragraphs (a)(3), (4), (5), (6), (8), (10), (12) and (13); and
Application and re-application procedures for national accrediting organizations. (a) * * *
(3) A detailed crosswalk (in table format, as specified by CMS) that identifies, for each of the applicable Medicare conditions (as defined in § 488.1) or requirements, the exact language of the organization's comparable accreditation requirements and standards. Such crosswalk must include the language of the CMS requirements and standards, and those accreditation standards that exceed the CMS conditions.
(4) A detailed description of the organization's survey process including, but not limited to, the core activities of the survey process such as, but not limited to, documentation supporting Pre Survey Preparation/Offsite Preparation, Entrance Interview/Activities, Information Gathering/Investigation, Analysis of Information, Exit Conference, Post Survey Activities/Statement of Deficiencies activities, to confirm that a provider or supplier meets or exceeds the Medicare program requirements, and maintains the integrity of the survey process, which is intended to be a non-biased evaluation of a facility's ability to provide safe care and protect the health and safety of patients. This description must include all of the following information:
(i) Frequency of surveys performed and an agreement by the organization to re-survey every accredited provider or supplier, through unannounced surveys, no later than 36 months after the prior accreditation effective date, including an explanation of how the accrediting organization will maintain the schedule it proposes. If there is a statutorily mandated survey interval of less than 36 months, the organization must indicate how it will adhere to the statutory schedule.
(ii) Documentation demonstrating the comparability of the organization's survey process and surveyor guidance to those required for State survey agencies conducting Federal Medicare surveys for the same provider or supplier type, in accordance with the applicable requirements or conditions of participation or conditions for coverage or certification.
(iii) Copies of the organization's survey forms, guidelines, and instructions to surveyors, including, but not limited to, specific processes of how surveyors survey facilities for the core survey activities: Governing Body, Patient Rights, Emergency Preparedness, Quality Assessment and Performance Improvement, Medical Staff, Nursing Services, Medical Records Services, and Infection Control. This would also include interpretive guidelines and survey probes, including patient and staff interview questions, and processes used by surveyors when interviewing facilities for compliance based on each of the specific survey standards, comparable to those instructions required for State survey.
(iv) Documentation demonstrating that the organization's survey reports identify, for each finding of non-compliance with accreditation standards, the comparable Medicare CoPs, CfCs, conditions for certification, or requirements.
(v) Description of the organization's accreditation survey review process, to include, but not limited to, processes for review of medical records; medical staff credentialing procedures based on services provided; staff record review to review for competency and personnel files; adequate number of patient observations; and confidential patient interviews and staff interviews.
(vi) Description of the organization's procedures and timelines for notifying surveyed facilities of non-compliance with the accreditation program's standards.
(vii) Description of the organization's procedures and timelines for monitoring the provider's or supplier's correction of identified non-compliance with the accreditation program's standards, including the deadlines for initial and reaccreditation surveys, accreditation decisions, as well as the investigative and organizational process which the accrediting organization uses to make these determinations.
(viii) A statement acknowledging that, as a condition for CMS approval of a national accrediting organization's accreditation program, the organization agrees to provide CMS with the following information as part of its initial and renewal applications and, upon request from CMS, and as part of the data submissions required under paragraph (a)(11)(ii) of this section:
(A) a copy of all survey reports, including, but not limited to, initial, re-survey, and complaint survey reports, upon request by CMS, and
(B) any other information related to survey activities as CMS may require (including corrective action plans).
(ix) A statement acknowledging that the accrediting organization will provide timely notification to CMS when an accreditation survey or complaint investigation identifies an immediate jeopardy as that term is defined at § 489.3 of this chapter. Using the format specified by CMS, the accrediting organization must notify CMS within 2 business days from the date the accrediting organization identifies the immediate jeopardy.
(x) For accrediting organizations applying for approval or re-approval of CMS-approved hospice programs, a statement acknowledging that the accrediting organization (AO) will include a statement of deficiencies (that is, the Form CMS-2567 or a successor form) to document findings of the hospice Medicare conditions of participation in accordance with section 1822(a)(2)(A)(ii) of the Act and will submit such in a manner specified by CMS.
( printed page 36465)
(xi) Documentation summarizing the AO's staff training programs, whether web-based electronic or hard-copy materials, on how the AO provides training or education to surveyors on the AO's survey processes, and, where applicable, highlight differences from CMS survey processes.
(5) The criteria the accrediting organization uses in determining the size and composition of the organization's survey teams for the type of provider or supplier to be accredited. These criteria at a minimum should address survey team size and composition based on:
(i) The size of the facility to be surveyed, based on average daily census;
(ii) The complexity of services offered, including outpatient services;
(iii) The type of survey to be conducted;
(iv) Whether the facility has special care units or off-site clinics or locations;
(v) Whether the facility has a historical pattern of serious deficiencies or complaints; and
(vi) Whether new surveyors are to accompany a team as part of their training.
(6) The overall adequacy of the number of the organization's surveyors to ensure sufficient amount of time is allotted to complete all survey activities, including how the organization will increase the size of the survey staff to match growth in the number of accredited facilities while maintaining re-accreditation intervals for existing accredited facilities.
* * * * *
(8) A description of the content and frequency of the organization's in-service training it provides to survey personnel, including the training materials provided, and, with respect to CMS training, a statement acknowledging that:
(i) The accrediting organization will ensure all of its surveyors complete two mandatory CMS online documentation courses and the relevant program-specific CMS online basic surveyor training course (established for State survey agency surveyors), initially, and thereafter when updates are necessary;
(ii) The required CMS online surveyor training will be completed by each existing surveyor before serving on a survey team (except as a trainee); and
(iii) The accrediting organization must document in the staff personnel records for each surveyor, that the CMS online surveyor documentation and basic training courses were completed and the date of completion. The statement must acknowledge that the accrediting organization will maintain documentation of the initial completion and any subsequent completions.
* * * * *
(10) The organization's policies and procedures to avoid conflicts of interest, (as defined in paragraph (a)(10)(v) of this section) including the appearance of conflicts of interest, involving individuals who conduct surveys or participate in accreditation decisions. These policies and procedures will include the following:
(i) The accrediting organization's policies and procedures for separation of its fee-based consulting services from its accreditation services;
(ii) The accrediting organization's policies and procedures for protecting the integrity of the accrediting organization's accreditation program, including the requirements of § 488.8(i) and (k);
(iii) The accrediting organization's policies and procedures for the prevention and handling of potential or actual conflicts of interest that could arise from situations in which an accrediting organization owner, surveyor, or other employee has an interest in or relationship with a State survey agency or with a healthcare facility to which the accrediting organization provides accreditation services. Such interests or relationships include, but are not limited to:
(A) Being employed as a State survey agency surveyor;
(B) Being employed in a healthcare facility that is accredited by the accrediting organization;
(C) Having an ownership, financial, or investment interest in a healthcare facility that is accredited by the accrediting organization;
(D) Serving as a director of or trustee for a healthcare facility that is accredited by the accrediting organization;
(E) Serving on a utilization review committee of a healthcare facility that is accredited by the accrediting organization;
(F) Accepting fees or payments from a health facility or group of health facilities that is/are accredited by the accrediting organization;
(G) Accepting fees for personal services, contract services, referral services, or for furnishing supplies to a healthcare facility that is accredited by the accrediting organization;
(H) Providing consulting services to a healthcare facility that the accrediting organization accredits;
(I) Having members of their immediate family engaged in any of the above stated activities. The term “immediate family member” is defined as any person with which the accrediting organization owner(s), surveyors or other employees have a lineal or immediate familial or marital relationship, including a husband or wife, birth or adoptive parent, child, or sibling; stepparent, stepchild, stepbrother, or stepsister; father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law, or sister-in-law; grandparent or grandchild; and spouse of a grandparent or grandchild.
(J) Engaging in any activities during the course of the survey of the facility that would be or cause a conflict of interest.
(iv) The accrediting organization's policies and procedures for notification of CMS when a conflict of interest is discovered.
(v) For the purposes of this section, a conflict of interest exists when an accrediting organization, the accrediting organization's successors, transferees, or assigns, the accrediting organization owner(s), surveyors, or other employees, or the immediate family members of the accrediting organization owners(s), surveyors, and other employees have an employment, business, financial, or other type of interest in or relationship with a healthcare facility the accrediting organization accredits.
* * * * *
(12) The organization's procedures for responding to, and investigating, complaints against accredited facilities, including policies and procedures regarding referrals to appropriate licensing bodies and ombudsman programs, when applicable. This would also include:
(i) Accrediting organization's process for triaging and categorizing complaints about the surveyed facility;
(ii) Timeframes for responding to complaints and a method to track and trend complaints received with respect to the accrediting organization's accredited facilities;
(iii) Procedures and persons responsible for the review of plans of corrections and procedures for follow up if the plans of corrections are not adequate;
(iv) Accrediting organization requirements for plans of corrections for standard-level deficiencies;
(v) Follow-up survey procedures and monitoring of condition-level findings;
(vi) Procedures for addressing immediate jeopardy deficiencies; and
(vii) Sharing of previous deficiency findings or complaints with survey teams.
(13) The organization's accreditation status decision-making process,
( printed page 36466)
including its policies and procedures for granting, withholding, or removing accreditation status for facilities that fail to meet the accrediting organization's standards or requirements, assignment of less than full accreditation status or other actions taken by the organization in response to non-compliance with its standards and requirements. The organization must furnish the following:
(i) A description of all types and categories of accreditation decisions associated with the program for which approval is sought, including the duration of each.
(ii) The accrediting organization's general notification procedures to notify CMS, including the timeframes for notification of any decision to revoke, withdraw, or revise the accreditation status of a specific deemed status provider or supplier. Such notification must be made within 3 business days from the date the organization takes an action.
(iii) A statement acknowledging that the organization agrees to notify CMS (in a manner CMS specifies) of any decision to revoke, withdraw, or revise the accreditation status of a specific deemed status provider or supplier, within 3 business days from the date the organization takes an action.
(iv) The organization's process for facilities that withdraw from accreditation, to include timeframes for notification to CMS and the process for surveying facilities which may require an upcoming survey.
* * * * *
(21) A statement certifying that, in response to a written notice from CMS notifying the organization that one of its accredited providers or suppliers has been terminated from the Medicare/Medicaid program, the accrediting organization agrees to terminate or revoke its accreditation of the terminated provider or supplier within 5 business days from receipt of said written notice, and not re-accredit the provider until CMS has approved the provider or supplier for participation in Medicare.
(22) A declaration by each surveyor of any employment, business, financial or other interests in or relationships with a State survey agency or a healthcare facility the accrediting organization accredits as described in paragraph (a)(10)(iii) of this section, which must be updated and submitted to CMS upon request and during each application review process.
(2) Analysis of the results of the validation surveys under § 488.8(a)(4), surveys from substantial allegations of noncompliance, and the process disparity rate as determined from direct observation validation surveys.
* * * * *
(4) When an accrediting organization's performance measure scores, as determined from l direct observation validation surveys, reveal that the accrediting organization's accreditation survey activities do not meet an acceptable performance threshold established by CMS, the accrediting organization will be required to submit an acceptable plan of correction that meets the requirements set forth below:
(i) The accrediting organization's acceptable plan of correction must be submitted to CMS for review within 10 business days of CMS notification of not meeting acceptable performance. An acceptable plan of correction must:
(A) Document specific actions being taken by the accrediting organization to address improving performance.
(B) Document the timeframe for implementation of this plan.
(C) Plan for ongoing monitoring of the plan of correction toward achieving an acceptable level of performance.
(D) Identify the individual responsible for implementation and monitoring of the acceptable plan of correction.
(ii) Upon review and approval of the plan of correction, CMS will provide ongoing evaluation of the progress of plan implementation.
(iii) The accrediting organization's plan of correction is subject to public reporting by CMS.
* * * * *
(i)
Restrictions on fee-based consulting provided by accrediting organizations or their fee-based consulting divisions or separate fee-based business entities.
(1) Except as provided in paragraph (i)(4) of this section, an accrediting organization, or its fee-based consulting division or separate business entity (such as a company or corporation that provides fee-based consulting), may not provide fee-based consulting services (as defined at § 488.1) to any new healthcare provider or supplier before the initial accreditation survey has been completed. For purposes of this paragraph, the term “initial survey” means the first accreditation survey performed of a healthcare provider or supplier by an accrediting organization that has not previously received accreditation services from that accrediting organization. If a healthcare provider or supplier is terminated or withdraws from the services of an accrediting organization and later retains the services of the same or a new accrediting organization, the first survey performed by the same or new accrediting organization of that healthcare provider or supplier would be considered an initial accreditation survey.
(2) Except as provided in paragraph (i)(4) of this section, an accrediting organization, its fee-based consulting division or separate business entity, such as a company or corporation that provides fee-based consulting, may not provide fee-based consulting services to a healthcare provider or supplier the accrediting organization accredits within 12 months prior to the next scheduled re-accreditation survey of that provider or supplier. For purposes of this paragraph, the term “re-accreditation survey” means any subsequent accreditation surveys performed by the accrediting organization following the initial survey.
(3) Except as provided in paragraph (i)(4) of this section, an accrediting organization, its fee-based consulting division, or separate business entity, such as company or corporation that provides fee-based consulting, may not provide fee-based consulting services to a healthcare provider or supplier, to which the accrediting organization provides accreditation services, in response to a complaint received by the accrediting organization regarding that provider or supplier.
(4) An accrediting organization, its fee-based consulting division, or separate business entity, such as a company or corporation that provides fee-based consulting, may provide fee-based consulting to the healthcare providers and suppliers it accredits only under the following circumstances:
(i) During the 24-month period after an initial or re-accreditation survey is performed.
(ii) To address complaints received and investigated by the State survey agency regarding an accrediting organization's accredited provider or supplier in which one or more condition-level or immediate jeopardy deficiencies are identified. Such fee-based consulting by an accrediting organization may occur only after the State survey agency complaint investigation and survey has been
( printed page 36467)
completed and must only address those issues identified by the complaint survey.
(iii) Fee-based consulting services provided to healthcare providers or suppliers the accrediting organization does not accredit at the time the consulting services are furnished.
(iv) Non-fee-based consulting or general education provided by the accrediting organization about their accreditation program.
(5) The accrediting organization must provide to CMS, upon request and during each application review process, a document which contains the following information:
(i) Whether the accrediting organization or an associated consulting division or company established by the accrediting organization provides fee-based consulting services;
(ii) The names and CCN numbers of all healthcare providers and suppliers to which the accrediting organization or its associated consulting division or company has provided fee-based consulting services during the previous 6-month period;
(iii) The dates the fee-based consulting services were provided to each provider and supplier;
(iv) Whether the accrediting organization has, at any time in the past provided, or is currently providing accreditation services to each healthcare provider or supplier listed in said document;
(v) For each healthcare provider and supplier listed in said document, the date of the most recent accreditation survey performed, and the date the next re-accreditation survey is due to be performed; and
(vi) A description of the fee-based consulting services provided to each healthcare provider or supplier listed in said document.
(6) If an accrediting organization provides fee-based consulting services to a healthcare provider or supplier it accredits, in violation of the restrictions set forth in paragraphs (i)(1), (2) and (3) of this section, CMS may take the following actions:
(i) CMS may place the accrediting organization on a CMS-approved accreditation program review in accordance with paragraph (c) of this section; or
(ii) CMS may involuntarily terminate the CMS approval for the accreditation programs in accordance with paragraph (g) of this section.
(j)
Accrediting organization fee-based consulting firewall policies and procedures.
(1) An accrediting organization, its fee-based consulting division, or separate business entity, such as a company or corporation that provides fee-based consulting services to the healthcare providers and suppliers the accrediting organization accredits, must have written fee-based consulting firewall policies and procedures, which, at a minimum, include the following provisions:
(i) The accrediting organization's fee-based consulting services must be provided by a separate division of the accrediting organization or separate business entity, such as a company or corporation, that is separate from the accrediting organization's accreditation division;
(ii) An accrediting organization's fee-based consulting division or separate business entity must maintain separate staff from that of the accrediting organization's accreditation divisions to ensure that the fee-based consulting division staff do not perform the accrediting organization's accreditation division functions, and that the accrediting organization's accreditation division staff do not perform fee-based consulting division functions; and
(iii) An accrediting organization's accreditation staff and surveyors are prohibited from marketing the accrediting organization's fee-based consulting services to the accrediting organization's accreditation clients.
(2) An accrediting organization that provides fee-based consulting services must submit its written consulting firewall policies and procedures to CMS by a date specified by CMS and with each application submitted seeking renewal of the CMS approval for their accreditation programs as required at § 488.5(a)(10).
(k)
Conflict of interest due to accrediting organization owner, surveyor, or other accrediting organization employee relationship with a healthcare facility accredited by the accrediting organization.
(1) If an accrediting organization owner, surveyor, or other employee, currently or within the previous 2 years, has an interest in or relationship (as defined in § 488.5(a)(10)(iii)(B) to (J)) with a healthcare facility accredited by the accrediting organization, the accrediting organization owner, surveyor or other employee must not be permitted to:
(i) Participate in the survey of that healthcare facility;
(ii) Have input into the results of the survey and accreditation for that healthcare facility;
(iii) Have involvement with the pre-or post-survey activities for that healthcare facility; or
(iv) Have contact with, or access to, the records for the survey and accreditation of that healthcare facility.
(2) For the purposes of this section, the term “immediate family member” is defined as any person with which the accrediting organization owner(s), surveyors or other employees have a lineal or immediate familial or marital relationship, including a husband or wife, birth or adoptive parent, child, or sibling; stepparent, stepchild, stepbrother, or stepsister; father-in-law, mother-in-law, son-in-law, daughter-in-law, brother-in-law, or sister-in-law; grandparent or grandchild; and spouse of a grandparent or grandchild.
(a)
Basis for survey.
CMS may require a survey of an accredited provider or supplier to validate the accrediting organization's CMS-approved accreditation process. These surveys are conducted on a representative sample basis, or in response to substantial allegations of non-compliance.
(1) For a representative sample, the survey may be comprehensive and address all Medicare conditions or requirements, or it may be focused on a specific condition(s) as determined by CMS.
(2) For a substantial allegation of noncompliance, the SA surveys for any condition(s) or requirement(s) that CMS determines is related to the allegations.
(b)
Validation surveys.
Direct observation validation surveys are performed at the discretion of CMS, on a sample of the accrediting organization's surveys and are performed concurrently by the accrediting organization and the State survey agency or CMS. The State survey agency or CMS surveyors are present to observe the accrediting organization's survey process.
(c)
Rules for direct observation validation surveys.
(1) All direct observation validation surveys will be unannounced to the accrediting organization and the facility being surveyed.
(2) The State survey agency or CMS surveyors will generally be assigned to the accrediting organization surveyors on a 1:1 basis, matching the experience of the accreditation surveyor where possible, and using the CMS-approved standards and processes to determine compliance with the Medicare conditions.
(3) The State survey agency or CMS surveyors will observe the accrediting organization survey in accordance with CMS established policies and procedures and will report the findings directly to CMS.
( printed page 36468)
(4) Where the State survey agency or CMS surveyors disagree with the findings of the accrediting organization surveyors, and these differences cannot be reconciled, CMS will render a final decision. Such decisions would not be appealable under part 498 of this chapter.
(d)
Provider or supplier not in compliance.
A provider or supplier will be deemed non-compliant with the validation process, in accordance with this section, if any of the following conditions are present:
(1) The provider or supplier refuses to authorize its accrediting organization to release a copy of their current accreditation survey to CMS; or
(2) The provider or supplier refuses to allow a validation survey.
(e)
Consequences for a finding of non-compliance.
CMS may take actions for any deficiencies identified in the direct observation validation survey in accordance with § 488.24, or may first direct the State survey agency to, or CMS may, conduct another survey of the provider's or supplier's compliance with specified Medicare conditions or requirements before taking the enforcement actions provided for at § 488.24.
(f)
Re-instating deemed status.
An accredited provider or supplier will be deemed to meet the applicable Medicare conditions or requirements in accordance with this section, if, in addition to substantive re-approval of the facility, the following requirements are met, as applicable:
(1) It withdraws any prior refusal to authorize its accrediting organization to release a copy of the provider's or supplier's current accreditation survey.
(2) It withdraws any prior refusal to allow a direct observation validation survey, if applicable.
(g)
Impact of adverse actions.
The existence of any performance review, comparability review, deemed status review, probationary period, or any other action by CMS, does not affect or limit conducting any validation survey.
PART 489—PROVIDER AGREEMENTS AND SUPPLIER APPROVAL
7. The authority citation for part 489 continues to read as follows:
(z) In the case of a provider that has been involuntarily terminated by CMS under § 489.53, or by the OIG under § 489.54, reinstatement of the provider agreement is subject to § 489.57(b).
9. Section § 489.57 is revised to read as follows:
When a provider agreement has been terminated by CMS under § 489.53, or by the OIG under § 489.54, a new agreement with that provider will not be accepted unless:
(a) CMS or the OIG, as appropriate, finds —
(1) That the reason for termination of the previous agreement has been removed and there is reasonable assurance that it will not recur; and
(2) That the provider has fulfilled, or has made satisfactory arrangements to fulfill, all of the statutory and regulatory responsibilities of its previous agreement.
(b) The terminated provider or supplier that had deemed status meets the following requirements before a new agreement with that provider or supplier may be approved:
(1) The terminated provider or supplier must become and remain under the exclusive oversight of the State survey agency for a reasonable assurance period of a length of time to be determined by CMS, for the purposes of the initial survey, certification and demonstration of compliance with the Medicare conditions.
(2) The terminated provider or supplier must remain under the exclusive oversight of the State survey agency until the State survey agency or CMS has certified that the provider or supplier is in compliance with all applicable Medicare conditions and the agreement for participation in the Medicare/Medicaid program has been approved.
(3) During the time period in which a terminated provider or supplier is not certified to participate in the Medicare program, while the prospective provider or supplier is under the oversight of the State survey agency, and while the new agreement for Medicare participation is pending, CMS will not accept or recognize accreditation from a CMS-approved accrediting organization for deeming purposes until the applicable Medicare requirements have been met or exceeded, as described in § 488.4 of this chapter.
Robert F. Kennedy, Jr.,
Secretary, Department of Health and Human Services.
6.
In section IV.B.6. of the proposed rule, we proposed to require any AO that provides fee-based consulting services, or its associated fee-based consulting division or company, have written fee-based consulting “firewall” policies and procedures.
11.
FY 2020 Report to Congress: Review of Medicare's Program Oversight of Accrediting Organizations (AOs) and the Clinical Laboratory Improvement Amendments of 1988 (CLIA) Validation Program
https://www.cms.gov/files/document/qso-22-06-ao-clia.pdf.
20.
S. Armour, Psychiatric Hospitals With Safety Violations Still Get Accreditation,
Wall Street Journal,
December 26, 2018.
21.
D. Gilbert Behind Joint Commission's `Gold Seal of Approval,' a history of missed safety violations at psychiatric hospitals,
Seattle Times,
October 9, 2019.
23.
The May 2024 OEWS release does not include data for Colorado and its areas. For more information, see the Notice Regarding Suspension of Publication of Colorado Occupational Employment and Wage Statistics.
Use this for formal legal and research references to the published document.
91 FR 36370
Web Citation
Suggested Web Citation
Use this when citing the archival web version of the document.
“Medicare Program; Strengthening Oversight of Accrediting Organizations (AOs) and Preventing AO Conflicts of Interest, and Related Provisions,” thefederalregister.org (June 16, 2026), https://thefederalregister.org/documents/2026-12069/medicare-program-strengthening-oversight-of-accrediting-organizations-aos-and-preventing-ao-conflicts-of-interest-and-re.